The microbiota plays an important part in host defense by excluding pathogenic species in a process called colonization resistance. This property is elusive and not endowed by one or two species alone. Spragge et al. discovered that colonization resistance is a higher-order effect of a diverse community of bacteria underpinned by essential key species such as Escherichia coli (see the Perspective by Radlinski and Bäumler). In vitro and in vivo experiments showed that given the right composition, a diverse microbiota will collectively consume the nutrients that an incoming species requires to grow and establish in a host. Colonization resistance is predictable because if the symbiont community encodes many of the same (or similar) proteins as the pathogen, then it provides better colonization resistance and can potentially deliver health benefits to the host. —Caroline Ash
Structured Abstract
INTRODUCTION
The diverse bacterial species that colonize the human gut, which are collectively known as the gut microbiota, provide important health benefits. One of the key benefits is colonization resistance—the ability to restrict colonization of the gut by pathogens that can trigger disease. Multiple mechanisms have been found to influence the ability of the microbiota to provide colonization resistance, but these mechanisms are often context-specific and dependent on particular strains or species of bacteria. As a result, we lack general principles to predict which microbiota communities will be protective versus those that will allow pathogens to colonize.
RATIONALE
We used an ecological approach to study the colonization resistance provided by human gut symbionts against two important bacterial pathogens, Klebsiella pneumoniae and Salmonella enterica serovar Typhimurium. We studied colonization resistance provided by symbionts both alone and in combinations of increasing diversity to identify general patterns underlying colonization resistance, using both in vitro assays and in vivo work with gnotobiotic mice.
RESULTS
We cultured 100 human gut symbionts individually with K. pneumoniae and then S. Typhimurium and ranked the symbionts on the basis of their ability to provide colonization resistance. However, even the best-performing species provided limited protection against the pathogens in our assays. By contrast, when we combined species into diverse communities of up to 50 species, we found cases in which pathogen growth was greatly limited. The same patterns were observed when germ-free mice were colonized by a subset of these communities and challenged with a pathogen. Ecological diversity, therefore, was important for colonization resistance, but we also found that community composition was important. Both in vitro and in vivo, we found that colonization resistance rested upon certain species being present, even though these species offer little protection on their own. We were able to explain these patterns from the ability of some communities to block pathogen growth by consuming the nutrients that the pathogen needs. Nutrient blocking is thus promoted both by diversity and by the presence of certain key species that increase the overlap between the nutrient use of a community and a pathogen. As a result, the inclusion of a key species closely related to a pathogen can be central to making a community protective because it provides a higher degree of metabolic overlap. However, this alone is typically not sufficient. We found that the presence of additional, often distantly related species is also needed to ensure that nutrient blocking—and consequently, colonization resistance—occurs. Lastly, we used the nutrient-blocking principle to predict in silico more-protective and less-protective communities for a new target strain, an antimicrobial resistant Escherichia coli clinical isolate. We then tested the colonization resistance of these communities experimentally. This work revealed that we can successfully identify protective communities from a large number of possible combinations, using both phenotypic measures of metabolic overlap but also a more general measure of genomic overlap.
CONCLUSION
Our results support the idea that more-diverse microbiomes can provide health benefits, specifically that they can improve protection against pathogen colonization. We also find that colonization resistance is a collective property of microbiome communities; in other words, a single strain is protective only when in combination with others. Crucially, although increased microbiome diversity increases the probability of protection against pathogens, the overlap in nutrient-utilization profiles between the community and the pathogen is key. Our work suggests a route to optimize the composition of microbiomes for protection against pathogens.
Microbiome diversity protects against pathogens by nutrient blocking.Pathogens (red) fail to colonize when they overlap with the community (yellow and green bacteria) in nutrient-utilization profiles (nutrient niches are indicated by colored circles). As microbiome diversity increases, the probability that different nutrients are consumed increases, which helps to block pathogen growth and improve colonization resistance.
Abstract
The human gut microbiome plays an important role in resisting colonization of the host by pathogens, but we lack the ability to predict which communities will be protective. We studied how human gut bacteria influence colonization of two major bacterial pathogens, both in vitro and in gnotobiotic mice. Whereas single species alone had negligible effects, colonization resistance greatly increased with community diversity. Moreover, this community-level resistance rested critically upon certain species being present. We explained these ecological patterns through the collective ability of resistant communities to consume nutrients that overlap with those used by the pathogen. Furthermore, we applied our findings to successfully predict communities that resist a novel target strain. Our work provides a reason why microbiome diversity is beneficial and suggests a route for the rational design of pathogen-resistant communities.
Although chronic diarrhea and constipation are common, the treatment is symptomatic because their pathophysiology is poorly understood. Accumulating evidence suggests that the microbiota modulates gut function, but the underlying mechanisms are unknown. We therefore investigated the pathways by which microbiota modulates gastrointestinal motility in different sections of the alimentary tract.
Methods
Gastric emptying, intestinal transit, muscle contractility, acetylcholine release, gene expression, and vasoactive intestinal polypeptide (VIP) immunoreactivity were assessed in wild-type and Myd88-/-Trif-/- mice in germ-free, gnotobiotic, and specific pathogen-free conditions. Effects of transient colonization and antimicrobials as well as immune cell blockade were investigated. VIP levels were assessed in human full-thickness biopsies by Western blot.
Results
Germ-free mice had similar gastric emptying but slower intestinal transit compared with specific pathogen-free mice or mice monocolonized with Lactobacillus rhamnosus or Escherichia coli, the latter having stronger effects. Although muscle contractility was unaffected, its neural control was modulated by microbiota by up-regulating jejunal VIP, which co-localized with and controlled cholinergic nerve function. This process was responsive to changes in the microbial composition and load and mediated through toll-like receptor signaling, with enteric glia cells playing a key role. Jejunal VIP was lower in patients with chronic intestinal pseudo-obstruction compared with control subjects.
Conclusions
Microbial control of gastrointestinal motility is both region- and bacteria-specific; it reacts to environmental changes and is mediated by innate immunity-neural system interactions. By regulating cholinergic nerves, small intestinal VIP plays a key role in this process, thus providing a new therapeutic target for patients with motility disorders.
Iain Campbell, a researcher in Scotland, has lived with bipolar disorder since he was young. After trying the ketogenic diet, he discovered profound improvements in his symptoms — and now wants to learn if it can do the same for others. He shared his recent findings at the Metabolic Health Summit in Clearwater, Fla., on Jan. 25.
Iain Campbell was gazing out the bus window on his way to work when he first sensed something radical was reshaping how he experienced the world.
The inkling emerged from an altogether ordinary observation: He felt peaceful, maybe even happy as he watched the trees along the road pass by.
“I hadn’t experienced that in a really long time, probably since I was a kid,” says Campbell, who lives in Edinburgh, Scotland.
“I didn’t know what was going on at the time, but I thought this might be what it feels like to be normal.”
Campbell had lived with bipolar disorder for much of his life. Mental illness runs in his family, and he’d lost loved ones to suicide. Over the years, he tried different treatments, but it had become “increasingly difficult to live with.”
What had changed? A few weeks earlier, he’d started a new diet.
Campbell dealt with unwanted weight gain and metabolic troubles, a common side effect of psychiatric medications.
In an effort to lose weight, he drastically cut back on carbs and instead focused on protein and fat. It turns out he’d unknowingly entered ketosis: A metabolic state where the body switches from glucose as its primary energy source to ketones, which come from fat.
He started learning about the ketogenic diet, which is high fat and very low carb, on podcasts and YouTube videos. Soon, he was tracking his ketone levels, courtesy of an at-home blood test.
“I realized it was actually the ketone level that was making this shift in my symptoms in a way that nothing else ever had,” he says. “It struck me as really significant, like life-changing.”
A career-launching moment
How exactly was a diet performing this alchemy? Campbell decided to pursue a Ph.D. in mental health at the University of Edinburgh, hoping to do his own research and learn whether it could help others.
In online forums, people with bipolar disorder were sharing similar anecdotes — they were finding improvements in their mood, increased clarity and fewer episodes of depression.
But as Campbell searched for ways to launch a proper clinical trial to test the diet’s effectiveness, he became discouraged.
“It was really like you were considered wacky,” he says. “At one point, I thought nobody’s going to pay for this research.”
He put together a 45-minute video summing up the biological rationale for using the ketogenic diet in bipolar disorder and posted it on social media, not expecting much after that.
The ketogenic diet avoids most carbs and instead focuses on high-fat foods, proteins and vegetables.
But some doctors had already started researching it after seeing the potential in their practice, among them Chris Palmer, a psychiatrist at Harvard Medical School and McLean Hospital.
Palmer had his own revelation about the diet a few years earlier, which he detailed in a 2017 case report. Two patients with schizo-affective disorder had “truly dramatic, life-changing improvement in their psychotic symptoms,” he says.
In early 2021, he started working with the eldest son of Jan and David Baszucki, a wealthy tech entrepreneur. Their son Matt had bipolar disorder and had been on many medications in recent years.
Jan Baszucki enlisted Palmer’s help as her son gave the ketogenic diet a try.
“Within a couple of months, we saw a dramatic change,” she says.
Inspired, she started contacting clinicians and researchers, looking to bring more visibility — and funding — to the treatment. Since rigorous data on the diet is still lacking, she wants to see researchers conduct large clinical trials to back up anecdotes like her son’s recovery.
Soon a big-time philanthropist was in touch with Campbell, ready to pay for his bipolar study — and others.
Now, around a dozen clinical trials are in the works, testing the diet’s effect on mental illness, most notably for bipolar disorder, schizophrenia and depression, but also for conditions like anorexia, alcoholism and PTSD.
“The research and the clinical interest is suddenly exploding,” says Dr. Georgia Ede, a psychiatrist in Massachusetts, who began using the ketogenic diet in her own practice about a decade ago.
From epilepsy care to the mainstream
The classic ketogenic diet contains an eye-popping amount of fat, roughly 90% of calories coming from that alone. Other versions have come along that dial down the fat and allow more room for protein and slightly more carbohydrates.
Dr. Chris Palmer (left) signs a copy of his book, Brain Energy, for Addanilka Ramos during the Metabolic Health Summit in Clearwater, Fla. Palmer has been researching the keto diet for years.
Serious followers may buy a device to measure ketone levels in their blood, to track whether they’ve entered a range that means they’re experiencing what’s called nutritional ketosis.
The diet’s entrance into the mainstream has fed plenty of debate about its merits, with some medical groups raising concerns. Yet, there’s also growing attention — and clinical trials underway — on its potential, not only for obesity but a variety of other conditions.
“It’s not a fad diet,” says Dr. Shebani Sethi, who’s leading research into the diet’s potential for mental health at Stanford University. “It’s a medical intervention.”
The ketogenic diet was developed over a hundred years ago for pediatric epilepsy and has seen a resurgence in that field over the last three decades.
“It’s a general standard of care for epilepsy,” says Dr. Eric Kossoff, a pediatric neurologist at Johns Hopkins University.
This track record in epilepsy, the thinking goes, paves the way for its adoption in psychiatry. There are links between the conditions. Medications developed for seizures are regularly prescribed for a range of psychiatric conditions such as bipolar disorder.
“We use them off label, even when we don’t have studies to suggest or prove that they are helpful for people with mental illness,” says Palmer. “So, in many ways, this is nothing new.”
People with psychiatric disorders are at an increased risk. And it’s not just that psychiatric meds can cause weight gain and other issuses. Research shows these problems can arise even before someone with serious mental illness takes medication or is diagnosed.
“We’ve known for a long time that there’s something going on in the metabolism of the brain that’s not quite right in people with severe mental illness,” says Dr. Dost Öngür, chief of the division of Psychotic Disorders at McLean Hospital and a professor at Harvard Medical School.
This evidence of energy problems in the brain and elsewhere in the body has accumulated over the decades in psychiatry — unrelated to the ketogenic diet.
“We can’t say that there’s a causal relationship, but there are a lot of connections that should be explored further,” says Öngür, whose work has focused on this theme in bipolar and schizophrenia.
All of this data is strong enough to suspect that “metabolic problems may be more than just innocent bystanders,” that they may, in fact, play a direct role in the development, severity or course of psychiatric conditions,” says Ede.
Some people use at-home devices to measure ketone levels in the blood to track whether they’ve entered nutritional ketosis.
The theory behind keto’s power
So, how exactly could a diet that stops seizures also exert powerful effects on tough-to-treat psychiatric illness?
Even after decades, scientists who study epilepsy aren’t exactly sure why it works for that illness.
“It’s impacting so many different mechanisms,” says Dominic D’Agostino, a professor of molecular pharmacology and physiology at the University of South Florida who studies the ketogenic diet.
That’s why he likes to characterize the diet as being more like a “shotgun” than a “bullet.”
During ketosis, the body essentially changes metabolic gears. It increasingly draws on ketones — made from the breakdown of fat in the liver – instead of glucose.
“We know this happens on a ketogenic diet,” says Kossoff. “Ketones can be used for energy, but how that helps seizures is the next tricky question.”
Because the diet eliminates carbohydrates, blood sugar comes down and insulin sensitivity improves.
“You take pressure off of your really delicate insulin signaling system,” says Ede, while offering cells another fuel that could bring parts of the “brain back online that may have been stuttering.”
Palmer and other scientists believe problems with mitochondria — the powerhouses of the cells that produce energy — are central to mental illness.
“This is likely due to mitochondria’s essential role in maintaining key brain function,” says Ana Andreazza, a professor of pharmacology and psychiatry at the University of Toronto.
In her lab, Andreazza studies what biological pathways make people with psychiatric illness more vulnerable to mitochondrial dysfunction.
Cumulative damage to these vital powerhouses ultimately leads to a “metabolic shift” that wreaks havoc in myriad ways — what’s apparent in their increased production of lactate.
“The findings are compelling for many psychiatric disorders,” she says.
It’s possible the ketones help the mitochondria by relieving oxidative stress — a harmful buildup of free radicals, she says, and by providing an energy source that circumvents the dysfunctional machinery in the mitochondria.
“Once you trend towards more normal mitochondrial function and metabolic health, that’s restoring neurotransmitter systems, it’s even restoring blood flow to the brain,” says D’Agostino.
Keto diet followers have to get used to embracing larger amounts of fat in their diet. The classic form calls for 90% of calories from fat.
Scientists search for more clues
The effect of ketosis on the mitochondria is one hypothesis for why keto diets could work, but it may not be the whole story.
Much of the data on how the diet affects the brain comes from research into epilepsy and other neurological diseases like Alzheimer’s and Parkinson’s.
Scientists find serious mental illnesses like schizophrenia, major depression and bipolar disorder share notable similarities with these conditions: Inflammation in the brain, oxidative stress, mitochondrial dysfunction, and issues with glucose and insulin.
Research suggests ketosis can be beneficial on these fronts, although human studies are limited. Some of the larger clinical trials now underway for keto diets will seek to pin down what’s going on.
For example, Dr. Deanna Kelly is trying to determine if the diet’s potential benefits emerge from the microbiome in the gut.
“You’re potentially changing the way bacteria are functioning and that could affect your behavior and your brain,” says Kelly, a professor of psychiatry at the University of Maryland School of Medicine, who’s leading an inpatient trial on the ketogenic diet for schizophrenia.
Other scientists are studying the diet’s effect on neurotransmitters like GABA — which acts as a kind of brake in the brain.
Dr. Mary Phillips, who has studied how dopamine affects the reward circuit in bipolar disorder, thinks that may help explain its therapeutic effects.
She hopes her clinical trial of bipolar and the keto diet, which launched recently, also gets at a very practical question:
“How do you know which people the ketogenic diet is going to work for?” says Phillips, a professor of psychiatry at the University of Pittsburgh. “It’s not the easiest diet in the world to get started on.”
Early evidence shows promise
Much of the current evidence on its potential for mental health comes from case reports, observational data and open trials that have laid the groundwork for more rigorous studies.
The research that exists shows improvements in both mental and metabolic health.
Iain Campbell’s small pilot study, designed to test the feasibility of a randomized controlled trial, found patients lost an average of about 10 pounds and had “significant reductions” in blood pressure.
“As the ketone level went up, we saw their mood improved, their energy improved, their anxiety decreased and their impulsivity decreased,” says Campbell, who’s now a Baszucki research fellow in metabolic psychiatry at the University of Edinburgh.
Their blood lactate levels, a sign of mitochondrial dysfunction, dropped as did glutamate in the brain, an effect also seen with anti-seizure medications.
A recent study from Toulouse, France, is the largest to look at hospitalized patients with severe mental illness.
Though three patients couldn’t stick with it, the 28 who did had substantial improvements in their symptoms of depression and psychosis by the third week, says Ede, a co-author of the study.
Ultimately, 43% achieved clinical remission.
There was no control group, but she points out these patients had been hospitalized before under the care of the same psychiatrist — with the only clear difference in treatment this time being the ketogenic diet.
“So we believe the diet probably had something to do with the outcome,” says Ede.
At Stanford, Sethi’s pilot study found the majority of patients with schizophrenia or bipolar disorder had “clinically meaningful improvement” on the diet and close to half “achieved recovery.”
A quarter of those who entered the study had metabolic syndrome — a cluster of risk factors like insulin resistance and high blood pressure — and by the end, had reversed the condition.
Dr. Anissa Abi-Dargham, who isn’t involved in the research, calls the initial data “intriguing,” when considered alongside the existing evidence on epilepsy, and metabolic dysfunction in psychiatric illness.
“All this together convinces me there is a signal that is worth pursuing in a rigorous way,” says Abi-Dargham, chair of the department of psychiatry and behavioral health at Stony Brook University.
But the rush of attention ahead of solid clinical data has raised eyebrows among some psychiatrists.
Dr. Drew Ramsey worries the hype has created an unrealistic perception about the ketogenic diet in mental health. For now, he remains skeptical.
“Does it work? It works for some people, which is awesome, but most things work for some people in mental health,” says Ramsey, a nutritional psychiatrist.
Proponents readily acknowledge the field is still in the early stages.
“You have to be modest about this,” says Öngür. “The ketogenic diet is really a test case, but it’s not the silver bullet.“
Palmer says the diet is a powerful intervention, but “it’s not going to cure everybody with mental illness, or even necessarily help everybody.”
Metabolic psychiatry takes off
The groundswell of excitement around a high-fat, minimal carb diet reflects a broader movement to better recognize the link between metabolic health and mental illness.
Ketogenic diet research is just one branch of a growing area of research now being called metabolic psychiatry.
Dr. Shebani Sethi, a psychiatrist at Stanford, is pioneering research in the field of metabolic psychiatry, including the ketogenic diet’s potential for treating serious mental illness.
Sethi, who coined the term when she launched Stanford’s program in 2015, says the idea is to study how treating metabolic health — tackling conditions like high blood sugar, insulin resistance and obesity — may also improve psychiatric problems.
While keto is the most prominent example, she says medications are also under study, including drugs that make the body more sensitive to insulin — the hormone that helps usher glucose into cells.
This approach is intuitive for Sethi, who trained in obesity medicine and psychiatry. It was in medical school that she first witnessed keto’s potential for her psychiatric patients.
A woman with treatment-resistant schizophrenia had tried the diet to lose weight and manage her diabetes. To her surprise at the time, Sethi recalls it also helped the patient with hallucinations.
A recent clinical trial underscores the promise of targeting metabolic problems, beyond just the ketogenic diet.
Patients with treatment-resistant bipolar depression and insulin resistance, but not Type 2 diabetes, were prescribed the diabetes drug metformin.
By the end of the study, half of those who took the medication had reversed their insulin resistance — and also found dramatic improvements in their psychiatric symptoms, even though most had been ill for 25 years without any remission.
“I was kind of blown away,” says Dr. Cynthia Calkin, a psychiatrist at Dalhousie University in Canada who led the study. “It’s not that metformin is an antidepressant, it’s that it can reverse insulin resistance, and that improves outcomes.”
“A tailwind” to wellness
Neither patients nor clinicians are waiting for the results of larger trials to try keto.
Online, patients share their experiences with — and challenges — trying the diet. And doctors like Sethi and Ede, who trains other clinicians, regularly treat patients with it.
Lori Katz, pictured here with her support dog, started the ketogenic diet under Dr. Sethi’s supervision. She quickly noticed a difference. “It wasn’t just the depressive symptoms, but it was the feeling of lack of control,” she says. The diet “was like a tailwind — just blowing me into a better future.”
About four years ago, Lori Katz ended up at Sethi’s Stanford clinic after trying many treatments for bipolar disorder — a diagnosis she received when she was 18 years old.
She also struggled with chronic pain, binge eating and emotional eating, and unwanted weight gain. Her episodes of depression had led her to consider electroconvulsive therapy (ECT).
The ketogenic diet was quite the adjustment, but Katz gave it a go, under Sethi’s supervision.
“Suddenly, I was losing weight really fast and was extremely satisfied with what I was eating,” says Katz, a dog trainer who lives in Santa Cruz, Calif.
She says those around her quickly noticed a change in her mood.
“It wasn’t just the depressive symptoms, but it was the feeling of lack of control,” she says. The keto diet, she says, “was like a tailwind — just blowing me into a better future.”
Eventually, she started going to the gym and taking longer walks. And after years without a romantic drive, a girlfriend entered her life.
Katz says she can’t always follow the diet perfectly and notices the change in mood when she is less strict. It hasn’t erased the reality of living with a mental illness.
“I will live with this but it’s a question of am I more resilient? Yes. Am I more optimistic? Yes. Am I feeling like I have this tool? Yes, when I get in there and I get the support. I need to stay in ketosis.”
Can it be done?
Indeed, any kind of diet can be hard to stick to, and one that involves largely giving up common comfort foods like bread and sweets may be even more challenging.
About a quarter of those in Campbell’s study withdrew, which he notes is similar to other pilot trials with the ketogenic diet.
Dr. Rif El-Mallakh, a psychiatrist at the University of Louisville, became interested in the diet more than two decades ago and believes it works.
He says he had early success with a few patients, but hasn’t had much luck over the years: “I haven’t been able to get people to stay on it, so I’m not at all as excited as maybe others.”
However, doctors who already use it in their practice say with enough education and support patients can be successful.
Dr. Matt Bernstein has found striking results in some of his patients.
Some opt for the most restrictive form of the diet, especially if they have severe symptoms, but he emphasizes it can be tailored and even a “modest version” has made an “incredible difference” for some patients.
He’ll ease them into it, lowering their carbohydrate intake gradually.
“Some people like to do it cold turkey, but for a lot of people, that’s not the best thing,” says Bernstein, chief medical officer at Ellenhorn, a psychiatric recovery program in Boston.
“The idea is that this is going to be sustainable and not just something you do for a few months and then stop.”
Not many psychiatrists are trained to offer the diet, although the numbers are growing.
Bernstein and other doctors say those with a history of serious mental illness should have medical supervision. There can be lab work and medications that need to be adjusted.
Despite the optimism, there are still many unanswered questions.
In his initial research, Iain Campbell’s already hearing some real results of his dream to help others find this treatment.
“They would describe it to me like, ‘This changed my life completely. I’m reconnecting with my family. I can work again for the first time,'” he says.
A study by the University of Louisville has revealed that nicotine salts in e-cigarettes, especially at higher doses, could increase the risk of heart arrhythmias more than previously believed. This challenges the notion that nicotine in e-cigarettes is harmless and highlights the need for careful consideration and potentially stricter regulations to protect public health.
E-cigarettes that use pods with higher nicotine concentrations are more likely to cause an irregular heartbeat.
As the new year begins, individuals who smoke or vape might have made resolutions to quit or reduce their consumption for better health. However, they should exercise caution if they plan to transition from traditional cigarettes to e-cigarettes, which some believe to be a safer option.
A new study from the University of Louisville shows the nicotine in certain types of e-cigarettes may be more harmful than others, increasing the risk for irregular heartbeat, or heart arrhythmias.
A popular claim is that nicotine in e-cigarettes is relatively harmless, whereas additives and combustion products largely account for the harms of traditional cigarettes. The UofL research, which tested the effects of e-cigarettes with various types and doses of nicotine in animal models, showed that the nicotine form contained in pod-based e-cigarettes, nicotine salts, led to heart arrhythmias, particularly at higher doses.
Comparative Analysis of Nicotine Types
In the study, published in Nicotine and Tobacco Research, researchers compared heart rate and heart rate variability in mice exposed to vape aerosols containing different types of nicotine. The aerosols contained either freebase nicotine, used in older types of e-cigarettes; nicotine salts, used in Juul and other pod-based e-cigarettes; or racemic freebase nicotine, simulating the recently popularized synthetic nicotine; and their effects were compared to nicotine-free e-cigarette aerosols or air. In addition, the research team delivered increasing concentrations of the nicotine over time, from 1% to 2.5% to 5%.
The nicotine salts induced cardiac arrhythmias more potently than freebase nicotine, and the cardiac arrhythmias increased with the higher concentrations of nicotine.
Implications for E-cigarette Regulation and Use
“This suggests the nicotine is harmful to the heart and counters popular claims that the nicotine itself is harmless,” said Alex Carll, assistant professor in UofL’s Department of Physiology, who led the study. “Our findings provide new evidence that nicotine type and concentration modify the adverse cardiovascular effects of e-cigarette aerosols, which may have important regulatory implications.”
The study also revealed that the higher levels of nicotine salts increased sympathetic nervous system activity, also known as the fight-or-flight response, by stimulating the same receptor that is inhibited by beta-blockers, heart medications that are prescribed to treat cardiac arrhythmias. In the autonomic nervous system, sympathetic dominance increases the fight-or-flight response in bodily functions, including heart rate.
“The nicotine in e-cigarettes causes irregular heartbeats (arrhythmias) in a dose-dependent manner by stimulating the very receptor that many heart medications are designed to inhibit,” Carll said.
The findings conclude that inhalation of e-cig aerosols from nicotine-salt-containing e-liquids could increase cardiovascular risks by inducing sympathetic dominance and cardiac arrhythmias.
The researchers concluded that, if these results are confirmed in humans, regulating nicotine salts through minimum pH standards or limits on acid additives in e-liquids may mitigate the public health risks of vaping.
Even without regulatory changes, however, the research suggests that users may reduce potential harm by opting for e-cigarettes with freebase nicotine instead of nicotine salts or using e-cigarettes with a lower nicotine content.
Close to 5 million deaths are associated with antimicrobial resistance (AMR) globally in 2019
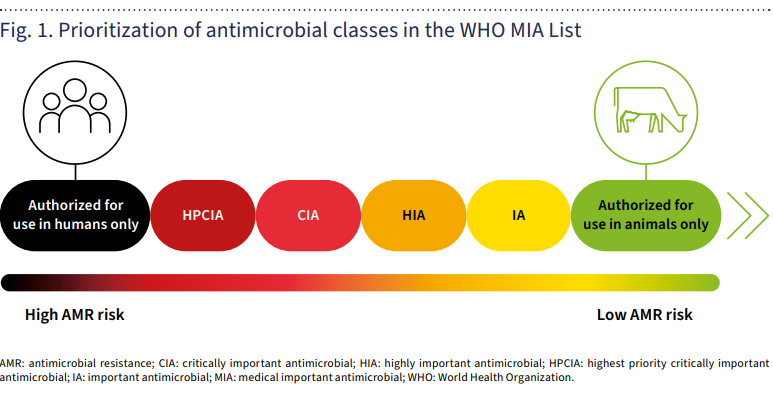
The WHO has released a first-ever list of 21 antimicrobials earmarked as “authorized for use in humans only” – a first for the organization in its efforts to protect overuse and abuse of critical first-line drugs that need to be protected by overuse in animal and plant health sectors – and consequent antimicrobial resistance (AMR).
Significantly, most of the 21 antimicrobials earmarked by WHO as “authorized for use in humans only” include mostly novel compounds developed and authorized over the past six years.
The category “mainly contains newer antimicrobials that are very important in treating serious multidrug-resistant infections in humans,” WHO explains in its guidance. So the new WHO label is effectively a warning sign to the farm industry that they should not be used in animals or plants in the future.
Among the antimicrobials authorized “for use in humans only” are: plazomicin, aminomethylcycline, anti-pseudomonal penicillins with and without β-lactamase inhibitors, carbapenems with or without inhibitors, third- and fourth-generation cephalosporins with β-lactamase inhibitors, sulfones, as well as drugs critical to treating tuberculosis and other mycobacterial diseases.
Some of the older ones on the WHO list, e.g. carbapenems, are not licensed for use in animals in the United States, but are sometimes used in companion animals.
The report aims to provide guidance for authorities in the public health and animal health sectors, veterinarians, prescribers of antimicrobials, and agricultural professionals, as well as classify antimicrobial categories by importance to human use, WHO said.
Reducing risks to human health
Antibiotics are commonly overused in animals—often without the input of veterinarians—to boost their growth and keep them from picking up infections.
A second category of medically important antimicrobials refers to drugs “authorized for use in both humans and animals.”
But this is further broken down into “highest priority critically important antimicrobials (HPCIA),” “critically important antimicrobials (CIA),” “highly important antimicrobials,” and “important antimicrobials.”
Widespread animal use of leading antibiotics has become a major driver of growing ‘superbug’ resistance to common drug treatments, or AMR. In 2019 AMR was associated with the deaths of close to 5 million people globally.
To address these risks, the use of critical antimicrobials needs to be rationalized more systematically in both animal as well as human health. WHO’s drug classifications create an order of priority for doing this, notes an analysis from the University of Minnesota-based Center for Infectious Disease Research and Policy (CIDRAP.)
“The risk to human health is greatest if the antimicrobials listed as ‘authorized for use in humans only’ are used in non-human sectors,” noted the CIDRAP analysis. “Those risks and impacts decline progressively with the use of agents from the other categories.”
“For instance, the criteria for inclusion in the first two medically important antimicrobial categories is whether the antimicrobial class is one of the limited available therapies or the sole available therapy to treat serious bacterial infections and if it’s used to treat bacterial infections possibly transmitted from non-human sources (such as Salmonella and Escherichia coli).
“Among the classes categorized as HPCIA are third- and fourth-generation cephalosporins, quinolones, and polymyxins. The CIA category includes aminoglycosides and macrolides,” CIDRAP noted.
Scale of prioritization of medically important antimicrobials (MIA)
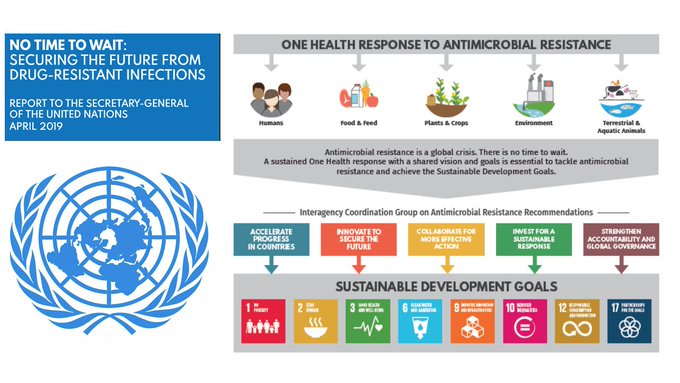
One Health and AMR
A One Health approach
The non-human use of antimicrobials in fact includes a broad range of species, beyond the historical focus on food-producing animals. These include aquaculture, companion animals, and fur-bearing animals. Reducing antimicrobial use in the non-human sector remains vital for preserving the efficacy of these substances, WHO said.
Antimicrobial resistance (AMR) occurs when pathogens like bacteria, viruses, fungi, and parasites no longer respond to antimicrobial medicines, making infections harder to treat while increasing the risk of disease spread, severe illness, and death. Infections typically treated with routine medicines thus become life threatening.
“Because AMR develops and transfers within and among all sectors, minimizing the risk of emergence and transmission of AMR calls for a One Health approach,” WHO explained in the new guidance.
“To improve the responsible and prudent use of antimicrobial agents—and in particular medically important antimicrobial agents—it is thus essential to decrease their inappropriate use across sectors.”
Additionally, the report advocates for the more systematic inclusion of medically important antimicrobials in AMR monitoring and surveillance programs – which continue to be patchy and incomplete in most countries of the world.
New WHO category ‘for use in animals only’
In addition to the existing “highly important antimicrobials” (HIA) and “important antimicrobials” (IA) classifications, the WHO now includes an “authorized for use in animals only.” This group was added to “ensure that all antimicrobials used in animals come under scrutiny as part of the standard evaluation approach, so that they would not be placed in a low priority category by default, without proper assessment of the potential risk of AMR in humans.”
Living organisms often create what is needed for life from scratch. For humans, this process means the creation of most essential compounds needed to survive. But not every living thing has this capability, such as the parasite that causes malaria, which affected an estimated 249 million people in 2022.
Virginia Tech researchers in the College of Agriculture and Life Sciences have found that by preventing the malaria parasite from scavenging fatty acids, a type of required nutrient, it could no longer grow. Their work is published in the journal Proceedings of the National Academy of Sciences.
“The key to this breakthrough is that we were able to develop a screening method for the malaria parasite and block this process,” said Michael Klemba, associate professor of biochemistry and principal investigator on the project. “While very much in its infancy, the results could open the door to a new way to fight malaria.”
Malaria is caused while the parasite is replicating in human red blood cells and it relies on scavenging, rather than creating, to satisfy its need for fatty acids. Many fatty acids are obtained by metabolizing a class of host lipids, called lysophospholipids. However, scientists didn’t know how the parasite releases fatty acids from the host lipids.
The Virginia Tech research team did experiments with infected red blood cells and found chemicals that can stop the parasite from getting the needed fatty acids. Researchers discovered that two enzymes were instrumental in breaking down host lipids to release the fatty acids the parasite needs. These enzymes work in different places: One works outside in the red blood cell, and the other works inside the parasite.
When scientists removed these two enzymes, they found that the parasite struggled to get the needed fatty acids and couldn’t grow well. This was especially true when that host lipid was the only fatty acid source available. When both enzymes were stopped from working, either by changing the parasite’s genes or by using drugs, the parasites couldn’t grow in human blood.
This shows that breaking down the host lipid, called lysophosphatidylcholine, to get fatty acids is critical for the malaria parasite’s survival in our bodies and that targeting these two enzymes could be a new way to fight malaria.
Laying the groundwork
In 2017, a study showed when lysophosphatidic acid levels drop in the host that the malaria parasite, known as Plasmodium falciparum, converts into a form that can be taken up by mosquitoes. P. falciparum causes malaria while replicating in host erythrocytes, or red blood cells, and relies on scavenging rather than synthesis, or the creation of compounds, to satisfy its need for fatty acids.
This seemed to be an important environmental cue, Klemba said, and there was also evidence that host lipids were a preferred source of fatty acids.
“There wasn’t clarity on what the metabolic pathways were,” he said. “If we could show that these metabolic pathways were useful, then that would be an important contribution to the field.”
For Klemba, this was an important question to answer and one that his lab—and students—were in a unique position to do. Two graduate students worked on the project—Jiapeng Liu, now a postdoctoral scholar at Rutgers University, and Christie Dapper, a former professor at Virginia Tech. Liu was the lead author and Katherine Fike assisted with the project as a research specialist.
“There are two enzymes that are really important for this process: One is inside the parasite, and the other is exported into the host cell,” Klemba said, “which is not typical of metabolic processes as they are typically carried out within the parasite. Why did the parasite find it useful to put one of these enzymes into the host? We have some ideas that that could be involved in host modification, which could be that the parasite remodels the red cell once it’s once it’s set up shop.”
The researchers found that only removing one of the two enzymes, which they named XL2 and XLH4, doesn’t do anything. Both have to be removed to inhibit parasitic growth.
Future work
There are some limitations of the discovery: The research was conducted only using a culture dish, commonly referred to as in vitro. The researchers also are not sure if the compounds used to inhibit the two enzymes are toxic.
Some level of toxicity is expected, Klemba explained, and it may be possible to engineer the toxicity out of the compounds.
“But that could be a major challenge,” he said.
In the meantime, this discovery could open the door to therapeutic treatments for malaria.
Scientists using the eROSITA X-ray telescope have released a trove of data that reveals more than 900,000 objects in space, including 700,000 supermassive black holes and other ‘exotic’ objects
The sky section of the eROSITA All-Sky Survey catalog in two different representations. The left image shows extended X-ray emission, while the right image shows point-like X-ray sources. (Image credit: MPE, J. Sanders für das eROSITA-Konsortium)
Astronomers have unveiled the largest and most detailed X-ray map of the universe ever created. The newly released data reveal the light of more than 700,000 monster black holes, a mysterious “bridge” of gas connecting distant galaxies, and hundreds of thousands of other “exotic” deep-space objects.
The massive new X-ray data release comes courtesy of the eROSITA All-Sky Survey, a mission to scan the entire sky from December 2019 to June 2020 using the eROSITA X-ray telescope. In that time, the survey detected more than 170 million X-ray photons (particles of light) in the sky, which astronomers later identified as roughly 900,000 distinct objects in space, most of which are supermassive black holes, according to a statement from the Max Planck Society in Germany, which helped manage the mission.
“These are mind-blowing numbers for X-ray astronomy,” Andrea Merloni, eROSITA principal investigator and lead author of a new paper describing the breadth of the mission’s findings, said in the statement. “We’ve detected more sources in 6 months than the big flagship missions XMM-Newton and Chandra have done in nearly 25 years of operation,” Merloni added, referring to the X-ray telescopes currently operated by the European Space Agency and NASA, respectively.
X-rays are a form of high-energy radiation that’s invisible to the naked eye. Most X-ray emissions in space come from concentrations of extremely hot gases, which can arise from massive galaxy clusters; the remnants of supernova explosions, like the famous Crab Nebula; or active black holes that can outshine entire galaxies as hot, fast-moving matter plummets into their insatiable maws. Studying cosmic X-rays can not only suss out massive, high-energy objects like these but also reveal the overarching structure of the universe itself.
An eROSITA X-ray image with the newly discovered filament between two galaxy clusters more than 42 million light-years apart. (Image credit: Dietl et al. (2024))
One of the most intriguing new discoveries to come from the survey is an enormous “filament,” or bridge, of hot gas connecting two clusters of galaxies across more than 42 million light-years (more than 400 times the length of the Milky Way). The filament is thought to be a piece of the cosmic web — the vast superhighway of gas that feeds all galaxies in the universe and reveals the empty voids where elusive dark matter is thought to dwell. (The research has yet to be peer-reviewed.)
In addition to releasing the latest batch of data, researchers from the project have submitted more than 50 papers to scientific journals discussing a small fraction of eROSITA’s new findings. This fresh ream of astronomical reading material adds to more than 200 papers already published on prior eROSITA discoveries, the researchers said.
The full data release, along with free tools for reading it, are available courtesy of the eROSITA website. More data and scientific papers based on it are expected in the near future. In the meantime, eROSITA will continue stargazing from its home aboard the Spectrum-Roentgen-Gamma (SRG) space observatory, operated jointly by Germany and Russia.
A recent study suggests that the Tyrannosaurus rex may have ruled the Late Cretaceous Period with brawn and brains. Paleoneurologists share what a T. rex skull can tell us about its brain and intelligence.
The name Tyrannosaurus rex means the “king of the tyrant lizards,” and by all accounts, that’s exactly what T. rex was. A ruthless and fearsome predator, it ruled the world in the Late Cretaceous Period, around 90 million years ago. With teeth as big as a banana, a crushing bite and a sense of smell as keen as a cat, this infamous theropod was a vicious predator. But how smart was T. rex? What do we know, and what can we know about the brains of the most ferocious predator that the world has ever seen?
Clues From the T. Rex Skull
According to Ashley Morhardt, a paleoneurologist at the Washington University School of Medicine, some things are evident from fossils that might give us some clues into a dinosaur’s intelligence. For example, we can observe and measure the cavity space where the brain was once housed.
T. Rex Brain
If the skull has been broken open due to damage, researchers can physically study the insides of the brain. The skull can also be placed in a computerized axial tomography (CAT) scan, which provides a detailed image of the inside of the brain cavity. In some cases, scientists might also make an endocast or a 3D representation of the brain cavity made in a similar method to a jello mold. Endocasts are particularly helpful because they show the size of the brain cavity as well as the anatomical details of the brain.
“We can get a sense of how much of the brain tissue was devoted to different regions of the brain by being able to analyze the anatomy of the endocast,” says Morhardt.
Regarding T. rex, we know that it had extra large olfactory bulbs and, as a result, a great sense of smell. We also know from the size of the eye sockets that it had excellent vision.
Size of a T. Rex Brain
A July 2022 study published in theJournal of Comparative Neurology took it a step further, using the information we have about the neuronal density and brain size of animals living today and attempting to apply that knowledge to T. rex.
As Smart as a Baboon?
The study, authored by Suzana Herculano-Houzel, even estimates that T. rex was about as smart as a baboon, which means they were smarter than we thought. But Morhardt contends that there are too many caveats in the study to be able to take it that far. “I don’t personally find this claim to be realistic because brain size only tells us a small portion of the story,” she says.
T. Rex Brain Size and Neurons
Brain size is important, as is neuronal density. Still, we also need to be able to map the neuronal connectivity of the brain to assess its efficiencies and to look at how support cells in the brain are impacting brain activity. So there’s a lot we don’t know, and it’s best not to jump to conclusions. “We have to be careful to stay within the limits of the data,” says Morhardt.
Evaluating T. Rex Intelligence
Matthew Carrano, curator of the Smithsonian’s National Museum for Natural History, agrees that there’s a lot that we just don’t know. He says we haven’t even mastered measuring intelligence in live human beings. “To go back in time and measure intelligence in an ancient animal, it’s really hard to even approach this question in any sort of precise way,” he says.
Tree of Life
He contends that we have secondary ideas that may provide a window into T. rex intelligence, but it would be challenging to go beyond that for now. We can get an idea of dinosaur intelligence based on where they fit into the tree of life, says Carrano.
“We know that we have living dinosaurs in birds and close cousins of dinosaurs in crocodilians, so we can use what we know about these living animals to bracket the possibilities for dinosaur intelligence,” he says.
Bird Brained?
Still, there’s a range of intelligence in birds. Some are quite smart, like parrots and crows, but others are not as sophisticated. Moreover, birds have changed a lot in the past 66 million years. And then there are crocodiles, which in some research, are highly intelligent, working in teams to hunt their prey and displaying advanced parental care. And they haven’t changed much, but we’re still not sure how close they were to dinosaurs regarding intelligence.
In the end, there’s a lot we don’t know about dinosaurs or T. rex intelligence, and it seems difficult that without the brain, we could know. But the more specimens we find to indicate behavior, culture and sophistication, the more we can pull back the curtain on the brains of this fantastic beast. Until then, we’ll have to hang our hats on the idea that T. rex was as smart as it needed to be to rule its prehistoric world.
An analysis of more than 2,000 languages reveals differences in the way feelings are conceptualized among cultures
Humans boast a rich trove of words to express the way we feel. Some are not easily translatable between languages: Germans use “Weltschmerz” to refer to a feeling of melancholy caused by the state of the world. And the indigenous Baining people of Papua New Guinea say “awumbuk” to describe a social hangover that leaves people unmotivated and listless for days after the departure of overnight guests. Other terms seem rather common—“fear,” for example, translates to “takot” in Tagalog and “ótti” in Icelandic. These similarities and differences raise a question: Does the way we experience emotions cross cultural boundaries?
Scientists have long questioned whether human emotions share universal roots or vary across cultures. Early evidence suggested that, in the same way that primary colors give rise to all of the other hues, there was a core set of primary emotions from which all other feelings arose. In the 1970s, for instance, researchers reported that people in an isolated cultural group in Papua New Guinea were able to correctly identify emotional expressions in photographed Western faces at rates higher than chance. “This was largely taken as evidence that people around the world could understand emotions in the same way,” says Kristen Lindquist, an associate professor of psychology and neuroscience at the University of North Carolina at Chapel Hill.
But more recent studies have challenged this idea. Work from a variety of fields—psychology, neuroscience and anthropology—has provided evidence that the way people express and experience emotions may be greatly influenced by our cultural upbringing. Many of these studies have limitations, however. Most have either looked only at comparisons between two cultures or focused on big, industrialized countries, says Joshua Jackson, a doctoral student in psychology at Chapel Hill. “We haven’t really had the power to test [the universality of emotion] on an appropriate scale.”
To explore the question of common emotions, Jackson, Lindquist and their colleagues teamed up with researchers at the Max Planck Institute for the Science of Human History in Jena, Germany, in one of the largest studies of cross-cultural emotional expression to date. Their work, which was published today in Science, drew on vocabulary from 2,474 languages. It revealed a great deal of variability in the way emotions are verbally expressed—as well as some underlying commonalities. “Psychologists have been debating whether emotions are universal or variable across cultures for a long time,” Jackson says. “I think what this paper shows is that both sides have some merit.”
To examine variability in emotional expression, the researchers used computational toolsto create a massive database of colexifications, instances where a single word has multiple meanings. Examples include “ruka,” which means both hand and arm in Russian, and “funny,” which means both odd and humorous in English. Previous investigations of nonemotional words have demonstrated that colexified ones tend to have common properties—words that describe “sea” and “water” are more likely to be paired than those for “sun” and “water”—suggesting that speakers of a language perceive similarities in them.
The team then used its database to generate networks of colexified words among 20 language families (groups of languages that share ancestral roots) to compare emotion-associated vocabulary worldwide. Doing so revealed significant differences in how emotions were conceptualized across cultures—three times more variation than in terms used to describe color. For example, in some languages, the words for “surprise” tended be grouped with those for fear, while in others, the same concept was paired with more pleasant states, such as happiness. Through further analysis, the researchers also found that this diversity was partially dependent on the geographical proximity of language families—the closer they were, the more commonalities they were likely to share. “That suggests the extent to which cultures were likely to have historical contact, either via trade or migration or conquest allowed these cultures to interact and perhaps transmit and borrow emotion concepts from one another,” Lindquist says.
On the other hand, the researchers also found some underlying similarities. Language families tended to differentiate emotions based on their valence (how pleasant or unpleasant they were) and activation (the level of excitement they elicited). For instance, words that expressed joy were unlikely to be grouped together with those for regret. There were exceptions, however: some Austronesian languages paired the concept of love, a typically positive emotion, with pity, a typically negative one.
“This is an important study,” says William Croft, a professor of linguistics at the University of New Mexico, who wasn’t involved in the work. “It’s probably the first time an analysis of the meanings of words has been done at this scale.” One of the novel things about this project is that the findings show both universal and culture-specific patterns, Crofts adds. He points out, however, that because some of these families cover a large number of languages across a wide geographical area, it will be important to further examine the underlying cultural factors.
Another limitation of the study lies in the imperfect nature of translations, says Asifa Majid, a professor of psychology at the University of York in England, who penned an accompanying commentary. This is especially the case when it comes to words for emotion, which can be difficult to express in words—linguists may only obtain approximate translations of such terms while documenting word lists out in the field. Nevertheless, these findings raise a fascinating question about cross-cultural variation in human emotion, Majid adds. “Where we find variation, is it only in language or is it reflecting something deeper about how people experience emotions, too?”
If you or someone you love has ever been diagnosed with a blood cancer such as leukemia or lymphoma, you’re probably already familiar with the concept of remission.
But what about composite remission? Is that the same thing?
We checked in with leukemia specialist Courtney DiNardo, M.D., for insight into this term, which is generally used only with blood cancers.
What is composite remission?
It’s a measurement used to include all patients receiving a particular treatment who achieved either a standard complete remission (CR) or a lesser form of complete remission, such as CRi (which encompasses both CRn and CRp).
These terms each mean something slightly different, but in general, they indicate that someone has achieved all the components of a complete remission, meaning the leukemia is no longer detectable, but their blood counts haven’t fully recovered.
What do CRi, CRn and CRpmean when it comes to remission?
CRi is the least specific. It stands for “complete remission with incomplete count recovery.” It can be further subdivided into either CRn or CRp. CRn means your neutrophil count is low, while CRp means your platelet count is low.
How does composite remission differ from complete remission?
With complete remission, the disease is gone and your blood counts have fully recovered.
With composite remission, the disease is gone, but your blood counts might not have fully recovered.
Sometimes different cancer treatments can impact the speed or degree of blood count recovery. In patients receiving the newer, small-molecule chemotherapy drug venetoclax, for instance, neutrophil counts tend to remain on the lower side. So, they don’t always qualify to use the term “complete remission,” even though the therapy has successfully treated the leukemia.
Composite remission is a way of making sure we still account for patients who are responding well to therapy, even if they don’t fit the typical criteria.
Does composite remission mean the same thing as partial remission?
No. Partial remission indicates that someone still has disease present, but their blood counts have fully recovered. It’s not the same thing as composite remission, because the disease hasn’t been eradicated. A partial remission is very rare.
Is there anything else people should know about composite remission?
There’s another relatively related new term that the Food and Drug Administration (FDA) has adopted in the approval of new treatments for leukemia: CRh. It stands for “complete remission with partial hematologic recovery.”
A CRh is defined as all the elements of a CR, except a neutrophil count above 500 (but not above 1,000, which is required for a full CR) and a platelet count above 50,000 (but not above 100,000, which is required for a full CR).
So, while their blood counts aren’t perfect, they don’t need frequent transfusions and aren’t as tied to a hospital setting. That’s why some patients joke that the “h” in CRh stands for “Hawaii,” because it means you’re doing well enough to go on vacation without the frequent need for blood product transfusions.














{kind=link}