Ribociclib has been shown to have a significant overall survival benefit in patients with hormone receptor (HR)–positive, human epidermal growth factor receptor 2 (HER2)–negative advanced breast cancer. Whether this benefit in advanced breast cancer extends to early breast cancer is unclear.
METHODS
In this international, open-label, randomized, phase 3 trial, we randomly assigned patients with HR-positive, HER2-negative early breast cancer in a 1:1 ratio to receive ribociclib (at a dose of 400 mg per day for 3 weeks, followed by 1 week off, for 3 years) plus a nonsteroidal aromatase inhibitor (NSAI; letrozole at a dose of 2.5 mg per day or anastrozole at a dose of 1 mg per day for ≥5 years) or an NSAI alone. Premenopausal women and men also received goserelin every 28 days. Eligible patients had anatomical stage II or III breast cancer. Here we report the results of a prespecified interim analysis of invasive disease–free survival, the primary end point; other efficacy and safety results are also reported. Invasive disease–free survival was evaluated with the use of the Kaplan–Meier method. The statistical comparison was made with the use of a stratified log-rank test, with a protocol-specified stopping boundary of a one-sided P-value threshold of 0.0128 for superior efficacy.
As of the data-cutoff date for this prespecified interim analysis (January 11, 2023), a total of 426 patients had had invasive disease, recurrence, or death. A significant invasive disease–free survival benefit was seen with ribociclib plus an NSAI as compared with an NSAI alone. At 3 years, invasive disease–free survival was 90.4% with ribociclib plus an NSAI and 87.1% with an NSAI alone (hazard ratio for invasive disease, recurrence, or death, 0.75; 95% confidence interval, 0.62 to 0.91; P=0.003). Secondary end points — distant disease–free survival and recurrence-free survival — also favored ribociclib plus an NSAI. The 3-year regimen of ribociclib at a 400-mg starting dose plus an NSAI was not associated with any new safety signals.
CONCLUSIONS
Ribociclib plus an NSAI significantly improved invasive disease–free survival among patients with HR-positive, HER2-negative stage II or III early breast cancer.
The first British Society of Gastroenterology (BSG) and Healthcare Infection Society (HIS)-endorsed faecal microbiota transplant (FMT) guidelines were published in 2018. Over the past 5 years, there has been considerable growth in the evidence base (including publication of outcomes from large national FMT registries), necessitating an updated critical review of the literature and a second edition of the BSG/HIS FMT guidelines. These have been produced in accordance with National Institute for Health and Care Excellence-accredited methodology, thus have particular relevance for UK-based clinicians, but are intended to be of pertinence internationally. This second edition of the guidelines have been divided into recommendations, good practice points and recommendations against certain practices. With respect to FMT for Clostridioides difficile infection (CDI), key focus areas centred around timing of administration, increasing clinical experience of encapsulated FMT preparations and optimising donor screening. The latter topic is of particular relevance given the COVID-19 pandemic, and cases of patient morbidity and mortality resulting from FMT-related pathogen transmission. The guidelines also considered emergent literature on the use of FMT in non-CDI settings (including both gastrointestinal and non-gastrointestinal indications), reviewing relevant randomised controlled trials. Recommendations are provided regarding special areas (including compassionate FMT use), and considerations regarding the evolving landscape of FMT and microbiome therapeutics.
BACKGROUND: Cholinesterase inhibitors (ChEIs) are regularly used in Alzheimer’s disease. Of the three ChEIs approved for dementia, donepezil is among the most prescribed drugs in the United States with nearly 6 million prescriptions in 2020; however, it is classified as a “known risk” QT interval-prolonging medication (QTPmed). Given this claim is derived from observational data including single case reports, we aimed to evaluate high-quality literature on the frequency and nature of proarrhythmic major adverse cardiac events (MACE) associated with donepezil.
METHODS: We searched Medline, Embase, International Pharmaceutical Abstracts, and Cochrane Central from 1996 onwards for randomized controlled trials (RCTs) involving patients age =18 years comparing donepezil to placebo. The MACE composite included mortality, sudden cardiac death, non-fatal cardiac arrest, Torsades de pointes, ventricular tachyarrhythmia, seizure or syncope. Random-effects meta-analyses were performed with a treatment-arm continuity correction for single and double zero event studies.
RESULTS: Sixty RCTs (n = 12,463) were included. Twenty-five of 60 trials (n = 5886) investigated participants with Alzheimer’s disease and 33 trials monitored electrocardiogram data. The mean follow-up duration was 31 weeks (SD = 36). Mortality was the most commonly reported MACE (252/331, 75.8% events), the remainder were syncope or seizures, with no arrhythmia events. There was no increased risk of MACE with exposure to donepezil compared to placebo (risk ratio [RR] 1.08, 95% CI 0.88-1.33, I2 = 0%) and this was consistent in the subgroup analysis of trials including participants with cardiovascular morbidities (RR 1.14, 95% CI 0.88-1.47). Subgroup analysis suggested a trend toward more events with donepezil with follow-up =52 weeks (RR: 1.32, 0.98-1.79).
CONCLUSIONS: This systematic review with meta-analysis found donepezil may not be arrhythmogenic. Donepezil was not associated with mortality, ventricular arrhythmias, seizure or syncope, although longer durations of therapy need more study. Further research to clarify actual clinical outcomes related to QTPmed is important to inform prescribing practices.
Multi-faceted evidence from a range of cancers suggests strongly that de novo expression of voltage-gated sodium channels (VGSCs) plays a significant role in driving cancer cell invasiveness. Under hypoxic conditions, common to growing tumours, VGSCs develop a persistent current (INaP) which can be blocked selectively by ranolazine.
Methods
Several different carcinomas were examined. We used data from a range of experimental approaches relating to cellular invasiveness and metastasis. These were supplemented by survival data mined from cancer patients.
Results
In vitro, ranolazine inhibited invasiveness of cancer cells especially under hypoxia. In vivo, ranolazine suppressed the metastatic abilities of breast and prostate cancers and melanoma. These data were supported by a major retrospective epidemiological study on breast, colon and prostate cancer patients. This showed that risk of dying from cancer was reduced by ca.60% among those taking ranolazine, even if this started 4 years after the diagnosis. Ranolazine was also shown to reduce the adverse effects of chemotherapy on heart and brain. Furthermore, its anti-cancer effectiveness could be boosted by co-administration with other drugs.
Conclusions
Ranolazine, alone or in combination with appropriate therapies, could be reformulated as a safe anti-metastatic drug offering many potential advantages over current systemic treatment modalities.
Clinical potential and conclusion
From the available evidence, taken together, we can propose that ranolazine could be utilised as an anti-metastatic drug [56]. Indeed, the evidence, at all levels from in vitro to human, is consistent for the role of ranolazine in suppressing cellular invasiveness and full-blown metastasis in several different carcinomas. Ranolazine has been in clinical use against angina pectoris for several years and, more recently, it has proven to be highly effective also against arrhythmia. Thus, it has a well-known dosage and safety profile. Nevertheless, some adverse side effects have been reported, including dizziness, headaches, nausea, debility and constipation [https://www.ncbi.nlm.nih.gov/books/NBK507828/]. Furthermore, it is recommended that ranolazine is not used together with some drugs such as other VGSC modulators (e.g., carbamazepine, phenytoin), as mentioned above for propranolol [31], antidepressants (e.g., nefazodone, amitriptyline), anticonvulsants (e.g., phenobarbital), CYP3A4 inhibitors (e.g., ketoconazole, diltiazem, verapamil), and anti-fungals/bacterials (e.g, itraconazole, ketoconazole, clarithromycin) [https://www.ncbi.nlm.nih.gov/books/NBK507828/]. There are also some reports of ranolazine inducing long QT, but this is likely to occur only at higher doses [57].
Another advantage of targeting INaP is the fact that the VGSC generating this current is essentially a functional biomarker. Accordingly, patients can readily be stratified by their profile of VGSC protein expression by immunohistochemical staining of their biopsies which is done routinely in hospital pathology laboratories. Ranolazine therapy would be appropriate only for patients whose biopsies were found to express VGSC protein. In this regard, we have already developed a polyclonal antibody specific for nNav1.5 [58] and a novel monoclonal antibody is currently being validated.
In overall conclusion, ranolazine has the potential to be readily adopted as an anti-metastatic drug, either by itself or in appropriate combination with a mechanistically compatible agent and this can be done as precision medicine. Further studies are justified to examine whether ranolazine could keep tumours in a localised state and thus enable patients to live with their cancer as a chronic disease, as with chronic angina.
The beneficial effects of folate have been observed under different conditions, but the available evidence on inflammation and reduction of cardiovascular disease (CVD) in type 2 diabetes mellitus (T2DM) is limited. The study aimed to explore the effects of folate on inflammation and homocysteine amongst individuals with T2DM.
Methods
PubMed, Scopus, and Cochrane Library were used to search for evidence. A random-effect model meta-analysis through Review Manager (version 5.4) and metaHun was performed. Results were reported as standardized mean differences (SMD) and 95% confidence intervals graphically using forest and funnel plots.
Results
Data from 9 trials with 426 patients living with T2DM were analyzed. Folic acid supplementation significantly revealed a large effect size on homocysteine levels compared to placebo, SMD = −1.53, 95%CI (−2.14,−0.93), p < 0.05. Additionally, we observed a medium marginal effect size on C-reactive protein (SMD = −0.68, 95%CI (−1.34, −0.01), p = 0.05). However, no significant effect on tumor necrosis factor-α (SMD = −0.86, 95%CI (−2.65, 0.93), p = 0.34), and interleukin-6 (SMD = −0.04, 95%CI (−1.08, 1.01), p = 0.95) was observed.
Conclusion
Evidence analyzed in this study suggests that folic acid supplementation in T2DM reduces homocysteine and may mitigate CVDs. However, its effect on inflammation is inconclusive.
Discussion
To the best of our knowledge, this is the first comprehensive meta-analysis of RCT to evaluate the effect of folic acid supplementation on homocysteine and inflammation in adult patients with T2DM. We found that folic acid supplementation was associated with a reduction in homocysteine levels. The observed SMD (1.52) was large effect, suggesting anti-homocysteine properties. Additionally, there was a marginal effect of folic acid on CRP without a significant effect on TNF-α and IL-6 in patients with T2DM. Subgroup analysis showed that the folate effect on homocysteine was more pronounced at a higher dose (10 mg) than 5 mg supplementation. However, it is important to note that only one trial used 10 mg compared to 5 mg that used 5 mg of folic acid. It was evident that studies with a sufficient sample size (50 and above patients) had a more pronounced effect than those with a smaller sample size. Although folic acid supplementation at both short and medium periods reduced homocysteine, the reduction was more pronounced at short periods (0–4 weeks) compared to medium periods (8–12 weeks). Our research reveals lower homocysteine levels in individuals living with T2DM receiving folate supplements, indicating a potential decrease in the risk of CVD. We are confident with the evidence synthesized in this study as the evidence showed moderate certainty in homocysteine. In T2DM, insulin resistance and associated impaired kidney function results in an elevated homocysteine level [43,44,45,46,47]. This elevation promotes the development of CVD complications associated with T2DM.
Interestingly, the evidence from this study shows that folic acid supplementation can reduce homocysteine by converting it into methionine, lowering the risk of cardiovascular complications in T2DM patients [26]. Notably, previous evidence has shown that folic acid supplementation can reduce homocysteine levels in patients living with T2DM by increasing the 5-methyltetrahydrofolate intracellular pool [37]. This effect is crucial as an elevated level of homocysteine can damage blood vessels and contribute to the development of CVD [45]. Therefore, any strategies therapeutically that reduce homocysteine may assist in alleviating CVD among T2DM. In obese children, similar trends have been observed when administering a minimum of 1 g of folic acid, leading to a substantial reduction in homocysteine levels [48]. Similar findings are observed in gestational diabetes, as 1 mg and 5 mg of folic acid supplementation significantly reduced homocysteine levels [49]. Although the pathological and physiological mechanisms of these conditions differ, these findings demonstrate the efficacy of folate supplementation across diverse conditions and age groups. A non-randomized trial in menopausal T2DM women also showed that 800 µg of folate significantly reduced homocysteine levels. However, this study revealed an inverse correlation between folic acid and homocysteine (r = −0.4876, p-value = 0.0134) [50]. Although the mechanism by which folate reduces homocysteine in T2DM is poorly documented, it is assumed that this is associated with the role of folate in one-carbon metabolism. Folic acid supplementation increases the availability of one-carbon units, which then promotes the remethylation of homocysteine to methionine [51]. This subsequently results in a decrease in homocysteine levels in the body. While such benefits are acknowledged, contrasting findings from other studies suggest a possible risk of CVD in T2DM, even with folic acid supplementation [52]. These findings suggest a limitation in the beneficial effect of folate, especially in T2DM. It is assumed that folate deficiency impairs the conversion of homocysteine to methionine, resulting in homocysteine accumulation in the blood [53]. High homocysteine levels are associated with an increased risk of CVDs and other health problems.
Although there was a marginal effect on hs-CRP (p = 0.05), no significant effect of folic acid supplementation on other markers of inflammation was observed. This was shown by no significant effect on TNF-α and IL-6 following supplementation with folic acid compared to placebo. A reduction in hs-CRP following folic acid supplementation reveals, to some extent, the beneficial effect of folic acid as an anti-inflammatory agent. However, as not all inflammatory markers were reduced, the findings are thus inconclusive. Among some factors contributing to the challenge in elucidating conflicting findings regarding the impact of folic acid on inflammation is the limited number of trials conducted. The inability of folic acid to improve some markers of inflammation indicates that it does not exhibit anti-inflammatory properties. For instance, Spoelstra-de Man et al., [23] reported no effect of folic acid on hs-CRP, IL-6, and TNF-α. The same findings were observed by Title et al. [27], however, only TNF-α and hs-CRP were investigated, and no effect was observed. Despite these null findings, another trial observed a significant effect of folic acid on hs-CRP in T2DM, as demonstrated by a significant decrease in hs-CRP within the folic acid group before and after folic acid supplementation. This same trend was also observed when folic acid supplementation was compared to placebo [24]. The latter supports our findings as we observed a reduction in hs-CRP with a medium to large effect size (Cohen d = 0.68). Other researchers reported a significant decrease in IL-6 and TNF-α following folic acid supplementation compared to placebo, suggesting the anti-inflammatory effects of folic acid in T2DM [38]. These findings differ from our overall findings in this study as we reported no significant effect of folic acid on TNF-α and IL-6. Another study showed a significant change between baseline and post-treatment on hs-CRP, however, there were no significant changes between the folic acid and placebo groups [38]. In obese children, 1 mg of folic acid has proven to offer an anti-inflammatory effect, as demonstrated by a significant decrease in IL-6, TNF-α, and IL-8 [48].
Similarly, El-khodary et al. [37] also showed a significant decrease in hs-CRP between baseline and post-treatment (p = 0.008). The same trial reported a significant decrease in hs-CRP following three months of folic acid supplementation compared to placebo (p = 0.005). This study also showed a positive correlation between homocysteine and hs-CRP (r = 0.308, p = 0.002). Due to these contradicting results on inflammation, the effect of folic acid on inflammation is not clear, other researchers have suggested that folic acid may be involved in the reduction of hs-CRP by reducing homocysteine and oxidative stress. For instance, Talari et al., [24] reported an increased adjusted glutathione (GSH) following folic acid supplementation in T2DM compared to placebo.
Additionally, folic acid exhibits anti-insulinemic activities [54, 55] may further alleviate inflammation by suppressing the synthesis of inflammatory cytokines. It is important to note that while the benefits were not observed in this study, this might be attributable to the number of trials analyzed primarily because observational differences were noted. Previous evidence suggests that homocysteine promotes the expression of inflammatory markers by increasing the activation of nuclear factor kappa β (NF-kβ) and poly-adenosine diphosphate (ADP) ribose polymerase. Therefore, we speculate that folic acid anti-homocysteine properties may alleviate inflammation by inhibiting the activation of NF-κβ and ADP and thus suppressing the expression of inflammatory markers [56, 57]. Evidence from in vitro studies has also shown that folic acid may reduce inflammation by inhibiting the phosphoinositide 3-kinases (PI3K)/hypoxia-inducible factor 1-alpha (HIF-1α) pathway [58]. Even though the reduction in homocysteine following folate supplementation is normally accompanied by a reduction in CRP and subsequent deactivation of NF-κβ and low IL-6 and TNF-α, the contradictory findings observed in our study may be due to few trials and sample size across the trials analyzed in this study.
Strength and limitation
The present analyses exclusively examined evidence from randomized trials, considered to provide high clinical evidence. Notably, there was a low risk of bias observed across various domains in the risk of bias assessment, indicating that the quality of the studies was satisfactory. The GRADE tool was also employed to evaluate the overall quality of the analyzed evidence, and it was categorized as either moderate or very low in one outcome due to the small sample size.
Furthermore, a comprehensive subgroup analysis was performed, considering various confounding factors. The I2 statistics revealed moderate heterogeneity. For transparency, the study was registered with PROSPERO, and the experienced researchers adhered to PRISMA guidelines, boosting confidence in the reliability of the current findings. However, it is crucial to acknowledge certain limitations in our study, such as few relevant trials, indicating a minimal sample size of only 426 patients living with T2DM. Moreover, existing trials have employed varying quantitative methodologies, introducing potential differences in sensitivity and specificity, especially with the use of ELIZA AND HPLC for the determination of homocysteine.
Conclusion and future recommendations
The findings from nine trials involving a sample of 426 participants in this study indicate that folic acid supplementation in T2DM may reduce homocysteine levels, a potential biomarker for CVDs. However, due to the limited number of trials analyzed, null effects were observed concerning some of the inflammatory markers. It is crucial to interpret the conclusions of our study with caution, emphasizing the need for further trials with adequate sample sizes.
Considering the limitations acknowledged in this study, we propose recommendations for future investigations into folic acid in T2DM, particularly focusing on inflammation. We suggest that forthcoming RCTs use sufficient sample sizes and adhere to the reporting guidelines outlined in the consolidated standards of reporting trials (CONSORT). Additionally, these trials should adhere to standardized methodologies, implementing an accurate randomization process, blinding of personnel and participants. Furthermore, we emphasize the necessity for high-quality meta-analyses to comprehensively elucidate the benefits of folic acid supplementation in managing T2DM.
Dietary imbalance, such as a lower proportion of complex carbohydrates and a higher protein diet, may contribute to gestational diabetes mellitus (GDM) risks through their metabolisms. However, there is a lack of knowledge regarding the association between butyrate, iso-butyrate, and GDM, which are metabolisms of the two primary nutrients above. This study aimed to clarify the association of butyrate and iso-butyrate with GDM.
Methods
A nested case–control study was conducted based on the Beijing Birth Cohort Study (BBCS) from 2017 to 2018. Totally, 99 singleton women were involved (GDM: n = 49, control: n = 50). All participants provided blood samples twice (in their first and second trimesters). Gas chromatography-mass spectrometry (GC-MS) was used for butyrate and iso-butyrate detection. Unconditional logistic regression and receiver operating characteristic (ROC) curve analysis were used for statistical analysis.
Results
The results showed that butyrate in the first trimester was negatively correlated with GDM (odds ratio (OR): 0.00, 95% confidential interval (CI): 0.00–0.21, P = 0.008), and iso-butyrate in the second trimester was positively related to GDM (OR: 627.68, 95% CI: 40.51–9724.56, P < 0.001). The ratio (butyrate/iso-butyrate) was negatively associated with GDM, both in the first trimester (OR: 0.00, 95%CI: 0.00–0.05, P < 0.001) and in the second trimester (OR: 0.52, 95% CI: 0.34–0.80, P = 0.003). The area under the curve (AUC) using the ratio in the first trimester combined with clinical risk factors achieved 0.89 (95% CI: 0.83–0.95). Iso-butyrate in the second trimester combined with clinical risk factors achieved an AUC of 0.97 (95% CI: 0.92–1.00).
Conclusions
High iso-butyrate and low butyrate levels may be associated with an increased risk of GDM. As they are produced through dietary nutrient formation by gut microbiota, further studies on the association of dietary intake and butyrate or iso-butyrate concentration in plasma may help find a novel approach to nutritional intervention for GDM.
Discussion
This nested case–control study evaluated the association of butyrate and iso-butyrate with the risk of GDM. We found that butyrate was negatively correlated with GDM risks, while iso-butyrate was positively related to GDM risks in the first half of pregnancy. Clinical risk factors combined with butyrate/iso-butyrate in T1 or iso-butyrate in T2 showed a superior predictive efficiency for GDM.
One cohort study conducted in the Mediterranean region of Northern Spain reported an average level and reference interval (2.5 percentile to 97.5 percentile) of butyrate and iso-butyrate in pregnant women with normal glycemia during the first and third trimesters [35]. As reported, the median level of butyrate and iso-butyrate in T1 were 0.73 μmol/L (0.16–1.01 μmol/L) and 0.45 μmol/L (0.32–1.67 μmol/L). The average level of butyrate in our study was lower than that in the previous research, while iso-butyrate was much higher. Dietary diversity may mediate differences in metabolite levels between studies. It has been reported that the Mediterranean diet (MD) score was associated with a higher concentration of butyrate [36]. Participants in the previous study made a MD the primary diet, which referred to a rich variety of plant foods (fruits, vegetables, potatoes, whole grains, legumes, nuts, seeds, etc.). Full contains complex insoluble dietary fiber provide sufficient substrate for butyrate production. However, Chinese eating habits are still omnivorous, and animal protein accounts for a large proportion.
Butyrate’s protective effect on plasma glucose level and insulin resistance has also been evidenced in type 2 diabetes population and animal studies [17, 18, 37,38,39,40,41,42,43,44]. However, current study results on the relationship between butyrate and GDM were inconsistent. A few previous studies showed a decreased level of butyrate and an impaired butyrate metabolism in women with GDM [23, 45, 46]. A previous study with a sample size of 30 women with GDM and 30 women without gestational complications explored potential serum metabolites biomarkers of GDM and related pathways. The results showed that 36 differential metabolites and corresponding metabolic pathways were identified in serum, including fatty acid metabolism, butyrate metabolism, bile secretion, and amino acid metabolism [46]. Study conducted in Beijing with 20 women with GDM and 40 healthy controls unveiled a lower butyrate in GDM group in the second and third trimester [23]. An experimental study investigated the effect of butyrate on insulin signaling defects in an in vitro model of GDM. Butyrate was found to reverse TNF-induced increases in IRS-1 serine phosphorylation and decreases in glucose uptake, indicating that the butyrate may be able to improve insulin sensitivity in GDM models [45]. Consistent with the above findings, our results also revealed a lower level of butyrate in women with GDM and a negative relationship between butyrate and GDM, both in T1 and T2. However, there was still at least one previous study reported that there was no significant difference in butyrate concentration between the GDM and control group [22, 47]. Pregnant healthy women without GDM (n = 20) and women with GDM in three different patterns (n = 31, 31, 22, respectively) were included in the analysis and liquid chromatography coupled with mass spectrometry (LC-MS/MS) was used for SCFA detection [47]. Small sample sizes, different population characters and diet habits, sampling time, and detection methods for SCFAs may account for different study results. The possible mechanism of butyrate in glucose and insulin resistance regulation may be related to the following aspects [11, 48] 1) appetite inhibition, leading to reduced energy intake; 2) intestinal barrier protection. It can protect the body from endotoxemia and chronic low-grade systemic inflammation; 3) free fat acid receptors (FFAR) activation or histone deacetylase inhibition. It may affect the expression of glucose regulation related genes or the secretion of glucose regulatory hormones directly or indirectly; 4) Immunosuppression. Butyrate may inhibit the expression of inflammatory factors and systemic inflammatory response; 5) β cell protection.
As part of branched short chain fatty acids (BSCFAs), iso-butyrate was mainly produced from the formation of BCAAs (including leucine, isoleucine or valine) by gut microbiota. Data on the metabolic effects of iso-butyrate is sparse. An animal study proposed for the first time claimed that protein derived from the western diet-induced insulin resistance in mice by increasing the level of iso-butyrate [49]. Results from human study also showed an increased level of iso-butyrate in the GDM group with a small sample size (n = 28 in the GDM group and n = 27 in the healthy pregnant women group) [50]. Similarly, our results revealed a positive relationship between iso-butyrate concentration and GDM risks. The superior predictive effect using iso-butyrate in the second trimester combined with clinical risk factors with an AUC of 0.97 also indicates that iso-butyrate may be a prospective biomarker for GDM diagnosis in the second trimester. However, a contrary conclusion was made through an experimental study conducted in vitro. It found that iso-butyrate has effects on adipocyte lipid and glucose metabolism that can contribute to improved insulin sensitivity in individuals with disturbed metabolism [51]. The difference in the environment of vivo and vitro may mediate the contradictory results. Limited research focused on the mechanism of iso-butyrate on GDM or insulin resistance. Only one study published in Nature Communications in 2021 proclaimed that elevated BSCFAs were associated with insulin resistance and glucose intolerance in mice [49]. The study further showed that the BSCFA, iso-butyrate and iso-valerate, induced hepatocytes insulin resistance by potentiating hepatic mTORC1/S6K1 signaling [49]. Further studies are needed to confirm the relationship between iso-butyrate and glucose regulation and clarify the possible mechanisms.
Since the different sources of fermentation substrate of butyrate and iso-butyrate, complex carbohydrates and dietary protein respectively, butyrate/iso-butyrate may reflect the balance of dietary nutrition intake to some extent and be a good health indicator. A cross-sectional study declared a tendency for butyrate levels to be higher in vegetarians (high dietary fiber intake) than omnivores, while iso-butyrate levels were lower in vegetarians [16]. A high-protein/low-fiber diet shifts the utilization of dietary to endogenously supplied proteins, causing elevated levels of cytotoxic and pro-inflammatory metabolites (such as iso-butyrate) [52]. However, there were no studies focused on the relationship between the ratio and GDM. Our results suggested that butyrate/iso-butyrate may be a protector for GDM and had a better predictive effect than butyrate or iso-butyrate alone. The superior predictive efficiency of butyrate/iso-butyrate in T1 for GDM evidenced its potential as a promising biomarker for GDM prediction.
Various studies have reported that women with GDM were characterized by a lower Firmicutes/ Bacteroidetes ratio, with a depleted abundance of butyrate-product bacteria, such as Prevotella, Coprococcus, Ruminococcaceae, Eubacterium species, Roseburia, Dialister, Lachnospiraceae, et al. [53,54,55,56]. Coprococcus has been evidenced to be positively correlated with serum SCFA levels (acetate, valerate, butyrate, et al.) in women with GDM [22]. In addition, BSCFAs abundance, the marker of BCAAs fermentation, has also been reported to be related to decreased Firmicutes and increased unknown Bacteroidetes in an artificial colon model of high-protein diets [57]. Blautia, a kind of BSCFAs (mainly including iso-butyrate, iso-valerate) production bacteria, was found in higher abundance in people with GDM [58]. Moreover, It has been reported that patients with GDM were characterized by an up-regulated metabolite of valine, which was the main substrate for iso-butyrate production [55]. Random forest analysis using fecal metabolites (5-Hydroxyindoleacetic acid and valine) also showed a high diagnostic performance with an AUC of 0.843 [55]. The findings above indicate that microbiota disturbance might contribute to GDM risks through metabolites. However, direct evidence still needs to prove the possible relationship among gut microbiota, metabolisms, and GDM in further studies.
Our study proclaimed for the first time that butyrate/iso-butyrate may be a potential biomarker for GDM early prediction in views of nutrition metabolism. It may also provide a new insight for GDM prevention in views of nutrition intake. Besides, this nested case–control study relied on a prospective cohort study conducted in Beijing; we were able to obtain the accurate information required in the survey, which minimized recall bias.
Still, several limitations should be considered when explaining our results. First, we included no information on dietary nutrient intake, and we could not evaluate the relationship between dietary carbohydrate and protein intake and circulating butyrate and iso-butyrate levels; second, the sample size was relatively small, and it might not be completely transferable to the general population. Besides, the small sample size also restricted further stratified analysis. Future studies with a larger sample size and more detailed analysis are needed to confirm this study’s results.
All in all, our findings suggested that high levels of iso-butyrate and low levels of butyrate may be associated with an increased risk of GDM. As they are produced through dietary nutrients formation by gut microbiota, further studies on the association of dietary intake and butyrate or iso-butyrate concentration in plasma may help find a novel approach to nutritional intervention for GDM. Our findings may also provide new insights into the nutrition intake and the underlying mechanisms linking them to the risk of GDM to inform diet-related preventive strategies for GDM.
Hemoglobin (Hb) Vancleave (NM_000518.5:c.431 A > T; dbSNP: rs33918338) is an extremely rare structural hemoglobin variant worldwide, and studies are limited. This report describes the case of a 16-year-old male patient who presented with secondary erythrocytosis. The diagnosis of Hb Vancleave, in combination with codon 41/42 (-TTCT) (NM_000518.5:c.126_129del; dbSNP: rs80356821), was confirmed by direct sequencing. This report highlights the importance of sequencing in the differential diagnosis of beta-thalassemia syndrome in Malaysia.
Hemoglobin abnormalities are caused by molecular changes involving two primary globin gene clusters (alpha and/or beta) located on chromosomes 11 (beta; 11p15.4; OMIM# 141900)1 and 16 (alpha; 16p13.3; OMIM# 141800 and 141850)2. The clinical consequences are associated with qualitative (hemoglobinopathies) and/or quantitative (thalassemia) defects in globin chain expression3. Coinheritance of both structural hemoglobinopathies and thalassemia in a patient results in a continuum of complex phenotypes. To date, more than 100 high-oxygen-affinity hemoglobinopathies have been described worldwide, and their presence usually leads to erythrocytosis. Although patients with erythrocytosis are generally asymptomatic, identifying patients with high oxygen affinity is important in young patients or those with high hemoglobin concentrations and a family history of polycythemia4. A correct diagnosis is important for the clinical management and long-term outcome of patients4,5,6.
Hemoglobin Vancleave (HGVS: NM_000518.5:c.431A > T; dbSNP: rs33918338) is an extremely rare beta-globin chain variant, and its prevalence is unknown. Two entries for Hb Vancleave were found in public databases (HbVar ID: 1234 and IthaID: 1298), but no clinical case reports were found in the literature. The molecular basis of Hb Vancleave is based on a single-nucleotide substitution at codon 143 (CAC > CTC) of the HBB gene, which changes the coding amino acid from histidine (His) to leucine (Leu). Theoretically, the side chain difference between leucine and histidine will affect the biochemical characteristics of Hb Vancleave relative to normal hemoglobin. In the normal hemoglobin tetramer, histidine has a positively charged imidazole side chain, which is one of the vital components of the binding site for 2,3-diphosphoglycerate (2,3-DPG), which is essential for regulating the affinity of hemoglobin for oxygen. In contrast, in Hb Vancleave, histidine is substituted with leucine, which contains an isobutyl side chain that converts the 2,3-DPG binding site to a nonpolar form. This subsequently modifies the oxygen affinity of hemoglobin. The same effects of high oxygen affinity were also observed for Hb Abruzzo7, Hb Syracuse8, and Hb Little Rock9, which are similarly altered at codon 143 of the HBB gene.
Malaysia is a tropical country in Southeast Asia where multiethnic populations and mixed marriages are common. Thus, complex genetic interactions from different ethnic backgrounds cause a wide clinical spectrum of hemoglobin disorders in Malaysia. Most of the patients registered in the Malaysian Thalassemia Registry were Malays (63.95%), Chinese (11.75%), and Kadazan-Dusuns (11.36%). However, hemoglobin disorders have rarely been reported among Malaysian Indians10,11. Several clinically important mutations in the HBB gene have been reported in major ethnic groups in Malaysia. Codon 26 (GAG > AAG) Hb E, codon 41/42 (–TTCT), IVS 1–1 (G > T), and IVS 1–5 (G > C) are the most common disease-associated HBB gene variations in Malays, while codon 41/42 (–TTCT) and IVS 2–654 (C > T) were predominantly detected among the Malaysian Chinese population with beta-thalassemia12. Here, we report the first case of Hb Vancleave combined with a severe beta-thalassemia mutation associated with secondary erythrocytosis in a Malaysian Indian teenager.
A 16-year-old student (RS873/23) of Indian Sikh descent initially volunteered to participate in the National Thalassemia Screening Program for secondary school students in Malaysia. His parents provided informed consent for the screening program at his school. Peripheral blood samples and data were collected following the Declaration of Helsinki and the Malaysian National Institute of Health (NIH) guidelines for the conduct of research at Ministry of Health (MOH) institutions and facilities.
The patient was a smoker and currently vapes. At presentation, he was asymptomatic, with a Hb level of 18.3 g/dL. No history of transfusion was reported. The peripheral blood film (PBF) showed packed red cells with hypochromic microcytic erythrocytes for his age. He has two siblings, including his younger sister, who is also asymptomatic. His parents were not consanguineous. His father is a Malaysian Sikh who died at the age of 51 from heart disease and dyslipidemia. No paternal history of thalassemia was reported. His mother is a 42-year-old Indian woman from Uttar Pradesh, India, and she has three siblings who were suspected of having thalassemia, but the diagnosis was never confirmed. In 2014, it was suspected that she had thalassemia during pregnancy, yet no confirmatory test was performed. The family tree of patient RS873/23 is shown in Fig. 1A.
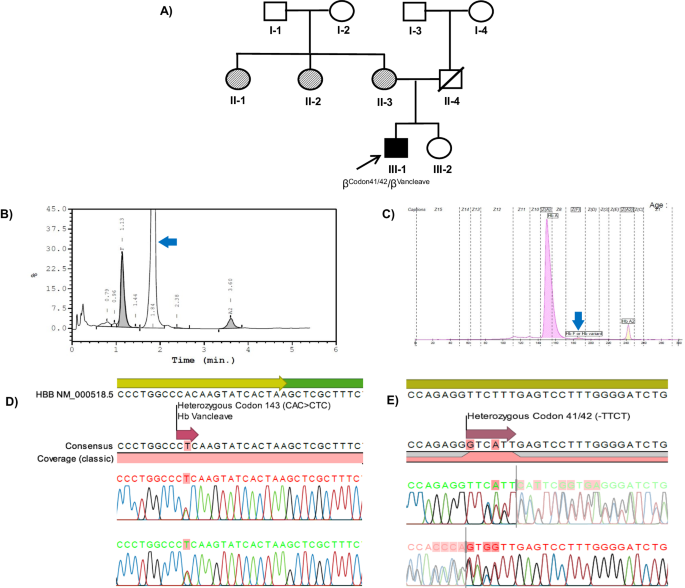
Fig. 1: Family tree, hemoglobin analysis, and sequencing chromatograms of thecase report (III-1; RS873/23).
The peripheral blood of patient RS873/23 was collected for full blood count (FBC) and hemoglobin analysis (Hb analysis). Both FBC and Hb analyses were performed in primary health care facilities. His FBC showed hypochromic microcytic erythrocyte indices, with a red blood cell (RBC) count, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and red cell width (RDW) of 8.94 × 106/µL, 64.2 fL, 20.5 pg and 20.4%, respectively. The peripheral blood film (PBF) showed packed erythrocytes with a hypochromic microcytic morphology. Hemoglobin analysis by capillary electrophoresis (CE; Sebia, France) revealed elevated HbA2 (4.2%) and normal HbA (82.3%) levels (Fig. 1B). An abnormal HbF peak was detected by CE. High-performance liquid chromatography (HPLC; Bio-Rad, USA) revealed that 76.1% of the hemoglobin variants were abnormal, with a retention time of 1.84 min. The HbA2 level was borderline high (3.7%), and the HbF level was elevated (16.8%) (Fig. 1C). The results of hemoglobin analysis suggested hereditary persistence of fetal hemoglobin (HPFH) or delta-beta-thalassemia.
Molecular investigations to detect common and unknown beta-globin gene cluster deletions that are associated with HPFH and delta-beta-thalassemia phenotypes were carried out by using multiplex gap polymerase chain reaction (MGap-PCR) and multiplex ligation probe-dependent amplification (MLPA). However, no deletions were detected. Therefore, we suspected that this patient might have compound or homozygous HBB gene mutations that can cause both elevated HbF (16.8%) and an abnormal peak (76.1%) at a retention time of 1.84 min on HPLC. Direct sequencing was carried out to detect disease-associated variations in the beta-globin gene (HBB; RefSeq ID: NM_000518.5), and the results confirmed the presence of compound heterozygous variants of codon 41/42 (-TTCT) [HGVS: (NM_000518.5:c.126_129del)] (Fig. 1D) and codon 143 (CAC > CTC) Hb Vancleave (Fig. 1E). A summary of the hematology and molecular test results in this study is provided in Table 1.Table 1 Hematology and DNA analysis findings for the case RS873/23.
Our case is an incidental finding from the National Thalassemia Screening Program in Malaysia. This is the first case report in the literature and the first identification of Hb Vancleave in the Malaysian population. The majority of hemoglobin disorders are inherited as autosomal recessive. However, in some cases, disease-associated genetic variations in globin gene clusters can be caused by de novo or dominant genetic variations. In this study, we identified a case of a Malaysian patient with compound heterozygous variants of Hb Vancleave and codon 41/42 (-TTCT), which are rare among Indian Sikh in Malaysia. The inheritance pattern of these variations cannot be determined because parental samples were not available. Nevertheless, we speculate that his father might be homozygous for Hb Vancleave, which could cause polycythemia and hyperviscosity syndrome; this condition might have led to his heart problems and subsequent death at the age of 51 years, which is considered young for heart disease and complications of cardiomyopathy. The clinical phenotypes were comparable to those of another patient with high oxygen affinity—a 4-year-old Malay girl with homozygous Hb Tak who presented with symptomatic polycythemia and congestive heart failure13. Hb Tak is mildly unstable; thus, patients in a homozygous state are more symptomatic and present with symptoms early in life.
A common disease-associated frameshift variation at codon 41/42 (-TTCT) compounded with Hb Vancleave was detected in our index patient. The four-nucleotide deletion between codons 41 and 42 of the HBB gene results in a stop codon at codon 59, which subsequently terminates translation and reduces the rate of beta-globin chain synthesis. The genetic alteration of codon 41/42 (-TTCT) has been reported in many populations, including Chinese, Malaysian, Singaporean, Taiwanese, Thai, Punjabi, Pakistani, Japanese, Korean, English, and Indonesian populations14. Particularly in Malaysia, the codon 41/42 (-TTCT) variation is commonly found in Malaysian Chinese and Malays but has never been reported in Malaysian Indians12. We noted that the patient’s mother was originally from Uttar Pradesh, India, which has a high prevalence of beta-thalassemia with codon 41/42 (-TTCT) being one of the most common beta-thalassemia alleles15. Hence, based on the family history of the index patient, we postulate that codon 41/42 (-TTCT) and Hb Vancleave could have been inherited from the maternal and paternal sides, respectively. In addition, although both the Hb Vancleave and codon 41/42 (-TTCT) alleles were functionally altered, the Hb value was still high, likely due to physiological compensation from smoking and vaping habits.
Differential diagnosis of high oxygen affinity may be laborious and complex due to its plethora of clinical presentations and its unknown prevalence in the population5,16. Particularly in Malaysia, where hemoglobin disorders are highly prevalent, patients with erythrocytosis should be prioritized for hemoglobin anomaly investigations via direct DNA sequencing. This is an important step to ensure that clinical management is successful and that effective investigations can be performed for patients with erythrocytosis5,17. Previous studies have also shown that coinheritance of high-affinity hemoglobin with delta-beta thalassemia or beta-thalassemia leads to marked polycythemia; otherwise, patients are clinically healthy, but the risk of thrombosis increases later in life4. In addition, Percy and colleagues recommended that if the P50 value is not available, HPLC and Sanger sequencing can be used as alternative methods for the differential diagnosis of high-affinity hemoglobin. Erythrocytosis with concomitant iron deficiency can normalize hemoglobin levels and therefore make it difficult to detect high-affinity hemoglobin by performing only routine laboratory tests18. Some of the silent variants may be overlooked in the presumptive diagnosis. Hence, when encountering these atypical cases, molecular DNA analysis is recommended17,19. In summary, this is the first reported case of Hb Vancleave, a rare variant worldwide, in Malaysia. The present study highlights the importance of hemoglobin disorder awareness and the advantage of DNA analysis for patients with erythrocytosis, which can be challenging due to the clinical and genetic heterogeneity of thalassemia syndrome in Malaysia.
Targeted cancer therapies are a group of oral medications directed at tumours harbouring specific driver mutations that occur in a subset of patients with cancer.
Around one-third to one-half of patients with advanced non–small cell lung carcinoma may harbour an actionable mutation, which can be identified from molecular analysis of a biopsy or surgical specimen.
Patients treated with targeted therapy generally have better symptom control, response rates (i.e., shrinking tumours), and overall survival than those treated with conventional chemotherapy.
Targeted therapy is typically well tolerated and does not carry the same risks of emesis, alopecia, immunosuppression, and febrile neutropenia as chemotherapy.
Lung cancer is the leading cause of cancer-related death in Canada, with non–small cell lung carcinoma (NSCLC) making up 85% of cases.1 Lung cancer has been associated with a poor prognosis, particularly for patients with metastatic disease. Since Health Canada’s initial approval of gefitinib in patients with advanced NSCLC in 2003, targeted therapies have emerged as an important treatment option for patients and are now widely used in clinical practice.
What is targeted therapy?
Targeted therapies are a group of personalized anti-cancer medications. While chemotherapy attacks all rapidly dividing cells, targeted therapies select for cancer cells that harbour specific genomic driver alterations. Driver alterations are the principal trigger of growth for cancer cells, and many of these driver alterations now have matched targeted therapies. About 30%–50% of patients with NSCLC harbour a tumour-driver alteration and about 50%–75% of these are targetable.2 The prevalence of specific driver alterations varies by patient age, degree of tobacco exposure, ethnicity, and histology.2
Small-molecule tyrosine kinase inhibitors are the most common type of targeted therapy used in the treatment of NSCLC, and they work by inhibiting tyrosine kinase enzymes. Tyrosine kinase enzymes are membrane-spanning proteins made up of an extracellular (ligand-binding domain) and an intracellular kinase domain. Under normal physiologic conditions, ligand binding of the extracellular domain results in phosphorylation of downstream proteins, leading to their activation in a highly regulated fashion. The presence of an activating oncogenic alteration causes the tyrosine kinase enzyme to become constitutively active (i.e., does not need ligand binding to be in the “on” position), which drives cancer cell growth and proliferation. Targeted therapies treat cancer by inhibiting these overactive tyrosine kinase enzymes. Practically, targeted therapies are oral medications that can be taken at home without the number of hospital attendances associated with intravenous therapies.
Who is eligible for targeted therapy?
To assess whether targeted therapy is a suitable option, patients must undergo molecular profiling of their tumour. Molecular testing can be performed on most biopsy specimens, often on the same sample used to make the initial histopathologic cancer diagnosis. In some instances, especially when the procurement of a biopsy is difficult, analysis of circulating tumour DNA in the patient’s blood can also identify tumour-related gene alterations. Modern next-generation sequencing techniques can test for multiple alterations in parallel. Next-generation sequencing capacity has rapidly improved in Canada in recent years, although the turnaround time for molecular testing varies, with the ideal scenario being 1–2 weeks from biopsy to result. Figure 1 depicts the workflow in assessing candidacy for targeted therapy.
A schematic depicting the workflow of assessing patients for and prescribing targeted therapy. (A) The patient undergoes a biopsy for histopathologic diagnosis of non–small cell lung carcinoma. (B) Tumour tissue is sent for molecular analysis. If a driver mutation is detected, the patient may be a candidate for a targeted agent. (C) The patient reviews the results with their oncologist and consents to targeted therapy. (D) The prescription can be filled at an outpatient pharmacy, and targeted therapy can be taken at home.
Molecular testing is performed reflexively (i.e., ordered by the pathologist) for newly diagnosed non-squamous lung cancers at most institutions, while others require a requisition from the oncologist. Many Canadian cancer centres offer in-house molecular testing, but others will send tissue samples externally for molecular analysis. All standard-of-care molecular testing can be performed in Canada.
What is the evidence of benefit?
Metastatic NSCLC is associated with poor clinical outcomes. Efficacy of cancer treatments is generally measured by response rates (proportion of patients with substantial tumour shrinkage), quality of life, and overall survival. Before the introduction of targeted therapy in the management of metastatic lung cancer, patients treated with chemotherapy had a median survival of less than 9 months, with response rates in the range of 25%–35%; only 10% of patients survived to the 2-year mark.3
Targeted therapy has improved outcomes tremendously, whereby most patients receiving a targeted drug have major tumour shrinkage, symptom improvement, and longer survival. 4 In the context of metastatic cancer, targeted therapies are given with palliative intent, with the goal improving quality of life and overall survival rather than to cure cancer. However, 2 targeted therapies, alectinib and osimertinib, have been shown to significantly decrease rates of recurrence when given as adjuvant treatment after surgery among patients with non-metastatic disease.5,6
Ten different alterations have been identified, treated with 20 effective targeted therapies (Table 1).7 Mutations in the epidermal growth factor receptor (EGFR) gene were initially discovered in 2004, and are the most common mutations identified in NSCLC. Among patients harbouring a classic EGFR mutation, osimertinib, an EGFR kinase inhibitor, approved by Health Canada for the treatment of non-metastatic NSCLC in 2021, has proven to be the optimal agent, with a median overall survival of 38.6 months, compared with 31.8 months for people receiving older generations of EGFR kinase inhibitors.8 Patients with metastatic NSCLC involving anaplastic lymphoma kinase (ALK) translocations have a 5-year survival rate of more than 60% when treated with alectinib, compared with 45.5% among those treated with crizotinib, the first ALK inhibitor approved.9 For patients with RET translocations treated with selpercatinib, 84% of patients had a major tumour shrinkage, with the response being durable for close to 2 years, although no comparator arm was used in this single-arm, phase 2 study.10Figure 2 shows the radiographic response of a patient harbouring a RET mutation treated with selpercatinib. Targeted agents directed at KRAS, BRAF, MET, NTRK, ROS1, and HER2 have also shown meaningful clinical benefit, although in some cases, the data are too recent to report 5-year survival rates.2,4 Patients can receive targeted therapy at home with remarkable response rates and the ability to maintain quality of life and symptom control, in addition to better odds at long-term survival.11–13
List of Health Canada–approved targeted agents by the genes harbouring the sensitizing alteration7
Figure 2:
Axial computed tomography (CT) chest scans of a female patient in her late 80s, diagnosed with metastatic lung adenocarcinoma harbouring a RET rearrangement (ERC1 exon 17 to RET exon 12) treated with selpercatinib (A) at the time of diagnosis and (B) 9 months after starting therapy, showing radiographic response below the aortic arch.
The efficacy of targeted therapies is heterogeneous and varies depending on the specific drug and target protein. This results in variable magnitudes of benefit with regard to response rate, progression-free survival, and overall survival. Given the rarity of certain actionable mutations, many targeted agents have been studied only in single-arm, phase 2 clinical trials.
What are the harms?
Targeted therapies have more favourable adverse effect profiles than chemotherapy. Adverse effects are specific to the agent used and the protein being inhibited. They are usually mild and can typically be managed supportively. Table 2 provides an overview of adverse effects related to targeted therapy. If symptoms persist or affect a patient’s quality of life or functionality, dose reductions are usually considered as the next step in management. Severe or life-threatening adverse effects are uncommon; thus, the risk–benefit balance for targeted therapies almost always favours treatment, unlike traditional cytotoxic chemotherapy. Unlike chemotherapy, targeted therapies do not cause notable immunosuppression and most patients presenting with fever can be managed as per routine clinical practice. Most targeted agents require regular blood work to monitor blood counts and electrolytes, as well as kidney and liver function. Some agents may require cardiac testing (e.g., electrocardiography, echocardiography). This monitoring is typically organized by the patient’s oncologist
Adverse effects related to targeted therapy classes, grouped by their target gene*
What are the resource implications and how is targeted therapy accessed?
Targeted therapies are usually more costly than chemotherapy and sometimes more than immunotherapy. Using estimates from wholesale prices in the United States, the average cost of targeted therapy is US$5000–US$10 000 monthly. Treatments are usually continuous until signs of cancer progression in the metastatic setting. 14,15 However, costs vary considerably between agents, and are much lower in Canada than the list price as the prices paid by provinces are heavily discounted based on negotiation by the pan-Canadian Pharmaceutical Alliance, although these negotiated prices are not publicly available. In general, the costs of targeted therapies are likely to decrease as more agents expire from patent and become available as generic medications.
Interprovincial differences to access these drugs exist, leading to disparities across Canada. For instance, oral cancer drugs are funded the same way as intravenous drugs in some provinces (e.g., British Columbia), but through different pathways in other provinces (e.g., Ontario). Accessing therapies when they are not provincially funded is challenging. Options include public or private insurance, private pay, and compassionate access or co-pay programs through pharmaceutical companies.
What can be expected in the future?
Targeted therapy is the standard of care for patients with metastatic NSCLC driven by alterations in select oncogenes. In the future, these agents are likely to be used in earlier stages of disease with the aim of improving cure rates. Further expansion of targeted therapies will be observed as molecular testing becomes part of routine practice, as more patients with targetable mutations will be identified. More targetable alterations are being discovered. From the first mutation (EGFR) in 2004, to the second (ALK fusion) in 2009, 10 alterations have been identified, with other candidates in discovery. In addition, as mechanisms of resistance to targeted therapies are better understood, new agents are being developed that target resistant cancer cell clones.
Burton line and basophilic stippling in lead poisonin
A 47-year-old man who had been working as a self-employed plumber in Nara Prefecture, Japan, for about 30 years presented to the emergency department with a 2-week history of abdominal pain and anorexia. Blood tests showed microcytic anemia: the blood smear showed erythrocytes with basophilic stippling (Figure 1A). These small, punctate inclusions, derived from ribosomes or ribosomal RNA fragments, are classically associated with lead poisoning, but can also be observed in blood disorders such as thalassemia, sickle cell disease, and megaloblastic anemia.1 Physical examination showed a gum discoloration known as Burton line (Figure 1B). This bluish line along the gingival margin indicates chronic lead poisoning. It occurs when lead reacts with bacteria in dental plaque to form and deposit lead sulfide. It is found in about half of those with chronic lead poisoning with exposures of longer than 1 year.2 The patient’s blood lead level was markedly elevated at 108 μg/dL (5.2 μmol/L), and we diagnosed lead poisoning, with exposure attributed to work on old lead water pipes. We administered chelation therapy with calcium disodium ethylenediaminetetraacetic acid, resulting in symptom improvement within a few weeks. Regular monitoring of the patient’s blood lead level showed gradual improvement.
(A) Peripheral blood smear showing erythrocytes with basophilic stippling (arrows) in a 47-year-old male plumber with lead poisoning. (B) Burton line (arrows) in some of the patient’s gum lines.
Although lead poisoning is uncommon in high-income countries, owing to regulations limiting lead exposure, lead is still used in a variety of occupational and recreational applications. The symptoms of lead poisoning are nonspecific and include abdominal pain, constipation, anorexia, headache, fatigue, and neurologic features (e.g., irritability, drowsiness, convulsions, and coma), sometimes making diagnosis difficult. The threshold for the manifestation of symptoms related to blood lead level varies among individuals. Chelation therapy is indicated for asymptomatic patients with levels greater than 70 μg/dL (> 3.4 μmol/L) and for symptomatic patients with levels of 45–70 μg/dL (2.2–3.4 μmol/L).3 Burton lines and basophilic stippling are important clinical clues suggesting this uncommon diagnosis.
Summary: Researchers developed innovative, flexible devices that can gently wrap around nerve fibers, potentially transforming the diagnosis and treatment of neurological disorders. These tiny, flexible “nerve cuffs” employ soft robotics and flexible electronics to interface with peripheral nerves without causing damage.
Tested successfully in rats, these cuffs adjust their shape with minimal voltage, eliminating the need for surgical sutures or glues. This breakthrough could lead to less invasive treatments for conditions like epilepsy, chronic pain, and could improve the control of prosthetic limbs.
Author:
Source: University of Cambridge
Researchers have developed tiny, flexible devices that can wrap around individual nerve fibers without damaging them.
The researchers, from the University of Cambridge, combined flexible electronics and soft robotics techniques to develop the devices, which could be used for the diagnosis and treatment of a range of disorders, including epilepsy and chronic pain, or the control of prosthetic limbs.
Current tools for interfacing with the peripheral nerves—the 43 pairs of motor and sensory nerves that connect the brain and the spinal cord—are outdated, bulky and carry a high risk of nerve injury. However, the robotic nerve “cuffs” developed by the Cambridge team are sensitive enough to grasp or wrap around delicate nerve fibers without causing any damage.
For example, they might help relieve pain by blocking pain signals, or they could be used to restore movement in paralyzed limbs by sending electrical signals to the nerves.
Tests of the nerve cuffs in rats showed that the devices only require tiny voltages to change shape in a controlled way, forming a self-closing loop around nerves without the need for surgical sutures or glues.
The researchers say the combination of soft electrical actuators with neurotechnology could be an answer to minimally invasive monitoring and treatment for a range of neurological conditions.
The results are reported in the journal Nature Materials.
Electric nerve implants can be used to either stimulate or block signals in target nerves. For example, they might help relieve pain by blocking pain signals, or they could be used to restore movement in paralyzed limbs by sending electrical signals to the nerves.
Nerve monitoring is also standard surgical procedure when operating in areas of the body containing a high concentration of nerve fibers, such as anywhere near the spinal cord.
These implants allow direct access to nerve fibers, but they come with certain risks. “Nerve implants come with a high risk of nerve injury,” said Professor George Malliaras from Cambridge’s Department of Engineering, who led the research.
“Nerves are small and highly delicate, so anytime you put something large, like an electrode, in contact with them, it represents a danger to the nerves.”
“Nerve cuffs that wrap around nerves are the least invasive implants currently available, but despite this they are still too bulky, stiff and difficult to implant, requiring significant handling and potential trauma to the nerve,” said co-author Dr. Damiano Barone from Cambridge’s Department of Clinical Neurosciences
The researchers designed a new type of nerve cuff made from conducting polymers, normally used in soft robotics. The ultra-thin cuffs are engineered in two separate layers. Applying tiny amounts of electricity—just a few hundred millivolts—causes the devices to swell or shrink.
The cuffs are small enough that they could be rolled up into a needle and injected near the target nerve. When activated electrically, the cuffs will change their shape to wrap around the nerve, allowing nerve activity to be monitored or altered.
“To ensure the safe use of these devices inside the body, we have managed to reduce the voltage required for actuation to very low values,” said Dr. Chaoqun Dong, the paper’s first author.
“What’s even more significant is that these cuffs can change shape in both directions and be reprogrammed. This means surgeons can adjust how tightly the device fits around a nerve until they get the best results for recording and stimulating the nerve.”
Tests in rats showed that the cuffs could be successfully placed without surgery, and they formed a self-closing loop around the target nerve. The researchers are planning further testing of the devices in animal models, and are hoping to begin testing in humans within the next few years.
“Using this approach, we can reach nerves that are difficult to reach through open surgery, such as the nerves that control, pain, vision or hearing, but without the need to implant anything inside the brain,” said Barone. “The ability to place these cuffs so they wrap around the nerves makes this a much easier procedure for surgeons, and it’s less risky for patients.
“The ability to make an implant that can change shape through electrical activation opens up a range of future possibilities for highly targeted treatments,” said Malliaras.
“In future, we might be able to have implants that can move through the body, or even into the brain—it makes you dream how we could use technology to benefit patients in future.”



{kind=link}
{kind=link}