Findings suggest need to consider reproductive health alongside prevention of insect-borne diseases
Researchers have uncovered evidence hinting that the most common bug spray ingredient, DEET, might cause reproductive problems by affecting the formation of egg cells during pregnancy.
The findings come from a study in C. elegans — worms that don’t look like they have much in common with humans yet serve as surprisingly usefulbellwethers of how toxins in the environment affect human reproduction.
The research, published Jan. 4 in iScience, raises difficult questions. Chief among them is how to balance the possible reproductive harms of DEET-containing products in people — including infertility, miscarriage, or birth defects — with the need to ensure that people remain protected from diseases transmitted through insect bites, such as malaria, Lyme disease, West Nile virus, and Zika virus disease.
Whether and how much DEET use causes reproductive problems in humans will need to be confirmed in future studies. Such studies have been scarce to date in humans because of the ethical concerns involved.
Harvard Medicine News spoke with study senior author Monica Colaiácovo, professor of genetics in the Blavatnik Institute at Harvard Medical School, about what her team found and what it means.
Harvard Medicine News: Why did you conduct this study?
Monica Colaiácovo: The biggest motivator was how high DEET scored in our initial screens of how various chemicals in our environment affect meiosis, using the model organism C. elegans. Meiosis is the type of cell division that creates eggs and sperm. DEET was one of our top hits in terms of chromosomes not separating properly, so eggs end up with abnormal numbers of chromosomes. In humans, this can cause miscarriage, stillbirth, infertility, and genetic conditions such as Down syndrome. We knew we had to look at this carefully.
Learn about the worm-screening method the Colaiácovo lab developed to quickly identify chemicals that affect meiosis.
Research has shown that DEET products can have neurologic effects on people who use them, but no one had really looked at what DEET is doing in meiosis. We wanted to understand whether it would cause a problem. Only a few human studies have been done, and practically everyone uses DEET, so the possibility that it could affect reproduction felt palpable for people in our lab.
HMNews: What did you find?
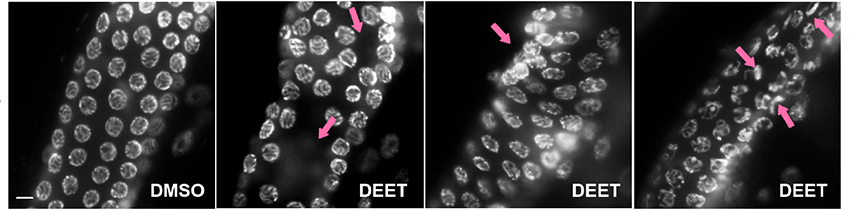
Colaiácovo: Using our worm model, we showed for the first time that DEET can have effects on meiosis. Then we showed why.
We saw that DEET has a significant impact on gene expression — the pattern of genes that are active or inactive in a cell. We found that the change resulted in oxidative stress (an imbalance between free radicals and antioxidants) and abnormal structure of the materials that form chromosomes, which compromised the ability of chromosomes to separate properly as the cell divided. Egg cells and the worm embryos they gave rise to were less healthy.
Left two images: Normal chromosome separation during meiosis in worms. Right three images: DEET exposure caused a variety of disruptions. Images: Nara Shin
HMNews: How applicable are the worm findings to humans?
Colaiácovo: That is always the big question. Many human genes have equivalents in C. elegans, and worms are a powerful model for looking at effects on reproduction. C. elegans have been instrumental in uncovering how environmental toxicants such as the plastics chemical BPA can harm reproductive health.
We observed the changes in meiosis when the levels of DEET inside the worms were the same as, and in some cases lower than, what you find in blood or urine samples from the regular human population. That said, the paradigm for exposure wasn’t the same as it is for most people. The worms were exposed to DEET for 24 hours at a time, which may not apply to anyone, or apply to only certain groups, such as agricultural workers. And there are some metabolic and physiological differences between worms and humans.
A very important thing from our studies is that we’re providing reproducible, well-controlled, substantial data. Other groups can take up this work in mice or other animal models and further advance our understanding of what DEET may be doing in human reproductive systems. We can also build on this evidence to flag chemicals of concern for policymakers.
DEET exposure led to missing, aggregated, and abnormal eggs in the worms. Images: Nara Shin
HMNews: At this stage, how would you frame recommendations for people? How do you balance reproductive health with prevention of diseases from mosquitoes and ticks?
Colaiácovo: My family is from South America, where Zika and dengue, for example, are common, and I want to make sure people are not scared away from being careful. So-called tropical diseases transmitted by insects are moving into new regions of the world as the climate changes, putting more and more people at risk. The consequences of stopping the use of insect repellents can be very serious
So, we want prevention. We want repellents. And DEET is a very effective option we have right now. At this moment, I would say we should be aware of the potential reproductive risks of DEET-containing products and be sure to follow the application instructions when using them. Our work suggests this is very important for pregnant women because female meiosis begins in the developing fetus in the womb.
I would love to see research give rise to best practices for applying DEET products during pregnancy, when there’s often so much confusion and anxiety about what to do or not do.
I also hope our work helps drive the development of DEET alternatives that are safe and effective. It would be great to have an effective insect repellent that doesn’t make us worry about our health or that of our children.
Unexpected rise of ‘decidual cast’ searches after COVID vaccine launch
(Shutterstock)
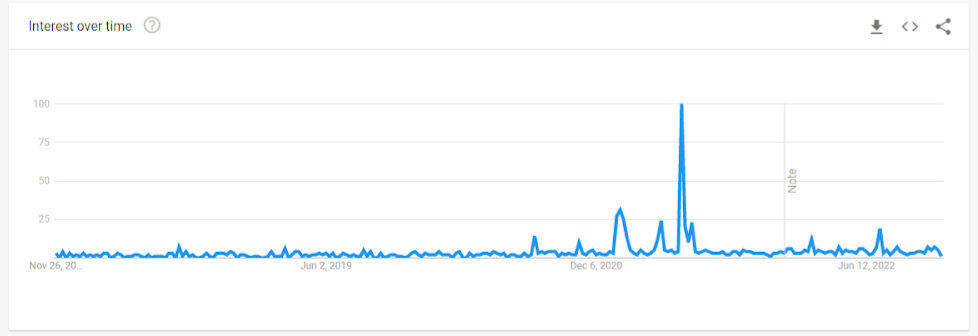
In late January, 2021, just a month after the Pfizer and Moderna COVID-19 vaccines were granted Emergency Use Authorization (EUA) by the Food and Drug Administration (FDA) in December 2020, a dramatic change in Google trend searches for “decidual cast” was evident.
Another surge in interest occurred in mid-June 2021, a month after the Pfizer vaccine was granted an expanded EUA for adolescents ages 12–15 years.
A decidual cast is defined as: “a large, intact piece of tissue that is passed through the vagina in one solid piece. It happens when the thick mucus lining of the uterus, called the decidua, sheds in the near exact shape of a uterine cavity, creating a triangular cast.”
Women began reporting unusual menstrual conditions on social media, including decidual cast shedding (DCS). This prompted several internet-based surveys, one of which was conducted by MyCycleStory.com.
While the literature contains only case reports of DCS, making the true prevalence difficult to measure, the condition is thought to be quite rare. Fewer than 40 cases have been published over the course of 100 years, usually related to ectopic pregnancy, miscarriage, or prolonged progesterone use.
Even though the absolute number of cases is not that high, this unusually increased incidence over the background rate requires further study to ascertain the cause, and any other potential contributors related to the pandemic.
Studies Observe an Impact on Women’s Menstrual Cycle
In the United States Vaccine Adverse Event Reporting System (VAERS), over 11,000 people self-reported a menstrual-related issue to the system following COVID-19 vaccination by April 2022. Events included heavy bleeding, irregular or delayed menstruation, oligomenorrhea, and amenorrhea.
Likewise, the United Kingdom’s Medicines and Healthcare Products Regulatory Agency (MHRA) yellow card surveillance scheme received 51,695 reports of menstrual disorders, including heavier or delayed periods, and unexpected bleeding, after the COVID-19 vaccine.
Findings from these databases suggested the possibility of negative impacts in menstrual cycles following COVID-19 vaccination. The relationship between COVID-19 vaccination and menstrual cycle has been evaluated in several peer-reviewed studies.
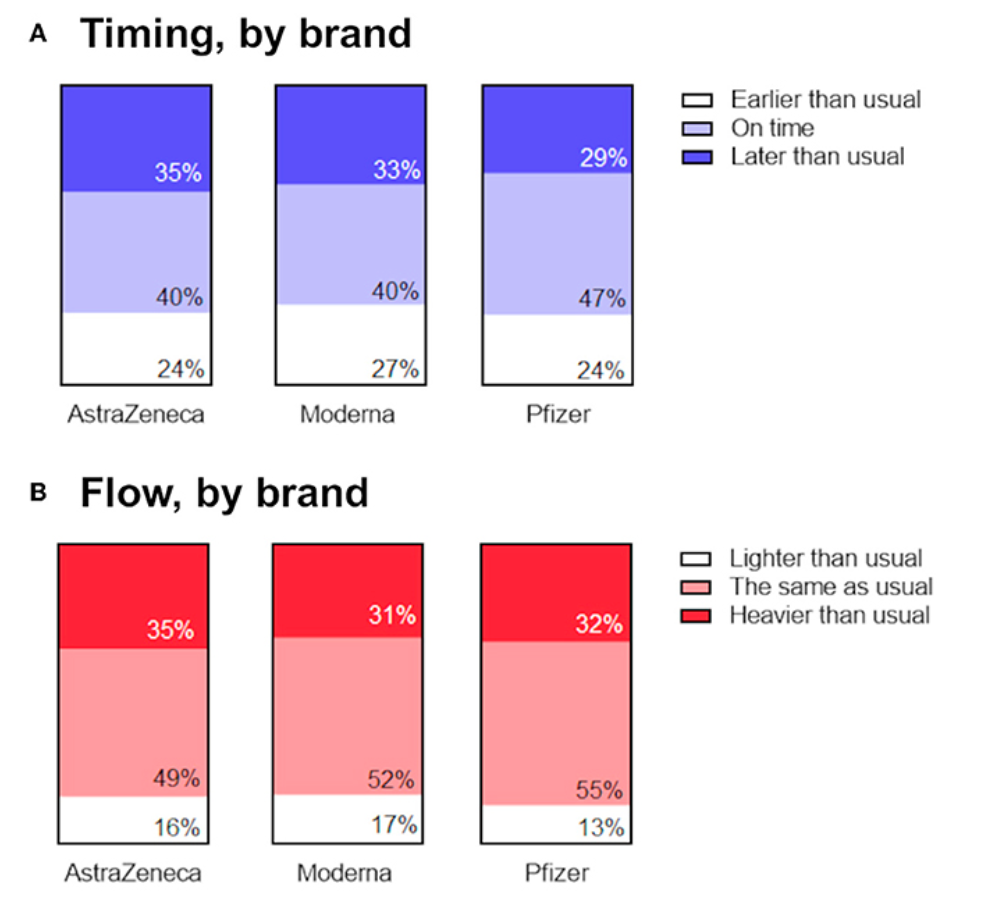
In a large prospective cohort study conducted by Harvard, the Apple Women’s Health study, cycle length was manually tracked by 9,682 vaccinated and unvaccinated women who contributed 128,094 menstrual cycles, most of whom were vaccinated (88 percent) with Pfizer (55 percent) or Moderna (37 percent). Both cycle length and menses length were tracked prospectively to capture baseline, vaccination, and follow-up measures.
This study found that mean cycle length did increase following vaccination, particularly for women who received their vaccine during the first two weeks of the cycle, during the follicular phase.
Following the first dose in the follicular phase, the cycle length increased by 0.97 days, and following the second dose by 1.43 days. The cycle remained longer for one to two months after vaccination then returned to baseline.
Women who were vaccinated during the luteal phase tended to have a shorter cycle (-0.97 days).
Another prospective United States cohort study of nearly 4,000 women ages 18 to 45 years evaluated those with normal cycle lengths for three consecutive cycles before the first vaccine dose and three post-vaccine cycles (cycles 4, 5, and 6). Those who were unvaccinated were evaluated over six cycles during a similar time period.
The investigators computed within-individual changes in cycle length and menses length for cycles 1–3 and 4–6 then used mixed-effects models to compare differences in cycle and menses length between the vaccinated and unvaccinated cohorts.
The investigators found a mean 0.91 day increase in mean cycle length for women receiving the mRNA vaccine during their second vaccine cycle.
More vaccine recipients had a cycle length change of at least 8 days than unvaccinated (6.5 percent vs 4.6 percent, p=0.017). The longer vaccine cycles seemed to be concentrated among the 358 individuals who received both doses within a single cycle.
In this subgroup of vaccinated women, the unadjusted mean cycle length increase was 2.38 days and a substantially larger proportion (10.6 percent) had an increased cycle length of at least 8 days compared with the unvaccinated cohort (4.3 percent, P<.001).
The authors found no difference in menses length between cohorts.
A smaller Israel study among 219 women regularly tracking cycles also found changes in menstruation reported by almost 40 percent of vaccinated women. Parity (number of pregnancies) and medication use seemed to be risk factors for menstrual irregularities.
Half of those suffering from irregular bleeding were multiparous versus 31.5 percent multiparity among women with no irregular bleeding. Presence of comorbidities was also higher among women reporting irregular bleeding.
Interestingly, women reporting regular medication use were less likely to report irregular bleeding.
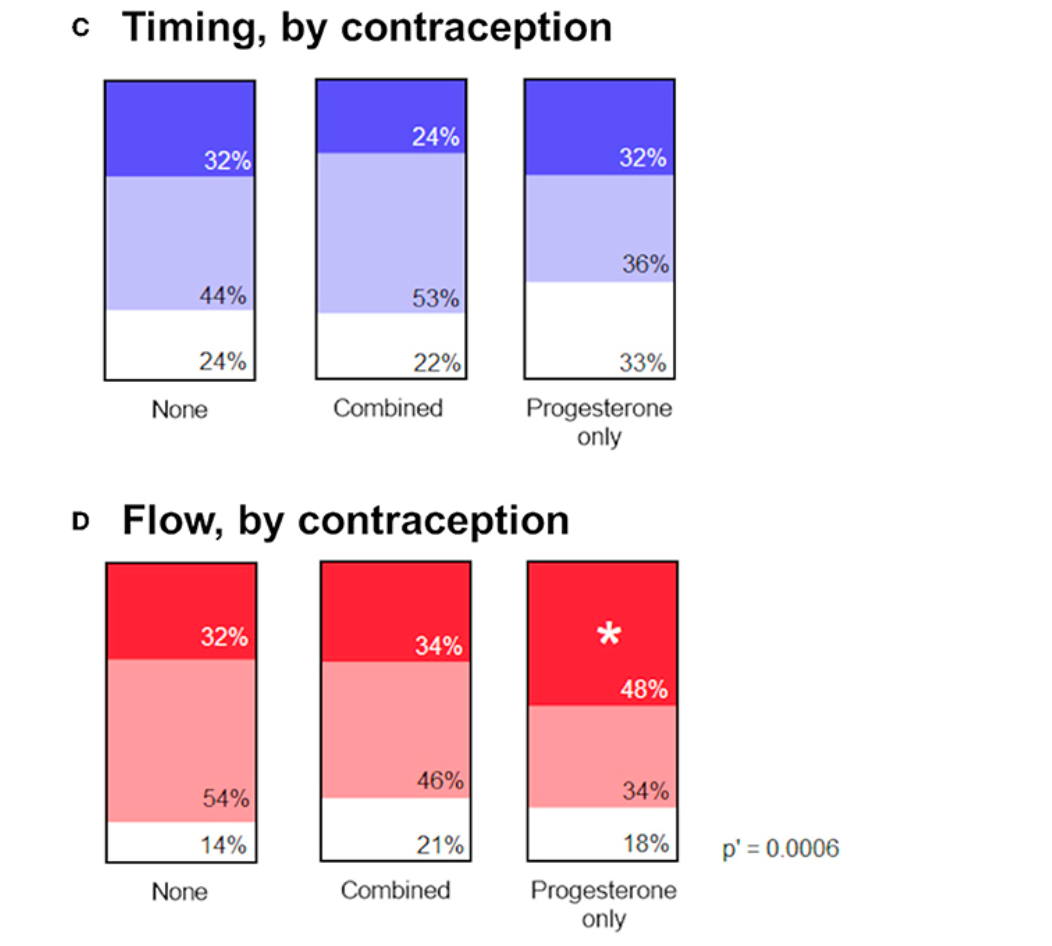
Another study included both a prospective cohort of 79 women and a retrospective cohort of 1273 women.
The study did also find a cycle length increase (delay to the next period) in women cycling spontaneously, suggesting that COVID-19 vaccination can lengthen the menstrual cycle.
However, no such change was observed among those using contraception, suggesting that this effect of COVID-19 vaccination may be mediated by ovarian hormones.
Source: Alvergne A, Woon EV and Male V (2022) Effect of COVID-19 vaccination on the timing and flow of menstrual periods in two cohorts. Front. Reprod. Health 4:952976. doi: 10.3389/frph.2022.952976
While several studies (references 9–14) have suggested that COVID-19 infection can cause changes in cycle length, the Nurses’ Health Study did not detect such an association following COVID-19 infection.
In this study, COVID-19 vaccination was associated with cycle length in the short term (within 6 months of vaccination), particularly among women with short, long, or irregular cycles prior to vaccination. Changes in cycle length were detected for both mRNA and adenovirus-vectored vaccines.
A plausible connection between COVID-19 vaccination–both mRNA and adenovirus-vectored vaccines–and increased cycle length appears reasonable. The effect seems most pronounced among women who have already had a child and who receive both doses within a single cycle, which is consistent with the survey study from Israel.
VAERS Data Suggests Increased Risks of Menstruation and Pregnancy Irregularities
A preprint study of adverse events (AE) reported to the Vaccine Adverse Events Reporting System (VAERS) compared the ratio of AEs due to COVID-19 vaccines to influenza vaccines. Thorp and colleagues gathered data on pregnancy and menstruation irregularities reported to VAERS between Jan. 1, 1998 to June 30, 2022.
The reporting ratio for AEs related to COVID-19 vaccines compared to influenza vaccines were at least double (and statistically significant at p<0.05) for the following:
menstrual abnormality (MA), miscarriage(M), fetal malformation (FM), fetal cardiac disorders (FCD), fetal growth abnormalities (FGA), fetal abnormal surveillance (FAS), fetal death/stillbirth (FS) and low amniotic fluid (LAF), which are listed In the below graph. A value greater than 1 implied that AE are reported more frequently with COVID-19 vaccine compared to influenza vaccines.
fetal chromosomal abnormalities, fetal cystic hygroma, fetal arrhythmia, fetal cardiac arrest, fetal vascular mal-perfusion, fetal placental thrombosis, which are not included in the Figure but also significantly increased.
It should be noted that for any VAERS study, this is a passive reporting system which relies on physician reporting and may not reflect the true rate for the AE. Detection of AEs may vary significantly depending on public awareness of the AE, thus sensitivity may be as low as 1% percent of all AEs or 67 percent. Self-reports by patients are not necessarily confirmed by a physician diagnosis. The VAERS database is appropriate for hypothesis-generation, but population-based studies are needed to understand true incidence and causation.
Global relative rates of AE reports after COVID-19 vaccines versus those after influenza vaccines by dose given. Source of preprint: James A. Thorp, Claire Rogers, Michael P. Deskevich, Stewart Tankersley, Albert Benavides, Megan D. Redshaw and Peter A. McCullough. COVID-19 Vaccines: The Impact on Pregnancy Outcomes and Menstrual Function. Link of preprint.
Canadian Study Observed Increased Risks of Severe Adverse Events During Pregnancy
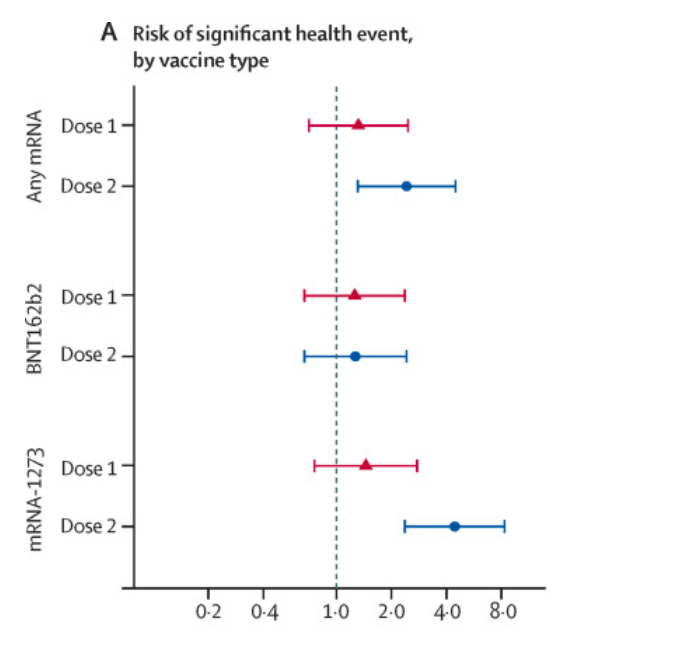
A Canadian prospective observational cohort study of COVID-19 vaccines, published in Lancet Infectious Disease pregnancy, evaluated the frequency of significant health events among 5625 pregnant / vaccinated, compared with 339 pregnant / unvaccinated and 185 735 nonpregnant / vaccinated controls, resulting a total of 191,360 women ages 15–49 years included.
The data were collected by survey with follow-up phone calls to those reporting any medically attended event.
The pregnant vaccinated females had a 4.4-fold (95 percent CI 2.4-8.3) increased risk of a severe health event after dose two of Moderna compared to pregnant unvaccinated females; this association was not seen for those vaccinated with Pfizer.
The dose of Moderna vaccine (100mcg) is more than 3 fold that of Pfizer (30mcg) in adults, which may well explain the different results among vaccine brands.
Sadarangani M, Soe P, Shulha HP, Valiquette L, Vanderkooi OG, Kellner JD, Muller MP, Top KA, Isenor JE, McGeer A, Irvine M, De Serres G, Marty K, Bettinger JA; Canadian Immunization Research Network. Safety of COVID-19 vaccines in pregnancy: a Canadian National Vaccine Safety (CANVAS) network cohort study. Lancet Infect Dis. 2022 Nov;22(11):1553-1564. doi: 10.1016/S1473-3099(22)00426-1.
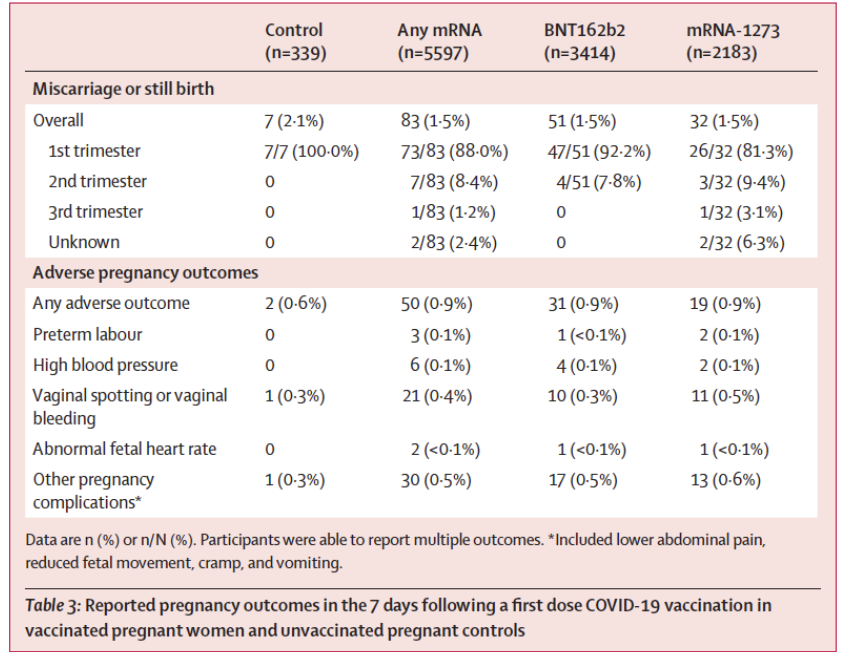
Miscarriage or stillbirth was the most frequently reported adverse pregnancy outcome. Both miscarriage and stillbirth describe pregnancy loss, but they differ according to when the loss occurs. In the United States, a miscarriage is usually defined as loss of a baby before the 20th week of pregnancy, and a stillbirth is loss of a baby at or after 20 weeks of pregnancy.
It was reported at similar rates between control (2.1 percent of 339) and vaccinated groups within seven days after dose one of any mRNA vaccine (1.5 percent of 5,597).
Other rare adverse pregnancy outcomes such as vaginal bleeding, abnormal fetal heart rate, and reduced fetal movement were increased slightly within seven days following any mRNA vaccination compared to control.
There were an additional individuals who reported experiencing miscarriage or stillbirth between the first COVID-19 vaccine dose and completion of the second (dose two) survey (up to 10 days after dose two), however the precise timing of these events relative to vaccination was not known.
Sadarangani M, Soe P, Shulha HP, Valiquette L, Vanderkooi OG, Kellner JD, Muller MP, Top KA, Isenor JE, McGeer A, Irvine M, De Serres G, Marty K, Bettinger JA; Canadian Immunization Research Network. Safety of COVID-19 vaccines in pregnancy: a Canadian National Vaccine Safety (CANVAS) network cohort study. Lancet Infect Dis. 2022 Nov;22(11):1553-1564. doi: 10.1016/S1473-3099(22)00426-1.
Impact on Fertility
The impact of vaccination and infection on ovarian function and fertility is a heavy topic. The key findings from a number of peer-reviewed publications and preprints has been summarized here.
Reduced Total Fertility Rate (TFR)
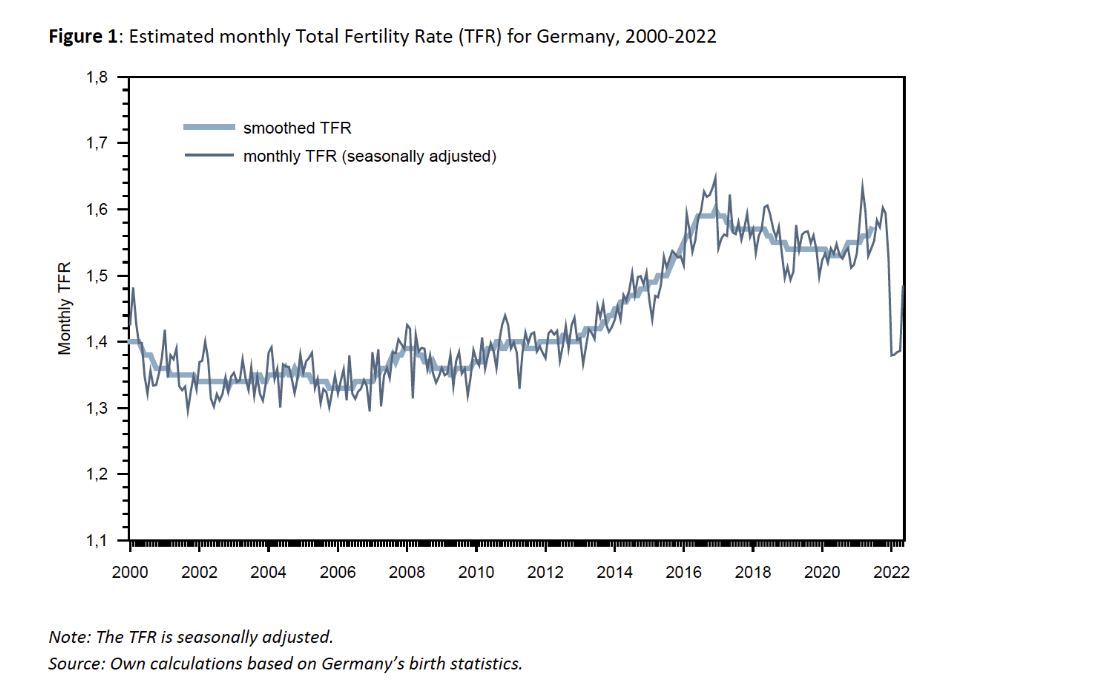
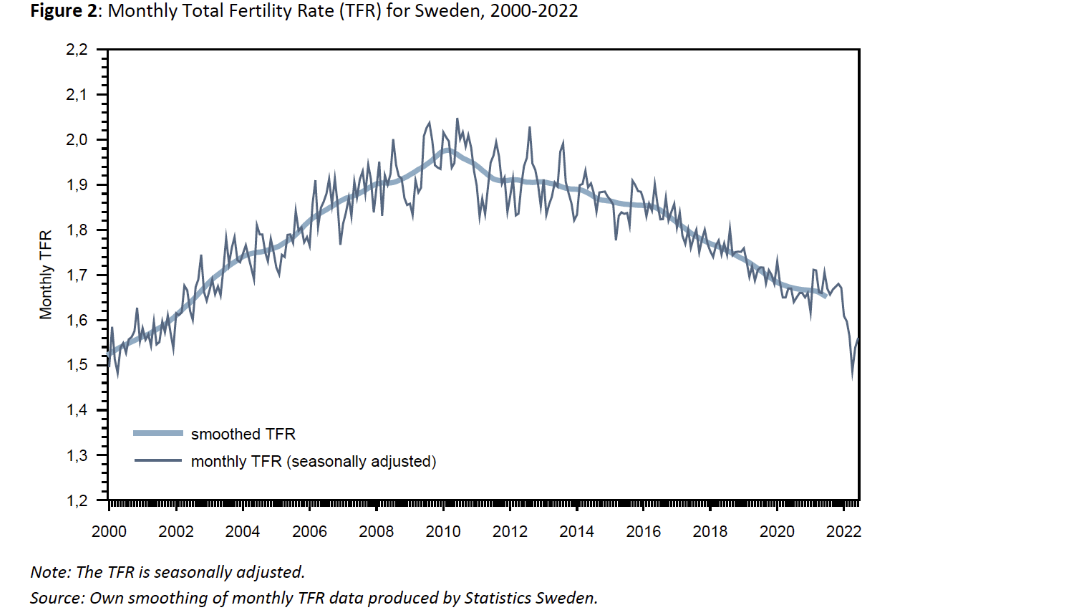
There is a population-wide change in fertility after vaccination campaigns. In a new preprint, the total fertility rate (TFR) in Sweden and Germany was trended over time, from early in the pandemic through 2022.
Many countries noticed a fertility decline early in the pandemic, but Germany and Sweden were largely unaffected. These countries, however, recently experienced a reduction in the TFR.
The seasonally-adjusted TFR in Germany declined 14 percent from 1.5-1.6 in 2021 to 1.3-1.4 in early 2022. A similar trend was seen in Sweden, with a 10 percent decline from 1.7 to 1.5-1.6.
The authors note that the sharp declines in TFR align with the onset of vaccination campaigns precisely nine months prior. The authors speculate that concerns about vaccine safety during conception and pregnancy might have caused women to hold off on starting their family until after vaccination.
Further population-based longitudinal research is necessary to detect any slight but significant effects of vaccination on fertility.
Source: Martin Bujard and Gunnar Andersson. Fertility declines near the end of the COVID-19 pandemic: Evidence of the 2022 birth declines in Germany and Sweden. Link of the source. Source: Martin Bujard and Gunnar Andersson. Fertility declines near the end of the COVID-19 pandemic: Evidence of the 2022 birth declines in Germany and Sweden. Link of the source.
In the systematic review, 29 studies conducted in Israel, United States, Russia, China, Italy, North America, and Turkey were included.
The pregnancy rates were observed to decline in the vaccinated group by 15 percent for biochemical pregnancy rate and by 4.3 percent for clinical pregnancy rate, in a comparison to the unvaccinated group.
It is reported that both declines did not reach a statistical difference among vaccinated and not vaccinated groups. However, a clinical meaningful decline is not necessarily to be statistically significant. And whether to achieve a statistical difference or not may be confounded by the power of studies.
Furthermore, meta-analyses were performed for pre- and post-vaccination sperm progressive motility (44 percent versus 43 percent, p = 0.07).
Anti-Müllerian Hormone (AMH)
Anti-Müllerian hormone (AMH) has been used as a marker to assess ovarian function in women and it impacts fertility. It gives an estimate of ovarian reserve–how many eggs are remaining in the ovaries. Older women normally have lower levels than younger women.
In a prospective study conducted in Israel among 129 women who received two mRNA vaccines, the change in AMH was assessed via baseline and 90-day measurements, pre- and post-vaccination.
In this study, no change was detected in AMH levels pre- vs post-vaccination (5.3 vs 5.3 µg/l, respectively).
The authors concluded that while this study was limited to a three-month followup after the first vaccination, there did not appear to be any effect of mRNA vaccination on ovarian function.
Another similar but smaller Israeli prospective study among 31 women undergoing in vitro fertilization (IVF) treatment found that AMH remained stable pre- and post-mRNA vaccination.
There are limitations of the AMH studies. First, there is no control group and only self control was used.
Second, serum AMF levels are known to be affected by multiple factors including obesity, vitamin D levels, oral contraceptive therapies, genes (BRCA mutations contributing to breast and ovarian cancers), chemotherapy, common ovulatory disorders (polycystic ovary syndrome, PCOS), and history of ovarian surgery. Any potential changes in common confounding factors for serum AMF levels (body weight, contraceptives, vitamin D levels) in these subjects should be analyzed and reported.
In a retrospective study including 200 women undergoing IVF, no difference in fertility outcomes was detected, including oocyte retrieval, fertilization and pregnancy rates, and embryo quality.
Although this study found similar pregnancy rates between vaccinated and unvaccinated (32.8 percent and 33.1 percent, respectively), it would have required a much larger sample size to detect a small but meaningful difference.
A sample of at least 985 participants would be needed to detect a smaller 5 percent difference in pregnancy rates. In other words, this study was underpowered to detect a meaningful difference of reduction in pregnancy rates.
In another retrospective cohort study of 222 vaccinated and 983 unvaccinated women who underwent ovarian hyperstimulation, no effect of vaccination was found for the primary outcome, fertilization rate, nor any of the secondary outcomes, including eggs retrieved, mature oocytes retrieved, mature oocyte ratio, blastulation rate, or euploid rate.
For 214 vaccinated and 733 unvaccinated women undergoing frozen-thawed euploid transfer, the adjusted analysis found no significant association for vaccination and the primary outcome, clinical pregnancy (adjusted odds ratio [aOR] 0.79, 95 percent CI 0.54-1.16), nor any of the secondary outcomes: pregnancy (aOR 0.88, 95 percent CI 0.58-1.33), ongoing pregnancy (aOR 0.90, 95 percent CI 0.61-1.31), biochemical pregnancy loss (aOR 1.21, 95 percent CI 0.69-2.14), or clinical pregnancy loss (aOR 1.02, 95 percent CI 0.51-2.06).
However, these confidence intervals are large and the sample size insufficient to rule out a small but clinically meaningful difference in outcomes.
A small cohort study of 32 individuals (9 recovered SARS-CoV-2 positive, 9 vaccinated, 14 uninfected/unvaccinated) found no differences in follicular function and oocyte quality.
Together, these studies suggest that any effect of either infection or vaccination on fertility will be difficult to detect unless studies are designed with sufficient statistical power geared to expected changes in primary and secondary endpoints.
A decrease of 0.3 percent in the vaccinated group is 30 fewer pregnancies per 10,000 women, thus any study designed to detect a difference this slight would need to enroll 770,000 women.
Some might suggest powering phase III clinical trials to detect fertility impact is impractical, but certainly intentional post-marketing surveillance when vaccine uptake is in the millions is possible.
Second, the spike protein induced local and systemic inflammation might impact the signaling between the brain and ovaries (the hypothalamus-pituitary-adrenal or HPA axis), resulting in hormone imbalances, prolongation of follicular recruitment during the early part of the cycle, and lengthening the cycle.
Third, ovarian inflammation may also be caused by lipid nanoparticles (LNP) effects on hormones, an autoimmune reaction with anti-syncytin antibodies at the endometrium, or inflammatory processes triggered by the spike protein either from the vaccine or infection.
Fourth, abnormal bleeding can be caused by abnormal local clotting in the endometrium during the period.
Based on the evidences of spike protein’s domino-like activities related to abnormal blood clotting, the potential role of spike protein originating from SARS-CoV-2 or COVID-19 vaccine in the abnormal bleeding of vaccinated women is likely to contribute to the surge of increased DCS and menstrual disorders during COVID pandemic, amongst other dysregulated immune and hormone mediated pathologies.
Impact on Lactation: Antibodies Detected in Milk and Symptoms Reported
A prospective cohort study included 50 lactating women who received mRNA vaccines with both blood and milk samples prior to their first vaccination dose, immediately prior to dose two, and four to ten weeks after their second dose.
Anti-SARS-CoV-2 receptor binding domain (RBD) antibodies were measured in each sample, and blood samples were collected from a subset of infants whose mothers were vaccinated while lactating.
After vaccination, levels of anti-SARS-CoV-2 IgG and IgM significantly increased in maternal plasma and there was significant transfer of IgA and IgG antibodies to milk.
Self-reported symptoms (fever, chills, headache, joint pain, muscle aches or body aches, and fatigue or tiredness) were reported by significantly more participants after the 2nd dose than after the 1st dose.
Two mothers reported slightly less milk production in the first 24-72 hours after vaccine doses.
Twelve percent of infants were reported with at least one symptom after the 1st maternal vaccine dose, which are primarily gastrointestinal symptoms and sleep changes.
The study lacked an unvaccinated control and these changes in infant behaviors are common; future studies should evaluate these reports.
The study also collected symptoms following vaccination and noted that more vaccine-related side effects may be experienced by those receiving Moderna compared to Pfizer, which should be again attributed to the higher dose of Moderna.
Natural Immunity Impact on Lactation
Finally, a study of mothers recently recovered from SARS-CoV-2 infection evaluated both antibodies and T cells in breastmilk. Because only about one in four women elect to be vaccinated during pregnancy, the ability of the mother to confer passive immunity to her infant through breast milk is an important question to assess.
In this small study of 30 lactating women, both antibody and T cell parameters were evaluated in milk samples collected at 12 timepoints over the course of a month.
A second set of samples were donated four months after a positive SARS-CoV-2 test to test durability of the immune markers.
The study confirms that women recently infected with SARS-CoV-2 have antibodies in their milk which can neutralize the spike complex. The milk is also enriched with mucosal memory T cells.
This study may be the first to demonstrate that breast milk from mothers who have recovered from SARS-CoV-2 infection contains long-lasting IgA and IgG antibody responses and that breastmilk can provide passive protection to the infant via mucosal-homing, effector-memory T cells which can seed the infant gastrointestinal tract.
Summary of Key Observations
Based on the available data collected from clinical studies, vaccine safety databases or surveys, a summary of key observations include:
Concerns about the negative impacts of COVID-19 vaccination on the menstrual cycle have been validated by peer-reviewed research.
The cycle length appears to increase following both mRNA and adenovirus-vectored vaccination, particularly for those women who received both doses within a single cycle (21-28 day interval), and those who were vaccinated during the follicular phase.
VAERS data suggests increased risks of menstruation and pregnancy irregularities. A Canadian study also observed increased risks of severe adverse events during pregnancy associated with the Moderna vaccine.
Sharp decline of total fertility rates were reported in Germany and Sweden in 2022. A 15 percent decline in the biochemical pregnancy rate and a 4.3 percent decline in the clinical pregnancy rate were reported, though AMU studies did not detect any meaningful change.
Spike protein induced inflammation, immune disorders, and hormone mediated mechanisms of action as well as abnormal clotting cascades and overactivation have been correlated to these clinical adverse events.
COVID vaccine induced antibodies have been detected in milk, as well as symptoms among mothers and infants post vaccination are reported.
The effect has been observed across spike protein-based COVID-19 vaccines regardless of vaccine type. The higher dose mRNA vaccine (Moderna) is associated with a higher likelihood of these events than the lower dose mRNA vaccine (Pfizer).
These findings strongly suggest that more rapid and intentional post-marketing surveillance is necessary to detect impacts of vaccination on menstrual, pregnancy, and lactation events.
The CDC continues to recommend vaccination and boosters for all individuals over 5 years of age despite a lack of evidence regarding an incremental reduction in serious COVID-19 illness among those younger than 40 years of age.
To address vaccine hesitancy, public health officials and regulatory agencies must demonstrate that individual concerns are addressed and that clinical trials are designed to detect rare adverse events in otherwise healthy, young individuals prior to issuing broad recommendations.
A phased trial rollout which prioritizes enrollment of higher risk individuals and follows them for clinically important endpoints, such as hospitalization and death, would allow rapid deployment of lifesaving vaccines while minimizing harm to those at low risk of serious illness.
There are some period problems that are unfortunately par for the course, like cramps, irritability, and bleeding more than you would like to be bleeding from your vagina.
But there are also some period problems that you should bring up to your doctor—just in case—because they’re a bit outside of what’s normally expected during menstruation. Here are some things to keep an eye out for.
1. You soak through a pad or tampon in an hour or less, your period lasts longer than seven days, or both.
The clinical term for an exceedingly heavy or long period is menorrhagia. These are basically horror movie-style periods, but some people don’t even realize this kind of bleeding is abnormal. “One of the biggest problems is someone being so used to heavy bleeding that she underplays the amount,” Lauren Streicher, M.D., an associate professor of clinical obstetrics and gynecology at Northwestern University Feinberg School of Medicine, tells SELF. “She’ll come in and say her periods aren’t too bad, then say she has to change her tampon every hour.” Passing clots larger than a quarter is also a sign your bleeding is too heavy, according to the Centers for Disease Control and Prevention (CDC).
WATCH THIS
Body Stories: Padma Lakshmi Tells the Story Behind Her Scar
It’s not just that bleeding way too much or for too long is messy and inconvenient. Losing more than the typical two to three tablespoons of blood during your period or bleeding for longer than seven days can lead to anemia, the CDC says. If you have anemia, you lack enough healthy red blood cells to get oxygen to all your tissues, so you may feel tired and weak, according to the Mayo Clinic.
Bleeding too much can also be a sign of various health issues, like uterine fibroids, which are benign growths in and on the uterus that can sometimes come along with problems like pelvic pain and frequent urination. Uterine polyps, which are growths on the inner lining of the uterus, can also cause heavy bleeding, as can cervical polyps, which are lumps that emerge from the cervix. Both types of polyps are typically non-cancerous but, in rare cases, may contain cancer cells.
The hormonal issue polycystic ovary syndrome (PCOS) can also cause heavy bleeding. Worse, this bleeding can strike after months of an MIA period. This gives your uterine lining a chance to build up over time, leading to an abnormally heavy period when it finally comes, Mary Jane Minkin, M.D., a clinical professor of obstetrics, gynecology, and reproductive sciences at Yale Medical School, tells SELF. PCOS can also cause symptoms like excess face and body hair or severe acne, thanks to high levels of male hormones.
Heavy menstrual bleeding could even be a sign of a disorder that causes you to lose too much blood, like idiopathic thrombocytopenic purpura (ITP). ITP usually comes along with other symptoms like easy and excessive bruising or a rash of reddish-purple dots on a person’s lower legs.
Clearly, figuring out what’s causing your heavy bleeding won’t be easy on your own, so you should see your doctor. They’ll typically ask about your other symptoms and perform exams to determine what exactly is going on, and treatment will depend on what you’re dealing with.
2. Your period brings days of pain that make it practically impossible to leave your bed.
Dr. Streicher’s rule is essentially that if you’re experiencing even an iota of period pain beyond what you’re fine with, it’s too much. The first step is typically to take nonsteroidal anti-inflammatory drugs, since they block hormone-like chemicals known as prostaglandins that cause uterine cramping. If that knocks out your cramps, you’re good to go. If you’re still curled up in the fetal position after a few hours, that’s a sign that you need evaluation, Dr. Streicher says. You’re dealing with dysmenorrhea (severe menstrual cramps), and doctors can help.
There are many different causes of overboard menstrual cramps. Fibroids are a common culprit. So is endometriosis, a condition many experts think happens when tissue lining the uterus travels outside of it and begins growing on other organs. (Other experts believe that tissue is actually different in that it can make its own estrogen, which can create painful inflammation in people with endometriosis.) In addition to causing extremely painful periods, endometriosis can lead to painful intercourse, occasional heavy periods, and infertility, according to the Mayo Clinic.
Adenomyosis, which happens when the endometrial tissue lining the uterus grows into the muscular walls of the organ, can also cause terrible menstrual pain, along with expelling big clots during your period and pain during intercourse.
3. You never know when your period is going to show up.
Pour one out for all the times you thought you’d have a period-free vacation, only for it to show up right as you hit the beach. Fun! Irregular periods could be due to a number of different things that are (at least somewhat) in your control, like stress and travel, Dr. Streicher says. But they can also happen because of various health conditions.
Take thyroid issues, for instance. Hypothyroidism, which is when your thyroid gland in your neck doesn’t produce enough hormones, can lead to an irregular period, according to the Mayo Clinic. It can also cause myriad other symptoms, like heavier than usual periods, fatigue, constipation, dry skin, weight gain, impaired memory, and more. Treatment typically involves taking medication that mimics the thyroid hormone.
On the flip side, hyperthyroidism, which is when your thyroid gland is overactive, can cause light or infrequent menstruation, along with issues like sudden weight loss, rapid heart rate, increased appetite, and more frequent bowel movements, according to the Mayo Clinic.
Irregular periods are also a sign of premature ovarian failure, which is when a person younger than 40 starts losing their normal ovarian function, according to the Mayo Clinic. It can also cause menopausal symptoms like hot flashes, night sweats, vaginal dryness, and difficulty conceiving. Doctors can offer estrogen therapy to relieve symptoms like hot flashes (typically in conjunction with progesterone to avoid the precancerous cells that may take hold if you take estrogen alone). They can also counsel you about the possibility of in vitro fertilization if you’d like to physically conceive and carry children in the future.
PCOS and uterine polyps be behind irregular bleeding, too.
4. Your period decides not to show up for a while.
While it’s true that you can sometimes randomly miss a period for reasons like stress, you shouldn’t just ignore a long-term missing period. Suddenly being period-free may feel blissful, but you’ll want to make sure there’s not a health issue going on, like PCOS, an eating disorder or excessive exercise affecting your menstruation…or, yes, pregnancy.
“If you’re menstruating normally then suddenly go months without a period, that’s not something to ignore,” Dr. Streicher says. If your period vanishes for three months or longer (this is known as amenorrhea), see your doctor for evaluation.
It’s worth noting that the use of some hormonal birth control methods—especially the hormonal IUD—can make your period basically disappear. Still, check with your doctor, just in case, when this happens.
5. You’re dealing with a lot of unexpected spotting between periods.
It could be something that’s ultimately pretty harmless, like a benign uterine or cervical polyp that’s causing bleeding between periods. But spotting is also a hallmark of pelvic inflammatory disease (PID), which is the result of sexually transmitted bacteria from infections like chlamydia and gonorrhea spreading to reproductive organs like your uterus, fallopian tubes, and ovaries. In addition, pelvic inflammatory disease can cause issues like fever, strange vaginal discharge that smells bad, and burning when you pee.
If you have PID, your doctor will first address the STI in question with antibiotics, says the CDC, then treat your partner for an STI if necessary. Pelvic inflammatory disease is a leading cause of chronic pelvic pain and infertility in women, so if you suspect you have it, treatment is of the essence.
More rarely, spotting in between periods can be a sign of cervical cancer, according to the Mayo Clinic. Cervical cancer can come along with watery, bloody discharge that might have a bad odor and pelvic pain, including during intercourse. Even though this likely isn’t your issue, you’ll want to get checked out, just in case. Treatment for cervical cancer may involve a hysterectomy, radiation, or chemotherapy.
6. You experience debilitating mood issues before your period.
When your estrogen and progesterone drop before your period, you may experience the typical mood swings that mark premenstrual syndrome (PMS). (Bear in mind that this may not be as drastic if you’re on hormonal birth control, which stabilizes your hormones throughout your cycle.)
But if you deal with severe mood swings, irritability, anger, a lack of enjoyment in things you usually enjoy, and other symptoms that affect your life, you may have premenstrual dysphoric disorder (PMDD). PMDD happens when you experience these symptoms in the week before your period, then they start getting better in the first few days of bleeding, and disappear in the weeks after your period. It’s listed in the DSM-5, the most recent version of the Diagnostic and Statistical Manual of Mental Disorders, for good reason: This psychological issue can completely turn your life upside down.
“If you suspect you have PMDD, the one thing I would encourage is keeping a daily record of the severity of your symptoms,” Dr. Minkin says. If these symptoms only rear their head the week before your period, PMDD might be your issue. If you realize you’re constantly dealing with them and your period just makes them worse, it might be premenstrual exacerbation, which is another way of saying you have a mental illness like depression that gets worse during your period.
Either way, a doctor can help. If you have PMDD, your doctor may have you take antidepressants in the timeframe when you usually experience symptoms, then stop once your period starts, Dr. Minkin says. (If you have premenstrual exacerbation, they may recommend staying on the antidepressants through the month and potentially upping your dosage in the week before your period.)
Or your doctor may suggest you go on birth control using a synthetic version of progesterone called drospirenone, Dr. Minin says, like Yaz and Beyaz. These are FDA-approved to treat PMDD. Though experts aren’t sure why they can be so successful in this arena, it may be because drospirenone reduces a person’s response to hormonal fluctuations. It’s also a diuretic, meaning it can flush out liquids that could otherwise cause fluid retention and contribute to annoying issues like bloating.
7. You have excruciating migraines before or during your period.
If migraines had any home training, they’d at least leave you alone when you’re about to get your period. Unfortunately, period migraines are indeed a thing.
It’s not that menstruation will just randomly cause migraines in unsuspecting people who have never had one, but women with a history of migraines may experience them before or during their periods, according to the Mayo Clinic, which adds that this may be due to estrogen fluctuations. “They tend to get the headache right as they go into their periods, and it seems to get better after they have had their menses for a day or two,” Dr. Minkin says.
If you’re dealing with this, your typical migraine medication may work for you. As you probably know if you’ve grappled with migraines, the treatment options are legion. They include pain-relieving medications to relieve symptoms ASAP and preventive drugs to ward off migraines altogether, according to the Mayo Clinic. In the former camp, you have choices like anti-nausea meds and triptans, which constrict swollen blood vessels and block pain pathways in the brain. In the latter, you’ve got meds like tricylic antidepressants, which affect brain chemicals like serotonin that may be implicated in migraines.
No matter what your period problem may be, you don’t have to suffer in silence.
You have no reason to feel embarrassed about your period—or the myriad problems that can come with it. After all, celebrities are out here talking about menstruation! Some pad commercials even—gasp—use red “blood,” these days! What a time to be alive.
If you’re having period problems, see your doctor for help. If they aren’t committed to relieving your symptoms, that’s a sign you should try to find a more sympathetic medical professional who can help you find the best treatment.
On 13 March 2017, the House of Commons voted by 172 to 142 in favour of a second reading for the Reproductive Health (Access to Terminations) Bill. The bill, introduced by Diana Johnson MP, would decriminalise abortion until the end of the 24th week of pregnancy, meaning that abortion could be performed until the end of the 24th week of pregnancy without the need to satisfy any statutory grounds, or to obtain two doctors’ authorisation. Many campaigners see this bill as a first step toward the longer-term goal of fully decriminalising abortion. [1]
The prospect of decriminalisation raises a number of interesting and important issues, including an issue which has been neglected in the debates over decriminalisation so far, namely what any change in the law might mean for the right of health professionals to withdraw from participation in abortion on grounds of conscience, under section 4 of the Abortion Act 1967.
In the case of Greater Glasgow Health Board v Doogan, [2] the UK Supreme Court decided that section 4 only covered “direct” participation in the course of action which “begins with the administration of the drugs designed to induce labour and normally ends with the ending of the pregnancy by delivery of the foetus, placenta and membrane.” [3] Speculating about what “must” have been in Parliament’s contemplation at the time of the passing of the Act, the court held that there is no right to opt out of “indirect” participation (such as “delegation, supervision and support” in relation to abortion) on grounds of conscience. It also confirmed that the statutory conscience right offers no protection to general practitioners; what legal protection they have, they have under the terms of the GP contract with the NHS. Although this means that GPs conscience rights will be unaffected by any decriminalisation process, it also means that they have no statutory conscience rights at all and could be left without any protection were the terms of the GP contract to change.
There is ongoing academic debate about whether individual conscience should be accommodated at all in the healthcare context. [4] When the law does decide to provide for it, however (as it does in the case of abortion), the provision should be interpreted in a manner consistent with its purpose. The purpose of a conscience clause is to protect individuals from sharing in moral responsibility for an outcome that they regard as seriously immoral. Those who help to arrange for something to happen, or who support and facilitate it in necessary but “indirect” ways, share in the responsibility (credit or blame, depending on one’s view) for the outcome. Thus, a fit-for-purpose conscience clause must protect those who regard abortion as serious wrongdoing from participating in it indirectly (so it must cover senior midwives and GPs); restricting protection to those immediately involved defeats the purpose.
Weakened as it is by the Supreme Court’s decision, section 4 remains a vital lifeline for those whose roles it doescover. Moves to decriminalise abortion have the potential to restrict conscience rights much more severely, however. Section 4 provides that “no person shall be under any duty…to participate in any treatment authorised by this Act to which he has a conscientious objection” (my emphasis). In Doogan, the court held that “treatment authorised by this Act” means treatment “made lawful by” the Act. [5] If abortion were decriminalised, the 1967 Act would no longer be “making abortion lawful” (either at all, or until the end of the 24th week, depending on the scale of the decriminalisation), and it could be argued, following the reasoning in Doogan, that the section 4 conscience right no longer applied to recently-decriminalised abortion. If that argument succeeded, individual professionals could no longer rely on the protection of section 4 in the overwhelming majority of abortions (and perhaps even all abortions).
Influential supporters of decriminalisation, like Ann Furedi (CEO of Bpas) and Professor Sally Sheldon, have indicated their support for accommodating conscientious objection. [6,7] To ensure that any liberalisation of abortion law does not have the unintended side effect of depriving professionals of their conscience rights, it is imperative that a meaningful conscience provision be added to Johnson’s Bill if it progresses beyond the second reading, and to any subsequent bill seeking to decriminalise abortion. In my view, such a clause ought also to put GPs’ protection on a statutory footing.
Mary Neal is a senior lecturer in law at the University of Strathclyde in Glasgow, researching and teaching medical law and ethics with a particular focus on beginning and end of life issues and rights of conscientious objection. She is a current member of the BMA Medical Ethics Committee.
[4] For a range of views, see the following special issues: Bioethics (Volume 28, Issue 1, January 2014); Medical Law Review (Volume 23 Issue 2, May 2015); Cambridge Quarterly of Healthcare Ethics (Volume 26 Issue 1, January 2017); and Journal of Medical Ethics (Volume 43 Issue 4, April 2017).
[5] Greater Glasgow Health Board v Doogan [2014] UKSC 68, paragraph 38
Screening for thyroid disease should be considered in women with fertility problems and recurrent early pregnancy loss, according to a review published in The Obstetrician & Gynaecologist.
“Abnormalities in thyroid function can have an adverse effect on reproductive health and result in reduced rates of conception, increased miscarriage risk and adverse pregnancy and neonatal outcomes,” Amanda Jefferys, BMBS, BMedSci, MRCOG, of the Bristol Center for Reproductive Medicine at Southmead Hospital in the United Kingdom, said in a press release. “However, with appropriate screening and prompt management, these risks can be significantly reduced.”
Jefferys and colleagues conducted the review to gather information on the effect of thyroid disorders on reproductive health. The researchers also sought to gather information on how to optimize thyroid function in order to improve reproductive outcomes.
There can be adverse effects on reproductive health, decreased conception rates, increased early pregnancy loss, and adverse pregnancy and neonatal outcomes with abnormalities in thyroid function, including hyperthyroidism and hypothyroidism.
Compared with 1.5% of women in the general population, 2.3% with fertility problems have hyperthyroidism. Menstrual irregularity has been linked to hyperthyroidism. Preterm delivery, preeclampsia, growth restriction, heart failure and stillbirth are all possible adverse outcomes of pregnancy in women with hyperthyroidism.
Less than 1% of women of reproductive age have hypothyroidism, which can cause a delay in reaching sexual maturity during childhood and adolescence as well as menstrual problems in adulthood.
Currently, national guidelines do not recommend screening for asymptomatic women with problems conceiving.
“Thyroid disease can have significant effects on reproduction from conception to birth; however, with appropriate screening, a high index of suspicion and prompt management, risks can be significantly reduced if not ameliorated,” the researchers wrote. “The benefits of [levothyroxine] replacement in euthyroid women and with [autoimmune thyroid disease] both preconceptually and during pregnancy remain a grey area and further research is needed to confirm benefit.”
Thyroid disease can have significant effects on a woman’s reproductive health and screening for women presenting with fertility problems and recurrent early pregnancy loss should be considered, suggests a new review published today (23 January) inThe Obstetrician & Gynaecologist (TOG).
The review examines the effect of thyroid disorders on reproductive health and reviews the current evidence on how to optimise thyroid function to improve reproductive outcomes.
Thyroid hormones control the metabolism via the production of two hormones triiodothyronine and thyroxine. These hormones also have key roles in growth and development, particularly brain development. Changes in thyroid function can impact greatly on reproductive function before, during and after conception.
Thyroid disease is divided into hyperthyroidism (overactive thyroid) and hypothyroidism (underactive thyroid), and the causes of the diseases are numerous.
The review highlights that hyperthyroidism is found in approximately 2.3% of women presenting with fertility problems, compared with 1.5% of women in the general population. The condition is linked with menstrual irregularity. Hypothyroidism affects around 0.5% of women of reproductive age. Hypothyroidism in childhood and adolescence is associated with a delay in reaching sexual maturity, and in adulthood is associated with menstrual problems and in some cases a lack of ovulation, state the authors.
The authors note that thyroid disease has long been associated with fertility problems, however, national guidance does not currently recommend routine measurement of thyroid function in asymptomatic women presenting with problems conceiving.
Additionally, the authors of the review note that miscarriage is common, affecting approximately one in five pregnancies and recurrent miscarriage, defined as three consecutive miscarriages, affects 1% of couples. Given that thyroid hormone plays an important part in embryonic development, thyroid disease has long been associated with an increased risk of miscarriage.
Thyroid disease, in particular hyperthyroidism, can also have a significant effect on pregnancy, the authors of the review state. Adverse outcomes can include preterm delivery, pre-eclampsia, growth restriction, heart failure and stillbirth.
The authors conclude that screening for thyroid disease should be considered in women presenting with fertility problems and recurrent pregnancy loss. Additionally, the authors highlight that there is evidence to suggest that routine screening of the general population for thyroid dysfunction at the start of pregnancy may be beneficial.
Furthermore, women diagnosed with thyroid disease should continue on anti-thyroid medication throughout pregnancy and receive close monitoring, emphasise the authors.
Amanda Jefferys, from the Bristol Centre for Reproductive Medicine, Southmead Hospital, Bristol, and co-author of the study said:
“Abnormalities in thyroid function can have an adverse effect on reproductive health and result in reduced rates of conception, increased miscarriage risk and adverse pregnancy and neonatal outcomes.
“However, with appropriate screening and prompt management, these risks can be significantly reduced.”
Jason Waugh, TOG Editor-in-chief, added:
“Thyroid disease is common in the reproductive medicine setting, in fact, it is the most common endocrine condition affecting women of reproductive age.
“This paper highlights how thyroid disorders can affect fertility and pregnancy and makes a case for universal screening.”
It was 100 degrees out but I couldn’t stop shivering. I wore two shirts, jeans, and a heavy hoody but was still colder than I had ever been in my life.
Several months prior to the chills I started to have trouble sleeping. The urge to urinate woke me up about every two hours. I woke up about four times a night to take a piss. Each time hardly anything would actually come out.
At first I wrote it off.
Maybe I’m drinking too much water before bed, I thought. After all, I did drink tons of water throughout the day.
Then I started having problems urinating during the day. I’d whip it out to piss and then…nothing. Sometimes it’d be a full minute until I could actually get a stream going.
The pain started a few weeks later. It felt like a burning-hot screwdriver was being shoved up my phallus every time I tried to pee. There was pain even when I didn’t go to the bathroom. The sensation was as if everything beneath my stomach was crammed into a blender, torn apart, and then lit on fire. There was also pain in my sides. I don’t have quite as dramatic an explanation for that pain. If you’ve ever been punched before, imagine that but coming from the inside.
Regular visits to the gynecologist are essentially a must for a woman. While this has to suck, the upshot is that it forces them to understand their sexual health and reproductive health better than any man understands their own. It also, presumably, makes them less afraid of invasive tests since they have to endure them on a semi-regular basis. That’s why I put off going to the urologist for so long, because I was afraid of getting a tube put in my dick. Eventually, I couldn’t stand the pain and constant chills anymore, and I saw the doctor.
The doctor said I had a severe bacterial kidney infection that spread to the bladder and prostate—so basically a kidney infection, a urinary tract infection, and prostatitis.
I took the most powerful antibiotics they’re allowed to prescribe and after a while the pain went away…but the nocturia (getting up to pee a lot during the night) and the long delay before urinating. I went back to the doctor and he said the bladder muscle had become spastic and overactive as a result of the prolonged infection.
He prescribed a medicine to help me with my symptoms. I can’t remember the name, but I know it belonged to a class of medicines calledAlpha Blockers.
“One thing about this medicine,” the doctor said as he typed the prescription into the computer. “There’s a chance it can cause retrograde ejaculation.”
“Um…what?” I asked. I obviously knew what ejaculation meant but “retrograde” could’ve meant anything.
“Dry orgasms. No seminal fluid,” he said. In more specific terms, retrograde ejaculation is when semen gets sent into the bladder rather than out into a sock, condom, or, if you’re lucky, a crevasse belonging to your significant other.
I was weirded out but he said there was only a chance, right? So that meant there was a chance it didn’t cause retrograde ejaculation.
This pathetic bit of self delusion lasted until my first jerk-off session on the medicine. I felt the familiar build-up of pleasure and tension (I call it plension) and then… nothing. Not only was there no semen, there was no electric rush, no hip-bucking, and no release.
After about a month of this, I asked to switch to a different medicine. As far as I knew, that’d be the last time I’d ever have to think or hear about dry orgasms and retrograde ejaculation.
I was wrong.
Male birth control is swift becoming a highly discussed issue among social justice circles and the Internet in general.
One proposed method of male birth control is the use of alpha blockers to intentionally cause dry orgasms. Another, more recently publicizedstrategy is using gel to block the vas deferens—the tube sperm travels through—thereby preventing sperm from ever coming out of the penis (forgive the pun). The latter product could be available in three years.
The Daily Beast’s Samantha Allen, who is also a frequent contributor at the Daily Dot, noted that male birth control could have a multitude of wondrous impacts on society, and would greatly aid women since they would no longer be subject to the deleterious affects of The Pill.
Allen’s interpretation of the facts is accurate, but it paints too rosy a picture. The coming wave of male birth control will make conversations about reproductive health more vitriolic and hateful, not less.
First, insertion of gel into the vas deferens is an invasive procedure—far more invasive than popping a pill every day. A significant percentage of America’s 150 million-plus men will not go for it no matter how economical it is or how beneficial to society it is. American culture is too patriarchal and while #NotAllMen are this selfish, most are.
The bigger concern, however, isn’t the procedure but the dry orgasm.
“Dry orgasm” is a misnomer. Yeah it’s dry, but calling it an orgasm is just wrong. My dry “orgasms” felt like being 12 again—old enough to get a boner looking at porn illegally downloaded from Napster but not actually old enough for your member to spew forth any precious fluids.
I’m not alone in realizing that dry orgasms remove pleasure from sex. Astudy performed in 2009 found that “a strong decline in ejaculatory volume is associated with reduced sexual pleasure” when they gave men alpha blockers. The study noted the men were “greatly dissatisfied with the ejaculatory dysfunction” from the alpha blockers.
I lost all sex drive almost immediately once I started having dry orgasms. I didn’t even respond to a “booty call” I got while I was on the alpha blockers because I just didn’t care. What was the point of having sex if I knew I was incapable of enjoying it?
Cynics and jokesters would say “Well, if male birth control reduces libido then mission accomplished: No kids!”
Birth control isn’t just a preventative measure; it enables people to fully enjoy sex while avoiding the grave biological and financial consequences of sex. Male birth control, however, prevents pleasure as well as pregnancy.
Look, I’m not a men’s rights activist. I’m not trying to say women should be subjugated and forced to take the pill for as long as they live. I’m just saying that male birth control is highly imperfect. If you’re expecting it to take the world by storm in 2017, don’t. Once the first crop of men feel what a dry orgasm is like, it’ll start a new culture war. Imagine the GIF vs. JIF debate, but 10,000 times worse because it’ll be filled with more hate and it’ll be an issue that actually matters.
I guarantee you there will be a contingent of men comparing male birth control to female circumcision in that it robs both groups of pleasure. The web will be inundated with articles just like this one explaining just how awful male birth control is for men’s sexual health. And maybe we don’t deserve sexual health for all the atrocities we’ve committed against females, but good luck convincing America of that.
This birth control innovation isn’t a solution, it’s 150 million problems waiting to happen.
The researchers say the new type of imaging – which tracks the movement of water in the brain – will enable them to explore how the disruption of key processes might cause conditions such as autism.
It could also be used to monitor possible treatments to prevent brain damage.
Interrupted development
The scans showed cortical development was reduced in the preterm babies compared with those born at full term, with the greatest effect in the most premature infants – those born at about 27 weeks.
The brain regions affected govern social and emotional processing, as well as memory.
The same children were assessed at two years of age and those who had been born prematurely performed less well on neurodevelopmental tests, which the researchers say suggests the weeks a baby loses in the womb may matter.
Lead investigator Prof David Edwards said: “The number of babies born prematurely is increasing, so it has never been more important to improve our understanding of how preterm birth affects brain development and causes brain damage.
“We know that prematurity is extremely stressful for an infant, but by using a new technique we are able to track brain maturation in babies to pinpoint the exact processes that might be affected by premature birth.”
Andy Cole, chief executive of the premature baby charity Bliss, said: “It is very exciting that this ground-breaking research is being driven forward here in the UK.
“A better understanding of the way that preterm babies’ brains develop is an important step for doctors to help identify improvements in care that will benefit the 60,000 preterm children born every year.
“It is important to mention that most premature babies are unaffected by their early arrival and families of these babies should not be unduly concerned.”
The treatment of hyperthyroidism during pregnancy with both methimazole/carbimazole and propylthiouracil was linked to birth defects, but the type of malformations differed, according to recent study findings.
The prevalence of birth defects was greater among children exposed to antithyroid drugsduring early pregnancy (propylthiouracil, 8%; methimazole/carbimazole, 9.1%; methimazole/carbimazole and propylthiouracil, 10.1%;P<.001), according to data. Researchers did not see an increased risk for birth defects in infants born to mothers treated with antithyroid drugs before or after pregnancy (no antithyroid drugs, 5.4%; nonexposed, 5.7%;P<.001).
“It is imperative to treat overt hyperthyroidism in pregnant women, but the use of [antithyroid drugs] in early pregnancy should be limited when possible,” the researchers said. “For the present, it may be optimal to shift women planning pregnancy from [methimazole/carbimazole] to [propylthiouracil] before pregnancy.”
The researchers used the Danish nationwide register-based cohort study, including 817,093 children live-born from 1996 to 2008 to determine how the use of antithyroid drugs used in early pregnancyincreased the prevalence of birth defects.
Patients were assigned to the following groups:
Propylthiouracil (n=564);
Methimazole/carbimazole (n=1,097);
Methimazole/carbimazole and propylthiouracil (n=159);
No antithyroid drugs during pregnancy, but taken before or after pregnancy (n=3,543); and
Nonexposed females (n=811,730).
Data indicate that mothers who were assigned both methimazole/carbimazole (adjusted OR=1.66; 95% CI 1.35-2.04) and propylthiouracil(OR=1.41; 95% CI, 1.03-1.92) with maternal shift between methimazole/carbimazole and propylthiouracil during early pregnancy (OR=1.82; 95% CI, 1.08-3.07) demonstrated an increased prevalence of birth defects, researchers wrote.
In particular, methimazole/carbimazole and propylthiouracil were associated with urinary system malformation, and propylthiouracil with malformations in the face and neck region.
Moreover, choanal atresia, esophageal atresia, omphalocele, omphalomesenteric duct anomalies and aplasia cutis were common in methimazole/carbimazole-exposed children (combined, adjusted OR=21.8; 95% CI, 13.4-35.4), according to data.
Further studies are warranted to confirm these results, researchers wrote.
PERSPECTIVE
There is concern over whether carbimazole/methimazole or propylthiouracil is the most appropriate antithyroid drug to use when treating hyperthyroidism in pregnant women. Traditionally, propylthiouracil has been preferred, as it was felt to be associated with a lower risk for congenital abnormalities. However, concerns regarding propylthiouracil use have arisen owing to the rare complication of propylthiouracil-induced hepatitis in pregnancy, which can have catastrophic consequences.
This study is very important, as it substantially adds to our current knowledge of birth defects associated with antithyroid drug exposure for carbimazole/methimazole and propylthiouracil. This study crucially highlighted that both carbimazole/methimazole and propylthiouracil were associated with an increased risk for birth defects. However the birth defects associated with propylthiouracil may be less common and severe than those associated with carbimazole/methimazole. Of particular note was that, in the small number of women who switched from carbimazole/methimazole to propylthiouracil during the first trimester, there was no obvious amelioration in the risk for birth defects. This implies switching to propylthiouracil during the first trimester may be too late to prevent carbimazole/methimazole-associated abnormalities. This would support the argument that in women considering pregnancy, propylthiouracil should be used instead of carbimazole/methimazole, as swapping in the first trimester may be too late. However, further studies are needed.
The use of robust national registry data provided the very large population required to identify rare but clinically important outcomes and also protected against differential recall of exposure between carbimazole/methimazole and propylthiouracil-treated pregnancies. This is a particular strength as traditional reporting methods may be biased by clinicians’ preconceptions regarding these antithyroid drugs.
Peter N. Taylor, MRCP
Welsh clinical academic trainee in diabetes and endocrinology
Thyroid Research Group
Institute of Molecular and Experimental Medicine
Cardiff University School of Medicine
John Amory, a doctor at the University of Washington, has been developing a male contraceptive for 15 years. Turns out, it’s harder than it sounds. We spoke with him to find out why.
PopSci: Why is it taking so long to produce a birth-control pill for men?
John Amory:Women make one egg a month, but men make 1,000 sperm every second of every day, from puberty until the day they die. Turning that off is difficult.
JA:If you give a man enough testosterone, the brain will shut down the secretion of gonadotropins, which are the hormones that signal the testes to make sperm. This is why most bodybuilders are infertile, by the way. But it doesn’t work in all men.
PS: How many men does testosterone work for?
JA:We have never been able to get more than 95 percent effectiveness. It’s possible to identify who testosterone won’t work for, but it involves getting a lot of sperm counts. It would be much nicer if you could just say, “Take this and it will work.” Women don’t have to undergo ovulation detections and testing to see if the Pill is going to work for them.
PS: The World Health Organization funded a study across eight countries for hormone-based contraception, but last year, it shut down the study early. What happened?
JA:There were side effects, including severe depression. Some men don’t take hormonal shifts very well.
PS: What other approaches might work?
JA:Sperm have a pretty daunting mission. There’s a lot that can go wrong. Researchers have injected monkeys with eppin, a protein that coats sperm so they can’t swim. There’s also the process by which sperm make energy. If you can block that, you’d get tired sperm. Also, the testes need vitamin A to produce sperm, and there’s an enzyme that converts vitamin A to its active metabolite, retinoic acid. No retinoic acid, no sperm. I’m developing drug inhibitors that stop retinoic-acid production in the testes. I’m hopeful that we’ll have something approved in five years.
PS: Do you expect much demand for the male pill?
JA:Yes. Men are interested in having sex. Most of the time they’re not as interested in fathering a pregnancy.