That persistent cough and wheezing is bad enough without gum disease making it worse. New research reveals why periodontitis, a common gum infection, accelerates the progression of chronic obstructive pulmonary disease (COPD), the irreversible and often deadly lung condition affecting almost 16 million Americans.
Chinese scientists have discovered how bacteria from inflamed gums can travel to the lungs, exacerbating COPD symptoms. The findings from Sichuan University offer hope for new treatment possibilities for managing the breath-stealing disease.
Oral Bacteria Directly Trigger Flare-Ups in COPD Lungs
COPD, encompassing emphysema and chronic bronchitis, is the world’s sixth leading cause of death.
The condition is quietly hurting millions of Americans, as many are unaware they have it. In the United States, cigarette smoking drives most COPD cases, while cooking over open fires drives cases in underdeveloped countries, Dr. Norman Edelman, a pulmonologist at Stony Brook Medicine, professor of internal medicine, and core member of the public health program at Stony Brook University, told The Epoch Times.
COPD impedes airflow and breathing by damaging the airways and lungs. Key symptoms are coughing, excess mucus, and wheezing. Patients also suffer acute exacerbations where symptoms abruptly worsen for days.
While prior research has linked mouth infections to COPD progression, the exact mechanisms were unclear. A 2018 study posited the two were only connected by smoking as a shared risk factor.
The new research from Sichuan University, published in the American Society for Microbiology Journals, finds gum disease pathogens directly associate with COPD flare-ups by activating lung immune cells, which increase lung inflammation-driving bacteria. The researchers demonstrated this in animal models.
“We’ll further carry out additional studies on human subjects to confirm the mechanism,” microbiologist and co-study author Yan Li said in a press statement. “Our findings could lead to a potential new strategy for treating COPD.”
The study shows how poor dental care enables oral bacteria like P. gingivalis to enter the lungs, said Dr. Thomas Kilkenny, director of critical care in pulmonary medicine at Staten Island University Hospital, who was not involved in the research.
“This sets up chronic levels of inflammation beyond that found in COPD,” he told The Epoch Times. Although the various bacteria alone can cause an increased number of respiratory infections, “the heart of the study was the inflammatory cells,” he noted.
Circulating oral bacteria trigger the overproduction of immune signaling chemicals called cytokines. The cytokines spark harmful inflammation and disturb normal lung structures, Dr. Kilkenny said.
70 Percent of COPD Cases Due to Smoking
The root cause behind most preventable COPD cases is cigarette smoking. Smoking activates lung immune cells to release cytokines, fueling inflammation, Dr. Kilkenny added. Smoking accounts for 70 percent of cases.
Nonsmoking risk factors include:
A history of childhood lung infections.
A history of asthma.
Smoke from home cooking and heating fuels.
Secondhand tobacco smoke.
Genetic mutations that can cause the disease.
Vitamin D deficiency may also raise COPD risk. A 2020 meta-analysis of randomized controlled trials found many COPD patients to be vitamin D deficient. Further, vitamin D supplements helped improve lung function for these patients.
Fight Gum Infections to Maintain Overall Health: Expert
While the study could result in future COPD treatments, that lies far in the future, according to Dr. Edelman. He stressed that it would be better for people to take care of their periodontal health.
“To me, the real story, which many people don’t know, is that periodontal disease is a risk factor for systemic disease,” he said. These diseases include diabetes and heart disease.
The prevalence of gum infections in disadvantaged communities constitutes a significant public health issue, he noted.
Specifically, Dr. Edelman said he had observed about one-third of low-income kids on Long Island, where he practices, having tooth decay or gum disease. Getting the word out on the health impacts tied to poor oral health should take priority over any long-term therapeutic implications of this research, he noted.
People with depression have higher body temperatures, suggesting there could be a mental health benefit to lowering the temperatures of those with the disorder, a new UC San Francisco-led study found.
The study, published today in Scientific Reports, doesn’t indicate whether depression raises body temperature or a higher temperature causes depression. It’s also unknown whether the higher body temperature observed in people with depression reflects decreased ability to self-cool, increased generation of heat from metabolic processes or a combination of both.
Researchers analyzed data from more than 20,000 international participants who wore a device that measures body temperature, and also self-reported their body temperatures and depression symptoms daily. The seven-month study began in early 2020 and included data from 106 countries.
The results showed that with each increasing level of depression symptom severity, participants had higher body temperatures. The body temperature data also showed a trend toward higher depression scores in people whose temperatures had less fluctuation throughout a 24-hour period, but this finding didn’t reach significance.
The findings shed light on how a novel depression treatment method might work, said Ashley Mason, Ph.D., the study’s lead author and associate professor of psychiatry at UCSF Weill Institute for Neurosciences. A small body of existing, causal studies has found that using hot tubs or saunas can reduce depression, possibly by triggering the body to self-cool, for example, through sweating.
Average self-reported body temperature by time-of-day. Figure depicts expected diurnal pattern of lowest self-reported body temperatures reported in the early morning hours and higher self-reported body temperatures during daytime hours. Note. Blue line depicts average self-reported body temperature (right Y axis) by time of day; blue shading indicates standard error of the mean. Red shading indicates number of responses (left Y axis) provided at each minute (X axis). Credit: Scientific Reports (2024). DOI: 10.1038/s41598-024-51567-w
“Ironically, heating people up actually can lead to rebound body temperature lowering that lasts longer than simply cooling people down directly, as through an ice bath,” said Mason, who is also a clinical psychologist at the UCSF Osher Center for Integrative Health. “What if we can track the body temperature of people with depression to time heat-based treatments well?”
“To our knowledge, this is the largest study to date to examine the association between body temperature—assessed using both self-report methods and wearable sensors—and depressive symptoms in a geographically broad sample,” added Mason. “Given the climbing rates of depression in the United States, we’re excited by the possibilities of a new avenue for treatment.”
A a view from inside the OMEGA target chamber during a direct-drive inertial fusion experiment at the University of Rochester’s Laboratory for Laser Energetics. Scientists fired 28 kilojoules of laser energy at small capsules filled with deuterium and tritium fuel, causing the capsules to implode and produce a plasma hot enough to initiate fusion reactions between the fuel nuclei. The temperatures achieved at the heart of these implosions are as high as 100 million degrees Celsius (180 million degrees Fahrenheit). The speed at which the implosion takes place is typically between 500 and 600 kilometers per second (1.1 to 1.35 million miles per hour). The pressures at the core are up to 80 billion times greater than atmospheric pressure.
Scientists from the University of Rochester’s Laboratory for Laser Energetics (LLE) led experiments to demonstrate an effective “spark plug” for direct-drive methods of inertial confinement fusion (ICF). In two studies published in Nature Physics, the authors discuss their results and outline how they can be applied at bigger scales with the hopes of eventually producing fusion at a future facility.
LLE is the largest university-based U.S. Department of Energy program and hosts the OMEGA laser system, which is largest academic laser in the world but still almost one hundredth the energy of the National Ignition Facility (NIF) at the Lawrence Livermore National Laboratory in California.
With OMEGA, Rochester scientists completed several successful attempts to fire 28 kilojoules of laser energy at small capsules filled with deuterium and tritium fuel, causing the capsules to implode and produce a plasma hot enough to initiate fusion reactions between the fuel nuclei. The experiments caused fusion reactions that produced more energy than the amount of energy in the central hot plasma.
The OMEGA experiments use direct laser illumination of the capsule and differ from the indirect drive approach used on the NIF. When using the indirect drive approach, the laser light is converted into X-rays that in turn drive the capsule implosion. The NIF used indirect drive to irradiate a capsule with X-rays using about 2,000 kilojoules of laser energy. This led to a 2022 breakthrough at NIF in achieving fusion ignition—a fusion reaction that creates a net gain of energy from the target.
“Generating more fusion energy than the internal energy content of where the fusion takes place is an important threshold,” says lead author of the first paper Connor Williams ’23 Ph.D. (physics and astronomy), now a staff scientist at Sandia National Labs in radiation and ICF target design. “That’s a necessary requirement for anything you want to accomplish later on, such as burning plasmas or achieving ignition.”
By showing they can achieve this level of implosion performance with just 28 kilojoules of laser energy, the Rochester team is excited by the prospect of applying direct-drive methods to lasers with more energy. Demonstrating a spark plug is an important step, however, OMEGA is too small to compress enough fuel to get to ignition.
“If you can eventually create the spark plug and compress fuel, direct drive has a lot of characteristics that are favorable for fusion energy compared to indirect drive,” says Varchas Gopalaswamy ’21 Ph.D. (mechanical engineering), the LLE scientist who led the second study that explores the implications of using the direct-drive approach on megajoule-class lasers, similar to the size of the NIF. “After scaling the OMEGA results to a few megajoules of laser energies, the fusion reactions are predicted to become self-sustaining, a condition called ‘burning plasmas.'”
Gopalaswamy says that direct-drive ICF is a promising approach for achieving thermonuclear ignition and net energy in laser fusion.
“A major factor contributing to the success of these recent experiments is the development of a novel implosion design method based on statistical predictions and validated by machine learning algorithms,” says Riccardo Betti, LLE’s chief scientist and the Robert L. McCrory Professor in the Department of Mechanical Engineering and in the Department of Physics and Astronomy. “These predictive models allow us to narrow the pool of promising candidate designs before carrying out valuable experiments.”
The Rochester experiments required a highly coordinated effort between large number of scientists, engineers, and technical staff to operate the complex laser facility. They collaborated with researchers from the MIT Plasma Science and Fusion Center and General Atomics to conduct the experiments.
A genetic signature for HER2-low tumors has been found that may solve a problem for those seeking wider use of drugs targeting such cancers, particularly antibody drug congugate (ADC) Enhertu (trastuzumab-deruxtecan/T-DXd). ADCs carry a payload that helps them be especially effective.
Their 20-gene signature, the team says, shows promise in distinguishing between HER2 0 and HER2-low expressing tumors, including those scored as 1+ at IHC, and in developing a selection approach for ADC candidates.
The study was published in Nature Scientifice Reports, and the lead author was Serena Di Cosimo of Milan’s Fondazione IRCCS Istituto Nazionale Dei Tumori.
In August 2022, the U.S. Food and Drug Administration (FDA) approved Enhertu for the treatment of patients with unresectable or metastatic HER2-low breast cancer. The drug was the first approved therapy for patients with the newly identified HER2-low breast cancer subtype.
Of the more than 287,000 news cases of breast cancer diagnosed in the U.S. last year, between 80% and 85% were previously considered to be HER2-negative subtype. Of those cases, as many as 60% of patients previously classified as having HER2-negative subtype can now be considered as HER2-low.
Assessment of Human Epidermal growth factor Receptor 2 (HER2) status is a standard practice in breast cancer diagnostics. Patients with breast cancer scoring 3+ at immunohistochemistry (IHC) and/or exhibiting gene amplification at in situ hybridization (ISH) are deemed HER2-positive. Tumors are considered negative for the marker when IHC scores are 0, 1+, or 2+ without amplification.
However, emerging evidence is challenging this binary classification.
For instance, in the DESTINY-Breast04 study, T-DXd demonstrated a 50% reduction in the risk of progression, and a 36% reduction in the risk of death in patients with HER2-low (IHC 1+, and 2+ without amplification) metastatic breast cancer (MBC). This finding led to the ongoing DESTINY-Breast06 trial, which is evaluating T-DXd in patients with even lower HER2 expression in MBC – IHC 0 or 1+. This level is referred to as ultralow.
Concerns have arisen regarding the reproducibility such testing in daily practice. Until now, pathologists have not needed to differentiate between IHC 0, with incomplete and faint staining in ≤ 10% of tumor cells, and IHC 1+, same staining intensity in > 10% of tumor cells. Nor have they been required to distinguish IHC 1+ from 2+ showing weak to moderate staining.
This team aimed to analyze breast cancer gene expression profile (GEP) with respect to HER2 IHC categories, and to train a genomic classifier for identifying HER2-low tumors.
In clinical trials evaluating ADCs, HER2-low breast cancer is defined through protein immunohistochemistry scoring (IHC) 1+ or 2+ without gene amplification. However, in daily practice, the accuracy of IHC is compromised by inter-observer variability.
The team “…aimed to identify HER2-low breast cancer primary tumors by leveraging gene expression profiling. A discovery approach was applied to gene expression profile of institutional INT1 (n = 125) and INT2 (n = 84) datasets.”
They identified differentially expressed genes (DEGs) in each specific HER2 IHC category 0, 1+, 2+ and 3+. A HER2-low signature was computed based on HER2 IHC category-specific DEGs. The twenty genes included in the signature were significantly enriched with lipid and steroid metabolism pathways, peptidase regulation, and humoral immune response.
Researchers at the University of Granada (UGR), Spain have shown that sclerostin, a bone formation inhibitor protein, is also protective of the cardiovascular health of patients with type 2 diabetes.
The research was conducted by the MP20-Biomarkers of Metabolic and Bone Diseases research group at the Biohealth Research Institute in Granada (ibs.GRANADA). Led by Manuel Muñoz Torres, MD, PhD, a professor of medicine at UGR, the study of 260 people included 121 controls and 139 patients with type 2 diabetes. The study authors noted that this study was the first of its kind to examine whether sclerostin, a bone formation inhibitor protein, plays a detrimental or protective role in the development of atherosclerotic process in T2D population.
The study showed that patients with both type 2 diabetes who also had heart disease had significantly higher levels of sclerostin, pointing to a potential link between the protein and atherosclerosis. Sclerostin was also demonstrated to play a beneficial role in reducing arterial calcification, which is also associated with the development of atherosclerosis. They found that sclerostin overexpression reduced calcium deposits, decreased cell proliferation and inflammation, and promoted cell survival.
“Sclerostin could play a protective role in the development of atherosclerosis in T2D patients by reducing calcium deposits, decreasing proliferation and inflammation, and promoting cell survival in VSMCs under calcifying conditions,” the researchers wrote in their study which appears in the journal Cardiovascular Diabetology. “Therefore, considering the bone-vascular axis, treatment with anti-sclerostin for bone disease should be used with caution.”
The published results were a part of the doctoral thesis of researcher Sheila González Salvatierra and raise concerns about the use of anti-sclerostin antibody treatments in patients with type 2 diabetes as this may increase cardiovascular risk in this patient population. This class of drugs is often used in treating patients with osteoporosis and other bone diseases.
The investigators noted that a broad number of previous studies has described how the elevation of serum sclerostin levels associated with cardiovascular alterations. However, the function of this protein at the vascular level had not been studied in depth.
“Our biochemical results suggest a potential beneficial role of sclerostin on (cardiovascular diseases) in type 2 diabetes patients due to its inverse association with some cardiovascular risk factors such as LDL-c, calcium, and diastolic blood pressure, which are considered the main factors contributing to susceptibility to atherosclerosis,” the team noted.
The researchers noted that while sclerostin is clinically important in vascular calcification, the exact biochemical processes that regulate the protein are not yet well understood. This suggests the need for additional research to better understand the potential protective role it plays at the vascular level.
The investigators did note some limitation of the study, namely that the cross-sectional design did not allow for the establishment of a cause and effect relationship; the study cohort was comprised of only Caucasians; and the use of common antihypertensive, antihyperlipidemic and antidiabetic drugs in patients may have influenced the results.
Nevertheless, the team believes their findings have clinical significance.
“These findings, both basic and clinical, contribute to the current understanding of the shared mechanisms between systemic bone and vascular physiology and pathology,” the researchers concluded. “Thus, our results emphasize the importance of considering the bone-vascular axis when designing therapeutic approaches for the treatment of impaired bone metabolism or vascular diseases.”
A molecule known as resolvin T4 (RvT4) could help treat patients with rheumatoid arthritis-associated atherosclerosis in the future, according to research led by Queen Mary University of London.
Between one and two million people in the U.S. have the degenerative autoimmune joint condition rheumatoid arthritis. Like many autoimmune conditions, people with rheumatoid arthritis have a number of associated health problems including being more susceptible to cardiovascular diseases such as atherosclerosis.
“Atherosclerosis is characterized by the accumulation of lipids, macrophages, and fibrotic elements in the intima of large arteries at sites of low or disturbed flow. This accumulation results in the formation of atherosclerotic plaques that in most cases are silent with limited clinical consequence,” explained Jesmond Dalli, a professor at the William Harvey Institute, Queen Mary University of London, and colleagues in the journal Nature Communications.
“However, in some instances, altered macrophage responses with ensuing excessive lipid accumulation and defective efferocytosis lead to the formation of a necrotic core and a thin fibrous cap. This results in unstable plaques that rupture, causing ischemic cardiovascular disease and even death.”
In this preclinical study, Dalli and colleagues used a mouse model of rheumatoid arthritis to study this kind of atherosclerosis and investigate potential treatments.
Recent research suggests patients with inflammatory conditions such as rheumatoid arthritis have lowered or defective activity of protective “mediator” molecules that normally help to keep excessive immune reactions under control. For example, resolvins such as RvT4. It is thought that these mediator molecules could help prevent or treat conditions such as atherosclerosis.
“The potential relevance of RvTs in regulating vascular disease is supported by findings made in recent studies where administration of highly purified eicosapentaenoic acid, the precursor of n-3 docosapentaenoic acid, together with statins reduced incidence of ischemic events in patients with high triglycerides,” write the authors.
Dalli and team first looked at the role of the larger group of 13-series resolvins (RvTs) in the model mice to assess their function. They found that RvT4 was greatly reduced in animals with rheumatoid arthritis who also had atherosclerosis.
When RvT4 was given to these mice, blood vessel inflammation dramatically decreased. The researchers found this was due to RvT4’s ability to reprogram a type of white blood cell called a macrophage and trigger release of stored lipids from the blood vessel walls.
“The study is important because it identifies for the first time the loss of RvT4 production as a potential new cause of blood vessel inflammation in the context of arthritis, offering a mechanistic explanation on the cause of this important disease in rheumatoid arthritis patients,” said Dalli in a press statement.
“It also showed that RvT4 restores the biological activities of lipid loaded macrophages by promoting lipid breakdown and efflux from the cells, an observation that can guide the development of new treatments to limit the incidence and/or severity of cardiovascular disease in patients with rheumatoid arthritis.”
The spiritual meaning of inflammation is all about the ego, whether it’s righteous, victimized, entitled, or needy.
Typically, the word inflammation is associated with the different ways that bodies respond to their environment. This can include reactions to certain types of food in which allergens are capable of producing an inflammatory or toxic response in the body. Ego is what happens when the personality gets inflamed. For example, when you see someone who is angry, they are in a state of emotional inflammation. To say that they’re in ego may be a true statement, but through the eyes of the Universe, you are able to see how they are having an “allergic reaction” to their conditioned state of being. This means ego is much like an allergy toward the unconsciousness that each of us came here to resolve. When the ego is active, the innocence within you, or within anyone else, exists in an exaggerated manner.
When you start to see ego as the inflammation of the personality, you notice how often you can become “puffed up.” Whether puffed up in righteousness, defensive postures, or in response to the evidence of injustice, an inflamed personality creates an exaggerated perception of life. When living with an allergic reaction to the vibration of the planet, an exaggerated level of consciousness causes you to oscillate between spiritual highs and emotional lows. This can create much suffering until you cultivate love as a potent form of energy medicine to return your personality to its original form.
I’ve come to recognize four basic types of inflammation:
1. Righteous inflammation. It is characterized by an ego structure that feeds on needing to always be right by making others wrong. Even in the presence of one who is saying something totally correct, the ego that is righteously inflamed must make another point in an attempt to be even more right than the other. This type of ego lives to have the upper hand and final word — even if both parties agree on the topic at hand. The theme of righteous inflammation is, “I’m always right.”
2. Victimized inflammation. This is the kind of inflammation in which an ego believes it is always a victim of circumstances. From this perception, even when life seems to be going right, something always happens to turn it upside down. A victimized ego holds very tightly to its judgments, beliefs, and opinions as the reasons their life is regularly in chaos. Whether a belief in light versus dark or pitting good against bad, a victimized ego typically acts as an instigator of turmoil that is guaranteed to be hurt or heartbroken by the way others respond to it. Even if others do not respond at all, a victimized ego uses such feedback to feel invisible or inferior to the world around it.
3. Entitled inflammation. This occurs when a person believes it is their right to have whatever they want, exactly when they want it, even at the expense or to the detriment of others. In entitled inflammation, the ego tends to believe that everyone must fulfill their every whim and demand with little to no regard for the well-being of other people’s experiences. As you can imagine, the theme of an entitled ego is “What about me?” Even when served by others, there is never an end to the requests and demands of an ego that believes it controls the characters in its life.
4. Needy inflammation. In this type of ego, no matter how much attention is received from others, it never feels like enough to be properly filled up. Despite how intently someone listens, there is always a lingering sense of being invisible, unrecognized, undervalued, or unheard. In needy inflammation, it’s easy to feel misunderstood. No matter how much time, interest, and attention you receive from others, it only makes this type of ego hungry for more. Whether active in you or someone you know, needy inflammation can be quite draining for those held in the grip of it.
While you may recognize yourself or others in these descriptions, it is common to embody combinations of those aspects or to flow in and out like the changing of weather patterns. I’ve even seen ego structures that are combinations of all four aspects at once. In each of these aspects of inflammation, there is always a kernel of truth.
By exploring ego in a more heart-centered way, you can have greater patience and compassion throughout your daily encounters. Instead of ridiculing or persecuting the characters within your life, you will be able to see the light of divinity dancing in a play of exaggerated perception. While the ability to see at this level may be limited by an inflamed personality, any amount of time spent incubating in a cocoon of ego prepares you to awaken a greater truth for all.
Corn, or maize, is one of the world’s most widely grown and consumed crops. It is a staple food in many parts of the world, particularly in Latin America, Africa, and parts of Asia. Corn is a highly versatile crop that can be used in a variety of ways, from being eaten fresh, to being processed into flour, oil, and other products.
In terms of its nutritional value, corn is a good source of carbohydrates, fiber, and some key vitamins and minerals. However, the nutritional value of corn can vary depending on the way it is prepared and consumed.
One of the most important things to keep in mind when considering the health benefits of corn is its carbohydrate content. Corn is a high-carbohydrate food, with around 25 grams of carbs per 100 grams of raw corn. This means that it can be a good source of energy, particularly for people who engage in physical activity or have high energy needs.
However, for people who are trying to manage their blood sugar levels or lose weight, corn may not be the best choice. This is because the carbohydrates in corn are mainly in the form of starch, which can cause a rapid increase in blood sugar levels when consumed in large quantities.
In addition to its carbohydrate content, corn is also a good source of fiber. Fiber is an important nutrient that helps to promote healthy digestion and can help to reduce the risk of certain diseases, such as heart disease and diabetes. Raw corn contains around 2 grams of fiber per 100 grams, which is a moderate amount.
Another important aspect of corn’s nutritional value is its vitamin and mineral content. Corn is a good source of vitamin C, thiamin, and folate, all of which are important for maintaining good health. It also contains small amounts of other vitamins and minerals, such as vitamin E, riboflavin, and potassium.
However, it is worth noting that the vitamin and mineral content of corn can be reduced depending on how it is processed and prepared. For example, corn that has been processed into cornmeal or other products may have reduced levels of certain nutrients, such as vitamin C.
Overall, while corn can be a healthy addition to a balanced diet, it is important to consume it in moderation and to choose the right types of corn products. Fresh, unprocessed corn is generally the best choice, as it retains most of its nutritional value and is less likely to contain added sugars or other unhealthy additives.
Casgevy, a one-and-done gene editing cell therapy for patients with the “first molecular disease,” is a triumph but comes with an arduous clinical process and a $2.2 million price tag
There is a certain irony that the first approved CRISPR therapy—a technology barely 10 years old—should be for the genetic disorder that Linus Pauling famously dubbed “the first molecular disease” almost 75 years ago. On December 8, 2023, the U.S. Food and Drug Administration (FDA) approved Casgevy, a groundbreaking CRISPR-based gene editing therapy from Vertex Pharmaceuticals and CRISPR Therapeutics, for sickle cell disease (SCD). The approval was never seriously in doubt, as the therapy—also known as exagamglogene autotemcel, or exa-cel—demonstrated spectacular clinical results dating back to the first patient, Victoria Gray, who was dosed in July 2019.
The FDA also announced approval of another SCD gene therapy, Bluebird Bio’s lentiviral therapy, Lyfgenia. However, that approval comes with a black box warning given the occurrence of rare instances of blood cancers in patients.
“Going from the lab to an approved [CRISPR] therapy in just 11 years is a truly remarkable achievement,” said Nobel laureate Jennifer Doudna, PhD, following news of the United Kingdom’s approval of Casgevy last November. She was especially pleased because the approval helps patients with “a disease that has long been neglected by the medical establishment.”
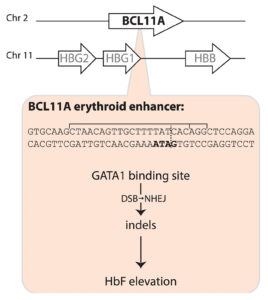
Casgevy, a gene editing treatment made by Vertex Pharmaceuticals and CRISPR Therapeutics, involves the use of CRISPR-Cas9 to inactivate BCL11A expression in the precursors of red blood cells, thus releasing the handbrake on fetal globin expression, which in turn compensates for the sickle cell disease mutation in the β-globin gene. [Fyodor Urnov/The CRISPR Journal]
The Casgevy strategy is to compensate for the SCD mutation in the b-globin gene by restoring expression of fetal hemoglobin (HbF), which is expressed in utero and switched off shortly after birth. The CRISPR-Cas9 scissors is applied in patients’ harvested stem cells to inactivate the BCL11A repressor, which in turn releases the handbrake on HbF expression.
That target was identified some 15 years ago, in foundational genome-wide association studies led by Vijay Sankaran, MD, PhD, Lodish Family Chair in the Division of Hematology/Oncology at Boston Children’s Hospital, and independently by Swee Lay Thein, MD, chief of the sickle cell branch at the National Institutes of Health (NIH).
“This experience underscores a critical lesson—the indispensable role of fundamental discovery science,” Sankaran told GEN. “Without such studies, many of these pivotal advances would remain beyond our reach.” Thein agreed, telling GEN, “This is a major triumph for translational science and a major step toward curative treatment for patients with sickle cell disease. … But let’s not forget the rest of the patients; we still need more small-molecule disease-modifying drugs for patients with sickle cell disease.”
Among other notable reactions to the FDA news was Victoria Gray. “I am crying real tears of joy, and I can’t stop shaking!!,” she posted on LinkedIn. “To all my fellow Sickle Cell Warriors help is here! We will never forget the warriors who we lost along the way! … Our prayers were not in vain! This is only the beginning!!!”
In Tanzania, Julie Makani, MD, PhD, a leading SCD physician-scientist, hailed the news as “a momentous milestone” for SCD, one that would have “a major impact on our approach” to SCD therapeutic interventions. Two decades ago, “the message to patients was that there is no cure for SCD,” she told GEN. “Today, we can tell patients that gene therapy is available for treatment of SCD in the USA and UK.” Makani is leading efforts to expand access to gene therapy for SCD patients in Africa, which is where the SCD mutation first arose more than 7,000 years ago.
A century of hurt
Sickle cell disease affects some 100,000 people in the United States, the vast majority African Americans, and millions more worldwide. A point mutation in the b-globin gene results in the polymerization of the oxygen-carrying hemoglobin protein. That in turn warps the shape of the beautiful, biconcave red blood cells, leading to blocked blood vessels, excruciating pain crises, and the risk of organ damage.
In 1910, Chicago physician James Herrick, MD, published a case report of an unnamed 20-year-old dental student from the Caribbean island of Grenada, who had first been treated in 1904 by a resident, Ernest Irons, MD. Herrick noted the presence of peculiar “pear shaped” red blood cells. Following a few additional case reports over the next decade, Johns Hopkins resident Verne Mason, MD, coined the term “sickle cell anemia” in 1922.
Herrick’s patient was identified decades later by historian Todd Savitt, PhD, as Walter Clement Noel, who arrived in Chicago in 1904 to enroll in dental school. He returned to Grenada to set up his own dental practice in 1907 but died less than a decade later in 1916. Noel is buried in a family grave on Leapers Hill, a famous landmark on the north coast of the island, in a Catholic church cemetery overlooking the ocean.
Walter Clement Noel (1884–1916) was the first person recognized in Western medicine as having suffered from sickle cell disease. He is buried in a cemetery in Sauteurs, Grenada. On the left, a plaque outside the cemetery entrance; on the right, the family grave where Noel is buried with seven relatives.
Two major discoveries occurred in the late 1940s. In 1948, a Long Island pediatrician named Janet Watson, MD, deduced that higher levels of HbF, such as in SCD patients shortly after birth, was correlated with a reduced level of sickling—an important observation that laid the foundation for the CRISPR strategy employed by Casgevy. A year later, Linus Pauling, PhD, demonstrated that SCD was a recessively inherited disease caused by a molecular alteration in hemoglobin.
Seven years later, Vernon Ingram, PhD, working in the same Cavendish Laboratory where Crick and Watson assembled the double helix model of DNA, identified the precise amino acid substitution in b-globin. Around the same time, epidemiological studies in East Africa by Anthony Allison, MD, proved that the incidence of SCD coincided with rates of malaria—a vivid example of heterozygous advantage.
Rewriting the medical system
But despite these and other scientific milestones, the experience of SCD patients has not advanced to the same degree. As the late science journalist Sharon Begley put it: “The U.S. healthcare system is killing adults with sickle cell disease.” And while FDA approval of Casgevy is a moment for celebration, this approach won’t help the vast majority of patients worldwide. As Dhruv Khullar wrote in the New Yorker: “If we truly want to cure sickle cell disease, editing genomes will only get us so far. We’ll need to rewrite our medical system, too.”
Even today, more than a century after the first case report, SCD patients are still subject to profiling and suspicion by hospital staff as they seek pain medications. “There may be no population of patients whose healthcare and outcomes are more affected by racism” than those with SCD, hematologists Alexandra Power-Hays, MD, and Patrick McGann, MD, wrote in the New England Journal of Medicine. Making matters worse, many SCD patients lack basic information and/or access to generic drugs and screening tools that could ward off disease complications.
As the gene and cell therapy field celebrates another approval for precision medicine, we should be ashamed that fewer than one in five children with SCD are prescribed antibiotics or the generic anticancer drug hydroxyurea, which boosts levels of HbF. “To have teenage patients who never heard the word hydroxyurea—that’s preposterous,” McGann declares. There isn’t even a national registry of SCD patients, so no one can say precisely how many individuals are affected.
More than 50 years ago, President Nixon signed the Sickle Cell Control Act, creating new treatment centers and increased funding. But the benefit was short lived. In a study published in 2020, Duke University hematologist John J. Strouse, MD, and colleagues argued that by many metrics, including federal funding, philanthropic support, and new drug approvals, support for SCD lags that afforded cystic fibrosis, even though cystic fibrosis affects roughly one third of the number of patients in the United States as SCD.
A new hope
In August 2022, Pfizer acquired Bay Area biotech Global Blood Therapeutics (GBT) for $5.4 billion. GBT’s small-molecule drug Oxbryta binds to the b-globin molecule and prevents polymerization. Other small-molecule drugs are showing promise in the clinic.
But the value of gene and cell therapy approaches is that they promise “one and done” therapies that do not depend on a relative to donate stem cells. NIH hematologist John Tisdale, MD, who has been treating SCD patients with Bluebird Bio’s lovo-cel, a form of gene therapy that uses a lentiviral vector, was profiled on 60 Minutes two years ago. The program included a comment from former NIH director Francis Collins. He said, “This looks like a cure.”
Meanwhile, Beam Therapeutics and Editas Medicine are also pursuing SCD among their lead gene editing programs. At Boston Children’s Hospital, David Williams, MD, and Erica Esrick, MD, have published promising clinical data treating SCD patients using a short hairpin RNA approach, again targeting the BCL11A pathway.
Taking over the exa-cel program launched by CRISPR Therapeutics, Vertex published the initial exa-cel results in the New England Journal of Medicine in 2021. These represented not only a huge advance in treating SCD but also a crucial early validation of the clinical promise of CRISPR. Fyodor Urnov, PhD, scientific director at the Innovative Genomics Institute, hailed the results as “borderline utopian.”
Writing in The CRISPR Journal, Urnov proposed that Victoria Gray—who has been featured in a series of interviews on National Public Radio since 2019—be added to “the pantheon of names inscribed in golden letters in the history of biomedicine.” That list includes James Phipps (the boy vaccinated by Edward Jenner), Albert Alexander (the first recipient of penicillin), Louise Brown (the first test tube baby) and Emily Whitehead (the pioneering chimeric antigen receptor T-cell patient).
Utopian or not, the positive exa-cel trial results have been extended to dozens of SCD patients, with no reported serious adverse events, although a couple of patients have continued to experience some vaso-occlusive events. The only potential concern among FDA regulators was the possibility of CRISPR-induced off-target effects.
Five weeks ago, an FDA advisory committee meeting assembled a panel of experts to consider this issue. The Vertex investigators, led by chief science officer David Altshuler, MD, PhD, satisfied most of the panel’s lingering concerns about off-target editing and emphasized plans to monitor the long-term health of the exa-cel trial volunteers.
The FDA’s concern is understandable. In August 2022, Graphite Bio, a Bay Area gene editing company co-founded by Stanford University physician-scientist Matthew Porteus, MD, PhD, launched its own SCD gene editing trial. But five months later, the company voluntarily paused the trial after its first patient developed complications. Graphite Bio subsequently halted the trial completely, downsized, and agreed to a reverse merger with LENZ Therapeutics, a biotech company developing ocular therapies. Porteus has since launched a new company, Kamau Therapeutics, and acquired the rights to the SCD program, believing that the adverse events suffered by the first patient were caused by a drug used to treat low platelet counts and unrelated to gene editing.
Long road ahead
Immediately following Casgevy’s approval, Vertex announced a list price of $2.2 million, while Bluebird priced Lyfgenia at $3.1 million. But an ex vivo genome editing protocol that involves toxic chemotherapy, stem cell harvesting, and weeks in hospital is not going to be easily affordable or scalable.
If Gray’s inspiring story is the medical equivalent of the Lindbergh flight across the Atlantic, the next challenge, Urnov says, is to develop the equivalent of “routine, scalable, safe, and reasonably priced affordable air travel in a Dreamliner.” Urnov has been advocating regulatory and organizational incentives to fully realize the clinical potential of gene editing (see his recent video interview on GEN’s “Close to the Edge”).
How will these therapeutic advances be translated to the millions of SCD patients living in Africa, Asia, and beyond? Speaking at GEN’s State of Biotech virtual event in 2022, Doudna predicted that a one-time in vivo delivery approach—without ex vivo manipulation and bone marrow transplantation—would ultimately be achievable. “Is that going to be possible? My answer is yes,” she said. “Is it possible today? No.”
For SCD patients suffering from “the most famous point mutation in genetics,” as Beam’s CEO John Evans calls it, Casgevy is not the end of the journey, merely a long-awaited beginning.


 by time of day; blue shading indicates standard error of the mean. Red shading indicates number of responses (left Y axis) provided at each minute (X axis). Credit: Scientific Reports (2024). DOI: 10.1038/s41598-024-51567-w")
. The speed at which the implosion takes place is typically between 500 and 600 kilometers per second (1.1 to 1.35 million miles per hour). The pressures at the core are up to 80 billion times greater than atmospheric pressure. Credit: University of Rochester Laboratory for Laser Energetics photo / Eugene Kowaluk")