A study suggests yet another potential adverse effect of gabapentinoid drugs.
In 2019, the U.S. Food and Drug Administration issued a warning related to nearly 50 case reports of breathing difficulties following use of gabapentinoids. opens in new tab (i.e., gabapentin and pregabalin) that were reported between 2012 and 2017; however, such warnings are not reflected in current pain management guidelines. To explore this issue further, Canadian investigators retrospectively studied a cohort of patients with chronic obstructive pulmonary disease (COPD): 14,000 new users of gabapentinoids were propensity matched with 14,000 nonusers, based on duration of COPD, age, sex, and gabapentinoid indication.
Gabapentinoid use was associated with significantly higher risk for severe COPD exacerbations requiring hospitalization (15.1% vs. 8.3% annually; adjusted hazard ratio, 1.4). New users of gabapentinoids also had significantly higher risks for respiratory failure (5.7% vs. 3.6% annually, aHR, 1.3) and moderate-to-severe COPD exacerbations (53% vs. 29% annually; aHR, 1.1). Gabapentin did not differ from pregabalin in risk for severe COPD exacerbations.
COMMENT
Although this study has typical limitations of a retrospective cohort design, it affirms reported cases of respiratory problems related to these medications and parallels anesthesia-setting cohort studies that have suggested respiratory depression associated with gabapentinoid use. Clinicians should have informed risk-benefit discussions with their patients who have COPD prior to initiating these medications; these discussions should reflect not only the adverse effects of gabapentinoids but also that evidence of their effectiveness for many painful conditions is limited
A groundbreaking discovery in pain management could revolutionize how we treat chronic pain. In a report from a study published in the Proceedings of the National Academy of Sciences, researchers at New York University, in collaboration with colleagues at the University of Pittsburgh, have announced the discovery of a novel medication that could treat centralized pain that targets Cav2.2 calcium channels (also called N-type calcium channels).
First, what is centralized pain? Why don’t other pain medications work well against it? And why does this medication target Cav2.2 calcium channels? An example of a pain-relieving medication working through ion channels is lidocaine. Lidocaine binds to and inactivates voltage-gated sodium channels. Since these are important for peripheral pain reporting nerves, it can block pain for several hours.
Researchers at the Pain Research Center at NYU College of Dentistry were very interested in calcium channels called Cav2.2 because they play a crucial role in the transmission of pain signals in the central nervous system. If we could slow down or block these channels, we could reduce the ability of these second and third-order neurons to produce pain signals. This would be incredibly important to most chronic pain sufferers since these channels are integral to pain transmission in second and third-order afferent nociceptive neurons.
Drugs like gabapentin and pregabalin, Neurontin, and Lyrica bind these receptors at the alpha-2-delta subunit of the Cav2.2 channel, reducing pain signal transmission. This class of medications is called gabapentinoids, and while these medications are now widely used for nerve pain and epilepsy, as they are the best we have right now, they are not without problems.
Gabapentin is recommended as a first-line treatment for chronic neuropathic pain by various medical authorities, and this is a general recommendation applicable to all neuropathic pain syndromes except for trigeminal neuralgia, where it may be used as a second or third-line agent.
Gabapentin and pregabalin, while therapeutic, also produce feelings of relaxation and euphoria. And human beings tend to want to repeat activities that generate these feelings. It turns out that with the increasing prescription rates of gabapentin, there’s been a corresponding rise in its misuse. People subject to substance abuse issues, which is pretty much everyone under the right circumstances, may be drawn to gabapentin and pregabalin for their calming effects. If mixed with opioids, alcohol, or other depressants, a synergistic response can be elicited, and gabapentin’s effects can be amplified, leading to increased sedation and, in some cases, dangerous respiratory depression. An alcohol-like effect if you will.
Overdose-related deaths due to gabapentinoids themselves are still quite rare, and of course, any medication or substance can kill you if you take enough of it. Much more commonly a problem, however, is the potential for the gabapentinoids to produce euphoric effects in a subset of patients. This can quickly lead to a substance use disorder, even addiction perhaps.
A substance use disorder can be considered a situation where someone chooses to use a substance or activity to alter their mood or experience euphoria despite negative life consequences. Addiction, on the other hand, could be considered a loss of control of the use of a substance or activity. These people cannot stop even if they really want to. This loss of control is mediated by overexpression of the gene deltaFosB, in the nucleus accumbens of the brain, and seems to be directly related to euphoric effects.
The risk of Gabapentin abuse highlights the need for careful prescription and monitoring practices. Health care providers are advised to screen patients for a personal or family history of substance abuse, especially to alcohol or sedatives, and for mood disorders like depression and anxiety, before prescribing gabapentinoids.
Patients should also be educated about the risks of misuse with regular follow-ups and monitoring as always. Understand, however, that just because a medication has drawbacks, does not mean that politicians and government agents need to Monday morning quarterback a doctor’s decision to use these medications.
In fact, there is evidence that gabapentinoids can be used effectively in the treatment of alcohol and sedative addiction through medication-assisted therapy (MAT). MAT is where a doctor can take a substance that has a similar but milder effect than the drug of abuse, and uses that to help someone maintain control of their addiction. This is how medications like Suboxone work. Hopefully, tapering off the milder medication later, though some people need maintenance therapy to avoid relapse.
Gabapentinoids have been an amazing medication for those suffering from nerve-related pain. But what if we could find a better way to produce this effect? Without the potential for euphoria?
There is a natural 17-amino acid molecule called CBD3 that specifically binds and deactivates the Cav2.2 calcium channel. What if we found a medication that worked like this natural molecule? In a report from a study published in the Proceedings of the National Academy of Sciences, it was announced that we may have a significant breakthrough in this pursuit.
Researchers at New York University, in collaboration with colleagues at the University of Pittsburgh, ran a computer simulation that screened a library of 27 million compounds to look for a small molecule that would “match” the CBD3 amino acids. The simulation narrowed the library down to 77 compounds, which the researchers experimentally tested to see if they lessened the amount of calcium influx. This further pared the pool down to nine compounds, which were assessed using electrophysiology, to measure decreases in electrical currents through the calcium channels.
One compound, which the researchers named CBD3063, emerged as the most promising candidate for treating centralized pain through this approach. Biochemical tests revealed that CBD3063 disrupted the interaction between the CaV2.2 calcium channel and CRMP2 protein. CRMP stands for Collapsin Response Mediator Protein, and it is critical to neuroplasticity in these central pain nerves. CRMP2 regulates the trafficking and surface expression of various ion channels and receptors, including Cav2.2 calcium channels, thereby reducing the rate of calcium entering the channel. This reduces the firing rate of central pain neurons and lessens the release of neurotransmitters, reducing the pain signal.
This new compound was later proven effective at reversing four types of chronic pain in animal studies: chemotherapy-induced neuropathy, inflammatory pain, acute injury-related pain, and trigeminal neuralgia. What’s remarkable is that it outperformed gabapentin, without any evidence so far of troublesome side effects. This discovery is not just a scientific achievement; it’s a beacon of hope for millions suffering from severe chronic pain, and it underscores the importance of innovative research in developing new pain therapies.
Pregabalin and Gabapentin are non-natural, branched chain amino acids. Both are chemical analogues of gama-aminobutyric acid (GABA); however, neither drug has activity in GABAergic neuronal systems. Both these drugs are efficacious in certain types of neural pain control.
Dosage: The treatment for neuropathic pain with Gabapentin is usually initially started with one dose of 300 mg per day.It can be given orally at a dose of 300-1200 mg 3 times per day. Maximum dose should be 3600 mg per day.
The suggested maximum therapeutic dose of Pregabalin in neuropathic pain associated with diabetic peripheral neuropathy is 300 mg per day; it can be initiated at a dose of 50 mg thrice a day. The dose of the drug can be increased up to 300 mg per day within a week of starting the treatment.
For neuropathic pain associated with spinal cord injury, the recommended therapeutic dose of Pregabalin should be 150 to 600 mg daily. The suggested starting dose is 75 mg twice per day. The dose might be increased to 150 mg twice/day within one week of starting treatment. In patients having suboptimal pain relief after 2 to 3 weeks of treatment with 150 mg twice daily, the dose might be increased up to 300 mg twice/day.[1]
Excretion: It is estimated that elimination half-life parameter for the two drugs are same. The elimination half-life for Gabapentin is estimated to be in the range of 5-7 hours, and that for Pregabalin is about 6.3 hours, indicating that both drugs can reach a steady state within 24-48 hours.
Adverse effects: Generally, Pregabalin and Gabapentin are well tolerated. Dizziness is the most frequently reported negative effect of Pregabalin, followed by somnolence, which accounts for the most frequent reason for treatment discontinuation. The negative effects of both the drugs are dose-dependent and are reversible.
Pregabalin and Gabapentin are non-natural, branched chain amino acids. Both are chemical analogues of gama-aminobutyric acid (GABA); however, neither drug has activity in GABAergic neuronal systems. Both these drugs are efficacious in certain types of neural pain control.
Dosage: The treatment for neuropathic pain with Gabapentin is usually initially started with one dose of 300 mg per day.It can be given orally at a dose of 300-1200 mg 3 times per day. Maximum dose should be 3600 mg per day.
The suggested maximum therapeutic dose of Pregabalin in neuropathic pain associated with diabetic peripheral neuropathy is 300 mg per day; it can be initiated at a dose of 50 mg thrice a day. The dose of the drug can be increased up to 300 mg per day within a week of starting the treatment.
For neuropathic pain associated with spinal cord injury, the recommended therapeutic dose of Pregabalin should be 150 to 600 mg daily. The suggested starting dose is 75 mg twice per day. The dose might be increased to 150 mg twice/day within one week of starting treatment. In patients having suboptimal pain relief after 2 to 3 weeks of treatment with 150 mg twice daily, the dose might be increased up to 300 mg twice/day.[1]
Excretion: It is estimated that elimination half-life parameter for the two drugs are same. The elimination half-life for Gabapentin is estimated to be in the range of 5-7 hours, and that for Pregabalin is about 6.3 hours, indicating that both drugs can reach a steady state within 24-48 hours.
Adverse effects: Generally, Pregabalin and Gabapentin are well tolerated. Dizziness is the most frequently reported negative effect of Pregabalin, followed by somnolence, which accounts for the most frequent reason for treatment discontinuation. The negative effects of both the drugs are dose-dependent and are reversible.
Painful diabetic neuropathy is frustratingly difficult to treat. Even the best prescription medication for the condition, gabapentin (Neurontin), only works for a small minority of those who try it, and some members of the diabetes community have never found anything that works. Patients that do find some relief often use a combination of prescription medication, over-the-counter treatments, and non-medicinal techniques such as massage or foot elevation.
Tim Swartztrauber tried it all, and he found no benefit from any of it. His diabetic neuropathy pain was so debilitating that it was robbing him of his life.
That all changed when his doctor suggested a trial of an uncommon treatment: spinal cord stimulation. Tim was an instant convert, and today he’s enjoying life again, his pain largely resolved.
[The manufacturers of Nevro HFX put Diabetes Daily in touch with Tim, but this is not a sponsored post. Tim is not a paid spokesman.]
Tim’s journey with diabetes had a traumatic beginning — a diagnosis of myelodysplastic syndrome and leukemia. His treatment odyssey eventually led to what was probably a case of steroid-induced diabetes. Steroids can cause hyperglycemia, and in Tim’s case, the effect was extreme.
“Back in 2015, I was diagnosed with leukemia. I had a bone marrow transplant and shortly after I developed graft versus host disease. I was on extremely high doses of steroids, and in January 2016 I was experiencing blurred vision and all that. I went in for an appointment. My blood sugar was 530 [mg/dL], and I had to stay in the hospital for seven days.”
Just when Tim thought he was getting his diabetes under control, his doctors ramped up his steroids usage again. With his blood sugar spiking back up to dangerous levels, he began to experience painful diabetic neuropathy.
“I was diagnosed with neuropathy, and it was severe. I had trouble walking. It was just miserable. It was 24 hours a day, I was only sleeping about two or three hours at a time. When I laid down to go to bed, my left foot hurt the worst, and I had to prop it up on my other foot so it wouldn’t touch the mattress.
“There were times I didn’t even want put on shoes because it hurt so bad. It would hurt to the touch. Just laying my foot on something would kill me.”
Tim tried a lot of different therapies to help with the pain, but nothing seemed to work.
“They had me on opioids, at one point I was taking 15mg of oxycodone four times a day, and it wasn’t even touching the pain. In my opinion, opioids don’t solve the problem, they don’t even mask the problem. All it did was make me sleepy and goofy. It’s not a quality of life you would want to have, living on pain medicines.
“I used gabapentin. I tried a cream I applied to my feet. It really didn’t help all that much.
“We tried some shots to my legs, hips, and ankles. I didn’t know there were steroids in those shots, and after I got the shots, my sugar went up to 589 and I had to go to the hospital again.
“I even went to a month’s worth of yoga. I did learn to relax a little more, but it didn’t really help.”
Although the degree of pain that Tim felt was unusual, the pattern of his general experience was typical. Many people with neuropathic pain find themselves trying all sorts of remedies, pharmaceutical and otherwise, sometimes with little success. (Opioids, probably the most commonly-prescribed treatment for painful neuropathy, are no longer recommended due to the danger of addiction and a lack of evidence that they are effective.)
“For a number of years, I didn’t do anything. I’d work and when I got home I’d just get in my chair and that was it.
“I was pretty miserable. Me and my wife were always at each other’s throats because I never wanted to do anything. I was really depressed. I started on depression medicine.
“Finally, my palliative care doctor referred me to a specialist who put me through a very thorough check. He mentioned the spinal cord stimulation implant.”
Spinal cord stimulation involves a small device that delivers mild electrical pulses along thin wires to the spinal cord. These pulses essentially block pain signals from reaching the brain. Spinal cord stimulation been used for years for many types of chronic pain (in the US, it is most commonly used for failed back surgery syndrome).
The scientific evidence in favor of spinal cord stimulation for people with diabetes is encouraging, but still emerging. A 2021 review noted that there have yet to be any blinded and randomized long-term trials of the technology, but observational trials suggest that many patients do enjoy long-lasting pain relief. The American Association of Clinical Endocrinology has recently endorsed high-frequency spinal cord stimulation as an option for people with “painful diabetic peripheral neuropathy that failed at least one medication.”
New patients undergo a trial period during which a temporary device is used to test the treatment. If everything goes well, a permanent device is surgically implanted underneath the skin. HFX reports that 90 percent of the patients that go through with a trial of the device decide to get the permanent implant.
“I did a trial. The next morning, I noticed that my feet didn’t hurt as bad. The next day they got better, and the next day they got a little better.”
When they removed the temporary device, the pain came back. “I decided right then and there that I was gonna get the implant.”
Tim says that the procedure was a snap, and only took a few hours: “The surgery is very easy, not very invasive, and not very painful.”
“The day after the implant was installed, my feet again got better. By the end of the week, I was like, ‘Oh my gosh, this is simply amazing.’ Every day it got better and better.
“I quit the gabapentin probably three to four days after surgery. Within a few months, I was totally off all pain meds. I don’t even hardly take aspirin. I’m off my depression meds.”
“My life has totally changed ever since.”
“Since the implant, that fall I went on a 10-day fishing trip with no problems whatsoever. You just don’t know how this really changed my life.”
The HFX Nevro implant comes with a remote control that Tim can use to modulate the type of pain relief he receives. He worked with his medical team to install multiple programs that target different parts of his body, so he can deliver relief where and when he needs it most.
“I charge it every night, it takes about 15 minutes a night. You have this belt with a power pack and you have this pad that you put right over your implant.”
He reports that the implant itself is unobtrusive. “It’s just a little square under my skin. It doesn’t bother me, I don’t even know it’s in there.”
“Now I’m sleeping 7 hours a night, straight through. It’s been amazing for me. I can’t really put it into words. I can’t say it enough, it’s just crazy.”
“This thing just totally changes your life. I was skeptical of this at first, but you have to try it. I would recommend, go through the trial, see how it helps you. Just give it a chance.”
Summary: Researchers characterize a novel neural population within the striatum that appears to be responsible for the interplay between acetylcholine and GABA.
Source: Karolinska Institute
A new study from the Department of Neuroscience at Karolinska Institutet characterizes a novel neuronal population in the basal ganglia, responsible for the interaction between two types of neurotransmitters, GABA and acetylcholine.
The study was recently published in Cell Reports.
The striatum is the main input structure of the basal ganglia, a brain region involved in a variety of sensorimotor functions and reinforcement learning. 99% of striatal neurons are inhibitory GABAergic cells, and the only exception is the population of cholinergic interneurons.
“In previous studies we have showed the interactions between cholinergic interneurons and the dopamine system, and here we focused on the interactions between the cholinergic and GABAergic systems in the striatum,” explains Gilad Silberberg, Professor at the Department of Neuroscience, and main author of the study.
The striatum is strongly modulated by acetylcholine and early treatment for Parkinson’s disease was based on the cholinergic system. Cholinergic interneurons have been shown to change their activity in Parkinson’s disease, Huntington’s disease and in various forms of dyskinesia, all of which are disorders related to striatal function.
“Here we wanted to study how the cholinergic activity shapes striatal activity via nicotine receptors, a specific receptor of acetylcholine,” says Anna Tokarska, Ph.D. student in the Silberberg laboratory and first author of the study.
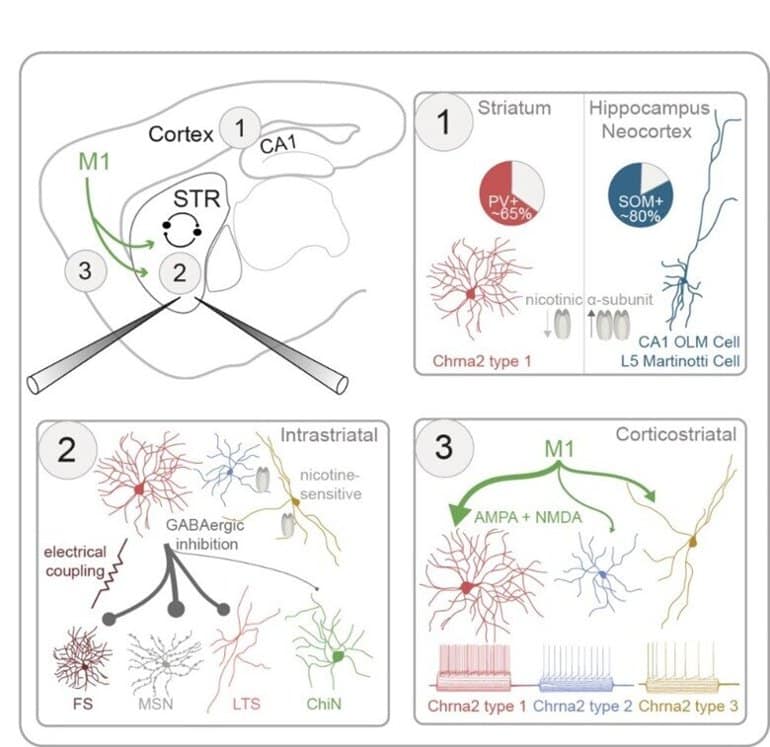
Tokarska and Silberberg characterize the properties of striatal interneurons expressing Chrna2, the gene encoding for the nicotinic α2 receptor subunit. Using patch-clamp recordings they find that striatal Chrna2-interneurons form a diverse neuronal population, which is distinct from Chrna2 neurons in other brain regions (1). Using optogenetics they then map their synaptic outputs (2) and inputs (3) within the striatal network. Credit: Anna Tokarska, Gilad Silberberg
“To do that, we used transgenic mice, marking the striatal interneurons expressing these nicotinic receptors through the Chrna2 gene. We could then use various methods including patch-clamp and optogenetics, to characterize these neurons and their synaptic connectivity in the striatum,” she continues.
The striatal Chrna2 interneuron population was very diverse, including at least three main subpopulations with distinct anatomical and electrical properties. One population was of particular interest, showing novel characteristics including strong response to acetylcholine.
Future steps in this line of research will be to study this population in further detail, including its involvement in striatal function and dysfunction.
Abstract
GABAergic interneurons expressing the α2 nicotinic receptor subunit are functionally integrated in the striatal microcircuit
Highlights
Triple whole-cell recordings are used to study striatal interneurons in Chrna2-Cre mice
Unlike in other brain regions, most striatal Chrna2-interneurons express parvalbumin
Three distinct subtypes of striatal Chrna2-interneurons are defined
Their synaptic connectivity is mapped using optogenetics and patch-clamp recordings
Summary
The interactions between the striatal cholinergic and GABAergic systems are crucial in shaping reward-related behavior and reinforcement learning; however, the synaptic pathways mediating them are largely unknown.
Here, we use Chrna2-Cre mice to characterize striatal interneurons (INs) expressing the nicotinic α2 receptor subunit.
Using triple patch-clamp recordings combined with optogenetic stimulations, we characterize the electrophysiological, morphological, and synaptic properties of striatal Chrna2-INs.
Striatal Chrna2-INs have diverse electrophysiological properties, distinct from their counterparts in other brain regions, including the hippocampus and neocortex.
Unlike in other regions, most striatal Chrna2-INs are fast-spiking INs expressing parvalbumin. Striatal Chrna2-INs are intricately integrated in the striatal microcircuit, forming inhibitory synaptic connections with striatal projection neurons and INs, including other Chrna2-INs. They receive excitatory inputs from primary motor cortex mediated by both AMPA and NMDA receptors.
A subpopulation of Chrna2-INs responds to nicotinic input, suggesting reciprocal interactions between this GABAergic interneuron population and striatal cholinergic synapses.
Summary: Gabapentin, a medication commonly prescribed to control seizure activity, may enhance stroke recovery and restore fine motor function, a new study reports.
Source: Ohio State University
The drug gabapentin, currently prescribed to control seizures and reduce nerve pain, may enhance recovery of movement after a stroke by helping neurons on the undamaged side of the brain take up the signaling work of lost cells, new research in mice suggests.
The experiments mimicked ischemic stroke in humans, which occurs when a clot blocks blood flow and neurons die in the affected brain region.
Results showed that daily gabapentin treatment for six weeks after a stroke restored fine motor functions in the animals’ upper extremities. Functional recovery also continued after treatment was stopped, the researchers found.
The Ohio State University team previously found that gabapentin blocks the activity of a protein that, when expressed at elevated levels after an injury to the brain or spinal cord, hinders re-growth of axons, the long, slender extensions of nerve cell bodies that transmit messages.
“When this protein is high, it interferes with neurological recovery,” said lead author Andrea Tedeschi, assistant professor of neuroscience in Ohio State’s College of Medicine.
“Imagine this protein is the brake pedal and recovery is the gas pedal. You can push on the gas pedal but can’t accelerate as long as you’re also pushing on the brake pedal,” Tedeschi said.
“If you start lifting the brake pedal and continuously press on the gas, you can really speed up recovery. We think that is gabapentin’s effect on neurons, and there is a contribution of non-neuronal cells that tap into this process and make it even more effective.”
The study is published today (May 23, 2022) in the journal Brain.
This work builds upon a 2019 study in which Tedeschi’s lab found in mice that gabapentin helped restore upper limb function after a spinal cord injury.
The primary treatment focus after an ischemic stroke is re-establishing blood flow in the brain as quickly as possible, but this research suggests that gabapentin has no role at that acute stage: The recovery results were similar whether the treatment started one hour or one day after the stroke.
Instead, the drug’s effects are evident in specific motor neurons whose axons carry signals from the central nervous system to the body that tell muscles to move.
After the stroke in study mice, the researchers observed, neurons on the undamaged, or contralateral, side of the brain began sprouting axons that restored signals for upper extremity voluntary movement that had been silenced by neuron death after the stroke. This is an example of plasticity, the central nervous system’s ability to fix damaged structures, connections and signals.
“The mammalian nervous system has some intrinsic ability to self-repair,” said Tedeschi, also a member of Ohio State’s Chronic Brain Injury Program. “But we found this increase in spontaneous plasticity was not sufficient to drive recovery. The functional deficits are not so severe in this experimental model of ischemic stroke, but they are persistent.”
Neurons after an injury have a tendency to become “hyperexcited,” leading to excessive signaling and muscle contractions that may result in uncontrolled movement and pain. While the neural receptor protein alpha2delta2 contributes to the development of the central nervous system, its overexpression after neuronal damage means it hits the brakes on axon growth at inopportune times and contributes to this problematic hyperexcitability.
This is where gabapentin does its work: inhibiting alpha2delta1/2 subunits and enabling post-stroke central nervous system repair to progress in a coordinated way.
“We blocked the receptor with the drug and asked, will even more plasticity occur? The answer is yes,” Tedeschi said.
Because a technique that temporarily silenced the new circuitry reversed behavioral signs of recovery, Tedeschi said the findings suggested the drug normalizes conditions in the damaged nervous system to promote cortical reorganization in a functionally meaningful way.
Compared to control mice that did not receive the drug, mice that received six weeks of daily gabapentin treatment regained fine motor function in their forelimbs. Two weeks after treatment was stopped, researchers observed, functional improvements persisted.
The experiments mimicked ischemic stroke in humans, which occurs when a clot blocks blood flow and neurons die in the affected brain region. Image is in the public domain
“This confirmed that functional changes are solidified in the nervous system,” Tedeschi said.
Gabapentin also appeared to have an effect in the stroke-affected brain on non-neuron cells that influence the timing of message transmission. An examination of their activity after the drug treatment suggested these cells can dynamically change their behavior in response to variations in synaptic communication, further enabling smooth sprouting of axons that were compensating for the lost neurons.
The team is continuing to study the mechanisms behind stroke recovery, but Tedeschi said the findings suggest gabapentin holds promise as a treatment strategy for stroke repair.
Head and neck cancer (HNC) patients endure a gamut of physical sequelae while undergoing a course of radical chemoradiation therapy (CRT). Of these, mucositis and its related symptoms, including pain, remain particularly troublesome for both the patients and their treating clinicians. Current strategies to manage mucositis-related pain rely heavily on opioids; however, this strategy is frequently inadequate, and consequently, many patients will still experience significant discomfort and pain throughout their treatment. The typical escalation of opioids also introduces a host of additional unwanted challenges, such as nausea and vomiting, sedation, and constipation. These concerns have driven mounting interest in the use of adjunct medications such as gabapentin to increase pain control and possibly reduce the need for high-dose opioids. The Multinational Association of Supportive Care in Cancer and International Society of Oral Oncology recently updated their evidence-based clinical practice guidelines for managing mucositis.
The recommendations provided for mucositis-related pain relief are focused mainly on systemic opioids and topical morphine, as a paucity of randomized data has prohibited the development of guidelines specifically addressing the role of adjunct analgesics such as gabapentin.
report the results of a randomized, placebo-controlled, double-blind phase 3 study evaluating the role of prophylactic gabapentin in reducing treatment-related oral mucositis symptoms in patients with oropharyngeal cancer treated with definitive CRT. Eligible patients had stage III to IV disease (American Joint Committee on Cancer Cancer Staging Manual, seventh edition) and could be either human papillomavirus (HPV) positive (49 of 58 [84%]) or negative. All patients received concurrent platinum-based chemotherapy, including carboplatin (7 of 58 [12%]) or high- (32 of 58 [55%]) or low-dose (19 of 58 [33%]) cisplatin. There were competing cooperative group trials enrolling during this period, which were prioritized, and of the 112 study-eligible patients, 65 consented; 58 patients were included in the per-protocol analysis.
The 2 arms were well balanced across relevant demographic, disease, and treatment variables, including baseline opioid use, disease staging, primary and nodal target volumes, and dosimetric factors (mean pharyngeal constrictor and oral cavity doses). Gabapentin was commenced at 300 mg thrice daily during the first week of treatment and increased to 600 mg thrice daily in week 2 (total daily dose 1800 mg)—a dose that was continued through to the week after treatment, at which point patients were quickly weaned off. The placebo was scheduled in a similar fashion, and compliance was documented at weekly interviews, with 12 of 21 doses in any given week considered protocol compliant. Noncompliant patients in the first 2 weeks of treatment (n = 3) were excluded from the final analysis. All patients were recommended lidocaine oral rinses, and opioids were prescribed at the discretion of individual physicians when self-reported pain scores were in excess of 4 of 10 on a numerical scale. The timing and insertion of a feeding tube were individualized and at the discretion of the multidisciplinary team.
This study documented patient-reported outcome measures, opioid use, weight loss, and frequency and duration of feeding tube use. The primary endpoint evaluated the change in the Patient-Reported Oral Mucositis Symptom (PROMS) total score over the entire treatment period (baseline to 6-week post-CRT follow-up). The PROMS scale was developed and validated in the bone marrow transplant setting and includes 10 items assessing mouth pain (single item), the functional impact of mucositis (8 items), and taste change (single item) using a visual analog scale. Secondary outcomes included a prespecified analysis of PROMS item 1 (mouth pain) and a composite score of items 4, 5, 6, and 9; health-related quality of life assessed by the Functional Assessment of Cancer Therapy-Head & Neck (FACT-HN); and a composite score of 4 items on the patient-reported outcomes version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE) relevant to the study toxicities. Repeated-measures analysis of variance demonstrated no between-arm differences in the primary or secondary PROMS endpoints. Interesting, however, was that throughout the study, the primary endpoint scores numerically favored the placebo arm, differences that at times approached but did not reach statistical significance. Importantly, opioid use was also similar for both arms. Similar quality-of-life outcomes were observed with the exception of a smaller negative change from baseline to follow-up in the functional well-being domain of the FACT-HN in favor of the placebo arm (gabapentin −6.0 vs placebo −1.0; P = .03). An increase in the composite PRO-CTCAE score also favored the placebo arm (gabapentin 6.5 vs placebo 1.0, P = .01). Keeping in mind that investigators were blinded to arm allocation, feeding-tube placement was more frequent in the gabapentin arm (18 of 29 [62.1%] vs 6 of 29 [20.7%]; P < .01); however, the median duration of placement was not statistically different (47.5 vs 39.0 days; P = .82). Weight loss from baseline to the last week of treatment was also similar (−11.4% vs −10.7%; P = .81). Overall, this study concluded that gabapentin was ineffective in reducing mucositis-related symptoms and suggested that patients may be adversely affected across several clinically relevant measures.
This study provides arguably the strongest data to date in evaluating the role of prophylactic gabapentin in HNC patients undergoing CRT, given its homogeneous inclusion criteria and placebo-controlled, double-blind design. A number of published retrospective
studies have also reported their outcomes, with mixed results (Table 1). In placing the current study in context, one needs to consider the variations in study design, inclusion criteria (adjuvant/definitive intent, mixed HNC subsites, utilization of induction chemotherapy), gabapentin dosing (protocol specified and received dosing), concomitant analgesics, and the primary assessment of efficacy. A strength to the Cook et al
No difference in breakthrough opioid pain medication
Abbreviations: aCRT = adjuvant CRT; bid = twice daily; BT = breakthrough; CRT = chemoradiation therapy; CUP = carcinoma unknown primary; HPC = hypopharyngeal cancer; LC = laryngeal cancer; MME = morphine milligram equivalent; NACT = neoadjuvant chemotherapy; NPC = nasopharyngeal cancer; OC = oral cavity cancer; OMWQ-HN = oral mucositis weekly questionnaire-head and neck cancer; OPC = oropharyngeal cancer; OR = odds ratio; PROMS = Patient-Reported Oral Mucositis Symptom; Q4h = every 4 hours; qid = 4 times a day; RT = radiation therapy; Sx = surgery; tid = 3 times a day; VAS = visual analog scale; VHNSSv2 = Vanderbilt Head and Neck Symptom Survey version 2.
Primary endpoint was clinician reported.
† Interim analysis.
‡ suggests that patient on the gabapentin arm would have approximately 55% chance of exceeding a given pain score compared to a patient in the standard therapy arm.
has demonstrated any efficacy in pain reduction with prophylactic gabapentin. In this study, 71 HNC patients undergoing CRT (either definitive or adjuvant) had their pain assessed with the 4-item composite pain subscale of the Vanderbilt Head and Neck Symptom Survey.
With the use of a proportional odds model adjusted for time and baseline pain scores, the authors reported that gabapentin resulted in a significant reduction in the composite pain subscale (odds ratio = 0.549; 95% confidence interval, 0.364-0.827; P = .004). However, when the analysis was restricted to mucositis-related pain, gabapentin failed to show ongoing efficacy. Furthermore, the authors did not observe any reduction in opioid use, an outcome reported in only 1 of the 4 prospective studies. In that study, Hermann et al
reported a reduction in the number of patients requiring opioids when treated with high-dose gabapentin. Conversely, patients in the low-dose gabapentin and methadone arm were reported to have lower total opioid requirements. Drawing definite conclusions from this study is difficult owing to differences in gabapentin dosing and the use of different short- and long-acting opioids in the 2 study arms.
One criticism of the current study may be the protocol-specified dosing of gabapentin (1800 mg daily). Daily gabapentin maintenance doses ranged from 900 mg to 2700 mg across the 4 prospective studies. Patients may not tolerate dosages at the higher end of this range, largely due to somnolence and fatigue, and this may be compounded by cisplatin-induced kidney injuries, given gabapentin is exclusively renally eliminated. Although Smith et al
recommended titrating to a maximal daily dose of 2700 mg, most patients were maintained at the lower dose of 900 mg daily, providing support for the use of the dose specified by Cook et al.
In addition, >80% of participants in the current study had HPV-positive oropharyngeal cancer, a group shown to experience higher rates of acute and subacute mucositis and more severe mucositis-related pain.
Although HPV status was balanced between the 2 arms in the current study, it is possible that gabapentin is simply too weak a remedy for this kind of pain.
There are some caveats to this study. The analysis was per protocol rather than intention to treat, and arguably patients who were noncompliant (n = 3) or who experienced acute renal impairment during treatment (n = 1) should not have been excluded from the analysis. The study may also have been slightly underpowered; however, any effect seen in this study was in favor of the placebo arm, and it is very unlikely that a slightly larger study would have yielded a benefit in favor of gabapentin. Although the instrument (PROMS) used for primary assessment of efficacy has not been specifically validated in the studied population, its validity has been tested in patients with oral mucositis in other settings and seems highly likely to be fit for this purpose.
should be commended for conducting this important study and providing the most compelling evidence to date on the efficacy of prophylactic gabapentin in managing mucositis-related symptoms and pain during HNC-CRT. Although this study comes with several caveats, it is the only placebo-controlled, double-blind study available, thus providing results that are likely to be the least biased. Although larger, well-designed studies would be welcome in the future, there is, at present, little evidence to recommend prophylactic gabapentin during HNC-CRT. Treatment of mucositis-induced pain in HNC patients receiving CRT remains an unmet need, and preclinical and clinical research efforts are required to find novel solutions to this highly demanding symptom.
Gabapentin and pregabalin (Lyrica) are prescribed frequently for lumbosacral radicular pain, despite a lack of evidence that they are effective for this condition. In this randomized trial from Australia, researchers randomized 209 patients with sciatica to receive either pregabalin (titrated from 150 mg to 600 mg, depending on response and side effects) or placebo for as long as 8 weeks. At enrollment, duration of pain had been 1 week to 1 year (mean, 2 months); all patients had pain radiating below the knee and either dermatomal pain distribution, motor or sensory deficit, or diminished reflex. The primary outcome was leg pain at 8 weeks.
Improvement in the mean leg-pain score at 8 weeks actually was slightly greater in the placebo group than in the pregabalin group (decrease of 3.0 vs. 2.6 points, from a mean baseline of ≈6.1 on a 10-point scale), but the difference was not statistically significant; pain scores remained similar in the two groups at 1 year. Moreover, the groups did not differ on any secondary outcome (e.g., ratings of disability, quality of life, and global perceived effect). However, the frequency of side effects was significantly higher with pregabalin than with placebo — dizziness was most common (40% vs. 13%).
COMMENT
Pregabalin does not relieve pain associated with sciatica and should not be prescribed for this purpose; presumably, the same holds true for the related drug gabapentin. This finding is not surprising: Although pregabalin has some efficacy — and is FDA-approved for use — in patients with postherpetic neuralgia or diabetic peripheral neuropathy, the pathogenesis of pain in those conditions is different from that of radicular pain.





COMMENT
Pregabalin does not relieve pain associated with sciatica and should not be prescribed for this purpose; presumably, the same holds true for the related drug gabapentin. This finding is not surprising: Although pregabalin has some efficacy — and is FDA-approved for use — in patients with postherpetic neuralgia or diabetic peripheral neuropathy, the pathogenesis of pain in those conditions is different from that of radicular pain.
Source:http://www.jwatch.org