Summary: New research highlights the critical role of unique gut bacteria in newborns, producing serotonin to educate immune cells and prevent allergic reactions early in life.
The study reveals that these bacteria encourage the development of T-regulatory cells, crucial for suppressing inappropriate immune responses and preventing autoimmune diseases. This work suggests that before the neonatal gut matures to produce its own neurotransmitters, specific bacteria supply essential serotonin, promoting a balanced immune system.
Such findings underscore the importance of early exposure to beneficial bacteria for preventing allergies and potentially autoimmune diseases later in life.
Key Facts:
Serotonin-Producing Gut Bacteria: Newly born infants’ guts harbor special bacteria that produce serotonin, crucial for developing a healthy immune system by fostering T-regulatory cells.
Prevention of Allergies: This mechanism helps in preventing dangerous allergic reactions to food and beneficial microbes by maintaining a high level of serotonin, which keeps the immune response in check.
Critical Early Development Role: The research emphasizes the significance of the right microbial exposure after birth, suggesting a potential link between reduced diversity in gut bacteria due to modern lifestyles and the rise in food allergies among children in developed countries.
Source: Weill Cornell University
Weill Cornell Medicine investigators discovered that unique bacteria colonize the gut shortly after birth and make the neurotransmitter serotonin to educate gut immune cells. This prevents allergic reactions to food and the bacteria themselves during early development.
The preclinical study, published in Science Immunology on Mar. 15, showed that bacteria abundant in the guts of newborns produce serotonin, which promotes the development of immune cells called T-regulatory cells or Tregs.
These cells suppress inappropriate immune responses to help prevent autoimmune diseases and dangerous allergic reactions to harmless food items or beneficial gut microbes.
The researchers observed that the neonatal mouse gut had much higher levels of neurotransmitters, including serotonin, than the adult gut.
“The gut is now known as the second human brain as it makes over 90 percent of the neurotransmitters in the human body. While neurotransmitters such as serotonin are best known for their roles in brain health, receptors for neurotransmitters are located throughout the human body,” explained the study’s senior author, Dr. Melody Zeng, an assistant professor of immunology in the Gale and Ira Drukier Institute for Children’s Research and the Department of Pediatrics at Weill Cornell Medicine.
Gut Bacteria in Babies Provide a Helping Hand
The researchers observed that the neonatal mouse gut had much higher levels of neurotransmitters, including serotonin, than the adult gut.
“So far, almost all studies of gut neurotransmitters were conducted in adult animals or human subjects, where a specific gut cell type called enterochromaffin cells produce neurotransmitters,” said Dr. Zeng.
“However, we discovered that this isn’t the case in the newborn gut where most of the serotonin is made by bacteria that are more abundant in the neonatal gut.”
This was also confirmed in babies through a human infant stool biobank that the Zeng lab has established in collaboration with the Neonatal Intensive Care Unit in the NewYork-Presbyterian Alexandra Cohen Hospital for Women and Newborns. These samples were obtained with parental consent and deidentified.
The study results suggest that before the neonatal gut is mature enough to make its own neurotransmitters, unique gut bacteria may supply neurotransmitters that are needed for critical biological functions during early development.
“We found that gut bacteria in young mice not only directly produce serotonin but also decrease an enzyme called monoamine oxidase that normally breaks down serotonin, thus keeping gut serotonin levels high,” said the study’s lead author Dr. Katherine Sanidad, postdoctoral associate in pediatrics at Weill Cornell Medicine.
The high serotonin levels shift the balance of immune cells by increasing the number of Tregs, which helps prevent the immune system from overreacting and attacking gut bacteria or food antigens. “The neonatal gut needs these serotonin-producing bacteria to keep the immune system in check,” Dr. Sanidad added.
Healthy Immune System Helps Later in Life
Dr. Zeng noted that this work underscores the importance of having the right types of beneficial bacteria soon after birth. Babies in developed countries have better access to antibiotics, less exposure to diverse microbes in their clean environments and potentially unhealthy diets that may significantly impact the abundance of serotonin-producing bacteria in their intestines.
As a result, these babies may have fewer Tregs and develop immune reactions to their own gut bacteria, or allergies to food. This may be one reason food allergies have become increasingly common in children, particularly in developed countries.
“If educated properly, the immune system in babies would recognize that things like peanuts and eggs are okay, and it doesn’t have to attack them,” she said. This may also have an impact on developing autoimmune diseases—when the immune system attacks the body’s own healthy cells—later in life.
The team next plans to look at bacteria in human infant stool samples to measure their production of serotonin, other neurotransmitters and molecules that may help train the immune system to prevent future immune-related diseases, such as allergies, infections and cancer.
“It’s essential to understand how the immune system is trained during early life, but this is understudied in newborns and children. Further studies of these developmental periods may hopefully lead us to mitigation approaches to reduce the risk of inflammatory diseases like food allergies and inflammatory bowel disease later in life,” Dr. Sanidad said.
Funding: Dr. Melody Zeng’s lab is supported in part by the National Institutes of Health grants R01HD110118, R01HL169989, R21CA270998, and K01DK114376; The Starr Cancer Consortium; the Hartwell Foundation; and the Jill Roberts Center for Inflammatory Bowel Disease, the Children’s Health Council, and the Drukier Institute for Children’s Health at Weill Cornell Medicine.
Abstract
Gut bacteria-derived serotonin promotes immune tolerance in early life
The gut microbiota promotes immune system development in early life, but the interactions between the gut metabolome and immune cells in the neonatal gut remain largely undefined.
Here, we demonstrate that the neonatal gut is uniquely enriched with neurotransmitters, including serotonin, and that specific gut bacteria directly produce serotonin while down-regulating monoamine oxidase A to limit serotonin breakdown.
We found that serotonin directly signals to T cells to increase intracellular indole-3-acetaldehdye and inhibit mTOR activation, thereby promoting the differentiation of regulatory T cells, both ex vivo and in vivo in the neonatal intestine.
Oral gavage of serotonin into neonatal mice resulted in long-term T cell–mediated antigen-specific immune tolerance toward both dietary antigens and commensal bacteria.
Together, our study has uncovered an important role for specific gut bacteria to increase serotonin availability in the neonatal gut and identified a function of gut serotonin in shaping T cell response to dietary antigens and commensal bacteria to promote immune tolerance in early life.
Serotonin deficiency occurs when serotonin doesn’t act as well as it should in your body. This can happen if your body doesn’t produce enough serotonin or if it doesn’t use serotonin efficiently.
Serotonin, also called 5-hydroxytryptamine (5-HT), is best known for the part it plays in mood and behavior.
But did you know that it also affects your sleep, appetite, digestion, and more? Low levels of serotonin can have wide-ranging effects on your mental and physical health.
Scientists don’t yet understand exactly how serotonin works, what it does, and what causes low levels in the body. They’re also not certain exactly what the right levels are and how these might vary for different people.
Read on to learn what serotonin deficiency is and how it can affect your body.
Serotonin deficiency is a complex condition for which there are no diagnostic criteria and no clear tests. It’s generally discussed in terms of the symptoms that result, rather than the exact levels that might bring it on.
Serotonin deficiency has been linked to many physical and psychological symptoms. However, its exact role in any of them isn’t fully understood. Much research continues within the medical and scientific communities.
For example, researchers continue to debate the linkTrusted Source between serotonin and depression. The connection between sleep and serotonin is also controversialTrusted Source. About the only thing researchers agree on is that serotonin’s function in the human body is complex and far-reaching.
Research has found that the overwhelming amount of serotonin in your body — 95 percent — is produced in the lining of your gastrointestinal (GI) tract. The remaining 5 percent is produced in your brain. There it acts as a neurotransmitter that carries signals between brain nerve cells (neurons).
Some researchTrusted Source about serotonin has to do with its role in what is called the gut-brain axisTrusted Source. This is a communication line between the central nervous system and the enteric, or intestinal, nervous system. This effectively links the brain and the gut, giving rise to the name: gut-brain axis.
Research has shown that some of the serotonin produced in your gastrointestinal (GI) tract moves through your body in circulating platelets, or tiny blood cells, to help regulate important body processes such as:
immune response
bone development
digestion
cardiac function
Study of serotonin’s role in this gut-brain axis is relatively new, and ideas are changing rapidly. Much further research is needed.
Below, we’ll discuss the symptoms of serotonin deficiency and what may cause it. We’ll also outline ways to increase your serotonin levels.
Serotonin deficiency affects people differently. For example, researchTrusted Source shows that people who haven’t experienced depression previously may not become significantly depressed with lower levels of serotonin, whereas those with a history of depression may.
Physical symptoms
Research has begun to show serotonin’s activity in increasing numbers of bodily processes, including:
metabolism
sleep
blood clotting
energy balance
digestion
body sugar balance
cardiac function
liver function
immune system response
pain production
Given serotonin’s wide scope of bodily functioning, it comes as no surprise that serotonin deficiency has been associated with many physical conditions, including:
Scientists are unsure what causes serotonin deficiency. Some research shows early life stressors might negatively affect the transport of serotonin in the body.
Other researchTrusted Source shows that microbes in the gut help produce serotonin. This production might be disrupted when the microbiome, or gut bacteria as a whole, is disturbed because of stress, disease, diet, or other causes.
Both of these studies were done with animals, and researchers emphasized that further clinical research is needed.
Other potential causes of serotonin deficiency include:
chronic stress
nutritional deficiencies
digestion issues
certain drugs
hormone changes
lack of sunlight
Lower levels of serotonin are also thought to be related to a person’s particular biology, which may include:
fewer or less effective serotonin receptors
a body that breaks down serotonin or absorbs it too soon
Medical professionals generally don’t diagnose serotonin deficiency and choose instead to treat the symptoms.
This is because serotonin deficiency is a complex condition whose cause is very difficult to nail down. There are no diagnostic criteria, and it’s often unclear whether the symptoms cause the deficiency or the deficiency causes the symptoms.
There’s a test that measures the amount of serotonin in your blood, but medical professionals typically use this test only to check for tumors that produce serotonin outside of the brain. Your blood level of serotonin doesn’t accurately reflect the amount in your brain.
Serotonin generally can’t pass through the blood-brain barrier (BBB). This is a semi-permeable barrier surrounds your brain that lets some substances pass through, but not others.
This means that serotonin in your brain must be produced in your brain. For this reason, your body’s overall blood levels of serotonin are unreliable measurements of the amount of serotonin in your brain.
Urine tests are equally unreliable measures of your brain serotonin. They measure the amount of serotonin that your body is producing and how much is in your body, but they don’t measure the amount in your brain.
Your doctor may prescribe a urine test in combination with blood tests to test for serotonin-producing tumors, but not for serotonin deficiency.
If you think you have symptoms of a serotonin deficiency, it’s best to work with a medical professional to narrow down potential causes and develop a treatment plan. Read on to learn about potential treatments.
SSRIs help your body use serotonin more efficiently. They don’t create more serotonin.
Only a portion of the serotonin that your brain releases is used by your body. Some of the serotonin goes back into the cell that it came from. SSRIs block some of this reabsorption (reuptake) of serotonin, leaving more available for the body to use.
SSRIs can take weeks to have an effect, and sometimes they may not work at all. Also, they can also cause a range of side effects that you may not tolerate well.
When SSRIs do work, they work very well and are a good option. Sometimes, if one SSRI doesn’t work, another one will.
If SSRIs aren’t the best treatment for you, you might ask your doctor about one of the following options.
Mood induction
Mood induction is an experimental treatment in which you create a positive mood by doing something you like or thinking about something that lifts your mood. Music, film clips, and imagery are common methods.
Regular exercise is useful, but aerobic exercise is the most effective type of exercise for boosting serotonin levels. Aerobic exercises include:
walking
running
swimming
Diet
ResearchTrusted Source suggests a diet high in tryptophan may help increase serotonin levels in the body. Tryptophan is an essential amino acid in the body that is needed for the production of serotonin.
Significant amounts of tryptophan will probably not be absorbed into the brain from foods. Regularly consuming a variety of foods containing tryptophan may combine to make a difference, especially when combined with healthy carbs like whole grains or oatmeal.
Try these seven foods to start adding tryptophan to your diet.
Other substances that are thought to promote serotonin production in the body include:
Serotonin deficiency can have far-reaching effects on both your mental and physical health. After more than 70 years of research, scientists and researchers still don’t entirely understand how serotonin is produced and used in the body.
If you have symptoms that make you think you might have a serotonin deficiency, talk with a doctor. Together, you can decide the best treatment options for you.
You might also try natural remedies, such as adding more sunlight, certain foods, and aerobic exercise to your lifestyle. These are best used as add-ons to medical treatment, not substitutions.
Serotonin deficiency is a complex condition, and a medical professional is the best person to guide you through it.
A study at the Icahn School of Medicine has uncovered that asenapine, an antipsychotic medication, may work through the TAAR1 receptor, revealing crucial differences between human and rodent TAAR1. This discovery suggests new avenues for treating substance use and neuropsychiatric disorders and rethinking drug development strategies. Credit: SciTechDaily.com
Study sheds light on TAAR1, pointing to potential enhancement opportunities in drug development.
Researchers at the Icahn School of Medicine at Mount Sinai have uncovered insights into the potential mechanism of action of the antipsychotic medication asenapine, a possible therapeutic target for substance use and neuropsychiatric disorders. This discovery may pave the way for the development of improved medications targeting the same pathway.
Their findings, detailed in the January 2 online issue of Nature Communications, show that a brain protein known as the TAAR1 receptor, a drug target known to regulate dopamine signaling in key reward pathways in the brain, differs significantly in humans compared to the preclinical rodent models on which drugs are typically tested.
The study suggests considering species-specific differences in drug-receptor interactions and further investigation into ways asenapine affects the body, as steps toward potential therapeutic improvements.
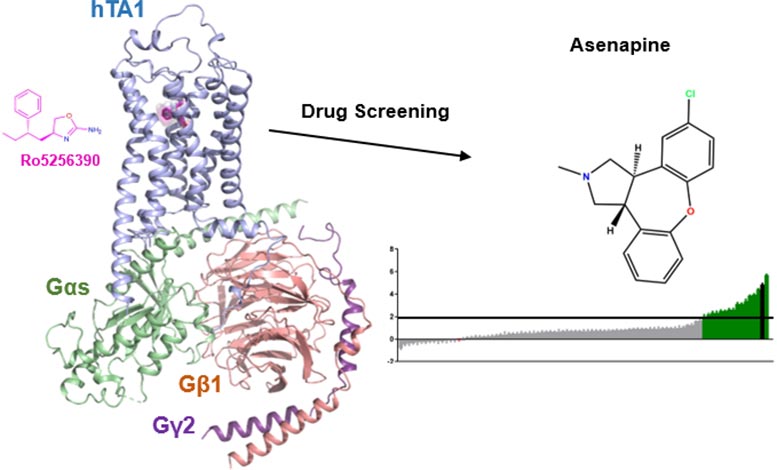
Mount Sinai Icahn scientists took detailed pictures of how drugs can bind to the TAAR1 receptor using CryoEM. They also discovered that an antipsychotic drug, asenapine, unexpectedly activates TAAR1, which could potentially contribute to asenapine’s therapeutic effects. Credit: Wacker et al., Nature Communications
“In investigating the functional and structural properties of TAAR1, our study aimed to shed more light on its mechanisms and pharmacology,” says study first author Gregory Zilberg, a PhD candidate at Icahn Mount Sinai. “Our findings may guide the development of novel TAAR1 drugs and prompt more exploration of medications similar to asenapine.”
Using advanced techniques to investigate TAAR1’s structure and function, the researchers identified three important elements. First, there are differences between rodent and human TAAR1 that likely affect how preclinical model studies can be translated to humans. Second, TAAR1 is much more closely related to serotonin and dopamine receptors than previously assumed. This suggests that several serotonin-targeting medications might have unknown therapeutic efficacy or side effects that are in fact due to their actions at TAAR1.
Finally, the investigators highlight that the clinically used antipsychotic asenapine unexpectedly shows strong activation of TAAR1, suggesting in fact that this serotonin- and dopamine-targeting antipsychotic could derive some of its therapeutic effects from TAAR1 activation. If proven in further studies, this could open up new possibilities for its potential in other TAAR1-related therapeutic applications such as its use in substance use disorders, as well as the development of new asenapine-based drugs.
The researchers noted the absence of information about differences in how TAAR1 works in rodents and humans, and emphasized that some of these differences could account for why preclinical data on TAAR1 has not yet been successfully translated into effective therapies in humans. Next, the researchers plan to study where TAAR1 is located within cells and what its precise role is in influencing serotonin and dopamine signaling.
“This study provides a significant leap in understanding TAAR1, offering potential avenues for drug development and encouraging further research into its therapeutic applications,” says senior author Daniel Wacker, PhD, Assistant Professor of Pharmacological Sciences, and Neuroscience, at Icahn Mount Sinai. “As our work advances, we anticipate it may play a crucial role in shaping the development of new drugs targeting TAAR1 and offering valuable insights into how drugs similar to asenapine might work.”
Millions believe depression is caused by ‘serotonin deficiency,’ but where is the science in support of this theory?
“Depression is a serious medical condition that may be due to a chemical imbalance, and Zoloft works to correct this imbalance.”
Herein lies the serotonin myth.
As one of only two countries in the world that permits direct to consumer advertising, you have undoubtedly been subjected to promotion of the “cause of depression.” A cause that is not your fault, but rather; a matter of too few little bubbles passing between the hubs in your brain! Don’t add that to your list of worries, though, because there is a convenient solution awaiting you at your doctor’s office…
What if I told you that, in 6 decades of research, the serotonin (or norepinephrine, or dopamine) theory of depression and anxiety has not achieved scientific credibility?
You’d want some supporting arguments for this shocking claim.
So, here you go:
The Science of Psychiatry is Myth
Rather than some embarrassingly reductionist, one-deficiency-one-illness-one-pill model of mental illness, contemporary exploration of human behavior has demonstrated that we may know less than we ever thought we did. And that what we do know about root causes of mental illness seems to have more to do with the concept of evolutionary mismatch than with genes and chemical deficiencies.
In fact, a meta-analysis of over 14,000 patients and Dr. Insel, head of the NIMH, had this to say:
“Despite high expectations, neither genomics nor imaging has yet impacted the diagnosis or treatment of the 45 million Americans with serious or moderate mental illness each year.”
To understand what imbalance is, we must know what balance looks like, and neuroscience, to date, has not characterized the optimal brain state, nor how to even assess for it.
A New England Journal of Medicinereview on Major Depression, stated:
” … numerous studies of norepinephrine and serotonin metabolites in plasma, urine, and cerebrospinal fluid as well as postmortem studies of the brains of patients with depression, have yet to identify the purported deficiency reliably.”
The data has poked holes in the theory and even the field of psychiatry itself is putting down its sword. One of my favorite essays by Lacasse and Leo has compiled sentiments from influential thinkers in the field – mind you, these are conventional clinicians and researchers in mainstream practice – who have broken rank, casting doubt on the entirety of what psychiatry has to offer around antidepressants:
Humble Origins of a Powerful Meme
In the 1950s, reserpine, initially introduced to the US market as an anti-seizure medication, was noted to deplete brain serotonin stores in subjects, with resultant lethargy and sedation. These observations colluded with the clinical note that an anti-tuberculosis medication, iproniazid, invoked mood changes after five months of treatment in 70% of a 17 patient cohort. Finally, Dr. Joseph Schildkraut threw fairy dust on these mumbles and grumbles in 1965 with his hypothetical manifesto entitled “The Catecholamine Hypothesis of Affective Disorders” stating:
“At best, drug-induced affective disturbances can only be considered models of the natural disorders, while it remains to be demonstrated that the behavioral changes produced by these drugs have any relation to naturally occurring biochemical abnormalities which might be associated with the illness.”
Contextualized by the ripeness of a field struggling to establish biomedical legitimacy (beyond the therapeutic lobotomy!), psychiatry was ready for a rebranding, and the pharmaceutical industry was all too happy to partner in the effort.
Of course, the risk inherent in “working backwards” in this way (noting effects and presuming mechanisms) is that we tell ourselves that we have learned something about the body, when in fact, all we have learned is that patented synthesized chemicals have effects on our behavior. This is referred to as the drug-based model by Dr. Joanna Moncrieff. In this model, we acknowledge that antidepressants have effects, but that these effects in no way are curative or reparative.
The most applicable analogy is that of the woman with social phobia who finds that drinking two cocktails eases her symptoms. One could imagine how, in a 6 week randomized trial, this “treatment” could be found efficacious and recommended for daily use and even prevention of symptoms. How her withdrawal symptoms after 10 years of daily compliance could lead those around her to believe that she “needed” the alcohol to correct an imbalance. This analogy is all too close to the truth.
Running With Broken Legs
Psychiatrist Dr. Daniel Carlat has said:
“And where there is a scientific vacuum, drug companies are happy to insert a marketing message and call it science. As a result, psychiatry has become a proving ground for outrageous manipulations of science in the service of profit.”
So, what happens when we let drug companies tell doctors what science is? We have an industry and a profession working together to maintain a house of cards theory in the face of contradictory evidence.
We have aglobal situation in which increases in prescribing are resulting in increases in severity of illness (including numbers and length of episodes) relative to those who have never been treated with medication.
To truly appreciate the breadth of evidence that states antidepressants are ineffective and unsafe, we have to get behind the walls that the pharmaceutical companies erect. We have to unearth unpublished data, data that they were hoping to keep in the dusty catacombs.
A now famous 2008 study in the New England Journal of Medicine by Turner et al sought to expose the extent of this data manipulation. They demonstrated that, from 1987 to 2004, 12 antidepressants were approved based on 74 studies. Thirty-eight were positive, and 37 of these were published. Thirty-six were negative (showing no benefit), and 3 of these were published as such while 11 were published with a positive spin (always read the data not the author’s conclusion!), and 22 were unpublished.
In 1998 tour de force, Dr. Irving Kirsch, an expert on the placebo effect, published a meta-analysis of 3,000 patients who were treated with antidepressants, psychotherapy, placebo, or no treatment and found that only 27% of the therapeutic response was attributable to the drug’s action.
This was followed up by a 2008 review, which invoked the Freedom of Information Act to obtain access to unpublished studies, finding that, when these were included, antidepressants outperformed placebo in only 20 of 46 trials (less than half!), and that the overall difference between drugs and placebos was 1.7 points on the 52 point Hamilton Scale. This small increment is clinically insignificant, and likely accounted for by medication side effects strategically employed (sedation or activation).
When active placebos were used, theCochrane database found that differences between drugs and placebos disappeared, given credence to the assertion that inert placebos inflate perceived drug effects.
The finding of tremendous placebo effect in the treatment groups was also echoed in two different meta-analyses by Khan et al who found a 10% difference between placebo and antidepressant efficacy, and comparable suicide rates. A trial examining the role of “expectancy” or belief in antidepressant effect, found that patients lost their perceived benefit if they believed that they might be getting a sugar pill even if they were continued on their formerly effective treatment dose of Prozac.
The largest, non-industry funded study, costing the public $35 million dollars, followed 4000 patients treated with Celexa (not blinded, so they knew what they were getting), and found that half of them improved at 8 weeks. Those that didn’t were switched to Wellbutrin, Effexor, or Zoloft OR “augmented” with Buspar or Wellbutrin.
Guess what? It didn’t matter what was done, because they remitted at the same unimpressive rate of 18-30% regardless with only 3% of patients in remission at 12 months.
How could it be that medications like Wellbutrin, which purportedly primarily disrupt dopamine signaling, and medications like Stablon which theoretically enhances the reuptake of serotonin, both work to resolve this underlying imbalance? Why would thyroid, benzodiazepines, beta blockers, and opiates also “work”? And what does depression have in common with panic disorder, phobias, OCD, eating disorders, and social anxiety that all of these diagnoses would warrant the same exact chemical fix?
Alternative options
As a holistic clinician, one of my bigger pet peeves is the use of amino acids and other nutraceuticals with “serotonin-boosting” claims. These integrative practitioners have taken a page from the allopathic playbook and are seeking to copy-cat what they perceive antidepressants to be doing.
The foundational “data” for the modern serotonin theory of mood utilizes tryptophan depletion methods which involve feeding volunteers amino acid mixtures without tryptophan and are rife with complicated interpretations.
Simply put, there has never been a study that demonstrates that this intervention causes mood changes in any patients who have not been treated with antidepressants.
In an important paper entitled Mechanism of acute tryptophan depletion: Is it only serotonin?, van Donkelaar et al caution clinicians and researchers about the interpretation of tryptophan research. They clarify that there are many potential effects of this methodology, stating:
“In general, several findings support the fact that depression may not be caused solely by an abnormality of 5-HT function, but more likely by a dysfunction of other systems or brain regions modulated by 5-HT or interacting with its dietary precursor. Similarly, the ATD method does not seem to challenge the 5-HT system per se, but rather triggers 5HT-mediated adverse events.”
So if we cannot confirm the role of serotonin in mood and we have good reason to believe that antidepressant effect is largely based on belief, then why are we trying to “boost serotonin”?
Causing imbalances
All you have to do is spend a few minutes on https://survivingantidepressants.org/ or https://beyondmeds.com/ to appreciate that we have created a monster. Millions of men, women, and children the world over are suffering, without clinical guidance (because this is NOT a part of medical training) to discontinue psychiatric meds. I have been humbled, as a clinician who seeks to help these patients, by what these medications are capable of. Psychotropic withdrawal can make alcohol and heroin detox look like a breeze.
An important analysis by the former director of the NIMH makes claims that antidepressants “create perturbations in neurotransmitter functions” causing the body to compensate through a series of adaptations which occur after “chronic administration” leading to brains that function, after a few weeks, in a way that is “qualitatively as well as quantitatively different from the normal state.”
Changes in beta-adrenergic receptor density, serotonin autoreceptor sensitivity, and serotonin turnover all struggle to compensate for the assault of the medication.
Andrews, et al., calls this “oppositional tolerance,” and demonstrate through a careful meta-analysis of 46 studies demonstrating that patient’s risk of relapse is directly proportionate to how “perturbing” the medication is, and is always higher than placebo (44.6% vs 24.7%). They challenge the notion that findings of decreased relapse on continued medication represent anything other than drug-induced response to discontinuation of a substance to which the body has developed tolerance. They go a step further to add:
“For instance, in naturalistic studies, unmedicated patients have much shorter episodes, and better long-term prospects, than medicated patients. Several of these studies have found that the average duration of an untreated episode of major depression is 12–13 weeks.”
Harvardresearchers also concluded that at least fifty percent of drug-withdrawn patients relapsed within 14 months. In fact:
“Long-term antidepressant use may be depressogenic . . . it is possible that antidepressant agents modify the hardwiring of neuronal synapses (which) not only render antidepressants ineffective but also induce a resident, refractory depressive state.”
So, when your doctor says, “You see, look how sick you are, you shouldn’t have stopped that medication,” you should know that the data suggests that your symptoms are withdrawal, not relapse.
Longitudinalstudies demonstrate poor functional outcomes for those treated with 60% of patients still meeting diagnostic criteria at one year (despite transient improvement within the first 3 months). When baseline severity is controlled for, two prospective studies support a worse outcome in those prescribed medication:
One in which the never-medicated group experienced a 62% improvement by six months, whereas the drug-treated patients experienced only a 33% reduction in symptoms, and another WHO study of depressed patients in 15 cities which found that, at the end of one year, those who weren’t exposed to psychotropic medications enjoyed much better “general health”; that their depressive symptoms were much milder”; and that they were less likely to still be “mentally ill.”
I’m not done yet. In a retrospective 10-year study in the Netherlands, 76% of those with unmedicated depression recovered without relapse relative to 50% of those treated.
Unlike the mess of contradictory studies around short-term effects, there are no comparable studies that show a better outcome in those prescribed antidepressants long term.
First Do No Harm
So, we have a half-baked theory in a vacuum of science that that pharmaceutical industry raced to fill. We have the illusion of short-term efficacy and assumptions about long-term safety. But are these medications actually killing people?
The answer is yes.
Unequivocally, antidepressants cause suicidal and homicidal behavior. The Russian Roulette of patients vulnerable to these “side effects” is only beginning to be elucidated and may have something to do with genetic variants around metabolism of these chemicals. Dr. David Healy has worked tirelessly to expose the data that implicates antidepressants in suicidality and violence, maintaining a database for reporting, writing, and lecturing about cases of medication-induced death that could make your soul wince.
What about our most vulnerable?
I have countless patients in my practice who report new onset of suicidal ideation within weeks of starting an antidepressant. In a population where there are only 2 randomized trials, I have grave concerns about postpartum women who are treated with antidepressants before more benign and effective interventions such as dietary modification and thyroid treatment. Hold your heart as you read through thesereportsof women who took their own and their childrens’ lives while treated with medications.
Then there is the use of these medications in children as young as 2 years old. How did we ever get the idea that this was a safe and effective treatment for this demographic? Look no further than data like Study 329, which cost Glaxo Smith Klein 3 billion dollars for their efforts to promote antidepressants to children. These efforts required ghost-written and manipulated data that suppressed a signal of suicidality, falsely represented Paxil as outperforming placebo, and contributes to an irrepressiblemountainofharmdone to our children by the field of psychiatry.
“Our analysis indicates that there are no specific antidepressant drugs, that most of the short-term effects of antidepressants are shared by many other drugs, and that long-term drug treatment with antidepressants or any other drugs has not been shown to lead to long-term elevation of mood. We suggest that the term “antidepressant” should be abandoned.”
So, where do we turn?
The field of psychoneuroimmunology dominates the research as an iconic example of how medicine must surpass its own simplistic boundaries if we are going to begin to chip away at the some 50% of Americans who will struggle with mood symptoms, 11% of whom will be medicated for it.
There are times in our evolution as a cultural species when we need to unlearn what we think we know. We have to move out of the comfort of certainty and into the freeing light of uncertainty. It is from this space of acknowledged unknowing that we can truly grow. From my vantage point, this growth will encompass a sense of wonder – both a curiosity about what symptoms of mental illness may be telling us about our physiology and spirit, as well as a sense of humbled awe at all that we do not yet have the tools to appreciate. For this reason, honoring our co-evolution with the natural world, and sending the body a signal of safety through movement, diet, meditation, and environmental detoxification represents our most primal and most powerful tool for healing.
Experts have uncovered a biological signature of desire that causes us to lust over certain people more than others. Study authors observed that this imprint fades if there is no contact with the person for a while and that time can indeed heal heartbreak.
“As humans, our entire social world is basically defined by different degrees of selective desire to interact with different people, whether it’s your romantic partner or your close friends,” says Associate Professor Zoe Donaldson from the University of Colorado Boulder, in a media release. “This research suggests that certain people leave a unique chemical imprint on our brain that drives us to maintain these bonds over time.”
The study utilized neuroimaging technology on prairie voles, chosen for their propensity to form monogamous pair bonds, a trait shared by only three to five percent of mammals. In scenarios where a vole attempted to reach its partner in another room, researchers noticed that dopamine levels in the brain spiked, illuminating the sensor.
Researchers say some people create a distinctive chemical mark in our brains that drives us to maintain connections over time. (Credit: Photo by Tim Mossholder On Unsplash)
Researchers describe the reunion as lighting up “like a rave,” with continued activity as the voles snuggled and sniffed each other. However, when faced with a stranger, the sensor dimmed significantly.
“This suggests that not only is dopamine really important for motivating us to seek out our partner, but there’s actually more dopamine coursing through our reward center when we are with our partner than when we are with a stranger,” explains study first author and graduate student Anne Pierce.
Interestingly, after a four-week separation, equivalent to an eternity in the rodent world, the dopamine surge nearly vanished upon reunion.
“We think of this as sort of a reset within the brain that allows the animal to now go on and potentially form a new bond,” Dr. Donaldson concludes.
“The hope is that by understanding what healthy bonds look like within the brain, we can begin to identify new therapies to help the many people with mental illnesses that affect their social world.”
Consuming tree nuts such as macadamia nuts may have cardiovascular benefits.
A new study suggests that tree nuts may reduce certain risk factors for cardiovascular disease by modifying the metabolism of L-tryptophan, an amino acid.
In a controlled parallel trial, people with obesity or overweight who snacked on tree nuts as part of a 24-week weight loss and weight maintenance program experienced increased levels of serotonin, which can enhance mood.
Tree nuts are rich in nutrients, and eating them instead of other snacks was not associated with gaining weight.
The authors of a new study recently established a link between the consumption of tree nuts — almonds, cashews, hazelnuts, macadamia, pecans, pistachios, and walnuts — and a reduction in blood pressure, an important risk factor for cardiovascular disease (CVD). They’ve just published a new study that may explain the connection.
The researchers found that tree nuts increased levels of cardio-protective L-tryptophan metabolites in plasma and stool samples collected from study participants.
The study was a randomized, controlled, parallel study that involved 131 people with obesity or overweight over the course of a 24-week weight loss and weight maintenance program.
The diet of all participants included a daily 1.5-ounce snack. Of the 95 people who completed the study, 39 individuals snacked on pretzels as a control, while 56 other people ate tree-nut snacks of the same caloric value instead. At the end of the study period, the researchers analyzed fecal and blood plasma samples from each participant to ascertain the effects of their different snacks.
People who ate tree nuts experienced significant increases in levels of blood serotonin at week 12 (60.9%), and week 24 (82.2%), compared to their baseline levels. Those who ate pretzels experienced an increase in blood serotonin levels during the maintenance phase of the study, between weeks 12 and 24.
Tryptophan is the body’s only precursor of serotonin, which is credited with supporting a range of body functions, including mood, sleep, and digestion.
The research was funded by the International Tree Nut Council Nutrition Research & Education Foundation, along with the U.S. Department of Defense, VA Merit Review, and VA Career Development Award.
According to the Institute of Food Technologists (IFT), Americans eat 2.7 snacks a day, with an increasing number of young adults consuming as many as five or more.
Children get about 27% of their daily calorie intake from snacks, according to Harvard’s T.H. Chan School of Public Health.
Snacking can lead to unwanted weight gain, and unhealthy snacks often wind up replacing more nutritious foods in one’s daily diet.
Tree nuts contain substantial amounts of tryptophan, which is an essential amino acid that helps support growth and overall health.
Tryptophan is metabolized via three pathways, the kynurenine and serotonin pathways in body cells, and via the indole pathway in gut bacteria.
Disrupted tryptophan metabolism has been linked to metabolic diseases, including obesity and CVD.
The study’s corresponding author, Dr. Zhaoping Li, said the new study at least partially answers the question posed by her group’s earlier research: “One of the possible mechanisms is through [a] change of tryptophan metabolism.”
Dr. Li said in a press release issued by the International Tree Nut Council Nutrition Research & Education Foundation:
“We discovered some new associations between tryptophan metabolites and blood pressure, heart rate, and satiety in overweight/obese subjects, suggesting a broader impact of tryptophan metabolism in overall health, including cardiovascular health.”
“Gut microbiome and their metabolites can contribute to the regulation of our metabolism and mood,” she told Medical News Today.
There are other reasons the study makes sense, said Michelle Routhenstein, cardiology dietitian and preventive cardiology nutritionist at EntirelyNourished:
“[The authors’ interpretation of t]his study’s findings that tree nuts encourage CVD protective tryptophan metabolites and heart health makes sense due to its ability to help reduce inflammation, one of the main causes for atherosclerosis and heart disease.”
Dr. Li explained the connection between eating and emotions.
“Emotional eating is a significant factor [that contributes] to obesity. Nuts may improve mood through an increase of serotonin that is one of the key neurotransmitters to regulate mood,” she said.
The researchers were surprised to find an increase in serotonin levels in the tree nut group during the weight loss and maintenance sections of the study. Only the tree-nut group experienced increased levels of fecal serotonin.
By the end of the study, both groups had higher blood serotonin levels.
The authors speculate this final increase in blood serotonin for all participants may be evidence of the body’s response to weight loss.
“An increase in serotonin levels may be beneficial for people who are overweight or obese trying to achieve weight loss because of its role in energy expenditure and appetite suppression,” Routhenstein also noted.
“One and one-half ounces of tree nuts or peanuts provides [greater than] 10% of the adult male recommended dietary allowance for protein, iron, magnesium, phosphorus, zinc, copper, thiamin, and vitamin E. In addition, 1.5 oz (42 g) of tree nuts provides [greater than] 10% of the adult male RDA for vitamin B-6 and selenium.”
By way of example, Routhenstein listed some significant nutrients associated with a few tree nuts:
Pistachios contain phytosterols, potassium, and carotenoids that promote good blood vessel health and blood lipids.
Brazil nuts contain selenium, which helps combat oxidative stress and boost heart health and immune health.
Pecans are rich in copper, which helps with blood sugar metabolism and may help maintain a healthy thyroid gland.
Almonds are high in antioxidants, fiber, and protein. A single Brazil nut delivers 100% of the recommended daily amount of selenium. Although nuts are rich in energy, concerns about them being linked to weight gain appear unwarranted. Studies have shown that higher nut intake is associated with reductions in body weight and body fat, suggesting they do not contribute to weight gain.
Summary: Taking SSRIs and having the “long-long” serotonin SERT genetic variant lowers SERT activity in the mitral valve, leading to degenerative mitral regurgitation, one of the most common heart valve diseases.
Source: CHOP
The neurotransmitter serotonin can adversely affect the heart’s mitral valve, contributing to a heart disease known as degenerative mitral regurgitation, according to a new multicenter study involving researchers from the Pediatric Heart Valve Center at Children’s Hospital of Philadelphia.
The study, which was co-led by CHOP’s Robert J. Levy, MD, and Columbia University’s Giovanni Ferrari, Ph.D., and also involved collaborators at the University of Pennsylvania and Valley Hospital Heart Institute, was recently published in Science Translational Medicine.
Degenerative mitral regurgitation is one of the most common cardiac valve diseases. A healthy mitral valve tightly closes the opening between the left atrium and the left ventricle when the heart contracts. With degenerative mitral valve regurgitation, the mitral valve shape becomes deformed, and the valve cannot close completely when the heart contracts, which allows some blood to leak backwards into the left atrium. This abnormal blood flow is called regurgitation.
Although patients initially are asymptomatic, over time the mitral valve becomes thickened and deformed, and patients progressively feel tired and short of breath. As pumping becomes less efficient due to this leak, the heart needs to work harder. This extra work for the heart eventually causes congestive heart failure.
Certain medications can ease symptoms and prevent complications, but they do not treat the underlying cause of the disease. If the degeneration of the mitral valve becomes severe, surgery to repair or replace the mitral valve is needed.
To better understand factors that contribute to the progression of the disease, CHOP researchers and their collaborators analyzed data from more than 9,000 patients who had undergone surgery for degenerative mitral valve disease and evaluated 100 human mitral valve biopsies, in addition to studying mouse models.
The researchers found that taking selective serotonin reuptake inhibitors (SSRIs)—the most commonly-prescribed antidepressants—was associated with severe mitral regurgitation, which required surgery at a younger age than those not taking SSRIs.
In animal models, they found that normal mice treated with high doses of SSRIs developed thickened mitral valves. They also found that mice lacking the serotonin transporter (SERT) gene, the target of SSRIs,—which transports serotonin into cells, where it cannot bind to receptors and send signals—developed thicker mitral valves.
Degenerative mitral regurgitation is one of the most common cardiac valve diseases.
Through genetic analysis, the researchers identified genetic variants in a region of the SERT gene (5HTTLPR) that affect how active SERT is. Patients with two copies of a “long” variation of the gene that make SERT less active—one copy from the mother, and one from the father—had much lower SERT activity and required surgery more often.
Patients with this “long-long” variant were more likely to react to serotonin in a way that could change the shape of the mitral valve. Additionally, “long-long” mitral valve cells were more sensitive to SSRI treatment than cells from other variants.
The researchers noted that they did not find a negative effect with normal doses of SSRIs and that a healthy mitral valve may tolerate low SERT without deforming, as it is unlikely that low SERT can cause degeneration of the mitral valve by itself. They suspect that once the mitral valve has started to degenerate, it may be more susceptible to serotonin and low SERT.
“Our study shows that taking SSRIs and having the ‘long-long’ SERT genetic variant lowers SERT activity in the mitral valve,” said Dr. Levy, attending cardiologist in the Cardiac Center and the William J. Rashkind Endowed Chair in Pediatric Cardiology at Children’s Hospital of Philadelphia.
“We suggest that assessing patients with known degenerative mitral regurgitation for potential low SERT activity by genotyping them for 5HTTLPR may help identify patients that may need mitral valve surgery earlier.”
If you are driving home from work along a road you’ve travelled numerous times before, your mind is likely to wander. You might become absorbed by a great conversation on the radio, or start rehearsing for an important meeting the next day. You steer your car down your usual route in a largely automatic way, without having to pay deliberate attention to the steering wheel, the subtle movements of your feet on the pedals, or the ever-changing traffic conditions around you. Yet if you encounter a sudden cognitive challenge, such as an unexpected road closure, you are quickly able to shift gears, identifying a new route home via a side street that you rarely use.
This kind of shift toward more deliberate thinking happens in a variety of different situations: for instance, when you have to carefully search for the solution to an especially tricky crossword clue, or think of a new way to frame an argument to change a stubborn friend’s mind. How the brain balances between the cognitive modes involved in these scenarios – relatively automatic processing and more deliberate processing – remains poorly understood, which suggests we need new ways of thinking about it.
It’s instructive to start by considering the kinds of features in our brains that might help us handle challenging multitasking situations. Firstly, we need to be able to learn all the ins and outs of a particular challenge – otherwise, how might we anticipate the next step in a complex sequence, like driving along a road occupied by other cars and pedestrians? We also need to be able to process all the information related to the task at hand, without it seeping over into another process we’d like to run in parallel – otherwise, we might allow a crescendo on the stereo to affect whether we swerve our car’s steering wheel into oncoming traffic. In addition, we’d like to be alerted when any process we’re allowing to run on its own goes awry. Deprived of this control, we’d plough right through a red light or fail to notice a pesky detour sign.
None of these complex functions are controlled by a single neural structure. Rather, they are emergent properties of the interactions among widespread regions in the nervous system. There is ample evidence that coordinated interactions between the cerebral cortex and the thalamus allow us to link opportunities for action (such as a steering wheel and pedals) with goals and plans (driving a car to get to the store). However, these two major neural systems don’t work alone. For instance, both structures are strongly connected to the cerebellum, a massive structure at the base of the brain. The cerebellum creates a high-resolution copy of the actions that we take in a given context, and then learns to recombine features of the situation and our planned action into the best response for what to do next in that situation. In contrast, inhibitory circuits within the thalamus and cerebral cortex are better suited for ensuring that different sequences (eg, steering the car and listening to music) don’t blend into one another.
The ability to control the balance between automatic and deliberate processing is well suited to the neuromodulatory arousal system. This system is made up of nuclei (collections of nerve cells) that project widely throughout the brain, wherein they release neurochemicals that change the way that different regions interact. Based on their widespread connectivity, these structures provide modulatory control of all of the other processes. For instance, the neurochemical noradrenaline controls key features of arousal, whereas dopamine is more important for motivation.
What if we use the gastrointestinal system as an analogy for how the brain uses serotonin?
With this perspective in mind, which neurochemical system is the most crucial for controlling the balance between more automatic and more deliberate cognitive processing? Based on previous research, my colleagues and I had a hunch that the serotonergic system might be a good place to look. Serotonin is released into the brain from multiple different nuclei, including the raphe nuclei and the medullary reticular formation. Once released, serotonin has an extremely complex set of effects, as there are a wide range of different serotonin receptors that can turn the presence of the neurochemical into different cellular outcomes. In fact, researchers have struggled to produce simplified explanations for the system that capture all of its inherent complexity.
My collaborators and I found a new way to tackle both the serotonin and cognitive-mode problems. We started from an interesting fact: more than 95 per cent of the serotonin in the body is actually used by the gastrointestinal tract. Serotonin released in the gut controls peristalsis, the involuntary muscle movement that pushes along the contents of the digestive system. So, we wondered: what if we use the gastrointestinal system as an analogy for how the brain uses serotonin? Instead of digesting (ie, processing) food, what if serotonin was being used by our brains to digest information – that is, to process information flow between the distributed circuits of neurons required to identify, decide and act?
Sign-up to our weekly newsletter
Intriguing articles, practical know-how and immersive films, straight to your inbox.
Any time there is a problem to be solved or a decision to be made, our brains must figure out which resources to deploy to meet the challenge. It stands to reason that the brain would like to use tried-and-tested approaches as a first pass. When you reach for a mug of coffee on the table, you use a normal grip that is consistent with the shape of a typical mug. If this simple approach works, you’ve freed up the rest of your brain to focus on other tasks (such as talking to a friend). The cerebellum, which is responsible for executing well-learned actions such as this one, is absolutely doused in serotonergic inputs that increase its ability to provide rapid, precise feedback to the cortex. In the cortex, serotonin also acts to inhibit cortical output via inhibitory 5-HT1 receptors – effectively signalling that the cerebellum can digest the information without any cortical help.
Through these processes, serotonin helps the brain continue with an automatic or habitual approach to a situation when that seems to be working well. This is analogous to digestion: if the food you eat can be broken down easily, serotonin will help to ease its passage through the typical digestive process.
Individuals who compulsively focus on negative thoughts might be viewed as suffering from a state akin to cognitive ‘constipation’
Sometimes, however, the in-built approach fails. Maybe the mug is oddly shaped, or turned away from the easy reach of your grasp. Or, going back to the driving example, your usual route home is closed off. In these instances, excitatory 5-HT2A receptors in the cortex are poised to take over. These receptors – which are activated by serotonin – coat excitatory pyramidal cells in the cortex and boost context-specific inputs to the cells. In this way, serotonin increases the range of different cortical cells that can be used to solve the problem at hand – eg, to figure out a way to grasp the mug or to make your way home. This idea maps on to the situation in the gut. If there is a blockage (perhaps caused by overindulgence at a fondue party), then the gut can turn up the peristalsis to deal with it. We envision an analogous situation with cognitive problems: if there is a blockage (eg, your initial approach doesn’t work), then you need to create new options for solving the problem.
Why should serotonin play this role in cognitive processing, and not some other neurotransmitter? The answer, like many in evolutionary neuroscience, is difficult to pin down, given how much time has passed since the events that catalysed this putative function. There’s nothing particularly special about serotonin compared with other neuromodulatory chemicals, such as dopamine and noradrenaline. They each arise as metabolites of food products and use similar types of cellular mechanisms to enact change in the nervous system. Simply put, they were likely the kinds of fodder that were around when animals (or perhaps single cells) needed a means for conveying a simple message (eg, We just ate, it’s time to digest) to a complex system of interconnecting parts. What was striking to my colleagues and me, however, was just how cleanly the idea of digestion and satiation mapped on to the language of cognition, and how fitting the new framing seemed to be for thinking about what serotonin might do (and not do) when the system is pushed to its natural extremes.
This perspective could help to make sense of some other effects of serotonin. For instance, the active component of many psychedelic drugs is the activation of the excitatory 5-HT2A receptor, albeit in ways that alter the typical timescales upon which the receptors normally act. The effect could be a bit like the brain acting as if previously learned solutions to problems aren’t feasible, and doing so in a manner that is mismatched to the current situation – you could be sitting quite comfortably on your couch listening to music, but experience altered visual perceptions induced by the sounds you hear, causing you to process the song in a completely new way. This viewpoint is consistent with a range of recent imaging and modelling projects showing that psychedelic agents heighten coordinated activity around the brain, helping to explain the integration of sensory experiences across different modalities.
Similarly, our perspective could help to reframe long-standing problems in psychiatry. For example, individuals who compulsively focus on negative thoughts might be viewed as suffering from a state akin to cognitive ‘constipation’. One possibility is that liberating serotonin in their brains (via commonly prescribed SSRIs) may contribute to a state of information-processing flux that opens up a set of possible options, potentially allowing individuals to reappraise situations that they had otherwise responded to relatively automatically. (It’s worth noting, though, that conditions such as depression have complex causes and are not due simply to low levels of serotonin.)
In contrast, chronically heightened levels of serotonin in the brain might be conceptualised as cognitive ‘diarrhoea’ – even when all the problems (food) have been digested, there might still be a high amount of functionally unnecessary cogitation (peristalsis) that leads to dysfunctional brain states.
Rather than attempting to solve these complex psychosocial problems, my colleagues and I simply hope that this novel perspective on the function of the serotonergic system opens up avenues for new ideas and treatments. For now, you might use it to reframe how you think about your own brain. The next time you’re driving home in a car or sitting down to enjoy a meal, spare some thought for the ways in which the neurochemical soup in your brain mimics your gut: helping you to digest complex patterns of information as you navigate the intricacies of your daily life.
Summary: A newly identified serotonin pathway that originates from the median raphe nucleus acts in opposition to the reward/aversion pathway in the nearby dorsal raphe nucleus. The findings could pave the way for the development of new treatments for major depression, addiction, and other disorders associated with serotonin.
Scientists in Japan have identified a nerve pathway involved in the processing of rewarding and distressing stimuli and situations in mice.
The new pathway, originating in a bundle of brain stem nerve fibres called the median raphe nucleus, acts in opposition to a previously identified reward/aversion pathway that originates in the nearby dorsal raphe nucleus.
The findings, published by scientists at Hokkaido University and Kyoto University with their colleagues in the journal Nature Communications, could have implications for developing drug treatments for various mental disorders, including addictions and major depression.
Previous studies had already revealed that activating serotonin-producing nerve fibres from the dorsal raphe nucleus in the brain stem of mice leads to the pleasurable feeling associated with reward.
However, selective serotonin reuptake inhibitors (SSRIs), antidepressant drugs that increase serotonin levels in the brain, fail to exert clear feelings of reward and to treat the loss of ability to feel pleasure associated with depression.
This suggests that there are other serotonin-producing nerve pathways in the brain associated with the feelings of reward and aversion.
To further study the reward and aversion nerve pathways of the brain, Hokkaido University neuropharmacologist Yu Ohmura and Kyoto University pharmacologist Kazuki Nagayasu, together with colleagues at several universities in Japan, focused their attention on the median raphe nucleus.
This region has not received as much research attention as its brain stem neighbour, the dorsal raphe nucleus, even though it also is a source of serotonergic nerve fibres.
The scientists conducted a wide variety of tests to measure activity of serotonin neurons in mice, in response to stimulating and inhibiting the median raphe, by using fluorescent proteins that detect entry of calcium ions, a proxy of neuronal activation in a cell-type specific manner.
They found that, for example, pinching a mouse’s tail—an unpleasant stimulus—increased calcium-dependent fluorescence in the serotonin neurons of the median raphe. Giving mice a treat such as sugar, on the other hand, reduced median raphe serotonin fluorescence.
An illustration of the facial expression changes in mice following stimulation and inhibition of the median raphe nucleus. Credit: Yu Ohmura
Also, directly stimulating or inhibiting the median raphe nucleus, using a genetic technique involving light, led to aversive or reward-seeking behaviours, such as avoiding or wanting to stay in a chamber—depending on the type of stimulus applied.
The team also conducted tests to discover where the switched-on serotonergic nerve fibres of the median raphe were sending signals to and found an important connection with the brain stem’s interpenduncular nucleus.
They also identified serotonin receptors within this nucleus that were involved in the aversive properties associated with median raphe serotonergic activity.
Further research is needed to fully elucidate this pathway and others related to rewarding and aversive feelings and behaviours.
“These new insights could lead to a better understanding of the biological basis of mental disorders where aberrant processing of rewards and aversive information occur, such as in drug addiction and major depressive disorder,” says Ohmura.
Appropriate processing of reward and aversive information is essential for survival. Although a critical role of serotonergic neurons in the dorsal raphe nucleus (DRN) in reward processing has been shown, the lack of rewarding effects with selective serotonin reuptake inhibitors (SSRIs) implies the presence of a discrete serotonergic system playing an opposite role to the DRN in the processing of reward and aversive stimuli.
Here, we demonstrated that serotonergic neurons in the median raphe nucleus (MRN) of mice process reward and aversive information in opposite directions to DRN serotonergic neurons.
We further identified MRN serotonergic neurons, including those projecting to the interpeduncular nucleus (5-HTMRN→IPN), as a key mediator of reward and aversive stimuli.
Moreover, 5-HT receptors, including 5-HT2A receptors in the interpeduncular nucleus, are involved in the aversive properties of MRN serotonergic neural activity.
Our findings revealed an essential function of MRN serotonergic neurons, including 5-HTMRN→IPN, in the processing of reward and aversive stimuli.
Summary: Inserting a microelectrode deep into the brain to measure serotonin and dopamine levels of patients scheduled to receive deep brain stimulation is safe and effective.
Source: Wake Forest University
Scientists at Wake Forest University School of Medicine have demonstrated that a neurosurgical procedure used to research and measure dopamine and serotonin in the human brain is safe.
Their findings are published online in PLOS One, a journal published by the Public Library of Science.
“Dopamine and serotonin are neurotransmitters that affect how people think, feel and act,” said Kenneth T. Kishida, Ph.D., associate professor of physiology and pharmacology and neurosurgery at Wake Forest University School of Medicine and principal investigator of the study. “These neurotransmitters are chemical messengers used by the nervous system to regulate countless functions and processes in the body.”
Measuring dopamine and serotonin in humans, with the speed (10 times per second) and accuracy that Kishida’s team is able to achieve, can only be done during invasive procedures such as deep-brain stimulation (DBS) electrode implantation, which is commonly used to treat conditions such as epilepsy, Parkinson’s disease, essential tremor and obsessive-compulsive disorder.
Since 2011, Kishida’s research team has collaborated with Atrium Health Wake Forest Baptist neurosurgeons Stephen B. Tatter, M.D., Ph.D., and Adrian W. Laxton, M.D., to study these neurotransmitters. To detect and record serotonin and dopamine released from neurons, a carbon fiber microelectrode is inserted deep into the brain of patients who are scheduled to receive a DBS implant to treat their conditions.
After the microelectrode insertion and while patients are awake in the operating room, they perform decision-making tasks similar to playing a simple computer game. As they perform tasks, measurements of dopamine and serotonin are taken in the striatum, the part of the brain that controls cognition, reward and coordinated movements.
After the microelectrode insertion and while patients are awake in the operating room, they perform decision-making tasks similar to playing a simple computer game.
For this study, researchers identified 602 patients who had the DBS implantation procedure between January 2011 and October 2020. Of these, 116 patients volunteered to also take part in the research protocol with the carbon fiber microelectrode, and 486 patients did not.
“We compared the infection rate across these two groups and found no significant increase or change,” Kishida said. “The brain is exposed a bit longer for the research procedure, but it does not elevate the risk of infection.”
Kishida’s team noted that infection was observed in 1 (.21%) out of the 486 patients that did not participate in the research procedure and 2 (1.72%) of the 116 patients that did have the procedure.
“These findings show that the research procedures used for monitoring of neurotransmitter release can be performed without increasing the rate of infection,” Kishida said.
According to Kishida, demonstrating the safety of the research procedure is critical for future studies.
“Having a better understanding of how these brain chemicals work in people may lead to improved medications or treatments for movement disorders, substance use disorder or depression,” Kishida said.









{kind=link}
{kind=link}