People with chronic tinnitus were more likely to have signs of damage to their cochlear nerve than people without the condition.
Therapies to regenerate this nerve, which helps route information from the ear to the brain, may hold promise for treating tinnitus in the future.
The study gives new insight into the causes of tinnitus. DimaBerlin / Shutterstock
More than 10% of adults worldwide will experience tinnitus during their lifetimes. For many people, this condition—a ringing, roaring, clicking, hissing or buzzing in the ears—is a temporary nuisance. But for others, it can be permanent and debilitating. Tinnitus may lead to sleep deprivation, anxiety, depression, and other symptoms that can damage quality of life.
The causes of tinnitus are not well understood, and there’s currently no cure. Most people with tinnitus have some degree of hearing loss. One theory of tinnitus suggests that, when hearing is damaged, the brain becomes hyperactive, leading to the perception of phantom sounds. But many people with tinnitus appear to have normal hearing on an audiogram test.
To look more closely at the association between tinnitus and nerve activity, a research team led by Dr. Stéphane Maison from Mass Eye and Ear recruited almost 300 people who had normal hearing results on an audiogram test.
The participants were sorted into one of three groups based on their self-reports of tinnitus. These included 201 people with no tinnitus (beyond the occasional phantom sound that resolved quickly); 64 people with intermittent tinnitus (defined as being continuous but lasting for less than 6 months at a time); and 29 people who had been experiencing chronic tinnitus for more than 6 months.
The researchers performed a range of testing on the participants. This testing covered numerous aspects of sound processing, from the sensory hair cell responses in their inner ears to the auditory reflexes of their brainstems. The study, which was funded in part by NIH, was published on November 30, 2023, in Scientific Reports.
The team found that people with chronic tinnitus were much more likely to have reduced responses to sound in their cochlear nerve compared with people in the other two groups. This nerve, which is also called the auditory nerve, carries sound information from the sensory hair cells to the brain. People with chronic tinnitus also had a weaker reflex in response to sound in the muscles of the middle ear.
Those with chronic tinnitus, however, were more likely to have increased activity in related nerves in the brainstem. This combination of findings supports the idea that reduced functioning in the cochlear nerve may lead to increased activity in the brain to cause phantom sounds.
“Our work reconciles the idea that tinnitus may be triggered by a loss of auditory nerve, including in people with normal hearing,” Maison says.
As not all people who experience cochlear nerve damage develop tinnitus, more research is needed to understand other contributors to the condition. Maison and his team plan to explore approaches to boost regeneration of the auditory nerve as a potential treatment for tinnitus.
Obesity is a disease in which a person has an unhealthy amount and/or distribution of body fat (1). Compared with people of healthy weight, those with overweight or obesity are at greater risk for many diseases, including diabetes, high blood pressure, cardiovascular disease, stroke, and at least 13 types of cancer, as well as having an elevated risk of death from all causes (2–5).
To determine if someone has obesity, researchers commonly use a measure known as the body mass index (BMI). BMI is calculated by dividing a person’s weight (in kilograms) by their height (in meters) squared (commonly expressed as kg/m2). BMI provides a more accurate measure of obesity than weight alone, and for most people it is a good (although imperfect) indicator of body fatness.
The National Heart Lung and Blood Institute has a BMI calculator for adults. The standard weight categories based on BMI for adults ages 20 years or older are:
Measurements that reflect the distribution of body fat are sometimes used along with BMI as indicators of obesity and disease risks. These measurements include waist circumference, waist-to-hip ratio (the waist circumference divided by the hip circumference), waist-to-height ratio, and fat distribution as measured by dual-energy X-ray absorptiometry (DXA or DEXA) or imaging with CT or PET.
These measures are used because the distribution of fat is increasingly understood to be relevant to disease risks. In particular, visceral fat—fat that surrounds internal organs—seems to be more dangerous, in terms of disease risks, than overall fat or subcutaneous fat (the layer just under the skin).
How common are obesity and severe obesity?
Obesity and severe obesity have become more common in the United States in recent years (7).
In 2011, 27.4% of adults ages 18 or older had obesity or severe obesity.
By contrast, in 2020, 31.9% of adults ages 18 or older had obesity or severe obesity.
The percentage of children and adolescents ages 2–19 years with obesity or severe obesity has also increased (6).
In 2011–2012, 16.9% of 2–19-year-olds had obesity and 5.6% had severe obesity.
By contrast, in 2017–2018, 19.3% of 2–19-year-olds had obesity and 6.1% had severe obesity.
According to the CDC, the prevalence of obesity in the United States differs among racial and ethnic groups (7). In 2020, the proportions of adults ages 18 years or older with obesity or severe obesity were:
Non-Hispanic Black, 41.6%
American Indian/Alaska Native, 38.8%
Hawaiian/Pacific Islander, 38.5%
Hispanic, 36.6%
Non-Hispanic White, 30.7%
Asian, 11.8%
In 2017–2018, the proportions of obesity among children and adolescents ages 2–19 years were (6):
What is known about the relationship between obesity and cancer?
Nearly all of the evidence linking obesity to cancer risk comes from large cohort studies, a type of observational study. However, data from observational studies cannot definitively establish that obesity causes cancer. That is because people with obesity or overweight may differ from people without these conditions in ways other than their body fat, and it is possible that these other differences—rather than their body fat—explain their increased cancer risk.
1.6 times as likely in people with obesity 1.2 times as likely in people with overweight
Breast Postmenopausal (23, 24) Premenopausal** (24,25)
1.2–1.4 times as likely in people with obesity or overweight 1.2 times as likely for every 5-unit increase in BMI 0.8 times as likely in people with obesity or overweight
1.3 times as likely in people with obesity 1.26 times as likely in people with overweight
BMI = body mass index. *Risk for type I endometrial cancer **Hormone receptor–positive premenopausal breast cancer ***Higher BMI is associated with a slight increase in the risk of ovarian cancer overall, particularly in women who have never used menopausal hormone therapy (26). The association differs by ovarian cancer subtypes, with strongest risk increases observed for rare, non-serous subtypes (27).
People who have a higher BMI at the time their cancer is diagnosed (29) or who have survived cancer (30, 31) have higher risks of developing a second, unrelated cancer (a second primary cancer).
How might obesity increase the risk of cancer?
Several possible mechanisms have been suggested to explain how obesity might increase the risks of some cancers (32, 33).
Fat tissue (also called adipose tissue) produces excess amounts of estrogen, high levels of which have been associated with increased risks of breast, endometrial, ovarian, and some other cancers.
People with obesity often have increased blood levels of insulin and insulin-like growth factor-1 (IGF-1). High levels of insulin, a condition known as hyperinsulinemia, is due to insulin resistance and precedes the development of type 2 diabetes, another known cancer risk factor. High levels of insulin and IGF-1 may promote the development of colon, kidney, prostate, and endometrial cancers (34).
People with obesity often have chronic inflammatory conditions such as gallstones or non-alcoholic fatty liver disease. These conditions can cause oxidative stress, which leads to DNA damage (35) and increases the risk of biliary tract and other cancers (36).
Fat cells produce hormones called adipokines that can stimulate or inhibit cell growth. For example, the level of an adipokine called leptin in the blood increases with increasing body fat, and high levels of leptin can promote aberrant cell proliferation. Another adipokine, adiponectin, is less abundant in people with obesity than in people with a healthy weight and may have antiproliferative effects that protect against tumor growth.
Fat cells may also have direct and indirect effects on other cell growth and metabolic regulators, including mammalian target of rapamycin (mTOR) and AMP-activated protein kinase.
Other possible mechanisms by which obesity could affect cancer risk include impaired tumor immunity and changes in the mechanical properties of the scaffolding tissue that surrounds developing tumors (37).
In addition to biological effects, obesity can lead to difficulties in screening and management. For example, women with overweight or obesity have an increased risk of cervical cancer compared with women of healthy weight, likely due to less effective cervical cancer screening in these individuals (38).
How many cancer cases may be due to obesity?
A nationwide cross-sectional study using BMI and cancer incidence data from the US Cancer Statistics database estimated that each year in 2011 to 2015 among people ages 30 and older, about 37,670 new cancer cases in men (4.7%) and 74,690 new cancer cases in women (9.6%) were due to excess body weight (overweight, obesity, or severe obesity) (39). The percentage of cases attributed to excess body weight varied widely across cancer types and was as high as 51% for liver or gallbladder cancer and 49.2% for endometrial cancer in women and 48.8% for liver or gallbladder cancer and 30.6% for esophageal adenocarcinoma in men.
Globally, a 2019 study found that in 2012, excess body weight accounted for approximately 3.9% of all cancers (544,300 cases), with the burden of these cancer cases higher for women (368,500 cases) than for men (175,800 cases) (40). The proportion of cancers due to excess body weight varied from less than 1% in low-income countries to 7% or 8% in some high-income Western countries and in Middle Eastern and Northern African countries.
Does losing weight lower the risk of cancer?
Most of the data about whether losing weight reduces cancer risk comes from cohort and case–control studies. Observational studies of obesity and cancer risk should be interpreted with caution because they cannot definitively establish that obesity causes cancer and people who lose weight may differ in other ways from people who do not.
Some of these studies have found decreased risks of breast, endometrial, colon, and prostate cancers among people with obesity who had lost weight. For example, in one large prospective study of postmenopausal women, intentional loss of more than 5% of body weight was associated with lower risk of obesity-related cancers, especially endometrial cancer (41). However, unintentional weight loss was not associated with cancer risk in this study.
A follow-up study of weight and breast cancer in the Women’s Health Initiative (42) found that, for women who were already overweight or obese at the beginning of the study, weight change (either gain or loss) was not associated with breast cancer risk during follow-up. However, in a study that pooled data from 10 cohorts, sustained weight loss was associated with lower breast cancer risk among women 50 years and older (43).
To better understand the relationship between weight loss among people with obesity and cancer risk, some researchers are examining cancer risk in people with obesity who have undergone bariatric surgery (surgery performed on the stomach or intestines to provide maximum and sustained weight loss). Studies have found that bariatric surgery among people with obesity, particularly women, is associated with reduced risks of cancer overall (44); of hormone-related cancers, such as breast, endometrial, and prostate cancers (45); and of obesity-related cancers, such as postmenopausal breast cancer, endometrial cancer, and colon cancer (46).
How does obesity affect cancer survivors?
Most of the evidence about obesity in cancer survivors comes from people who were diagnosed with breast, prostate, or colorectal cancer. Research indicates that obesity may worsen several aspects of cancer survivorship, including quality of life, cancer recurrence, cancer progression, prognosis (survival), and risk of certain second primary cancers (29, 30, 47, 48).
For example, obesity is associated with increased risks of treatment-related lymphedema in breast cancer survivors (49) and of incontinence in prostate cancer survivors treated with radical prostatectomy (50). In a large clinical trial of patients with stage II and stage III rectal cancer, those with a higher baseline BMI (particularly men) had an increased risk of local recurrence (51). Death from multiple myeloma is 50% more likely for people with the highest levels of obesity compared with people at healthy weight (52).
Is weight loss after a cancer diagnosis beneficial for people with overweight or obesity?
Most studies of this question have focused on breast cancer. Several randomized clinical trials in breast cancer survivors have reported weight loss interventions that resulted in both weight loss and beneficial changes in biomarkers that have been linked to the association between obesity and prognosis (53, 54).
However, there is little evidence about whether weight loss reduces the risk of breast cancer recurrence or death (55). The NCI-sponsored Breast Cancer WEight Loss (BWEL) Study, an ongoing randomized phase III trial, is examining whether participating in a weight loss program after breast cancer diagnosis affects invasive disease-free survival and recurrence in overweight and obese women (56).
What research is being done on obesity and cancer?
Many studies are exploring mechanisms that link obesity and cancer (34, 57). One research area involves understanding the role of the microbes that live in the human gastrointestinal tract (collectively called the gut microbiota, or microbiome) in both type 2 diabetes and obesity. Both diseases are associated with dysbiosis, an imbalance in the community of these microbes. For example, the gut microbiomes of people with obesity differ from and are less diverse than those of people of healthy weight. Imbalances in the gut microbiota are associated with inflammation, altered metabolism, and genotoxicity, which may in turn be related to cancer.
Researchers are also studying how obesity alters the tumor microenvironment, which may play a role in cancer progression. For example, studies in mouse models show that obesity (induced by feeding mice a high-fat diet) creates a competition for lipids between tumor cells and T cells that makes the T cells less effective at fighting the cancer (58).
Another area of investigation is the role of insulin receptor signaling in cancer. Many cancer cells express elevated levels of IR-A, a form of the insulin receptor that has a high affinity for insulin and related growth factors. Researchers are investigating how these factors contribute to metabolic disease and cancer and whether they may be useful targets for therapeutic interventions to prevent obesity-related cancers.
Investigators are also exploring whether the associations of obesity with cancer risk and outcomes vary by race or ethnicity (59). Also, researchers are investigating whether different cutoffs for overweight and obesity should be used for different racial/ethnic groups. For example, the World Health Organization (WHO) has suggested the alternate thresholds of 23.0 and 27.5 kg/m2 for overweight and obesity for people of Asian ancestry (60).
The NCI Cohort Consortium is an extramural–intramural partnership that combines more than 50 prospective cohort studies from around the world with more than seven million participants. The studies are gathering information on body mass index, waist circumference, and other measures of adiposity from each cohort. The large size of the consortium will allow researchers to get a better sense of how obesity-related factors relate to less common cancers, such as cancers of the thyroid, gallbladder, head and neck, and kidney.
NCI supports research on obesity and cancer risk through a variety of activities, including large cooperative initiatives, web and data resources, epidemiologic and basic science studies, and dissemination and implementation resources. For example, the Transdisciplinary Research on Energetics and Cancer (TREC) initiative supports ongoing training workshops for postdocs and early career investigators to enhance the ability to produce innovative and impactful transdisciplinary research in energetics and cancer and clinical care. The Trans-NCI Obesity and Cancer Working Group promotes the exchange of information and cross-cutting interests in obesity and cancer research within NCI by identifying and sharing state-of-the-science knowledge about obesity and cancer to document what is known and what is needed to move the science forward.
Researchers found that high levels of dietary fructose alter the gut to increase nutrient absorption in mice.
The results suggest a link between high fructose consumption, obesity, and certain cancers.
Research is revealing how fructose can affect villi—the fingerlike projections that line the inside of the small intestine—to raise the risk of obesity and related cancers. SciePro / Shutterstock
Moderate amounts of the sugar fructose, like those found in fruits, are taken up and broken down by intestinal cells. But increased use of sweeteners containing fructose has led to a large rise in its consumption. The major sources of fructose in the American diet are now sugar-sweetened beverages and ultra-processed foods. Increased fructose consumption has been linked to a rise in obesity and related cancers such as colorectal cancer. But how fructose may contribute to these conditions is unclear.
A team of researchers led by Dr. Marcus Goncalves at Weill Cornell Medicine explored the effects of dietary fructose on cells in the gut. NIH’s National Cancer Institute (NCI), National Institute for Allergy and Infectious Diseases (NIAID), and National Institute of General Medical Sciences (NIGMS) supported the research. Results appeared in Nature on August 18, 2021.
Fingerlike projections called villi line the inside of the small intestine. The researchers found that mice fed high-fructose corn syrup for four weeks had villi that were 25-40% longer than those in control mice. Villi help absorb nutrients from food by increasing the surface area of the intestinal walls. The researchers hypothesized that longer villi would lead to increased nutrient absorption. This could lead to increased fat absorption and weight gain when combined with a high-fat diet.
To test this, the researchers fed mice a diet in which almost half of the calories came from fat. Some mice were given fructose in their diet, while the rest had none. The mice that ate fructose had longer villi and absorbed more fats from their diet than those not eating fructose. They also gained significantly more weight and fat mass.
As a villus grows, new cells form at the base and migrate towards the tip. As the cells move towards the tip, away from blood vessels, they receive less oxygen. Cell death from oxygen deprivation, or hypoxia, at the villus tip limits the length of the villus. But the researchers found evidence that fructose lengthened the villi by improving the survival of cells at the tips.
To learn more, the researchers examined the effects of fructose on hypoxic human colorectal cancer cells. Upon entering cells, fructose is converted into fructose-1-phosphate (F1P). The researchers observed high levels of F1P in colorectal cancer cells in the presence of fructose. Fructose exposure also inhibited the last step of glycolysis, the glucose metabolism pathway. F1P interfered with one of the enzymes that catalyze this step, PKM2. When the researchers blocked the cells from making PKM2, fructose no longer affected cell survival.
The researchers next engineered mice lacking either PKM2 or the enzyme that converts fructose to F1P. Fructose consumption did not lead to elongated villi in these mice, nor did it lead to increased fat absorption and accumulation. They also tried treating mice with a molecule, TEPP-46, that activates PKM2. TEPP-46 countered the effects of fructose, protecting against villus elongation, lipid absorption and fat accumulation.
Earlier, the team had found that fructose promoted tumor growth in mice that were genetically predisposed to colorectal cancer. In this study, they found that activating PKM2 with TEPP-46 prevented this effect.
These results suggest how the high levels of fructose found in Western-style diets could contribute to obesity and colorectal cancer. “Fructose is nearly ubiquitous in modern diets, whether it comes from high-fructose corn syrup, table sugar, or from natural foods like fruit,” Goncalves says. “Fructose itself is not harmful. It’s a problem of overconsumption. Our bodies were not designed to eat as much of it as we do.”
A study found that control over blood sugar and blood pressure has declined among people with diabetes after years of progress.
Uncontrolled diabetes increases the risk for serious health issues and could foreshadow growing complications among people with the disease.
The study found that after years of progress, management of diabetes in the U.S. recently declined. fizkes / iStock / Getty Images Plus
More than 34 million adults in the U.S. have diabetes. Diabetes occurs when blood sugar, also called blood glucose, is too high. Over time, if not well controlled, it can cause serious health problems such as heart disease, kidney failure, blindness, and limb amputation. Most people with diabetes have type 2, which is linked to lifestyle factors like weight and physical activity levels.
Managing diabetes entails reducing high blood sugar, keeping it within a healthy range, and controlling blood pressure and cholesterol levels. Over the past two decades, new medications and treatment guidelines have expanded options for diabetes care.
A research team led by Dr. Elizabeth Selvin of Johns Hopkins University examined trends in diabetes control and treatment from 1999 to 2018. They analyzed data from about 6,600 U.S. adults with diabetes who had participated in the CDC’s National Health and Nutrition Examination Survey. NHANES is a periodic survey of a representative sample of the U.S. population. Participants were 20 years of age or older, not pregnant, and had been diagnosed with diabetes by a physician.
The study was funded by NIH’s National Heart, Lung, and Blood Institute (NHLBI). Results appeared in the New England Journal of Medicine, on June 10, 2021.
The team found that blood sugar (glycemic) control declined between the 2007-2010 period and the 2015-2018 period from 57.4% to 50.5%. This decline was after more than a decade of progress in glycemic control starting in 1999.
Blood pressure control showed a similar trend. After earlier progress, the percentage of among people with diabetes who had healthy blood pressure (<140/90 mm Hg) declined. From 2011–2014 to 2015–2018, blood pressure control decreased from 74.2% to 70.4% of the participants. This aligns with recent declines in blood pressure control among the general population.
Cholesterol control also improved among those with diabetes but then stalled, with little improvement after 2010. Only about one in five participants met the targets for controlling blood sugar, blood pressure, and cholesterol in 2018. That statistic was relatively unchanged since 2010.
The study examined trends in diabetes treatment as well. The use of medications to lower glucose or blood pressure plateaued after 2010. The use of statins to reduce cholesterol remained unchanged after 2014. Combination therapies, those using more than one drug, declined after 2010 among participants with uncontrolled blood pressure. These treatment declines likely contributed to worsening diabetes control.
“These are concerning findings,” Selvin says. “There has been a real decline in glycemic control from a decade ago, and overall, only a small proportion of people with diabetes are simultaneously meeting the key goals of glycemic control, blood pressure control, and control of high cholesterol.”
The findings suggest that diabetic complications may be set to rise among Americans in the future.
Researchers found several immune and hormonal differences between people with Long COVID and those without.
The findings shed light on possible causes of Long COVID and could eventually lead to more sensitive testing and personalized treatments.
Researchers are making progress in understanding the underlying causes of Long COVID. ShowRecMedia / Shutterstock
Some people may experience chronic symptoms for months or years after an acute viral infection. Long COVID, a syndrome that develops in some people after an acute SARS-CoV-2 infection, is a prominent recent example. More than 200 Long COVID symptoms have been documented. Typical ones include extreme fatigue, cognitive impairment, post-exertional malaise, and respiratory problems. Research suggests that about one in eight people who survive an acute SARS-CoV-2 infection go on to have persistent symptoms. The processes that give rise to Long COVID remain unclear.
To shed light on the biology underlying Long COVID, a research team with NIH funding, partly through the RECOVER(link is external) Initiative, conducted a study of more than 250 people. The participants included people who had been infected with SARS-CoV-2 and uninfected people. Among those who had been infected, some had Long COVID and some did not. The researchers measured levels of various immune cells and markers in the participants’ blood. They also measured antibody responses to SARS-CoV-2 and a range of other viruses. The results appeared in Nature on September 25, 2023.
The team found significant differences in the immune cells of participants with and without Long COVID. Those with Long COVID had higher levels of cells called non-conventional monocytes and activated B lymphocytes. They had lower levels of type 1 conventional dendritic cells and central memory T cells. These differences did not depend on age, sex, or body mass index. Participants with Long COVID also had different levels of immune signaling molecules.
Participants with Long COVID had much stronger antibody responses against the SARS-CoV-2 spike protein than those without Long COVID. They also had much stronger responses to an unrelated virus, Epstein-Barr virus (EBV). EBV is a common herpesvirus that causes mononucleosis. After infection, it remains latent in the body and can sometimes reactivate. The higher levels of antibodies to EBV suggest recent reactivation of this virus.
When the researchers used machine learning to identify which features could best predict Long COVID status, they found that the strongest predictor was the stress hormone cortisol. People with Long COVID had much lower cortisol levels than those without. Other strong predictors of Long COVID included elevated levels of a protein called galectin-1, elevated antibodies against EBV, and reduced levels of certain immune cells.
These findings identify potential biomarkers that could help with diagnosing Long COVID. They also suggest possible mechanisms that contribute to Long COVID. These include a lingering presence of SARS-CoV-2 components in the body, reactivation of latent EBV, and chronic inflammation.
“These findings are important,” says Dr. David Putrino of the Icahn School of Medicine at Mount Sinai, one of the senior authors. “They can inform more sensitive testing for Long COVID patients and personalized treatments for Long COVID that have, until now, not had a proven scientific rationale. This is a decisive step forward in the development of valid and reliable blood testing protocols for Long COVID.”
Dr. Akiko Iwasaki of the Yale University School of Medicine, another senior author, says, “These findings tell us something about the underlying disease pathogenesis of Long COVID and suggest potential paths for therapy.”
People with obesity and type 2 diabetes lost more weight using daily periods of fasting than by trying to restrict calories over a six-month period.
Blood sugar levels lowered in people in both groups, and no serious side effects were observed.
Time-restricted eating, also called intermittent fasting, may be an effective weight loss strategy. Katecat / Adobe Stock
Around 1 in 10 Americans live with type 2 diabetes, a disease in which levels of blood glucose, or blood sugar, are too high. Diabetes can lead to serious health issues such as heart disease, nerve damage, and eye problems.
Excess weight is a major risk factor for the development of type 2 diabetes, and weight loss is often recommended for those with excess weight and type 2 diabetes. Calorie restriction—reducing overall calorie intake—is a mainstay of most weight loss programs. But such regimens are very difficult to stick with over the long term.
Time-restricted eating, also called intermittent fasting, has emerged as an alternative weight loss paradigm. In this approach, the time of day during which food can be eaten is restricted, but the amount or types of food are not. Small studies have suggested that intermittent fasting is safe and promotes weight loss in people with type 2 diabetes. But these studies only tracked participants for a short period of time. They also didn’t compare the approach with traditional calorie restriction.
In a new clinical trial, an NIH-funded research team led by Dr. Krista Varady from the University of Illinois Chicago compared fasting and calorie restriction for weight loss and blood-sugar reduction. They recruited 75 people with obesity and type 2 diabetes. Of these, 70 were either Hispanic or non-Hispanic Black—two groups in the U.S. with an especially high prevalence of diabetes. The participants were randomly assigned to one of three diet groups for six months.
The fasting group could eat anything they wanted, but only between the hours of noon and 8 pm. The second group worked with a dietitian to reduce their calories by 25% of the amount needed to maintain their weight. A control group did not change their diet at all. All groups received education on healthy food choices and monitored their blood glucose closely during the study. The results were published on October 27, 2023, in JAMA Network Open.
After six months, participants in the fasting group lost an average of 3.6% percent of their body weight compared to those in the control group. In comparison, people in the calorie-restriction group did not lose a significant amount of weight compared to the control group.
Both groups had similarly healthy decreases in their average blood glucose levels. Both also had reductions in waist circumference. No serious side effects, including time outside of a safe blood glucose range, were seen in either treatment group. People in the fasting group reported that their diet was easier to adhere to than calorie restriction.
“Our study shows that time-restricted eating might be an effective alternative to traditional dieting for people who can’t do the traditional diet or are burned out on it,” Varady says. “For many people trying to lose weight, counting time is easier than counting calories.”
Some medications used to treat type 2 diabetes need adjustment for time-restricted eating. Therefore, people considering intermittent fasting should speak with a doctor before changing their eating pattern.
SARS-CoV-2 infected coronary arteries and increased inflammation in atherosclerotic plaques.
The findings suggest how COVID-19 could increase the risk of heart attack and stroke.
Foam cells, which accumulate within arteries to form plaques in atherosclerosis, proved particularly susceptible to infection with SARS-CoV-2. Kateryna Kon / Shutterstock
COVID-19 is known to increase the risk of heart attack and stroke. The intense inflammation that occurs throughout the body in severe cases likely contributes to this increased risk. But it’s not clear whether SARS-CoV-2, the virus that causes COVID-19, also affects blood vessels directly.
To find out, an NIH-funded research team, led by Dr. Chiara Giannarelli at New York University School of Medicine, analyzed coronary artery tissue samples from eight people who died of COVID-19 between May 2020 and May 2021. Results appeared in Nature Cardiovascular Research on September 28, 2023.
The team found SARS-CoV-2 viral RNA in coronary artery tissue from all patients. They found more viral RNA in the arterial walls than in the surrounding fat tissue. Many of the infected cells were macrophages, a type of white blood cell that ingests pathogens. Samples with more macrophages had more viral RNA.
Macrophages also help remove cholesterol from blood vessels. When macrophages become laden with cholesterol, they are known as foam cells. Accumulation of foam cells within arteries forms plaques that are a hallmark of atherosclerosis. The team confirmed that SARS-CoV-2 could infect human macrophages and foam cells in a petri dish. The foam cells were much more susceptible to infection than the macrophages. This could explain why people with atherosclerosis are more vulnerable to COVID-19.
In both cell types, infection depended on a protein on the surface of the cells called neuropilin. Turning off the gene for neuropilin in these cells reduced infection. So did blocking the virus from binding to neuropilin.
Infection triggered several inflammatory pathways in macrophages and foam cells. The cells also released molecules that are known to contribute to heart attacks and strokes. In arterial plaques that had been surgically removed from patients, the researchers saw an inflammatory response to SARS-CoV-2 infection like that seen in the cultured cells.
The findings suggest that SARS-CoV-2 may increase the risk of heart attacks and stroke by infecting artery wall tissue, including associated macrophages. This provokes inflammation in atherosclerotic plaques, which could lead to heart attack or stroke.
“These results shed light onto a possible connection between preexisting heart issues and Long COVID symptoms,” Giannarelli says. “It appears that the immune cells most involved in atherosclerosis may serve as a reservoir for the virus, giving it the opportunity to persist in the body over time.”
“Since the early days of the pandemic, we have known that people who had COVID-19 have an increased risk for cardiovascular disease or stroke up to one year after infection,” says Dr. Michelle Olive of NIH’s National Heart, Lung, and Blood Institute. “We believe we have uncovered one of the reasons why.”
The authors plan to further investigate the potential link between infection of the arteries and Long COVID. They also aim to see if their results also hold true for newer SARS-CoV-2 variants.
People with diabetes who took drugs called GLP-1 receptor agonists had a lower risk of colorectal cancer compared with those prescribed other diabetes drugs.
More research is needed to understand how GLP-1 receptor agonists may reduce the risk of colorectal cancer.
Drugs called GLP-1 receptor agonists may have benefits beyond diabetes control and weight loss. Myskin / Shutterstock
People with obesity are at increased risk for many chronic health problems. These include type 2 diabetes and heart disease. Obesity also increases the risk of many common cancers, including colorectal cancer.
Doctors often prescribe medications for people with type 2 diabetes. These include metformin, insulin, and other drugs that help manage blood glucose (blood sugar) levels to reduce long-term complications of diabetes.
Over the last two decades, a class of antidiabetic drugs called GLP-1 receptor agonists (GLP-1RAs) has become available for use by people with type 2 diabetes. These drugs—which include Ozempic, Trulicity, Wegovy, and Zepbound—not only help control blood glucose but can also promote weight loss. They reduce appetite both by their impact on the brain and by slowing movement of food through the digestive tract.
Researchers have wondered if these drugs could reduce the risk of other diseases in people with type 2 diabetes. In a new study, funded in part by NIH, a research team led by Drs. Rong Xu and Nathan Berger from Case Western Reserve University and the Case Comprehensive Cancer Center looked at this question for colorectal cancer.
The researchers examined the medical records of more than 1.2 million people with type 2 diabetes who were prescribed antidiabetic medications between 2005 and 2019. The team identified newly diagnosed colorectal cancer cases over a follow-up period of up to 15 years. They then compared the risk of developing colorectal cancer among people who were taking seven different types of antidiabetic drugs.
To compare the drugs, the team matched people between groups by known risk factors for colorectal cancer, other pre-existing medical conditions, age, sex, race, and socioeconomic status. Thousands of such matches were made between each of the drugs. The results were published on December 7, 2023, in JAMA Oncology.
The team found that, overall, people with type 2 diabetes who took GLP-1RAs had a lower risk of developing colorectal cancer than those taking the other medications. Those taking GLP-1RAs had a 44% lower risk of developing colorectal cancer than those who took insulin. They had a 25% lower risk than those who took metformin.
This reduced risk was seen whether or not people had obesity or overweight. Among people with excess weight, GLP-1RA users had an even stronger reduction in colorectal cancer risk. This group had a 50% lower risk of developing colorectal cancer than those who took insulin, and a 42% lower risk than those who took metformin.
A smaller but significant reduction in colorectal cancer risk was also seen with the use of GLP-1RAs compared to other antidiabetic drugs for people with obesity or overweight.
“[This] research is critically important for reducing incidence of colorectal cancer in patients with diabetes, with or without overweight and obesity,” Berger says.
These findings suggest that GLP-1RAs could be protective against colorectal cancer in people who have type 2 diabetes, regardless of weight. More research is needed to confirm these observations, to determine whether GLP-1RAs can reduce the risk of other types of cancer associated with obesity, and to understand their mechanisms of action.
The year 2023 has been confirmed as the warmest on record, driven by human-caused climate change and boosted by the natural El Niño weather event.
Last year was about 1.48C warmer than the long-term average before humans started burning large amounts of fossil fuels, the EU’s climate service says.
Almost every day since July has seen a new global air temperature high for the time of year, BBC analysis shows.
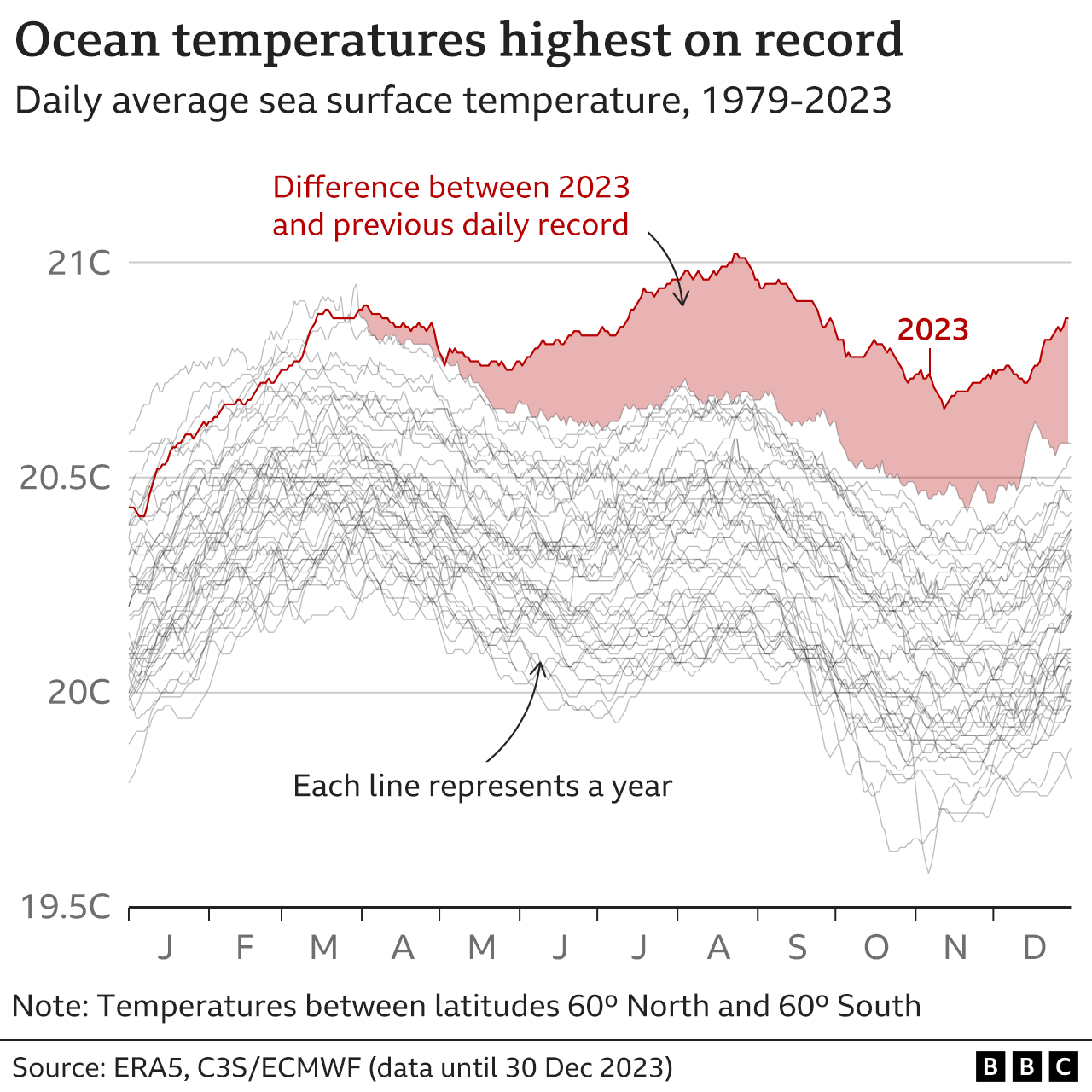
Sea surface temperatures have also smashed previous highs.
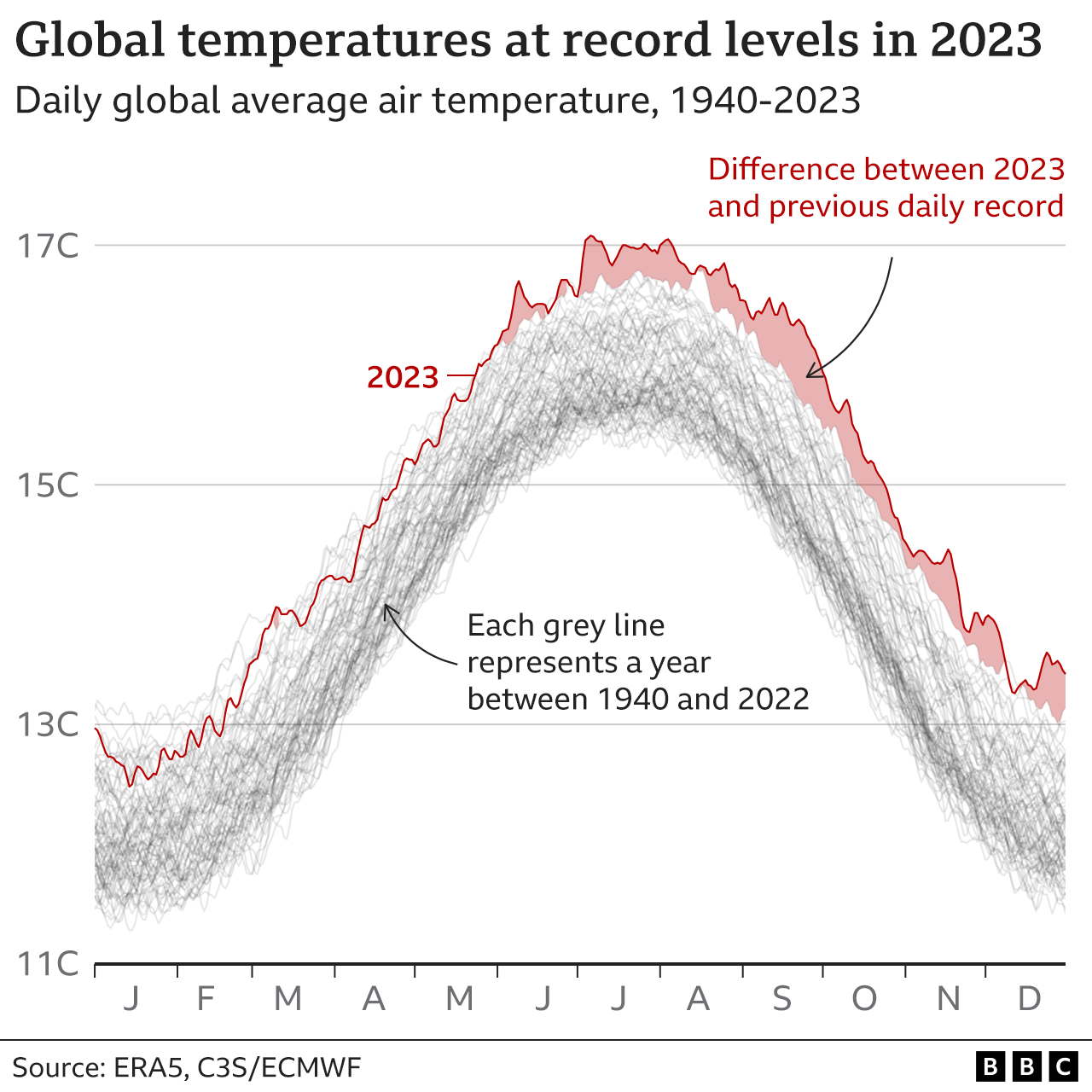
“What struck me was not just that [2023] was record-breaking, but the amount by which it broke previous records,” notes Andrew Dessler, a professor of atmospheric science at Texas A&M University.
The margin of some of these records – which you can see on the chart below – is “really astonishing”, Prof Dessler says, considering they are averages across the whole world.
An exceptional spell of warmth
It’s well-known that the world is much warmer now than 100 years ago, as humans keep releasing record amounts of greenhouse gases like carbon dioxide into the atmosphere.
But 12 months ago, no major science body actually predicted 2023 being the hottest year on record, because of the complicated way in which the Earth’s climate behaves.
During the first few months of the year, only a small number of days broke air temperature records.
But the world then went on a remarkable, almost unbroken streak of daily records in the second half of 2023.
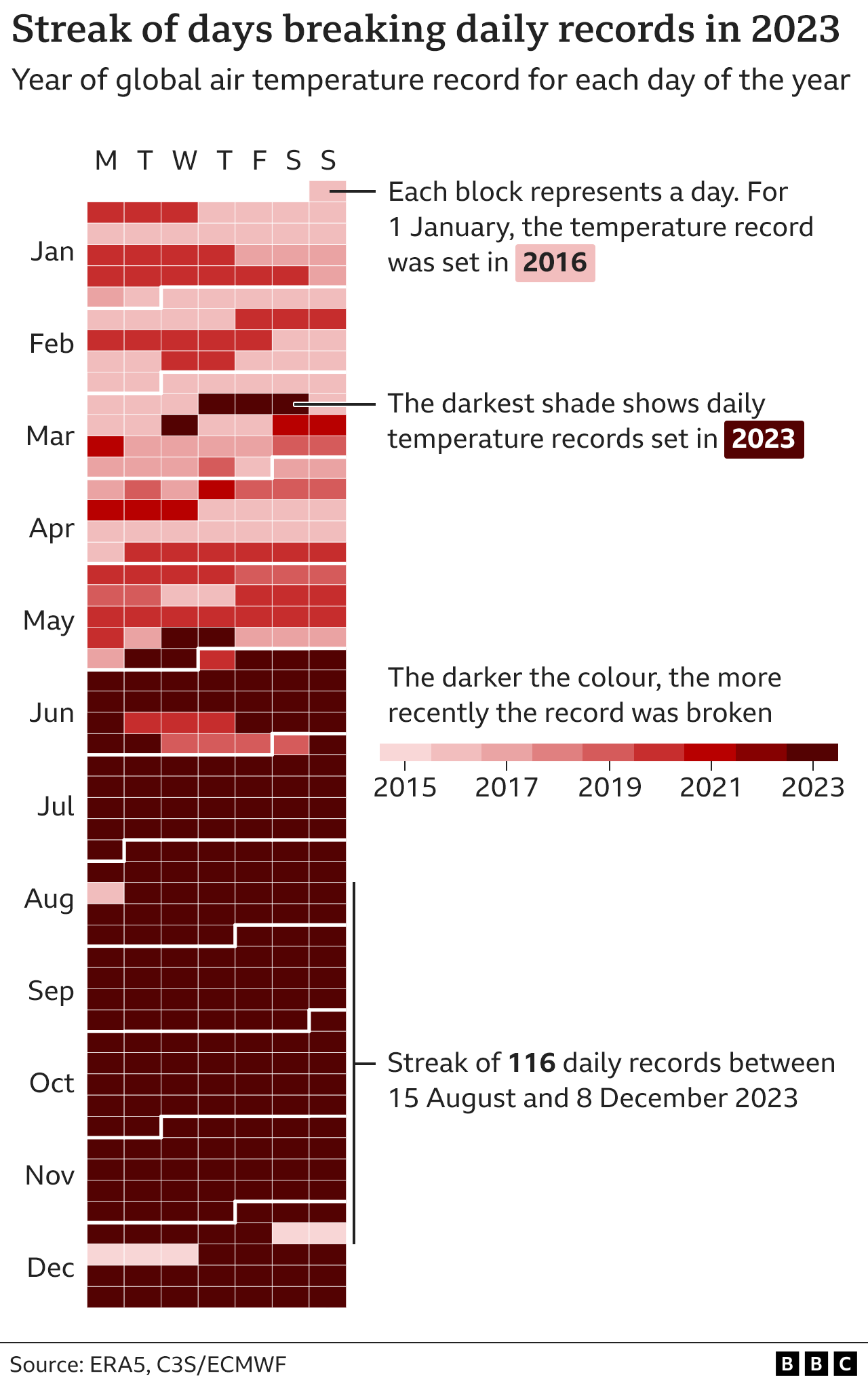
Look at the calendar chart below, where each block represents a day in 2023. Records were broken on the days coloured in the darkest shade of red. From June, we’re looking at a new record most days.
More than 200 days saw a new daily global temperature record for the time of year, according to BBC analysis of Copernicus Climate Change Service data.
This recent temperature boost is mainly linked to the rapid switch to El Niño conditions, which has occurred on top of long-term human-caused warming.
El Niño is a natural event where warmer surface waters in the East Pacific Ocean release additional heat into the atmosphere.
But air temperatures have been boosted unusually early on in this El Niño phase – the full effects had not been expected until early 2024, after El Niño had reached maximum strength.
“That raises a bunch of really interesting questions of why [2023 was] so warm,” notes Zeke Hausfather, a climate scientist at Berkeley Earth, a science organisation in the US.
Consequences felt worldwide
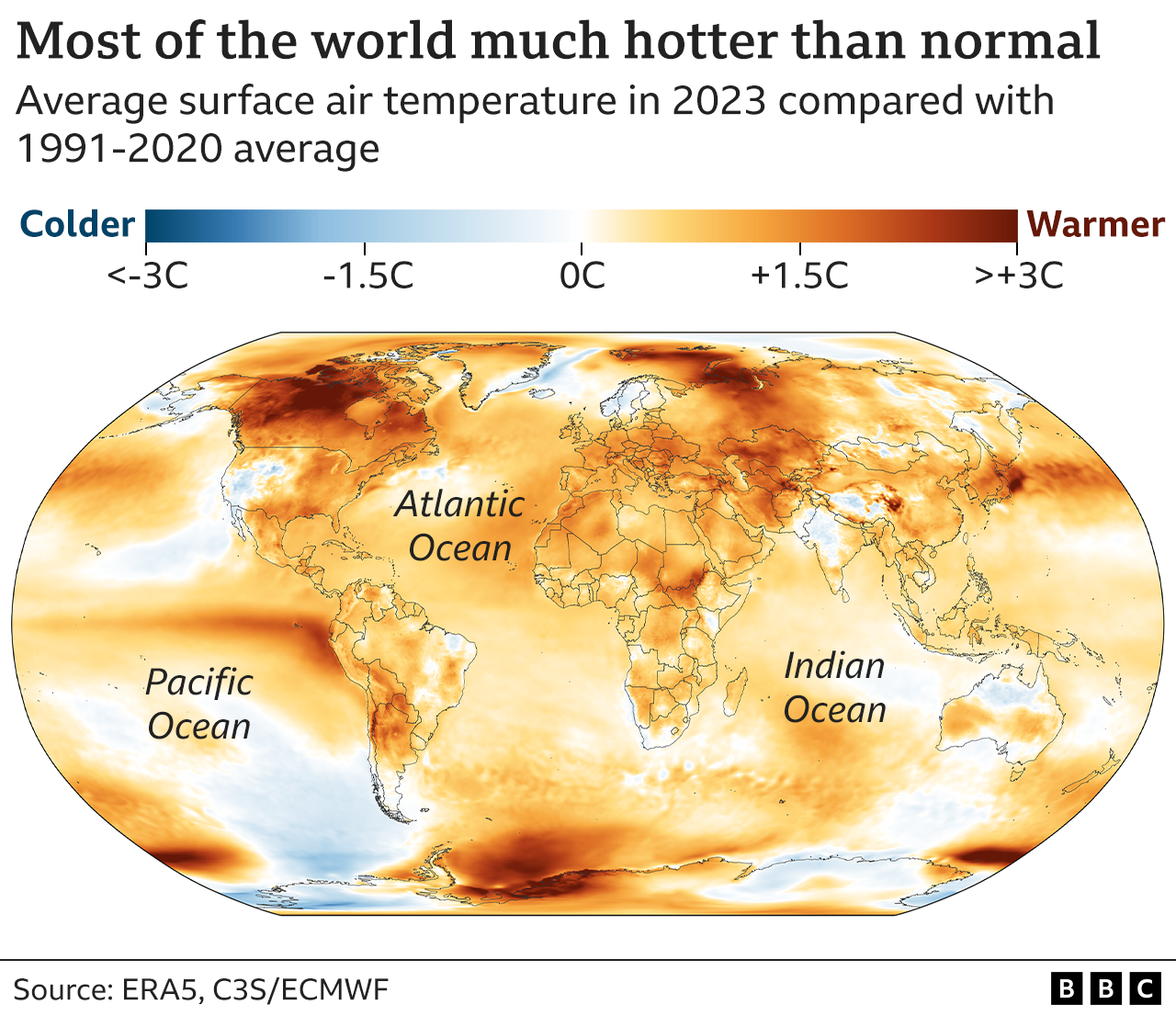
Another notable feature of the 2023 warmth is that it has been felt pretty much worldwide.
As the map below shows, almost all of the globe was warmer than recent 1991-2020 levels – a period that was itself nearly 0.9C warmer than before humans started burning large amounts of fossil fuels in the late 1800s.
This record global warmth has helped to worsen many extreme weather events across large parts of the world in 2023 – from intense heatwaves and wildfires across Canada and the US, to prolonged drought and then flooding in parts of east Africa.
In fact, the world’s ocean surface has been on an unbroken streak of record-breaking days since 4 May, BBC analysis of Copernicus data shows. As the chart below illustrates, many days have seen records broken by a huge margin.
A warning for 2024 and beyond
The year 2024 could be warmer than 2023 – as some of the record ocean surface heat escapes into the atmosphere – although the “weird” behaviour of the current El Niño means it’s hard to be sure, Dr Hausfather says.
It raises the possibility that 2024 may even surpass the key 1.5C warming threshold across the entire calendar year for the first time, according to the UK Met Office.
It refers to long-term averages over 20 or 30 years, so a year-long breach in 2024 wouldn’t mean the Paris agreement had been broken.
But it highlights the concerning direction of travel, with each hot year bringing the world closer to passing 1.5C over the longer term.
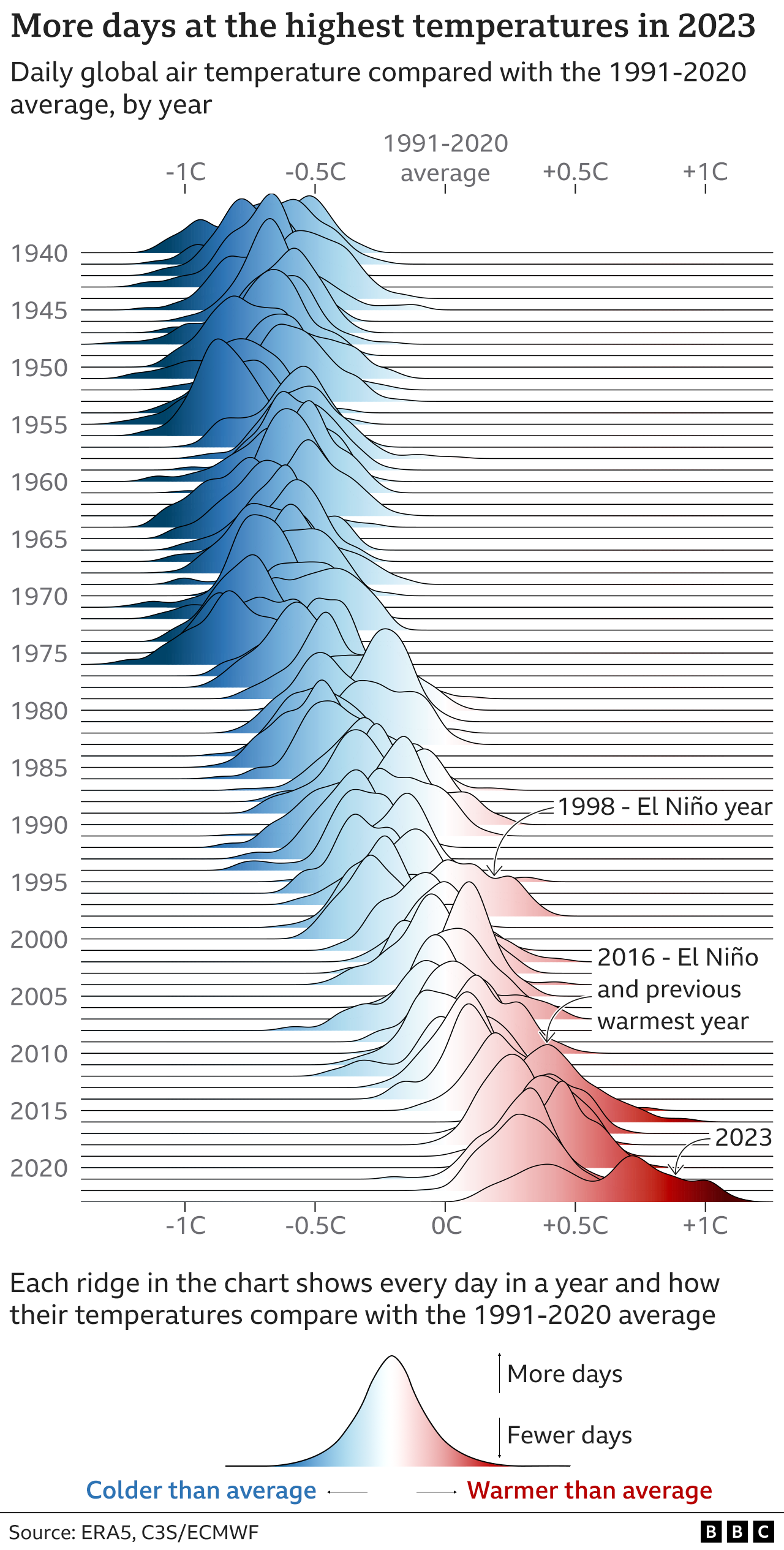
Human activities are behind this long-term global warming trend, even though natural factors like El Niño can raise or reduce temperatures for individual years, and the temperatures experienced in 2023 go far beyond simply natural causes.
Look at the chart below. At the time, 1998 and 2016 were record-breaking years, boosted by strong El Niño warming. But these don’t come close to the new 2023 records, marked in the darkest reds.
“2023 was an exceptional year, with climate records tumbling like dominoes,” concludes Dr Samantha Burgess, Deputy Director of the Copernicus Climate Change Service.
This latest warning comes shortly after the COP28 climate summit, where countries agreed for the first time on the need to tackle the main cause of rising temperatures – fossil fuels.
While the language of the deal was weaker than many wanted – with no obligation for countries to act – it’s hoped that it will help to build on some recent encouraging progress in areas like renewable power and electric vehicles.
This can still make a crucial difference to limit the consequences of climate change, researchers say, even though the 1.5C target looks likely to be missed.
“Even if we end up at 1.6C instead, it will be so much better than giving up and ending up close to 3C, which is where current policies would bring us,” says Dr Friederike Otto, a senior lecturer in climate science at Imperial College London.
Image caption,Portable X-ray machines, such as this one pictured, are seeing a big rise in use
By Christine Ro
Technology reporter
Portable X-ray machines “can literally be the difference between life and death”, says radiographer Sam Pilkington.
For most of us, if we need to be X-rayed the procedure is done in a hospital. But for acutely unwell patients, or for infection control, Miss Pilkington says that portable machines are very helpful.
This is because “they remove the excess burden of transportation from the patients”, says the final-year student at the University of the West of England in Bristol, who is also a member of the Institute of Physics. Instead the X-ray equipment goes to them.
There are obvious advantages for remote locations, including battlefields, roadsides and disaster zones.
And thanks to the increased availability – and ability – of such portable systems their usage is growing rapidly. With the coronavirus pandemic fuelling this increase, the global portable X-ray market was worth a reported $7.1bn (£5.6bn) last year. And this is expected to rise to $14bn by 2028.
In simple terms there are two types of portable X-ray machines – those on wheels, which are generally described as “mobile”, and the lightest devices that can be carried by a single person. These are generally described as “ultraportable”.
Image caption,Portable X-ray machines are now said to produce images of similar standard to big, fixed devices in hospitals
One remote place that has tested ultraportable X-ray hardware is the Orkney Islands in Scotland. Prior to a trial there from November 2021 to January 2022, 73% of patients who were due for an X-ray did not attend their appointments – due in large part to the costs and time needed to reach distant hospitals.
During the trial, a handheld device made by Japanese firm Fujifilm was taken to local clinics. Called the Fujifilm Xair, it weighs just 3.5kg, and is only 301mm (12 inches) wide and 144mm tall.
As a result of its use, the non-attendance rate for X-rays appointments was reduced to zero.
As one patient commented to the subsequent report: “This is hugely beneficial to people on the small islands. Much less upheaval for frailer patients.”
German company OR Technology is another manufacturer of portable X-ray machines. Tim Thurn, its chief commercial officer, says it is seeing great interest from emerging markets. “There’s a huge demand for bringing healthcare to the people,” he says.
Image caption,This mock-up shows how a portable X-ray machine could take pictures at accident scenes
In the Philippines, Nigeria and other countries in the developing world, portable X-ray systems are transforming screening for tuberculosis (TB), which kills approximately 1.3 million people a year despite being preventable and curable.
It’s long been known that a chest X-ray is the best screening tool for TB, explains Suvanand Sahu, the deputy executive director of the Stop TB Partnership. This Swiss-based organisation represents more than 1,500 government and non-government bodies around the world.
But he says that access to X-rays was historically hampered by a lack of hospitals. This was particularly the case in remote areas, and among remote, nomadic and displaced groups.
Dr Sahu says that portable X-ray machines, which often include artificial intelligence software to quickly process the images, have been a powerful solution that allows detection to be successfully done out in the field.
“About 10 years ago, if we would have said ‘we can we do an X-ray in the community, with the computer reading it’, I think people would have jumped out of their seats. But it has happened now.”
Dr Sahu adds that the AI has enabled a “quantum leap” in how accurately and quickly these X-rays can be read.
Image caption,Portable X-ray machines are now being used in countries such as the Philippines to test for TB
Yet some are worried about the radiation released by portable X-ray machines. Portable X-ray equipment works in the same way as the big, fixed machines in radiology departments in hospitals – the image is created by a targeted burst of ionizing radiation.
In hospitals, x-ray rooms are carefully designed to minimise radiation exposure, for instance with lead walls.
Mr Thurn says that with portable systems this lack of shielding is compensated for by the greater space where they are used, be it outdoors, or in a field hospital setup. In these cases he says that healthcare workers can stand much further away.
However, the issue of radiation needs to be clarified, as currently the international guidelines on radiation safety “are designed for the traditional fixed type of X-ray”, says Zhi Zhen Qin, a digital health specialist at the Stop TB Partnership.
The image quality of portable X-ray machines used to be a concern as well. But Miss Pilkington says that today’s machines rival fixed units in this regard: “The images that are taken on those machines are of a comparable diagnostic standard.”
New Tech Economy is a series exploring how technological innovation is set to shape the new emerging economic landscape.
However, there are barriers to just how small the components of an X-ray system can get. If an X-ray detector is too small to capture a body part in a single exposure, extra images might need to be taken, which would add to time burdens and radiation doses.
And units with a limited battery life or data storage, reduce how many patients can be imaged in one session.
Meanwhile, some systems described as portable aren’t exactly lightweight and easily transported, particularly if they need other hardware to make them work like a stand or computer equipment.
Yet Australian firm Micro-X is now making much lighter ultraportable x-ray machines, due to its new technology that can produce the X-rays without creating heat. This does away with the need for oil and motors for cooling, which add weight.
The high cost of portable X-ray machines is also an issue. While they are cheaper than the larger fixed machines, they are still very expensive.
The Stop TB Partnership says that the price of ultraportable machines ranges between $47,000 and $66,000. There are additional costs for warranties, installation and software.
Dr Suvanand says that as more manufacturers enter this space, “we hope that the competition will drive down the prices”.
Ultimately, his vision for the future is that “everybody who needs an X-ray should have access to this type of modern, digital, ultra-portable X-ray with AI capability”.