Researchers have found a new way to boost the body’s defense against neurodegenerative diseases by preventing the degradation of Nrf2, potentially slowing the progression of diseases such as Alzheimer’s and Parkinson’s. Credit: SciTechDaily.com
A groundbreaking study introduces a new method of targeting ‘undruggable’ proteins to fight neurodegenerative diseases by enhancing cellular antioxidant defenses, offering new hope for treatment advancements.
Researchers led by Northwestern University and the University of Wisconsin-Madison have introduced a pioneering approach aimed at combating neurodegenerative diseases such as Alzheimer’s disease, Parkinson’s disease, and Amyotrophic lateral sclerosis (ALS).
In a new study, researchers discovered a new way to enhance the body’s antioxidant response, which is crucial for cellular protection against the oxidative stress implicated in many neurodegenerative diseases.
The study was published on February 16 in the journal Advanced Materials.
Nathan Gianneschi, the Jacob & Rosaline Cohn Professor of Chemistry at Northwestern’s Weinberg College of Arts and Sciences and member of the International Institute for Nanotechnology, led the work with Jeffrey A. Johnson and Delinda A. Johnson of the University of Wisconsin-Madison School of Pharmacy.
Proteins are nature’s polymers, governing biological processes at every level. A new study presents artificial proteins made using modern, precision polymers to intervene and alter natural processes towards a new way of developing therapeutics.
Targeting Neurodegenerative Diseases
Alzheimer’s disease, characterized by the accumulation of beta-amyloid plaques and tau protein tangles; Parkinson’s disease, known for its loss of dopaminergic neurons and presence of Lewy bodies; and ALS, involving the degeneration of motor neurons, all share a common thread of oxidative stress contributing to disease pathology.
The study focuses on disrupting the Keap1/Nrf2 protein-protein interaction (PPI), which plays a role in the body’s antioxidant response. By preventing the degradation of Nrf2 through selective inhibition of its interaction with Keap1, the research holds promise for mitigating the cellular damage that underlies these debilitating conditions.
“We established Nrf2 as a principal target for the treatment of neurodegenerative diseases over the past two decades, but this novel approach for activating the pathway holds great promise to develop disease-modifying therapies,” Jeffrey Johnson said.
Limitations of Current Therapeutics
The research team embarked on addressing one of the most challenging aspects of neurodegenerative disease treatment: the precise targeting of PPIs within the cell. Traditional methods, including small molecule inhibitors and peptide-based therapies, have fallen short due to lack of specificity, stability and cellular uptake.
The study introduces an innovative solution: protein-like polymers, or PLPs, are high-density brush macromolecular architectures synthesized via the ring-opening metathesis polymerization (ROMP) of norbornenyl-peptide-based monomers. These globular, proteomimetic structures display bioactive peptide side chains that can penetrate cell membranes, exhibit remarkable stability and resist proteolysis.
This targeted approach to inhibit the Keap1/Nrf2 PPI represents a significant leap forward. By preventing Keap1 from marking Nrf2 for degradation, Nrf2 accumulates in the nucleus, activating the Antioxidant Response Element (ARE) and driving the expression of detoxifying and antioxidant genes. This mechanism effectively enhances the cellular antioxidant response, providing a potent therapeutic strategy against the oxidative stress implicated in many neurodegenerative diseases.
The Innovation Behind Protein-Like Polymers
PLPs, developed by Gianneschi’s team, could represent a significant breakthrough in halting or reversing damage offering hope for improved treatments and outcomes.
Focusing on the challenge of activating processes crucial for the body’s antioxidant response, the team’s research offers a novel solution. The team provides a robust, selective method enabling enhanced cellular protection and offering a promising therapeutic strategy for a range of diseases including neurodegenerative conditions.
“Through modern polymer chemistry, we can begin to think about mimicking complex proteins,” Gianneschi said. “The promise lies in the development of a new modality for the design of therapeutics. This could be a way to address diseases like Alzheimer’s and Parkinson’s among others where traditional approaches have struggled.”
This approach not only represents a significant advance in targeting transcription factors and disordered proteins, but also showcases the PLP technology’s versatility and potential to revolutionize the development of therapeutics. The technology’s modularity and efficacy in inhibiting the Keap1/Nrf2 interaction underscore its potential for impact as a therapeutic, but also as a tool for studying the biochemistry of these processes.
A Collaboration of Minds
Highlighting the study’s collaborative nature, Gianneschi’s team worked closely with experts across disciplines, illustrating the rich potential of combining materials science with cellular biology to tackle complex medical challenges.
“We were contacted by Professor Gianneschi and colleagues proposing to use this novel PLP technology in neurodegenerative diseases due to our previous work on Nrf2 in models of Alzheimer’s disease, Parkinson’s disease, ALS and Huntington’s disease,” Jeffrey Johnson said. “We had never heard of this approach for Nrf2 activation and immediately agreed to initiate this collaborative effort that led to the generation of great data and this publication.”
This partnership underscores the importance of interdisciplinary research in developing new therapeutic modalities.
Impact
With the development of this innovative technology, Gianneschi, his colleagues at the International Institute for Nanotechnology and the Johnson Lab at the University of Wisconsin-Madison, are not just advancing the field of medicinal chemistry, they are opening new pathways to combat some of the most challenging and devastating neurodegenerative diseases faced by society today. As this research progresses towards clinical application, it may soon offer new hope to those suffering from diseases of oxidative stress such as Alzheimer’s and Parkinson’s diseases.
“By controlling materials at the scale of single nanometers, we’re opening new possibilities in the fight against diseases that are more prevalent than ever, yet remain untreatable,” Gianneschi said. “This study is just the beginning. We’re excited about the possibilities as we continue to explore and expand the development of macromolecular drugs, capable of mimicking some of the aspects of proteins using our PLP platform.”
Usually, when something gets warmed up, heat tends to spread outward before eventually dissipating. But things are a little different in the world of superfluid quantum gas.
For the first time, MIT scientists have successfully imaged how heat actually travels in a wave, known as a “second sound,” through this exotic fluid.
Understanding this dynamic could help answer questions about high-temperature superconductors and neutron stars.
In the world of average, everyday materials, heat tends to spread out from a localized source. Drop a burning coal into a pot of water, and that liquid will slowly rise in temperature before its heat eventually dissipates. But the world is full of rare, exotic materials that don’t exactly play by these thermal rules.
Instead of spreading out as one would expect, these superfluid quantum gasses “slosh” heat side to side—it essentially propagates as a wave. Scientists call this behavior a material’s “second sound” (the first being ordinary sound via a density wave). Although this phenomenon has been observed before, it’s never been imaged. But recently, scientists at the Massachusetts Institute of Technology (MIT) were finally able to capture this movement of pure heat by developing a new method of thermography (a.k.a. heat-mapping).
The results of this study were published last week in the journal Science, and in an university press release highlighting the achievement, MIT assistant professor and co-author Richard Fletcher continued the boiling pot analogy to describe the inherent strangeness of “second sound” in these exotic superfluids.
MIT
Simplified example of “sloshing” heat in a superfluid compared to a normal fluid.
“It’s as if you had a tank of water and made one half nearly boiling,” Fletcher said. “If you then watched, the water itself might look totally calm, but suddenly the other side is hot, and then the other side is hot, and the heat goes back and forth, while the water looks totally still.”
These superfluids are created when a cloud of atoms is subjected to ultra-cold temperatures approaching absolute zero (−459.67 °F). In this rare state, atoms behave differently, as they create an essentially friction-free fluid. It’s in this frictionless state that heat has been theorized to propagate like a wave.
“Second sound is the hallmark of superfluidity, but in ultracold gases so far you could only see it in this faint reflection of the density ripples that go along with it,” lead author Martin Zwierlein said in a press statement. “The character of the heat wave could not be proven before.”
To finally capture this second sound in action, Zweierlein and his team had to think outside the usual thermal box, as there’s a big problem trying to track heat of an ultracold object—it doesn’t emit the usual infrared radiation. So, MIT scientists designed a way to leverage radio frequencies to track certain subatomic particles known as “lithium-6 fermions,” which can be captured via different frequencies in relation to their temperature (i.e. warmer temperatures mean higher frequencies, and vice versa). This novel technique allowed the researchers to essentially zero in on the “hotter” frequencies (which were still very much cold) and track the resulting second wave over time.
This might feel like a big “so what?” After all, when’s the last time you had a close encounter with a superfluid quantum gas? But ask a materials scientist or astronomer, and you’ll get an entirely different answer.
While exotic superfluids may not fill up our lives (yet), understanding the properties of second wave movement could help questions regarding high-temperature superconductors (again, still at very low temperatures) or the messy physics that lie at the heart of neutron stars.
Plus, how many of these small but mighty seeds you should have on the daily.
We may earn commission from links on this page, but we only recommend products we back.
Often referred to as a “superfood,” chia seeds are tiny black and white seeds from the desert plant Salvia hispanica, a member of the mint family. These little seeds are small, but they sure are mighty. In fact, there’s no shortage of chia seed benefits—or ways to include them in your daily meals.
So, what health benefits can you expect from your daily dose of chia seeds? We’ve tapped our nutritionists to give us the scoop on all the good these powerhouse seeds can do. Plus, how you can add them to your favorite meals every day.
Benefits of chia seeds
OatmealStories//Getty Images
1
Complete protein
As noted by Harvard Health, chia seeds are a complete protein and contain all nine essential amino acids that cannot be made by the body. You need these amino acids for energy production and immune function within your body. Other examples of complete proteins are animal-based foods like dairy, eggs, fish, meat, and poultry while plant-based options include buckwheat, edamame, and quinoa. With 5 grams of protein per serving, chia seeds can add protein to almost any recipe.
zeljkosantrac//Getty Images
2
Good source of fiber
Chia seeds are a good source of fiber which may help lower cholesterol levels, improve digestive health, and maintain blood glucose levels, says Keri Gans, M.S., R.D., registered dietitian and author of The Small Change Diet. When combined with water, chia seeds can help you feel full longer and reduce constipation, adds Melissa Prest, D.C.N., R.D.N., national media spokesperson for the Academy of Nutrition and Dietetics and member of the Prevention Medical Review Board. “The high fiber content is also beneficial to gut health by fueling our healthy gut microbes.”
Tolimir//Getty Images
3
Antioxidants and polyphenols
Another surprising health benefit of chia seeds is they are an excellent source of antioxidants and polyphenols such as caffeic acid, myricetin, quercetin, rosmarinic acid, and others. Antioxidants are substances that may protect your cells against free radicals, which may play a role in cancer, heart disease, and other diseases, while polyphenols are beneficial plant compounds with antioxidant properties that may help keep you healthy and protect against various diseases.
Westend61//Getty Images
4
Omega-3 fatty acids
Chia seeds are packed with omega-3 fatty acids that have anti-inflammatory properties which may help lower blood pressure and triglyceride levels, and reduce the risk for a heart attack or stroke, says Gans. Omega-3 fatty acids may also help control eczema, lupus, and rheumatoid arthritis. They may even play protective roles against cancer and other conditions.
KarinaUrmantseva//Getty Images
5
Heart healthy fats
Not only do chia seeds have omega-3 fatty acids, but they also contain heart-healthy fats. The Mayo Clinic writes that one serving of chia seeds contains 9 grams of fat, of which 8 grams are heart-healthy fats.
Cavan Images//Getty Images
6
Minerals
Chia seeds also have minerals including calcium, iron, magnesium, and zinc. Calcium and magnesium help maintain healthy bones while zinc is essential for cell division and growth. It is also an essential element needed to support the body’s immune system. Instead of supplements and vitamins, reach for a sprinkle or two of chia seeds at your next meal.
kajakiki//Getty Images
7
Low in Calories
Chia seeds can add a low calories crunch to any meal or snack. In fact, just one ounce (28 grams or two tablespoons) of chia seeds contains only 138 calories. So, because they’re also a great source of fiber, adding chia seeds to your low-calorie snack or meal can help you feel full for longer while still following a low-calorie diet.
Alicia Llop//Getty Images
8
May lower cholesterol and reduce blood sugar levels
Per Harvard Health, the fiber in chia seeds is mainly soluble fiber and mucilage, the substance responsible for the gluey texture of moistened chia seeds. These fibers may help to lower LDL cholesterol (bad cholesterol) and slow down digestion, which can prevent blood sugar spikes after eating a meal and promote a feeling of fullness. In fact, one 2013 study found that eating bread containing chia seeds helped lower post-meal rises in blood sugar among healthy adults, compared with eating bread without chia seeds.
Ivaylo Ivanov / EyeEm//Getty Images
9
May support bone health
Chia seeds contain calcium and phosphorus as well as magnesium. All three of these minerals have been known to help support optimal bone health. Many observational studies even suggest that getting enough of these nutrients is important for maintaining good bone mineral density, which is an indicator of bone strength.
Westend61//Getty Images
10
May protect against colorectal cancer
Chia seed components can play a key protective role in chronic diseases like cardiovascular disease, diabetes, and certain types of cancer, says Jackie Newgent, R.D.N., C.D.N., chef, nutritionist, and author of The Plant-Based Diabetes Cookbook. As you already read, chia seeds are an excellent source of fiber, which can promote intestinal health. The Mayo Clinic notes that eating a diet rich in fiber also is shown to protect against colorectal cancer.
Do chia seeds really reduce belly fat?
Contrary to popular belief, there is not one food or ingredient that specifically targets belly fat, says Gans. With that being said, Gans notes that, “if an individual is constipated and experiencing bloating, perhaps chia seeds could help with bowel regularity and reduce bloating.”
Due to the high fiber content, chia seeds can make you stay full longer, allowing you to naturally eat less and lose weight, including belly fat, adds Prest.
How many chia seeds should you eat a day?
Generally, enjoying around 2 tablespoons a day of chia seeds in meals and snacks is a healthy amount for most adults, says Newgent.
How to add chia seeds to daily meals
Chia seeds are super versatile because they do not have much flavor, says Prest, “so you can mix them with many different foods.”One easy way to enjoy chia seeds is as nourishing beverage boosters, says Newgent. “Just blend one or two teaspoons of them into your next smoothie or even stir some into a juicy cocktail!”
You can also make a chia seed pudding, add to overnight oats, jams, and even coleslaw, says Prest, for a thicker consistency and an added health boost. If you’re a baker, chia seeds also pair particularly well with baked goods like bread.
If you’re not one to follow a recipe, you can simply toss chia seeds into any salad, cereal, yogurt, oatmeal, or even sprinkle them into rice dishes for a variety of texture. The opportunities to add chia seeds into your day are endless!
“Prostate milking” typically refers to the massage of the prostate for sexual pleasure. Prostate milking may also have some health benefits, though more research is necessary.
The prostate is a gland in the male reproductive system. One of its main functions is to produce prostate fluid, which mixes with other fluids and sperm to make semen.
Here, we describe what prostate milking is and how to do it. We also explore why people do it and look into some of the risks and potential benefits.
A note about sex and gender
Sex and gender exist on spectrums. This article will use the terms “male,” “female,” or both to refer to sex assigned at birth.
Today, “prostate milking” usually refers to prostate stimulation for sexual pleasure, while “prostate massage” can refer to sexual or therapeutic stimulation.
However, some people find the massage painful or unpleasant to perform on themselves. In this case, depending on the goal of the stimulation, a person may ask a partner or a healthcare professional to perform the massage.
The prostate is a walnut-sized organ inside the rectum and just under the bladder. It wraps around the urethra, the tube that drains urine from the bladder.
The prostate tends to get larger with age, making it easier to locate.
To find the prostateTrusted Source, a person can insert a lubricated finger into the rectum, then push slightly on its front wall. They may feel a slight bulge.
Because the prostate is so close to the bladder and urethra, intense prostate stimulation can cause the urge to urinate. Prostatitis and other prostate problems may also lead to more frequent urination.
Once a person locates their prostate, they can begin to massage it with a finger, massager, or sex toy.
Technique
First, an individual should apply plenty of lubricant to the finger or sex toy. Wearing gloves can make inserting digits smoother, and it may also be a good idea due to hygiene concerns.
A person can gently insert the lubricated finger or sex toy into the anus, slowly pushing on the front wall of the rectum.
For most people, finding the prostate requires inserting the finger or sex toy at least halfway up the rectum. Touching the prostate may produce an unusual or pleasurable sensation.
Begin by massaging the prostate in a consistent motion that feels pleasurable. Some people opt to masturbate or have other sexual contact during the massage.
The person receiving the message may have a very intense orgasm or feel an unusual sensation followed by fluid from the penis.
Positions
There are several different positions a person can take to make prostate milking easier.
Lying face down: When lying face down comfortably and their legs slightly apart, a person can reach behind their back to their anus or perineum. From this position, they, their partner, or partners can perform a prostate massage.
On all fours: A person can rest on their hands and knees and reach one hand back between their legs or around their lower back to their anus or perineum. In this position, a partner can also stand or kneel behind them and carry out a prostate massage.
Lying on the back: Some people may feel more comfortable milking their prostate when lying on their back. Once comfortable, a person can pull both their knees toward their chest and hold them with one arm. Using their free hand, they can reach their anus or perineum.
Lying on one side: When lying on one side, a person can bring their outer knee up toward their chest and reach over their hips to their anus or perineum. They can then massage their prostate with their free hand.
Practice
It is important for people to find techniques and positions they are comfortable with. Practicing safe methods of prostate milking can help a person find which methods suit them.
For example, if someone is uncomfortable with anal insertion, it is possible to stimulate the prostate less directly. They can do this by pushing upward on the perineum — the skin between the testicles and the rectum.
People may also wish to experiment with massagers and other sex toys to massage their prostate.
The prostate is one of the male erogenous zones. An erogenous zone is a highly sensitive area of the body that may generate a sexual response during stimulation.
Prostate milking may be very pleasurableTrusted Source. Because the prostate plays a role in producing semen, stimulating it may produce a more intense orgasm during ejaculation.
Some people also practice prostate milking for its purported health benefits rather than for sexual stimulation.
The primary benefit of prostate milking is that it can feel good. It may make sex more pleasurable and enhance closeness between partners.
There is also limited evidence that prostate massage may improve prostate health.
An older preliminary trial from 2009 of a home prostate massage device found that men with chronic prostatitis or benign prostatic hyperplasia experienced a reduction in symptoms following this type of prostate massage.
However, a 2018 reviewTrusted Source concluded that there is insufficient evidence to claim that prostate massages affect symptoms.
Prostate milking is not usually dangerous. However, a very aggressive technique could, in theory, cause minor injury to the skin or rectum.
Also, prostate massage, especially when it is intense or forceful, could be painful.
Prostate massage also presents a small risk of prostate infection. If someone massages the prostate with unwashed hands, this could introduce bacteria into the area.
Similarly, bacteria from the rectum can travel elsewhere if a person does not wash their hands thoroughly after a prostate massage.
Additionally, some people do not enjoy the sensation of prostate milking or any other anal stimulation. This does not mean something is wrong — it is simply a personal preference.
It is important to note that individuals should take caution when experimenting with sex toys or devices while under the influence of drugs or alcohol.
The following are answers to commonly asked questions about prostate massage.
What is the difference between prostate and penile orgasm?
Many people experience an orgasm from prostate milking, especially if they masturbate during it.
A person may not be able to distinguish between prostate fluid and ejaculated semen. Prostate fluid is one component of semen. When a male has an orgasm and ejaculates, sperm, prostate fluid, and other fluids occur in the ejaculate.
Not all people ejaculate or have an orgasm during prostate milking. However, masturbation and other forms of sexual contact make ejaculation during the massage more likely.
Does prostate massage help erectile dysfunction?
In some cases, yes. Older researchTrusted Source has shown that regular prostate massage improved sexual function, so it may be useful for people with erectile dysfunction. However, there is no consensus that prostate massage improves sexual function.
Can prostate milking prevent cancer?
No, it cannot directly prevent cancer. However, researchTrusted Source has found that regular ejaculation is important for sexual health in males, and it is associated with a lower risk of developing prostate cancer.
How does a person find the prostate?
The prostate is inside the rectum and just under the bladder. To help locate the prostate, a person can insert a lubricated finger into the rectum and push slightly on its front wall.
What are the risks of prostate milking?
While prostate milking is generally safe, it is important to perform it safely. This includes being gentle and using lubrication to prevent injuries to the rectum. Additionally, a person should wash their hands before attempting prostate milking to reduce the risk of infection.
Prostate milking can be pleasurable. Some people perform it on themselves, while others seek the help of a partner.
Some preliminary research suggests that prostate milking may improve symptoms associated with prostate enlargement. However, confirming this requires further research.
Anyone with concerns about their sexual health or prostate health should consult a doctor.
Despite its prevalence, this immune-mediated dermatological condition still holds many mysteries.
Aside from psoriatic lesions on the skin, this condition can also influence less visible parts of the body.
One important example is its links to an increased risk of cardiovascular eventsTrusted Source. This increase in risk is independentTrusted Source of traditional cardiovascular risk factors, such as smoking, age, diabetes, and hypertension.
Medical News Today spoke with Dr. Joel Gelfand, a professor of dermatology and epidemiology at the University of Pennsylvania Perelman School of Medicine about the disease.
“There are many lifestyle, genetic, and immunologic connections between psoriasis and cardiovascular disease,” he explained.
He noted that scientists have known about this link for many years and it is an important area of research.
“The more extensive psoriasis is on the skin, the greater risk the patient has of heart attack, stroke, and mortality,” said Gelfand, who wasn’t involved in the study. “Underdiagnosed and undertreated, traditional cardiovascular risk factors in psoriasis patients are also critical to mediating this relationship.”
A recent study, which appears in the Journal of Investigative Dermatology, uses a new approach to investigate the precise mechanisms behind psoriasis and cardiovascular disease.
Experts say that the inflammation associated with psoriasis helps drive the development of cardiovascular disease.
This inflammation encourages the growth of plaques in blood vessels and can lead to atherosclerosis, a factor in the risk of cardiovascular diseases.
This includes an increased risk of coronary artery disease, where the blood vessels supplying the heart become narrower.
However, there are still some gaps in our understanding. Studies have shown that people with psoriasis have elevated cardiovascular risk before the appearance of coronary artery disease.
Some scientists believe that this may be due to coronary microvascular dysfunction (CMD). The latest study digs into this theory.
CMD affects the tiny blood vessels that supply the cardiac muscle. Like coronary artery disease, inflammationTrusted Source seems to be a driving factor in CMD.
However, while coronary artery disease and CMD are related, according to the authors of the recent paper, they “may play different roles in the pathogenesis of vascular disease.”
Some existing evidence suggests that the increased cardiovascular risk in people with psoriasis may be due to CMD, but previous investigations have been small in scale.
The latest study set out to replicate those findings in a larger group.
Because CMD affects the smallest blood vessels, most standard medical procedures cannot detect it. So, in this study, the researchers used a measure called coronary flow reserve, which can detect both coronary artery disease and CMD.
Coronary flow reserve is a measure of how much blood flow to the coronary arteries can increase during exertion. In other words, it assess how much the coronary circulation can dilate to increase its capacity.
In healthy people, coronary flow reserve is between 3 and 6. If someone has a score of 3, this means they can triple the blood flow when needed.
A score of 2.5 or lower indicates either CMD or coronary artery disease. So, if a routine coronary angiography reveals no coronary artery disease, this implicates CMD.
The researchers included data from 448 people with psoriasis.
Of these, they found that 31% had a coronary flow reserve of 2.5 or lower, but no sign of coronary artery disease in a follow-up scan. So, roughly 1 in 3 had CMD.
Compared with participants without CMD, those with CMD were more likely to:
They were also more likely to have more severe psoriasis and to have lived with the condition for longer. So, as disease duration and severity increased, so did the risk of CMD.
Researchers say the results show that disease duration and severity are linked to CMD. Because CMD is prevalent in people with other inflammatory conditions, this supports the theory that systemic inflammation drives CMD.
Also, their analysis found no association between CMD and conventional cardiovascular risk factors, such as smoking, blood fat levels, or type 2 diabetes, all of which are associatedTrusted Source with CMD in the general population.
The authors conclude that the high levels of CMD are “likely to contribute significantly to the increased risk of adverse [cardiovascular] outcomes in patients with psoriasis […] independently of traditional [cardiovascular] risk factors.”
The authors also note that some research suggests that treating psoriasis is associated with reduced levels of CMD. With this in mind, they write:
“[W]e might hypothesize that an early and effective treatment of psoriasis would restore a CMD and eventually prevent the future risk of myocardial infarction and heart failure associated with it.”
Gelfand explained how he and his colleagues are also investigating other ways of assessing cardiovascular risk in people with psoriasis.
“The risk of future cardiovascular events can be further refined with cardiac imaging, such as a coronary artery calcium score,” he said. “We are testing a novel, centralized, care coordination model to help psoriasis patients get better screening for, and management of, traditional cardiovascular risk factors. Our preliminary dataTrusted Source is quite promising.”
In the future, using a range of scanning and diagnostic technology might help assess and address cardiac risk earlier in this population.
Because inflammation plays an important role in increasing cardiovascular risk, psoriasis drugs that reduce inflammation may also help reduce this risk.
However, as Gelfand mentioned, the evidence is “quite mixed” at this point.
“To date, TNF [tumor necrosis factor] inhibitors seem to be the most promising for lowering cardiovascular risk in psoriasis, but a causal relationship has not been established,” he said.
Successfully treating psoriasis symptoms can also reduce risk in other ways.
“Improved disease control may change how patients live their lives,” Axel Svedbom, PhD, a researcher at the Karolinska Institutet in Sweden who was not involved in the latest research, told Medical News Today.
“Patients with well-controlled psoriasis may lead healthier lives due to reduced social stigma and their sleep may improve due to reduced itch — poor sleep is a risk factor for cardiovascular disease,” he said.
“Furthermore,” he noted, “psoriasis is associated with lipid dysfunction and it is possible that disease activity modifies lipid composition of function. Another potential mechanism is tryptophan metabolism, which has been implicated in both psoriasis and cardiovascular disease.”
We still have much to learn about psoriasis. This study adds another piece to the puzzle.
Epigenetic changes in blood immune cells suggest that viral infections and other external factors may play a role in Alzheimer’s risk.
Scientists are continuing to look for new ways to treat Alzheimer’s disease as rates are expected to increase.
Researchers from Northwestern University Feinberg School of Medicine found that immune cells in the blood of people with Alzheimer’s disease are epigenetically altered.
The study also discovered several genes that may be therapeutic targets for manipulating the body’s peripheral immune system.
With rates of Alzheimer’s disease expected to riseTrusted Source and still no cure for this type of dementia, finding new ways to treat this disease has been at the forefront of research over the past few years.
Adding to this research is a new study from Northwestern University Feinberg School of Medicine. The findings recently published in the journal NeuronTrusted Source found that immune cells in the blood of people with Alzheimer’s disease are epigenetically alteredTrusted Source.
This alteration, the researchers say, is potentially caused by a previous viral infection, environmental pollutants, or other lifestyle factors.
The body’s immune system can be considered as comprising two parts — the central immune system and the peripheral immune system, a term used to describe immune responses that happen outside the brain.
The peripheral immune system includes circulating white blood cells that detect antigens, such as bacteria or viruses, when they enter the body. This part of the immune system acts as the first wave of attack against any foreign substance.
According to Dr. David Gate, assistant professor of neurology at Northwestern University Feinberg School of Medicine and senior and corresponding author on this study, there is mounting evidence that the peripheral immune system plays a role in Alzheimer’s disease.
“In recent years, we have shown that immune cells of the cerebrospinal fluid — a fluid that flows in and around the brain — are clonally expanded and activated,” Dr. Gate told Medical News Today. “This means that they have previously responded to some type of immune stimulus.”
Previous researchTrusted Source has connected the peripheral immune system to neurodegenerative diseases, and studiesTrusted Source have shown an association between types of peripheral immune cells and cognition, brain structure, and Alzheimer’s disease pathology.
For this study, Dr. Gate said the team wanted to find out whether there might be epigenetic changes within the immune system of Alzheimer’s disease patients that might promote the trafficking of these changes to the cerebrospinal fluid and the brain.
“Epigenetics essentially reflects changes to our DNA that have occurred in the past,” he explained. “There are many influences on epigenetics, such as the environment, pollutants, viral infections, lifestyle factors, and behaviors. It is possible that these influences work in concert, or in isolation, to promote inflammation that puts one at risk of developing Alzheimer’s disease.”
Dr. Gate and his team examined immune cells from peripheral blood samples taken from people with Alzheimer’s disease. When compared to healthy controls, researchers found that every immune cell type in the participants with Alzheimer’s disease had epigenetic changes indicated by open chromatinTrusted Source.
Additionally, scientists looked for which genes were more open in the immune cells and found more exposure in the protein CXCR3Trusted Source on T cellsTrusted Source.
“Epigenetic changes alter the way our genes are translated into proteins,” Dr. Gate explained. “In this study, we observed an epigenetic change in a gene that encodes the protein CXCR3. CXCR3 is a signal receptor on the surface of immune cells called T cells. This receptor essentially serves as an antenna that we believe allows them to traffic signals put out by the Alzheimer’s brain.”
Researchers also found epigenetic changes in a type of white blood cell called monocytesTrusted Source.
“Monocytes are very important to immune defense. They secrete inflammatory proteins that protect your body in the case of infection. In this study, we found that there are epigenetic changes to genes that encode these inflammatory proteins. This is significant because it could signal that Alzheimer’s disease patients have a more pronounced pro-inflammatory immune system.”
As epigenetics only provides a snapshot into the past, Dr. Gate said we can only speculate on what might have caused these discovered epigenetic changes.
“However, in the past decade, we have grown to appreciate the fact that viral infections are a risk factorTrusted Source for the development of dementias like Alzheimer’s disease,” he continued.
“While our data do not provide evidence that epigenetic changes in Alzheimer’s disease patients’ immune systems were caused by viral infections, this is certainly a tantalizing possibility. In this scenario, viral infections promote inflammatory responses over the course of one’s life that promote Alzheimer’s disease risk via mechanisms that we do not yet understand,” suggested Dr. Gate.
“Our ultimate goal is to design immune cell therapies for Alzheimer’s disease,” Dr. Gate added. “Using information from this study, we can potentially target the genes that harbor epigenetic changes.”
After reviewing this study, Dr. Manisha Parulekar, chief of the Division of Geriatrics at Hackensack University Medical Center in New Jersey, not involved in the research, told MNT she was not surprised by its results.
“Basically, it reinforces the idea that the patient’s behavior or environment has caused changes that affect the way their genes work,” Dr. Parulekar explained. “Many of these altered immune genes are the very same ones that increase an individual’s risk for Alzheimer’s.”
“Alzheimer’s disease is known to have complex pathophysiology, possibly involving multiple genes in combination [with] lifestyle, environmental, and other risk factors. Reading this new article, I am excited to see more evidence of changes in immune cells with changes in genes that were attributed to Alzheimer’s disease. The advancement in this science will likely have implications in [the] prevention and treatment of Alzheimer’s disease.”
– Dr. Manisha Parulekar
MNT also spoke with Dr. Karen D. Sullivan, a board-certified neuropsychologist, owner of the I CARE FOR YOUR BRAIN program, and Reid Healthcare Transformation Fellow at FirstHealth in Pinehurst, NC, about this study.
Dr. Sullivan said that as we do not know much about the peripheral immune system in Alzheimer’s disease, this study is a novel contribution to our understanding of a very complex, multi-faceted neurodegenerative disease.
“The main question I have is the directionality here,” she continued. “Is the peripheral inflammatory response in Alzheimer’s disease a cause or effect? The best thing I take away is that we may have a new therapeutic target in Alzheimer’s disease: restricting peripheral inflammation.”
“We would need to see these results replicated in larger sample sizes and to more deeply understand their relationships to the functional decline of Alzheimer’s disease,” Dr. Sullivan added.
A functioning warp drive would allow humans to reach the far ends of the cosmos in the blink of an eye.
In late 2020, physicist Harold “Sonny” White, PhD, research director of the nonprofit Limitless Space Institute, noticed something peculiar—and familiar—in a circular pattern of data plots generated by a recent experiment.
White and his team in LSI’s Houston laboratory were conducting research for the Defense Advanced Research Projects Agency, or DARPA, and had set up these particular experiments to study the energy densities within Casimir cavities, the mysterious spaces between microscopic metal plates in a vacuum. The data plot indicated areas of diminished energy between the plates, which caused them to push toward each other as if trying to fill the void. This is known as negative vacuum energy density, a phenomenon in quantum mechanics called, appropriately enough, the Casimir effect. It’s something that’s helping scientists understand the soupy physics of microscale structures, which some researchers hope can be applied to energy applications that are more practical, such as circuits and electromechanical systems.
But White noticed that the pattern of negative vacuum energy between the plates and around tiny cylindrical columns that they’d inserted in the space looked familiar. It precisely echoed the energy pattern generated by a type of exotic matter that some physicists believe could unlock high-speed interstellar travel. “We then looked, mathematically, at what happens if we placed a one-micron sphere inside of a four-micron cylinder under the same conditions, and found that this kind of structure could generate a little nanoscale warp bubble encapsulating that central region,” White explains.
That’s right—a warp bubble. The essential component of a heretofore fictional warp drive that has for decades been the obsession of physicists, engineers, and sci-fi fans. Warp drive, of course, is the stuff of Star Trek legend, a device enclosed within a spacecraft that gives the mortals aboard the ability to rip around the cosmos at superhuman speed. To the lay sci-fi fan, it’s a “black box”—a convenient, completely made-up workaround to avoid the harsh realities of interstellar travel. However, after decades of speculation, research, and experimentation, scientists believe a warp drive could actually work.
To emphasize: White didn’t actually make a warp bubble. But the data from his study led to an aha moment: For the first time, a buildable warp bubble showed promise of success.
Casimir cavities are mysterious spaces between microscopic metal plates in a vacuum. Areas of diminished energy between the plates cause them to push toward each other, as if trying to fill the void—referred to as the Casimir effect or Casimir force.
Warp technology’s core science is surprisingly sound. Though the specific mechanics of an actual device haven’t been fully unpacked, the math points toward feasibility. In short, a real-life warp drive would use massive amounts of energy, which can come in the form of mass, to create enough gravitational pull to distort spacetime in a controlled fashion, allowing a ship to speed along inside a self-generated bubble that itself is able to travel at essentially any speed. Warp drives popped up in fiction intermittently for several decades before Star Trek creator Gene Roddenberry plugged one into the USS Enterprise in 1966. But Miguel Alcubierre, PhD, a Mexican theoretical physicist and professed Star Trek enthusiast, gave the idea real-world legs when he released a paper in 1994 speculating that such a drive was mathematically possible. It was the first serious treatment of a warp drive’s feasibility, and it made headlines around the world. His breakthrough inspired more scientists to nudge the theoretical aspects of warp drive toward concrete, practical applications.
“I proposed a ‘geometry’ for space that would allow faster-than-light travel as seen from far away, essentially expanding space behind the object we want to move and contracting it in front,” Alcubierre says. “This forms a ‘bubble’ of distorted space, inside of which an object—a spaceship, say—could reside.”
Physicists tend to speak in relative terms. By injecting the sly qualifier “as seen from far away,” Alcubierre might sound like he’s describing the galactic equivalent of an optical illusion—an effect perhaps similar to driving past a truck going the opposite direction on the highway when you’re both going 60 miles an hour. Sure feels like a buck-twenty, doesn’t it? But the A-to-B speed is real; the warp effect simply shortens the literal distance between two points. You’re not, strictly speaking, moving faster than light. Inside the bubble, all appears relatively normal, and light moves faster than you are, as it should. Outside the bubble, however, you’re haulin’ the mail.
THOUGH THE SPECIFIC MECHANICS OF AN ACTUAL DEVICE HAVEN’T BEEN UNPACKED, THE MATH POINTS TOWARD FEASIBILITY.
Alcubierre’s proposal had solved one of the initial hurdles to achieving warp speeds: The very idea clashes with Einstein’s long-accepted theory of general relativity, which states that nothing can travel faster than the speed of light, but it doesn’t preclude space itself from traveling faster than that. In fact, scientists speculate that the same principles explain the rapid expansion of the universe after the Big Bang.
While concluding that warp speed was indeed possible, Alcubierre also found that it would require an enormous amount of energy to sustain the warp bubble. He theorized that negative energy—the stuff hinted at by White’s experimentation with Casimir cavities—could be a solution. The only problem is that no one has yet proved that negative energy is real. It’s the unobtanium of our spacefaring imaginations, something researchers only believe to exist. In theory, however, this unknown matter may be sufficiently powerful that future warp drive designers could channel it to contract spacetime around it. In conceptual drawings of warp-capable spacecraft, enormous material rings containing this energy source surround a central fuselage. When activated, it warps spacetime around the entire ship. The more intense the warping, the faster the warp travel is achieved.
Of course, it’s not that simple. Physicist José Natário, PhD, a professor at the Instituto Superior Técnico in Lisbon, wrote his own influential paper about the mathematical feasibility of warp drives in 2001. However, he is concerned about practical conundrums, like the amount of energy required. “You need to be able to curve spacetime quite a lot in order to do this,” he says. “We’re talking about something that would be much, much more powerful than the sun.”
Alcubierre is similarly skeptical that his theoretical ideas might ever be used to develop a working warp drive. “In order to have a bubble about 100 meters wide traveling at precisely the speed of light, you would need about 100 times the mass of the planet Jupiter converted into negative energy, which of course sounds absurd,” he says. By that standard, he concludes, a warp drive is very unlikely.
In order to travel at faster-than-light speeds, a warp drive would have to expand space behind a spacecraft and contract space in front, creating a warp bubble that surrounds the vessel.
Physicists love a challenge, though. In the 29 years since Alcubierre published his paper, other scientists have wrestled with the implications of the work, providing alternative approaches to generating the energy using more accessible power sources, finding oblique entry points to the problem, and batting ideas back and forth in response to one another’s papers. They use analogies involving trampolines, tablecloths, bowling balls, balloons, conveyor belts, and music to explain the physics.
They even have their own vocabulary. It’s not faster-than-light travel; it’s superluminal travel, thank you. Then there’s nonphysical and physical—a.k.a. the critical distinction between theoretical speculation and something that can actually be engineered. (Pro tip: We’re aiming for physical here, folks.) They do mention Star Trek a lot, but never Star Wars. Even the scruffiest-looking nerf herder knows that the ships in Star Wars use hyperdrive, which consumes fuel, rather than warp drives, which don’t use propulsive technology but instead rely on, well, warping. They’re also vague about details like what passengers would experience, what gravity is like on board since you’re carrying around boatloads of energy, and what would happen if someone, say, jumped out of the ship while warping. (A speculative guess: Nothing good.)
Such research isn’t typically funded by academic institutions or the DARPAs and NASAs of the world, so much of this work occurs in the scientists’ spare time. One such scientist and Star Trek enthusiast is physicist Erik Lentz, PhD. Now a researcher at Pacific Northwest National Laboratory in Richland, Washington, Lentz was doing postdoctoral work at Göttingen University in Germany when, amid the early, isolated days of the pandemic, he mulled the idea of faster-than-light travel. He published a paper in 2021 arguing that warp drives could be generated using positive energy sources instead of the negative energy that Alcubierre’s warp drive seemed to require.
“There are a number of barriers to entry to actually being able to build a warp drive,” Lentz says. “The negative energy was the most obvious, so I tried to break that barrier down.”
He explored a new class of solutions in Einstein’s general relativity while focusing on something called the weak-energy condition, which, he explains, tracks the positivity of energy in spacetime. He hit upon a “soliton solution”—a wave that maintains its shape and moves at a constant velocity—that could both satisfy the energy-level challenge and travel faster than light. Such a warp bubble could travel along using known energy sources, though harnessing those at the levels needed are still far beyond our capabilities. The next step, he notes, may be bringing the energy requirements for a warp drive to within the range of a nuclear fusion reactor.
A fusion-powered device could theoretically travel to and from Proxima Centauri, Earth’s nearest star, in years instead of decades or millennia, and then go faster and faster as power sources improve. Current conventional rocket technology, on the other hand, would take 50,000 years just for a one-way trip—assuming, of course, there was an unlimited fuel supply for those engines.
“IF YOU COLLIDE WITH SOMETHING ON YOUR PATH, IT WOULD ALMOST CERTAINLY BE CATASTROPHIC.”
Like Alcubierre’s original thesis, Lentz’s paper had a seismic impact on the warp drive community, prompting yet another group of scientists to dig into the challenge. Physicist Alexey Bobrick and technology entrepreneur Gianni Martire have been particularly prolific. In 2021, they released a paper theorizing that a class of subliminal warp drives, traveling at just a fraction of light speed, could be developed from current scientific understanding. While that paper essentially argued that it’s perfectly acceptable to walk before you can run, they followed it up with another theory earlier this year that describes how a simulated black hole, created using sound waves and glycerin and tested with a laser beam, could be used to evaluate the levels of gravitational force needed to warp spacetime. The duo coded that breakthrough into a public app that they hope will help more quickly push theoretical ideas to practical ones. Though the team is waiting for the technology to clear a peer review stage before releasing details, the app is essentially a simulator that allows scientists to enter their warp-speed equations to validate whether they’re practical.
“When somebody publishes a warp metric for the first time, people say, ‘Okay, is your metric physical?’” Martire says. The answer to that question—whether the metric has practical potential or is strictly theoretical—is hard to establish given the challenges of testing these hypotheses. That determination could take six to eight months. “Now we can tell you within seconds, and it shows you visually how off you are or how close you are,” he says.
While useful, the app will speed up the preliminary math only for future researchers. Galaxy-sized challenges remain before we ever experience turbocharged interstellar travel. Alcubierre worries in particular about what may happen near the walls of the warp bubble. The distortion of space is so violent there, he notes, that it would destroy anything that gets close. “If you collide with something on your path, it would almost certainly be catastrophic,” he says.
Natário mulls even more practical issues, like steering and stopping. “It’s a bubble of space, that you’re pushing through space,” he says. “So, you’d have to tell space … to curve in front of your spaceship.” But therein lies the problem: You can’t signal to the space in front of you to behave the way you want it to.
His opinion? Superluminal travel is impossible. “You need these huge deformations that we have no idea how to accomplish,” Natário says. “So yes, there has been a lot of effort toward this and studying these weird solutions, but this is all still completely theoretical, abstract, and very, very, very, very far from getting anywhere near a practical warp drive.” That’s “very” to the power of four, mind you—each crushing blow pushing us exponentially, excruciatingly further and further away from our yearned-for superluminal lives
Ultimately, the pursuit of viable high-speed interstellar transportation also points to a more pressing terrestrial challenge: how the scientific community tackles ultra-long-term challenges in the first place. Most of the research so far has come from self-starters without direct funding, or by serendipitous discoveries made while exploring often unrelated research, such as Dr. White’s work on Casimir cavities.
Many scientists argue that we’re in a multi-decade period of stagnation in physics research, and warp drive—despite its epic time horizons before initial research leads to galaxy-spanning adventures—is somewhat emblematic of that stagnation. Sabine Hossenfelder, a research fellow at the Frankfurt Institute for Advanced Studies and creator of the YouTube channel Science Without the Gobbledygook, noted in a 2020 blog post that physics research has drifted away from frequent, persistent physical experimentation to exorbitant infusions of cash into relatively few devices. She writes that with fewer experiments, serendipitous discoveries become increasingly unlikely. Without those discoveries, the technological progress needed to keep experiments economically viable never materializes.
When asked whether this applied equally to warp drive, Hossenfelder sees a faint but plausible connection. “Warp drives are an idea that is not going to lead to applications in the next 1,000 years or so,” she says. “So they don’t play a big role in that one way to another. But when it comes to the funding, you see some overlap in the problems.”
So, despite all the advances, the horizon for a warp drive remains achingly remote. That hasn’t fazed the scientists involved, though. A few years ago, while teaching in France, White visited the Strasbourg Cathedral with his wife. While admiring its 466-foot-tall spire, he was struck by the fact that construction began in 1015 but didn’t wrap up until 1439—a span of 424 years. Those who built the basement had no chance of ever seeing the finished product, but they knew they had to do their part to aid future generations. “I don’t have a crystal ball,” White says. “I don’t know what the future holds. But I know what I need to be doing right now.”
Summary: Using antidepressants during pregnancy, specifically fluoxetine (found in Prozac and Sarafem), can significantly affect a child’s brain development, particularly in the prefrontal cortex, potentially increasing the risk of mental health disorders later in life.
The research highlights how serotonin, boosted by fluoxetine, directly impacts the development of synaptic connections in the prefrontal cortex, a critical area for high-order cognitive functions.
This study is pioneering in providing experimental evidence of serotonin’s role in early brain development and underscores the need for careful consideration and individualized care in prescribing antidepressants during pregnancy.
Key Facts:
Serotonin’s Role in Brain Development: The study identifies how serotonin directly influences the development of the prefrontal cortex during pregnancy, altering excitatory synaptic connections, which can lead to mental health disorders.
First Evidence of Fluoxetine’s Impact: This research provides the first experimental evidence of the direct effects of fluoxetine on the developing prefrontal cortex, highlighting the drug’s ability to cross the placenta and enter breast milk.
Potential for Early Intervention: Understanding the specific mechanisms by which serotonin affects brain development opens new avenues for early intervention and the creation of therapeutics targeting neurodevelopmental disorders related to serotonin dysregulation.
Source: University of Colorado
A new study published in Nature Communications provides direct evidence that antidepressant use during pregnancy can impact a child’s brain development and contribute to the risk of mental health disorders later in life.
The study, led by researchers at the University of Colorado Anschutz Medical Campus, focused on the effect of fluoxetine, commonly used in medications such as Prozac and Sarafem for treating depression and perinatal depression, on a developing prefrontal cortex.
Since fluoxetine works by increasing the levels of serotonin in the brain, the researchers looked at the impact serotonin has on prefrontal cortex development in a fetus.
“While it is known that serotonin plays a role in the brain development, the mechanisms responsible for this influence, specifically in the prefrontal cortex, have been unclear.
“The prefrontal cortex, the most evolved brain region, plays a central role in highest-order cognition, which is why we focused our study on finding the answer from this brain area,” said lead author Won Chan Oh, PhD, assistant professor in the Department of Pharmacology at CU Anschutz.
Oh and his student, Roberto Ogelman, a neuroscience PhD candidate, found serotonin directly influences nascent and immature excitatory synaptic connections in the prefrontal cortex, which if disrupted or dysregulated during early development can contribute to various mental health disorders.
“Our research uncovers the specific processes at the synaptic level that explain how serotonin contributes to the development of this important brain region during early-life fluoxetine exposure,” adds Oh.
“We are the first to provide experimental evidence of the direct impact of serotonin on the developing prefrontal cortex when fluoxetine is taken during pregnancy, because fluoxetine not only crosses the placenta but also passes into breast milk.”
To study the effect, the researchers looked at the impact of deficiency and surplus of serotonin on brain development in mice. They discovered that serotonin is not just involved in overall brain function but also has a specific role in influencing how individual connections between neurons change and adapt, contributing to the brain’s ability to learn and adjust.
“Understanding this correlation has the potential to help with early intervention and the development of new therapeutics for neurodevelopmental disorders involving serotonin dysregulation,” said Oh.
The researchers say healthcare professionals should be involved in decision-making around individualized care for pregnant women, including discussing the benefits and side effects of antidepressants and possible non-pharmacological interventions for postpartum depression.
The researchers plan to continue studying the impact of fluoxetine, next examining its impact on a developing teenage brain.
Summary: Researchers highlighted that around 13% of Norwegian employees are at high risk of burnout. The study introduces a novel tool, the Burnout Assessment Tool (BAT), designed to identify individuals at risk of burnout by measuring exhaustion, mental distancing, cognitive and emotional impairment.
This tool, now being tested in over 30 countries, aims to facilitate early intervention and prevent the long-term consequences of burnout, which include a range of physical and psychological issues. With a focus on both individual and workplace interventions, the researchers underscore the importance of addressing high demands and limited resources to safeguard employee health.
Key Facts:
Prevalence of Burnout: About 13% of Norwegian workers are identified as being at high risk for burnout, signaling a significant occupational health concern.
Introduction of BAT: The Burnout Assessment Tool is a new, promising instrument for early detection of burnout risks, measuring key factors like exhaustion and cognitive impairment.
Long-term Impact and Solutions: Burnout can lead to serious health issues and decreased productivity. The study emphasizes the need for both individual treatments and workplace adjustments to prevent recurrence and promote a healthier work environment.
Source: NTNU
It is not uncommon for people to “hit the wall” at work and experience burnout for short or long periods of time.
“We have found that approximately 13 per cent of Norwegian employees are at high risk of burnout,” says Leon De Beer, Associate Professor of Work and Organizational Psychology at the Norwegian University of Science and Technology (NTNU) Department of Psychology.
De Beer has contributed to a new study on burnout published in the Scandinavian Journal of Psychology with colleagues from the Healthy Workplaces research group.
“Not addressing the risk of employee burnout in time can have long-term consequences,” says De Beer.
They are working on a new tool that can identify people at risk of burnout. (A simplified version can be found at the bottom of this article.)
Signs that you might be at risk of burnout
If you are facing demands and stress at work that seem to be intractable, and you have frequently experienced the following symptoms in recent weeks, it might be a sign that you are on the verge of burning out:
You feel mentally exhausted at work.
You struggle to feel enthusiastic about your job.
You have trouble concentrating when working.
You sometimes overreact at work without meaning to.
Early intervention is key
It is important to identify the early signs of burnout in order to mitigate the harmful effects. The warning signs are often present before things have gone too far, as long as we manage to identify them.
“Not addressing the risk of employee burnout in time can have long-term consequences,” says De Beer.
The physical and psychological effects of burnout include cardiovascular disease, pain related to musculoskeletal injuries, sleeping problems, and depression. Organisations can also lose talented employees and experience an increase in sickness absence and lost productivity.
A new tool may become standard
De Beer’s research group has trialled a new measurement tool to identify the early warning signs of burnout. In the past, it has not always been that easy.
“Previously, we have not had a detailed enough measurement tool for use in both the field of practice and research that identifies workers who are at risk of burnout,” says De Beer.
There is currently no international standard for assessing burnout.
The new tool is called the Burnout Assessment Tool, or BAT among researchers who have a penchant for amusing abbreviations. The BAT consortium, of which the researchers are a part, is now testing the instrument in more than 30 countries.
“Our studies show that BAT is a good tool for identifying the risk of burnout,” says De Beer.
Burnout is the body’s response to stress
BAT measures four main groups of risk factors: exhaustion, mental distancing, cognitive impairment and emotional impairment.
Burnout is not really an illness, but a feeling of being mentally or physically exhausted – the body’s response to a lasting, demanding situation. (See the fact box.)
Burnout is normally defined as a work-related syndrome, but there is evidence that work–life balance also plays a role. Stress and burnout don’t necessarily stop when you go home at the end of the day, as these effects often extend into other areas of life and vice versa.
Some people may experience years of burnout
For some people, burnout can be stopped in its tracks and solutions found to improve their situation. For others, however, burnout can last for years if the problem isn’t addressed.
“We can deal with burnout through individual treatment, but it is of little use if people return to a workplace where the demands are too high and there are few resources. It is then highly likely that the employee will become ill again. Therefore, it is important to create good working conditions and structures that safeguard the health of employees,” says Professor Marit Christensen at NTNU’s Department of Psychology.
Studied 500 workers
The researchers studied a representative sample of 500 Norwegian workers. Norway is roughly on par with the EU average when it comes to mental health, but somewhat better when it comes to work-related matters.
A lower percentage of the Norwegian population struggles with exhaustion in connection with work. Somewhat fewer people than the EU average report health hazards at work, and we experience a better work–life balance.
“Using a recognised method, we found that around 13 per cent of the 500 surveyed workers were at high risk of burnout,” says Professor Christensen.
The tool can help identify who requires the most urgent follow up so that the risk of burnout can be reduced.
Uncertain whether Norwegian numbers are high
We do not yet know whether the prevalence of burnout in Norway is high in an international context. The Norwegian study is among several BAT studies that are currently taking place, so these answers will be available at a later date.
The tool is intended to be culturally independent, and it certainly works well in Norway. The researchers also found that the tool works regardless of gender.
“For entertainment and educational purposes, interested parties can use our online tool to test if they are at risk of burnout,” says Professor Christensen.
“Please note that the tool only gives an indication of risk and does not provide any type of formal diagnosis or medical advice. If you are concerned about your levels of work-related stress, we encourage you to visit a health care provider to discuss the matter,” says Professor Christensen.
Abstract
The psychometric properties of the Burnout Assessment Tool in Norway: A thorough investigation into construct-relevant multidimensionality
Objective
The World Health Organization recognizes burnout as an occupational issue. Nevertheless, accurately identifying employee burnout remains a challenging task. To complicate matters, current measures of burnout have demonstrated limitations, prompting the development of the Burnout Assessment Tool (BAT). Given these circumstances, conducting an in-depth examination of the BAT’s construct-relevant multidimensionality is crucial.
Method
This study focuses on both the original 23-item BAT and the short 12-item version, using modern factor analytic methods to investigate reliability, validity, and measurement invariance in a representative sample from Norway (n = 493; 49.54% women).
Results
Our findings revealed that the bifactor exploratory structural equation modeling solution (burnout global factor and four specific burnout component factors) best explained the data for both BAT versions. All factors demonstrated adequate omega coefficients, with the global factor showing exceptional strength. Both BAT versions correlated highly with each other and with another burnout measure, suggesting convergent validity. Furthermore, both BAT versions achieved full (strict) measurement invariance based on gender. Finally, our results showed that burnout acts as a mediator in our proposed job demands–resources model as preliminary evidence of predictive validity.
Conclusions
The study validates the Burnout Assessment Tool in the Norwegian context. The study supports the reliability, validity, and unbiased nature of the tool across genders. The findings also reinforce the importance of job demands and resources, along with burnout as a key mediator, in understanding workplace dynamics in accordance with job demands–resources theory.
“The superior physician treats the disease before it manifests; the average physician treats the disease on the verge of developing; the inferior physician treats the fully manifested diseases.” This quotation is from one of the earliest books on traditional Chinese medicine, written more than 1,400 years ago by the legendary physician and philosopher Sun Simiao. The statement echoes the essence of preventive medicine. More than a millennium later, it still holds true, testifying to its enduring wisdom and legacy.
The primary prevention of anthracycline-induced cardiotoxicity (AIC) aims to mitigate the cardiac injury during treatment. Ideally, the most effective approach would involve minimizing exposure to anthracyclines or avoiding their use entirely. Nevertheless, despite substantial advancements in cancer therapy, anthracyclines, which have been in clinical use for more than one-half a century, are still the mainstay for treating numerous cancers, including breast cancer, sarcoma, leukemia, and lymphoma. Consequently, AIC continues to hold importance in cardio-oncologic practice. Various cardioprotective strategies, including neurohormonal antagonists and statins, have been explored to mitigate AIC. Previously published small to medium-sized randomized trials have reported mixed results. Meta-analyses have showed an absolute 2% to 4% attenuation of left ventricular ejection fraction (LVEF) declines in groups with neurohormonal blockade compared with placebo, but these analyses are marked by heterogeneity (I2 >90%, where >50% indicates severe heterogeneity), severely limiting the interpretability of pooled estimates.1 Recent randomized studies further investigated their effects on LVEF decline measured by cardiac magnetic resonance, which is considered the gold standard for LVEF measurements.
PRADA (Prevention of Cardiac Dysfunction During Adjuvant Breast Cancer Therapy) demonstrated that candesartan but not metoprolol had an early protective effect on LVEF decline, but this effect was not apparent at 2-year follow-up.2 The mean LVEF decline was only 2.6% in the placebo group. With a cumulative doxorubicin-equivalent dose of 192 mg/m2, among 120 patients with breast cancer, 1 patient developed heart failure (HF) concurrent with atrial fibrillation. The PREVENT (Preventing Anthracycline Cardiovascular Toxicity With Statins) trial comparing atorvastatin 40 mg/d with a placebo revealed no difference in mean LVEF decline after anthracycline-based chemotherapy.3 Most patients had breast cancer, with a median cumulative dose of 240 mg/m2 doxorubicin equivalent, and had up to 2-year follow-up. The mean LVEF decline in the placebo group was 3.3%, and 1 HF event was reported among 279 patients.
The small to moderate cumulative doses of anthracycline in these 2 studies are likely a main factor accounting for the subtle declines in LVEF observed in the placebo group, which potentially renders the difference in LVEF decline a limited primary outcome for these trials. Notably, the incidence of HF events is scarce in these studies. It is well known that AIC is dose dependent, with risk escalating at a cumulative dose exceeding 250 mg/m2.4 This relationship is well reflected in the findings of the recently published STOP-CA (Statins to Prevent the Cardiotoxicity of Anthracyclines) trial.
The STOP-CA trial, investigating the efficacy of atorvastatin 40 mg/d in patients with lymphoma and a median cumulative dose of 300 mg/m2 doxorubicin equivalent, demonstrated a significant reduction in the primary endpoint of a 10% decrease to an LVEF <55% at 1 year in patients randomized to atorvastatin compared with placebo (9% vs 22%; P = 0.002).5 The mean LVEF decline of 5.4% in the placebo group was larger than in the PRADA and PREVENT trials. However, the overall difference in LVEF decline between the placebo and atorvastatin groups was only 1.3% (P = 0.029). In contrast, a much larger mean LVEF decline of 7.1% in the placebo group, with a cumulative dose of ≥250 mg/m2, was observed. Of particular note, among 300 patients, 13 adjudicated HF events (4% in total, 9 in the placebo group and 4 in the atorvastatin group) were reported over a 24-month follow-up. The study was not powered to show the benefit of atorvastatin in reducing HF events.
To date, no studies involving either neurohormonal therapies or statins have demonstrated a benefit in reducing the incidence of HF.4 The clinical implication of a mild LVEF decline and the risks for progression to HF are poorly understood, but HF has a profound clinical impact, with a 5-year mortality rate exceeding 50%, a rate worse than for many types of malignancy.6 The increased incidence rate of HF (4%) in the STOP-CA trial is concerning, which brings another cardioprotective medication, dexrazoxane, back into focus.
Dexrazoxane is the only U.S. Food and Drug Administration–approved drug for the prevention of AIC. This approval in 1997 was based on 2 randomized trials (088001 and 088006) involving 534 women with advanced breast cancer (Table 1).7 In these studies, women were randomized to receive doxorubicin, with or without dexrazoxane. Cardiac events were defined as a decline in LVEF from baseline of ≥10% and below the institution’s lower limit of normal, a decline in LVEF of ≥20% from baseline, or the new onset of HF. In study 088001, dexrazoxane was associated with a significant reduction in cardiac events at 15%, compared with 31% in the placebo group (HR: 2.63; 95% CI: 1.61-4.27). Study 088006 mirrored these findings, with 14% of dexrazoxane recipients experiencing cardiac events, compared with 31% in the placebo group (HR: 2.0; 95% CI: 1.01-3.96). The substantial effect led to open-label dexrazoxane use in patients on placebo who had received a cumulative doxorubicin dose of 300 mg/m2. Again these patients experienced a remarkable reduction in cardiac events, even with the delayed initiation of dexrazoxane (HR: 3.5; 95% CI: 2.2-5.7).8 In total, 24 patients (8%) developed HF: 22 in placebo groups and only 2 patients in dexrazoxane groups. The median cumulative dose of doxorubicin was not detailed in these studies. However, among those who developed HF, only 1 patient had HF at a cumulative dose of 150 mg/m2, 4 at 300 mg/m2, and the remaining 19 at doses exceeding 400 mg/m2.9
Subsequent trials and the most recent Cochrane analysis have consistently corroborated dexrazoxane’s efficacy in reducing the HF risk (2.5- to 4.5-fold compared with placebo) without compromising the anticancer efficacy of chemotherapy or increasing secondary malignancy risks in adults.10
Moreover, certain malignancies still necessitate large cumulative doses of anthracycline because of its substantial antitumor efficacy. Cardiotoxicity increases markedly when the cumulative dose of doxorubicin exceeds 400 mg/m2, with 26% of patients developing HF at doses reaching 550 mg/m2. In a pediatric trial (P9754) involving 242 patients with osteosarcoma, all patients received doxorubicin together with dexrazoxane. The cumulative dose of doxorubicin was between 450 and 600 mg/m2. Only 5 patients developed grade 1 or 2 cardiotoxicities (LVEF decline to ≤50%), and 4 of them were transient. Remarkably, there were no HF events, and concurrent use of dexrazoxane allowed cumulative doxorubicin doses up to 600 mg/m2.11 This underscored dexrazoxane’s efficacy in mitigating AIC, enabling the administration of higher cumulative doses of anthracycline while mitigating HF risk.
At present, the 2022 European Society of Cardiology (ESC) cardio-oncology guidelines do not recommend the routine use of dexrazoxane in patients undergoing anthracycline treatment. Dexrazoxane is listed as a Class 2a recommendation (Level of Evidence: B) for the primary prevention of AIC in adult patients at high and very high risk.4 These risk parameters, as outlined in the guidelines, include LVEF <50%, age ≥80 years, prior anthracycline exposure, and an intended cumulative dose of doxorubicin or its equivalent ≥250 mg/m2, among others, as categorized in the guidelines.4 In the STOP-CA trial,5 73% patients received cumulative doses ≥250 mg/m2, and 55% of patients received ≥300 mg/m2. None of them received dexrazoxane. Although the trial did not specify cumulative doses for the 13 patients who developed HF, given the well-established correlation between cumulative dose and HF, we speculate that the majority likely received doses exceeding 300 mg/m2. In such cases, the early introduction of dexrazoxane might have mitigated many of these HF events, given its proven efficacy in clinical studies. The STOP-CA trial preceded the current ESC guideline recommendations, but the significant benefits of dexrazoxane have been validated over 2 decades. In cardio-oncology, defining a primary vs secondary prevention strategy is complex. The current ESC cardio-oncology guideline recommendations regarding the specific indications for dexrazoxane use for primary prevention may require further validation. Nevertheless, the concomitant administration of doxorubicin and dexrazoxane (with dexrazoxane administered at least 30 minutes prior to each anthracycline cycle) could be valuable for patients at high or very high risk, who might otherwise be precluded from treatment because of baseline left ventricular dysfunction and other cardiovascular conditions. Furthermore, initiating dexrazoxane when the intended cumulative dose of doxorubicin exceeds 250 mg/m2, even for patients at otherwise low or moderate risk, could prevent AIC and allow patients to receive higher cumulative anthracycline doses for curative purposes. Therefore, it is our view that in clinical practice, dexrazoxane should not be overlooked, particularly for high-risk patients including those receiving atorvastatin. The use of dexrazoxane could further decrease the incidence of AIC, as uniformly demonstrated in clinical studies.
Dexrazoxane has been significantly underused since its approval, despite compelling evidence of its efficacy in mitigating anthracycline-induced HF, which reflects a broader disconnect between clinical trial evidence and real-world clinical practice. Oncologists’ reluctance to use dexrazoxane may stem from several concerns. The impact of dexrazoxane on antitumor efficacy was initially observed in 1 early study in which it was used concurrently with doxorubicin.7 However, this concern was not confirmed in the same study with longer follow-up8 or in subsequent studies and meta-analyses.10 Concerns regarding secondary malignancies, such as acute myeloid leukemia and brain tumors, have been reported only in pediatric patients, with a slight trend favoring the control group.10 Furthermore, there is a consideration that dexrazoxane may exacerbate myelosuppression caused by chemotherapeutic agents, as evidenced by a lower nadir in white blood cell count in the dexrazoxane group, although no significant differences were observed in the incidence rates of thrombocytopenia, neutropenia, and anemia.10 Overall, the totality of available evidence robustly supports the use of dexrazoxane in adult patients at high risk for developing AIC. To bridge this gap, a focused educational initiative is pivotal to augment awareness of dexrazoxane’s role in mitigating AIC and to translate trial findings into tangible clinical benefits. A coordinated effort should be made by cardio-oncology programs to have direct case-by-case discussions between cardiologists and oncologists to assess cardiotoxicity risks in patients undergoing anthracycline-based chemotherapy. An update to existing guidelines to reinforce the substantial cardioprotective evidence supporting dexrazoxane and to lessen the concern regarding its impact on chemotherapy efficacy and secondary malignancy risks could significantly aid such initiatives. Furthermore, in our view, a larger trial is needed to further explore the cardioprotective effect of dexrazoxane, both alone and possibly in combination with statins in patients receiving high cumulative doses of anthracycline, with the outcomes of LVEF decline and HF incidence. Defining the patient subset who would derive the greatest benefit is also an important priority for both cardiologists and oncologists.
In summary, with a low to moderate cumulative dose of anthracycline (<250 mg/m2), the LVEF decline tends to be modest, and the occurrence of HF events remains relatively rare. Although neurohormonal therapies and statins hold equivalent ESC guideline recommendations as dexrazoxane,4 the existing body of evidence for dexrazoxane is notably more compelling and consistent. In clinical practice, a reasonable approach would involve continuing statins or neurohormonal antagonists for those already receiving these drugs for the management of atherosclerotic cardiovascular disease5 and considering to start statins for those at high risk. Dexrazoxane should be considered for patients at high risk, and it is our view that there is benefit, particularly for those intending to receive cumulative doses of doxorubicin ≥250 mg/m2. Implementing such approaches in daily oncologic practice could significantly decrease the incidence of AIC and holds a promise for making anthracycline-induced HF a rarity in clinical practice.



 MIT
MIT
 OatmealStories//Getty Images
OatmealStories//Getty Images zeljkosantrac//Getty Images
zeljkosantrac//Getty Images Tolimir//Getty Images
Tolimir//Getty Images Westend61//Getty Images
Westend61//Getty Images KarinaUrmantseva//Getty Images
KarinaUrmantseva//Getty Images Cavan Images//Getty Images
Cavan Images//Getty Images kajakiki//Getty Images
kajakiki//Getty Images Alicia Llop//Getty Images
Alicia Llop//Getty Images Ivaylo Ivanov / EyeEm//Getty Images
Ivaylo Ivanov / EyeEm//Getty Images Westend61//Getty Images
Westend61//Getty Images




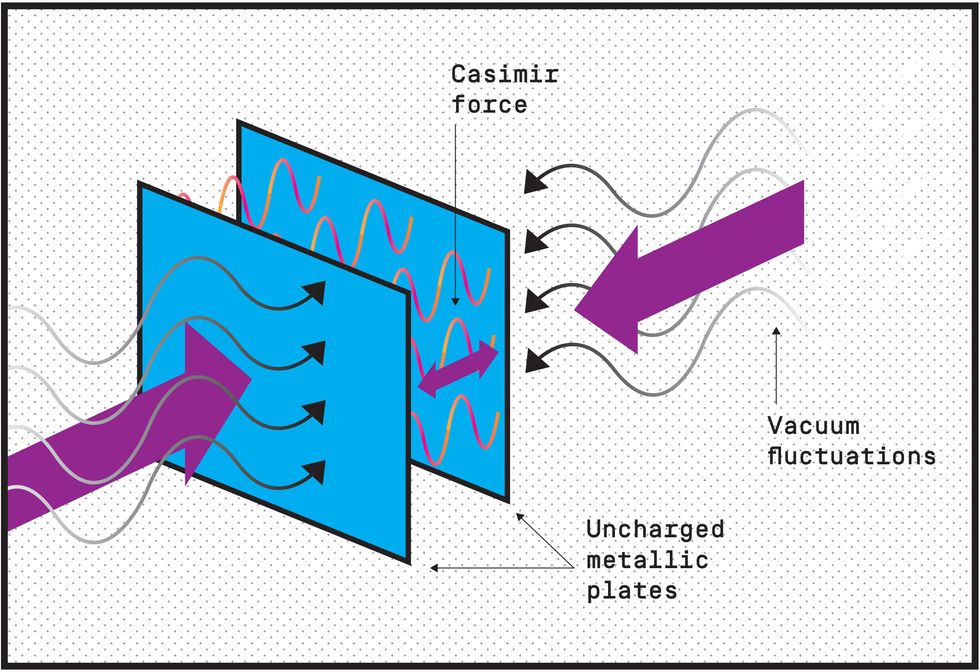


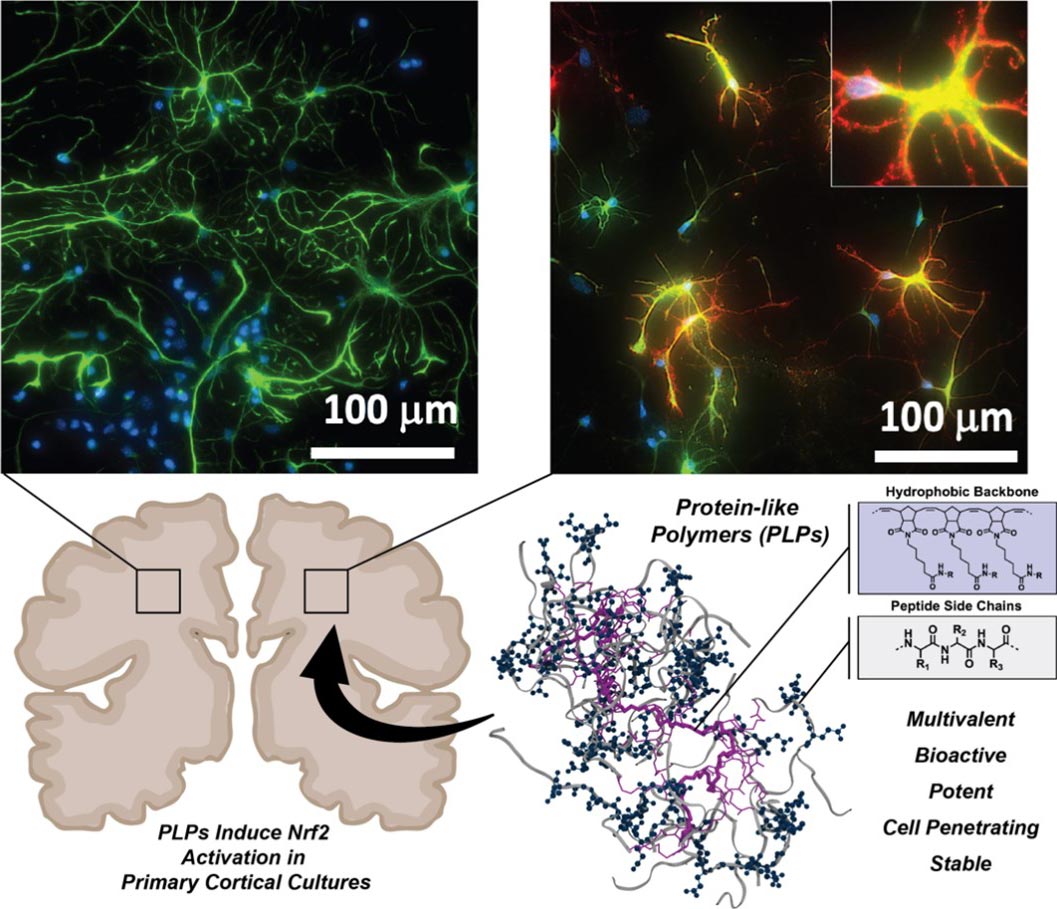{kind=link}