Short, toxic RNAs kill brain cells and may allow Alzheimer’s to develop
Alzheimer’s disease, which is expected to have affected about 6.7 million patients in the U.S. in 2023, results in a substantial loss of brain cells. But the events that cause neuron death are poorly understood.
A new Northwestern Medicine study shows that RNA interference may play a key role in Alzheimer’s. For the first time, scientists have identified short strands of toxic RNAs that contribute to brain cell death and DNA damage in Alzheimer’s and aged brains. Short strands of protective RNAs are decreased during aging, the scientists report, which may allow Alzheimer’s to develop.
The study also found that older individuals with a superior memory capacity (known as SuperAgers) have higher amounts of protective short RNA strands in their brain cells. SuperAgers are individuals aged 80 and older with a memory capacity of individuals 20 to 30 years younger.
“Nobody has ever connected the activities of RNAs to Alzheimer’s,” said corresponding study author Marcus Peter, the Tom D. Spies Professor of Cancer Metabolism at Northwestern University Feinberg School of Medicine. “We found that in aging brain cells, the balance between toxic and protective sRNAs shifts toward toxic ones.”
Relevance beyond Alzheimer’s disease
The Northwestern discovery may have relevance beyond Alzheimer’s. “Our data provide a new explanation for why, in almost all neurodegenerative diseases, affected individuals have decades of symptom free life and then the disease starts to set in gradually as cells lose their protection with age,” Peter said.
New avenue for treatment
The findings also point to a new way for treating Alzheimer’s and potentially other neurodegenerative diseases.
Alzheimer’s is characterized by a progressive occurrence of amyloid-beta plaques, tau neurofibrillary tangles, scarring and ultimate brain cell death.
“The overwhelming investment in Alzheimer’s drug discovery has been focused on two mechanisms: reducing amyloid plaque load in the brain — which is the hallmark of Alzheimer’s diagnosis and 70 to 80% of the effort — and preventing tau phosphorylation or tangles,” Peter said. “However, treatments aimed at reducing amyloid plaques have not yet resulted in an effective treatment that is well tolerated.
“Our data support the idea that stabilizing or increasing the amount of protective short RNAs in the brain could be an entirely new approach to halt or delay Alzheimer’s or neurodegeneration in general.”
Such drugs exist, Peter said, but they would need to be tested in animal models and improved.
The next step in Peter’s research is to determine in different animal and cellular models (as well as in brains from Alzheimer’s patients) the exact contribution of toxic sRNAs to the cell death seen in the disease and screen for better compounds that would selectively increase the level of protective sRNAs or block the action of the toxic ones.
What are toxic and protective short RNAs?
All our gene information is stored in form of DNA in the nucleus of every cell. To turn this gene information into the building blocks of life, DNA needs to be converted into RNA which is used by cell machinery to produce proteins. RNA is essential for most biological functions.
In addition to these long coding RNAs, there are large numbers of short RNAs (sRNAs), which do not code for proteins. They have other critical functions in the cell. One class of such sRNAs suppresses long coding RNAs through a process called RNA interference that results in the silencing of the proteins that the long RNAs code for.
Peter and colleagues have now identified very short sequences present in some of these sRNAs that when present can kill cells by blocking production of proteins required for cells to survive resulting in cell death. Their data suggest that these toxic sRNAs are involved in the death of neurons which contributes to the development of Alzheimer’s disease.
The toxic sRNAs are normally inhibited by protective sRNAs. One type of sRNA is called microRNAs. While microRNAs play multiple important regulatory roles in cells, they are also the main species of protective sRNAs. They are the equivalent of guards that prevent the toxic sRNAs from entering the cellular machinery that executes RNA interference. But the guards’ numbers decrease with aging, thus allowing the toxic sRNAs to damage the cells.
Key findings
The amount of protective sRNAs is reduced in the aging brain.
Adding back protective miRNAs partially protects brain cells engineered to produce less protective sRNAs from cell death induced by amyloid beta fragments (which trigger Alzheimer’s).
Enhancing the activity of the protein that increases the amount of protective microRNAs partially inhibits cell death of brain cells induced by amyloid beta fragments and completely blocks DNA damage (also seen in Alzheimer’s patients.)
How the study worked:
Scientists analyzed the brains of Alzheimer’s disease mouse models, the brains of young and old mice, induced pluripotent stem cell-derived neurons from normal individuals (both young and aged) and from Alzheimer’s patients, the brains of a group of older individuals over 80 with memory capacity equivalent to individuals 50 to 60 years old, and multiple human brain-derived neuron-like cell lines treated with amyloid beta fragments, a trigger of Alzheimer’s.
More than 80% of menopausal women experience hot flashes.
Previous research has shown that hot flashes can increase a person’s risk for certain diseases and negatively impact their sleep.
Researchers from the Physicians Committee for Responsible Medicine have now found that following a low-fat vegan diet that includes soy makes changes in the gut microbiome. Some of these changes were linked to a decrease in menopause-related hot flashes by as much as 95%.
Hot flashes can sometimes be reduced through lifestyle modifications like maintaining a healthy weightTrusted Source, avoiding alcohol and caffeine, and not eating spicy foods.
Now, new research recently published in the journal Complementary Therapies in Medicine says thatfollowing a low-fat vegan diet that includes soy leads to a decrease of menopausal hot flash by as much as 95%.
According to Dr. Hana Kahleova, director of clinical research at the Physicians Committee for Responsible Medicine and lead author of this study, one of the reasons she wanted to study the effect of a vegan diet on hot flashes is because obesity is a risk factor for hot flashes.
“Research, including our ownTrusted Source, shows that a vegan diet promotes weight loss and can help fight obesity,” Dr. Kahleova told Medical News Today. “A vegan diet also avoids meat and dairy products, which are high in saturated fat and compounds called advanced glycation end-productsTrusted Source, both of which cause inflammation that can contribute to hot flashes.”
“Also, some research shows that women who have hot flashes may be at increased risk of heart disease and breast cancer, and a vegan diet can help lower the risk of both,” she added.
Although estrogen and estrogen-progestin medications can be used to treat hot flashes, Dr. Kahleova said they have been shown to increase the risk of breast cancer and cardiovascular problems.
“Vegan diets, on the other hand, can reduce these risks, and research shows that soy products are associated with a reductionTrusted Source in breast cancer risk,” she added.
Study participants were randomly asked to either follow a low-fat vegan diet that included a half-cup of cooked soybeans a day, or to just continue with their normal diet for 12 weeks.
A subset of 11 participants were asked to provide stool samples for a gut microbiome analysis both before the start of the study and after being on a vegan diet for 12 weeks.
Scientists found changes in the species of bacteria in the gut microbiome of participants who followed the vegan diet.
For example, more of the bacteria PorphyromonasTrusted Source and Prevotella corporisTrusted Source were found in those who followed the vegan diet, and these were linked to a reduction in severe hot flashes, including after adjustment for body mass index (BMI), a calculation that infers adiposity.
At the same time, researchers found a decline in the number of the bacteria Clostridium asparagiformeTrusted Source in the gut microbiome, which was associated with a decrease in total severe and severe night hot flashes.
Dr. Kahleova explained:
“A vegan diet with soybeans is rich in fiber and compounds called isoflavonesTrusted Source, both of which help increase the abundance of gut bacteria that fight inflammation and stabilize estrogen levels, which helps to fight hot flashes. Avoiding meat also helps to decrease the amount [of] gut bacteria that are linked to increased inflammation.”
All told, researchers found that study participants who consumed the low-fat vegan diet with added soy decreased their overall hot flashes by 95% compared to those who continued their usual diet.
Researchers also reported the vegan diet led to a 96% decrease in moderate to severe hot flashes, as well as a reduction in daytime hot flashes by 96% and nighttime hot flashes by 94%.
And study participants following the vegan diet also lost an average of 6.4 pounds (lbs) over the 12 weeks.
“Based on what we already know about the benefits of a low-fat vegan diet, we expected that it would change the composition of gut bacteria and help decrease hot flashes,” Dr. Kahleova said. “In addition to confirming our expectations, our study is the first, to our knowledge, to find that reductions in the abundance of the bacteria Porphyromonas, Prevotella corporis, and Clostridium asparagiforme may help reduce severe hot flashes.”
“These findings are the latest example of how eating a vegan diet plays a pivotal role in fighting diet-related conditions and diseases and maintaining good health as we age,” she added.
MNT also spoke with Monique Richard, a registered dietitian nutritionist, owner of Nutrition-In-Sight, and national media spokesperson for the Academy of Nutrition Dietetics, about this study.
Richard commented that because only 11 participants’ stools were analyzed during the study, it is a very small sample even though the percentage of hot flash frequency was significant at 95%.
“It is a very small sample size to pull from and make a conclusive statement/headline,” she noted. “It would be important to see this study replicated in larger sample sizes. Looking at vegans, vegetarians, and omnivoresTrusted Source each as a population, measuring fiber in each group, or possibly seeing if simply adding the 1/2 cup soy a day to each sample size would elicit the same type of outcomes and similar microbiome profiles would be interesting.”
Richard said previous research shows isoflavones in soy may contribute to a reduction in hot flashes possibly from the estrogen-like constituents of the plant, but they are not able to ascertain direct cause and effect and some of the studies are inconsistent and inconclusive.
“What we do know is that soybeans are a great source of protein, fiber, phytochemicalsTrusted Source, and beneficial nutrients that also feed our ‘good’ gut bugs and provide many protective benefits,” she continued.
“Literally feeding the gut microbiome with a plant-centric diet of whole foods tends to be beneficial in numerous ways and also alters the gut microbiome configuration and how those bacteria interact with hormones, enzymes, proteins, and metabolic reactions. This in turn affects our general well-being, tolerance, and symptomatic consequences of menses, illness, disease management and so much more.”
When it comes to using diet to help reduce menopausal hot flashes, Richard said because each individual has unique needs and these specific transitional times in a woman’s life bring additional factors to consider, it is important to meet with a registered dietitian nutritionist to assess overall dietary needs, nutrient needs, possible supplement recommendations, and lifestyle modifications.
“Overall, adequate sources of lean protein, fiber — both soluble and insoluble — omega-3 fatty acids, possibly a reduction in saturated fats, caffeine, alcohol, refined carbohydrates, and added sugars may also be beneficial to preserving bone mass, staving off common symptoms and supporting energy, mood and managing weight fluctuations,” she detailed.
“In addition to a diverse, colorful, varied diet with fruits, nuts, vegetables, legumes, fermented foods, seeds, and healthy fats, weight resistance training, sleep hygiene, and hydration status should be assessed and modified as necessary,” Richard continued. “Working with a registered dietitian nutritionist and healthcare team may help an individual mitigate and alleviate some of the uncomfortable and inconvenient symptoms during this season of life.”
Most of the women said they swam explicitly to improve their stress and anxiety. They reported that the exercise was healing and an immediate reliever of stress and anxiety.
One 57-year-old woman described the experience this way: “Cold water is phenomenal. It has saved my life. In the water, I can do anything. All symptoms (physical and mental) disappear and I feel like me at my best.”
“Cold water has previously been found to improve mood and reduce stress in outdoor swimmers, and ice baths have long been used to aid athletes’ muscle repair and recovery,” Joyce Harper, a professor of reproductive science at University College London and a senior author of the study, said in a press release.
“Our study supports these claims. Meanwhile, the anecdotal evidence also highlights how the activity can be used by women to alleviate physical symptoms, such as hot flashes, aches, and pains,” she added.
Other experts agreed the study findings do provide some positive aspects to cold water therapies.
“Swimming in cold water can reduce anxiety, just as many other people participate in regular exercises,” Dr. Jennifer Leighdon Wu, an OB/GYN at Northwell Lenox Hill Hospital in New York who was not involved in the research, told Medical News Today. “I found this study interesting.”
“I am not surprised by the results of the current study,” Dr. Michael Krychman, medical director of Women’s Health Services at MemorialCare at Saddleback Medical Center in California who also was not involved in the study, told Medical News Today. “Swimming is good because it is an exercise where you must focus.”
Experts noted that study might have some biases because the survey addressed women who already swam in cold water and who had previously reported an association between menopause symptoms and cold water swimming.
More than 60% of the women in the study swam to relieve their symptoms. Most of them swam in summer and winter. They wore bathing suits, not wetsuits.
In addition to relieving symptoms, the women said they felt cold water swimming improved mental health, increased regular exercise, and gave them time outdoors. The women also felt the positive effects were more pronounced when it was colder.
The researchers also explored whether cold water swimming helped menstrual symptoms. They found:
JN.1, a new COVID-19 variant detected in August 2023, has quickly spread worldwide, showing significant evolutionary changes from previous strains. This development calls for ongoing vigilance and adaptation in global health strategies.
The JN.1 COVID-19 variant, emerging in late 2023, marks a significant shift in the virus’s evolution, emphasizing the need for sustained global health efforts.
The World Health Organization (WHO) classified JN.1 as a “variant of interest” in December 2023 and in January strongly stated COVID was a continuing global health threat causing “far too much” preventable disease with worrying potential for long-term health consequences.
JN.1 is significant. First as a pathogen – it’s a surprisingly new-look version of SARS-CoV-2 (the virus that causes COVID) and is rapidly displacing other circulating strains (omicron XBB).
It’s also significant because of what it says about COVID’s evolution. Normally, SARS-CoV-2 variants look quite similar to what was there before, accumulating just a few mutations at a time that give the virus a meaningful advantage over its parent.
However, occasionally, as was the case when omicron (B.1.1.529) arose two years ago, variants emerge seemingly out of the blue that have markedly different characteristics to what was there before. This has significant implications for disease and transmission.
Until now, it wasn’t clear this “step-change” evolution would happen again, especially given the ongoing success of the steadily evolving omicron variants.
JN.1 is so distinct and causing such a wave of new infections that many are wondering whether the WHO will recognize JN.1 as the next variant of concern with its own Greek letter. In any case, with JN.1 we’ve entered a new phase of the pandemic.
Where did JN.1 come from?
The JN.1 (or BA.2.86.1.1) story begins with the emergence of its parent lineage BA.2.86 around mid-2023, which originated from a much earlier (2022) omicron sub-variant BA.2.
Chronic infections that may linger unresolved for months (if not years, in some people) likely play a role in the emergence of these step-change variants.
In chronically infected people, the virus silently tests and eventually retains many mutations that help it avoid immunity and survive in that person. For BA.2.86, this resulted in more than 30 mutations of the spike protein (a protein on the surface of SARS-CoV-2 that allows it to attach to our cells).
The sheer volume of infections occurring globally sets the scene for major viral evolution. SARS-CoV-2 continues to have a very high rate of mutation. Accordingly, JN.1 itself is already mutating and evolving quickly.
How is JN.1 different to other variants?
BA.2.86 and now JN.1 are behaving in a manner that looks unique in laboratory studies in two ways.
The first relates to how the virus evades immunity. JN.1 has inherited more than 30 mutations in its spike protein. It also acquired a new mutation, L455S, which further decreases the ability of antibodies (one part of the immune system’s protective response) to bind to the virus and prevent infection.
The second involves changes to the way JN.1 enters and replicates in our cells. Without delving into the molecular details, recent high-profile lab-based research from the United States and Europe observed BA.2.86 to enter cells from the lung in a similar way to pre-omicron variants like delta. However, in contrast, preliminary work by Australia’s Kirby Institute using different techniques finds replication characteristics that are aligned better with omicron lineages.
Further research to resolve these different cell entry findings is important because it has implications for where the virus may prefer to replicate in the body, which could affect disease severity and transmission.
Whatever the case, these findings show JN.1 (and SARS-CoV-2 in general) can not only navigate its way around our immune system, but is finding new ways to infect cells and transmit effectively. We need to further study how this plays out in people and how it affects clinical outcomes.
JN.1 has some characteristics which distinguish it from other variants.
Is JN.1 more severe?
The step-change evolution of BA.2.86, combined with the immune-evading features in JN.1, has given the virus a global growth advantage well beyond the XBB.1-based lineages we faced in 2023.
Despite these features, evidence suggests our adaptive immune system could still recognize and respond to BA.286 and JN.1 effectively. Updated monovalent vaccines, tests, and treatments remain effective against JN.1.
There are two elements to “severity”: first if it is more “intrinsically” severe (worse illness with an infection in the absence of any immunity) and second if the virus has greater transmission, causing greater illness and deaths, simply because it infects more people. The latter is certainly the case with JN.1.
What next?
We simply don’t know if this virus is on an evolutionary track to becoming the “next common cold” or not, nor have any idea of what that timeframe might be. While examining the trajectories of four historic coronaviruses could give us a glimpse of where we may be heading, this should be considered as just one possible path. The emergence of JN.1 underlines that we are experiencing a continuing epidemic with COVID and that looks like the way forward for the foreseeable future.
We are now in a new pandemic phase: post-emergency. Yet COVID remains the major infectious disease causing harm globally, from both acute infections and long COVID. At a societal and an individual level we need to re-think the risks of accepting wave after wave of infection.
People are advised to continue to take active steps to protect themselves and those around them.
For better pandemic preparedness for emerging threats and an improved response to the current one it is crucial we continue global surveillance. The low representation of low- and middle-income countries is a concerning blind spot. Intensified research is also crucial.
Blue light, the high energy visible light from digital devices, has been increasingly recognized as hazardous over the past decade. While some blue light exposure is inevitable in the modern world, research shows that overexposure can damage the eyes and disrupt healthy circadian rhythms.
While the focus of this article is on how blue light affects your eye health, consider also that the eyes are a direct portal into your brain, another exremely EMF sensitive organ which can be profoundly adversely affected by excessive blue light exposure.
The manifold ways in which blue light harms the eye — and mitigation strategies — are documented below:
Cornea
Studies demonstrate that blue light decreases corneal epithelial cell survival rates and triggers inflammation, oxidative damage, and cell death pathways[1][2][3]. This can exacerbate dry eye disease[4]. Topical antioxidants may help defend corneal cells from blue light-induced damage[5].
Lens
The human lens absorbs blue light to shield the retina, but this stresses lens proteins over time, likely contributing to cataract development[6][7]. Antioxidants like lutein and zeaxanthin accumulate in the lens and help defend it from oxidative damage caused by blue light[8].
Retina
In the retina, blue light overexposure activates cell death pathways leading to photoreceptor apoptosis, inflammation, and retinal pigment epithelium (RPE) dysfunction[9][10]. Retinal oxidative damage and cell death from blue light involves upregulation of VEGF and inflammatory cytokines[11]. Dietary antioxidants like lutein and zeaxanthin accumulate in the macula to help filter high energy blue light[12].
Circadian Disruption
Because blue light suppresses melatonin, excessive evening exposure disrupts circadian rhythms by shifting the master body clock and preventing critically important melatonin release[13]. This impairs sleep quality with consequences for mental and metabolic health over the long term[14].
Protecting Yourself
Given the variety of pathways by which blue light damages ocular tissue, blue-blocking glasses, screen filters, and apps that shift color temperature towards the warmer end of the spectrum in the evening help reduce exposure.
Dietary antioxidants also play a protective role. Since some blue light exposure is beneficial for eye development and circadian entrainment[15], the goal should be moderation rather than complete avoidance. Blue light should also be balanced with red light exposure. The best way to supplement with these precious rays are exposure to the rising and setting sun, at dawn and dusk. Failing that, there are a wide range of beneficial technologies available to increase red light exposure on your own schedule. You can view some of our favorite products in the Regenerate Lifestyle Center.
With smart blue light avoidance strategies, we can remain productive and preserve healthy vision and sleep patterns in the digital age. But restraint is warranted, as overexposure comes at a cost to the eyes and body.
One last note about excessive blue light exposure. Recent research we reported on here indicates that excessive blue light exposure can actually accelerate skin aging as well, acting very similarly to excessive UVA or UVB light exposure.
For years, proton pump inhibitors were marketed to the public for stomach relief from ‘excess acid production,’ without the slightest clue that they were contributing to the burgeoning epidemic of neurodegenerative disease. All that has now changed…
A recent study published in Neurology has raised fresh concerns about the long-term use of proton pump inhibitors (PPIs), a class of widely used acid-blocking drugs. This research adds to a growing body of evidence, documented extensively at Greenmedinfo.com, which points to over 80 signals of harm associated with their use here, which incidentally includes increased heart disease risk.
The study found a significant correlation between prolonged use of PPI medications like Nexium or Prilosec and a 33% increased risk of developing dementia[1]. This association is not entirely new, as previous suspicions[2] have been substantially strengthened by this latest research, which utilized comprehensive medical records and in-person assessments of nearly 6,000 American seniors over a 20-year period[1].
This extensive analysis, incorporating multiple visits, has for the first time firmly established a connection between substantial PPI use and a rise in doctor-confirmed cognitive decline[1], signaling a strong warning regarding the brain health implications of these drugs.
The complexity of the mechanisms through which PPIs impact dementia risk makes it challenging to fully comprehend their effects. It’s evident, however, that long-term use can alter various body systems that influence dementia risk, such as nutrient status, vascular and kidney health, immune function, and gut microbiome[3].
For instance, PPIs can impair the absorption of vitamin B12, which is vital for cognitive health[4]. A deficiency in B12, more likely with prolonged use of acid blockers[1], is closely linked to Alzheimer’s disease biomarkers and genes associated with dementia susceptibility[5].
Furthermore, PPIs have been tied to an increased risk of stroke[6], heart attack[7], chronic kidney disease[8], and magnesium depletion[9], all of which are known to accelerate the risk of dementia.
The drugs also significantly alter digestive ecology over the years[10], potentially affecting neurological health via the microbiome-brain axis[11].
While research is ongoing to unravel the full “downstream” effects of PPIs, this study raises an important flag about the increased risk of dementia with their long-term use[1].
This raises a critical question: do the benefits of long-term PPI use outweigh the unfolding risks to brain health and overall well-being? Safer digestive aids like DGL licorice, mucilaginous herbs, and glutamine might be preferable first steps over acid suppression, if possible[12]. Even the simple act of drinking water could profoundly and immediately relieve symptoms according to this underreported research.
In cases where short-term PPI use is necessary for serious conditions, supplementing with B12, magnesium, and beneficial flora can mitigate side effects[13]. However, avoiding unnecessary extended use of PPIs is currently the safest approach.
As science continues to decode the systemic implications of chemically disrupting stomach acidity over years, prioritizing lifestyle changes and safer supplements for stomach and brain health becomes increasingly important.
Data from an African observatory show that jets from a collapsed star are capable of producing some of the Galaxy’s fastest particles.
The Manatee Nebula formed when a giant star exploded more than 10,000 years ago, leaving a black hole at its core.
An array of telescopes in Namibia has pinpointed the origin of some of the most energetic particles the Galaxy can produce. The observations point to a place where particles of matter spewed by a black hole in a region known as the Manatee Nebula are accelerated to near-light-speed.
The findings, published on 25 January in Science1 by researchers at the High Energy Stereoscopic System (HESS), are a step forward in the century-old quest to understand the origins of cosmic rays — fast-moving atomic nuclei and other particles that are continually hitting Earth’s upper atmosphere.
“For people like me who want to model astrophysical jets, including their internal composition, propagation and evolution”, the information produced by HESS is “incredible”, says Sera Markoff, a theoretical astrophysicist at the University of Amsterdam.
Rain from space
Cosmic rays can have a wide range of energies. The most abundant, lowest-energy cosmic rays consist of particles of solar wind that rain down on Earth’s atmosphere after spiralling in the planet’s magnetic field. Cosmic rays of much higher energies are thought to be produced by supernovae, the explosive deaths of massive stars. And yet-more-energetic cosmic rays originate outside the Galaxy, in particular from quasars — super-massive black holes that produce jets of plasma travelling at near-light-speed. These jets can have energies of up to 8 orders of magnitude higher than those produced in particle accelerators.
Astrophysicists have proposed that plasma jets from black holes that are smaller than quasars — but still several times as massive as the Sun — could also contribute to the cosmic-ray population. The energies produced by these ‘microquasars’, which are also bright sources of X-rays and radio waves, could reach a range intermediate between those from supernovas and those from quasars.
In the latest study, astrophysicist Laura Olivera-Nieto at the Max Planck Institute for Nuclear Physics in Heidelberg, Germany, and her collaborators studied a microquasar called SS 433. The black hole lies in the Aquila Constellation at around 18,000 light years (5.5 kiloparsecs) from the Solar System, and forms a binary system together with a large star. Matter ejected from the star swirls around the black hole then spirals into it, generating highly energetic jets.
The binary system is surrounded by a nebula nicknamed the Manatee owing to its elongated shape. The nebula is a shell of dust and gas left over from a supernova between 10,000 and 100,000 years ago, during which the core of an exploding star collapsed to form the black hole. The outflow of matter from the supernova would itself have produced cosmic rays for thousands of years after the event, an activity that has long since quietened down. But some time between 10,000 and 30,000 years ago, the system lit up again, when the black hole formed its jets. The researchers think that this is when it started producing cosmic rays again.
Cosmic clues
Any cosmic-ray particles originating from a microquasar would move across the Galaxy in spirals before reaching Earth, their trajectories bent by magnetic fields. This makes it impossible to trace their paths back to a specific source. Instead, astrophysicists searching for the possible origins of cosmic rays look for γ-ray photons, which should be produced in the same processes that accelerate cosmic-ray particles, but travel to Earth in straight lines.
Astronomers first observed γ-rays from SS 433 in 2018 from the High Altitude Water Cherenkov (HAWC) observatory in Mexico’s Pico de Orizaba National Park2. But, unlike the team at HESS, they were unable to locate the exact source with precision.
The High Energy Stereoscopic System telescope array in Namibia’s Khomas highlands.
Both HAWC and HESS detect γ-ray photons indirectly, but they use different approaches. When a γ-ray collides with an atomic nucleus in the upper atmosphere, it produces a shower of secondary particles, including electrons and their heavier siblings, muons. HAWC has water-filled tanks that pick up these particles as they reach the ground, whereas HESS works by imaging flashes of light that the particles produce as they move down the atmosphere. The five dishes of HESS can be pointed in a specific direction in the sky.
This allowed HESS to precisely locate where in the Manatee Nebula the γ-rays were produced, and to focus on distinguishing those with particular energies. More than 200 hours of observations, made over 3 years, show that the γ-ray emission starts around half-way between the black hole and the supernova remnant, and slowly peters out. “The highest-energy photons only come from closer to the black hole,” says Olivera-Nieto. “This was really the crucial discovery.”
This suggests that the γ-rays — and by implication, cosmic rays — are produced by mechanisms internal to the jets, rather than by collisions with other matter, Olivera-Nieto explains. The space surrounding the black hole is otherwise empty, swept clean by the supernova’s expanding shockwave.
The finding “strengthens the case that X-ray binaries are smaller analogues to supermassive black holes, and equally capable of accelerating cosmic rays”, says Markoff, who praises Olivera-Nieto’s data analysis. “Her technique allowed the use of more data, and amplified the sensitivity enough to do this fantastic study, and so sets the stage for much more work like this.”
Improvements in screening and diagnosis could help to eradicate this curable disease.
Mireille Kamariza is working on an affordable test for tuberculosis.
Growing up in Burundi, a country of 13 million people in East Africa, Mireille Kamariza was familiar with the devastating effects of tuberculosis (TB). “It’s a long and torturous disease,” she says. “You have relatives and loved ones that are sick, and you see them suffer through it. It’s not a quick death.”Part of Nature Outlook: Medical diagnostics
When she moved to the United States at 17, she was struck by how different the situation was there. “The question that I had when I arrived here was, how come this is not a problem here?” That question led Kamariza, now a chemical biologist at the University of California, Los Angeles, on a quest to find ways to eradicate the disease in areas where it is widespread. A key challenge is determining who is infected, so that they can be treated and the disease stopped from spreading. But current diagnostic methods are slow, often expensive, sometimes difficult to administer and not easily accessible in the low-income regions where TB is most prevalent.
TB researchers are pushing to develop faster, more accurate and more accessible tests. In 2014, the World Health Organization (WHO) set the goal of reducing the number of new cases worldwide by 80% between 2015 and 2030; it considers widespread screening and rapid diagnosis as crucial to achieving this. Replacing older testing methods with newer diagnostic and screening techniques could help individuals with the disease to be identified quicker and start treatment before their symptoms worsen — potentially before they can spread the disease. “It’s the people who have TB and don’t know they have it, they’re the ones who are spreading the disease,” says Jerry Cangelosi, an environmental-health scientist at the University of Washington School of Public Health in Seattle.
TB has been infecting people for at least 9,000 years, and it has often been the leading cause of infectious-disease deaths globally. It was eclipsed in the past few years by COVID-19, but, as the pandemic wanes, TB could retake the top spot. According to the WHO, an estimated 10.6 million people caught TB globally in 2022 and 1.3 million died1.
The disease is caused by Mycobacterium tuberculosis, a microorganism that is spread through coughing, sneezing and spitting. It thrives in crowded conditions where there is poverty, poor nutrition and a lack of accessible health care. Fortunately, the disease is treatable with antibiotics, and the drugs used now are less toxic and taken for a shorter time than those used in the past — a few months, rather than a couple of years — even for drug-resistant strains. Around 4% of new cases are resistant to multiple drugs, and that rises to 19% among people who have previously received treatment.
But treatment and prevention require the identification of people who have and could spread the disease. “There’s a huge gap in the number of TB cases that we know are out there and what we’re actually diagnosing,” says Adithya Cattamanchi, a pulmonologist and epidemiologist at the University of California, Irvine. At least 3 million people of the WHO’s 10.6 million estimate are undiagnosed, he says.
Part of the problem, Cattamanchi says, is that the most prevalent test for TB is the sputum smear test, for which health-care workers collect a mix of saliva and mucus coughed up from the lungs; stain it with auramine, a dye that attaches to a large family of bacteria; and examine it under a microscope. The technique behind the test was developed in the 1880s by the German microbiologist and Nobel prizewinner Robert Koch. “It’s still, 150 years later, the test that we most commonly use,” Cattamanchi says.
But it has limitations. Some people have trouble coughing up sputum; people with HIV and children under five are less likely to produce much of the substance. Health-care workers collecting the sample could be exposed to the pathogen while the person is coughing. The thick sputum has to be thinned to be placed on a microscope slide. Finding the bacteria can take a day or two, and even then, it is unknown whether the strain is drug resistant. To work this out, physicians can culture the bacteria against various drugs — but that takes several weeks, which can delay administration of the right treatment. Often, physicians simply start people on the most common treatment and see whether they improve.
Molecular tests can be faster than microscopy and more accurate than cultures, because they can amplify DNA and identify resistant strains directly. But the uptake of such tests has been slow. Nucleic acid amplification tests (NAATs) have been available for almost three decades, but the earliest ones were labour intensive and required specialized skills to administer. More recent NAATs, such as the semi-automated polymerase chain reaction tests, can identify the bacteria and whether they are resistant to the first-choice antibiotic, rifampicin, in about three hours. These tests still have limitations, Cattamanchi says, because the equipment is expensive and needs to be kept in a facility that can reliably supply power and maintain an appropriate temperature — putting the machines out of reach of many local health-care facilities, where people usually seek care first. The WHO recommended a molecular test, branded Xpert, in 2010, but the cost of the individual test cartridges is prohibitive to the communities that need them. Danaher in Washington DC, the company that sells Xpert, announced last September that it was lowering the price from US$10 per cartridge to $8. But health advocates want that to go down to $5, which they say would make the test more accessible while still allowing the company to make a profit.
Bodily fluids
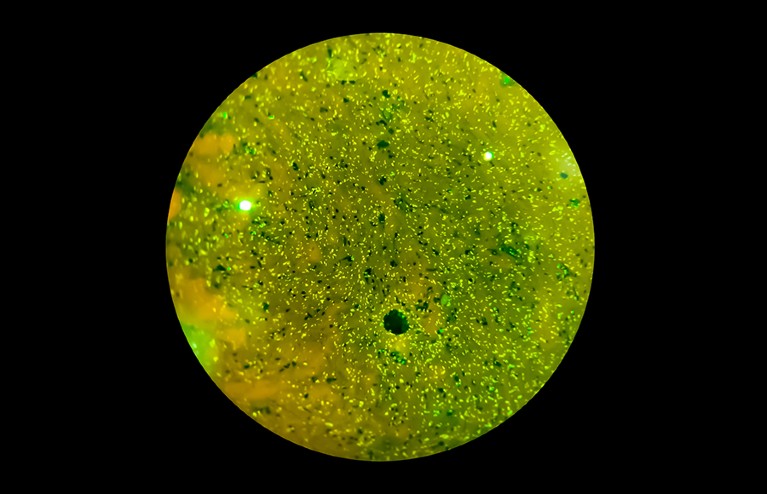
Kamariza is working on a cheaper diagnostic test, a fluorescent tag that binds to a product of living TB bacteria and makes them quickly identifiable under a microscope. Although fluorescent probes are common in biology, there are surprisingly few for TB, she says. In fact, auramine is the only other one.
The microorganism Mycobacterium tuberculosis causes tuberculosis and is spread through coughing and sneezing.
Kamariza developed a dye molecule that binds to a sugar, trehalose, on the surface of the bacterial cell. Staining a sputum sample with the dye does not require much preparation, Kamariza says, and the bacteria light up in minutes. While still a PhD student at Harvard University in Cambridge, Massachusetts, she co-founded a company — OliLux Biosciences, based in Los Angeles — to commercialize the probe. Since then, she has learnt that although her dye was easy to spot with the high-end microscope in her laboratory, it was too dim for the cheaper equipment used in a typical clinic in Uganda, where the company is testing the assay. So she is developing a brighter dye that those microscopes can detect1.
For now, Kamariza’s method still requires sputum and a microscope. That could change, however; she has collected some data (not yet published) suggesting that it will work on bacteria in blood samples as well. Although this is not the molecular approach that the WHO is pushing for, Kamariza feels that her test could be an intermediate step — many countries do not have the infrastructure to use molecular tests widely. She hopes that her test can speed up the identification of resistant strains during culturing as well. Getting results in a day or two will lead to people receiving the correct treatment more quickly, she says.
Other researchers are looking beyond sputum. Biochemist Tony Hu, who directs the Center for Cellular and Molecular Diagnostics at Tulane University’s School of Medicine in New Orleans, Louisiana, is developing several tests to detect products of TB bacteria in blood samples, which could be collected by a finger prick. In one test, he introduces a nanoparticle engineered to bind to a particular protein produced by the bacteria, called CFP-10. The nanoparticle amplifies the protein in the sample, making it more detectable by a mass spectrometer. Hu tested the method on blood samples from children under five, who can be difficult to diagnose because their TB symptoms can be attributable to other diseases. He found TB in 100% of children who also had HIV and had had TB confirmed by another method, and in 84% of children with HIV who had tested negative with other methods but were later diagnosed2. People with HIV are more likely to have extrapulmonary TB, which leaves fewer bacteria in the lungs and makes it harder to diagnose.
Hu also uses nanoparticles to target the TB-associated proteins lipoarabinomannan (LAM) and lipoprotein LprG. Cells shed waste by releasing particles called extracellular vesicles, which, in people with TB, contain LAM and LprG. “The most important thing for us is the abundance,” Hu says. “One cell can secrete 10,000 vesicles every day.” And those vesicles persist in the blood for longer than the proteins alone would, making them available for detection.
Hu coats his nanoparticles with antibodies that bind to the vesicles, and then looks for them using a microscope3. He’s even designed and tested a small system that can replace the microscope. It includes a smartphone and an objective lens, and uses a mobile app — aided by a machine-learning algorithm that screens out background noise — to find the nanoparticles. The portable device showed results similar to those from a microscope. A third test that Hu has developed, which uses gene-editing technology to amplify TB DNA floating in the blood, is also simple. It uses a paper strip to hold the sample, a small amount of reagent and a smartphone-sized reader4.
Another easy-to-collect sample is urine, which also contains LAM. The first WHO-recommended version of a LAM urine test has low sensitivity, identifying only about 40% of people with TB if they are also infected with HIV, and 20% of people without HIV5. New generation urine tests are being developed that have a sensitivity of around 70%.
That’s not as high as physicians would like, but the tests are still useful for targeted populations, such as people with HIV, says Ruvandhi Nathavitharana, an infectious-disease specialist at Harvard Medical School in Boston, Massachusetts. “If you can do a urine-based bedside test and it’s positive, then a clinician can get that person on TB treatment straight away,” she says.
Algorithm-aided screening
Whereas urine collection requires some privacy, swabbing people’s tongues is so straightforward that a nurse could walk around a classroom testing students while they sat at their desks, says Cangelosi. That sort of community screening will be necessary to get TB under control, he says. And “if we want to envision going into workplaces or schools or communities and actively screening people, sputum collection is a non-starter”.
Even when it’s not easy for someone to produce sputum, TB bacteria come up from the lungs when people cough, and land on the back of the tongue, where they can persist for hours6. So far, tongue swabs have not proved as sensitive as other tests, but that could be because they’re being used in conjunction with testing platforms that have been optimized for sputum, Cangelosi says. That could change, however. The COVID-19 pandemic led many diagnostic companies to develop platforms for testing nasal swabs, and those could be adapted for tongue swabs.
Whether it involves tongue swabs or another approach, community screening is important to stem the spread of TB. Chest X-ray has a venerable history as a screening tool. “We used it way back when in the United States to really reduce the prevalence of TB,” Cattamanchi says. Today’s portable, digital X-ray machines don’t require the expensive film and process of past machines, and they can be placed in local health centres or driven around in a van. The main barrier to X-ray screening is a lack of skilled radiologists to interpret the scans.
To address that shortage, several research groups are using artificial intelligence (AI) to identify TB in lung images. Google, for instance, has been training an AI system using X-rays of people who are known to have TB, so that the tool can learn how the various types of lung damage caused by the disease look in an image and can spot them in new X-rays7. People flagged by the AI tool could then take a more established type of test, such as a NAAT, to confirm whether they have TB, says Daniel Tse, a health researcher at Google Research in Mountain View, California. Such screening, which Google’s test7 found was comparable with that performed by radiologists, could reach more people and mean that diagnostic tests are targeted more specifically, keeping costs down. For now, Tse says, images are processed by Google’s cloud servers, but for areas that have unreliable Internet access, the diagnostic algorithm might be stored on a smartphone or a dongle. Google has licensed the technology to Right to Care, a non-profit health-care organization in Centurion, South Africa.
AI could be applied to other information as well. Researchers at Stellenbosch University in South Africa, for instance, are working on algorithms that can identify TB from coughing sounds, recorded by a smartphone8. Others have explored doing something similar with lung sounds recorded by digital stethoscopes9. Tse says that several researchers are exploring whether an AI tool that combines multiple data sources might boost TB identification further.
Screening and diagnostic tests are continuing to improve, but to really fulfil their potential, they need the kind of funding and political will that was directed against the COVID-19 pandemic, says Nathavitharana. “The technologies are advancing, but honestly, it’s too slow,” she says. “We saw how much could be achieved for COVID in a very short time with the resources and targeted attention.” TB is both preventable and curable, and a major push could end its devastation, she argues. “No one should be dying of a disease like TB when we can do better.”
Study compared SGLT2 inhibitors with GLP-1 agonists and DPP-4 inhibitors
One class of glucose-lowering agent may help lower the risk of kidney stones in adults with type 2 diabetes, a cohort study suggested.
Adults who newly started on an SGLT2 inhibitor had a 31% lower risk of nephrolithiasis compared with those starting on a GLP-1 receptor agonist (HR 0.69, 95% CI 0.67-0.72), found Julie M. Paik, MD, ScD, MPH, of Brigham and Women’s Hospital in Boston, and colleagues. This equated to 14.9 versus 21.3 nephrolithiasis events per 1,000 person-years for new SGLT2 and GLP users over a median 192-day follow-up, respectively.
New SGLT2 users also had a significantly lower risk of nephrolithiasis when compared with new initiators of a DPP-4 inhibitor (HR 0.74, 95% CI 0.71-0.77), the group reported in JAMA Internal Medicineopens in a new tab or window. This equated to 14.6 versus 19.9 nephrolithiasis events per 1,000 person-years for SGLT and DPP-4 users, respectively.
These findings didn’t come as much of a surprise to the researchers, Paik told MedPage Today, given what is already known about SGLT2 inhibitors and their renoprotective benefits. According to the study, the reduced kidney stone risk with SGLT2 inhibitor use could be explained by the drugs’ ability to increase urinary citrate excretion or urinary bicarbonate excretion, their anti-inflammatory properties, or by increasing urine flow.
“However, there had been no prior studies looking at the association between the use of this newer class of diabetes medication and the risk of kidney stones in a U.S. population receiving routine care,” she said. “The risk of kidney stones in a patient might be one additional consideration for a clinician to take into account when choosing among the different glucose-lowering agents for patients with type 2 diabetes.”
That being said, she pointed out that their study only included patients with type 2 diabetes and therefore it’s still unclear how this class of medications might modify risk in patients without type 2 diabetes but at risk for kidney stones.
In subgroup analyses, Paik’s group found that kidney stone risk was still significantly lower with SGLT2 inhibitors across various age groups, sex, race, and BMI. The only subgroup that didn’t have a lower nephrolithiasis risk were those falling into early chronic kidney disease (CKD) stages (1 to 2), but those in higher stages (3 to 4) had a significantly lower risk.
While all ages had significantly lower nephrolithiasis risk with SGLT2 inhibitors, the magnitude of the risk reduction was greater among those under 70 years.
The researchers pulled data on 716,406 adults with type 2 diabetes from Optum’s deidentified Clinformatics Data Mart Database (2013-2020), IBM MarketScan (2013-2019), and Medicare Fee-for-Service Parts A, B, and D (2013-2018). For inclusion, all patients had to be new adult users of an SGLT2 inhibitor, GLP-1 agonist, or DPP-4 inhibitor between 2013 and 2020. Those with a prior history of kidney or urinary tract stones were excluded. Nephrolithiasis was diagnosed by ICD codes in the inpatient or outpatient setting.
New SGLT2 users were propensity-score matched 1:1 to new users of GLP agonists and DPP-4 inhibitors.
Prior to matching, patients starting GLP agonists were more likely to be female and to have seen an endocrinologist or nephrologist; were more likely to have a higher combined comorbidity score, obesity, or CKD stage 3 to 4; and were more likely to be on insulin or a loop diuretic but less likely to be taking metformin.
The group initiating DPP-4 inhibitors were more likely to be older, to have seen a nephrologist, and to be taking a loop diuretic or an antihypertensive agent. They were also more likely to have a higher combined comorbidity score, CKD stage 3 to 4, heart failure, cerebrovascular disease, or a history of a urinary tract infection or acute kidney injury. This group was also less likely to have obesity, to be taking insulin, and to have seen an endocrinologist.
In the SGLT2- and GLP-matched cohort, the average age was 61 years, 51% were women, 71% were white, 40% had obesity, 7% had CKD stage 3 to 4, and 4% had a history of gout. In the cohort matched with DPP-4 inhibitors, the average age was 62 years, 47% were women, 62% were white, 34% had obesity, 6% had CKD stage 3 to 4, and 4% had a history of gout.
Because nephrolithiasis occurrence was measured with diagnostic codes, Paik’s group warned there was the potential for some outcome misclassification. Also, they couldn’t tell if kidney stones were new or recurrent, nor tell the composition of the stones.



.png)

.png)
.png)
.png)
.png)





{kind=link}
{kind=link}