Summary: A new study explores the molecular connections between Type 2 diabetes and Alzheimer’s, supporting the notion of Alzheimer’s as “Type 3 diabetes.”
This study finds that a high-fat diet suppresses a crucial gut protein, Jak3, leading to Alzheimer’s-like brain changes in mice. It underscores the importance of managing diabetes or avoiding it through diet to reduce Alzheimer’s risk.
The findings illuminate a potential path from diet through gut inflammation to brain health, offering hope for preventative strategies.
Key Facts:
Molecular Connection: The suppression of the Jak3 protein in the gut due to a high-fat diet can initiate a cascade of inflammation leading to Alzheimer’s-like symptoms in the brain.
Preventative Potential: Controlling or avoiding diabetes through diet and blood sugar management could significantly reduce the risk of developing Alzheimer’s disease.
Broad Implications: Given the vast number of U.S. adults with prediabetes, lifestyle changes to prevent diabetes may also mitigate Alzheimer’s risk, highlighting the critical intersection of diet, metabolic health, and neurodegeneration.
Source: ASBMB
New research conducted in mice offers insights into what’s going on at the molecular level that could cause people with diabetes to develop Alzheimer’s disease.
The study adds to a growing body of research on the links between Type 2 diabetes and Alzheimer’s disease, which some scientists have called “Type 3 diabetes.”
The findings suggest that it should be possible to reduce the risk of Alzheimer’s by keeping diabetes well controlled or avoiding it in the first place, according to researchers.
To find out how diet could influence the development of Alzheimer’s in people with diabetes, the researchers traced how a particular protein in the gut influences the brain.
Narendra Kumar, an associate professor at Texas A&M University in College Station, led the study.
“We think that diabetes and Alzheimer’s disease are strongly linked,” Kumar said, “and by taking preventative or amelioration measures for diabetes, we can prevent or at least significantly slow down the progression of the symptoms of dementia in Alzheimer’s disease.”
Kumar will present the new research at Discover BMB, the annual meeting of the American Society for Biochemistry and Molecular Biology, which is being held March 23–26 in San Antonio.
Diabetes and Alzheimer’s are two of the fastest-growing health concerns worldwide. Diabetes alters the body’s ability to turn food into energy and affects an estimated 1 in 10 U.S. adults. Alzheimer’s, a form of dementia that causes progressive decline in memory and thinking skills, is among the top 10 leading causes of death in the United States.
Diet is known to influence the development of diabetes as well as the severity of its health impacts. To find out how diet could influence the development of Alzheimer’s in people with diabetes, the researchers traced how a particular protein in the gut influences the brain.
They found that a high-fat diet suppresses the expression of the protein, called Jak3, and that mice without this protein experienced a cascade of inflammation starting with the intestine, moving through the liver and on to the brain.
Ultimately, the mice showed signs of Alzheimer’s-like symptoms in the brain, including an overexpressed mouse beta-amyloid and hyperphosphorylated tau, as well as evidence of cognitive impairment.
“Liver being the metabolizer for everything we eat, we think that the path from gut to the brain goes through liver,” Kumar said.
His lab has been studying functions of Jak3 for a long time, he added, and they now know that the impact of food on the changes in the expression of Jak3 leads to leaky gut. This in turn results in low-grade chronic inflammation, diabetes, decreased ability of the brain to clear its toxic substances and dementia-like symptoms seen in Alzheimer’s disease.
The good news, according to Kumar, is that it may be possible to stop this inflammatory pathway by eating a healthy diet and getting blood sugar under control as early as possible.
In particular, people with prediabetes — which includes an estimated 98 million U.S. adults — could benefit from adopting lifestyle changes to reverse prediabetes, prevent the progression to Type 2 diabetes and potentially reduce the risk of Alzheimer’s.
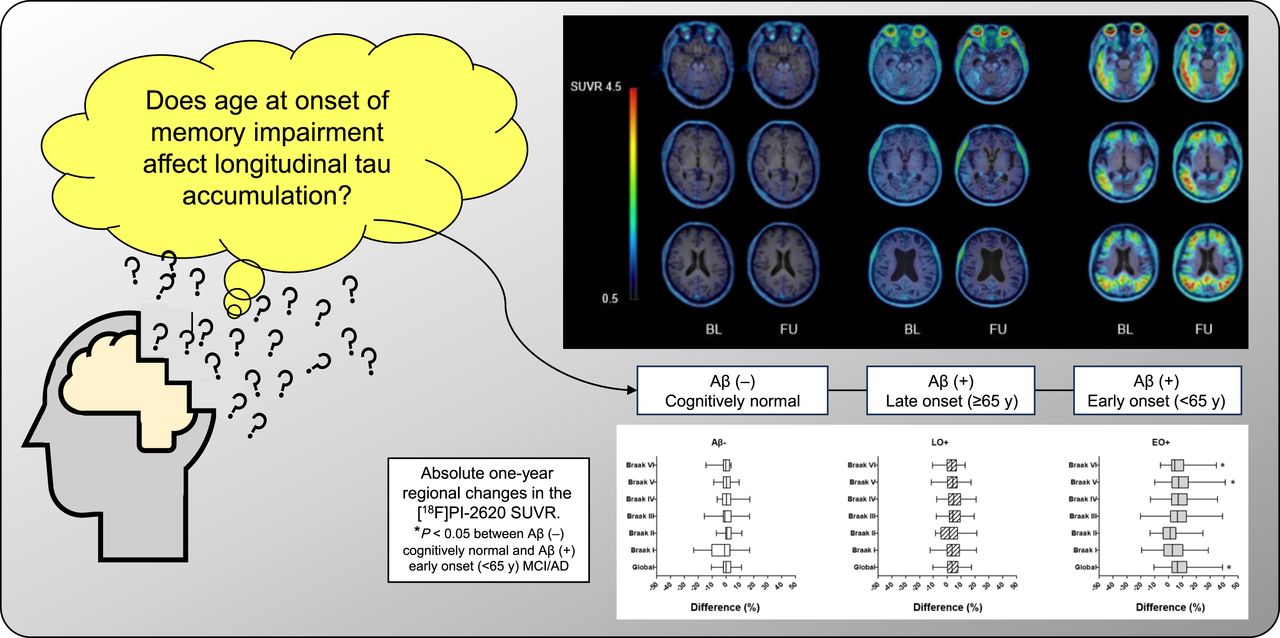
We investigated the longitudinal changes in cortical tau accumulation and their association with cognitive decline in patients in the Alzheimer disease (AD) continuum using 2-(2-([18F]fluoro)pyridin-4-yl)-9H-pyrrolo[2,3-b:4,5c′]dipyridine ([18F]PI-2620) PET. Methods: We prospectively enrolled 52 participants (age, 69.7 ± 8.4 y; 18 men and 34 women): 7 with normal cognition, 28 with mild cognitive impairment, and 17 with AD. They all completed the [18F]PI-2620 and [18F]florbetaben PET, MRI, and neuropsychologic tests at baseline and, excepting the [18F]florbetaben PET, at the 1-y follow-up. Amyloid-β (Aβ) PET images were visually scored as positive (+) or negative (−). Patients on the AD continuum, including Aβ+ mild cognitive impairment and AD, were classified into early-onset (EO+) (<65 y old) or late-onset (LO+) (≥65 y old) groups. [18F]PI-2620 PET SUV ratios (SUVRs) were determined by calculating the cerebral–to–inferior cerebellar ratio. Cortical volumes were calculated using 3-dimensional T1-weighted MRI. The correlation between tau accumulation progression and cognitive decline was also investigated. Results: The global [18F]PI-2620 PET SUVRs were 1.04 ± 0.07 in 15 Aβ− patients, 1.18 ± 0.21 in 20 LO+ patients (age, 76.7 ± 3.8 y), and 1.54 ± 0.38 in 17 EO+ patients (age, 63.4 ± 5.4 y; P < 0.001) at baseline. The global SUVR increased over 1 y by 0.05 ± 0.07 (3.90%) and 0.13 ± 0.22 (8.41%) in the LO+ and EO+ groups, respectively, whereas in the Aβ− groups, it remained unchanged. The EO+ group showed higher global and regional tau deposition than did the Aβ− and LO+ groups (P < 0.05 for each) and rapid accumulation in Braak stage V (0.15 ± 0.25; 9.10% ± 12.27%; P = 0.016 and 0.008), Braak stage VI (0.08 ± 0.12; 7.16% ± 10.06%; P < 0.006 and 0.005), and global SUVR (P = 0.013) compared with the Aβ− group. In the EO+ group, the changes in SUVR in Braak stages II–VI were strongly correlated with the baseline and changes in verbal memory (P < 0.03). The LO+ group showed higher tau accumulation in Braak stage I–IV areas than did the Aβ− group (P < 0.001 for each). In the LO+ group, the change in SUVR in Braak stages III and IV moderately correlated with the change in attention (P < 0.05), and the change in SUVR in Braak stages V and VI moderately correlated with the change in visuospatial function (P < 0.005). Conclusion: These findings suggest that [18F]PI-2620 PET can be a biomarker to provide regional and chronologic information about tau pathology in the AD continuum.
Alzheimer’s disease is the most common type of dementia.
There is currently no cure for Alzheimer’s disease. While anyone can develop Alzheimer’s, several factors may influence a person’s risk of developing the condition. These include:
Now, researchers from Rutgers University present evidence suggesting the amount and location of abdominal fat a person has can impact their brain health and cognition if they are at a high risk of developing Alzheimer’s disease.
Abdominal fat comprises subcutaneous or visceral fat located deep within the body’s abdominal cavity and surrounds organs such as the pancreas and liver.
A study presented at the annual meeting of the Radiological Society of North America in November 2023 reported visceral fat could trigger brain changes related to Alzheimer’s up to 15 years before diagnosis.
Research published in August 2018 found that higher levels of abdominal fat in older adults are associated with cognitive decline.
Dr. Michal Schnaider Beeri, director of the Herbert and Jacqueline Krieger Klein Alzheimer’s Research Center at Rutgers Brain Health Institute and senior author of this study, explained to Medical News Today why they decided to study the impact of abdominal fat on brain health and cognition in people with a high risk of developing Alzheimer’s disease.
“The pathology that develops in the brain of Alzheimer’s patients begins in middle age,” Dr. Schnaider Beeri detailed. “Also, the associations of risk factors — such as obesity — with Alzheimer’s (are) strongest when the risk factors evolve in midlife. So we have a great interest in focusing (on) midlife as a critical epoch for potential prevention of Alzheimer’s disease.”
“We focus on (the) offspring of Alzheimer’s patients because they are at higher risk for developing the disease — a group of people for whom discoveries for prevention would be of the highest clinical value,” she continued. “(And) in general, the focus of research on the relationships of obesity with Alzheimer’s has been on body mass index (BMI) which does not represent (fat well), especially in older adults.”
For this study, Dr. Schnaider Beeri and her team recruited 204 healthy middle-aged adults with a history of Alzheimer’s disease in their families. Study participants had a mean age of about 60, and 60% of the group was female.
Participants underwent abdominal magnetic resonance imaging (MRI) to measure their visceral and subcutaneous fat and measurements of their cognition and brain volumes.
Upon analysis, researchers found a higher amount of abdominal fat in their participant pool was associated with lower total gray matter volume in the brain and cognition.
They also discovered that middle-aged men at high risk for Alzheimer’s disease with higher amounts of pancreatic fat were correlated with lower cognition and brain volumes, compared to female participants.
“The finding regarding pancreatic fat cannot be named a surprise since this is likely the only study that investigated the potential role of pancreatic fat in brain and cognition,” Dr. Schnaider Beeri said.
“Diabetes and pre-diabetes — which occur because of impaired pancreatic function — are consistently associated with a higher risk of dementia, and our study suggests the involvement of pancreatic fat in this association.”
“Regarding the stronger findings in women, this was a surprise to us and we are investigating the causes for such differences,” she added. “Yet, our findings strongly suggest that research on the role of fat on brain aging must be done in the context of sex differences.”
After reviewing this study, Dr. Verna R. Porter, a board certified neurologist and director of the Dementia, Alzheimer’s Disease, and Neurocognitive Disorders at Pacific Neuroscience Institute in Santa Monica, CA, told MNT that this study underscores the importance of comprehensive risk assessment and management strategies for patients.
“Focusing not only on traditional risk factors like genetics and lifestyle but also on metabolic factors such as abdominal fat distribution,” Dr. Porter added.
For the next steps in this research, Dr. Porter said she would like to see further exploration into the mechanisms underlying the relationship between abdominal fat and brain health, particularly in different population groups and across various stages of Alzheimer’s disease progression.
“Longitudinal studies could provide valuable insights into the long-term impact of interventions targeting abdominal fat reduction on cognitive function and Alzheimer’s risk. Moreover, investigating the efficacy of targeted interventions, such as dietary modifications or exercise programs specifically aimed at reducing abdominal fat, would be beneficial in developing personalized approaches for Alzheimer’s risk management.”
Dr. Mir Ali, bariatric surgeon and medical director of MemorialCare Surgical Weight Loss Center at Orange Coast Medical Center in Fountain Valley, CA, said the main causes of abdominal obesity are poor diet — primarily too much sugar, alcohol, trans-fat, and not enough protein. Dr. Ali was not involved in the study.
“Unfortunately, you cannot target weight loss to certain areas like your abdomen,” Dr. Ali told MNT. “However, losing weight overall will lead to a reduction in truncal obesity. A diet high in fiber and protein as well as low in sugar is a great place to start.”
“Drinking plenty of water throughout the day can help support metabolism and promote feelings of fullness, potentially reducing overeating and abdominal fat accumulation,” Dr. Porter said.
Providing care for a loved one with Alzheimer’s disease immediately inducts you into an unfortunate club of people whose relatives have this condition. No one wants to be a member, but given that around 5.5 million people in the United States have Alzheimer’s, many, many people are.
Although there’s no roadmap for dealing with life when someone you love has Alzheimer’s, if you’re in this position, it can help to hear from other people in the same unbelievably tough spot. Here, we spoke with some Alzheimer’s caregivers to find out a few things they wish they’d known at the start of their journeys.
1. “You have to learn how to grieve losing someone while they’re still alive.”
Amy L. became one of her father, Art’s, caregivers after he was diagnosed with Alzheimer’s disease in 2012. Amy says she was ill-prepared for how much grief she experienced before her father passed away in 2015.
“You have to learn how to grieve losing someone while they’re still alive,” she tells SELF. “You always think about grief as something that happens once someone passes away, but this illness really changes who they are.”
Alzheimer’s disease is a progressive brain disorder, meaning someone has more (and more intense) symptoms as time passes. These symptoms include cognitive issues like confusion, difficulty doing normally minor tasks such as getting dressed, and memory loss that eventually becomes so severe your loved one may not recognize you, according to the National Institute on Aging (NIA). It would be crushing if these changes happened all at once, but the progression of Alzheimer’s stages is its own kind of awful.
“Each little change was devastating,” Amy says, describing difficult times like realizing that Art could no longer go to the bathroom alone, or his moments of clarity that something was wrong with his health. “You have to learn to cope with the new reality, and then another change comes,” Amy says. “When he passed, it was a whole different onslaught of grief.”
Amy wishes she had seen a grief counselor or therapist while she was going through this. “It would have been so helpful,” she says.
2. “I wish I had known from the beginning to just listen to and trust myself, because I am the only one who knows what it feels like to be in my own circumstance.”
Emmy G.’s mom, Linda, was diagnosed with Alzheimer’s disease five years ago and is now in a later stage of the disease. Emmy tells SELF that helping to care for her mother is “difficult and emotionally depleting.”
It’s not only that Emmy has had to adjust to her mom’s condition—it’s also changed how Emmy relates to other people besides her mom. “Being in my early 20s, it is hard to explain what I am feeling to those my own age, and for a while I felt distant from friends,” Emmy says. “In addition, older friends/family who have gone through similar experiences feel the need to judge or criticize how I treat my mom and offer up ‘suggestions’ for [how] I should act.
However, as Emmy gets more confident in her ability to care for her mom, people have commented less, and it affects her less when they do say something. “I wish I had known from the beginning to just listen to and trust myself, because I am the only one who knows what it feels like to be in my own circumstance,” she says.
3. “Alzheimer’s affects everyone differently.”
There’s a long list of potential symptoms people may exhibit as their Alzheimer’s evolves, but not everyone will experience each symptom. For instance, some people with Alzheimer’s disease undergo personality changes, but Cecelia N. tells SELF that her grandmother didn’t experience this before passing away in 2012. “However, some families aren’t that lucky,” she says. “Alzheimer’s affects everyone differently.”
4. “The most comforting feeling I found was talking to someone who could relate.”
Having a loved one with Alzheimer’s disease can be incredibly isolating, Amy says. After her father was diagnosed, she read everything she could online about the disease and tried to find others to talk to who had been through the same thing. “The most comforting feeling I found was talking to someone who could relate,” she says. “It made me feel not so alone.”
Amy says she even got in touch with two famous people who had been through a similar experience. “I reached out not because they were famous but because they had been where I was,” she says. “They both wrote me back, and it meant so much.”
Emmy also emphasizes the importance of this kind of support. She found help and resources through the Alzheimer’s Foundation of America, which has a national helpline staffed by licensed social workers from 9 A.M. to 9 P.M. Eastern Monday through Friday. You can reach the hotline at 866-232-8484.
The extent of resources out there for those dealing with Alzheimer’s and their loved ones might surprise you. Peggy M.’s husband, Tom, was diagnosed with early-onset Alzheimer’s in 2012 at the age of 57. (Early-onset Alzheimer’s means a person shows symptoms before they’re 65.)
“Our local Alzheimer’s Association offers some wonderful programs,” Peggy tells SELF. “We attend support groups and a memory café weekly.” (A memory café is a supportive gathering for those with memory loss and their loved ones to socialize and connect with each other.) Tom even sings in something known as the Forgetful Friends Chorus which is a choir based in Manassas, Virginia, made up of people living with early-stage Alzheimer’s. “We have made lifelong friends through these activities,” Peggy says. “Connecting with others who know what [we’re] going through and who can offer support and suggestions for dealing with the disease’s various challenges has been very helpful.”
5. “I should have said, ‘Can you come over on a Wednesday without me having to ask so I can go to the gym for an hour or get my nails done?’”
Amy says people regularly told her she should keep living her life while Art was sick, but she couldn’t bear to take much time for herself due to guilt. This contributed to her becoming completely overwhelmed, she says. Looking back, she wishes she would have told those who offered to help that she basically needed to be forced into self-care.
“I should have said, ‘Can you come over on a Wednesday without me having to ask so I can go to the gym for an hour or get my nails done?’ If someone came over and just said, ‘Go!’ I would have,” she says.
On a related note, Cecelia says her family had “no idea of the community resources that were available,” including respite care, which provides short-term and time-limited breaks for families and unpaid caregivers. “These programs help out families so much,” she says. “It would have been great to know of those.”
6. “Alzheimer’s hits you hard financially.”
“Financially, we had no idea,” Cecelia says. “My grandmother passed away in 2012, and just last year we paid the nursing home off. It takes a financial toll on the whole family.”
Kim B., whose husband, Jeff, was diagnosed with early-onset Alzheimer’s disease in 2016 at the age of 51, agrees. “Alzheimer’s hits you hard financially,” she tells SELF. “Jeff was the main breadwinner in our family. He qualified for social security disability, but it pays only a small fraction of what he was earning.” The couple currently has three kids in college, and Jeff’s parents live with them. “I am currently working two full-time jobs in addition to being a caregiver, wife, and mom,” Kim says. “My days start at 6:30 A.M. and do not end until 10 P.M. It gets pretty exhausting.”
7. “There will be good days and bad.”
“Initially, it scared me when Jeff was having an ‘off’ day—short-tempered and reserved—but I have learned those days come and go,” Kim says. “I, too, have good days and bad days, and that is OK! On my bad days, I acknowledge it and tell myself tomorrow will be better,” Kim says. “There will be good days and bad. I always tell my kids, it is OK to have a bad day, but then you have to get up and keep going.”
Kim has also learned what contributes to Jeff’s bad days, like traveling, which can be helpful when it comes to reducing the challenges Alzheimer’s can cause.
8. “Appreciate your loved one every single day. Be grateful for how much they can do in that day, in that moment.”
Emmy recommends trying to find joy in your current relationship with your loved one, as impossible as that may feel sometimes. “[I] wasted an entire year crying about the future rather than appreciating what my mom was still capable of,” Emmy says.
Now Emmy tries to savor the experiences she and her mom can still share. She does this by taking Linda out to a meal for just the two of them, traveling to nearby towns where Linda used to spend a lot of time, and dancing together to music that Linda’s loved for years. “Appreciate your loved one every single day,” Emmy says. “Be grateful for how much they can do in that day, in that moment.”
Biomarkers of Alzheimer’s disease are present early, and their levels evolve over time, according to a large study by researchers at Beijing’s Innovation Center for Neurological Disorders. The biological markers of Alzheimer’s progression included amyloid-beta (Aβ)42, the ratio of Aβ42 to Aβ40, phosphorylated tau 181, total tau, neurofilament light chain, and hippocampal volume. Notably, these signs’ appearance and persistence changed with time.
As cognitive impairment progressed, the team reports, the changes in CSF biomarker levels in the Alzheimer’s disease group initially accelerated and then slowed.
The study was published this week in The New England Journal of Medicine. Jianping Jia, MD, PhD, is the lead author.
It is estimated that over 50 million people worldwide have some form of dementia, and that by 2050 this number will climb to over 150 million. While new drugs are being introduced that finally address the underlying biology of the disease, these are few and don’t have much effect. It is believed that early diagnosis will aid drug development and treatment.
Preclinical Alzheimer’s disease is characterized by normal cognitive function and abnormal levels of specific cerebrospinal fluid (CSF) biomarkers. This preclinical stage is typically followed by mild cognitive impairment, which sometimes progresses to clinically apparent dementia.
Notably, changes in biomarker levels can begin 15 to 20 years before clinical signs of Alzheimer’s disease. Changes in CSF biomarkers. such as levels of amyloid-beta (Aβ), total tau, phosphorylated tau 181, and neurofilament light chain (NfL) have been indicators in preclinical Alzheimer’s disease that become abnormal sequentially rather than simultaneously.
There’s also a difference between familial and sporadic Alzheimer’s disease. In the sporadic disease a person’s clinical course, beginning with normal cognition and progressing to Alzheimer’s disease, “cannot be predicted,” the authors write. Also, they note, past studies have had an “Underrepresentation of Asian populations… In addition, the relatively short follow-up periods in previous studies do not reflect the lengthy trajectory over decades of biomarker alterations leading to the onset of Alzheimer’s disease.”
This team compared 648 people eventually diagnosed with Alzheimer’s with an equal number who did not develop the disease. All were enrolled in the China Cognition and Aging Study from January 2000 through December 2020. A subgroup of these patients underwent cerebrospinal fluid (CSF) testing, cognitive assessments, and brain imaging at two-year–to–three-year intervals.
The first sign the researchers saw was positive amyloid testing—18 years or 14 years prior to diagnosis depending on the test used. Differences in tau were also detected, followed by a marker of trouble in how neurons communicate. A few years later, differences in brain shrinkage and cognitive test scores between the two groups became apparent.
Specific findings were that CSF and imaging biomarkers in the Alzheimer’s disease group diverged from the cognitively normal group specific points: amyloid-beta (Aβ)42, 18 years; the ratio of Aβ42 to Aβ40, 14 years; phosphorylated tau 181, 11 years; total tau, 10 years; neurofilament light chain, nine years; hippocampal volume, eight years; and cognitive decline, six years.
A fluorescent coumarin-based, two-sensor array correctly discriminates between four different amyloids implicated in amyloid-related pathologies with 100 percent classification, according to research from an Australian team. Their work was published in ACS Sensors, and the lead author is Natalie Trinh of the University of Sydney.
One of the biggest challenges in many neurodegenerative diseases, including Alzheimer’s and Parkinson’s, is early diagnosis. These diseases may present similarly, but require very different treatments, causing delay or confusion about proper treatment.
Amyloids, aggregated self-assembled misfolded proteins, are considered the tell tale markers for some such conditions. Amyloids interrupt signal transfer and there is lot of evidence linking them to the progression of Alzheimer’s disease, so they could be used as a means of early diagnosis to expand treatment options. But early detection has so far been out of reach.
This test could help monitor disease progression or distinguish between different amyloid-related conditions as well as inform new approaches for earlier and more accurate diagnosis of amyloid-related diseases.
Currently, radioimaging techniques including positron emission tomography (PET) scans can detect amyloids, but these methods rely on sophisticated equipment and typically focus on one of several amyloids involved in the disease.
Fluorescence imaging techniques are being explored as a simpler, yet still sensitive, means of detecting multiple specific amyloids. This team wanted to develop a fluorescent sensor array for amyloids to monitor Alzheimer’s and other disease progression and to distinguish these atypical amyloids from similar, naturally occurring amyloid-forming proteins.
The team combined five coumarin-based molecular probes, each of which fluoresce to a different degree when it encountered the amyloids, into a sensor array. However, the team found that using just two of the probes with the strongest fluorescence responses offered a high level of sensitivity but accurately identified the individual amyloids.
The two-probe array was added to a sample mixture mimicking biological fluids containing molecules that could potentially interfere with sensing. The array still maintained a high sensitivity and selectivity.
The test’s performance was also tested on samples taken from the brains of mouse models of Alzheimer’s. The team observed that the fluorescence patterns differed between early (at age six months) and later (at age 12 months) stages of the disease. Additionally, a unique fluorescence fingerprint was generated for three amyloids typically involved in Alzheimer’s, another disease-associated amyloid and five naturally occurring “functional amyloids” not involved in the disease.
The flexibility of the array was assessed by expanding the analytes to include functional amyloids. The same two-sensor array correctly discriminated between eight different disease-associated and functional amyloids with 100 percent classification.
The authors conclude, “These results demonstrate the utility of our fluorescent sensing array for the detection of amyloids implicated in Alzheimer’s disease and the potential it holds as a tool for researchers investigating functional amyloids, such as hydrophobins.”
Scientists at the Buck Institute for Research on Aging, the University of California, San Francisco, and elsewhere have proposed a strategy for repairing damaged synapses in Alzheimer’s disease and related dementias in mice. Details of the study in mouse models are available in The Journal of Clinical Investigation in a paper titled “KIBRA repairs synaptic plasticity and promotes resilience to tauopathy-related memory loss.”
Current research into potential treatments for Alzheimer’s disease focus on preventing the accumulation of toxic proteins like tau and amyloid beta in the brain, which impact memory as the disease progresses. For this study, the researchers focused on methods of reversing the damage to the synapses to restore memory. The work hinges on a postsynaptic protein called KIBRA which is encoded by WWC1, a gene linked to memory and risk of late-onset Alzheimer’s diseases in humans.
KIBRA is found in the kidneys and the brain where it is localized at the synapses. The scientists showed that levels of this protein, which is required for synapses to form memories, are lower in brains with Alzheimer’s disease. Furthermore, they found that higher levels of KIBRA in cerebrospinal fluid and lower levels in the brain corresponded to the severity of dementia. “We also found this amazing correlation between increased tau levels and increased KIBRA levels in the cerebrospinal fluid,” said Tara Tracy, PhD, an assistant professor at Buck and the study’s senior author. “It was very surprising how strong the relationship was, which really points to the role of KIBRA being affected by tau in the brain.”
The team also dug into how KIBRA affects synapse signaling. Specifically, “we wondered how the lower levels of KIBRA affected signaling at the synapse, and whether understanding that mechanism better could yield some insight into how to repair the synapses damaged during the course of Alzheimer’s disease,” said Grant Kauwe, PhD, a staff scientist at Buck and co-first author of the study.
To answer that question, they created a shortened functional version of the KIBRA protein and tested it in transgenic mice with a condition that mimics Alzheimer’s disease. The results showed that KIBRA reversed the memory impairment associated with this type of dementia and rescued mechanisms that promote synapse resilience. “Interestingly, KIBRA restored synaptic function and memory in mice, despite not fixing the problem of toxic tau protein accumulation,” said Kristeen Pareja-Navarro, PhD, a Buck research scientist and a co-first author of the study. “Our work supports the possibility that KIBRA could be used as a therapy to improve memory after the onset of memory loss, even though the toxic protein that caused the damage remains.”
With further study, the KIBRA protein could potentially be used as a biomarker of synaptic dysfunction and cognitive decline which could help with Alzheimer’s disease diagnosis and progression, treatment planning, and treatment response. A KIBRA-based therapy could also work alongside other therapies that prevent pathologic protein accumulation in the brain. “Reducing toxic proteins is of course important, but repairing synapses and improving their function is another critical factor that could help,” Tracy noted. “That’s how I see this making the biggest impact in the future.”
A toxic protein called beta-amyloid is believed to destroy brain neurons in Alzheimer’s patients.
There was something odd about these Alzheimer’s cases.
Part of it was the patients’ presentations: Some didn’t have the classic symptoms of the condition. But it was also that the patients were in their 40s and 50s, even their 30s, far younger than people who normally develop the disease. They didn’t even have the known genetic mutations that can set people on the course for such early-onset Alzheimer’s.
But this small handful of patients did share a particular history. As children, they had received growth hormone taken from the brains of human cadavers, which used to be a treatment for a number of conditions that caused short stature. Now, decades later, they were showing signs of Alzheimer’s. In the interim, scientists had discovered that that type of hormone treatment they got could unwittingly transfer bits of protein into recipients’ brains. In some cases, it had induced a fatal brain disease called Creutzfeldt-Jakob disease, or CJD — a finding that led to the banning of the procedure 40 years ago.
It seemed that it wasn’t just the proteins behind CJD that could get transferred. As the scientific team treating the patients reported Monday in the journal Nature Medicine, the hormone transplant seeded the beta-amyloid protein that’s a hallmark of Alzheimer’s in some recipients’ brains, which, decades later, propagated into disease-causing plaques. They are the first known cases of transmitted Alzheimer’s disease, likely a scientific anomaly yet a finding that adds another wrinkle to ongoing arguments about what truly causes Alzheimer’s.
“It looks real that some of these people developed early-onset Alzheimer’s because of that [hormone treatment],” said Ben Wolozin, an expert on neurodegenerative diseases at Boston University’s medical school, who was not involved in the study.
Other outside scientists agreed that they found the findings legitimate, in particular because only people who had received cadaveric growth hormone prepared in a particular way — a method that doesn’t eliminate protein bits — went on to develop dementia.
Such incidents of illness are known as “iatrogenic,” meaning the result of a medical procedure. In conditions like iatrogenic CJD, the transmissible agents are known as prions — basically, misfolded pieces of protein that go on to cause disease, like a sort of infectious bug.
Researchers debate the definition of a prion and whether it could include amyloid. But regardless, the paper’s authors “provide tantalizing evidence that, under extraordinary circumstances, Alzheimer’s disease is transmissible by a prion-like mechanism,” Mathias Jucker of Germany’s University of Tübingen and Lary Walker of Emory University wrote in a commentary also published Monday.
Both the study’s authors and outside researchers stressed Alzheimer’s is not some contagious disease that you could catch by caring for a relative, for example. Cases tied to cadaveric growth hormone treatment are also no longer possible; a synthetic hormone has been used instead for decades. The paper’s authors, who run a special prion disease research and treatment center in London, describe just five Alzheimer’s patients out of the more than 1,800 people who were known to have received cadaveric growth hormone in the U.K. from 1959 to 1985. Still, the researchers said the findings were a reminder of the continuing importance of practices like sterilizing neurosurgical instruments, which, in theory, could transfer prions if not properly cleaned between patients.
But in addition to being a scientific curiosity — and another example of the fallout of the use of cadaveric growth hormone — these cases could also stir up the decades-long, oft-contentious fight over the roots of Alzheimer’s.
“We think from a public health point of view, this is probably going to be a relatively small number of patients,” said John Collinge of the MRC Prion Unit at University College London, the senior author of the paper. “However, the implications of this paper we think are broader with respect to disease mechanisms — that it looks like what’s going on in Alzheimer’s disease is very similar in many respects to what happens in the human prion diseases like CJD, with the propagation of these abnormal aggregates of misfolded proteins and misshapen proteins.”
Many scientists believe that beta-amyloid plays a role in the development of Alzheimer’s, and therapies that can clear the protein from people’s brains have finally, after decades of failed attempts, started showing some benefits for patients. But most experts also think amyloid isn’t solely responsible. So in these cases, was there something else going on in addition to the amyloid transfer?
“It raises questions about whether amyloid alone is able to cause problems,” said Marc Dhenain, an Alzheimer’s expert at the French research center CEA, who was not involved in the new study.
Outside researchers said they were also left scratching their heads about some of the findings. They said there was limited information, with findings reported from just a few patients, and data like genetic sequencing and autopsy results available from just a sample of them.
They noted, however, that there didn’t seem to be much inflammation in the patients’ brains, another hallmark of Alzheimer’s that can be induced by amyloid. They also wondered why there was so little presence of another protein called tau in the people’s brains despite their cognitive losses, even though tau levels often correlate to cognitive decline. Some researchers speculated that the patients may have had some other genetic mutation that could increase their risk of Alzheimer’s. Two of the patients had intellectual disabilities, another risk factor.
“Can the pathology be transmitted? Yes, it can, and that’s important conceptually,” Wolozin said. “The question is, what’s driving disease? There are many weird things about these rare cases. What’s unclear from the images is, why would they develop such severe dementia that quickly?”
Globally, more than 200 cases of iatrogenic CJD have been documented in recipients of cadaveric human growth hormone, with the bulk of patients in France, the U.K., and the U.S. And for years, researchers have been gathering clues that there may be an iatrogenic form of Alzheimer’s as well. (The vast majority of Alzheimer’s cases are what’s known as sporadic, developing among older people. There are also some early-onset cases that are tied to inherited mutations.)
In 2015, the UCL prion researchers reported finding lots of beta-amyloid in the brains of patients who died of iatrogenic CJD, including a buildup in the brain’s blood vessels, which is known as cerebral amyloid angiopathy and which is seen in most people with Alzheimer’s. It led them to hypothesize that the hormones the patient received had been contaminated not just with the CJD prions, but seeds of amyloid as well. It also made them wonder whether the patients, had CJD not killed them, would have gone on to develop Alzheimer’s.
The paper describes eight patients who were treated at the U.K.’s National Prion Clinic from 2017 to 2022, none of whom had CJD and only some of whom were found to have Alzheimer’s. They had received the hormone treatment as children for different causes of short stature: some had brain tumors, others had developmental conditions, others just lacked their own natural hormone.
Five of them had been diagnosed with Alzheimer’s or likely had Alzheimer’s disease, with their symptoms starting between the ages of 38 and 55. Among the other three patients, two had some cognitive impairments, while the third was asymptomatic.
The researchers noted that the presentation of iatrogenic CJD often differs from that of the more common sporadic cases, so it’s possible the transmitted Alzheimer’s cases would look somewhat distinct from typical cases.
Gargi Banerjee, the lead author of the paper, said the UCL researchers considered other possible causes of these patients’ Alzheimer’s. Given the age of the patients, these weren’t sporadic cases, which almost always develop only later in life. The patients didn’t have known genetic mutations that could cause early-onset dementia. The researchers also considered the underlying reasons why the patients had received the hormone in the first place — was it a result of their cancer treatment or congenital conditions? — but that wasn’t a likely explanation either.
“The thing about this group is thinking about them as a whole,” she said. “In the people who did have symptoms, they had various different illnesses, but the only combined fact was that they all had this particular type of growth hormone, this particular preparation in childhood. … There was no other unifying cause for this.”
A new study identified a set of 10 compounds in the blood that might be used to identify older adults at risk for developing memory deficits or Alzheimer’s disease. More research is needed to confirm the findings, but the study suggests one possible approach for the early identification and treatment of cognitive decline.
Alzheimer’s disease is a progressive brain disorder that affects older adults. It gradually destroys their ability to think and remember. Estimates vary, but Alzheimer’s disease may affect as many as 5 million people over age 65 in the U.S. That number is expected to more than triple by 2050.
Despite extensive research, there are no effective therapies for preventing Alzheimer’s disease or slowing its progression. Many experts believe that successful treatment will depend on early intervention before symptoms appear. However, there’s no sure way to identify pre-symptomatic Alzheimer’s disease. Brain scans and spinal fluid tests are now being evaluated to identify certain at-risk individuals. Scientists have been intensely searching for simpler ways to predict memory decline and Alzheimer’s disease well before signs of memory loss appear.
Dr. Howard Federoff of Georgetown University Medical Center and his colleagues decided to search for biomarkers of early-stage Alzheimer’s disease in circulating blood. They enrolled 525 healthy adults, ages 70 and older, in a 5-year observational study. The research was funded in part by NIH’s National Institute on Aging (NIA). Results appeared online on March 9, 2014, in Nature Medicine.
Cognitive tests at enrollment showed that 46 participants had previously undiagnosed mild Alzheimer’s disease or mild cognitive impairment that mostly affected memory. This type of memory loss is sometimes an early sign of Alzheimer’s disease. Over the course of the study, 28 people with normal memory eventually developed either mild Alzheimer’s disease or impaired memory. The researchers classified this group as “converters.”
In the study’s third year, the scientists used advanced technologies to analyze the blood of 53 participants (including 18 converters) who had either impaired memory or Alzheimer’s disease. The researchers also studied 53 cognitively normal age- and sex-matched participants for comparison. In an approach known as metabolomics, the scientists used mass spectrometry to sort through hundreds of blood-based chemicals, called metabolites, produced during the body’s everyday activities.
A series of analyses pinpointed 10 lipids, or fats, that differed between those who were cognitively impaired, healthy people who later “converted,” and participants who remained healthy. These lipid metabolites might represent the weakening of nerve cell membranes in the early stages of Alzheimer’s disease.
To validate their findings, the scientists tested the 10-lipid panel in a blinded analysis. The team evaluated blood from 40 separate participants, including 10 converters. The test could distinguish with 90% accuracy between cognitively normal participants who remained healthy and those who became impaired within 2 to 3 years.
“The preclinical state of the disease offers a window of opportunity for timely disease-modifying intervention,” Federoff says. “Biomarkers such as ours that define this asymptomatic period are critical for successful development and application of these therapeutics.” The researchers note that the biomarker panel would require further validation in larger, diverse populations before it could be used clinically.
Some early Alzheimer’s disease-related brain changes, including beta-amyloid buildup and lower cortical thickness, were greater among middle-aged adults with abdominal obesity. Findings from the NIA-funded pilot study were published in Aging and Disease.
Although midlife obesity is considered an Alzheimer’s risk factor, some studies suggest that high body mass index (BMI) — a measure of body fat based on height and weight — is not always associated with increased likelihood of developing the disease. In this study, researchers from Washington University in St. Louis explored whether abdominal obesity could be used to assess Alzheimer’s risk. Abdominal obesity occurs when more fat is stored deep in the belly compared to under the skin.
The research team analyzed BMI, insulin resistance, and brain scans from 32 cognitively normal, midlife adults (ages 40-60 years). They also used MRI to measure abdominal fat. This provided them with an alternative to using the BMI scale to assess obesity.
The researchers found that men had higher levels of abdominal obesity than women. However, they found no gender differences in BMI or insulin resistance, another obesity-related risk that may contribute to Alzheimer’s.
Analysis of brain scan data showed that higher BMI, abdominal obesity, and insulin resistance scores were associated with lower cortical thicknesses in the temporal lobe and other regions that are often damaged by Alzheimer’s.
In men, abdominal obesity was linked to higher levels of the hallmark protein beta-amyloid in the precuneus cortex, an area affected early by Alzheimer’s.
BMI, abdominal obesity, and insulin resistance were not found to be associated with tau buildup or brain volume, another key marker of Alzheimer’s. This may suggest that the association of abdominal obesity with beta-amyloid buildup and lower cortical thickness in midlife are early biomarkers, occurring before tau buildup and cognitive decline.
The findings of this pilot study support the idea that abdominal obesity may be used to assess Alzheimer’s risk. The researchers plan to recruit 20 participants for the next phase of research.
This research was supported by NIA grants 1RF1AG072637-01, P30AG066444, P01AG026276, and P01AG003991.
These activities relate to NIH’s Alzheimer’s and Related Dementias Research Implementation Milestones:
1.F, “Support the inclusion of measures of AD-related phenotypes and environmental exposures in non-AD cohorts to enable new discovery research and to accelerate cross-validation of discoveries made in AD cohorts.”
2.B, “Establish new research programs that employ data-driven, systems-based approaches to understand the interaction between peripheral systems (in particular: immune, metabolic, microbiome) and the brain and the impact of this interaction on brain aging and neurodegeneration.”










{kind=link}
{kind=link}