A French company is seeking to solve one of the biggest challenges in the emerging cell therapy industry by commercializing an automated system for manufacturing CAR-T at scale.
“Producing CAR-T cells at scale is one of the challenges to manufacturing these life-changing therapies,” says Dominique Yon, head of business development at CellQuest, in an exclusive interview with GEN.
“The industry is still in its infancy, but we’re expecting demand to increase in the years to come.”
CellQuest claims they’ve developed an automated system that can manufacture 6,000 CAR-T doses a year in less than 300 square feet of space. The company says this is 30 times the throughput of typical production today, and at a much lower cost.
According to Yon and CellQuest CEO, Guillaume Wallart, CellQuest’s technology consists of a unit about the size of a fridge, which can take up to 15 trays that work like mini production units.
Each tray contains a single patient dose and has a pouch with compartments where all critical CAR-T production steps, including cell sorting, selection, transduction, and expansion can take place.
The entire process is automated and delivered via a metal structure with clamps that can, for example, open and close compartments within the pouch or agitate the cells during culture.
The pouch is connected, sterilely, to four cartridges containing pre-filled and pre-dosed ingredients for the manufacturing process, such as microbeads for cell selection.
The sterile connection takes place automatically within a minute, they explain, at high temperatures inside another small machine. The pouch and cartridges, they added, are RFID labeled for traceability between the first and second units.
According to Yon, the company has gone for well-established technologies in developing their micro-factory, which, they claim, makes them unique in this emerging area.
“We went for technologies that are simple, compact, tried-and-tested, and nothing that hasn’t been used in the past,” he tells GEN.
“We’re the only company [among our competitors in this emerging area] that has a cartridge to minimize risk and optimize the process—so, in that sense, we’re scalable, safe, and robust.”
The pouch, he adds, is made of a standard medical material. It’s also transparent, allowing two traditional microscopes to monitor the process and do a cell count.
“It can tell you the speed of expansion,” he says. “And, by the second day, we already know when we’ll reach the [desired] dose.”
The company is also working on a fill-and-finish machine and hopes to have a prototype ready by the end of the year.
And the one thing you can do to turn diabetes around
You’ve probably heard of diabetes. And obesity. But what the heck is diabesity? It’s a new medical term for a condition that’s becoming a worldwide epidemic. And if you have it, losing weight could cure the condition. Endocrinologist Jay Waddadar, MD, explains.
What is diabesity?
Diabesity isn’t an official diagnosis. It means you have both obesity and Type 2 diabetes. Together, these closely related conditions greatly increase your risk of heart disease — the leading cause of death in the country.
“Diabesity is a disease with enormous potential to cause ill effects on the body in the long run,” says Dr. Waddadar. “Some people don’t understand the importance of taking the steps to manage it because they’re feeling well at the time of diagnosis. But that’s a big mistake. Diabesity is a silent disease that damages your body if it’s not controlled, even while you feel fine.”
The good news: You can prevent, control and even reverse it. Dr. Waddadar shares more about how obesity causes and worsens diabetes. And why losing weight holds the key to possibly making it all go away.
How diabetes is related to obesity
Having obesity makes you more likely to develop diabetes, the condition of having too much glucose (sugar) circulating in your bloodstream. Obesity also causes diabetes to worsen faster.
Here’s what happens: Managing the level of glucose in your blood is the job of the pancreas. The pancreas creates insulin, which is a hormone that moves glucose out of your blood. Normally, insulin transports glucose to your muscles to use right away for energy or to the liver, where it’s stored for later.
But when you have diabesity, your cells resist letting insulin move glucose into them. To make matters worse, the area of your liver where excess glucose is usually stored is filled with fat. It’s like trying to put furniture in a room that’s already packed. “There’s no space for anything else,” Dr. Waddadar explains.
With nowhere to be stored, the glucose remains in the bloodstream. “So your pancreas creates even more insulin trying to accomplish the job of moving glucose out of the blood,” says Dr. Waddadar. “It’s trying to push against the resistance created by the fat. Your pancreas becomes overworked, and as a result, it wears out. It starts producing less insulin. Diabetes develops and then quickly worsens if the fat resistance remains.”
Does everyone with obesity develop diabesity?
If you have obesity, you’re about six times more likely to develop Type 2 diabetes than those at a healthy weight. But not everyone with obesity automatically gets diabetes. Other factors are likely at play, too, including:
It may be that some people with obesity can produce more insulin without overtaxing the pancreas, says Dr. Waddadar. Others might be limited in insulin production, making it more likely that obesity will lead to diabesity.
Effects of weight loss on diabesity
Since excess fat worsens diabetes, losing weight can greatly improve the condition. “When you have diabesity, you may start with one medication to get the pancreas to produce enough insulin. But very soon and much earlier, you need two or more medicines for diabetes. But if you lose weight, you may do fine with just one medication or even go off medication entirely,” explains Dr. Waddadar.
Losing as little as 5% to 10% of your overall body weight can greatly improve Type 2 diabetes. For example, if you weigh 200 pounds, 5% of that is 10 pounds. So bringing your weight down to 190 pounds can significantly help your health. “The first treatment goal for diabesity is to get to and maintain a healthy weight along with eating a low-carb diet,” Dr. Waddadar says.
Changing your diet and increasing exercise to lose weight can be challenging. But the hard work is worth it to avoid serious complications of uncontrolled diabetes like heart disease, kidney failure and nerve damage.
Ready to take the first step toward better health? Ask your doctor for resources and guidance to help you beat diabetes.
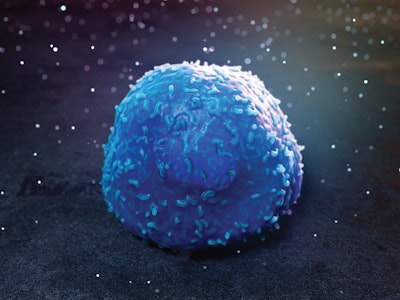
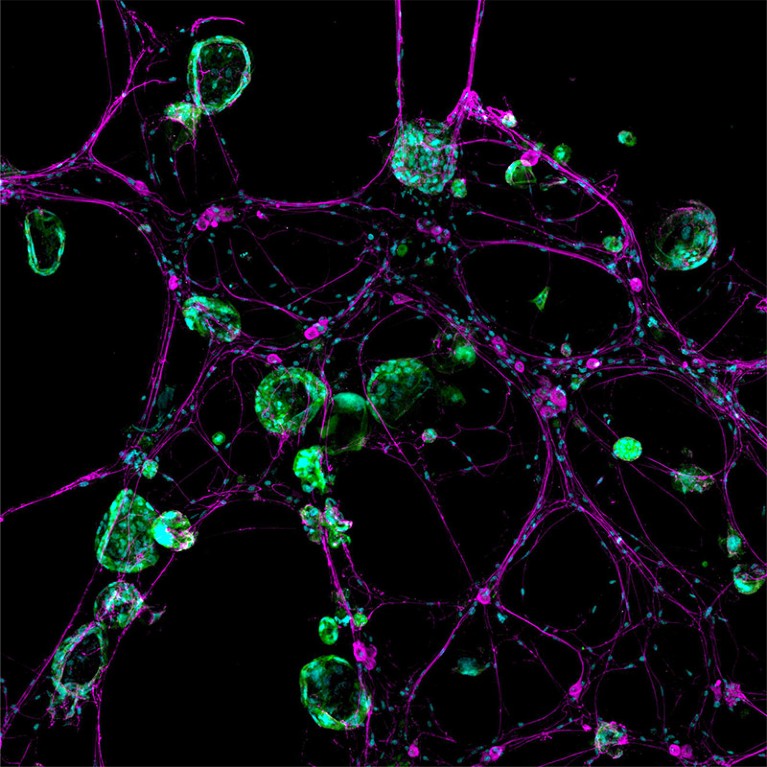
A new wave of research is unpicking the relationship between cancer and neurons — and looking for ways to stop the crosstalk.
A 3D model system shows how nerve cells (magenta) interact with cancer cells (green).
Lightning bolts of lime green flashed chaotically across the computer screen, a sight that stunned cancer neuroscientist Humsa Venkatesh. It was late 2017, and she was watching a storm of electrical activity in cells from a human brain tumour called a glioma.
Venkatesh was expecting a little background chatter between the cancerous brain cells, just as there is between healthy ones. But the conversations were continuous, and rapid-fire. “I could see these tumour cells just lighting up,” says Venkatesh, who was then a postdoctoral researcher at Stanford University School of Medicine in Stanford, California. “They were so clearly electrically active.”
She immediately began to think about the implications. Scientists just hadn’t considered that cancer cells — even those in the brain — could communicate with each other to this extent. Perhaps the tumour’s constant electrical communication was helping it to survive, or even to grow. “This is cancer that we’re working on — not neurons, not any other cell type.” To see the cells fizz with so much activity was “truly mind blowing,” says Venkatesh, who is now at Harvard Medical School in Boston, Massachusetts.
The findings have been pivotal in the emerging field of cancer neuroscience, in which researchers are parsing the many ways in which cancer — even outside the brain — co-opts the nervous system for its own benefit. In much the same way as tumours recruit blood vessels to feed themselves and grow, cancer relies on the nervous system for everything from initiation to spread.
The interaction between oncology and neuroscience is just beginning to unravel in this once-overlooked part of the tumour’s environment. Scientists are starting to understand which neurons and signals are involved, but new-found interactions with the immune system are making the story even more complicated. As researchers dig deeper into the relationship between cancer and the nervous system, therapies that target the connections are emerging. Some of these treatments use existing drugs to improve outcomes in people with cancer.
“Where we’re headed with this is helping patients,” says cancer biologist Erica Sloan at Monash University in Melbourne, Australia. “Yes, there’s the intellectual delight of understanding what goes on at the biology level. But the key goal is, ‘How do we translate this?’”
Invasion and persuasion
Scientists first spotted liaisons between cancer cells and neurons almost 200 years ago. In the mid-nineteenth century, French anatomist and pathologist Jean Cruveilhier described a case in which breast cancer had invaded the cranial nerve responsible for facial movement and sensations.
This was the first account of perineural invasion, in which cancer cells weave in and around nerves — and then spread. The phenomenon is a sign of an aggressive tumour and foreshadows poor health outcomes.
For a long time, scientists and health professionals thought that nerves served passively as a highway to transport cancer and its associated pain. Many viewed the nervous system as “the victim — the structure that gets destroyed by or damaged by the cancer”, says neuro-oncologist Michelle Monje at Stanford University School of Medicine, who was Venkatesh’s adviser.
But in the late 1990s, urological pathologist Gustavo Ayala, now at the University of Texas Health Science Center at Houston, started investigating the interaction a little more closely. He placed mouse nerves in dishes speckled with human prostate cancer cells. Within 24 hours, the nerves began growing little branches called neurites, which reached out towards the diseased cells. Once they made contact, the cancer travelled along the nerves until it reached the neuronal cell bodies3.
Nerves weren’t just bystanders: they actively sought a connection with cancer. “I thought it was real, and I decided to make it my career,” says Ayala. He soon became known as ‘the nerve guy’. “People didn’t quite make fun, but they didn’t share my interest in the field,” he says.The neuroscience of cancer
In 2008, Ayala reported another strange phenomenon. Prostate-cancer tumours taken from people who underwent surgery contained more nerve fibres, known as axons, than did samples from healthy prostates4.
Not everyone found this result odd, however. Some scientists were starting to view tumours as being organs themselves, because they contain multiple cell types, a scaffolding structure, blood vessels and other elements that distinguish them from being clumps of cancer cells.
But “there was a piece missing in the landscape — it was nerves”, says Claire Magnon, a cancer biologist at the French National Institute of Health and Medical Research in Paris.
That hunch led to a groundbreaking paper in 2013. She and her colleagues documented nerve fibres sprouting in and around prostate tumours in mice5. Moreover, severing the connections to the nervous system brought the disease to a standstill. In a few years, an avalanche of research demonstrated the same thing happening in cancers elsewhere, including in the stomach, pancreas and skin. Some of the severed nerves carry cancer-associated pain, and researchers already knew that blocking those paths in people with pancreatic cancer could bring some relief.
“The stars were sort of aligned,” says neuroscientist Brian Davis at the University of Pittsburgh in Pennsylvania. The converging results showed “that this component of the tumour microenvironment, that had basically been ignored, was playing some role”.
Hitting a nerve
But where these cancer-infiltrating nerves came from baffled researchers. Work conducted in the following years suggested that cells in the tumour can turn into neurons, or at least acquire neuron-like features. And in 2019, Magnon and her colleagues reported another origin6. They saw cells called neural progenitors travelling through the blood to prostate tumours in mice, where they settled and fledged into neurons. Somehow, cancers were influencing the brain region that contains these cells — an area called the subventricular zone. In mice, these cells are known to help heal certain brain conditions, such as strokes. Some evidence suggests that the same region produces neurons in adult humans, although the idea is controversial.
The following year, another team discovered that cancer can force neurons to change their identities. In a study of oral cancer in mice, researchers found that a group of nerves that relay sensations to the brain, called sensory neurons, acquired features of a different type of neuron that is usually rare in the oral cavity: sympathetic neurons, which are responsible for the ‘fight or flight’ response7.
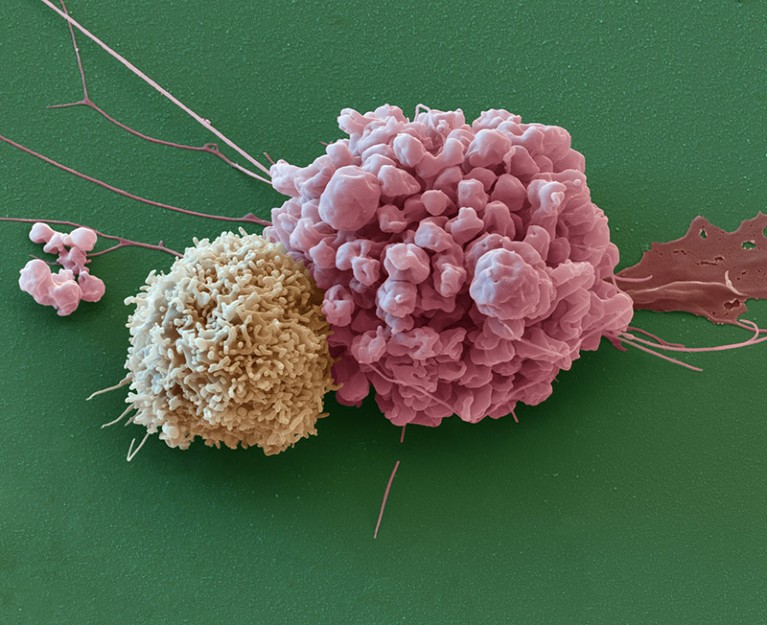
An immune cell (left) next to a cell from a nervous-system cancer called an ependymoma.
“Now they’re wearing two hats,” says cancer neuroscientist Moran Amit at the University of Texas MD Anderson Cancer Center in Houston, who co-led the study. The transformation might help tumour growth, because sympathetic nerves have been shown to benefit certain cancers.
But the relationships between nerve types and their effects on tumours are complicated. In the pancreas, for instance, a push and pull exists between two types of nerve that have opposite effects on tumours. Sympathetic nerves participate in a vicious feedforward loop that aids the growth of cancer. They release signals that instruct diseased cells to secrete a protein called nerve growth factor, which draws in more nerve fibres. Their counterparts — parasympathetic nerves, which are responsible for the ‘rest and digest’ response — send chemical messages that thwart disease progression.
But in stomach cancer, parasympathetic signals act in the opposite way, encouraging the tumour to grow. And in prostate cancer, both types of nerve aid tumours, with sympathetic nerves helping during the early stages of cancer development and parasympathetic nerves boosting later-stage spread.
“Every cancer is a little bit different in how it interacts with the nervous system,” says gastroenterologist Timothy Wang at Columbia University in New York City. This means that treatment targets must be specific to the type of cancer and how the cancer connects with or uses the nervous system.
Neurons can have direct effects on cancers, or they can act indirectly, by damping down the immune system so that it can’t fight tumours as effectively. A 2022 discovery hints at one such mechanism: a chemical called calcitonin gene-related peptide (CGRP), which is released by sensory nerves, can quell the activity of certain immune cells, making them ill-prepared to ward off cancer8.
Neurons can suppress immune-cell activity to keep themselves safe, because too much inflammation can harm them. So, not only do nerves provide a route and scaffolding for cancer’s spread, says cancer neuroscientist Jami Saloman at the University of Pittsburgh, but they also seem to provide a safe harbour.
A tumour can “tuck itself into the nerves”, Davis says, where it is protected from both the immune system and medication because drugs have a hard time entering nerves. “The cancer cells can hang out while they’re waiting for the storm of biologics and chemotherapy to pass,” he notes. “And then they can re-emerge.”
Central takeover
Some of the most aggressive cancers affect the brain. As Venkatesh and others found, cancer cells even form direct synapses with neurons, the signals of which help them to grow.
A paper published alongside the two 2019 brain-cancer papers showed that breast-cancer metastases in the brain could also form synapse-like connections9. And previous research has linked brain metastases with cognitive impairment.
There are yet more ways in which brain cancers seem to act like brain cells. Last November, Monje’s laboratory reported that gliomas strengthen their neuronal input using a classic brain-signalling method10. When exposed to a protein that helps neurons to grow, called brain-derived neurotrophic factor, glioma cells respond by spawning more receptors that can receive signals from neurons.
“It’s exactly the same mechanism that healthy neurons use in learning and memory,” Monje says. “Cancer doesn’t really invent anything new — it just hijacks processes that already exist.”How thought itself can drive tumour growth
Furthermore, just like in networks of neurons, some glioma cells can generate their own rhythmic waves of electrical activity11. “They are simply like little beating hearts,” says Frank Winkler, a neuro-oncologist at the German Cancer Research Center in Heidelberg, whose lab conducted the work.
Those electrical surges radiate throughout the cancer cells using a network of thin, stringy bridges called tumour microtubes, which Winkler’s group started studying several years ago. The activity choreographs cancer-cell proliferation and survival — just as pacemaker neurons orchestrate activity during the formation of neural circuits. “Yet again, cancer is hijacking an important neural mechanism of neurodevelopment,” Winkler says.
Brain cancers can even have effects on whole networks. A study last May found that gliomas can reshape entire functional circuits in the brain12. People with tumours that infiltrated speech-production areas were asked to name items described in audio or shown in pictures. Electrodes on the surface of their brains showed that the language task didn’t just stimulate those key language regions — the entire tumour-infiltrated area, including regions not usually involved in speech production, spiked in activity as well. The more functionally connected the tumour was to the rest of the brain, the worse people did on the task, and the less time they were expected to live.
“The tumour had remodelled the functional language circuitry to feed itself,” says Monje, who co-authored the work. She remembers her horror when she looked at the results. “I get goosebumps when I think about the first time I saw that data.”
Bench to bedside and beyond
These initial discoveries are already pointing to potential cancer treatments. They also hint at why existing options often bring brain-draining side effects. Many people undergoing chemotherapy experience cognitive decline, or ‘chemo brain’, and degeneration of nerve fibres elsewhere in the body, says Venkatesh.
Despite being an effective way to attack cancer, if chemotherapy destroys neurons elsewhere in the body, “that’s quite obviously not good for the patient”, she adds.
One tactic is to target specific prongs of the nervous system. And existing therapies might be able to help. “We have the drugs to target almost every branch of the nervous system,” Amit says. “Most of those drugs have a very established safety profile.”
Beta blockers, for instance, can disrupt signals from sympathetic nerves that drive cancer progression in the breast, pancreas, prostate and elsewhere. These drugs have been used to treat heart problems such as high blood pressure, and sometimes also anxiety, since the 1960s.
Sloan has wanted to repurpose the drugs for the past decade, but at first she faced resistance. People often remarked, “If beta blockers were going to do anything to cancer, we would know that already,” she recalls.
To explore the connection, she led a phase II clinical trial, published in 2020, testing the beta blocker propranolol in people with breast cancer. Taking the medication for just one week reduced signs of the cancer’s potential to metastasize13. Another phase II trial, inspired by observational studies that have linked beta-blocker use to better health outcomes, demonstrated that it was safe to combine chemotherapy and propranolol in people being treated for breast cancer14. And last year, Sloan found that the drug enhances a common chemotherapy treatment15.
Other researchers are repurposing drugs that interrupt neuronal communication, including medications developed for seizures and migraine. At least one clinical trial is aiming to block the synapses formed between neurons and cancer cells in gliomas using an anti-seizure drug, which calms hyperexcitable cells.
Another trial in the planning stages will look at whether people receiving immunotherapy for skin or head-and-neck cancer would also benefit from taking a migraine medication. It’s thought that migraines can be triggered by high levels of CGRP, the molecule that can blunt the activity of some immune cells in cancer. So the medication, which blocks CGRP receptors, could counteract CGRP and allow immune cells to help fight cancer again.
Venkatesh imagines that a cocktail of drugs with complementary effects will probably be needed to control the disease. “There is really no silver bullet,” she says.
The field is only just beginning to unravel this insidious relationship, and questions abound. “I think I would need 50 lives to go after all of them,” Winkler says.
A desktop-sized cardiac modeling system made of pliable, 3D-printed materials can be customized to accurately mimic the hydrodynamic characteristics of individual patients’ aortic stenosis (AS), ventricular remodeling and diastolic dysfunction. So reports a study published in Science Robotics by the Cleveland Clinic- and MIT-led team that developed the modeling system.
The soft robotic model consists of a flexible shell in the exact shape of a patient’s left ventricle (LV) and aorta and surrounded by “tunable” pneumatic sleeves that mimic the patient’s aortic valve lesions and loss of ventricular compliance as fluid circulates in the system.
When a transcatheter aortic valve replacement (TAVR) prosthesis is implanted in an individualized model, the resulting hydrodynamic changes match the postoperative hemodynamics of the relevant patient fitted with a comparably sized TAVR valve.
The model’s ability to replicate patient-specific disease morphology and treatment outcomes builds on previous research by the Cleveland Clinic/MIT team published in Nature Biomedical Engineering. The findings lay the groundwork for eventual deployment of the technology to inform clinical decision-making for individual patients with AS and other cardiac conditions, as well as to predict treatment outcome and support the design, testing and selection of personalized medical devices.
“Development of a patient-specific, clinically relevant model of aortic stenosis is vitally important,” says the study’s co-senior author, Christopher Nguyen, PhD, Director of the Cardiovascular Innovation Research Center and Director of MRI Research in Cleveland Clinic’s Heart, Vascular & Thoracic Institute. “With further validation and testing, we hope to translate this research into an effective tool for clinical guidance, education and device evaluation.”
Drawbacks of current modeling
Despite significant advances in TAVR technology and technique, there remains a need for high-fidelity modeling approaches to predict prosthetic valves’ fit, functionality and hemodynamic performance, particularly for high-risk patients with complex anatomic or physiological conditions. Selection of an improperly sized valve can cause paravalvular leakage and other complications.
Current modeling platforms typically use synthetic valve leaflet materials and fixed-volume pulsatile pumping systems that may not reliably and accurately replicate disease-state, patient-specific hemodynamics and demonstrate treatment-associated changes. In addition, existing methods cannot simulate the diastolic dysfunction resulting from AS-related LV remodeling.
Creating a soft robotic model
Dr. Nguyen and colleagues have worked to develop a more realistic, clinically relevant and customizable AS and ventricular remodeling simulator. They devised a soft, biomimetic robotic sleeve that encases and compresses the ascending aorta to mimic AS lesions arising from degenerative or congenital disease such as fused valve leaflets. Three inward-facing, inflatable pockets on the sleeve replicate the aortic valve’s trifold configuration (or that of a uni- or bicommissural valve if only one or two pockets are inflated). Thus, the sleeve can be tuned in real time to replicate patients’ aortic anatomies, unlike other models that must be iteratively tuned and reprinted or remanufactured.
Initial validation of a non-patient-specific aortic sleeve’s ability to recreate clinically relevant AS hemodynamics was conducted in a porcine model. The team subsequently developed a similar soft robotic LV sleeve that mimics loss of ventricular compliance and AS-associated diastolic dysfunction by the degree to which it is inflated, replicating impaired filling, emptying and wall motion during diastole and systole.
The researchers also used segmented CT imaging of selected AS patients’ left ventricles and aortas to create 3D digital anatomic models. The models were then 3D-printed using an elastomeric photopolymer resin to form soft, pliable, anatomically accurate cardiovascular shells.
By pairing an individualized ventricle/aorta shell with patient-specific, pneumatically tuned aortic and LV sleeves and circulating fluid through the system, the researchers could recreate the patient’s altered LV filling pressures, diastolic dysfunction and uniquely turbulent hemodynamics (Figure 1).
Figure 1. Representative 3D-printed left ventricle, aorta and aortic valve of a patient with aortic stenosis. The ventricle is driven by soft robotics mimicking the torsional motion of the heart and pumping blood out of the aorta, with the rest of the benchtop model connected to a mock flow loop matching a human body’s impedance.
“Current 3D printing methods create hard plastic cardiac models,” Dr. Nguyen says. “Our big leap was to make something that, although still synthetic, is close to the compliancy and response of the human cardiovascular system. The soft model allows you to determine whether the TAVR valve has the response desired when it deploys.”
Validating the model
To test the fidelity of their approach, Dr. Nguyen and colleagues created cardiac models representing 15 retrospectively chosen AS patients who had undergone transthoracic and/or transesophageal echocardiography as well as CT imaging for hemodynamic and anatomic AS evaluation. They compared each patient’s aortic valve cine CT imagery with the relevant robotic model’s aortic cross section under actuation of the aortic sleeve’s pockets as captured using an endoscopic camera.
They then compared critical hemodynamic parameters of AS measured in each patient — mean and maximum transaortic pressure gradients, peak aortic flow velocity and fluid volume ejected at each heartbeat — to the hydrodynamic values generated by the patient’s individualized model (Figure 2). The models replicated patient valve morphology and qualitative hemodynamic data with high accuracy in each case.
Figure 2. Live hydrodynamic echo data across the 3D-printed model recapitulating flow through the aortic valve.
Next, in a subset of five patients, the investigators compared performance of their individualized soft robotic models to models containing aortic valves fabricated using a more conventional approach, with 3D-printed patient-specific aortic sinus and leaflet anatomies and rigid, calcium-like patterns corresponding to mineralized nodules. The soft robotic models more closely matched patients’ clinical parameters than did the models equipped with conventional leaflet valves.
To evaluate the ability of the model’s LV sleeve to mimic loss of ventricular compliance and diastolic dysfunction, the researchers tuned the sleeve’s actuation pressures to simulate the hemodynamics of four of the AS patients who had differing degrees of LV remodeling and had undergone LV catheterization. Again, the model was able to replicate measurements of the patients’ LV and aortic hemodynamics.
Finally, to test the system’s ability to predict the hemodynamic outcome of TAVR, the researchers compared postoperative clinical data from a subset of six patients with data from their individualized models implanted with comparably sized TAVR valves. Pre- and post-TAVR implantation measurements of transaortic pressure gradients showed high correlation between the models and actual patient readings.
“To be able to predict with the model what we see in a patient is clearly important,” Dr. Nguyen says. “If we don’t match what we get from our clinical data, the model will not be informative.”
Goals and next steps
Ultimately, Dr. Nguyen envisions a process in which medical imaging prior to TAVR is used to generate an individualized model that guides decisions about the correct valve size to implant and, perhaps, the creation of a customized valve.
“Our goal is to be able to perform a 3D scan and then create a subject-specific valve,” he says. “An accurate, high-fidelity model is the first step of many towards a personalized valve.”
“Despite incredible advancements in the TAVR arena, there remains a significant number of patients who cannot proceed with TAVR with the valves that are currently commercially available, due to unfavorable anatomy and/or areas of calcification,” says Deborah Kwon, MD, Director of Cardiac MRI at Cleveland Clinic. “However, this important advancement in valve disease simulation and modeling provides an essential platform that enables the possibility of personalized valve interventions and potential customized valve development. It will be exciting to see how this technology enables further innovation and advancement in TAVR care.”
Dr. Nguyen also foresees the model’s use in medical education and procedural planning. “You can think of it as another visualization tool, a way to help interventionalists learn how to approach a procedure in advance,” he says.
To achieve those goals, however, the modeling system will need further validation and eventual human clinical trials. In the near term, the team is focusing on developing a method to use MRI rather than CT imaging to generate the digital model of a patient’s heart, as well as speeding up the 3D printing process from that digital data.
A Stanford Medicine study identifies an easily measured biophysical property that can identify Type 2 diabetics at increased risk for liver cancer who don’t meet current screening guidelines.
Collagen fibers in a three-dimensional hydrogel (left panel). When advanced glycation end products — a byproduct of poorly controlled diabetes — are added (right), the fibers are shorter and more cross-linked, creating conditions that favor cancer progression. Weiguo Fan
For centuries, doctors have used their hands as essential diagnostic tools — exploring joints and palpating abdomens to assess a patient’s health. Often a cancer will reveal itself as a lump or unusual stiffness in a normally bouncy tissue or organ.
More recently, the relationship between stiffness and cancer has been documented through biophysical studies and clinical trials, particularly in liver and breast cancer. For example, stiffness is a primary hallmark of liver cirrhosis, which can progress to liver cancer.
Now researchers at Stanford University have shown that another biophysical characteristic known as viscoelasticity — think of how stretching a ball of Silly Putty or a clump of bread dough is met at first with resistance, and then with release — is even more tightly correlated with liver cancer than stiffness, particularly in people with Type 2 diabetes.
The distinction matters because people with Type 2 diabetes are two to three times as likely as people without diabetes to develop liver cancer, which often occurs in the absence of cirrhosis. Liver cancer rates are increasing in part because the prevalence of diabetes is growing worldwide, particularly in marginalized communities where healthy food choices and opportunities for regular exercise are scarce.
“This is the first time that the dogma of matrix stiffness as a primary predictor of liver cancer is being challenged,” said professor of gastroenterology and hepatology Natalie Torok, MD. “Current guidelines recommend routine liver cancer screening only for people with cirrhosis. As a result, many people with Type 2 diabetes are not screened at all. These new findings have major implications not just for liver cancer, but also other cancers for which diabetes is a risk factor, including breast cancers.”
Torok is the senior author of the study, which was published online Jan. 31 in Nature. Postdoctoral scholar Weiguo Fan, PhD, is the lead author.
Torok and her colleagues collaborated with researchers in the laboratory of associate professor of mechanical engineering Ovijit Chaudhuri, PhD, to investigate the role of viscoelasticity in liver cancer in patient samples, animal models and cells grown in the laboratory in a Jell-O-like tissue scaffolding called a hydrogel.
“This study is the first on the role of viscoelasticity in cancer with data that spans from humans and mouse models to in vitro 3D culture studies and computational simulations,” Chaudhuri said. “It definitively establishes the role of viscoelasticity in liver cancer progression.”
Liver stiffness is measured non-invasively with imaging techniques called transient elastography or MR elastography involving a vibrating pad placed on the abdomen. The vibrations are transmitted from the imaging probe to the organ; the wave of vibration moving through a stiff medium differs from one moving through something more malleable. People with a liver stiffness that exceeds a certain threshold are diagnosed with liver cirrhosis; current guidelines recommend that they be screened every six months for liver cancer with an abdominal ultrasound and blood tests.
Measurements such as stiffness arise from what’s called the extracellular matrix — the space between and around an organ’s cells that is chock-a-block with proteins, sugars and minerals.
“Our organs are not just clumps of cells,” Chaudhuri said. “The cells exist in a scaffolding called the extracellular matrix that gives them physical support but also affects their maturation, specialization and functioning.”
Like a grade-school teacher, the matrix provides a physical framework that supports and organizes the cells, gentling and channeling them to harmoniously create a functional tissue. When the matrix is disrupted, any bad-apple cancerous or pre-cancerous cells more readily lose their way, spreading to places they shouldn’t; dividing uncontrollably; or morphing in to other, more dangerous versions of themselves.
People with diabetes have elevated levels of what are called advanced glycation end products, or AGEs. AGEs arise when blood sugar is poorly controlled and elevated levels of sugar molecules known as glucose begin to glom onto nearby proteins including collagen — a key structural component of the extracellular matrix. (AGEs are also present in protein- or fat-rich foods or in foods prepared at high heat such as frying or broiling.)
The researchers found that liver samples from people with Type 2 diabetes had higher levels of AGEs and were more viscoelastic — but no more stiff — than liver samples from people without Type 2 diabetes. A closer look in laboratory mice showed animals fed a diet high in AGEs had shorter and less interconnected collagen fibers in the liver’s extracellular matrix than those found in animals fed standard chow.
Next, the researchers studied how cells behaved when grown in the laboratory in a three-dimensional gel to mimic liver matrix structure. Tinkering with the cells outside the body allowed them to assess the effect of various changes in their growth and behavior.
“In our engineered hydrogels, we can tune one biophysical property such as viscoelasticity or stiffness at a time to understand how each property impacts the cells,” Chaudhuri said. “We saw that a change in viscoelasticity alone is enough to drive a more invasive behavior in the cells.”
In particular, the researchers noted that a more viscoelastic matrix promotes changes in liver cell shape and allows the formation of invasive protrusions on their membranes that help them escape natural barriers meant to keep cells in their rightful places.
Paradigm shift
Finally, Torok and her colleagues went one step further, dissecting a series of cellular signals that promote liver cancer progression in viscoelastic conditions that includes a cancer-associated protein called YAP.
“This is the first time that changes in collagen structure have been proven to promote viscoelasticity and liver cancer progression independent of stiffness,” Torok said. “It’s a complete change in paradigm that could explain the greater risk of liver cancer in people with Type 2 diabetes and may help select people should undergo regular liver cancer screening.”
Fortunately, like stiffness, viscoelasticity can be assessed non-invasively with MR elastography by changing a few parameters in vibration frequency and measurement. Torok is planning to launch a clinical trial to further study viscoelasticity, Type 2 diabetes and liver cancer progression.
“One of the major questions in medicine today is why people with diabetes and fatty liver disease are so prone to liver cancer, and how we can address this,” Torok said. “Our research suggests that many more people, particularly those with diabetes, should be screened for cancer. If we did that, perhaps we could act earlier and save lives.”
Researchers from Purdue University; Tsinghua University in Beijing; the University of Pittsburgh; the University of California, Davis; Albert Einstein College of Medicine; Keio University in Yokohama; and the University of Pennsylvania contributed to the work.
Summary: Researchers unveiled the most extensive single-neuron projectome database to date, featuring over 10,000 mouse hippocampal neurons.
The study provides an unprecedented view of the spatial connectivity patterns at the mesoscopic level, crucial for understanding learning, memory, and emotional processing in the hippocampus. By employing machine learning algorithms for categorizing axonal trajectories and integrating spatial transcriptome data, researchers identified 43 distinct projectome cell types, revealing intricate projection patterns and soma locations’ correspondence to projection targets.
This work, accessible via the Digital Brain CEBSIT portal, lays the structural foundation for advancing our knowledge of hippocampal functions and their molecular underpinnings.
Key Facts:
The study reconstructed whole-brain axonal morphology of over 10,000 mouse hippocampal neurons, creating the world’s most extensive single-neuron projectome database.
Researchers used machine learning to analyze morphological similarities among neurons, identifying 43 distinct projectome cell types.
The integration of projectome cell types with spatial transcriptome data revealed potential molecular and circuit targets for hippocampal functions, all accessible through a dedicated online platform.
Source: Chinese Academy of Science
A study published in Science on Feb. 1 reported a comprehensive database of single-neuron projectomes consisting of over 10,000 mouse hippocampal neurons, thus revealing the spatial connectivity patterns of mouse hippocampal neurons at the mesoscopic level.
The study was conducted by teams from the Center for Excellence in Brain Science and Intelligence Technology (CEBSIT), the Institute of Neuroscience of the Chinese Academy of Sciences (CAS), the HUST-Suzhou Institute for Brainsmatics, Hainan University, the Kunming Institute of Zoology of CAS, Lingang Laboratory, and the Shanghai Center for Brain Science and Brain-Inspired Technology.
Hippocampal neurons project widely to the brain-wide targets; thus, it is critical to investigate the projection patterns of hippocampal neurons at the single-neuron level. Credit: Neuroscience News
The hippocampus serves as an essential brain region for learning and memory as well as various brain functions such as spatial cognition and emotional processing. It is one of the most extensively studied brain regions.
Hippocampal neurons project widely to the brain-wide targets; thus, it is critical to investigate the projection patterns of hippocampal neurons at the single-neuron level.
This study reconstructed the whole-brain axonal morphology of over 10,000 neurons in the mouse hippocampus at a single-cell resolution with the neuronal cell bodies covering all subregions and multiple locations along different hippocampal axes, making this the most extensive single-neuron projectome database in the world.
This study took an innovative approach to categorize axonal trajectories with machine learning algorithms, thus allowing for a more efficient analysis of the morphological similarities among 341 projection patterns for mouse hippocampal neurons and ultimately identifying 43 distinct projectome cell types. It also incorporated the spatial transcriptome of mouse CA1 areas.
Based on these analyses, the study was able to elucidate the axonal projection pathways of hippocampal neurons along the anterior-posterior axis and reveal new projection patterns of hippocampal neurons. It also outlined the correspondence between hippocampal neuron soma locations and projection targets, and revealed basic organization principles of bilateral projections.
Furthermore, correlation analysis of projectome cell types and spatial transcriptome data identified spatial correspondence between various genes and projectome subtypes, providing potential molecular and circuit targets for hippocampal functions.
Taken together, this study provides a structural basis for future studies of hippocampal functions and deciphers the potential correspondences between their soma locations, gene expression, and circuitry functions.
The database for the hippocampal single-neuron projectomes, along with the database on the hippocampal longitudinal axis and spatial transcriptomes, are now publicly accessible through the Digital Brain CEBSIT portal (https://mouse.digital-brain.cn/hipp).
To facilitate broader usage of the databases, a team from the Computing and Data Center of CEBSIT has developed a website to integrate data visualization, user interface, online analysis, and data downloads.
Abstract
Whole-brain spatial organization of hippocampal single-neuron projectomes
INTRODUCTION
In the brain circuitry, a single neuron could broadcast output signals to other neurons located in nearby or distant areas. Therefore, understanding the spatial organization of axon projections at the single-cell level is crucial for elucidating the neural circuitry underlying various brain functions. As a brain structure essential for learning, memory, cognition, stress responses and emotional behaviors, it is known that the hippocampus (HIP) is widely connected with various brain areas, including the cortex, thalamus, hypothalamus, olfactory areas, and amygdala. However, it remains unclear how single HIP neurons project to brain-wide target areas and how a single-neuron projectome can be specified by the soma location within the HIP.
RATIONALE
To reconstruct single-neuron projectomes of the mouse HIP, we combined sparse-labeling methods with fluorescence micro-optical sectioning tomography and reconstructed the soma, axon arbors, and dendrites of individual neurons. We used a wide range of analytic tools for the projectome analysis and created a state-of-art web interface to visualize the projectome data.
RESULTS
We have created an open and comprehensive database with 10,100 single-neuron projectomes throughout the HIP, which allows interactive query, visualization, and analysis of reconstructed brain-wide projectomes. We classified HIP neurons into 341 projection patterns, and then 43 projectome subtypes, based on their axon morphology and brain-wide target areas.
Our study revealed previously unknown axon projection patterns, target-dependent soma distribution within HIP subdomains, a general rule for bihemispheric projections, axon orientation rules for mossy fibers and Schaffer collaterals, and topographic correlation between axon arbors and soma location along HIP axes.
CONCLUSION
Single-neuron projectome analyses have provided unprecedented information on axon projection patterns at the single-cell resolution and elucidated the organizational principles of whole-brain connectivity of HIP neurons. Such knowledge could be further combined with gene expression data to define HIP neuron subtypes and serve as the structural basis for understanding their diverse and coordinated functions.
The idea of de-extinction has been around for some time now and many have pondered upon it. Now, a startup plans to make this idea a reality by bringing back the woolly mammoth from the dead, thousands of years after it went extinct. The startup is partially funded by Harvard University’s renowned geneticist, George Church, and the company is called Colossal.
The woolly mammoth roamed the Arctic for thousands of years before eventually going extinct. Early humans began hunting these mammoths for food and used their bones as tools. Scientific studies show that changing climate conditions forced these freely moving animals into smaller habitats, where human hunting finished them off almost 4000 years ago. Models also show that if it weren’t for the hunting, the mammoths could have survived until recently.
Either out of guilt or to take the next big leap in science, researchers have been pondering about resurrecting the mammoth. This Jurassic Park-like experiment has also been aided by the finding of well-preserved mammoth remains that hold bits of mammoths’ DNA in them. Combining these with recent technological developments in the field, the resurrection or “de-extinction”, as it is called, is quite possible, the company says.
The company has condensed the entire process into a 13-step high-level plan on its website. The first step begins with the sourcing and then sequencing of the genome of the Asian elephant, a mammal that is reported to share 99.6 percent of its DNA with the woolly mammoth. The team will then sequence the genome of the woolly mammoth that the researchers in George Church’s Harvard Lab secured in 2018.
Since most characteristics are encoded by the sequences in our genomes, the researchers will be able to identify regions in the Asian elephant’s genome that differ from the woolly mammoth’s. Using CRISPR, the team will then edit the genome of the Asian elephant and verify if the edited cells demonstrate abilities to survive in cold environments. Once this is confirmed, they will insert the editing nucleus in an egg cell and then fertilize it artificially. Once complete, the cell will develop into an embryo that will then be implanted in an African elephant for the gestation of up to 22 months, bringing the woolly mammoth back on Earth.
In an interview with Venture Beat, Colossal said that all the fundamental science needed to achieve this is now solved, and the company could see their first woolly mammoth calves in the next four to six years. Co-founder Ben Lamm, a serial entrepreneur in the tech industry, said that the formation of the company will accelerate the research work.
But the de-extinction effort is not just for goosebumps. Colossal believes that returning the woolly mammoth to the Arctic grasslands will help in arresting the effects of climate change. In their time, the mammoths traversed vast regions in the Artic and conserved its environmental health. Restoring the mammoth to its habitat will help in methane suppression and carbon sequestration, thereby helping climate change.
As the years wear down on us, our bodies accumulate a whole host of damaged cells that stubbornly refuse to die. Called senescent cells, these cellular oddballs are like the moldy fruit in the basket, hastening the spoilage of the rest or, in our body’s case, ushering in a myriad of age-related diseases.
In the quest for the fountain of youth, senescent cells have become a hot ticket item. Scientists are actively researching the genes and other biological factors that make these cells so resilient, including testing a class of drugs called senolytics designed to wipe them out. Now, one group of researchers has figured out a way to reprogram a key player of the immune system to take down senescent cells like a heat-seeking missile of rejuvenation.
The process involves genetically engineering white blood cells called T cells to create what’s known as chimeric antigen receptor (or CAR) T cells. These specialized cells recognize and attack a specific cellular target. Researchers at Cold Spring Harbor Laboratory in New York tailored a CAR T cell to home in on a molecule found in large amounts of senescent cells called urokinase plasminogen activator receptor (uPAR). When these T cells were sicced on senescent cells in aged mice with metabolic issues and young mice fed a high-fat diet, which can trigger age-related senescence, the animals pulled a 180 with almost no side effects, losing weight, becoming more physically active, and seeing improvements in their metabolism.
“If we give it to aged mice, they rejuvenate. If we give it to young mice, they age slower. No other therapy right now can do this,” Corina Amor Vegas, the study’s first author and an assistant professor at Cold Spring Harbor Laboratory, said in a press release.
In recent decades, CAR T cells have made a name for themselves in fighting cancer as a promising immunotherapy. They are often dubbed “living drugs” because the white blood cells can be taken directly from someone through a blood sample and then reintroduced after they’ve been genetically altered, which is lately done with the gene-editing tool CRISPR.
One significant challenge with CAR T cells, however, is finding just the right molecule – or biomarker — specific to the cell you want to target, a concern especially crucial in cancer treatment where you wouldn’t want your “living drug” to target healthy instead of cancerous cells. No two cancer cells share the exact same cast of molecules on their cell surfaces, which is likewise for senescent cells.
The new study relies on earlier research that laid the groundwork for that search. In a 2020 paper published in Nature, researchers from the Memorial Sloan Kettering Cancer Center, which included Amor Vegas, found that senescent cells had more uPAR dotting their outside surfaces compared to other cell types.
When the researchers tested anti-uPAR CAR T cells in two separate groups of mice, one with lung cancer and the other with liver fibrosis (a condition where healthy liver tissue becomes scarred and can lead to cirrhosis and liver cancer), the animals, surprisingly, lived longer.
This success prompted a next step: testing whether a CAR T-cell therapy could extend longevity in regular mice.
The image shows healthy pancreatic tissue samples from an old mouse treated with CAR T cells as a young pup. Senescent cells visible in blue.
Amor Vegas and her colleagues used the same CAR T cells developed from their earlier experiment, intravenously infusing them into a group of mice between the ages of 18 to 20 months old (equivalent to 56 to almost 70 years old in humans); a control group didn’t get the treatment. These mice were fed a normal diet but, because of their advanced age, suffered from age-related metabolic dysfunction — a condition humans also develop as we age — where they had elevated blood sugar levels and weren’t able to move around or exercise all that much.
CAR T cells targeting uPAR were also given to a group of much younger mice, about three months old, before they were started on a high-fat diet, where about 60 percent of their calories came from fat. Studies show that consuming that amount of fat can promote senescent cells through the stress and inflammation caused by obesity. While these animals didn’t yet have any metabolic disorders, the CAR T cells were given as a prophylactic in an attempt to belay the inevitable aging.
For both groups of mice, the CAR T cells did their magic. Older mice found themselves healthier with lower glucose and insulin levels and fewer inflammatory markers circulating in their blood; they were moving around and weighed less. The younger mice who were given the treatment about a month and a half before starting their high-fat diet didn’t gain as much weight, and their blood sugar levels were better compared to their counterparts who didn’t get this treatment.
FURTHER RESEARCH NEEDED
These findings are striking in that we have a possible new path to use our own immune cells to shed the cellular damage wrought by aging that could be long-lasting even after one dose. For example, in the younger mice, the researchers found that the anti-uPAR CAR T cells were still hanging around in the animals’ spleens and livers and were mostly a subtype of T cells, known as a CD8+ T cell, that has the ability to fight off harmful cells.
“T cells have the ability to develop memory and persist in your body for really long periods, which is very different from a chemical drug,” said Amor Vegas. “With CAR T cells, you have the potential of getting this one treatment, and then that’s it. For chronic pathologies, that’s a huge advantage. Think about patients who need treatment multiple times per day versus you get an infusion, and then you’re good to go for multiple years.”
However, implementing an anti-aging CAR T-cell therapy needs to go through more clinical trials with both animals and eventually humans before it can ever reach the market. The good news is that research into engineering and developing CAR T cells is pretty advanced, and there are more clinical trials, specifically for cancer, now than ever. As plans for cheaper and even off-the-shelf CAR T-cell therapies are being explored, your anti-aging “living drug” could be here sooner than you think.
Scientists found leftover viral DNA may be crucial to embryonic development.
Some millions of years ago, a far distant ancestor of all animals encountered a virus that inserted its own genetic material into the creature. Over the course of animal evolution, these bits of viral DNA accrued with every new encounter and were passed down the generations.
In a study published Wednesday in the journal Science Advances, researchers at the Spanish National Cancer Research Center (CNIO) found some junk DNA may be crucial to embryonic development, a molecular turning point steering cells from a state of infinite potential to a more targeted trajectory.
EMBRYONIC DEVELOPMENT
The junk DNA at the heart of this switch is called MuERV-L (or MERVL) endogenous retroviruses. The researchers found in mice, MERVL-gag, a retroviral protein of MERVL endogenous retroviruses, interacts with a gene called URI, which influences whether or not an embryo develops smoothly and at the right pace.
“It is a totally new role for endogenous retroviruses,” Nabil Djouder, a cell biologist at CNIO who led the study, said in a press release. “We discovered a new mechanism that explains how an endogenous retrovirus directly controls” an embryonic cell’s ability to develop into many different cell types, what’s referred to as pluripotency.
URI, also known by its mouthful unconventional prefoldin RPB5 interactor, is part of the class of molecules called prefoldins whose job it is to ensure our cells’ proteins fold correctly and don’t clump together, akin to the backstage theater crew maintaining order behind the scenes.
MERVL endogenous retroviruses, on the other hand, are known to be active when a fertilized egg (or zygote) divides into a two-celled embryo, individually called blastomeres. At this point, these cells are totipotent, meaning they have the power and the potential to become any type of cell in the body. But to prevent blastomeres from going off the embryonic rails, becoming anything they want in an uncoordinated fashion, certain genes are turned on to coax the cells toward becoming specialized cell types, like muscle or nerve.
According to some studies, MERVL endogenous retroviruses are one of the first genes turned on in early embryos and seem to help drive genes related to totipotency. Interestingly, activating MERVL in pluripotent stem cells reverses them into an early embryo-like state. However, messing with MERVL can lead to big problems, like cells being unable to segregate into specific types. But just like with URI, how this fascinating piece of junk DNA is able to hold so much sway over an embryonic cell’s fate is still a bit of a mystery.
A NEW MECHANISM
To see if there’s a missed connection between the two, Djouder and his colleagues at CNIO played around deleting and turning on and off MERVL endogenous retroviruses — particularly the protein MERVL-gag — as well as the URI gene in mouse embryos.
They found the URI acts like a sort of molecular bodyguard for two other genes associated with development and pluripotency, called OCT4 and SOX2, respectively. It protects them from damage and allows the embryo to make the switch from totipotency to pluripotency. MERVL-gag, however, is the junk DNA hired gun taking out URI and keeping the early embryo totipotent.
But all this happens in a smooth, sequential order. In the beginning, when the early embryo is totipotent, MERVL-gag is circulating in high amounts and keeps URI silenced by binding to it. Eventually, its levels decline, which frees up URI to go back to protecting OCT4 and SOX2, allowing the early embryo to continue expanding its way to a tingling mass of pluripotent cells.
While this research is far from over, the scientists see this molecular mechanism opening up a whole range of possibilities, such as creating more stable embryonic stem cells (or ESCs), which are cells that possess unlimited self-renewal capabilities, turning into any cell type in the body.
“Such engineered ESCs could find diverse applications, including regenerative medicine, disease modeling, and the creation of artificial embryos,” the authors write in their paper.
Between 1990 and 2018, the incidence rate of pancreatic cancer increased in France by 2.7% per year on average for men and, more significantly, by 3.8% annually for women. Its prognosis remains very poor, with a net 5-year survival rate of under 10%. The classic risk factors (diabetes, smoking, obesity, alcohol) are well known. Likewise, a family history of the disease increases the risk for developing pancreatic cancer ninefold. It is estimated that 90% of the predisposing genes involved in the development of pancreatic cancer have yet to be identified.
In this context, any new approach for early diagnosis of early-stage pancreatic cancer is welcome. A US-based team seeks to develop and validate a model allowing clinicians to predict the risk for pancreatic cancer.
Data and AI
Using electronic health record (EHR) data from a multi-institutional federated network combining 55 hospitals over 13 years, a team of researchers from the Massachusetts Institute of Technology in Cambridge developed a neural network (PrismNN) and logistic regression analysis (PrismLR) to predict pancreatic duct adenocarcinoma (PDAC) risk at 6-18 months before diagnosis for patients 40 years or older.
With 35,387 PDAC cases, 1,500,081 controls, and 87 features per patient, PrismNN obtained a test area under the curve (AUC) of 0.826 (PrismLR: 0.800). PrismNN’s average internal-external validation AUCs were 0.740 for locations, 0.828 for races, and 0.789 for time. PrismNN sensitivity was just 35.9%. Its specificity was 95.3%.
Patients with a family history of or genetic predisposition to PDAC make up approximately 2%-10% of all cases in the literature. Identification of the genes involved in the development of cancer is expected, thanks to the development of high-throughput sequencing methods. In the meantime, we know to use MRI and endoscopic ultrasound scanning to monitor high-risk patients with precancerous lesions (intraductal papillary mucinous neoplasms, mucinous cystadenomas). However, in the general population, screening of a small de novo neoplasm (< 1 cm) is not based on any biological testing.
Prospective Validation Needed
The Prism deep learning algorithm uses 87 pieces of data from EHR comprising diagnosis, medicinal products, disparate laboratory data, and demographic data, from a population that is ethnically and geographically diverse. This model maintained its high specificity and accuracy throughout the internal-external validation.
This novel method detected 3.5-fold more patients than the current criteria used to identify patients for PDAC screening programs at similar risk levels and at 6-18 months before to onset. Nevertheless, this is a retrospective study (development and validation) in which certain ethnic groups and persons from disadvantaged socioeconomic backgrounds were underrepresented and, most of all, in which the biological parameters used were heterogeneous (from blood electrolytes to glucose levels). The study also included disparate data, with family history of the disease given without any genetic data, and there was no recognition of the respective weight of each item in the final positive prediction.
Validation in a prospective cohort is more essential than ever, as the sensitivity of this deep learning–based digital approach (around 35.9%) remains insufficient when considering individual application without an appropriate genetic biomarker. This factor makes the practical application of individual screening impossible for the time being, outside of institutions affiliated with a network using this technology. Still, the readability of the technology remains unclear unless it is known how many successive layers were used in this IT-based model.
We are, nonetheless, on the precipice of a new era in which artificial intelligence is set to transform the structure of EHRs and the integration of relevant biological and genetic data into algorithms capable of predicting the risk for certain occult cancers that remain symptomless in their early stages.
To conclude, this deep learning model has provided a specific basis for detecting individuals at high risk for PDAC, although the sensitivity is low. The 87 data items entered into the digital model are highly heterogeneous. Artificial intelligence needs to advance further to translate algorithmic advances into robust biomedical breakthroughs.






/img/iea/M3Oe9e0jON/biotech-startup-wants-to-bring-back-the-woolly-mammoth.jpg)