Fresh pieces of aloe vera. The peels of this plant can be used as a natural pesticide against harmful insects, research suggests.
Speed read
Aloe peels have bioactive compounds that can ward off bugs
Findings may offer new use for peels that are usually discarded as waste
Could be catalyst for organic farming and traditional medic
The discarded peels of aloe vera can be used as a natural pesticide, helping farmers protect staple food crops from harmful insects, research suggests.
Globally, between 20 and 40 per cent of crop yields are lost to pests, which has a direct impact on food security and nutrition, according to CABI (the parent organisation of SciDev.Net).
Aloe vera is a stemless, cactus-like plant that is widely cultivated in Australia, China, India, Jamaica, Mexico, South Africa, Tanzania and the US. Its gel-like substance is used to heal wounds, sunburns, and skin diseases, and to prevent baldness.
However, aloe vera peels or rinds are considered worthless and usually disposed of as agricultural waste.
“By repurposing the leftover aloe peels that are currently discarded, aloe production can be made more sustainable and contribute to achieving the UN Sustainable Development Goals.”
Debasish Bandyopadhyay, chemistry professor, University of Texas RGV
“It’s likely that millions of tonnes of aloe peels are disposed of globally every year,” says Debasish Bandyopadhyay, an assistant professor in chemistry at the University of Texas Rio Grande Valley, US, and principal investigator on a study to find ways to add value to aloe while reducing waste.
At a meeting of the American Chemical Society this month (17 August), Bandyopadhyay and his colleagues showed how aloe vera peels can act as a natural insecticide, staving off insects from crops such as maize or millet.
“We proved that [aloe] vera rinds’ derived extracts act as a feeding deterrent and eventually kill agricultural pests,” Bandyopadhyay tells SciDev.Net.
He explains that insects do not like aloe vera peels as it contains phytochemicals (chemicals produced by plants) that are toxic for them.
“Insects may be harmed or killed by natural substances contained in aloe peels,” he adds.
“Exposure to these compounds can cause discomfort, illness or even disruptions in an insect’s ability to travel, eat and reproduce.”
The researchers became interested in the potential use of aloe peels as insecticide after visiting a site where they noticed that insects left aloe leaves alone while attacking the leaves of other plants. They hypothesised that aloe peels have specific defence chemicals.
To investigate, they collected and dried out the peels and then produced extracts from the peels with substances such as dichloromethane (DCM), hexane and methanol.
Univera’s aloe farm in Tampico, Mexico. Researchers have become interested in the potential use of aloe peels in insecticide production. Photo by UNIVERA (CC BY-SA 4.0).
Their experiments showed that the DCM extract of aloe peels had substantial insect-killing properties against farm pests, as did six other compounds from the peels.
Significantly, the compounds did not show toxic properties, suggesting that aloe-peel-based insecticide wouldn’t have significant safety concerns for people.
“By repurposing the leftover aloe peels that are currently discarded, aloe production can be made more sustainable and contribute to achieving the UN Sustainable Development Goals,” Bandyopadhyay tells SciDev.Net, citing Zero Hunger as an example.
Economic potential
Chiranjib Chakraborty, a professor at the School of Life Science and Biotechnology, Adamas University in Kolkata, India, believes the findings have huge economic potential and could help promote organic farming and traditional plant medicines.
“The world is now looking at organic farming,” he tells SciDev.Net.
He believes the research findings could support a shift to a more sustainable farming and replacement of chemical-based practice in millions of farms devoted to rice, wheat, maize and millet.
According to a 2021 review published in the journal Molecules, indiscriminate and prolonged use of synthetic pesticides leads to human health issues, water, air and soil contamination, and pest resistance.
Plant-derived pesticides, which are cheap and eco-friendly, are an important alternative to synthetic pesticides, protecting the environment and human health and enhancing crop production.
Chakraborty believes the study opens up avenues for research on other traditional medicinal plants to find scientific evidence of the purported beneficial properties.
False-coloured scanning electron micrograph of two Plasmodium ookinetes (purple), each parasite measuring 12 micrometres. This represents one stage in the malaria parasite life cycle. Plasmodium is a parasitic protozoa that causes malaria.
Speed read
Sensitive diagnostic tools identify silent malaria, offering insights for control
Existing tests often fail to detect asymptomatic malaria
Researchers say method can enhance data, pivotal for advancing vaccines and drugs
Researchers in the USA and Uganda have developed tools that can detect the slightest traces of malaria in people who harbour the disease but do not show signs of sickness.
Malaria is the leading cause of illness and death in many low-income countries, with young children and pregnant women most affected.
In 2022, there were 608,000 malaria deaths worldwide, with 95 per cent of them occurring in the African region, according to the World Health Organization.
Detecting malaria in people who do not show symptoms is vital in order to better control the tropical disease in endemic areas, the researchers said in a study published this month (4 January) in the journal The Lancet Microbe.
“Our current findings provide critical information on the burden of asymptomatic malaria that we hope one day will be useful to the national malaria control program in Uganda and other malaria-endemic African countries.”
Tonny Owalla, researcher at Medical Biotech Laboratory, Kampala
The scientists from the University of Washington and Med Biotech Laboratories in Kampala said that due to the changing nature of malaria pathogens, parasite densities in the blood can suddenly drop below the level of detection. This is especially the case when older, less sensitive tests are used and when testing is done only at a single point in time.
Sean Murphy, professor of laboratory medicine and pathology at the University of Washington and lead author of the study, said: “To make anti-infection vaccines, drugs and therapeutics and test them in endemic areas means that you need diagnostic tools that can detect even the lowest density infections.”
He noted that the ultrasensitive molecular diagnostic tools are more analytically sensitive than other tests like blood smear, malaria rapid diagnostics tests, and even other types of molecular tests.
“This means we can ‘see deeper into the water’ and identify true, albeit low density infections that would have been missed by other tests,” Murphy said.
Murphy explains that having all this information can help researchers better assess candidate vaccines and drugs to decide which products provide the most effective outcomes.
Ultrasensitive tests
The researchers used ultrasensitive molecular diagnostic tools to test adults aged 18 to 59 and children aged eight to 17 who were not pregnant and were not under malaria medication in the Katawki district in eastern Uganda, which has a high incidence of malaria.
They tested dried blood spots for the presence of Plasmodium ribosomal RNA, which helps produce the parasite proteins, to determine and classify the type and densities of the parasites over a period of one month.
By analysing the resulting data, the researchers hoped to discern a sampling schedule -comparable to testing every day but less burdensome – to reliably identify asymptomatic cases.
About 60 per cent of participants had a Plasmodium infection at some point during the study. Fewer than half had an infection detected at the start of the study. The average infection rate was 30 per cent.
“We know that Plasmodium falciparum is common in Africa and is the most likely species to make people sick with malaria,” Murphy told SciDev.Net.
“I was surprised by the high number of P falciparum in our study,” he added.
“In some cases, these were present on their own in participants, but in other cases participants had mixed species infections.”
In a few cases, a species present at the start of the month tapered off and a new later emerged, he added.
“To capture these transitions with our approach was very enlightening,” he said.
‘Emerging trend’
Tonny Owalla, a researcher at Medical Biotech Laboratory in Kampala and co-author, told SciDev.Net that there is an emerging trend of parasite prevalence in children over five years old in Uganda with no symptoms.
He says more research is needed into the dynamics of asymptomatic malaria.
“We still need to build the body of evidence about asymptomatic infections before health ministries and other agencies can act on the information,” Owalla told SciDev.Net.
“Our current findings provide critical information on the burden of asymptomatic malaria that we hope one day will be useful to the national malaria control program in Uganda and other malaria-endemic African countries.”
Peter Ofware, Kenya’s country director for the global health and human rights organisation, HealthRight International, says multiple approaches are needed to fight malaria.
“It is encouraging that more vaccine candidates are being introduced, but none so far has achieved the desired efficacy rate,” he told SciDev.Net.
“Any innovations that can lead to better vaccines and treatments are most welcome.”
A new antibiotic class that works against multidrug-resistant bacteria has been discovered, offering new opportunities to tackle these dangerous microbes.
The macrocyclic peptide zosurabalpin showed promising antibacterial activity against Carbapenem-resistant Acinetobacterbaumannii (CRAB), according to two papers published in the journal Nature.
The Gram-negative bacteria is deemed an urgent threat by the U.S. Centers for Disease Control and Prevention and has also been classified as a priority 1 critical pathogen by the World Health Organization.
“The new molecule overcomes the existing drug-resistance mechanisms that the currently available antibiotics are failing to address,” said Kenneth Bradley, global head of infectious disease discovery at Roche pharma research & early development, which worked with Harvard researchers to establish the mechanism of action for the compound.
“With this significant breakthrough, zosurabalpin has the potential to address a major unmet need in the fight against antimicrobial resistance.”
Gram-negative bacteria are particularly difficult to kill because they are encased in both inner and outer membranes that are challenging for most antibiotics to cross. The cytoplasmic membrane is surrounded by an outer membrane containing lipopolysaccharide (LPS), which blocks the entry of most antibiotics.
Zosurabalpin traps this LPS during its transport to the outer membrane by inhibiting a complex of proteins called the LptB2FGC complex.
Specifically, the clinical candidate binds to both LPS and a transport complex that facilitates movement to its destination. The LPS transport complex is trapped in a substrate-bound state, which leaves it unable to move LPS and results in death of the bacterium.
A team led by Claudia Zampaloni, PhD, senior principal scientist in infectious diseases at Roche, initially examined around 45,000 tethered macrocyclic peptides, which have greater molecular weights than most antibiotics.
The researchers identified one that selectively killed A. baumannii, which was further honed for efficacy and tolerability using a new type of test based on blood-plasma compatibility, culminating in the discovery of zosurabalpin.
The drug was effective against more than 100 CRAB clinical samples tested in the lab and in multiple mouse infection models, including sepsis and thigh and lung infection induced by CRAB strains.
In another research article, Karanbir Pahil, PhD, from Harvard University, and colleagues use X-ray techniques to identify structures that show zosurabalpin engages LptB2FGC only when the complex is bound to LPS, indicating the importance of the latter for its action.
The basis for its specificity against A. baumannii lies in this protein complex, explaining why it is ineffective against other bacteria whose Lpt proteins may have different amino-acid sequences.
This previously unknown mode of antibiotic action suggests that pre-existing resistance is unlikely, note Morgan Gugger and Paul Hergenrother, PhD, both from the University of Illinois at Urbana-Champaign, in accompanying News and Views article.
They point out that the U.S. Food and Drug Administration has not approved any new classes of antibiotic for harmful Gram-negative bacteria in more than 50 years.
“Treatment options for CRAB infections continue to dwindle as mortality rates are rising, with some estimated death rates reaching approximately 50% for invasive infections,” they warn.
The commentators add that zosurabalpin might not have the damaging effect on normal gut microbes seen with most antibiotics, given its high specificity for A. baumannii.
“The movement towards bacterium-specific antibiotics is a new development, and one that can be facilitated by diagnostics that can rapidly identify specific harmful bacteria in infected individuals,” they wrote.
“Given that zosurabalpin is already being tested in clinical trials, the future looks promising, with the possibility of a new antibiotic class being finally on the horizon for invasive CRAB infections.”
For this issue of Inside Precision Medicine focused on gender medicine, I was asked to write a piece about overlooked diseases that affect women. This list is long and includes, among others, endometriosis, polycystic ovary syndrome, fibromyalgia, chronic fatigue syndrome, irritable bowel syndrome, and several autoimmune disorders like lupus and multiple sclerosis. However, for reasons that will become clear, I chose to focus on Ehlers-Danlos syndrome (EDS).
EDS is not one disease but a heterogenous group of 13 heritable connective tissue disorders, characterized by joint hypermobility, skin hyper extensibility, and tissue fragility, as classified by the International Consortium on Ehlers-Danlos Syndromes and Related Disorders in 2017. To date, 19 causal genes, mainly involved in collagen and extracellular matrix synthesis and maintenance, have been associated with 12 of these 13 EDS subtypes. In 2018, a 14th subtype, with a novel variation in the AEBP1 gene, was discovered but it has not yet been named and classified.
The only subtype that does not have an associated pathogenic variant is hypermobile (h)EDS. It is also the most common, with an estimated prevalence of around 1 in 3,100 people, as reported by The Ehlers-Danlos Society.
In contrast, 11 of the 14 subtypes (periodontal EDS, kyphoscoliotic EDS, spondylodysplastic EDS, brittle cornea syndrome, arthrochalasia EDS, musculocontractural EDS, classical-like EDS, dermatosparaxis EDS, myopathic EDS, cardiac-valvular EDS, and the AEBP1 subtype) are extremely rare, affecting fewer than one in a million people worldwide. The remaining two, classical EDS and vascular (v)EDS, have a reported prevalence of 1 in 20,000–40,000 and 1 in 100,000–200,000, respectively.
Women are disproportionately represented among people with EDS. They account for more than 70% of cases published in the literature but to date, there is no obvious genetic reason for the gender bias. In the context of this rare disease that primarily affects women, it is not surprising that patients must overcome some huge challenges before receiving a diagnosis.
As EDS is a connective tissue disorder, the affected tissues and organs are spread throughout the body. This can make diagnosis and management difficult. Patients frequently have multiple symptoms such as widespread pain, severe fatigue, easy bruising, fragile skin, joint dislocations, gastrointestinal symptoms like difficulty swallowing, nausea, vomiting, and food intolerance, and autonomic symptoms such as heart palpitations, excessive sweating, and fainting. Therefore, a multidisciplinary approach needed to ensure optimal care.
Lara Bloom CEO, The Ehlers-Danlos Society
Lara Bloom, CEO of The Ehlers-Danlos Society, says that the average wait for diagnosis is still 10 to 12 years, and even longer in developing countries where there is less awareness of EDS. During this time, many patients leave their studies or successful careers because their bodies do not function well enough to allow them to continue. This can impact their financial situations and personal relationships, particularly as without a diagnosis patients’ symptoms may not be taken seriously.
Although there are currently no specific treatments for EDS, there are ways to manage its symptoms. Bloom says “it is a huge disservice to patients when they’re not receiving that management and care, as even the simple validation of being believed goes such a long way and that is still not happening.”
Misdiagnosis plays a large part in a delayed EDS diagnosis. “We still have lots of people with symptoms being blamed on anxiety and depression or hormones and it’s simply not good enough,” says Bloom. “In addition, we are now seeing more people with hypermobile EDS, which historically did not shorten your life expectancy, dying from highly avoidable causes such as suicide or complications with malnutrition from gastrointestinal symptoms that were missed or put down to psychological issues.”
The Ehlers-Danlos Society, people with an EDS, and other patient advocacy groups have adopted the zebra as their symbol. The Ehlers-Danlos Society explains that medical students have been taught for decades that, “when you hear the sound of hooves, think horses not zebras.” In other words, look for the common diagnosis and not the surprising one. Yet sometimes when you hear hooves, it really is a zebra and people with an EDS or hypermobility spectrum disorder (HSD) are those unexpected cases.
Furthermore, no two zebras have identical stripes, just as no two people with an EDS or HSD are the same. They have different symptoms, different types, and different experiences. The Ehlers-Danlos Society says “we are all working towards a time when a medical professional immediately recognizes someone with an Ehlers-Danlos syndrome or HSD, reducing the time to diagnosis and improving pathways to care.”
A recent study by Colin Halverson, PhD, from the Center for Bioethics at Indiana University School of Medicine, and colleagues showed that people with hEDS have an average of ten co-diagnoses, most common of which are anxiety, depression, postural tachycardia syndrome (POTS), and irritable bowel syndrome. However, the study, which included 505 individuals with hEDS (91% women, 97% White) showed that 42% of these diagnoses were not endorsed as accurate by the patients.
The most rejected co-diagnoses were functional neurologic disorders (rejected by 95%), multiple sclerosis (76%), fibromyalgia (67%), bipolar disorder (62%), and ulcerative colitis (58%) and the most endorsed were POTS (91%), cervical instability (90%), mast cell activation syndrome (86%), temporo-mandibular joint disorder (85%), and small fiber neuropathy (83%).
The study participants saw an average of 15.6 clinicians (24% reported that they saw 20 or more) prior to diagnosis, with an average time to diagnosis of 10.4 years. The majority (57%) received their official hEDS diagnosis from a genetics specialist, followed by a rheumatologist (20%) and their primary care physician (5%). Following diagnosis, the average number of clinicians each patient saw dropped to 7.5.
“Because genetic markers have yet to be established to aid in diagnosis of hEDS, building an understanding of the specific phenotypes and of the variations within the presentation of hEDS is a crucial step in improving patient outcomes,” Halverson et al. wrote. They said that the study demonstrated the complexity of hEDS and stressed “the need for an interdisciplinary team approach for the appropriate management and care.”
Compounding the difficulties faced by patients is a lack of targeted funding, which Bloom says is the biggest challenge of all. She points out that in the U.K. there are very few National Health Service (NHS)-funded EDS clinics, while in the U.S. there is limited funding from the National Institutes for Health. “Other than us [The Ehlers-Danlos Society], there’s very few places where you can get funding to study these conditions.” Over the past five years, The Ehlers-Danlos Society has given out $6–8 million in funding, which will allow researchers to “start to etch away at the things that are needed,” says Bloom.
Christina Laukaitis associate professor University of Illinois and the Carle Illinois College of Medicine
Two of the largest projects funded to date are the EDS and HSD Global Registry and the Hypermobile Ehlers Danlos Genetic Evaluation (HEDGE) study. These two projects are important because the lack of reliable genetic causes for hEDS means that diagnosis currently rests on clinical criteria, which can be difficult to distinguish from other HSDs.
“This, in part, likely reflects genetic heterogeneity,” says Christina Laukaitis, MD, an associate professor at the University of Illinois and the Carle Illinois College of Medicine, who will lead analysis of the whole-genome sequencing data obtained for HEDGE with Joel Hirschhorn, PhD, MD, Concordia Professor of Pediatrics and Professor of Genetics at Boston Children’s Hospital and Harvard Medical School.
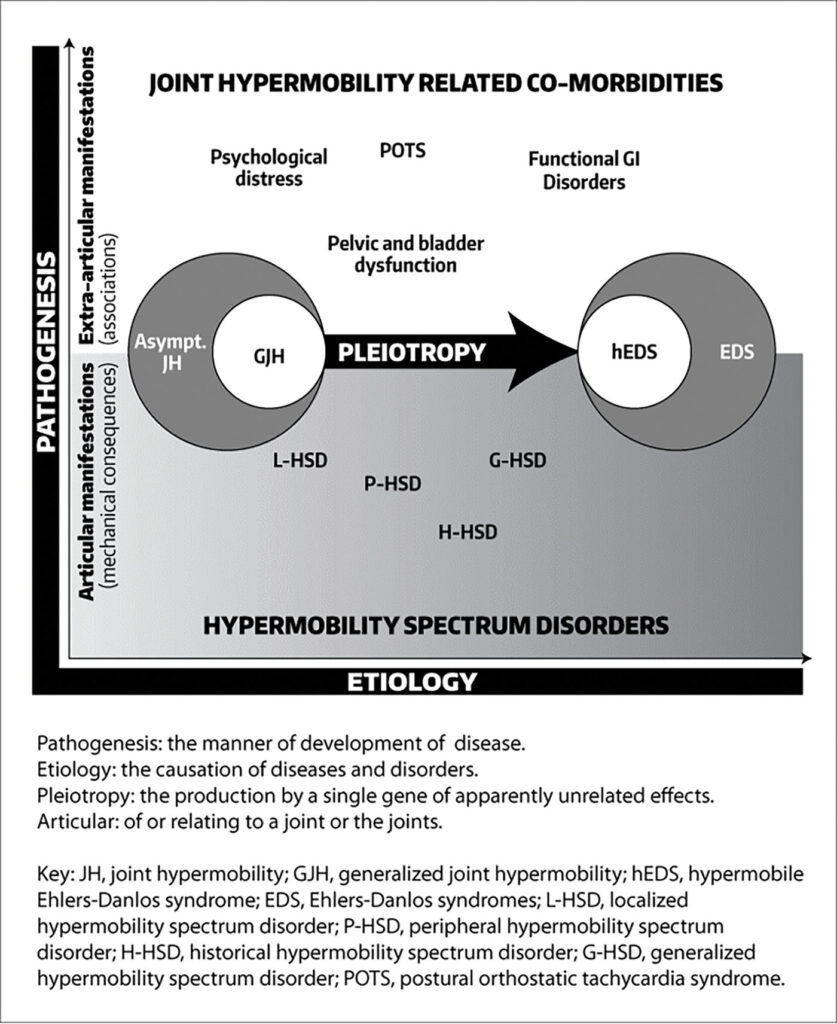
“In addition, there is a clinical spectrum ranging from asymptomatic joint hypermobility, through ‘non-syndromic’ hypermobility with secondary manifestations, to hEDS,” notes Laukaitis.
The concept of a spectrum of pathogenetically related manifestations of joint hypermobility (JH) was introduced by Marco Castori, MD, PhD, and colleagues in 2017. They noted that the 2017 classification criteria for hEDS led to the unification of two disorders—EDS-hypermobility type and JH syndrome—that were originally recognized by different sets of diagnostic criteria. However, this leaves many individuals with symptomatic JH and/or features of hEDS who do not meet the stricter hEDS criteria without an “identity.”
Castori et al. proposed that individuals with JH be classified into one of three groups: those with asymptomatic JH, those with a well-defined syndrome with JH, including hEDS, and those with symptomatic JH that does not meet the criteria for a syndrome. The term HSDs was proposed for people that meet the last criteria.
Although some experts believe that hEDS and HSD are essentially the same condition along a spectrum—with a combined prevalence of 1 in 600 to 900—others believe they are distinct conditions with different genetic causes.
The HEDGE study was launched in 2018 as a worldwide collaborative effort devoted to finding the genetic markers underlying hEDS. Since then, 1,021 people with hEDS from 86 countries have undergone whole genome sequencing, making it the largest study of hEDS genetics to date. The study entered its analysis phase in the spring of 2023, with the final results expected in a year or so.
Laukaitis says the HEDGE researchers are “expecting to find a number of gene candidates” for hEDS. They are also looking at some that were previously proposed along with those already associated with other EDS types. The team will analyze these known genes to not only ensure that people with other types of EDS are not mistakenly categorized in the hEDS cohort, but also find other variations within those genes that could affect the encoded protein differently from the classical mutation.
However, Laukaitis stresses that hEDS is likely not caused by just a single gene. “You know, we’ll be lucky if we have three or four major genes and less than a dozen minor ones. I really expect this to be complicated,” she remarks. “Hopefully, by the time we’re done with HEDGE in 12 months, more or less, we’ll at least have a sense of what the genetic milieu will be, and a number of genes that are ready to go through final validation and start being used clinically.”
Even if candidate genes are identified, Bloom says there will always “be a group within [the EDS] umbrella that do not have a genetic marker that we can find. We still need to make sure that they have the management and treatment that they need and deserve.” She also thinks that hEDS and HSD could “be the most mis- and underdiagnosed condition of our time.”
To aid the understanding of symptoms of these two conditions and other types of EDS, The Ehlers-Danlos Society launched the EDS and HSD Global Registry in 2018. The registry has collected standardized health information from more than 13,000 patients from 16 countries. It will allow researchers to compare and analyze patient data on a much larger scale than has been possible with individual research studies.
Other research groups that have recently received funding from The Ehlers-Danlos Society are the Norris Lab at the Medical University of South Carolina, who will be carrying out a separate study to identify a gene candidate for hEDS, and a group at John Hopkins University led by Harry Dietz, MD, who is trying to understand the mechanism driving vascular fragility and rupture in vEDS with the aim of developing new treatment strategies. Work is also underway at the University of Ghent in Belgium to elucidate the mechanisms causing hEDS using a multiomics approach. In addition, Clair Francomano, MD, is leading a study at the Indiana University School of Medicine to find out whether hormones impact symptom presentation and severity in hEDS.
The Ehlers-Danlos Society also supports research into the rarer subtypes of EDS, like a study to understand the significance of the mutations that cause kyphoscoliotic EDS and studies that look at the impact of EDS on patients’ lives.
In the commercial sector, work on developing treatments for any of the EDS subtypes is limited. Acer Therapeutics is carrying out a Phase III trial of the beta-blocker celiprolol in people with COL3A1-positive vEDS. It is already approved for use in the U.K., but the U.S. Food and Drug Administration (FDA) requires further evidence that the drug reduces the occurrence of vEDS-related clinical events, such as fatal and non-fatal cardiac or arterial events, uterine rupture, intestinal rupture, and/or unexplained sudden death, relative to placebo before granting approval.
A Phase III clinical trial of another potential treatment for vEDS, enzastaurin, was announced by Aytu BioPharma in July 2022. Enzastaurin is a first-in-class small molecule that showed preclinical efficacy in inhibiting a signaling pathway that drives vEDS. Unfortunately, Aytu BioPharma announced in October 2022 that they were suspending all clinical development programs to focus on revenue growth. No patients were treated with enzastaurin and to date, there is no indication as to when the trial might recommence.
Alongside clinical trials and laboratory-based research, The Ehlers-Danlos Society funds the EDS ECHO program, which is based on the “all teach, and all learn” philosophy of Project ECHO®. “Project ECHO is phenomenal,” says Bloom. She explains that it was founded by Sanjeev Arora, MD, in New Mexico to ensure more people had access to best-practice care for hepatitis C. He noticed that patients who did not have access to local care became sicker while waiting to travel to his clinic, so he set up a tele-mentoring program “to move knowledge, not patients,” Bloom notes.
EDS ECHO is a series of programs and courses for healthcare professionals across all disciplines who want to improve their ability to care for people with EDS, HSD, and associated symptoms and conditions. The tele-mentoring platform has already reached nearly 2,000 people across a wide area of the globe, with specific programs for clinicians, fundamentals of the Integral Movement Method, advocacy, allied health professionals, pediatrics, genetics and genomics, vEDS, and nutrition. It allows participants “to learn from experts and is a wonderful way to educate and support the healthcare professionals,” says Bloom.
Bloom believes that now is a transformative time for EDS. “We’re on the horizon of lots of change and discovery,” she says, adding that publications coming in the next few years, including the HEDGE study and data from EDS ECHO, will provide strong foundations for future work and show that “this is not a condition to be disputed any longer.”
Bloom continues, “We can finally move forward with education and what I always say critically is re-education, because there are so many people out there who think they know what EDS and HSD are and that they are benign conditions that just make you a bit bendy, but we know it’s so much more than that.
“It’s impacting people’s lives and you can have a good quality of life with EDS and HSD if you get diagnosed when your symptoms begin, and you have access to long-term management and care because these are chronic conditions. Six weeks of physiotherapy is not going to cut it, we need to truly understand the full picture and the full multisystemic nature and then manage it appropriately.”
Hypermobile EDS: two journeys toward diagnosis
Faye’s story
I first met Faye at an antenatal class 11 years ago. There were eight pregnant women and their partners in the room—she was the only one on crutches who had to leave to vomit after the coffee break. As we all got to know each other, we found out that she was experiencing severe pelvic girdle pain (PGP, which affects around 20% of pregnant women to varying degrees) and hyperemesis gravidarum (occurring in 1–3% of pregnancies) that had landed her in the hospital on several occasions. Although a thoroughly miserable experience, Faye put it down to one of those things. She had always had some quirky health issues and was happy to be focusing on her healthy baby boy.
Fast forward four years: Faye was juggling her full-time job in educational leadership with running around after a little boy when she found out she was pregnant with her second child. At five weeks, the hyperemesis gravidarum started and again, despite being on many medications, resulted in multiple hospitalizations. By the end of the pregnancy, Faye was in a wheelchair due to PGP and agreed to a cesarean section because she was so ill. The operation went well but afterward, Faye physically could not move because of pain in her hips. She was discharged a week later, unable to walk, and spent the next three months in a bed that had been set up in a downstairs room for her. She was still vomiting regularly and it was a year before she could walk properly again, but nobody knew why. It was around this time that she also started experiencing dizziness and blacking out.
It took another two years, multiple appointments, and a change of general practitioner (GP) due to a house move for Faye to get some understanding what was going on. She went to her new GP with fatigue and pain and was referred to a rheumatologist, who she said was the first person to ask her to start from the beginning with a list of all of her symptoms. The rheumatologist asked Faye to touch her toes and perform other exercises, which she now knows make up the Beighton score—a measure of hypermobility—and then diagnosed Faye with Ehlers-Danlos Syndrome.
“I came out of the appointment and cried, because somebody had actually diagnosed me with something that everybody else had been telling me there’s nothing wrong with me and it’s all in my head,” says Faye.
The rheumatologist then discharged her with referrals to multiple specialists: a cardiologist who diagnosed POTS, an orthopedic surgeon to consider foot surgery, a physiotherapist, and a rheumatherapist. Then came diagnoses of postpartum hypothyroidism and osteoarthritis. Faye has also seen or continues to see a dietician, neurologist, an oral medicine specialist, and attends an allergy clinic.
Despite receiving a diagnosis, Faye faces challenges every day. “The rheumatologist [who diagnosed me] changed my life in one way, but killed it off in another way,” she says. She is now categorized as disabled and had to take an extended break from her career, which had financial implications. It impacted her marriage as her husband must now “pick up the slack” when she is too exhausted or in too much pain to do things, and it has given her a very different perspective of the medical profession.
“There is so much gaslighting, people saying I’m making it up or having mental health issues,” she says. One incident was particularly upsetting. Faye had an appointment with an oral medicine specialist to investigate transient blood blisters on her tongue and the inside of her cheeks. On the day of the appointment, she was having a “good day” with few symptoms but explained to the consultant what usually happens, stressing that the blisters were not a result of biting her tongue. After further conversation, he told her he thought she was definitely biting her tongue.
Faye did not have the energy to complain and instead contacted Ehlers-Danlos Support U.K., who put her in touch with a private allergy specialist who diagnosed mast cell activation syndrome (MCAS). She also has idiopathic anaphylaxis, idiopathic edema, and idiopathic urticaria. The treatment she was given by the private specialist for MCAS completely cleared the symptoms, but it was not simple because the “NHS either don’t recognize the condition at this point or won’t pay for the drugs,” resulting in excessive private prescription charges. There is also no one to oversee all her prescriptions, putting her at risk for dangerous drug-drug interactions.
Faye describes the care she has received as a “system of chaos” and says that one thing that could improve her quality of life and treatment is some sort of flag on her medical record that immediately shows all treating physicians that she has hEDS and is under the care of multiple specialists. This does not exist and instead, she carries a large folder of medical letters to every appointment with information on each of her diagnoses and treatments. In addition, there is no specific individual coordinating her care. This is meant to be the responsibility of the GP, but the current difficulties in obtaining GP appointments means that the coordination simply does not happen.
Another frustration is the management of all the medical appointments that she attends. “Sometimes I have an appointment a week, sometimes more, and trying do any sort of work with that is nigh on impossible,” she says. “On top that, you have situations where you receive a letter that says you didn’t attend an appointment, then the next day receive the letter for that appointment. This is followed by another letter saying you’ve been discharged from the service—that you’ve been waiting to see for six months—because you failed to attend the appointment and that happens so much.”
Aside from more organized care, Faye would like to see people with EDS gain access to more proactive support like neurotherapy gyms where the staff “are not scared if you have to sit on the floor every five minutes,” to help with rehabilitation and more education for not only medical professionals but also across schools, particularly among PE teachers.
She appreciates the work that Lara Bloom and The Ehlers-Danlos Society are doing to improve the lives of people affected by EDS but wants more people to be shouting about it. “Just because it’s rare doesn’t mean it’s not important,” she says.
Claire’s story
I met Claire at a baby group around four months after I met Faye. As I got to know her, I was intrigued by the similar experiences the two women had had during pregnancy. Claire also experienced PGP and was hospitalized multiple times with hyperemesis gravidarum, but I put it down to coincidence. I did not know that throughout her life she had experienced numerous symptoms that were characteristic of hEDS.
At primary school she struggled with her handwriting, experiencing joint pain when holding a pen or pencil. In her early teens she was diagnosed with Osgood-Schlatter Disease, a condition that causes pain and swelling below the knee joints, and had to give up competitive sports because of recurrent injuries. In her later teens she experienced fatigue and bowel problems that were put down to a psychological issue and possible glandular fever. She had to repeat exams and delay graduating from her degree in physiotherapy. She was eventually signed off sick from work for 18 months due to what was thought to be post-viral chronic fatigue syndrome.
Claire
“I’d spent years going to the GP and it was always put down to stress; GCSE stress, A-level stress, university stress, new job stress, a stressful long commute to work, then I changed jobs to be closer to home. I didn’t have the commute anymore but still had the symptoms,” she says.
“And then I had a car accident in February of 2016. My life got blown apart, I went from being a busy mum to not being able to do anything. In 2018 I was medically retired in my mid-30s from a job I had wanted to do since I was 14 and needed to use a wheelchair.”
The car accident was not the kind most people would expect to have such an impact. Claire was stationary at traffic lights when a car shunted her from behind into the car in front. She thought she was fine, but that evening began to experience pain and stiffness in her neck that she presumed was whiplash. However, the collision set off a chain of events that ultimately led to the diagnoses of cervical instability (excessive movement in the top two vertebrae of her spine), cerebellar tonsillar ectopia (the brainstem sits on the top of the spinal cord and not in the skull), POTs, and idiopathic angioedema.
Despite this, Claire does not have an official EDS diagnosis. A rheumatologist has said she has benign JH, but this is an outdated term (Castori et al. said in their 2017 framework that its use should be discouraged for the classification of JH and related conditions) and does not account for her other symptoms. A neurocardiologist has spoken to her about EDS and was the only person to go over her full medical history, right back to primary school. But Claire says he was unable to give her a formal diagnosis because it was not his area of specialty and the diagnosis had to come from the rheumatologist.
Claire is not planning to chase that diagnosis even though it would validate her experiences, because people would then ask why she “needs” it and question the underlying mental health reasons. Indeed, at one point a neurologist referred her to a neuropsychiatrist because he believed she had functional neurological disorder. Having worked in healthcare, Claire says she knows that this can be a damaging diagnosis as many clinicians believe that one cannot treat patients with functional neurological disorder because it is “all in their head.” Yet, she could not refuse the referral because that would also go in her notes. When she went to the neuropsychiatrist, the doctor said that she did not need to be there.
“That’s the problem with EDS, you have multiple systems involved and no one pieces it all together, so you end up presenting like a hypochondriac,” Claire says.
She has faced similar problems to those faced by Faye throughout her diagnostic journey and highlights the financial impact a condition like EDS can have on a patient. She lost her income, had to pay to see specialists privately, and even funded her own electric wheelchair because NHS Wheelchair Services could only provide limited support. The NHS said that because her house was too small for her to use the wheelchair indoors, they would only fund an attendant-propelled wheelchair. This meant that she was not allowed to push herself because of her cardiac valve problems and would always be reliant on someone else to push her. All she wanted was to be able to get out and about independently with her daughter. Eventually, her sisters set up a GoFundMe page to raise the £6500 that was needed. They reached the target within 48 hours, which was “humbling and amazing and gave me a life that I couldn’t have had without it.” But Claire had initially rejected the idea. Till then she had kept her medical history fairly private and putting herself “out there” made her feel very vulnerable.
Like Faye, Claire believes that having someone to oversee her multidisciplinary care, be that a case manager, a nurse, or physiotherapist, would make a massive difference. Easier access to acute medication like strong painkillers and muscle relaxants would also help. She now has an understanding GP who is a “rare gem” because she has a “two-way conversation where we deal with it together.” The GP has prescribed Claire a small amount of diazepam to have ready at home if she experiences a torticollis (wryneck), which Claire says makes sense as it means avoiding a trip to hospital. Faye has tried to have something similar arranged for when she experiences joint dislocations, but has not yet been successful.
Claire says she has come to peace with the fact that she will not get back to work as a physiotherapist. She has a part time job that allows her to work from home, but she still feels a bit lost as it is difficult to plan for anything when symptoms fluctuate so much. She manages it with modified exercise, splints for joints when needed due to subluxations, treatment from her husband who is also a physiotherapist, rest, and activity management that has become part of her daily life. She continues to use her wheelchair and other mobility aids as required to manage fatigue and pain and as preventive measures. She says there still needs to be more support for people with EDS. “The medical professionals need to be supporting you and right now the majority are not.”
Brain zaps are sensory disturbances that can feel like electrical shock sensations in the brain. A person may also notice a brief buzzing sound and feel faint or black out momentarily.
Brain zaps can happen when a person decreases or stops using certain medications, particularly antidepressants.
There is no evidence to suggest they are harmful or damage the brain. However, they can be bothersome, disorienting, and disrupt sleep.
There is no medical term for brain zaps, but some experts describe them as a type of sensory disturbance. Sensory disturbances after stopping antidepressants can lead to burning, tingling, electric- or shock-like sensations in the body and brain.
A person may be able to minimize or prevent brain zaps by gradually tapering off their dosage of antidepressants. However, they should always speak with a healthcare professional before stopping their medication or lowering the dosage.
Abruptly stopping an antidepressant may make a person more likely to experience brain zaps and other symptoms.
Brain zaps have no cure, but they usually resolve over time. Once a person’s body has adjusted to the change in antidepressant dosage, brain zaps and some other side effects may decrease.
This article further explains brain zaps, including their causes, how they feel, and when to contact a healthcare professional.
hyperarousal, which may lead to jerkiness and irritability
Brain zaps can occur when a person decreases their dosage or stops taking antidepressants or certain other medications.
They can also happen if an individual forgets to take certain medications on their usual schedule.
Healthcare professionals do not know what exactly causes brain zaps. They are one of many different side effects a person may experience as they change their dosage or stop taking a medication completely.
Together, the symptoms a person may experience are called antidepressant withdrawal syndrome (AWS).
Brain zaps and other symptoms of AWS are common. A 2019 review and meta-analysis found that more than half of people who attempt to decrease their dosage or stop taking antidepressants altogether experience withdrawal symptoms.
Not everyone will experience these symptoms. According to a 2015 review, for some people who do experience symptoms, they may last only a few weeks.
A person should always speak with a healthcare professional if they wish to lower their antidepressant dosage or stop taking it altogether. A healthcare professional can help them safely and gradually taper off the medication.
Some research suggests that brain zaps may occur when a person moves their eyes from side to side during antidepressant withdrawal. However, in many cases, they seem to happen without warning at any time.
The best way to minimize or prevent brain zaps is to taper off medications gradually rather than stopping them abruptly.
However, some evidence has found that tapering does not guarantee that a person will not experience brain zaps or other withdrawal symptoms. However, it can make it easier to cope with the change.
Experts recommend a gradual taper of antidepressants to minimize withdrawal symptoms and ensure that a person maintains good mental health as they stop taking the medication.
In a 2019 review, those who underwent CBT while they tapered off antidepressants were more likely to successfully stop taking the medication than those who tried tapering alone.
It is important for individuals to always check with a healthcare professional before taking any vitamins or other supplements. This is because they may interfere with other medications or cause unpleasant side effects.
People who wish to decrease their dosage or stop taking antidepressants should speak with a healthcare professional. It is important not to stop taking antidepressants or other mental health medications without medical supervision.
If the side effects of antidepressants are intolerable, a doctor may be able to recommend a different medication.
If a person feels that they no longer need the medication, they can work with a healthcare or mental health professional to gradually decrease the dosage.
Although withdrawal symptoms are common, it is important to tell a healthcare professional about them. There may be ways to help minimize withdrawal symptoms and help a person feel better as they go through the process of reducing or stopping their medication.
If a person is experiencing severe symptoms or thoughts of self-harm or suicide, they should seek emergency medical care.
Suicide prevention
If you know someone at immediate risk of self-harm, suicide, or hurting another person:
Ask the tough question: “Are you considering suicide?”
Listen to the person without judgment.
Call 911 or the local emergency number, or text TALK to 741741 to communicate with a trained crisis counselor.
Stay with the person until professional help arrives.
Try to remove any weapons, medications, or other potentially harmful objects.
If you or someone you know is having thoughts of suicide, a prevention hotline can help. The 988 Suicide and Crisis Lifeline is available 24 hours a day at 988. During a crisis, people who are hard of hearing can use their preferred relay service or dial 711 then 988.
Here are some answers to questions people often ask about brain zaps.
How long does a brain zap last?
Usually, brain zaps and other side effects from discontinuing antidepressants stop within a few weeks. If they continue for longer or are bothersome, a person should seek medical advice.
Are brain zaps serious?
Brain zaps do not signal a serious problem, but people and doctors sometimes mistake them for signs of another condition. Being aware that they are a side effect can help a person avoid anxiety.
Are brain zaps a seizure?
Doctors do not know why they occur, but brain zaps are not a seizure. Experts describe the effects of antidepressant discontinuation syndrome as vague and nonspecific.
Brain zaps can occur when a person decreases or stops using certain medications, particularly antidepressants. They can be bothersome but do not cause damage to the brain.
While antidepressant withdrawal can be challenging, the symptoms will usually resolve on their own after a few weeks.
An individual should work with a healthcare professional to find the right dosage and always take their medication exactly as recommended. If side effects or withdrawal symptoms interfere with daily life, it is important to inform a healthcare professional.
Textile research has highlighted the advances in electroluminescent threads as suitable biomaterials for driving growth in the wearable electronics market. While the direct embroidery of textiles with custom designs and patterns can offer substantial benefits, machine embroidery can challenge the integrity of these threads.
emitting textiles for diverse flexible and
In a new report of applied science and engineering published in Science Advances, Seungse Cho and a team of scientists in biomedical engineering and medicine in the U.S., present embroiderable, multicolor, electroluminescent threads in blue, green, and yellow, that show compatibility with standard embroidery methods.
The researchers used the threads to stitch decorative designs onto a variety of consumer fabrics, without compromising their wearability or light-emitting capacity. The scientists illuminated specific messages or designs on the consumer products for the purpose of developing emergency alerts on helmet liners and as physical hazard signs.
The outcomes deliver a comprehensive toolkit to integrate light-emitting textiles into trendy customized crafts that can even be tailored for leisure wear, with diverse and flexible options.
Light-emitting wearables
Light-emitting textiles have gained increased attention due to their capacity to create dynamic and interactive lighting effects to make them well-suited as wearable fashion in health care and for display purposes. Light-emitting diodes and other light sources such as electroluminescent thin films can be glued directly onto garments of interest. However, such approaches can still affect the inherent properties of the fabric, such as flexibility, wearability, and washability.
Recent advances in electroluminescent threads that can be woven or knitted have facilitated the integration of light-emitting textiles on a large-scale to include vast arrays of lighting lines or pixels. A versatile tool that can include light-emitting textiles into fashionable and customized crafts directly onto consumer fabrics remains to be implemented to suit wide-ranging applications. Physical and optical characterizations of EL threads. (A) Shear rate dependence of the viscosity of ZnS phosphor/TPU slurries. (B) Weight ratio dependence of thread diameter with respect to ZnS phosphors and TPU. Error bars represent SD, n = 3 for each group. (C) Load-strain curves comparison of a plain thread and the EL threads with different weight ratios of ZnS phosphors and TPU. (D) Surface roughness comparison of a plain thread and the EL threads with different weight ratios of ZnS phosphors and TPU. (E) Weight ratio dependence of EL intensity of the EL threads with respect to ZnS phosphors and TPU. Error bars represent SD, n = 3 for each group. (F) Luminance distribution around the circumference of the EL threads. Error bars represent SD, n = 3 for each group. a.u., arbitrary units. Credit: Science Advances, doi: 10.1126/sciadv.adk4295
While embroidery and machine embroidery aim to deliver fast and precise knitting and weaving for large-scale production. The electroluminescent threads remain to meet the machine embroidery requirements due to their high tensile strength and a smooth surface.
In this work, Cho and team presented embroiderable multicolor electroluminescent threads in blue, green, and yellow, which showed compatibility with universal embroidery machines to stitch decorative designs on a variety of consumer fabrics. These threads were durable against folding, stretching, and machine washes, to satisfy the necessities of machine embroidery. Cho and team presented a range of machine-crafted, light-emitting textiles, for pragmatic applications in display messages and to design functional emergency signals.
The scientists covered the production of embroiderable multicolor electroluminescent threads with subsequent machine embroidery inserted into the light-emitting textiles. At the onset, they coated the electroluminescent layer with a mixture of zinc sulfide phosphors and thermoplastic polyurethane across the surface of a conductive, embroiderable thread.
They conducted the process using a household manual winder and a tapered nozzle tip to achieve a maximum coating rate. The team applied the electroluminescent layer across the threads and used doped zinc sulfide phosphors with copper and manganese for the blue, green, and yellow light.
The researchers prepared a transparent conductive fiber by coating a transparent, embroiderable nylon fiber with silver nanowires using an adhesion promoter made of ethyl acetate and resorcinol. The team chose silver nanowires for their low electrical resistance, high optical transmittance, and mechanical flexibility. Overall structure and characterization of light-emitting pixels. (A) Schematic representation, side-view, and top-view photographs of a light-emitting pixel created at the point of contact between the EL thread and TCF. (B) Photographs of the light-emitting pixels at various stitch distances and angles. (C) Relative EL intensity of the light-emitting pixels in relation to the stitch distance and angle between the EL thread and TCF. Error bars represent SD, n = 3 for each group. (D) Relative EL intensity of the light-emitting pixels as a function of upper thread tension. Error bars represent SD, n = 3 for each group. (E) Relative EL intensity of the light-emitting pixels under repetitive pressing and releasing cycles. Credit: Science Advances, doi: 10.1126/sciadv.adk4295
Physical and optical characterization of electroluminescent threads and light-emitting pixels
The electroluminescent threads met specific requirements including consistent coverage, a tensile strength of greater than 6 Newton and moderate elongation with a surface finish with minimal roughness. The scientists prepared the electroluminescent layers with different weight ratios of zinc sulfide phosphors and thermoplastic polyurethane.
When the shear rate increased, the electroluminescent layers showed shear-thinning behavior as their viscosity decreased. Cho and team noted the overall structure and characterized the light-emitting pixels to present a schematic illustration and a representative microscopic image of a light-emitting pixel that contained an electroluminescent thread at the bottom and a transparent conductive fiber at the top.
The relative change in the electroluminescent intensity of the light-emitting pixels remained constant across these cases. The scientists used a live streaming demonstration to show how the light-emitting pixels on a rug remained intact even after stepping on its surface, to facilitate an on/off switch on the material by an adult with a robust weight.
Light emission characteristics
The scientists varied the alternating current voltage to show its influence and frequency on the electroluminescence. The increased frequency at a fixed voltage gradually increased the light-emission intensity to obtain a variable luminance. The scientists conducted multiple laundry cycles on the light-emitting pixels, while also conducting stretching and folding actions.
During the wash, the researchers included a commercial liquid detergent in autosensing mode for 45 minutes in a spin-rinse-and-spin-drying cycle. The light-emitting pixels showed minimal temperature changes for more than six hours during the wash cycle to highlight their suitability for long-term continuous use.
Proof-of-concept
To demonstrate the capacity of wearable displays, the scientists embroidered a 6 x 3 array of light-emitting pixels onto a commercial helmet liner as a football helmet equipped with an impact sensor. They aimed to detect potentially severe head impacts to alert the wearer of a potential concussion, with a real-time warning system. Such wearables can prevent and manage traumatic brain injury prevalent in collision sports, for the early detection and treatment of potential head impacts or concussions.
The measurement setup contained a football helmet equipped with an accelerometer, microcontroller, relay, and power supplier. The construct also maintained a stretchable helmet liner with light emitting pixels, for real-time detection of impact severity.
Cho and team applied mechanical impacts to a mannequin head with a dumbbell and classified the severity as mild, moderate, to severe. The experiments showed how the mechanical impact on the head could be visualized to detect early concussion management in sports or in situations that include the risk of danger in daily life.
Outlook
In this way, Seungse Cho and colleagues present a versatile concept for crafting light-emitting textiles with multicolor electroluminescent threads and transparent conductive fiber that are compatible with standard embroidery machines. These strings were thinner and more durable for machine embroidery with adjustable colors, luminescent intensities, and pixel positions to attain higher versatility and creative potential to meet an array of applications.
The proof-of-concept, light-emitting textiles emphasize the integration of safer power mechanisms, and insulation strategies to ensure the safety and practicality of the wearable electronics.
The team suggests the inclusion of a circuit driver specifically tailored for power supply—to meticulously regulate the voltage, frequency, and waveform. This setup can be used to display real-time measurements of collisions as an ideal solution for health-related applications and to visualize data.
Hop in the car to meet your lover for dinner and a flood of dopamine— the same hormone underlying cravings for sugar, nicotine and cocaine—likely infuses your brain’s reward center, motivating you to brave the traffic to keep that unique bond alive. But if that dinner is with a mere work acquaintance, that flood might look more like a trickle, suggests new research by University of Colorado Boulder neuroscientists.
“What we have found, essentially, is a biological signature of desire that helps us explain why we want to be with some people more than other people,” said senior author Zoe Donaldson, associate professor of behavioral neuroscience at CU Boulder.
The study, published Jan. 12 in the journal Current Biology, centers around prairie voles, which have the distinction of being among the 3% to 5% of mammals that form monogamous pair bonds.
Like humans, these fuzzy, wide-eyed rodents tend to couple up long-term, share a home, raise offspring together, and experience something akin to grief when they lose their partner.
By studying them, Donaldson seeks to gain new insight into what goes on inside the human brain to make intimate relationships possible and how we get over it, neurochemically speaking, when those bonds are severed.
The new study gets at both questions, showing for the first time that the neurotransmitter dopamine plays a critical role in keeping love alive.
“As humans, our entire social world is basically defined by different degrees of selective desire to interact with different people, whether it’s your romantic partner or your close friends,” said Donaldson. “This research suggests that certain people leave a unique chemical imprint on our brain that drives us to maintain these bonds over time.”
How love lights up the brain
For the study, Donaldson and her colleagues used state-of-the art neuroimaging technology to measure, in real time, what happens in the brain as a vole tries to get to its partner. In one scenario, the vole had to press a lever to open a door to the room where her partner was. In another, she had to climb over a fence for that reunion.
Meanwhile a tiny fiber-optic sensor tracked activity, millisecond by millisecond, in the animal’s nucleus accumbens, a brain region responsible for motivating humans to seek rewarding things, from water and food to drugs of abuse. (Human neuroimaging studies have shown it is the nucleus accumbens that lights up when we hold our partner’s hand).
Each time the sensor detects a spurt of dopamine, it “lights up like a glow stick,” explained first-author Anne Pierce, who worked on the study as a graduate student in Donaldson’s lab. When the voles pushed the lever or climbed over the wall to see their life partner, the fiber “lit up like a rave,” she said. And the party continued as they snuggled and sniffed one another.
In contrast, when a random vole is on the other side of that door or wall, the glow stick dims.
“This suggests that not only is dopamine really important for motivating us to seek out our partner, but there’s actually more dopamine coursing through our reward center when we are with our partner than when we are with a stranger,” said Pierce.
Hope for the heartbroken
In another experiment, the vole couple was kept apart for four weeks—an eternity in the life of a rodent—and long enough for voles in the wild to find another partner.
When reunited, they remembered one another, but their signature dopamine surge had almost vanished. In essence, that fingerprint of desire was gone. As far as their brains were concerned, their former partner was indistinguishable from any other vole.
“We think of this as sort of a reset within the brain that allows the animal to now go on and potentially form a new bond,” Donaldson said.
This could be good news for humans who have undergone a painful break-up, or even lost a spouse, suggesting that the brain has an inherent mechanism to protect us from endless unrequited love.
The authors stress that more research is necessary to determine how well results in voles translate to their bigger-brained, two-legged counterparts. But they believe their work could ultimately have important implications for people who either have trouble forming close relationships or those who struggle to get over loss—a condition known as Prolonged Grief Disorder.
“The hope is that by understanding what healthy bonds look like within the brain, we can begin to identify new therapies to help the many people with mental illnesses that affect their social world,” said Donaldson.
Researchers at the Scripps Research Institute, Florida, have developed a new method to counteract α-synuclein protein levels by targeting the mRNA that forms them. The strategy unlocks many research doors with potential therapeutic approaches for addressing neurodegenerative diseases.
In a paper, “Decreasing the intrinsically disordered protein α-synuclein levels by targeting its structured mRNA with a ribonuclease-targeting chimera,” published in PNAS, the team introduces Synucleozid-2.0 and Syn-RiboTAC, an mRNA binding and degradation duo that allowed modulation of the highly undruggable protein, α-synuclein, by targeting its encoding mRNA.
Neurodegenerative diseases, especially Parkinson’s disease (PD), pose significant therapeutic challenges due to the difficulty in targeting specific proteins like α-synuclein, which have increased levels associated with disease progression.
Conventional methods, such as antibodies or antisense oligonucleotides, are limited when targeting intrinsically disordered proteins like α-synuclein as they lack stable three-dimensional structures, typical small-molecule binding sites or pockets, which are often the conventional targets for drug compounds.
By creating a method to target the encoding mRNA structure before it forms the protein, the researchers created a tool that can bypass the difficulty of targeting the fully formed protein by limiting its initial production levels.
In PD patient-derived neurons, Syn-RiboTAC indirectly restored the expression of around half of the dysregulated genes. The reduction in α-synuclein levels likely allowed for the restoration of some dysregulated genes disrupted by its abnormal accumulation. The downstream effects of α-synuclein reduction could also alleviate cellular stresses, allowing cells to regain normal function and gene expression patterns.
The results are a breakthrough, illustrating that traditionally “undruggable” proteins like α-synuclein can be targeted via mRNA binding, expanding the druggability of disease-related proteins through small molecule binders and degraders.
As PD currently has no cure, effective symptom relief treatments are needed to maintain quality of life. The new strategy requires further research in a clinical therapeutic setting where many unmet medical needs urgently await expanded druggability of currently undruggable proteins.
Researchers at Zhejiang University School of Medicine, China, have investigated how the body’s innate immune system of renal macrophages works to prevent kidney stones. In a paper, “Renal macrophages monitor and remove particles from urine to prevent tubule obstruction,” published in Immunity, the authors detail their findings of mechanistic actions and strategic positioning of macrophages to surveil epithelial cells and intratubular environments.
When urine passes through the tubular system of the kidneys, it generates various microscopic sediment particles, including mineral crystals, from the concentrated urine. Pathological conditions can lead to the presence of proteins and inflammatory cells. These particles can become lodged in the tubules, blocking urine flow and causing renal dysfunction.
The researchers observed renal macrophages adjacent to the tubules in real-time, using high-resolution microscopy, live recordings and two-photon microscopy techniques. They were able to record macrophages extending transepithelial protrusions and interacting with intratubular particles, as well as their migration to assist in the excretion of urine particles.
These techniques captured the association of macrophages with particles in urine and demonstrated the role of macrophages in particle removal. Renal macrophages located near medullary tubules display specific behaviors, extending transepithelial protrusions and constantly sampling urine contents.
The macrophages were then seen to migrate and surround intratubular particles, aiding in their removal from the tubular system. Mice were injected with fluorescent inert latex beads into the kidney, and within 12 hours, free beads were almost absent from the lumen of the collecting ducts.
To confirm the role of the macrophages, the latex bead experiment was repeated with mice lacking renal macrophages. Macrophage-depleted mice showed increased retention of the fluorescent beads even after 36 hours despite the more prolonged exposure to natural urine flushing.
This result suggests that normal urine flushing alone could not efficiently remove big particles in the renal tubule system without the macrophage pre-disposal assistance.
The findings suggest potential therapeutic implications for kidney stones (nephrolithiasis or renal calculi) and for developing kidney-specific drug delivery methods based on these distinctive macrophage features.
AD subtype comparisons on MRI and clinical outcomes. a, Median hippocampal volume as the percentage of total intracranial volume (TIV) compared to subtypes in the dementia stage. b, Choroid plexus volume as the percentage of TIV compared to subtypes in the dementia stage. c, Cortical atrophy associated with AD subtypes in the dementia stage compared to controls. d, Clinical progression from MCI to dementia according to subtype and time from dementia to death according to subtypes (right). Credit: Nature Aging (2024). DOI: 10.1038/s43587-023-00550-7
A large team of neuroscientists and neurodegenerative disease specialists affiliated with multiple entities across the Netherlands, working with colleagues from the U.S., Belgium, the U.K. and Sweden, has found five categories of fluid surrounding the brain in Alzheimer’s patients. Their study is published in the journal Nature Aging.
Prior research has shown that people who develop Alzheimer’s disease have differences in protein levels in their cerebrospinal fluid compared to people without the disease—differences associated with certain molecular processes in the brain. In this new effort, the research team discovered differences in protein levels among patients who had the disease.
The work involved studying 1,058 proteins in cerebrospinal fluid from 419 patients and 187 control volunteers known to be different for Alzheimer’s patients when they noticed some patterns developing. The patterns, they found, could be divided into five distinct subtypes, suggesting that there may be five distinct types of Alzheimer’s disease. They named the subtypes 1 through 5.
More specifically, the researchers found that patients with subtype 1 had altered levels of proteins associated with hyperplasticity in addition to increased levels of amyloid production. Those with subtype 2 had proteins associated with innate immune activation associated with excessive pruning of microglia synapses and proteins. Subtype 3 patients showed signs of RNA dysregulation, while subtype 4 patients showed signs of choroid plexus (where cerebrospinal fluid is made) dysfunction. And subtype 5 patients had impairments in the blood-brain barrier along with reduced levels of amyloid production.
The research team noted that each of the subtypes also had a unique associated genetic profile. They also suggest that if Alzheimer’s disease has five major types, it could explain why finding therapies to treat it has met with so little success, pointing out that a different therapy may be needed for each subtype. They further suggest that treatment for future Alzheimer’s patients might begin by first testing their cerebrospinal fluid and identifying their subtype.











{kind=link}