New gene-editing approach to studying immune gene function could improve treatments for cancer, other diseases
Over the past two decades, the immune system has attracted increasing attention for its role in fighting cancer. As researchers have learned more and more about the cancer-immune system interplay, several antitumor immunotherapies have become FDA-approved and are now regularly used to treat multiple cancer types.
Yet despite these advances, much remains unknown about how the immune system fights cancer — and about immunity in general, said Martin LaFleur, a postdoctoral fellow in the laboratory of Arlene Sharpe, chair of the Department of Immunology in the Blavatnik Institute at Harvard Medical School.
CRISPR-based gene editing, in which scientists modify the genome using a tool developed just over a decade ago, has become a mainstay of biological discovery, providing relatively quick insight into the function of individual genes and targets for new therapies.
However, LaFleur said, this approach is not without challenges. Chief among them is that it is hard to modify immune cells without changing their biology, which hampers the ability to study immune cell behavior in its full complexity in a living organism.
Now, LaFleur, Sharpe, and their team have succeeded in bypassing this hurdle by deploying CRISPR in a new way to study the function of immune genes.
Their work, described in two papers — one in Nature Immunologyand one in the Journal of Experimental Medicine — could eventually yield insights about cancer immunology as well as about other diseases driven by immune system dysfunction.
Harvard Medicine News spoke with LaFleur about what this advance means for the future of immunology research.
Harvard Medicine News: Let’s set the stage with a refresher on how CRISPR works.
LaFleur: Programmable CRISPR-based gene editing was developed in 2012 and became such a powerful tool for biologic research that its discoverers won the Nobel Prize in Chemistry in 2020.
The CRISPR gene-editing system uses an enzyme called Cas-9 that acts like a pair of molecular scissors that cuts both strands of DNA and in doing so disrupts or knocks out the function of a gene. To select the gene to knock out, this system uses a complementary piece of RNA that matches the gene and acts as a guide. It’s a very flexible approach for very quickly knocking out and studying the function of almost any gene you want.
HMNews: How is CRISPR used to understand the immune function of genes?
LaFleur: Immune cells interact with a lot of other cell types that can’t be modeled well in petri dishes, so we prefer immune studies to happen inside a living organism like a mouse — a far more reliable way to capture the complexity of cell-to-cell interactions as they occur in the body rather than in a lab dish. CRISPR editing inside the body is difficult, so immune cells typically need to come out and be modified using this tool in a petri dish. The edited cells are then put back into the body.
However, only certain immune cell types can be incorporated efficiently when transferred back into a mouse. Also, the actual process of manipulating immune cells in a dish can change their biology, so you may not be studying what you actually want to study once they’re removed from the body.
Also, CRISPR had been used only to turn off a single gene at a single time in immune cells. But our cells contain thousands of genes, so what if we want to knock out multiple genes in different cell types at different times in the same animal? This would provide greater insight into the complexities of genes and their interactions in immune cells over time.
HMNews: How does your new study address these challenges?
LaFleur: We decided to take a completely different approach for using CRISPR. Rather than directly modify the immune cells we’re interested in, we modified their precursors, the stem cells found in bone marrow that produce all immune cells. We removed those from mice and used CRISPR to knock out the genes we were interested in, and then replaced these stem cells in mice whose native bone marrow stem cells had been removed. We call this system CHimeric IMmune Editing, or CHIME.
In an earlier study, we used CHIME to knock out a gene called Ptpn2, which has shown some promise for cancer immunotherapy, one of the focuses of the Sharpe Lab. When we deleted that one gene in a subset of immune cells known as CD8+ T cells, they became better cancer fighters.
With our Nature Immunologystudy, we wanted to see if we could modify CHIME and make it both more precise and more versatile. We used it to knock out two genes at once in several different cell types, we deployed it to target genes specifically in a single cell type, we used CRISPR to disrupt genes in modified cells once they were already back inside the animal, and we also used it to knock out two different genes at different points in time.
We used different tactics, such as packaging multiple guide RNAs together and using a trick that disables genes only under certain circumstances, such as when mice receive a drug. We were able to demonstrate that each of these strategies is feasible.
HMNews: What is your ultimate goal with this research?
LaFleur: Our ultimate goal is to better understand the immune system, particularly in its capacity to fight cancer. We want to encourage strong anticancer immunity — meaning we want to optimize how immune cells fight tumors — but also want spare healthy cells and tissues from the immune attack. This requires a very nuanced calibration of the immune system and can be a tricky balance.
Moreover, the benefits could extend beyond cancer and be applied to many other diseases driven by the immune system, including autoimmune conditions.
HMNews: What are your next steps?
LaFleur: We just published a second paper in the Journal of Experimental Medicine that lays out a framework for the field in studies using CRISPR to screen immune gene function in living animals. Central to our framework is adding a genetic “barcode” to CRISPR-edited immune cells so we can track them as they multiply and spread within animals.
We’re hoping that this framework and CHIME will give researchers new tools to study immune cells in cancer or any other disease model of their choice, eventually leading to new immune-centered therapies.
The gene-editing technique CRISPR disabled HIV that lay dormant in immune cells in a lab experiment, raising hopes for an eventual cure
An electron micrograph of HIV, which currently requires lifelong medication
A new way to eradicate HIV from the body could one day be turned into a cure for infection by this virus, although it hasn’t yet been shown to work in people.
The strategy uses a relatively recent genetic technique called CRISPR, which can make cuts in DNA to introduce errors into viral genetic material within immune cells. “These findings represent a pivotal advancement towards designing a cure strategy,” researcher Elena Herrera Carrillo at the University of Amsterdam in the Netherlands said in a statement.
While infection with HIV was once nearly always fatal, those with the virus can now take drugs that stop it from reproducing. This gives them a nearly normal lifespan, as long as they diligently take their medicines every day.
But when people are first infected, some of the virus inserts its DNA into their immune cells, where it stays dormant. If they stop taking their HIV medicines, this DNA “reawakens” and the virus starts spreading through their immune systems again.
For a cure, we need some way of killing any dormant virus in the body. Several strategies have been tried, but none has so far been found to work.
The latest approach uses a gene-editing system called CRISPR. Originally discovered in bacteria, this homes in on a specific DNA sequence, making cuts in it. By changing the DNA sequence being targeted, the system can potentially be turned into a form of gene therapy for many conditions, with the first such treatment having been approved last year in the US and UK as a cure for sickle cell anaemia.
Several groups are investigating using CRISPR that targets a gene in HIV as a way of disabling dormant virus. Now, Carrillo and her team have shown that, when tested on immune cells in a dish, their CRISPR system could disable all virus, eliminating it from these cells. The work is due to be presented at the European Congress of Clinical Microbiology and Infectious Diseases in Barcelona, Spain, next month.
Jonathan Stoye at the Francis Crick Institute in London says that although the results are encouraging, the next step is trials in animals and eventually people to show the treatment can reach all the immune cells with dormant HIV. Some of these cells are thought to reside in bone marrow, but there may be other body sites involved too, he says. “There’s still a fair amount of uncertainty about whether there are other reservoirs in other parts of the body,” he says.
Two RNA-editing therapies for genetic diseases have in the past few months gained approval for clinical trials, raising hopes for safer treatments.
Tools to edit messenger RNA (artist’s illustration) are touted as being safer and more flexible than the CRISPR–Cas9 system, which changes the genome itself.
RNA editing is gaining momentum. After decades of basic research into how to manipulate this complex molecule, at least three therapies based on RNA editing have either entered clinical trials or received approval to do so. They are the first to reach this milestone.
Proponents of RNA editing have long argued that it could be a safer and more flexible alternative to genome-editing techniques such as CRISPR, but it poses substantial technical problems.
The launch of human trials signals the growing maturity and acceptance of the field, scientists say. “There’s a much greater understanding of RNA technology, and that’s been partially enhanced by the RNA vaccine and the COVID pandemic,” says Andrew Lever, a biologist at the University of Cambridge, UK. “RNA is now seen as a very important therapeutic molecule.”
Temp job
RNA has a crucial role in protein synthesis: the genetic information encoded in DNA is transcribed into messenger RNA (mRNA) before being translated into proteins. RNA molecules are composed of building blocks called nucleotides, each containing one of four bases, or letters.RNA therapies explained
RNA-editing techniques aim to compensate for harmful mutations by changing the sequence of RNA, allowing normal proteins to be synthesized. RNA editing can also increase the production of beneficial proteins.
Unlike CRISPR genome editing, RNA editing doesn’t change genes. Nor does it introduce permanent changes, because RNA molecules are transient. This means that the duration of the therapeutic effect could be shorter.
But that transience could offer safety advantages. One risk of CRISPR therapies is off-target effects, or unintended changes outside the target genomic region, notes Joshua Rosenthal, a neurobiologist at the Marine Biological Laboratory in Woods Hole, Massachusetts. “An off-target effect in DNA is potentially quite dangerous. In RNA, it’s less so, because it’s going to turn over.”
One letter at a time
One common RNA-editing approach, single-base editing, harnesses an enzyme that is already found in cells: adenosine deaminase acting on RNA (ADAR). This enzyme swaps a base called adenine in the RNA sequence for a base called an inosine.
Wave Life Sciences in Cambridge, Massachusetts, is exploring single-base editing to treat a genetic disorder called alpha-1 antitrypsin deficiency (AATD), which can damage the lungs and the liver. The disease reduces the production of AAT, a protein made in liver cells that protects lungs from damage caused by inhaling polluted air or other irritants.
Wave’s product is a short chain of nucleotides that directs naturally occurring ADAR enzymes to change a specific letter in each mRNA molecule to correct the mutation that affects AAT production. “By using the cell’s endogenous machinery to edit that single base, you now make a normal protein. And we’ve shown that the normal protein can be expressed at high levels,” says Paul Bolno, Wave’s president and chief executive.
In mice, the drug edited around 50% of the target mRNA in liver cells, which is enough to produce therapeutic effects, Bolno says.
The company’s clinical trial of the drug began last December in the United Kingdom and Australia, and will evaluate the drug’s safety and other features.
Editing whole paragraphs
Another approach, called RNA exon editing, changes thousands of genetic letters in an RNA molecule at once, as opposed to changing just one letter. Exon editing is akin to editing a whole paragraph instead of correcting one typo, says Lever. This technology is particularly important for disorders caused by multiple mutations in a person’s genome; such arrays of mutations are difficult to address with single-base changes, he adds.
The technique targets pre-mRNA, which is transcribed from DNA and then processed to make mRNA. Pre-mRNA includes both exons — parts of the RNA transcript that contain instructions for making proteins — and introns, which don’t contain such instructions. Through a mechanism called RNA splicing, the introns are cut out of the pre-mRNA, and the exons are stitched together to form the final mRNA, which is translated into protein.Collect more data from Africa to improve gene therapy
Companies such as Ascidian Therapeutics in Boston, Massachusetts, are leveraging the RNA-splicing process to remove mutation-containing exons and replace them with healthy ones. Last month, Ascidian received approval from the US Food and Drug Administration for a clinical trial of an exon editor to treat Stargardt disease, which causes vision loss. People with the disease have several mutations in a single gene, leading to the production of a defective protein that normally protects the retina.
Ascidian’s therapy relies on an engineered DNA segment that is delivered into cells and produces normal RNA exons. These replace the mutated ones during the splicing process, resulting in functional proteins. The DNA also produces RNA sequences that facilitate exon editing.
“With one molecule, [the therapy] is able to replace 22 exons at one time,” says biologist Robert Bell, head of research at Ascidian.
Cancer-quashing RNA
The potential of RNA-based therapies is not limited to genetic diseases. Rznomics, a biopharmaceutical company in Seongnam, South Korea, is testing an RNA editor to treat hepatocellular carcinoma, the most common type of liver cancer. In September 2022, the company started a clinical trial in South Korea, which it intends to expand internationally.
Rznomics’s approach involves mRNA splicing — but, unlike Ascidian’s method, it doesn’t use the cell’s own splicing machinery. Instead, the company co-opted a naturally occurring ribozyme, an RNA molecule that can induce splicing in target regions of mRNA. Researchers engineered the ribozymes to cut open mRNAs in tumour cells and insert a lethal cargo: an RNA sequence that is translated into a protein that generates a toxin that induces cell death. When surrounding cancer cells come into contact with these cells, the toxin spreads, promoting their death as well. This therapeutic molecule replaces an RNA sequence that is associated with tumour growth.
The use of the splicing approach against more than one disease is very exciting, says Lever, who is also the chief medical officer of Spliceor in Cambridge, UK, a firm that is working on RNA-splicing therapies. “It opens up a whole new range of possibilities of treatment for things which otherwise can’t be treated.”
Scientists introduced CRISPR to the world as a gene-editing tool in summer 2012, when landmark papers from two independent groups demonstrated how the system could be wielded to make cuts in DNA. Now, less than 12 years later, we’re seeing CRISPR put to use in groundbreaking medical treatments.
“It’s really rewarding to see how fast the fundamental discoveries that were made in the lab actually are translated into the clinics,” said Šikšnys, who is chief scientist and head of the Department of Protein-DNA Interactions at the Vilnius University Institute of Biotechnology in Lithuania.
Prior to those seminal papers, other researchers had begun unraveling how CRISPR works inside microbes. Although best known as a gene-editing tool, CRISPR was first found in bacteria, and scientists realized that it acts as a kind of immune system — a defense against viruses. In this immune system, the bacterium has a memory bank full of virus’ genetic material. The bacterium will stash away this material after being attacked by a virus so it can guard against future invasions.
This memory bank is paired with tiny, molecular scissors called Cas proteins that snip through DNA, and a molecule that guides the scissors to their target. In bacteria, that target is a viral invader. But Šikšnys and his colleagues demonstrated that scientists could co-opt these scissors for their own purposes, targeting any DNA they want to edit. They specifically showed this with the protein Cas9.
Live Science spoke with Šikšnys about what it’s been like to see CRISPR enter clinical use and how he thinks the system might be applied and improved upon in the future.
Šikšnys studies the diversity of CRISPR systems found in nature. (Image credit: Vilnius University)
Nicoletta Lanese: Could you describe when you first began working with CRISPR-Cas? And could you give a sense of when you clued into the idea that this could be “a big deal” — a big-ticket technology that kind of shifts gene-editing as we know it?
Virginijus Šikšnys: We jumped into the CRISPR field, I would say, from the very beginning. It happened probably in 2007 when a paper appeared in Science, describing for the first time the possible function of the CRISPR-Cas system as an antiviral defense system in bacteria. And we decided to look, actually, at how this system functioned. This is how we started our CRISPR journey.
Of course, in the very beginning, we were very much interested in very basic biological questions. … It took us a while to understand the mechanisms behind the CRISPR-Cas systems. …
In [our 2012] paper, we showed that we can reprogram Cas9 protein and address it to any sequence in the genome. This was probably the moment where we understood that, indeed, this is a kind of really versatile system that could be employed for genome editing in different model organisms. And this is how, then, this kind of gene-editing field started.
NL: Did you envision right away that this might be applied in the treatment of genetic disorders? Did you see that as a possibility, even early on?
VS: If I recall, what we put in our paper at that time — we said that these CRISPR-Cas systems, or Cas9 protein programmed by CRISPR RNA, could be used for precise “DNA surgery.”
It means that, actually, you can direct Cas9 to any sequence in the genome, including the sequences where [there are] mutations that cause genetic disease.
NL: Having seen, within the last year, the first CRISPR-based therapies come to market — I’m wondering how it feels to have seen the progression of the field from that basic research to now seeing it applied at that level?
VS: Indeed, looking backwards, it’s really amazing to see that Cas9 made it into the clinics, nearly, in 10 years. I think it’s a really great achievement, and I’m sure that more therapeutic applications will follow in the near future and will provide cure[s] for genetic diseases that were incurable before.
And if you look at the list of clinical trials that are currently ongoing, where the Cas9 genome-editing tool is employed to treat different genetic diseases — the list is really very impressive. And it’s really rewarding to see how fast the fundamental discoveries that were made in the lab actually are translated into the clinics.
CRISPR-Cas9 system uses Cas9 as molecular scissors and an RNA molecule as a guide for those scissors. (Image credit: VectorMine via Getty Images)
NL: Having seen the graduation into the clinic now, how do you anticipate the gene-editing systems borne of CRISPR-Cas might be refined in the future?
VS: Indeed, the CRISPR-Cas9 technology is a great tool that is rapidly advancing into the clinics. But still, there are several challenges that need to be overcome, and there are, of course, avenues for improvement of this tool. …
Recently, it made headlines that that CRISPR tool was used for treatment of SCD disease [sickle-cell disease]. In fact, [it] showed that this is really a tool that could be used in the clinics for the treatment of the patients.
But of course, this treatment has several limitations, because, in this case, the treatment is occuring ex vivo. It means that the cells that need to be treated are removed from the patient’s body, then Cas9 tool is applied to correct the mutation — or actually, trigger production of fetal hemoglobin. And then these engineered cells, they have to be delivered back to the patient’s body. And of course, this is kind of a challenging and time-consuming procedure.
So of course, it would be great if the CRISPR treatment could be done directly in [the] human body — we call it in vivo. But actually, to do that, you have to overcome several challenges: First, you have to deliver this CRISPR tool into specific tissues or organs in human body. And of course, there are many ways to deliver CRISPR tools, but after COVID, mRNA vaccines were approved as a therapeutic modality for treatment [prevention] of COVID. And currently, mRNA coupled with lipid nanoparticles became one of the key modalities that could deliver Cas9 into different cells and tissues in a human body.
[Other] delivery systems are also [being] explored, including virus-like particles and adeno-associated viruses. So AAVs are also used as delivery tools and they are approved as safe delivery tools into human body — but, for example, in the case of AAV, there is a packaging cargo limitation and you need to find smaller gene editing tools that could be packaged into a single AAV particle.
In my lab, in fact, we are looking at the avenues — how do you improve the existing tools or, actually, find new tools? To find new tools, we look at the diversity of CRISPR-Cas systems. These CRISPR-Cas systems [in nature] are very, very diverse, and we aim to understand this diversity of CRISPR-Cas systems from a fundamental perspective. And also, we hope that, looking at this diversity, we’ll be able to find new tools for genome editing applications.
NL: Could you paint a picture of what it looks like to dig into the diversity of these systems?
VS: In my lab, we’re using a combined bioinformatics-based, biochemical approach. So we try to identify putative new CRISPR-Cas systems bioinformatically, and then, we try to characterize them biochemically using the tools available in the wet lab. …
First, we look at [microbial DNA] sequences that are present in really huge databases — you can just try to find new CRISPR systems there. Then, we try to express them in different bacteria, isolate them, characterize, and then move them to human cells to see whether they can be applied as new genome modification tools.
NL: We touched on the sickle cell treatments that have just been approved — I’m wondering if you, like others, anticipated that sickle cell would be one of the first diseases to get a CRISPR treatment? And what diseases do you see as the next frontier?
VS: I would say that it was clear from the very beginning that genetic diseases that are caused by a single mutation, like sickle-cell disease, will be the first target. It looked like low-hanging fruit, because you have to correct just a single mutation in the genome. And of course, I think part of the credit for this Cas9-based treatment of sickle-cell disease should also go toward the people who were studying sickle-cell disease for decades. They were providing us with understanding of the mechanisms of the disease that were harnessed into the treatment.
The other reason why SCD was a clear target was because, as I mentioned before, you can do the treatment [ex] vivo. You can remove cells that contain [the] mutation, actually engineer them in the lab, and put the cells back into human body. So that makes manipulations easier.
But of course, when you think about the next step — treatment of genetic diseases that are caused by multiple mutations, like cancer, for example, is still a challenge. But of course, scientists are trying to develop approaches how to tackle such complex genetic disease. And, for example, T-cell-based therapies are already in the clinics, and CRISPR [systems] are used there to facilitate engineering of these T cells … that could be used to treat cancers like lymphomas and solid tumors.
And of course, the CRISPR treatments in the human body, as I discussed before, is the next big step.
The beauty of CRISPR-Cas9 technology is that it’s a kind of versatile, or universal technology, because you can use this tool to engineer any living organism.Virginijus Šikšnys, Vilnius University
NL: This is somewhat tangential, but we’ve covered the idea of developing CRISPR as an antibacterial, as a kind of alternate antibiotic — do you see that as a fruitful research area?
VS: The beauty of CRISPR-Cas9 technology is that it’s a kind of versatile, or universal technology, because you can use this tool to engineer any living organism. You are just trying to engineer DNA, and DNA is the blueprint of every living organism. So instead of doing gene-editing in human cells, you can also think about doing editing of bacterial population — let’s say, that are present in [the] human gut. And these bacterial populations could be engineered. …
And as you mentioned, Cas9, CRISPR technologies could be used also as antiviral agents. Currently, the problem with antibiotics is pretty clear — we are probably losing our battle against bacteria using antibiotics. Novel antibiotics are always required and it’s really difficult to find them, and challenging and costly. So therefore, alternative technologies like viral therapies or CRISPR antibacterial systems are developed.
NL: Obviously CRISPR has so much potential, especially in the realm of treating genetic disease — I think people also have a lot of questions about the ethics of applying CRISPR in different contexts. Could you speak on that?
VS: I think it’s a very important question, and of course, CRISPR is a very important technology, and you can use CRISPR to do many things. But of course, you should keep in mind what you are doing and you need to be in touch and in conversation with society — Are these things acceptable? Or, what are the societal views on these technologies that scientists are developing in the lab? And I think it’s very important to communicate with people and explain, actually, what are these technologies, what they can achieve, and then what can be downsides, also, of these technologies.
We already heard about these stories that CRISPR was used several years ago in China for engineering human embryos — so that’s a line that scientists actually agree not to cross, because this could be a really dangerous thing.
Scientists are seeking FDA approval to bring the edited pigs to market.
Using CRISPR-Cas9 technology, British animal genetics firm Genus has generated a population of pigs that are resistant to the deadly PRRSV infection. [Genus]
CRISPR-based genome editing has already been successfully applied to sickle cell disease and additional companies are working on developing their CRISPR-based therapeutics. It seems only natural that the technology would make its way to animals. Now a team of scientists at Genus, a British animal genetics company with research facilities in Wisconsin and Tennessee, have developed a new generation of CRISPR-edited pigs that are resistant to porcine reproductive and respiratory syndrome (PRRS) virus, a disease that has had a widespread impact on porcine populations around the world for decades.
The Genus team describes a scaled gene editing program that introduced “a single modified CD163 allele into four genetically diverse, elite porcine lines.” The work produced healthy pigs that “resisted PRRS virus infections as determined by macrophage and animal challenges.” Edited pigs showed “no signs of infection or viral replication in lung and lymph node tissue when challenged with PRRSV.” The Genus team believes this is potentially the first integration of CRISPR gene editing into a livestock breeding program and could completely eliminate a major infectious disease in swine.
“This is a milestone study illustrating the potential of CRISPR-based technologies for commercial livestock breeding,” said Rodolphe Barrangou, PhD, professor of food, bioprocessing, and nutrition sciences at North Carolina State University and editor-in-chief of The CRISPR Journal. “A commercially-relevant proof of concept that genome editing can be used to generate healthy PRRS-resistant pigs that are otherwise indistinguishable from the parent population sets the stage for deploying that approach for other diseases and traits of commercial interest.”
“They were able to generate in a couple of generations a founder population of breeding boars (10–15 per line) and gilts to serve as a gene edited nucleus herd for ultimate commercial pork production and sale using classical breeding,” said Alison Van Eenennaam, PhD, an extension specialist in animal genomics and biotechnology in the department of animal science at the University of California, Davis. “There are more sophisticated approaches to guarantee the edited allele is in a homozygous state and absent off-target indels in all animals produced, e.g., using edited porcine embryonic stem cells, but at the end of the day the approach they used did the job.”
Genus works on improving the genetics of livestock to ensure healthy, robust pigs and cattle for agricultural production, Elena Rice, PhD, Genus’ CSO and head of research and development and a co-author on the paper told GEN. “Livestock have a lot of diseases, and there are several that [are] just really devastating for farmers,” Rice said. Until the recent emergence of African swine flu, PRRS infections topped that list.
Murky beginnings
Also known as blue-ear pig disease, the first PRRS cases in the United States were reported in 1987. While the exact origins of the virus are murky, its impact is all too clear. The disease is now found in pig production facilities around the world, accounting for the death of as much as 20% of livestock produced annually. Its impact is environmental, psychological, and personal—not to mention economically devastating for the swine industry. By some estimates, annual losses in the United States exceed $600 million.
Multiple vaccines have been developed to stop the spread of PRRS, but with limited effectiveness, according to Rice. As explained in the paper, the PRRS virus has “a high rate of mutation due to an error-prone viral RNA-dependent RNA polymerase and a significant rate of genetic recombination.”
Vaccines are typically administered when the pigs are already showing symptoms, but by then it is often too late to save them. Even if the pigs survive the infection, their immune systems are usually too weak to combat secondary infections like pneumonia that can develop. Just a few infected pigs are enough to decimate an entire herd. Attempts to breed PRRS-resistant pig populations have also not worked out well to date.
Alongside breeding efforts, scientists in academia have also studied the genetic basis for PRRS infections. It turns out that several genes are involved in viral infection, including CD163, which encodes the entry receptor for the virus. In pigs, this particular protein is expressed on the surface of macrophages and monocytes and mediates inflammation among other functions.
Genus’ work builds on the research into the role of CD163. “We had some evidence from university studies that we could edit a single host gene to confer resistance,” Brian Burger, PhD, senior research manager at Genus and first author on The CRISPR Journal paper, told GEN. “The challenge was: how do you go from that proof of concept work to a commercial breeding program?” It seemed like the ideal opportunity to bring CRISPR technology to bear on animal disease.
CRISPR’s efficiency also made it the right fit for editing animals. Finding the right edit for a gene without introducing dangerous off-target effects requires a lot of trial and error. “Ethically and morally, it’s very important [that] we designed the whole process so that we eliminate unnecessary production of animals,” Rice told GEN.
Farm to table?
To edit the genomes, the Genus scientists injected CRISPR-Cas9 editing reagents into the genomes of pig zygotes. Their goal was to make a precise deletion in CD163 that removed a single exon encoding the domain that directly interacts with the virus. Importantly, the edit did not impact CD163’s function in the new population. They also genotyped the edited animals to ensure that the edit was consistent across the animals, there were no unforeseen off-target effects, and there was enough genetic diversity within the potential breeding population. Edited pigs that passed muster were then moved through the breeding process to establish a population of pigs that are PRRS-resistant. The paper also covers details of how the team optimized their editing reagents to ensure that their work would translate to a commercial breeding program, Burger added.
The repercussions of this work could be major. Genus is not the only company working on PRRS by targeting CD163. But Genus certainly hopes to be the first to market with its edited pigs. It has its sights set on getting the edited pigs through the FDA’s regulatory process.
Rice told GEN that the company is also working with regulatory agencies in other countries to seek broader approval as well. “Everything is going well, but it’s just a long process,” she said. ”The FDA is making a lot of effort to create a much better environment for gene editing [in livestock]. We’re learning together as we go through the process.”
Barrangou noted that “regulatory approval will be critical” and that “there are already established Ag-relevant frameworks for crops, notably in the U.S. and very recently in the EU that set the stage and precedence.” Furthermore, “the enthusiasm related to last week’s EU vote on the use of new genomic techniques and plant breeding technologies in Ag” makes the publication of this study “very timely and encouraging,” he added.
Van Eenennaam has some reservations about the approval process in the United States. “The United States FDA is alone in the world in regulating ‘intentional’ genetic alterations including single base pair deletions as an animal drug, and requiring a ‘new animal drug’ approval for commercialization. This expensive regulatory path is basically a non-starter for smaller companies,” she told GEN in an email.
Furthermore, “Until the pigs are approved, they are all considered unsalable new animal drugs and therefore cannot enter commerce or the food supply,” she added. “That means all of the 435 edited pigs produced in the paper in the development and testing process need to be incinerated, composted, or buried. Such a multiyear endeavor requires very deep pockets.” And the road to approval will likely be quite long. She pointed to the multi-year approval timeframe that was required for the genetically engineered AquAdvantage salmon as an example of just how long the process can be.
But regulatory approval is just the first hurdle. Genus scientists hope their pigs will be widely disseminated in the livestock industry to stop losses due to PRRS. Building PRRS-resistant piglets requires two gene-edited parents. Genus plans to sell aliquots of semen from gene-edited males to breeders who could use it to begin breeding programs that ultimately produce PRRS-resistant pigs after a few generations.
If all goes well, the public could be faced with the choice of eating pork from gene-edited animals. Historically, the conversation around the production and consumption of genetically modified foods has been very polarizing. But the public response in this case may not follow historical trends given the central reason for the gene editing in the first place. Early consumer research conducted by Genus indicates that consumers are more open to CRISPR-edited foods when there is a good reason for the genetic modification. Given the impact PRRS has had on the livestock industry, there is a clear benefit here, Rice said.
Casgevy, a one-and-done gene editing cell therapy for patients with the “first molecular disease,” is a triumph but comes with an arduous clinical process and a $2.2 million price tag
There is a certain irony that the first approved CRISPR therapy—a technology barely 10 years old—should be for the genetic disorder that Linus Pauling famously dubbed “the first molecular disease” almost 75 years ago. On December 8, 2023, the U.S. Food and Drug Administration (FDA) approved Casgevy, a groundbreaking CRISPR-based gene editing therapy from Vertex Pharmaceuticals and CRISPR Therapeutics, for sickle cell disease (SCD). The approval was never seriously in doubt, as the therapy—also known as exagamglogene autotemcel, or exa-cel—demonstrated spectacular clinical results dating back to the first patient, Victoria Gray, who was dosed in July 2019.
The FDA also announced approval of another SCD gene therapy, Bluebird Bio’s lentiviral therapy, Lyfgenia. However, that approval comes with a black box warning given the occurrence of rare instances of blood cancers in patients.
“Going from the lab to an approved [CRISPR] therapy in just 11 years is a truly remarkable achievement,” said Nobel laureate Jennifer Doudna, PhD, following news of the United Kingdom’s approval of Casgevy last November. She was especially pleased because the approval helps patients with “a disease that has long been neglected by the medical establishment.”
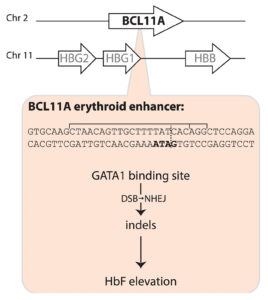
Casgevy, a gene editing treatment made by Vertex Pharmaceuticals and CRISPR Therapeutics, involves the use of CRISPR-Cas9 to inactivate BCL11A expression in the precursors of red blood cells, thus releasing the handbrake on fetal globin expression, which in turn compensates for the sickle cell disease mutation in the β-globin gene. [Fyodor Urnov/The CRISPR Journal]
The Casgevy strategy is to compensate for the SCD mutation in the b-globin gene by restoring expression of fetal hemoglobin (HbF), which is expressed in utero and switched off shortly after birth. The CRISPR-Cas9 scissors is applied in patients’ harvested stem cells to inactivate the BCL11A repressor, which in turn releases the handbrake on HbF expression.
That target was identified some 15 years ago, in foundational genome-wide association studies led by Vijay Sankaran, MD, PhD, Lodish Family Chair in the Division of Hematology/Oncology at Boston Children’s Hospital, and independently by Swee Lay Thein, MD, chief of the sickle cell branch at the National Institutes of Health (NIH).
“This experience underscores a critical lesson—the indispensable role of fundamental discovery science,” Sankaran told GEN. “Without such studies, many of these pivotal advances would remain beyond our reach.” Thein agreed, telling GEN, “This is a major triumph for translational science and a major step toward curative treatment for patients with sickle cell disease. … But let’s not forget the rest of the patients; we still need more small-molecule disease-modifying drugs for patients with sickle cell disease.”
Among other notable reactions to the FDA news was Victoria Gray. “I am crying real tears of joy, and I can’t stop shaking!!,” she posted on LinkedIn. “To all my fellow Sickle Cell Warriors help is here! We will never forget the warriors who we lost along the way! … Our prayers were not in vain! This is only the beginning!!!”
In Tanzania, Julie Makani, MD, PhD, a leading SCD physician-scientist, hailed the news as “a momentous milestone” for SCD, one that would have “a major impact on our approach” to SCD therapeutic interventions. Two decades ago, “the message to patients was that there is no cure for SCD,” she told GEN. “Today, we can tell patients that gene therapy is available for treatment of SCD in the USA and UK.” Makani is leading efforts to expand access to gene therapy for SCD patients in Africa, which is where the SCD mutation first arose more than 7,000 years ago.
A century of hurt
Sickle cell disease affects some 100,000 people in the United States, the vast majority African Americans, and millions more worldwide. A point mutation in the b-globin gene results in the polymerization of the oxygen-carrying hemoglobin protein. That in turn warps the shape of the beautiful, biconcave red blood cells, leading to blocked blood vessels, excruciating pain crises, and the risk of organ damage.
In 1910, Chicago physician James Herrick, MD, published a case report of an unnamed 20-year-old dental student from the Caribbean island of Grenada, who had first been treated in 1904 by a resident, Ernest Irons, MD. Herrick noted the presence of peculiar “pear shaped” red blood cells. Following a few additional case reports over the next decade, Johns Hopkins resident Verne Mason, MD, coined the term “sickle cell anemia” in 1922.
Herrick’s patient was identified decades later by historian Todd Savitt, PhD, as Walter Clement Noel, who arrived in Chicago in 1904 to enroll in dental school. He returned to Grenada to set up his own dental practice in 1907 but died less than a decade later in 1916. Noel is buried in a family grave on Leapers Hill, a famous landmark on the north coast of the island, in a Catholic church cemetery overlooking the ocean.
Walter Clement Noel (1884–1916) was the first person recognized in Western medicine as having suffered from sickle cell disease. He is buried in a cemetery in Sauteurs, Grenada. On the left, a plaque outside the cemetery entrance; on the right, the family grave where Noel is buried with seven relatives.
Two major discoveries occurred in the late 1940s. In 1948, a Long Island pediatrician named Janet Watson, MD, deduced that higher levels of HbF, such as in SCD patients shortly after birth, was correlated with a reduced level of sickling—an important observation that laid the foundation for the CRISPR strategy employed by Casgevy. A year later, Linus Pauling, PhD, demonstrated that SCD was a recessively inherited disease caused by a molecular alteration in hemoglobin.
Seven years later, Vernon Ingram, PhD, working in the same Cavendish Laboratory where Crick and Watson assembled the double helix model of DNA, identified the precise amino acid substitution in b-globin. Around the same time, epidemiological studies in East Africa by Anthony Allison, MD, proved that the incidence of SCD coincided with rates of malaria—a vivid example of heterozygous advantage.
Rewriting the medical system
But despite these and other scientific milestones, the experience of SCD patients has not advanced to the same degree. As the late science journalist Sharon Begley put it: “The U.S. healthcare system is killing adults with sickle cell disease.” And while FDA approval of Casgevy is a moment for celebration, this approach won’t help the vast majority of patients worldwide. As Dhruv Khullar wrote in the New Yorker: “If we truly want to cure sickle cell disease, editing genomes will only get us so far. We’ll need to rewrite our medical system, too.”
Even today, more than a century after the first case report, SCD patients are still subject to profiling and suspicion by hospital staff as they seek pain medications. “There may be no population of patients whose healthcare and outcomes are more affected by racism” than those with SCD, hematologists Alexandra Power-Hays, MD, and Patrick McGann, MD, wrote in the New England Journal of Medicine. Making matters worse, many SCD patients lack basic information and/or access to generic drugs and screening tools that could ward off disease complications.
As the gene and cell therapy field celebrates another approval for precision medicine, we should be ashamed that fewer than one in five children with SCD are prescribed antibiotics or the generic anticancer drug hydroxyurea, which boosts levels of HbF. “To have teenage patients who never heard the word hydroxyurea—that’s preposterous,” McGann declares. There isn’t even a national registry of SCD patients, so no one can say precisely how many individuals are affected.
More than 50 years ago, President Nixon signed the Sickle Cell Control Act, creating new treatment centers and increased funding. But the benefit was short lived. In a study published in 2020, Duke University hematologist John J. Strouse, MD, and colleagues argued that by many metrics, including federal funding, philanthropic support, and new drug approvals, support for SCD lags that afforded cystic fibrosis, even though cystic fibrosis affects roughly one third of the number of patients in the United States as SCD.
A new hope
In August 2022, Pfizer acquired Bay Area biotech Global Blood Therapeutics (GBT) for $5.4 billion. GBT’s small-molecule drug Oxbryta binds to the b-globin molecule and prevents polymerization. Other small-molecule drugs are showing promise in the clinic.
But the value of gene and cell therapy approaches is that they promise “one and done” therapies that do not depend on a relative to donate stem cells. NIH hematologist John Tisdale, MD, who has been treating SCD patients with Bluebird Bio’s lovo-cel, a form of gene therapy that uses a lentiviral vector, was profiled on 60 Minutes two years ago. The program included a comment from former NIH director Francis Collins. He said, “This looks like a cure.”
Meanwhile, Beam Therapeutics and Editas Medicine are also pursuing SCD among their lead gene editing programs. At Boston Children’s Hospital, David Williams, MD, and Erica Esrick, MD, have published promising clinical data treating SCD patients using a short hairpin RNA approach, again targeting the BCL11A pathway.
Taking over the exa-cel program launched by CRISPR Therapeutics, Vertex published the initial exa-cel results in the New England Journal of Medicine in 2021. These represented not only a huge advance in treating SCD but also a crucial early validation of the clinical promise of CRISPR. Fyodor Urnov, PhD, scientific director at the Innovative Genomics Institute, hailed the results as “borderline utopian.”
Writing in The CRISPR Journal, Urnov proposed that Victoria Gray—who has been featured in a series of interviews on National Public Radio since 2019—be added to “the pantheon of names inscribed in golden letters in the history of biomedicine.” That list includes James Phipps (the boy vaccinated by Edward Jenner), Albert Alexander (the first recipient of penicillin), Louise Brown (the first test tube baby) and Emily Whitehead (the pioneering chimeric antigen receptor T-cell patient).
Utopian or not, the positive exa-cel trial results have been extended to dozens of SCD patients, with no reported serious adverse events, although a couple of patients have continued to experience some vaso-occlusive events. The only potential concern among FDA regulators was the possibility of CRISPR-induced off-target effects.
Five weeks ago, an FDA advisory committee meeting assembled a panel of experts to consider this issue. The Vertex investigators, led by chief science officer David Altshuler, MD, PhD, satisfied most of the panel’s lingering concerns about off-target editing and emphasized plans to monitor the long-term health of the exa-cel trial volunteers.
The FDA’s concern is understandable. In August 2022, Graphite Bio, a Bay Area gene editing company co-founded by Stanford University physician-scientist Matthew Porteus, MD, PhD, launched its own SCD gene editing trial. But five months later, the company voluntarily paused the trial after its first patient developed complications. Graphite Bio subsequently halted the trial completely, downsized, and agreed to a reverse merger with LENZ Therapeutics, a biotech company developing ocular therapies. Porteus has since launched a new company, Kamau Therapeutics, and acquired the rights to the SCD program, believing that the adverse events suffered by the first patient were caused by a drug used to treat low platelet counts and unrelated to gene editing.
Long road ahead
Immediately following Casgevy’s approval, Vertex announced a list price of $2.2 million, while Bluebird priced Lyfgenia at $3.1 million. But an ex vivo genome editing protocol that involves toxic chemotherapy, stem cell harvesting, and weeks in hospital is not going to be easily affordable or scalable.
If Gray’s inspiring story is the medical equivalent of the Lindbergh flight across the Atlantic, the next challenge, Urnov says, is to develop the equivalent of “routine, scalable, safe, and reasonably priced affordable air travel in a Dreamliner.” Urnov has been advocating regulatory and organizational incentives to fully realize the clinical potential of gene editing (see his recent video interview on GEN’s “Close to the Edge”).
How will these therapeutic advances be translated to the millions of SCD patients living in Africa, Asia, and beyond? Speaking at GEN’s State of Biotech virtual event in 2022, Doudna predicted that a one-time in vivo delivery approach—without ex vivo manipulation and bone marrow transplantation—would ultimately be achievable. “Is that going to be possible? My answer is yes,” she said. “Is it possible today? No.”
For SCD patients suffering from “the most famous point mutation in genetics,” as Beam’s CEO John Evans calls it, Casgevy is not the end of the journey, merely a long-awaited beginning.
Jiankui was sent to prison for three years in China for his unethical practices.
The original goal was to edit genes to offer complete or partial HIV resistance, which may not have worked anyway.
He Jiankui shocked the scientific community in 2018 by announcing his team had used the CRISPR-Cas9 gene-editing tool on twin girls when they were just embryos, resulting in the birth of the world’s first genetically modified babies. A third gene-edited child was born a year later.
Now, the disgraced gene-editing scientist, who was imprisoned in China for three years for the unethical practices, tells the South China Morning Post that all three children are doing well. “They have a normal, peaceful, and undisturbed life,” He says. “This is their wish, and we should respect them. The happiness of the children and their families should come first.”
He’s original goal was to use gene editing to attempt—many call this a live human experiment—to rewrite the CCR5 gene to create resistance to HIV. He says the genes were edited successfully and believed it gave the babies either complete or partial HIV resistance because of the mutation
He’s claim of success is unsubstantiated. In fact, it remains unclear if the experiment was even effective at all, setting aside for a minute the (huge) ethical implications. According to a 2019 MIT Technology Review report, “the team didn’t actually reproduce the known mutation. Rather, they created new mutations, which might lead to HIV resistance, but might not.”
He tells the SCMP he anticipates and worries for the future of the three girls as a traditional father would. He plans to track their medical needs and hopes to raise money to pay for health-related expenses. “After the age of 18,” He says, “the children will decide whether to do medical follow-ups for their individual needs. We committed to doing this for their lifetimes.”
He, who was released from prison in April 2022, admits his experiments were rushed. “I did it too quickly,” he says. Still, the scientist has already set up a Beijing laboratory to work on gene therapies for genetic diseases.
The ethical dilemma that He introduced may just be the start of a long line of questions regarding gene editing. He and his three test subjects won’t be the only players in the saga, but they’ll always be on the main stage.
Researchers in Japan and the United States have developed a new technology to increase visibility of cancer cells to the immune system using CRISPR. The findings were led by Koichi Kobayashi, professor at Hokkaido University and Texas A&M Health Center, and Paul de Figueiredo, Bond LSC principal investigator and NEXTGEN Precision Health endowed professor at the University of Missouri.
Major histocompatibility complex (MHC) class I molecules are an immune complex present on the surface of all cells in humans. MHC class I molecules are a prerequisite for the immune system to recognize and eliminate cancer. When cancer cells are faced with pressure from the immune system, they actively reduce their MHC class I molecules, so cancer cells can hide.
The researchers developed their technology to robustly augment the amount of MHC class I in cancer cells.
“Our discovery has the potential to transform the way we approach cancer treatment,” explained Kobayashi. “Our technology enables us to specifically target immune responsive genes and activate the immune system against cancer cells, offering hope to those who are resistant to current immunotherapy.”
Kobayashi and his team previously identified a gene, called NLRC5, that regulates MHC class I levels. They further found that NLRC5 is suppressed by turning off molecular switches existing on DNA in cancers through DNA methylation to reduce levels of MHC class I.
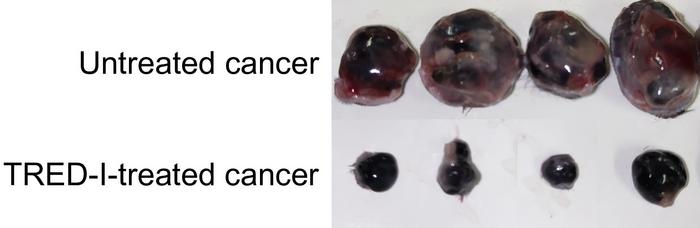
Their technology, known as TRED-I (Targeted Reactivation and Demethylation for MHC-I) system, was able to restore DNA methylation of NLRC5 gene and further activate NLRC5, thus increasing MHC class I levels in cancer without causing severe side effects.
Compared with untreated cancer, the TRED-I system significantly reduced cancer size in mice models. [Xin Sun, et al.
“New modalities for fighting cancer like this are desperately needed because we have few solutions to fight some cancer types,” said de Figueiredo. “This is a radically new approach, and I’ve felt lucky to be part of it.”
TRED-I was tested with animal cancer models. It reduced tumor sizes significantly and increased activity of cytotoxic CD8+ T cells. When used in conjunction with existing immunotherapy, TRED-I markedly enhanced treatment efficacy.
“This work is the culmination of our team’s research over the past decade,” Kobayashi concluded. “It’s great to shed light on moving our findings to potential clinical applications. We believe with further refinement, the TRED-I system could contribute significantly to cancer therapy.”
Their findings and method pave the way for new ways to combat cancer.
Scientists in the global south use the popular technique to protect local crops against local threats.
A field of sorghum in Botswana. Gene editing has created sorghum plants that are resistant to a destructive parasite called witchweed.
Molecular biologist Steven Runo once thought that his team would make history as the first to plant gene-edited seeds in African soil. The competition turned out to be stiffer than he’d anticipated.
A research group working on maize “beat us by two or three months”, says Runo, who works at Kenyatta University in Nairobi and whose gene-editing project focuses on sorghum. “But that’s good — African countries will see that this is actually possible.”
The friendly rivalry is a sign of progress. Researchers have long hoped that the relative ease and low cost of CRISPR gene-editing systems would make it possible for scientists in low- and middle-income countries to produce crops with traits tailored to the needs of local farmers — rather than relying on seeds developed in foreign countries. Now scientists are overseeing at least a dozen efforts to develop such gene-edited crops.
Among those projects is Runo’s effort to engineer sorghum to be resistant to Striga hermonthica, a troublesome species of a parasitic plant known as witchweed. Field trials of the new variety are scheduled for later this year, Runo said at the Plant and Animal Genome Conference in San Diego, California, on 16 January.
“It’s not as easy as people make it out to be to do gene editing, but it is pretty accessible,” says Kevin Pixley, a research director at the International Maize and Wheat Improvement Center in Texcoco, Mexico. “Runo is a perfect example of that.”
CRISPR takes on a witchy weed
Sorghum is a hardy crop that is used widely in Africa for food, building materials and feedstock. But more than 60% of African farmland is contaminated with species of Striga, a parasitic plant that attaches itself to sorghum roots and siphons away nutrients and water. A witchweed infestation can wipe out an entire crop.
Some wild varieties of sorghum are resistant to Striga because they carry mutations that alter the crop’s production of compounds called strigolactones, which promote germination of Striga seeds. Runo and his collaborators have used CRISPR–Cas9 to mimic these mutations.
Witchweed, which infests a large proportion of farmland in Africa, can devastate a crop.
Under Kenya’s 2022 regulations governing gene-edited crops, such plants are treated like conventionally bred crops because they do not contain DNA from another species. This means that these gene-edited plants can bypass some of the heavy testing and requirements imposed on genetically modified crops that contain foreign DNA. Nigeria and Malawi have similar policies, and other African countries, including Ethiopia and Uganda, are expected to follow suit, Runo says.
Last year, Kenyan authorities gave Runo and his collaborators permission to grow the gene-edited seeds under those regulations, and he plans to launch field studies later this year. It is a significant step, Runo said at the conference, because Striga is not a problem in wealthier regions — meaning that large, multinational corporations have little incentive to develop solutions for it.
Seeking cattle that can beat the heat
Other gene-editing projects are underway to improve African agricultural products. Pixley and his collaborators, including researchers at the Kenya Agricultural and Livestock Research Organization in Nairobi, have developed ways to edit maize (corn) to make it resistant to maize lethal necrosis disease. They are also editing pearl millet to make its flour less prone to becoming rancid soon after milling, and groundnuts to make them more resistant to infection by the fungus that produces cancer-causing aflatoxins
African livestock are also being edited. At the Plant and Animal Genome Conference, Dan Carlson, chief scientific officer at Recombinetics in Eagan, Minnesota, described a project in which African breeds of cattle are being edited improve their milk yields and tolerance to heat and disease.
Although gene editing is relatively cheap to perform in the laboratory, there are still significant hurdles to bringing edited crops to the farm, says Klara Fischer, who studies rural development at the Swedish University of Agricultural Sciences in Uppsala.
“Sometimes the discourse around this technology is overly enthusiastic,” she says. And because the market is unlikely to provide for poor small-scale farmers with limited purchasing power, government involvement would probably still be needed for the gene-edited products to benefit them.
Markets and money
Runo has relied on funding from the US Agency for International Development and has collaborated with Corteva Agriscience, an agricultural company in Indianapolis, Indiana. Pixley and his team have received funds from the Bill & Melinda Gates Foundation in Seattle, Washington, and have also gotten technical assistance from Corteva.
Runo is mindful that this support might not always be available. He and his team are working on cutting the cost of lab supplies and equipment and finding alternative funding sources.
Also unknown, says Pixley, is how intellectual-property battles over CRISPR gene editing will ultimately affect efforts in Africa, and whether foreign markets — particularly in Europe — will be open to African-grown gene-edited crops.
But as for local acceptance of the crops, Runo says the farmers he has spoken to feel more comfortable with crops developed by a local researcher than with seeds developed abroad. “This is not a multinational company. The people using the technology are people you have grown up with,” he says. “The narrative is very different.”
The type I CRISPR protein Cas3 works like Pac-Man, chomping away at a continuous stream of nucleotides with intrinsic activity for introducing targeted large deletions from a few hundred base pairs to as large as 200 kb. However, without the molecular equivalent to the four colored ghosts who chase and capture Pac-Man, the broad and unidirectional genome editing activity of Cas3 is essentially unregulated.
Yan Zhang, PhD, assistant professor in the department of biological chemistry at the University of Michigan Medical School, and her collaborators at Cornell University identified two anti-CRISPR proteins that can “turn off” Cas3, paving the way toward safer and better-controlled CRISPR applications.
Anti-CRISPR proteins in biotechnological applications
Certain phages have evolved small inhibitor proteins known as anti-CRISPRs to inactivate bacteria’s use of CRISPR effectors for immune defense.
Researchers have used anti-CRISPR (Acrs) proteins that inactivate Cas9, a Type II CRISPR system, to change the timing, location, or tissue-specific spread of gene editing activity or lower the number of unwanted off-target events.
Acrs against the Cas9 nuclease have provided genetically encodable brakes to control gene editing in numerous application contexts. For instance, delayed introduction of AcrIIA4 after Cas9 RNP delivery can reduce off-target editing in human cells. Tissue-specific control of Acr expression reinforced safe in vivo Cas9 editing only in the target organs of mice. Acrs have also been exploited as safety controls for gene drives, enablers for biosensors and synthetic gene circuits, facilitators for phage therapies, and are used to capture ligands to quantify Cas9’s presence in vitro.
Though CRISPR-Cas9 can induce large genomic deletions by using two targeting RNAs, called single guide RNAs (sgRNAs), that flank the region to be deleted, Cas9 with two sgRNAs may also increase the chance of undesirable off-target mutations as well as unintended reverse mutations between the cutting sites.
Regulating Cas3-mediated genomic deletions
CRISPR-Cas3, a Type I CRISPR system, relies on a multi-subunit ribonucleoprotein (RNP) complex called the CRISPR-associated complex for anti-viral defense (Cascade) to facilitate DNA target searching and activation upon forming a complex with target DNA. Despite the growing list of type I CRISPR-enabled eukaryotic applications, no Acr off-switches have been developed to control these technologies.
By comparing and analyzing cryoelectron microscopy “snapshots” of several Cascade-Cas3 complexes, Zhang and colleagues revealed the binding and cleavage mechanisms in high resolution. With this structural evidence, they identified two highly efficient anti-CRISPR proteins, AcrIC8 and AcrlC9, which work through two slightly different mechanisms to block Cascade from engaging DNA targets. Importantly, in human genome editing experiments, both Acrs were shown to inhibit Cascade-Cas3-induced DNA deletion and gene activation mediated by Cascade fused with the P65 transcription activator domain.
Acrl8 and Acrl8 represent the first set of Acrs harnessed as off-switches for multi-subunit CRISPR gene editors, paving the way toward safer and better-controlled type I CRISPR applications. This sets the stage to improve type I editing outcomes through temporal, spatial, tissue-specific, and light- or drug-controlled Acr regulation. The dose-dependent response observed with AcrIC8 and AcrIC9 may allow tunable control beyond a simple on-off switch.
While Acr proteins carry great promises as off-switches to mitigate undesired editing by Cas effectors, Zhang and colleagues say that it is unlikely to find Acrs that are highly effective against a broad spectrum of CRISPR-Cas systems, as structural variations among Cas homologs may weaken the high-affinity interactions from Acr. Narrow-spectrum Acrs may allow control of one CRISPR variant without interfering with the others, whereas broad-spectrum Acrs can shield the entire organism from any leaky activity of all editing agents. It is, therefore, important to understand the cross-reactivity of each Acr against different CRISPR systems.