Ever wonder about the unique diet and language of the Neanderthals? Learn how our closest ancient relatives lived and interacted with their environment.
The Neanderthals represent the richest, most robust and most studied species in the hominin record, other than our own. And thanks to the wealth of available specimens — including their remains, tools, trash, and many more traces of their activities — scientists are piecing together a picture of their basic behavior, bit by bit.
From the unique diet of the Neanderthal to the advanced language ability and communication skill, the picture that they’re producing is far from primitive. In fact, though the Neanderthals were a solitary species before they disappeared, sticking to themselves and a couple close companions, they were also accomplished and adaptable, with behavior traits that allowed them to weather some of the coldest conditions that the world has yet seen.
Among their most adaptive behaviors were their acquisition of food, manufacture of tools and articulation of ideas through speech and symbols.
Where Did the Neanderthals Live?
In the terrains of Africa around 400,000 years ago (or maybe as many as 800,000 years ago), an ancient population of hominins started to split apart, forever changing the course of human history. While one portion of this population stayed put, the other trudged to Europe and settled there, initiating a period of geographic isolation in which the two groups accumulated their own genetic traits gradually, generation after generation.
Over time, the two groups turned into two separate species, with Homo sapiens arising in Africa and Homo neanderthalensis appearing in Europe. And it was there that these so-called Neanderthals would contend with the impossibly cold conditions of the Ice Age, adapting to the temperatures by becoming shorter, broader and bigger-brained.
What Were Neanderthal Behavior Traits?
Armed with these adaptations, the Neanderthals thrived for thousands of years, producing an ample record of their activities throughout that time. And more than transmitting their genetic material to the genomes of many modern individuals, they also left many material traces from their lives, allowing archaeologists and anthropologists to speculate about their behavior.
Overall, scientists suspect that the Neanderthals behaved in an isolated, insular way, though they also showed adaptability and intelligence in several areas. Targeting an array of prey animals according to the season, they made and manipulated an assortment of tools and probably produced simple speech. Not only that, but they also participated in symbolic behaviors, dabbling in art, personal adornment and ritual burial, according to some scientists.
Neanderthal Society
Archaeologists tend to agree that the Neanderthals occupied open settlements or took shelter from the cold in caves, cycling through a couple of separate settlements according to the time of year. In these sites, they typically resided alongside 12 to 25 relatives.
Though these tribes usually stuck to themselves, they weren’t wholly isolated. Studies suggest that they probably interacted with 10 to 20 neighboring troops, and sometimes as many as 50, with whom they shared social identities and maintained associations for mating, manufacturing and collective coping in times of trouble.
The social organization of these tribes is still stuck in the shadows, though some genetic studies state that the females pursued partners in neighboring troops in an attempt to avoid inbreeding. And while some sites show the telltale signs of treatment for the sick and injured, so, too, appear the traces of intraspecies violence, suggesting a complexity of social interaction that’s similar to our own.
Neanderthal Diet
Anatomically, the Neanderthals were omnivores, though scientists suspect that they consumed more meat than plants thanks to the reduced availability of flora in their cold climate. In fact, the chemical composition of several Neanderthal skeletons substantiates this, showing scientists that the average Neanderthal diet consisted of meat, meat and more meat (with the addition of plant material only occasionally).
As such, the Neanderthals played the part of an apex predator, targeting species according to the seasons. Munching on reindeer in the winter and red deer in the summer, the Neanderthals also ate aurochs, mammoths and boars — among other animals — though they weren’t always as widely available.
Fans of flavor, the Neanderthals applied an assortment of tricks to make their meals tastier, pounding, crushing and cooking their food over fires prior to consumption. And though archaeologists aren’t absolutely certain whether the Neanderthals manufactured these fires themselves, the species frequently manipulated flames, according to the piles of ash in many of their settlements.
Neanderthal Language
Some scientists say that the sophistication of these tools testifies to the Neanderthals’ astute observational abilities, while others think that their toolmaking was too specialized to share and spread without words and sentences. That said, whether the language of the Neanderthal was necessary to make and manipulate these tools or not, studies do demonstrate a shared neurological basis for toolmaking and speech.
Ultimately, while scientists still struggle to pinpoint the particulars of Neanderthal language and speech, anatomical and genetic analyses suggest that they possessed auditory and speech abilities similar to ours.
Neanderthal Rituals
Neanderthals weren’t constrained to verbal communication. Whether or not they spoke, archaeologists speculate that they also articulated themselves symbolically, creating a material culture of art and adornment.
Some scientists add that the Neanderthal’s tendency to deliberately bury their dead represents their symbolic thinking, too. And though there’s no single burial that’s universally interpreted as an instance of symbolism, the analysis of pollen particles at some sites suggests that the Neanderthals did decorate their dead with flowers, such as yarrow and bachelor’s button, before burial.
Neanderthal Tools
One of the clearest signs of their intelligence, Neanderthal toolmaking centered around the creation of sophisticated stone flakes (though they fashioned tools out of other materials, too). To form these flakes, the innovative Neanderthal selected a small lump of stone and struck slivers off the sides until it took the shape of a shell — flat on one side and spherical on the other. They then smashed the top of the stone several times over, hacking off a series of similarly sized slices, which they then wielded as tools.
The Neanderthals used some of these flakes without any added modification, though they turned some into points, spears, scrapers, awls and axes — among types of tools — for a wider assortment of applications.
For instance, though they thrust or threw their stone-tipped spears into their prey, they selected scrapers and awls to prepare and punch holes in hides, which they then tied together with torn animal tissues to create a simple form of clothing.
In fact, though it’s a popular theory that the Neanderthals were wiped away around 40,000 years ago when their close cousins from Africa — our own species — started streaming into their European territories, there’s not much in the archaeological record to indicate that the Neanderthals disappeared due to interspecies violence alone.
Instead, a confluence of factors probably played a part in the extinction of the species, with small population sizes, sicknesses, worsening climate conditions and interspecies competition and assimilation, all contributing to their disappearance in different areas and times.
These findings challenge the previously held views of this species as primitive beings. Understanding their unique capability for language and their sophisticated use of tools to maintain their diet underscores the importance of continued study and excavation of archeological sites.
The history of psychedelics spans the spiritual, the recreational, and the legal—and now the medical, thanks to safer and more convenient molecules and protocols
Psychedelic drugs should be administered in a safe and supportive medical setting, such as the simulated setting shown in this image from Compass Pathways. Notice that the setting’s variables include a comfortable bed, a blindfold, and a set of headphones. These variables can help patients focus on their internal well-being while receiving a drug such as Compass’s COM360, a synthetic psilocybin currently in a Phase III trial in patients with treatment-resistant depression.
Psychedelics have a rich history, one that began well before the 1950s, when chemist Albert Hofmann synthesized lysergic acid diethylamide (LSD) and psilocybin. Nonetheless, Hofmann’s work can be credited with opening a new chapter to the psychedelics story. His discoveries encouraged researchers to explore how psychedelics could be applied in psychiatry. Over a period that lasted about two decades, hundreds of studies were performed.
Some of the most promising studies suggested that psychedelics could be used to treat mental illnesses such as anxiety, depression, and alcoholism. However, as psychedelics attracted medical interest, they also stimulated recreational use. This led to the Convention on Psychotropic Substances of 1971, a United Nations treaty. It placed a global ban on all psychedelics, and it ended the production of medical-grade compounds and any related research funding and studies.
Today, we are seeing a resurgence of psychedelics and other dissociative drugs in the research and medical communities. The drugs are seen as a way to meet a growing unmet need for mental disorder treatments. Although the mechanisms of action for the drugs are still unclear, scientists believe that the drugs work by stimulating the release of reward chemicals such as dopamine or oxytocin, and by facilitating neural connectivity between brain regions. Scientists also think that the drugs enable patients to open up emotionally without suffering self-criticism. This capability may allow patients to confront and successfully address the emotional consequences of trauma.
Thus far, psychedelics have had little success securing approvals from the U.S. Food and Drug Administration (FDA). The psychedelic named ketamine gained FDA approval in 1970, but only as an anesthetic. Although ketamine has antidepressant effects and is offered off-label in intravenous form by some hospitals and clinics, the drug has not been approved by the FDA for the treatment of any psychiatric disorder. In October 2023, the FDA issued an alert about the risks of treating psychiatric disorders with compounded versions of ketamine.
More encouragingly, a ketamine derivative called esketamine won FDA approval in 2019 for patients with treatment-resistant depression. Another psychedelic, 3,4-methylenedioxymethamphetamine (MDMA), may soon gain FDA approval now that MAPS PBC, a prescription psychedelic research company, has staged two Phase III clinical trials in which MDMA was successfully used to treat patients with post-traumatic stress disorder.
Psychedelic drugs still pose many development and testing challenges, including funding and supply constraints and limited patient accessibility. Nevertheless, galvanized by the success stories, companies are tirelessly working to study more types of psychedelic and dissociative drugs, identify other diseases they can treat, and improve the drugs themselves.
Are hallucinations really necessary?
Although ketamine has been used in hospitals and veterinary clinics as an anesthetic for decades, it has attracted notice only recently for its antidepressant effects. At present, ketamine treatments are being developed for a variety of illnesses. One company doing this work is Silo Pharma.
“Drugs in this class work on the brain,” says James Kuo, MD, vice president of research and development, Silo Pharma. “And the brain is involved in many illnesses.”
Silo Pharma is testing drug candidates that could relieve the pain caused by fibromyalgia, or lessen the stress and anxiety experienced by patients with Alzheimer’s disease. The company is also addressing the timing issues that attend the use of psychedelic and dissociative drugs.
With respect to timing, psychedelics offer certain advantages—and one big disadvantage. Let’s begin with the advantages. Unlike traditional antidepressants, which take effect after several weeks, psychedelics take effect immediately. Also, psychedelics have effects that can last for months. And the disadvantage? Psychedelics can cause a “high” that lasts several hours, requiring those who receive a psychedelic treatment to stay at a clinic overnight. Many patients would be unable or unwilling to make such a time commitment.
This is a problem that Silo Pharma hopes to solve with a sustained-release delivery system. The company is developing a ketamine-loaded implant that can enable at-home drug delivery. With this implant, ketamine can be delivered so gradually that its hallucinogenic effects are diminished. Silo Pharma plans to study the effects of implant-delivered ketamine on patients with fibromyalgia to determine if hallucinations are necessary for treatment.
“There is a big debate within the psychedelic community about whether the hallucinogenic effect has to occur for a therapeutic benefit,” Kuo says. “No one truly knows the answer.”
Increasing accessibility
The association that psychedelic drugs have with wild trips is quite a burden for drug developers and medical professionals. It has contributed to skepticism and resistance to psychedelics. Federal regulations alone have resulted in some of these drugs, such as MDMA, being in short supply. Many companies are reluctant to commit to production.
PharmAla Biotech is not one of those companies. One of the reasons it was founded was to help overcome the global MDMA shortage by manufacturing and distributing MDMA to research laboratories and clinics worldwide—wherever studying and prescribing MDMA is legal. The company is currently supporting over a dozen clinical trials in the United States, Canada, and Australia.
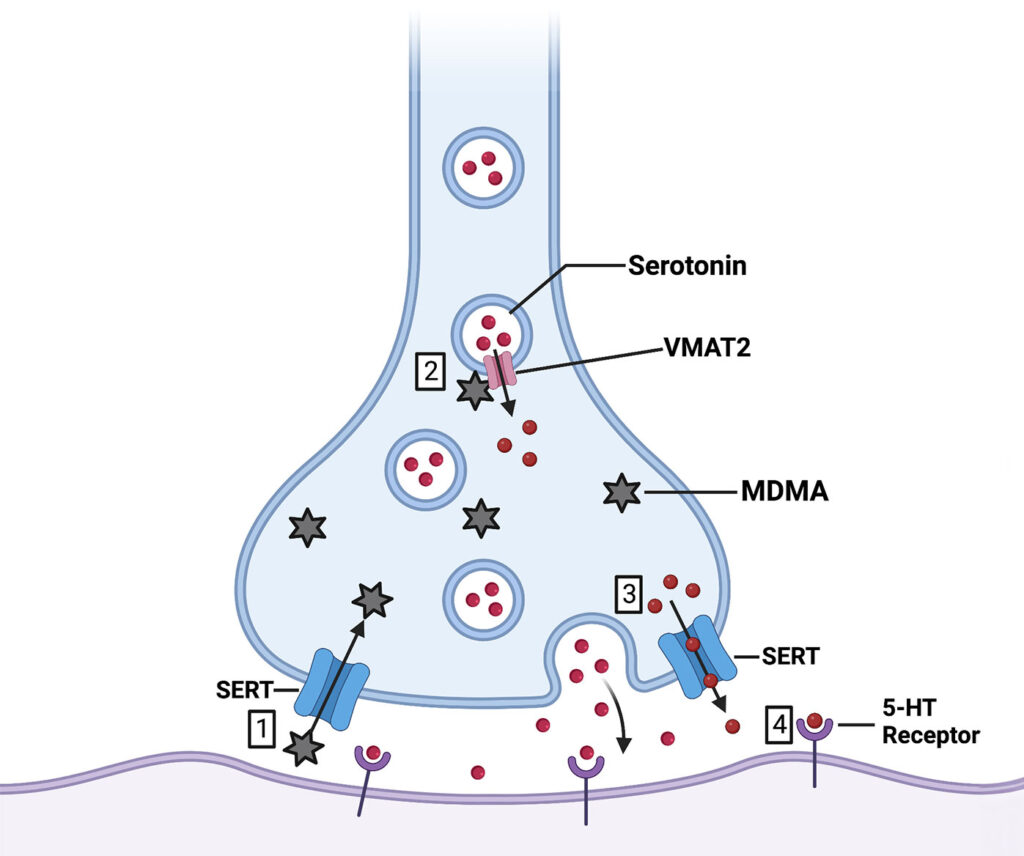
A mechanism of action for MDMA has been suggested by research involving PharmAla Biotech, a company focused on ensuring the supply and enhancing the safety of MDMA and its analogs. 1. Synaptic MDMA binds to SERT and is transported into the cytosol. 2. MDMA binds to VMAT2 and causes it to release vesicular 5-HT. 3. Cytosolic 5-HT rises in concentration and is transported into the synapse. 4. Synaptic 5-HT binds to various receptors. 5-HT: 5-hydroxytryptamine; MDMA: 3,4-methylenedioxymethamphetamine; SERT: serotonin transporter. VMAT2: vesicular monoamine transporter type 2.
While the results are promising, the side effects associated with MDMA, such as a rise in blood pressure and temperature and in body temperature, limit the patient population to those without any indication of cardiac issues. However, PharmAla Biotech is seeking to overcome this challenge as well and thereby expand the number of patients who could benefit from this drug.
“We’ve identified regions of the molecule that bind to receptors and cause it to be toxic, and we’ve changed that chemistry,” says Harpreet Kaur, PhD, vice president of research at PharmAla Biotech. “It still binds to the receptors and does the work on the transporters that we need to show the efficacy, but it doesn’t bind with the same intensity to the negative receptors.”
In animal studies, PharmAla Biotech has demonstrated that its molecule, ALA-002, does not result in a rise in body temperature or blood pressure. ALA-002 also has a much lower abuse potential than generic MDMA. A Phase II trial will begin in 2024 to treat social anxiety in autistic adults.
Minimizing adverse effects
Tactogen is another company working to make MDMA safer—safe enough so that it could be taken at home, increasing treatment accessibility. The company is developing new molecules based on the MDMA structure that minimize adverse side effects such as blood pressure changes and the “high” feeling, while still maintaining the positive effects.
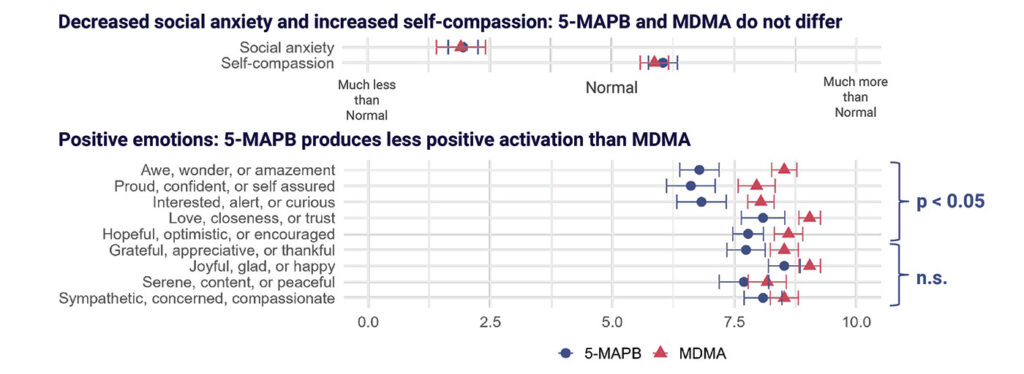
Tactogen’s candidate compounds, developed to minimize adverse events, contain the chemical substructure benzofuran. In a preliminary analysis comparing another benzofuran-based molecule, 5-MAPB, to MDMA, Tactogen scientists found no difference in the degree of change in social anxiety and self-compassion. However, 5-MAPB did not have as strong an effect on high-energy, positive emotions as did MDMA, suggesting potentially lower abuse liability.
“MDMA and drugs in its class seem to help people contemplate without discomfort things that would normally be upsetting,” says Matthew Baggott, PhD, the co-founder and CEO of Tactogen. “Traumatic events that would normally cause panic can be evaluated in a grounded, sympathetic manner that weakens the hold the events have on people. This type of pharmacotherapy seems to help people get unstuck and move forward with their lives. We seek to retain the self-compassionate, nonreactive effects that make the molecules so useful for mental health.”
Tactogen has several promising candidate compounds in development. Preclinical tests in animals suggest that they are well tolerated, retain the key effects of MDMA without depleting serotonin, and may have durable fast-acting antidepressant effects. Tactogen is preparing for clinical trials and anticipates beginning Phase I trials with healthy volunteers and Phase II trials in patients with post-traumatic stress disorder within 18 months.
Creating a long-lasting response
Another psychedelic drug showing great promise as a treatment for mental health disorders is psilocybin, the hallucinogenic compound found in certain mushrooms. For example, a synthetic psilocybin from Compass Pathways has performed well in patients with treatment-resistant depression. Phase III testing of the drug, COMP360, started in 2023.
Compass reports that a single dose of COMP360 could have long-lasting effects, acting more durably than esketamine, for example. (Esketamine is often given weekly.) Compass’s Phase III program will investigate whether a second or third dose could be more effective for some patients. Even in these cases, and even with psilocybin treatment taking several hours longer than esketamine, this would greatly reduce the number of doctor visits, potentially leading to greater patient compliance.
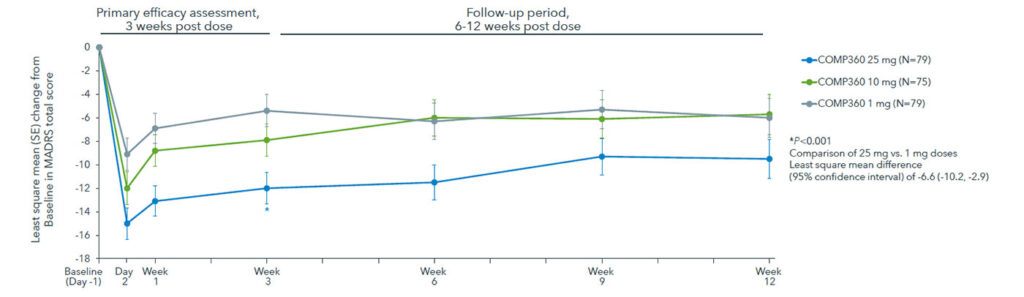
Compass Pathways demonstrated the efficacy of its proprietary, synthetic formulation of psilocybin, COMP360, on patients with treatment-resistant depression in a Phase IIb trial. The MADRS score (a depression rating) showed a highly significant and clinically relevant effect at the week 3 primary endpoint with a 25 mg dose compared to a 1 mg dose. The benefit of the 25 mg dose was evident at day 2 and week 1 following administration, confirming the rapid-acting nature of the effect.
“We’re very encouraged by the success of esketamine, which shows that this kind of time-demanding treatment can be achieved within the U.S. healthcare system,” says Guy Goodwin, MD, PhD, chief medical officer of Compass Pathways. “[It’s significant that these] inroads can be made with a very demanding program, where patients comply and actually come back for more, and we think that we’re offering an advantage over that.”
In Compass’s Phase IIb trial, a single 25 mg dose of COMP360 reduced depression scores significantly more than a 1 mg dose and resulted in a 20.3% sustained response rate at the end of the study, 12 weeks after treatment.
Overall, the effects were well tolerated. However, in the 233 patients, there were 19 serious adverse events, including suicidal thoughts and self-injury in about 5% of the study population. These are not unusual considering the patient group, and Compass will further characterize the safety profile of COMP360 in its Phase III trials.
Compass is also working on treatments for other mental health disorders and is nearing completion of an open-label, Phase II trial on patients with post-traumatic stress disorder. The company plans to publish the results in the coming months.
Making a treatment worthy of funding
Forward-thinking drug developers like those mentioned in this article are exactly what some investors are looking for. These investors believe that it’s not enough for companies to focus on what the drugs can do, but that companies also need to consider how their drugs will be accessed and what safeguards will be in place to avoid their abuse, especially considering the vulnerability of the population that would use these drugs.
“What does the future and success look like if these treatments get approved and rolled out into the clinic?” asks Dana Watt, PhD, principal at Breakout Ventures. “When you take medications that are conducted in a brick-and-mortar setting that require a lot of staff, there’s a big risk of having some problems that we’ve seen in other areas of assembly-line medicine.”
Dialysis centers and ketamine clinics have both met their fair share of concerns over their safety practices and high costs. But in addition to the risk of abuse, physical infrastructure and staffing require a lot of capital. Those companies developing safer, at-home psychedelic treatments could be a way to reduce costs while also reaching a larger population.
Overall, investors such as Breakout Ventures are exercising due caution before investing. They are waiting for more clinical evidence of the effectiveness of the new psychedelic treatments and more detailed exit and financing information.
“This is such a nascent area, and there haven’t been a lot of success stories yet,” Watt observes. “But when we have something like this that has been used for hundreds of years, I think one of the really interesting things is the maturity of the psychedelic story and how the passed-down wisdom has real scientific weight behind it.”
For people with hard-to-treat depression, a non-invasive technique called transcranial magnetic stimulation (TMS) can provide relief.
Approved over a decade ago, transcranial magnetic stimulation (TMS) is moderately effective. Tailoring the treatment to individual brains may improve results.
In the mid-1970s, a British researcher named Anthony Barker wanted to measure the speed at which electrical signals travel down the long, slender nerves that can carry signals from the brain to muscles like those in the hand, triggering movement. To find out, he needed a way to stimulate nerves in people.
Researchers had already used electrodes placed on the skin to generate a magnetic field that penetrated human tissue — this produced an electric current that activated the peripheral nerves in the limbs. But the technique was painful, burning the skin. Barker, at the University of Sheffield in England, and his colleagues started to work on a better method.
In 1985, with promising results under their belts, they tried positioning the coil-shaped magnetic device they’d developed on participants’ heads. The coil emitted rapidly alternating magnetic pulses over the brain region that controls movement, generating weak electrical currents in the brain tissue and activating neurons that control muscles in the hand. After about 20 milliseconds, the participants’ fingers twitched.
The technique, now called transcranial magnetic stimulation (TMS), has proved a vital tool for investigating how the human brain works. When targeted to specific brain regions, TMS can temporarily inhibit or enhance various functions – blocking the ability to speak, for instance, or making it easier to commit a series of numbers to memory. And when brain imaging technologies such as functional magnetic resonance imaging (fMRI) emerged in the 1990s, researchers could now “see” inside people’s brains as they received TMS stimulation. They could also observe how neural pathways respond differently to stimulation in psychiatric illnesses like schizophrenia and depression.
In recent decades, this fundamental research has yielded new treatments that alter brain activity, with TMS therapies for depression at the fore. In 2008, the US Food and Drug Administration approved NeuroStar, the nation’s first TMS depression device, and many other countries have since sanctioned the approach.
Yet even though TMS is now a widely available depression treatment, many questions remain about the method. It’s not clear how long the benefits of TMS can last, for example, or why it appears to work for some people with depression but not others. Another challenge is disentangling the effects of TMS from the placebo effect — when someone believes that they will benefit from treatment and gets better even though they’re receiving a “sham” form of stimulation.
Whether TMS can “cure” depression “is an open question — there’s evidence for and against,” says David Pitcher, a cognitive neuroscientist at the University of York who wrote a 2021 overview in the Annual Review of Psychology on using TMS to study human cognition. But as researchers fine-tune the approach and run more sophisticated clinical trials, TMS is emerging as a powerful tool for dissecting depression’s complexities — and for some people, loosening its grip.
From electric fish to magnets
TMS may be relatively new, but using electricity as medicine is ancient. As early as the 1st century CE, Roman physicians recommended using live electric torpedo fish to treat headache. Almost two millennia later, in the 1930s, physicians discovered that inducing brain seizures with electricity could reduce symptoms of schizophrenia and other forms of mental illness.
That was the beginning of electroconvulsive therapy (ECT) — pejoratively known as shock therapy. The practice spread rapidly despite the risk of memory loss, confusion and injuries from muscle spasms. Administering ECT without fully informing patients about the therapy and its risks also raised ethical concerns, an issue that medicine as a whole was seriously grappling with at the time.
Eventually, muscle relaxants, anesthetics and more stringent consent protocols improved ECT, although side effects such as headache and temporary short-term memory loss are still reported. ECT remains one of the most effective treatments for people who don’t respond to first-line antidepressant treatments such as serotonin reuptake inhibitors (SSRIs), a group of drugs that includes Zoloft and Prozac.
Yet both those drugs and ECT are difficult to control precisely, because they affect the whole brain. A more targeted approach is deep brain stimulation (DBS), which involves directly stimulating neurons with electrodes that are surgically implanted in regions known to affect mood and motivation. DBS has shown promise in pilot studies and was approved for investigative use in 2022, but has yet to receive clinical approval.
TMS, by contrast, requires no surgery and has fewer side effects than ECT, says Alvaro Pascual-Leone, a neurologist at Harvard Medical School. Though it’s not as easy to target to a specific brain region as DBS, it is much more precise than antidepressant drugs or ECT.
Pascual-Leone began investigating magnetic stimulation to treat major depressive disorder in the early 1990s. It excited him because of the ability to noninvasively focus the stimulation, and its few and relatively minor side effects, which commonly include scalp discomfort, tingling, spasms and lightheadedness and, rarely, seizures and hearing loss.
Although its mechanisms aren’t fully understood, TMS appears to act by reconfiguring neural circuits, kickstarting more typical communication between different brain areas, says Noah S. Philip, a psychiatrist at Brown University who researches TMS for treating depression.
At rest, people with depression often have reduced activity levels in an area of the brain called the dorsolateral prefrontal cortex (DLPFC) compared with non-depressed individuals, neuroimaging studies have shown. The region is a primary site for TMS therapy, says Philip. A hub for short-term memory, planning and abstract reasoning, the DLPFC is connected to several brain circuits implicated in depression: the salience network, which helps to focus attention on some things and ignore others; the default mode network, which is active when a person is not engaged in any particular task; and the executive network, key to planning, decision-making and impulse control. Together, these circuits underlie our ability to focus on relevant information and switch our attention between self-directed thinking and our environment.
Scientists think that abnormal communication between the networks can lead to the constant rumination, self-criticism and tendency to overly focus on negative aspects in life that people with depression often experience. Using fMRI to measure how nodes in the networks communicate before and after TMS, Philip, among other researchers, has found that multiple sessions of TMS can restore more typical activity. He says the change can endure beyond a year and can possibly be maintained longer with additional TMS treatments.
The sustained effects of TMS are likely due to the remodeling of neuronal connections brought on by microscopic changes to brain cells, Philip says. Studies have shown that TMS can stimulate neurons to sprout new dendrites, the branched appendages that receive signals from other neurons.
An early clinical trial found that people with severe depression who received daily TMS for several weeks were up to four times as likely to go into remission as participants in control groups, who were fitted with a TMS device but didn’t receive actual stimulation. In later studies that lacked control groups — meaning both the patients and the doctors knew TMS was being administered — 30 percent to 40 percent of patients who hadn’t improved with medications went into remission, defined by a low score on a standard measure such as the Hamilton Depression Rating Scale. That’s roughly on par with the number of people who respond well to antidepressant medications, according to a 2013 review in Current Opinion in Psychiatry.
Still, many questions remain — including whether better results can be gained by targeting specific regions in individual patients. “Some people with depression experience sadness, others have more of a lack of motivation or apathy,” says Pascual-Leone. “Some people eat too much; others eat too little.” Unlike more general treatments, he says, TMS holds such targeting potential.
Bespoke brain stimulation
In many clinics and research labs, the process of determining where to place TMS coils on a person’s head is relatively simple. The FDA-sanctioned method harks back to Barker’s original experiments: A participant sticks their thumb out like a hitchhiker, and technicians move the magnetic coil around their scalp until the electrical stimulation hits a part of the motor cortex that makes their thumb involuntarily twitch. Using this spot as their landmark, the technicians then move the coil to a position that targets the left DLPFC.
The approach is moderately effective, but many researchers think it doesn’t adequately account for the large variations in brain structure among individuals. Increasingly, scientists are using fMRI and other brain imaging technologies to tailor TMS stimulation to each person’s unique brain structure and observe how it affects their neural activity patterns. “An exciting advance in the last 10 years with TMS is to use it on patients, then neuroimage their brain to look at changes in the connectivity between the DLPFC and the areas we know it’s connected to,” says Pitcher of the University of York.
A team of investigators at Stanford University, led by psychiatrist Nolan Williams, director of the Stanford Brain Stimulation Lab, is one of the groups developing this combined approach. In a small 2021 study, the team used fMRI scans, which measure changes in blood flow associated with brain activity, to locate a small subregion in the DLPFC in individual patients. This subregion’s activity shows an inverse relationship to that of another brain area, the subgenual cingulate (SGC): In people who are experiencing depression, the SGC’s activity is boosted while the DLPFC subregion’s activity is lowered. Conversely, the more active the node in the DLPFC, the less active the SGC becomes. The SGC, for its part, appears to influence the default mode network, anchoring people in negative patterns of self-rumination.
In the Stanford study, Williams and colleagues targeted the DLPFC subregion in 29 people with what’s known as treatment-resistant depression: They scored “moderate to severe” on a standard assessment that considers how they responded to previous depression treatments and the duration and severity of their symptoms. The group received an experimental, accelerated treatment regimen with more than one daily TMS session. To control for a potential placebo effect, some group members were randomly assigned to receive sham stimulation that sounded and felt like TMS but didn’t deliver the electromagnetic pulses.
After five days of treatment, 79 percent of the participants who received the focused TMS experienced remission, compared with 13 percent of the control group. The team also observed that stimulating the area of the DLPFC that’s most strongly connected with the SGC normalizes the relevant connections among the three regions. “You see it when you scan people after,” Williams says.
Stanford researcher Nolan Williams and his colleagues have developed a new, TMS-based treatment for depression, guided by fMRI. In 2022, the US Food and Drug Administration cleared the approach for commercialization.
One participant in his early sixties, Tommy Van Brocklin, had battled depression for about 45 years. In recent years, the medication he had been taking stopped working.
The five-day treatment made him feel “like a tree being pecked by a woodpecker,” because of the knocking sounds that the TMS device emits, he jokes. But on day three, he noticed a difference in his mood: “Everything seemed to kind of kick into gear, and it was good.”
The researchers believe this individualized approach to TMS treatment could be a fast, effective intervention for suicidal patients. In 2022, Williams’s method passed an important regulatory hurdle: The FDA granted permission to commercialize it.
Seeing such high remission rates after just five days of treatment — a highly practical intervention — is exciting, says William T. Regenold, director of a research unit that studies noninvasive neuromodulation at the US National Institute of Mental Health. He and his colleagues are currently conducting a clinical trial investigating changes in brain activity in severely depressed patients who receive TMS along with talk therapy. “The idea is to have a synergistic effect between the psychotherapy and the TMS,” he says.
By adjusting the treatment to each person’s brain anatomy, the Stanford study’s success is “very aligned with the notions of precision medicine — of individually targeted interventions,” says Pascual-Leone.
But there’s still much work ahead. One urgent challenge is to tease out the benefits of stimulation from the placebo effect; some research suggests that this effect plays a role in the improvements that many experience from TMS. This problem isn’t unique to brain stimulation, but is common to all depression treatments. Several meta-analyses of the placebo effect for antidepressant medications, for example, have found that people who get inactive pills experience a 20 percent to 40 percent improvement in their symptoms, typically measured by one of several standard questionnaires.
Research groups are starting to achieve clearer, more impressive outcomes using brain scans to guide individualized stimulation, as the Stanford team did. But they’ll need more studies to determine if TMS will find similar success in larger populations, as well as in groups such as teenagers, the elderly and people who have conditions that often accompany depression, such as anxiety and post-traumatic stress. Some labs are experimenting with the design of TMS devices — comparing figure-8-shaped magnetic coils to ones shaped like butterfly wings, for example — and altering the frequency of stimulation to see how that alters brain activity and treatment outcomes.
Still, many fundamental questions about TMS remain. Although scientists know it disrupts normal neuronal firing, “we don’t really understand how TMS works in a mechanistic way” to alter brain states like mood, says Pitcher. One reason is that researchers can’t record activity from a single neuron in a human being and do TMS at the same time, he says. It’s not clear why certain frequencies of TMS appear to ramp up activity in some brain regions, while turning it down in other areas — or how the new neuronal connections spurred by TMS affect the different brain networks.
“Fortunately, we can do that work, advancing science while helping people with disabling diseases,” says Pascual-Leone. “That’s an amazing position to be in.”
For people with hard-to-treat depression, a non-invasive technique called transcranial magnetic stimulation (TMS) can provide relief.
Approved over a decade ago, transcranial magnetic stimulation (TMS) is moderately effective. Tailoring the treatment to individual brains may improve results.
In the mid-1970s, a British researcher named Anthony Barker wanted to measure the speed at which electrical signals travel down the long, slender nerves that can carry signals from the brain to muscles like those in the hand, triggering movement. To find out, he needed a way to stimulate nerves in people.
Researchers had already used electrodes placed on the skin to generate a magnetic field that penetrated human tissue — this produced an electric current that activated the peripheral nerves in the limbs. But the technique was painful, burning the skin. Barker, at the University of Sheffield in England, and his colleagues started to work on a better method.
In 1985, with promising results under their belts, they tried positioning the coil-shaped magnetic device they’d developed on participants’ heads. The coil emitted rapidly alternating magnetic pulses over the brain region that controls movement, generating weak electrical currents in the brain tissue and activating neurons that control muscles in the hand. After about 20 milliseconds, the participants’ fingers twitched.
The technique, now called transcranial magnetic stimulation (TMS), has proved a vital tool for investigating how the human brain works. When targeted to specific brain regions, TMS can temporarily inhibit or enhance various functions – blocking the ability to speak, for instance, or making it easier to commit a series of numbers to memory. And when brain imaging technologies such as functional magnetic resonance imaging (fMRI) emerged in the 1990s, researchers could now “see” inside people’s brains as they received TMS stimulation. They could also observe how neural pathways respond differently to stimulation in psychiatric illnesses like schizophrenia and depression.
In recent decades, this fundamental research has yielded new treatments that alter brain activity, with TMS therapies for depression at the fore. In 2008, the US Food and Drug Administration approved NeuroStar, the nation’s first TMS depression device, and many other countries have since sanctioned the approach.
Yet even though TMS is now a widely available depression treatment, many questions remain about the method. It’s not clear how long the benefits of TMS can last, for example, or why it appears to work for some people with depression but not others. Another challenge is disentangling the effects of TMS from the placebo effect — when someone believes that they will benefit from treatment and gets better even though they’re receiving a “sham” form of stimulation.
Whether TMS can “cure” depression “is an open question — there’s evidence for and against,” says David Pitcher, a cognitive neuroscientist at the University of York who wrote a 2021 overview in the Annual Review of Psychology on using TMS to study human cognition. But as researchers fine-tune the approach and run more sophisticated clinical trials, TMS is emerging as a powerful tool for dissecting depression’s complexities — and for some people, loosening its grip.
From electric fish to magnets
TMS may be relatively new, but using electricity as medicine is ancient. As early as the 1st century CE, Roman physicians recommended using live electric torpedo fish to treat headache. Almost two millennia later, in the 1930s, physicians discovered that inducing brain seizures with electricity could reduce symptoms of schizophrenia and other forms of mental illness.
That was the beginning of electroconvulsive therapy (ECT) — pejoratively known as shock therapy. The practice spread rapidly despite the risk of memory loss, confusion and injuries from muscle spasms. Administering ECT without fully informing patients about the therapy and its risks also raised ethical concerns, an issue that medicine as a whole was seriously grappling with at the time.
Eventually, muscle relaxants, anesthetics and more stringent consent protocols improved ECT, although side effects such as headache and temporary short-term memory loss are still reported. ECT remains one of the most effective treatments for people who don’t respond to first-line antidepressant treatments such as serotonin reuptake inhibitors (SSRIs), a group of drugs that includes Zoloft and Prozac.
Yet both those drugs and ECT are difficult to control precisely, because they affect the whole brain. A more targeted approach is deep brain stimulation (DBS), which involves directly stimulating neurons with electrodes that are surgically implanted in regions known to affect mood and motivation. DBS has shown promise in pilot studies and was approved for investigative use in 2022, but has yet to receive clinical approval.
TMS, by contrast, requires no surgery and has fewer side effects than ECT, says Alvaro Pascual-Leone, a neurologist at Harvard Medical School. Though it’s not as easy to target to a specific brain region as DBS, it is much more precise than antidepressant drugs or ECT.
Pascual-Leone began investigating magnetic stimulation to treat major depressive disorder in the early 1990s. It excited him because of the ability to noninvasively focus the stimulation, and its few and relatively minor side effects, which commonly include scalp discomfort, tingling, spasms and lightheadedness and, rarely, seizures and hearing loss.
Although its mechanisms aren’t fully understood, TMS appears to act by reconfiguring neural circuits, kickstarting more typical communication between different brain areas, says Noah S. Philip, a psychiatrist at Brown University who researches TMS for treating depression.
Neuroscientist Alvaro Pascual-Leone, shown at Beth Israel Deaconess Medical Center in 1998, has spent decades studying how TMS affects brain activity. Using neuroimaging techniques such as functional magnetic resonance imaging (fMRI), his lab has shown that repetitive TMS can induce lasting changes in the neural networks involved in depression and other psychiatric conditions.
At rest, people with depression often have reduced activity levels in an area of the brain called the dorsolateral prefrontal cortex (DLPFC) compared with non-depressed individuals, neuroimaging studies have shown. The region is a primary site for TMS therapy, says Philip. A hub for short-term memory, planning and abstract reasoning, the DLPFC is connected to several brain circuits implicated in depression: the salience network, which helps to focus attention on some things and ignore others; the default mode network, which is active when a person is not engaged in any particular task; and the executive network, key to planning, decision-making and impulse control. Together, these circuits underlie our ability to focus on relevant information and switch our attention between self-directed thinking and our environment.
Scientists think that abnormal communication between the networks can lead to the constant rumination, self-criticism and tendency to overly focus on negative aspects in life that people with depression often experience. Using fMRI to measure how nodes in the networks communicate before and after TMS, Philip, among other researchers, has found that multiple sessions of TMS can restore more typical activity. He says the change can endure beyond a year and can possibly be maintained longer with additional TMS treatments.
The sustained effects of TMS are likely due to the remodeling of neuronal connections brought on by microscopic changes to brain cells, Philip says. Studies have shown that TMS can stimulate neurons to sprout new dendrites, the branched appendages that receive signals from other neurons.
An early clinical trial found that people with severe depression who received daily TMS for several weeks were up to four times as likely to go into remission as participants in control groups, who were fitted with a TMS device but didn’t receive actual stimulation. In later studies that lacked control groups — meaning both the patients and the doctors knew TMS was being administered — 30 percent to 40 percent of patients who hadn’t improved with medications went into remission, defined by a low score on a standard measure such as the Hamilton Depression Rating Scale. That’s roughly on par with the number of people who respond well to antidepressant medications, according to a 2013 review in Current Opinion in Psychiatry.
Still, many questions remain — including whether better results can be gained by targeting specific regions in individual patients. “Some people with depression experience sadness, others have more of a lack of motivation or apathy,” says Pascual-Leone. “Some people eat too much; others eat too little.” Unlike more general treatments, he says, TMS holds such targeting potential.
Bespoke brain stimulation
In many clinics and research labs, the process of determining where to place TMS coils on a person’s head is relatively simple. The FDA-sanctioned method harks back to Barker’s original experiments: A participant sticks their thumb out like a hitchhiker, and technicians move the magnetic coil around their scalp until the electrical stimulation hits a part of the motor cortex that makes their thumb involuntarily twitch. Using this spot as their landmark, the technicians then move the coil to a position that targets the left DLPFC.
The approach is moderately effective, but many researchers think it doesn’t adequately account for the large variations in brain structure among individuals. Increasingly, scientists are using fMRI and other brain imaging technologies to tailor TMS stimulation to each person’s unique brain structure and observe how it affects their neural activity patterns. “An exciting advance in the last 10 years with TMS is to use it on patients, then neuroimage their brain to look at changes in the connectivity between the DLPFC and the areas we know it’s connected to,” says Pitcher of the University of York.
A team of investigators at Stanford University, led by psychiatrist Nolan Williams, director of the Stanford Brain Stimulation Lab, is one of the groups developing this combined approach. In a small 2021 study, the team used fMRI scans, which measure changes in blood flow associated with brain activity, to locate a small subregion in the DLPFC in individual patients. This subregion’s activity shows an inverse relationship to that of another brain area, the subgenual cingulate (SGC): In people who are experiencing depression, the SGC’s activity is boosted while the DLPFC subregion’s activity is lowered. Conversely, the more active the node in the DLPFC, the less active the SGC becomes. The SGC, for its part, appears to influence the default mode network, anchoring people in negative patterns of self-rumination.
In the Stanford study, Williams and colleagues targeted the DLPFC subregion in 29 people with what’s known as treatment-resistant depression: They scored “moderate to severe” on a standard assessment that considers how they responded to previous depression treatments and the duration and severity of their symptoms. The group received an experimental, accelerated treatment regimen with more than one daily TMS session. To control for a potential placebo effect, some group members were randomly assigned to receive sham stimulation that sounded and felt like TMS but didn’t deliver the electromagnetic pulses.
After five days of treatment, 79 percent of the participants who received the focused TMS experienced remission, compared with 13 percent of the control group. The team also observed that stimulating the area of the DLPFC that’s most strongly connected with the SGC normalizes the relevant connections among the three regions. “You see it when you scan people after,” Williams says.
Stanford researcher Nolan Williams and his colleagues have developed a new, TMS-based treatment for depression, guided by fMRI. In 2022, the US Food and Drug Administration cleared the approach for commercialization.
One participant in his early sixties, Tommy Van Brocklin, had battled depression for about 45 years. In recent years, the medication he had been taking stopped working.
The five-day treatment made him feel “like a tree being pecked by a woodpecker,” because of the knocking sounds that the TMS device emits, he jokes. But on day three, he noticed a difference in his mood: “Everything seemed to kind of kick into gear, and it was good.”
The researchers believe this individualized approach to TMS treatment could be a fast, effective intervention for suicidal patients. In 2022, Williams’s method passed an important regulatory hurdle: The FDA granted permission to commercialize it.
Seeing such high remission rates after just five days of treatment — a highly practical intervention — is exciting, says William T. Regenold, director of a research unit that studies noninvasive neuromodulation at the US National Institute of Mental Health. He and his colleagues are currently conducting a clinical trial investigating changes in brain activity in severely depressed patients who receive TMS along with talk therapy. “The idea is to have a synergistic effect between the psychotherapy and the TMS,” he says.
By adjusting the treatment to each person’s brain anatomy, the Stanford study’s success is “very aligned with the notions of precision medicine — of individually targeted interventions,” says Pascual-Leone.
But there’s still much work ahead. One urgent challenge is to tease out the benefits of stimulation from the placebo effect; some research suggests that this effect plays a role in the improvements that many experience from TMS. This problem isn’t unique to brain stimulation, but is common to all depression treatments. Several meta-analyses of the placebo effect for antidepressant medications, for example, have found that people who get inactive pills experience a 20 percent to 40 percent improvement in their symptoms, typically measured by one of several standard questionnaires.
Research groups are starting to achieve clearer, more impressive outcomes using brain scans to guide individualized stimulation, as the Stanford team did. But they’ll need more studies to determine if TMS will find similar success in larger populations, as well as in groups such as teenagers, the elderly and people who have conditions that often accompany depression, such as anxiety and post-traumatic stress. Some labs are experimenting with the design of TMS devices — comparing figure-8-shaped magnetic coils to ones shaped like butterfly wings, for example — and altering the frequency of stimulation to see how that alters brain activity and treatment outcomes.
Still, many fundamental questions about TMS remain. Although scientists know it disrupts normal neuronal firing, “we don’t really understand how TMS works in a mechanistic way” to alter brain states like mood, says Pitcher. One reason is that researchers can’t record activity from a single neuron in a human being and do TMS at the same time, he says. It’s not clear why certain frequencies of TMS appear to ramp up activity in some brain regions, while turning it down in other areas — or how the new neuronal connections spurred by TMS affect the different brain networks.
“Fortunately, we can do that work, advancing science while helping people with disabling diseases,” says Pascual-Leone. “That’s an amazing position to be in.”
Scientists at the Buck Institute for Research on Aging, the University of California, San Francisco, and elsewhere have proposed a strategy for repairing damaged synapses in Alzheimer’s disease and related dementias in mice. Details of the study in mouse models are available in The Journal of Clinical Investigation in a paper titled “KIBRA repairs synaptic plasticity and promotes resilience to tauopathy-related memory loss.”
Current research into potential treatments for Alzheimer’s disease focus on preventing the accumulation of toxic proteins like tau and amyloid beta in the brain, which impact memory as the disease progresses. For this study, the researchers focused on methods of reversing the damage to the synapses to restore memory. The work hinges on a postsynaptic protein called KIBRA which is encoded by WWC1, a gene linked to memory and risk of late-onset Alzheimer’s diseases in humans.
KIBRA is found in the kidneys and the brain where it is localized at the synapses. The scientists showed that levels of this protein, which is required for synapses to form memories, are lower in brains with Alzheimer’s disease. Furthermore, they found that higher levels of KIBRA in cerebrospinal fluid and lower levels in the brain corresponded to the severity of dementia. “We also found this amazing correlation between increased tau levels and increased KIBRA levels in the cerebrospinal fluid,” said Tara Tracy, PhD, an assistant professor at Buck and the study’s senior author. “It was very surprising how strong the relationship was, which really points to the role of KIBRA being affected by tau in the brain.”
The team also dug into how KIBRA affects synapse signaling. Specifically, “we wondered how the lower levels of KIBRA affected signaling at the synapse, and whether understanding that mechanism better could yield some insight into how to repair the synapses damaged during the course of Alzheimer’s disease,” said Grant Kauwe, PhD, a staff scientist at Buck and co-first author of the study.
To answer that question, they created a shortened functional version of the KIBRA protein and tested it in transgenic mice with a condition that mimics Alzheimer’s disease. The results showed that KIBRA reversed the memory impairment associated with this type of dementia and rescued mechanisms that promote synapse resilience. “Interestingly, KIBRA restored synaptic function and memory in mice, despite not fixing the problem of toxic tau protein accumulation,” said Kristeen Pareja-Navarro, PhD, a Buck research scientist and a co-first author of the study. “Our work supports the possibility that KIBRA could be used as a therapy to improve memory after the onset of memory loss, even though the toxic protein that caused the damage remains.”
With further study, the KIBRA protein could potentially be used as a biomarker of synaptic dysfunction and cognitive decline which could help with Alzheimer’s disease diagnosis and progression, treatment planning, and treatment response. A KIBRA-based therapy could also work alongside other therapies that prevent pathologic protein accumulation in the brain. “Reducing toxic proteins is of course important, but repairing synapses and improving their function is another critical factor that could help,” Tracy noted. “That’s how I see this making the biggest impact in the future.”
Tranexamic acid is highly efficacious for the treatment of melasma, with optimal outcomes seen through oral administration plus routine topical agents.
The efficacy of tranexamic acid alone against melasma is independent of the mode of administration in the long term; however, oral administration is more efficacious than intradermal administration in the short term. The greatest overall efficacy was seen with combination therapy oral tranexamic acid plus routine topical agents. These study results were published in the Journal of Cosmetic Dermatology.
Tranexamic acid, a synthetic derivative of lysine, has been confirmed as a safe and effective treatment for melasma, but consensus on the optimal mode of administration is lacking. Therefore, investigators compared several modes of treatment administration to evaluate their efficacy and safety in the management of melasma.
Investigators conducted a systemic review and meta-analysis that included 44 randomized controlled trials with a total of 3164 patients. Treatment duration in these studies varied from 1 to 6 months. Significant outcomes included melasma area severity index (MASI) measurements and adverse events. Oral tranexamic acid was administered at 500 mg per day, as were routine topical agents. Conversely, tranexamic acid was administered intradermally or through microneedling every 2 to 4 weeks at a concentration of 4 mg/mL.
Compared with tranexamic acid administered intradermally, topically, or through microneedling, oral tranexamic acid plus routine topical agents was associated with a greater and statistically significant change in MASI at weeks 4, 8, and 12, and at the last follow-up visit.
The results of the present study indicate that among the different modes of TA administration applied to melasma treatment, oTA+RTA has the best efficacy.
Among patients receiving oral tranexamic acid, the change in MASI was greater than that observed in patients receiving intradermal tranexamic acid, reaching statistical significance at week 8. Tranexamic acid administered orally yielded a statistically significant difference at week 4 compared to placebo, as did intradermal, topical, and microneedling administration, beginning at week 8.
Oral tranexamic acid alone and oral tranexamic acid plus routine topical agents each had an onset time of approximately 4 weeks. Onset time for intradermal, topical, and microneedling administration was approximately 8 weeks. Possibly owing to its high concentration and high frequency of administration, oral tranexamic acid had a more rapid effect than treatment administered intradermally or through microneedling.
Treatment with oral tranexamic acid was primarily associated with gastrointestinal discomfort and irregular menstruation. Routine topical agents were primarily associated with skin irritation, pigmentation, and contact dermatitis. Among patients receiving topical tranexamic acid, skin irritation was the only adverse event. Intradermal treatment was associated with a high incidence of pain and redness during injection. Furthermore, microneedling administration resulted in slight pain, skin irritation, and erythema among patients. Those receiving tranexamic acid plus routine topical agents experienced skin irritation, discoloration, decreased menstrual volume, and gastrointestinal discomfort.
Limitations of this systematic review and meta-analysis include the lack of subgroup analysis of the dose and frequency of treatment and lack of comprehensive safety data. Moreover, there is potential exaggeration in efficacy calculations across modes of administration due to the heterogeneity of MASI data across included studies.
The investigators concluded, “The results of the present study indicate that among the different modes of [tranexamic acid] administration applied to melasma treatment, [tranexamic acid plus routine topical agents] has the best efficacy.”
There’s an increasing link between the debilitating neurological illness and the microbes that live in our intestines.
It can start small: a peculiar numbness, a subtle facial tic, an inexplicably stiff muscle. But then time goes by — and eventually, the tremors set in.
Roughly a million people in the United States (and roughly 10 million people worldwide) live with Parkinson’s disease, a potent neurological disorder that progressively kills neurons in the brain. As it does so, it can trigger a host of crippling symptoms, from violent tremors to excruciating muscle cramps, terrifying nightmares, and constant brain fog. While medical treatments can alleviate some of these effects, researchers still don’t know exactly what causes the disease to occur in the first place.
A growing number of studies, however, are suggesting that it may be tied to an unlikely culprit: bacteria living inside our guts.
Every one of us has hundreds or thousands of microbial species in our stomachs, small intestines, and colons. These bacteria, collectively called our gut microbiome, are usually considerate guests: Although they survive largely on food that passes through our insides, they also give back, cranking out essential nutrients like niacin (which helps our body convert food into energy) and breaking down otherwise indigestible plant fiber into substances our bodies can use.
As Parkinson’s advances in the brain, researchers have reported that the species of bacteria present in the gut also shift dramatically, hinting at a possible cause for the disease. A 2022 paper published in the journal Nature Communications recorded those differences in detail. After sequencing the mixed-together genomes of fecal bacteria from 724 people — a group with Parkinson’s and another without — the authors saw a number of distinct changes in the guts of people who suffered from the disease.
The Parkinson’s group had dramatically lower amounts of certain species of Prevotella, a type of bacterium that helps the body break down plant-based fiber (changes like this in gut flora could explain why people with Parkinson’s disease often experience constipation). At the same time, the study found two harmful species of Enterobacteriaceae, a family of microbes that includes Salmonella, E. coli, and other bugs, proliferated. Those bacteria may be involved in a chain of biochemical events that eventually kill brain cells in Parkinson’s patients, says Tim Sampson, a biologist at Emory University School of Medicine and co-author of the study.
At first glance, the relationship between bacteria and brain disease isn’t exactly obvious. How can a change in gut microbes kick off a devastating neurodegenerative disorder? The relationship between the two may seem counterintuitive — but Sampson says it comes down to the subtle ways that the brain and the gut are connected.
In the walls of the intestines, a network of neurons called the enteric nervous system lets the body sense what’s going on in the gut and respond accordingly. This circuitry controls muscle movement, local blood flow, secretion of mucus, and other essential digestive functions.
Since the cells of the enteric nervous system are embedded in the gut wall, many of them come into close contact with the lumen — the cavity of the gut that contains the microbiome — where they can interact directly with biochemicals created by bacteria. Some of these are sticky proteins called curli (pronounced CURL-eye) that may be implicated in Parkinson’s.
Under normal circumstances, curli proteins let Enterobacteria build biofilms, the gooey mats that protect the microbes and help them stay put in the gut. Yet if a curli molecule touches a common protein created by nerve cells — called alpha-synuclein — that protein begins to misfold and form a dangerous mass called an aggregate. Once created, these aggregates can spread widely through the nervous system, leapfrog from cell to cell, and eventually enter the brain through the vagus nerve, the main pathway that carries signals between the brain and the gut. It’s thought that in some cases of Parkinson’s in humans, changes in the gut microbiome may activate that process, says Emeran Mayer, a gastroenterologist, and neuroscientist at UCLA and coauthor of a recent overview of the gut-brain connection in the Annual Review of Medicine.
The suspicion that the vagus plays a key role in neurodegenerative disease has been growing in recent years. A 2017 study in the journal Neurology, Mayer notes, showed that “If you cut the vagus nerve, it decreases the risk for Parkinson’s disease. That’s a pretty strong indication that … this degenerative material is transported, apparently, through the vagus nerve.”
Over the past few decades, a number of animal studies have shown that the vagus provides a physical conduit that molecules can use to move between the gut and brain — but although this neurological superhighway could play an important role in Parkinson’s, it’s still not clear if the nerve is a lynchpin in causing the disease itself.
In addition to aggregates moving through the vagus, different triggers — like the lipids, vitamins, and other organic compounds that gut bacteria produce — could travel through blood vessels to the brain, where they may cause inflammation and damage tissue. Likewise, says David Hafler, a neuroimmunologist at Yale University, immune cells that are activated in the gut may contribute to the neurological damage and dysfunction that occurs in Parkinson’s.
These immune cells, called T cells, can migrate out of the gut, enter the bloodstream, and cross the blood-brain barrier, where they may ultimately kill off neurons. This sort of autoimmune response is the driver for other neurological diseases like multiple sclerosis and Hafler reasons, so it’s feasible that it plays a role in Parkinson’s as well. In both diseases, changes in the gut microbiome could be the potential trigger.
There’s already strong evidence for this idea. In 2016, Sampson found a direct connection between gut microbes and Parkinson’s disease: Using fecal samples from Parkinson’s patients, Sampson inoculated the guts of germ-free mice (animals with no naturally occurring microbiome), and the animals quickly developed Parkinson’s symptoms. Today, using the new genetic survey of gut microbes he and his colleagues published in Nature Communications, he’s narrowing in on a few microbe families and using similar methods to reveal which precise species are the culprits.
Sampson’s approach comes with some caveats: Parkinson’s disease, after all, might be linked to multiple bacteria interacting in complex ways — so there likely won’t be a single smoking gun. It’s also not totally clear if changes in the microbiome are the root cause or if they just accelerate damage already taking place in the brain. The complexity of the microbiome is mind-boggling: There are hundreds of different types of bacteria involved, and each creates myriad molecules that affect digestion, the immune system, and other important bodily functions. Sorting through all those components and identifying how they change in the face of disease will be an important next step.
And so, as tantalizing as the links between the microbiome and Parkinson’s may be, it could be decades before people who suffer from the disorder can reap any tangible benefits. Many of the researchers examining those links, like Mayer, also warn patients to be wary of sweeping claims about drugs, supplements, or even fecal transplants — seeding the gut with microbes from another, healthy person — that “treat” Parkinson’s by altering the microbiome.
“A lot of people make a lot of money selling individual supplements, telling you that they’re going to slow your cognitive decline or prevent Parkinson’s disease,” says Mayer. But, he adds, “we don’t know the causal roles of the microbiome for sure. We know it from animal studies, so we have indirect evidence for it — but it’s been difficult to show in humans without a doubt that the microbes, and some of their signal molecules, play the main causal role.”
Until definitive answers are found, researchers like Mayer will continue to chip away at the problem, microbe by microbe
Behold! Scientists in China have announced the birth of a glowing green monkey.
Yes, it’s real. As The Independent reports, the lab-born primate has made history as the world’s first live-born “chimeric” monkey. A chimera, as the report explains, is an animal with more than two sets of DNA; in this case, the long-tailed macaque was created by combining two genetically distinct embryos of the same species.
And by all accounts, this little monkey — which, sadly, was euthanized by researchers after ten days — was a strange fellow indeed. According to the researchers’ proof-of-concept study, published Thursday in the journal Cell, the macaque had a glowing green face and fingertips, in addition to fluorescent green eyes.
The researchers aren’t just trying to build a chimeric primate for the hell of it. As the Independent notes, scientists often use chimeric mice and rats in lab settings as a means of studying embryonic development, as well as examining disease progression in living organs and tissues. Mice and rats, however, aren’t nearly as genetically similar to humans as our primate cousins are, meaning that the successful engineering of chimeric monkeys could offer humanity much more accurate — and thus, hopefully, more fruitful — means of cellular study and disease modeling. (Sorry, it’s a little sad, we know.)
“Mice don’t reproduce many aspects of human disease for their physiology being too different from ours,” senior study author Zhen Liu, a researcher at the Chinese Academy of Sciences, told CNN. “In contrast, human and monkey are close evolutionary, so human diseases can be more faithfully modeled in monkeys.”
To create the monkey, scientists took stem cells from a seven-day-old embryo — the donor embryo — and added them to another, slightly younger embryo. These embryos were then implanted into several female macaques, leading to 12 pregnancies in total. Of those twelve, six infants were born — and one, the lil’ guy in question, was born alive.
Though the monkey didn’t live for long, its successful birth represents a notable stride in genetic modification research. As ScienceAlert notes, in past attempts to create chimeric primates, the donor DNA was deeply underrepresented in the offspring’s body tissues. But this time, according to the study, donor DNA was found in 26 different types of body tissue — and in rates varying from 21 to an astonishing 92 percent, no less. These are significant increases from previous trials, and an exciting turning of the tides for genetic researchers.
Scientists seem particularly thrilled about a large aggregation of donor cells found in the primate’s brain tissue. As study coauthor Miguel Esteban, principal investigator at the Guangzhou Institute of Biomedicine and Health at the Chinese Academy of Sciences, told CNN, this finding suggests that chimeric macaques could one day be useful for “modeling neurodegenerative diseases.”
By the way, if you’re wondering why this perfect little goblin was green, it was on purpose. When the scientists combined the embryos, they added a green fluorescent protein to the donor cells — that way, they could more easily track where some of that DNA was disseminating. This in mind, the fact that it was visible from the outside-in is pretty wild.
As fascinating as this breakthrough is, however, it’s important to remember that the monkey wasn’t born healthy; if it was, researchers wouldn’t have had to euthanize the guy after only ten days. So, there’s still a long way to go in the journey toward the first truly viable chimera primate.
Regardless, this study may well be seen as a landmark trial — or at least, a trial that opens the door to future breakthroughs. RIP, little freak. You made history!
“EVERY MAJOR PHARMA COMPANY HAS INVESTED IN PARTNERSHIPS WITH AT LEAST ONE, IF NOT MULTIPLE, AI COMPANIES.”
For the first time, a drug both discovered and designed by an AI system is officially undergoing mid-stage testing in human clinical trials.
The drug called NS018_055 was developed by the biotech firm Insilico Medicine and is designed to treat idiopathic pulmonary fibrosis, a chronic lung disease known to cause often debilitating breathing problems.
The drug was approved for phase 2 trials, meaning that scientists are now testing whether the drug actually works.
According to the folks at Insilico, it could prove to be a consequential step forward for the burgeoning AI-enhanced pharmaceutical field, which could lead to a completely new — and potentially lucrative — era of drug research and development.
“This first drug candidate that’s going to Phase 2 is a true highlight of our end-to-end approach to bridge biology and chemistry with deep learning,” Insilico CEO Alex Zhavoronko said in a statement. “This is a significant milestone not only for us, but for everyone in the field of AI-accelerated drug discovery.”
The executive made some pretty lofty promises about the future of the tech. According to Zhavoronko, this new era in AI-assisted pharmaceuticals will, in theory, be defined by massive increases in the industry’s “productivity.”
“For Insilico, it is the moment of truth… but it is also a true test for AI and the entire industry should be watching,” Zhavoronkov told the Financial Times. “Our company, and it’s a big, bold claim, can double the productivity of pretty much every big pharma company.”
In other words, if the CEO is to be believed, the time it takes to develop a drug could be halved with the help of AI.
Insilico has been deploying AI models that can quickly and efficiently churn through massive datasets to come up with new molecules that can eventually be turned into a drug.
In short, the company claims to use AI to first identify a potential target for a pharmaceutical, conceptualize said pharmaceutical candidate, and then predict its effectiveness.
The company is using NVIDIA graphics processing units to power its AI, an approach that is seemingly already paying off. According to NVIDIA, coming up with the drug NS018_055 took less than 18 months, a process that usually takes up to six years.
Insilico has used its AI platform to discover 12 pre-clinical drug candidates, three of which have advanced to early clinical trials so far. Of these three, NS018_055 is the first to make it to Phase 2 trials.
“When we first presented our results, people just did not believe that generative AI systems could achieve this level of diversity, novelty and accuracy,” Zhavoronkov added in his statement. “Now that we have an entire pipeline of promising drug candidates, people are realizing that this actually works.”
Of course, these are pretty ambitious statements considering that the drug is only starting the years-long process of human clinical trials. Only time will tell if the drug is even effective in humans.
After all, as University of Michigan pharmaceutical sciences professor Duxin Sun noted in an essay in The Conversation last year, roughly 90 percent of drugs that go to clinical trials ultimately fail.
And, as the FT points out, there is precedent for failure in the sector, as exemplified by the London-based biotech AI firm Benevolent AI laying off half of its staff last month after its lead drug candidate flopped.
Despite these early warning signs, pharma firms are investing heavily in AI startups like Insilico. And with this clinical trial milestone under the company’s belt, coupled with the gold rush nature of the broader AI marketplace, we’ll likely see a lot more money flowing in.
“There is no shortage of interest,” Eric Topol, founder and director of the Scripps Research Translational Institute and the author of “Deep Medicine,” told the FT. “Every major pharma company has invested in partnerships with at least one, if not multiple, AI companies.”
“I LIKE TO THINK IT’S THE BEGINNING OF NONADDICTIVE MEDICINES FOR PAIN.”
As the opioid crisis worsens, one Boston-based pharmaceutical company has used some impressive biology to create what it says amounts to a non-addictive, non-opioid painkiller.
As the New York Times reports, Vertex Pharmaceuticals seems to have shown some promising results in Phase 3 clinical trials, announced earlier this week in a statement, for patients who experienced “moderate-to-severe acute pain” after getting surgery.
Whereas opioids generally target both the brain and the body, which ultimately leads to their addictiveness, non-opioid drugs like Vertex’s VX-548 focus on peripheral nerves, or those outside of the brain and spine, the NYT explains. By blocking pain at the source, the logic goes, it can be averted before reaching the brain and developing the kind of feedback loop that lends itself to dependency.
This concept isn’t exactly novel to Vertex. Still, as Reuters points out in its reporting on the matter, other drugmakers like Eli Lilly and Regeneron Pharmaceuticals have failed to make effective non-opioid painkillers, setting VX-548 apart.
Vertex, a publicly traded company, has not released full data or results from the Phase 3 trials. But in media interviews, researchers and analysts within and outside the company are already singing the drug’s praises as it prepares to file for approval with the Food and Drug Administration later this year.
“This has the potential to be a blockbuster,” Yale pharmacology and neuroscience expert Stephen Waxman, who was once paid a $1,000 speaking honorarium by Vertex but was not involved in the drug’s trials, told the NYT. “I like to think it’s the beginning of nonaddictive medicines for pain.”
As the press release admits, VX-548 didn’t meet its secondary goal of superior pain reduction over a combination of the opioid hydrocodone and the over-the-counter pill acetaminophen, but the company’s stock value jumped two percent regardless. As Reuters reports, the company’s stock to date has risen 35 percent in the past year as it continuously announced good news out of its trials.
“Investors and the company did not expect superiority over opioid[s],” Wells Fargo analyst Mohit Bansal told Reuters, “as there is a huge safety (and) addiction advantage even without that.”
With all the social damage wreaked by opioids, there’s no question that they remain the gold standard treatment for treating severe pain. But there’s long been a need for a middle ground between OTC medicines for pain and the heavy-duty addictiveness of opioids, which could, some analysts predict, be something of a Holy Grail if found to be safe and effective.
“I don’t think anybody expects that this drug will replace or mean the end of opioid pain medicines,” Piper Sandler analyst Christopher Raymond told Reuters, “but it absolutely offers an alternative that is sorely needed.”
Assessing connectivity across the entire brain could help identify likely ADHD development
Using neuroimaging data of nearly 12,000 participants, researchers have confirmed there is a need for a ‘whole brain approach’ to diagnosing, researching and treating attention-deficit hyperactivity disorder (ADHD).
Previous studies have focused instead on certain regions or networks in the brain, which scientists at the Oregon Health & Science University (OHSU) and the University of Minnesota Masonic Institute for the Developing Brain believe risks overlooking aspects of the condition that can be detected by zooming out and viewing the bigger picture.
“By evaluating the cumulative effects of regions across the entire brain, we are now looking at ADHD as a whole-brain issue, which could make it easier to predict which kids have ADHD and how severe it may be,” said corresponding author Michael A. Mooney, assistant professor of medical informatics and clinical epidemiology in the OHSU School of Medicine. “Down the road, we hope this will help with early identification of kids at most risk, so they can get the help they need as soon as possible.”
ADHD, which has a broad range of symptoms and severity, officially affects around 3.5% of the US population, or more than 11 million people, however, the actual figure is thought to be much higher. Presently, there is no single test that can be used to diagnose the often debilitating condition that is present in both children and adults. The best we have at the moment is a mix of medical tests to rule out other conditions, as well as anecdotal and ‘symptom checklist’ examinations, which form the basis of a diagnosis and inform treatment.
In this study, the researchers used neuroimaging data of nearly 12,000 children aged nine and 10 in the Adolescent Brain Development Study (ABCD), which mapped behavioral, social and brain development over a decade. With this, they constructed a polyneuro risk score (PNRS), to estimate the likelihood of an ADHD diagnosis based on connectivity across the entire brain.
Knowing the kind of connectivity issues associated with different ADHD symptoms, the researchers were able to provide a PNRS score based on the participants’ resting state functional connectivity magnetic resonance imaging (rs-fcMRI) data. The higher the score, the greater the correlation between known ADHD brain activity.
What they found was that there was a significant correlation between score and ADHD diagnosis, when the whole brain was taken into account.
“This is exciting, because much of the prior research has focused on individual regions of the brain, but our study was seeing that this isn’t the case across the board,” Mooney said. “In fact, there is signal from all areas of the brain that are contributing to the risk of ADHD.”
The next step, the team says, is to see if these results are consistent across different ages, with the hope of it being able to provide a robust neurological tool for diagnosis. They also hope it could help researchers zoom out to instead look at how connectivity across the brain could provide a basis for better treatment.
The current methods of diagnosis are often considered outdated, now more is known about ADHD and its many behavioral manifestations. While symptoms can involve hyperactivity, impulsivity and disruptiveness, there’s also an inattentive and distractible ‘type’, as well as a third category that’s a combination of the two extremes.
“At this stage of research, we’re still evaluating the clinical utility of these findings,” said Mooney. “However, it certainly points toward not looking at behavioral conditions in a silo. “Our hope is to continue research into this area so that in the future, we can improve the method to a point that it could actually be used in health care settings, providing ADHD risk prediction and assessment.”