Primary series and booster dose model fit results. (A) Example individual model fits for the primary series (blue) and booster dose (orange) Anti-S trajectory data. Dashed lines for D1, D2, and D3 indicate timing of dose 1, dose 2, and dose 3, respectively. (B) Distribution of all individual half lives for primary series (blue) and booster dose (orange). (C) Individual Anti-S half life as a function of chronological age for primary series and booster dose, where a decreasing trend as a function of increased age is found. (D) Violin plots of Anti-S half lives and number of chronic morbidities. Points are plotted with a jitter function to display the density of individuals with each chronic morbidity count. (E) Parametric plot of chronic morbidity count and chronological age, where the size of each point corresponds to the number of data points at a given age with the same chronic morbidity count. The number of individuals within each chronic morbidity category are shown to the right of the plot. Credit: Scientific Reports (2024). DOI: 10.1038/s41598-024-58811-3
Thinking about getting a spring-time booster shot? A new study coming out of York University’s Centre for Disease Modelling in the Faculty of Science shows that immunity after a COVID-19 booster lasts much longer than the primary series alone. These findings are among other—sometimes “unintuitive”—revelations of how factors like age, sex and comorbidities do and don’t affect immune response.
The work is published in the journal Scientific Reports.
The study’s authors—York Post Doctoral researchers Chapin Korosec and David Dick, Applied Mathematics Professor Iain Moyles and Professor James Watmough with the University of New Brunswick—used health data submitted to the COVID Immunity Task-Force project for more than 150 individuals who received either Pfizer-BioNTech or Moderna COVID-19 vaccines to look at how immunity holds up over time.
“Our approach as mathematicians is to create mathematical models of the immune system, and then calibrate those models to health care data in order to advance our understanding of the human immune system. It was really interesting to see the SARS-CoV-2 booster dose have such a huge increase in protective longevity capacity as compared to the primary series of two doses,” says Korosec, the study’s lead author.
The study used Canadian vaccine data collected from individuals living in long-term care, as well as frontline health-care workers working in long-term care and hospitals.
Looking at the group as a whole, the median length for the antibody half-life immune response was 63 days for the primary series, and increased to 115 days for those who went on to receive their boosters, a statistically significant finding, says Korosec.
It is well-established that age can affect how adept the body is at priming an immune response after vaccines, so much so that advanced age is considered a comorbidity itself, says Korosec.
“Chronological age is your time since birth. But you also have an immunological age, which is correlated to your chronological age, and is related to how your body loses its ability to prime against invading pathogens and produce antibodies as time marches on,” explains Korosec. “What’s convoluted is that as we age chronologically, the probability that we accrue diseases that can affect the immune system in unintuitive ways also increases.”
Looking into this aspect, the researchers found that older adults did have a less long-lasting immune response, but once they controlled for other comorbidities such as hypertension, lung disease and cancer, age no longer had as significant of an influence on the immune response.
Other interesting findings include a small, but statistically significant immune response for males versus females, and people with asthma having a longer lasting immune response—more durable, in fact, than those with hybrid immunity from vaccines and contracting COVID-19.
“We found that some outcomes were surprising and worth further study, but of course we’re not advocating any particular comorbidity is beneficial,” says Dick. “We don’t have any information from this study on how asthma would affect the severity of the COVID-19 illness, for example.”
Outside of the strict findings, the researchers also say the study points to the importance of interdisciplinary research and are excited about the possibilities for collaboration, with plans to open York’s medical school in 2028.
“While we’re all from math and stats departments, the data comes from clinicians who went through medical school and are now professors studying immunology, and I think this study shows how people with different skill sets can come together and do really interesting science,” says Korosec.
Moyles adds, “We have a really top applied math program at York, and now the university has announced a medical school. Imagine these clinicians were at York and we had access to the data on the ground floor. This would cut the research timeline by years and has huge potential for future interdisciplinary research at the university.”
DNA within the core of our cells is vulnerable to harmful insults. Many people are unaware that our DNA may be altered by a COVID-19 infection or vaccination.
Since the COVID-19 pandemic, we’ve seen an increase in mortality from cancer in the United States, England, and Wales. China has also reported clusters of blood cancer cases.
Multiple factors lie behind this trend in cancer, and DNA impairment appears to be one of them.
The World Health Organization and many other authorities have repeatedly stated that the COVID-19 vaccine is safe and cannot alter human DNA. But is this true?
SARS-CoV-2 May Alter Our DNA
Many scientists believe that the mRNA vaccine cannot alter human genes because of a theory called the central dogma of molecular biology, which was introduced by Francis Crick in 1958. In short, genetic information flows from DNA to RNA to protein. An exception would be a retrovirus harboring “reverse transcriptase” which can transform the mRNA into DNA, or the genome of human cells.
Because SARS-CoV-2 is not a retrovirus, this was not a concern in 2020.
However, there are exceptions beyond the central dogma. After all, science makes progress by challenging ideas that may no longer be relevant.
A 2009 paper in Science and a 2014 Nature article have shown that nonretroviral RNA viruses can be reverse-transcribed into DNA. Subsequently, DNA copies of the RNA viral sequences have been shown to be integrated into human DNA
A May 2021 Massachusetts Institute of Technology study published in PNAS further changed people’s perceptions.
After infecting human kidney cells with the virus, researchers found SARS-CoV-2 gene sequences integrated into the human genome.The Human Genome Project discovered that only about 2 percent of our DNA encodes for proteins, which inturn determines the structure and function of all cells. The other 98 percent of so called “dark matter” is thought to be nonfunctional. However, hidden in this noncoding DNA are numerous regulatory elements that may have a significant impact on the function of thousands of genes. These elements appear to be critical in the development of diseases such as cancer, heart disease, and autism.
Intriguingly, the SARS-CoV-2 virus is preferentially integrated into the translatable areas of genes. The integration does not appear to be random and could lead to serious consequences.
A few studies indicate a link between COVID-19 and an increased incidence of cancer—especially blood cancer, which is highly related to gene alteration.
In July 2021, a clinical case report from Iran showed that a 61-year-old man who had recovered from COVID-19 infection 40 days previous was newly diagnosed with acute myeloid leukemia. The researchers suggested a “concerning probable association” between the COVID-19 infection and the onset of the patient’s acute blood cancer.
In 2023, an Eastern European patient suffered from chronic myeloid leukemia three months after recovering from COVID-19, followed by a diagnosis of two melanomas and one skin cancer within two years. The authors deemed it essential to consider the impact of COVID-19 and the increased incidence of malignancies.
A 2023 systematic review analyzed the potential risk factors associated with COVID-19 on cancer development. This included its effect on immune function, inflammation, stress, awakening of dormant cancer cells, the possible viral integration into the human genome, changes in gene activity, and gene mutations.
COVID-19 Vaccine May Alter Our DNA
COVID-19 infects nearly 10 percent of the total global population. However, the COVID-19 vaccine has been administered to about two-thirds of people on Earth.
In February 2022, a study conducted at Lund University in Sweden and published in Current Issues in Molecular Biology showed that mRNA vaccines can integrate into human genes or DNA through reverse transcription.
Six, 24, and 48 hours after the Pfizer/BioNTech COVID-19 mRNA vaccine was added to the liver cancer cell line (Huh7), the corresponding COVID-19 vaccine DNA segments were detected in the liver cells’ DNA.
How did mRNA make its way into the human genome? The researchers found that the mRNA elevated a mechanism called the human cellular endogenous reverse transcriptive mechanism (termed as LINE-1).
It is fully recognized that the liver cancer cell line used by the researchers is not the same as normal human non-dividing cells, and displays a highly active cell proliferation. However, cell proliferation, which involves cell growth, division, differentiation, and death, is also active in several human tissues, such as blood-generating cells in the bone marrow.
Genetic researcher Kevin McKernan also recently found that the COVID-19 mRNA vaccines can potentially be reverse-transcribed into DNA and then integrated into the DNA of two human cancer cell lines—the breast and the ovaries, as reported by The Epoch Times.
In 2021, American pathologist Dr. Ryan Cole, who normally diagnoses cancer via microscopic slides, discovered a disturbing increase in certain cancer cases during the COVID-19 vaccine era. At that time, he attributed this to the possibility that vaccine components may alter natural immunity.
A surge in the number of blood cancer cases has also been reported in China after the COVID-19 vaccine era. Most blood cancer originates in the bone marrow when our blood stem cells, which are susceptible to DNA damage, have been injured.
Most Chinese people have been injected with the inactivated vaccine, which involves growing the virus in large quantities, inactivating or killing it using physical or chemical means, and using the killed mixture to inject people.
There is concern that the inactivation technique is not well controlled and that vaccine quality is not guaranteed in China. It’s important to consider this possibility.
According to Pfizer’s tissue distribution studies, the mRNA vaccine components were found to accumulate in organs such as the bone marrow 24 hours after injection.
Spike Protein May Lead to Fragile DNA
Additionally, spike protein has been shown to hinder the function of DNA self-repair.
Many things can damage our DNA, including exposure to an excessive amount of radiation or toxic chemicals, although DNA does have the ability to repair itself.
As early as October 2021, Swedish scientists found that the COVID-19 virus spike protein can impair two human cell DNA self-repair mechanisms, the non-homologous end joining (NHEJ) and homologous recombination (HR).
The NHEJ repair mechanism is critical for fixing significant breaks in DNA. It is also essential for immune cells to recognize and target changing variants, and loss of this function can result in immune deficiencies.
According to this research, when the COVID-19 spike protein challenges the cellular DNA, it can open the door to external genetic material, such as allowing DNA from the vaccine to sneak into the human genome.
It appears that the Swedish paper has been retracted once again for unknown reasons. However, given the enormous implications and the highly sensitive nature of this topic, scientists have an ethical responsibility to thoroughly investigate any evidence of a potential impact on the human genome caused by the COVID-19 vaccine.
COVID-19 Vaccine May Alter Our Natural Immunity
While the mRNA vaccinations introduce highly modified genetic material into the body, they have also been shown to downregulate critical self-protective mechanisms related to cancer surveillance.
Our natural immunity is the most powerful surveillance system we have against cancer cells.
An MIT paper by Seneff and her colleagues found that COVID-19 mRNA vaccination induces a substantially impaired type I interferon—a major anti-virus, anti-cancer substance in our body—resulting in an increased risk of cancer.
Type 1 interferon can induce cancer cell death and make cancer visible to our immune system.
Type I interferons have downstream effects that can suppress tumors, notably through other related genes and pathways. These subsequent processes have an impact on controlling cancer development, including breast, prostate, uterus, ovaries, and pancreatic cancers. However, the companion genes and pathways generally appear dysregulated by the mRNA vaccines.
Furthermore, vaccines not only injure our natural immune defense against cancer, but also alter our natural defense against viruses.
Scientific research has shown that the immune response elicited by an infection with SARS-CoV-2 significantly differs from that produced by an mRNA vaccine.
In COVID-19 patients with natural infection, peripheral blood dendritic cells showed a substantial increase in antiviral interferon response, as indicated by gene expression analysis. However, this crucial antiviral response is almost absent in vaccine recipients.
An Uptick in Cancer Incidence
The Vaccine Adverse Event Reporting System (VAERS) showed a significant increase in new cancers following the COVID-19 vaccines, accounting for 98 percent of cancers reported in VAERS in the last 30 years.
Reports indicate that mortality rates have increased over the last three years, with a 3.3 percent excess in 2020, 7.9 percent in 2021, and 9.8 percent in 2022. All these figures are statistically significant.
In another study of 15- to 44-year-olds in England and Wales, researchers observed a major increase in all-cause mortality from 2020 to 2022 and in cancer-associated mortality that began in 2021 and “accelerated substantially” in 2022.
Several common reasons may account for the increase in cancer-related deaths in the United States, England, and Wales.
Factors such as stress, anxiety, depression and isolation can affect cancer screening and treatment, cause a decrease exercise, and an increase drug abuse.
However, COVID-19 infection and vaccines are significant factors that cannot be ignored.
Any respectable scientist who wants to develop safe and effective drugs would seriously investigate this topic without interference from the media or pharmaceutical companies.
While the issue of problematic pharmaceuticals is undoubtedly concerning, the greater threat lies in the deteriorating ethics of our society.
The COVID-19 vaccines may weaken our ability to fight viruses at the cellular level.
Many people may be aware that neutralizing antibodies significantly wane after only a few months following COVID-19 vaccination. Newly emerging subvariants have developed a solid ability to escape from neutralizing antibodies.
However, another significant facet of the COVID-19 vaccine is that it can damage our cellular immunity, especially T-cell immunity. Cellular immunity, or cell-mediated immunity, does not involve antibodies and is pivotal in preventing the severe form of COVID-19. Recent evidence shows that after a fifth vaccine booster dose, cellular immunity waned as well.
Fifth Dose Fails to Strengthen Cell Immunity
A study, published in Frontier Immunology looked at the long-term impact of the COVID-19 mRNA vaccine on cellular immunity.
The immune responses of 61 subjects who received five doses of the vaccine were tracked from 2021 to 2023. The first four doses were the Pfizer monovalent mRNA vaccine, and the fifth dose was the Pfizer-BioNTech bivalent vaccine (Comirnaty Bivalent Original/Omicron BA.4/5).
All subjects were on hemodialysis and at high risk for severe COVID-19. The average age was 70 years. About 90 percent (55), had high blood pressure, almost half (30) had diabetes, and a smaller group of about 11.5 percent (7), had dyslipidemia, which is an abnormal amount of lipids in the blood. For their third vaccine dose, 26.2 percent of the participants (16) received a different type of vaccine booster, specifically Moderna (mRNA-1273).
The study found that while most patients maintained a strong antibody response (humoral immunity), their immune cell-based defense, as measured by interferon production T-cell immunity, weakened in many cases. After the fifth vaccine dose, only half of the patients maintained strong cellular immunity. Older participants, those aged 70 and above, were more likely to have a slightly weaker cellular immune response.
The proportion of vaccinated people who acquired cellular immunity was 75.4 percent at 10 months post-first dose, with a slight increase to 87.5 percent one month following the fourth dose; however, after the fifth dose, cellular immunity decreased significantly from 58.6 percent at one month to 50 percent at three months.
This finding aligns with a previous mouse study, which showed a decrease in T helper and killer cell activity and an increase in suppressive T cells after the fifth and sixth mRNA vaccine doses, suggesting evidence of immune tolerance and exhaustion.
The study confirmed that protective immune memories were overturned by extended booster vaccination by promoting adaptive immune tolerance. “We found that the protective effects from the humoral immunity and cellular immunity established by the conventional immunization were both profoundly impaired during the extended vaccination course. Specifically, extended vaccination not only fully impaired the amount and the neutralizing efficacy of serum RBD-specific antibodies, but also shortened the long-term humoral memory,” the researchers concluded.
This finding highlights the potential risks associated with continued use of SARS-CoV-2 boosters.
So, what are these immune cells doing? Why do these findings matter?
Importance of Cellular Immunity
Our immune system is composed of natural immunity and adaptive immunity. Natural immunity is the body’s inborn ability to fight off broad-spectrum infections, regardless of the specific type of virus, while adaptive immunity is the body’s second line of defense against particular invaders.
Adaptive immunity is executed by specialized immune cells that respond to specific viruses. These include lymphocytes—white blood cells such as T cells, B cells, and natural killer cells.
Our B cells are like “antibody factories” and are responsible for producing virus-specific antibodies to neutralize a virus.
T cells are a diverse group with several roles. Some act like team leaders, helping other cells do their jobs and coordinating the entire immune response; these are known as “T helper cells.” There are also “cytotoxic T cells,” known as “killer T cells,“ which specialize in destroying infected cells. Additionally, there are ”regulatory T cells,” which help regulate the immune system response by suppressing the actions of other cells.
Studies have found that new variants of SARS-CoV-2 can dodge the immune response created by mRNA vaccines, but they can’t escape T-cell-associated defense.
Interferon: A Powerful Antiviral Weapon
Cellular immunity is part of adaptive immunity that responds via T cells and B cells, etc., and mucosal immunity is part of our innate immunity (e.g., the skin and nose). Both types of immunity use interferon as a potent antiviral weapon to fight against a virus.
In mucosal immunity, when our body is confronted with a virus at the epithelial layer (surface layer of the mucosa), the epithelial cells can produce interferon, helping the cells enter an antiviral state to eradicate the virus effectively before it spreads deeply into our body. When interferon is produced naturally via our mucosa, it’s the most effective way our body eradicates a virus at the frontline. This is not possible with commonly used injected vaccinations.
In cellular immunity, interferons also act as a powerful secret weapon and play a pivotal role in antiviral immunity by eradicating pathogens.
Interferon can be reproduced by killer T cells and natural killer cells during viral infection to maximize its antiviral effects. This early and rapid increase of killer T-cell activity may explain why some people don’t experience symptoms of COVID-19 infection.
A 2023 study found that those who experienced infection had significantly lower levels of interferons compared to uninfected participants. Furthermore, participants with a significantly higher level of cellular immunity were less likely to develop breakthrough infections after vaccination.
A study published in Cell Reports shows that during the early stages of a COVID-19 infection, if a person can quickly generate SARS-CoV-2- specific T cells or interferon-producing T cells, the body can get rid of the virus faster, resulting in a less severe case of COVID-19.
The researchers analyzed the virological and immunological changes in 12 patients with acute SARS-CoV-2 infection from disease onset through recovery or death and found that patients with only mild symptoms had an early induction of interferon-gamma-secreting SARS-CoV-2-specific T cells.
mRNA Vaccines Weaken Cellular Immunity
Some may wonder how COVID-19 mRNA vaccines can suppress our cellular immunity. Here are some plausible explanations.
Spike Protein
COVID-19 vaccines bypass our body’s mucosal and vascular barriers when injected into the deltoid muscle. How our immunity responds to a vaccine will determine the impact of the vaccination.
The spike protein in mRNA vaccines is known to dysregulate our normal antiviral immunity. A study found that at 28 days after vaccination, spike protein caused consistent alteration of gene expression in peripheral immune cells, resulting in impaired interferon responses and suppressed cellular immunity, including lymphocyte and monocyte suppression.
The spike protein from the vaccine doesn’t break down quickly and can circulate in the body for over four months, which can negatively impact our immunity.
Modified mRNA
The mRNA vaccines use a slightly altered genetic code, which includes something called N1-methylpseudouridine instead of the usual uracil. This change has been found to cause regulatory T cells to activate in a way that suppresses cellular immunity.
These modified mRNA particles go to specific cells in the spleen responsible for presenting antigens without triggering necessary co-stimulatory immune responses. This will cause a decrease in the number of functioning T cells and an increase in regulatory T cells, resulting in impaired cellular immunity.
Lipid Nanoparticles
The vaccine’s ingredients include lipid nanoparticles (LNPs), tiny fat-like particles that can gather in various organs like the liver and the spleen. These LNPs, along with the mRNA they carry, can cause further inflammation, resulting in dysregulated cellular immunity.
Blood Vessel Injury
The antibodies our bodies produce in response to the vaccine’s spike protein might accidentally harm cells and tissues creating spike proteins. This includes damage to the endothelial cells, which line our blood vessels and could potentially harm organs vital to our immunity, like the adrenal gland.
Antibody-Dependent Enhancement and Immune Imprint
Another possibility known as antibody-dependent enhancement, can wreak havoc on the normal function of cellular immunity.
This could occur when the immune system’s memory of the original Wuhan-type vaccine interferes with its ability to fight off new variants, making the vaccine ineffective against these variants, potentially strengthening the COVID-19 virus’s ability to replicate.
New Variants Escape T-cell Immunity
Starting from Omicron emergence, this SARS-CoV-2 variant family has learned to escape from B cell immunity with vastly increased infectivity and immune escape from spike protein-induced antibodies. Recent variants (e.g., JN.1) have learned to mutate in the non-spike regions to escape original T-cell immunity. This could make it more challenging for our original cellular immunity to eradicate an Omicron variant.
In summary, the extensive promotion of the COVID-19 vaccine has had significant long-term negative consequences, necessitating a thorough and objective reassessment of whether we should continue to encourage vaccination among the population. Relying solely on blind faith or irrational beliefs in this context can be counterproductive and potentially harmful. Health authorities and public officials have been calling for a complete discontinuation of all mRNA vaccines.
It’s also crucial to highlight the value of non-pharmacological preventive measures and primary health education about our immune system’s role in combating viruses. There are numerous ways to holistically boost our endowed immunity based on modern biomedical research. Such knowledge is essential and should be given due attention by health authorities. This approach empowers individuals with vital information and should be a part of a comprehensive public health strategy.
The COVID-19 vaccines may weaken our ability to fight viruses at the cellular level.
Many people may be aware that neutralizing antibodies significantly wane after only a few months following COVID-19 vaccination. Newly emerging subvariants have developed a solid ability to escape from neutralizing antibodies.
However, another significant facet of the COVID-19 vaccine is that it can damage our cellular immunity, especially T-cell immunity. Cellular immunity, or cell-mediated immunity, does not involve antibodies and is pivotal in preventing the severe form of COVID-19. Recent evidence shows that after a fifth vaccine booster dose, cellular immunity waned as well.
Fifth Dose Fails to Strengthen Cell Immunity
A study, published in Frontier Immunology looked at the long-term impact of the COVID-19 mRNA vaccine on cellular immunity.
The immune responses of 61 subjects who received five doses of the vaccine were tracked from 2021 to 2023. The first four doses were the Pfizer monovalent mRNA vaccine, and the fifth dose was the Pfizer-BioNTech bivalent vaccine (Comirnaty Bivalent Original/Omicron BA.4/5).
All subjects were on hemodialysis and at high risk for severe COVID-19. The average age was 70 years. About 90 percent (55), had high blood pressure, almost half (30) had diabetes, and a smaller group of about 11.5 percent (7), had dyslipidemia, which is an abnormal amount of lipids in the blood. For their third vaccine dose, 26.2 percent of the participants (16) received a different type of vaccine booster, specifically Moderna (mRNA-1273).
The study found that while most patients maintained a strong antibody response (humoral immunity), their immune cell-based defense, as measured by interferon production T-cell immunity, weakened in many cases. After the fifth vaccine dose, only half of the patients maintained strong cellular immunity. Older participants, those aged 70 and above, were more likely to have a slightly weaker cellular immune response.
The proportion of vaccinated people who acquired cellular immunity was 75.4 percent at 10 months post-first dose, with a slight increase to 87.5 percent one month following the fourth dose; however, after the fifth dose, cellular immunity decreased significantly from 58.6 percent at one month to 50 percent at three months.
This finding aligns with a previous mouse study, which showed a decrease in T helper and killer cell activity and an increase in suppressive T cells after the fifth and sixth mRNA vaccine doses, suggesting evidence of immune tolerance and exhaustion.
The study confirmed that protective immune memories were overturned by extended booster vaccination by promoting adaptive immune tolerance. “We found that the protective effects from the humoral immunity and cellular immunity established by the conventional immunization were both profoundly impaired during the extended vaccination course. Specifically, extended vaccination not only fully impaired the amount and the neutralizing efficacy of serum RBD-specific antibodies, but also shortened the long-term humoral memory,” the researchers concluded.
This finding highlights the potential risks associated with continued use of SARS-CoV-2 boosters.
So, what are these immune cells doing? Why do these findings matter?
Importance of Cellular Immunity
Our immune system is composed of natural immunity and adaptive immunity. Natural immunity is the body’s inborn ability to fight off broad-spectrum infections, regardless of the specific type of virus, while adaptive immunity is the body’s second line of defense against particular invaders.
Adaptive immunity is executed by specialized immune cells that respond to specific viruses. These include lymphocytes—white blood cells such as T cells, B cells, and natural killer cells.
Our B cells are like “antibody factories” and are responsible for producing virus-specific antibodies to neutralize a virus.
T cells are a diverse group with several roles. Some act like team leaders, helping other cells do their jobs and coordinating the entire immune response; these are known as “T helper cells.” There are also “cytotoxic T cells,” known as “killer T cells,“ which specialize in destroying infected cells. Additionally, there are ”regulatory T cells,” which help regulate the immune system response by suppressing the actions of other cells.
Studies have found that new variants of SARS-CoV-2 can dodge the immune response created by mRNA vaccines, but they can’t escape T-cell-associated defense.
Interferon: A Powerful Antiviral Weapon
Cellular immunity is part of adaptive immunity that responds via T cells and B cells, etc., and mucosal immunity is part of our innate immunity (e.g., the skin and nose). Both types of immunity use interferon as a potent antiviral weapon to fight against a virus.
In mucosal immunity, when our body is confronted with a virus at the epithelial layer (surface layer of the mucosa), the epithelial cells can produce interferon, helping the cells enter an antiviral state to eradicate the virus effectively before it spreads deeply into our body. When interferon is produced naturally via our mucosa, it’s the most effective way our body eradicates a virus at the frontline. This is not possible with commonly used injected vaccinations.
In cellular immunity, interferons also act as a powerful secret weapon and play a pivotal role in antiviral immunity by eradicating pathogens.
Interferon can be reproduced by killer T cells and natural killer cells during viral infection to maximize its antiviral effects. This early and rapid increase of killer T-cell activity may explain why some people don’t experience symptoms of COVID-19 infection.
A 2023 study found that those who experienced infection had significantly lower levels of interferons compared to uninfected participants. Furthermore, participants with a significantly higher level of cellular immunity were less likely to develop breakthrough infections after vaccination.
A study published in Cell Reports shows that during the early stages of a COVID-19 infection, if a person can quickly generate SARS-CoV-2- specific T cells or interferon-producing T cells, the body can get rid of the virus faster, resulting in a less severe case of COVID-19.
The researchers analyzed the virological and immunological changes in 12 patients with acute SARS-CoV-2 infection from disease onset through recovery or death and found that patients with only mild symptoms had an early induction of interferon-gamma-secreting SARS-CoV-2-specific T cells.
mRNA Vaccines Weaken Cellular Immunity
Some may wonder how COVID-19 mRNA vaccines can suppress our cellular immunity. Here are some plausible explanations.
Spike Protein
COVID-19 vaccines bypass our body’s mucosal and vascular barriers when injected into the deltoid muscle. How our immunity responds to a vaccine will determine the impact of the vaccination.
The spike protein in mRNA vaccines is known to dysregulate our normal antiviral immunity. A study found that at 28 days after vaccination, spike protein caused consistent alteration of gene expression in peripheral immune cells, resulting in impaired interferon responses and suppressed cellular immunity, including lymphocyte and monocyte suppression.
The spike protein from the vaccine doesn’t break down quickly and can circulate in the body for over four months, which can negatively impact our immunity.
Modified mRNA
The mRNA vaccines use a slightly altered genetic code, which includes something called N1-methylpseudouridine instead of the usual uracil. This change has been found to cause regulatory T cells to activate in a way that suppresses cellular immunity.
These modified mRNA particles go to specific cells in the spleen responsible for presenting antigens without triggering necessary co-stimulatory immune responses. This will cause a decrease in the number of functioning T cells and an increase in regulatory T cells, resulting in impaired cellular immunity.
Lipid Nanoparticles
The vaccine’s ingredients include lipid nanoparticles (LNPs), tiny fat-like particles that can gather in various organs like the liver and the spleen. These LNPs, along with the mRNA they carry, can cause further inflammation, resulting in dysregulated cellular immunity.
Blood Vessel Injury
The antibodies our bodies produce in response to the vaccine’s spike protein might accidentally harm cells and tissues creating spike proteins. This includes damage to the endothelial cells, which line our blood vessels and could potentially harm organs vital to our immunity, like the adrenal gland.
Antibody-Dependent Enhancement and Immune Imprint
Another possibility known as antibody-dependent enhancement, can wreak havoc on the normal function of cellular immunity.
This could occur when the immune system’s memory of the original Wuhan-type vaccine interferes with its ability to fight off new variants, making the vaccine ineffective against these variants, potentially strengthening the COVID-19 virus’s ability to replicate.
New Variants Escape T-cell Immunity
Starting from Omicron emergence, this SARS-CoV-2 variant family has learned to escape from B cell immunity with vastly increased infectivity and immune escape from spike protein-induced antibodies. Recent variants (e.g., JN.1) have learned to mutate in the non-spike regions to escape original T-cell immunity. This could make it more challenging for our original cellular immunity to eradicate an Omicron variant.
In summary, the extensive promotion of the COVID-19 vaccine has had significant long-term negative consequences, necessitating a thorough and objective reassessment of whether we should continue to encourage vaccination among the population. Relying solely on blind faith or irrational beliefs in this context can be counterproductive and potentially harmful. Health authorities and public officials have been calling for a complete discontinuation of all mRNA vaccines.
It’s also crucial to highlight the value of non-pharmacological preventive measures and primary health education about our immune system’s role in combating viruses. There are numerous ways to holistically boost our endowed immunity based on modern biomedical research. Such knowledge is essential and should be given due attention by health authorities. This approach empowers individuals with vital information and should be a part of a comprehensive public health strategy.
A health care worker prepares a dose of Pfizer BioNTech COVID-19 vaccine in a file image.
Hundreds of young people who received Pfizer’s vaccine at their school reported cardiac symptoms and a significant percent had abnormal electrocardiogram results, researchers in Taiwan reported in a new study.
A second dose of Pfizer’s shot was administered to students aged 12 to 18 across four schools in Taipei in late 2021 and researchers ran electrocardiograms, or ECGs, before and after the second vaccination on the students—all of whom had already received a single dose.
Of the 4,928 students included in the study, 17 percent reported at least one cardiac symptom, such as chest pain, after vaccination.
Most of the ECGs conducted after vaccination returned normal but 51, or 1 percent, showed enough change from the pre-vaccine ECGs for pediatric cardiologists to designate the results as abnormal.
That included four students who had significant arrhythmia, or abnormal heartbeat, and one student who experienced myocarditis, or heart inflammation—a condition that can be caused by the Pfizer and Moderna COVID-19 vaccines.
“After the second dose of BNT162b2 vaccine in a young population, cardiac-related symptoms were common. The incidences of subclinical myocarditis and significant arrhythmia were 0.1%,” the researchers, with the National Taiwan University Hospital and Medical College and other institutions, wrote.
Researchers also discovered that the heart rate in the students increased after vaccination and a decrease in other parameters, including the QT interval, or a measure of the heart’s electrical activity.
Of the 51 students with abnormal findings, 33 sought medical help, including the boy diagnosed with myocarditis. Laboratory data for the boy was normal 10 days after vaccination. The others who had issued saw their conditions improve over time.
The 18 students who did not receive medical care showed no symptoms in a one-month follow-up visit, according to the researchers.
Pfizer did not respond to a request for comment.
“The fact that there’s potential arrhythmias and you got a bona fide case of myocarditis out of this, and four serious arrhythmias, that’s a pretty heavy price to pay for a vaccine that 99 percent-plus of these kids don’t even need,” Dr. Andrew Bostom, an American heart expert, told The Epoch Times.
The ECG screening was able to detect cardiac adverse events but limitations of the research included uncertainty as to whether ECG screening can identify all myocarditis cases.
Bostom in 2021 called for studies to examine the incidence of myocarditis and a related condition, pericarditis, after COVID-19 vaccination and a moratorium on the shots until such studies were completed.
He and Dr. Clare Path of the United Kingdom pointed to a prospective study done by U.S. government researchers after heart issues were detected following a smallpox vaccine. The government has not conducted similar research for heart issues following COVID-19 vaccination, though studies using health records have shown post-vaccination heart issues lingering for at least months.
A pedestrian walks by Pfizer’s New York City headquarters in a file photograph.
Previous Research
Other studies have found that many post-vaccination cases of myocarditis were not resolved months later, and that myocarditis was the only possible cause of death for some people who died unexpectedly at home.
In a study conducted by U.S. Centers for Disease Control and Prevention (CDC) researchers, 54 percent of the 151 patients who had follow-up cardiac MRIs had abnormal results, including evidence of heart scarring.
In another paper, German researchers reported ruling out all possible causes of death but myocarditis for multiple people who died suddenly at home after vaccination.
A third paper from researchers studying Thailand students who received a Pfizer dose found that nearly 3 in 10 experienced heart effects, including palpitations and shortness of breath.
Researchers, who examined vital signs, echocardiography, and cardiac enzymes in addition to ECG results, recommended monitoring all adolescents who receive a Pfizer or Moderna shot for side effects.
Myocarditis is one of hundreds of safety signals the CDC discovered through crunching data from post-vaccination adverse event reports, according to results obtained by The Epoch Times. Most people who experience myocarditis after COVID-19 vaccination are hospitalized, according to CDC data.
Another Recent Study
The exact cause of myocarditis and other cardiac adverse events has not been pinpointed, but researchers in another recent paper said it likely stems from the spike protein in the vaccines.
Massachusetts researchers collected blood from 16 patients hospitalized with myocarditis after vaccination and detected elevated levels of spike protein in the patients, compared to no spike protein in asymptomatic, vaccinated control subjects.
While high levels of spike protein could be a consequence of myocarditis, it could also be the cause, researchers said.
The spike protein “may contribute to myocarditis,” they wrote.
Some studies have suggested that COVID-19 can also cause myocarditis, but many studies have estimated the incidence is higher after vaccination for key groups, particularly young males. A group of researchers, in a recent paper, estimated that a Pfizer or Moderna booster dose would lead to more cases of myocarditis than COVID-19 hospitalizations prevented.
The CDC and some other experts, including the Massachusetts researchers, say the benefits of the vaccines outweigh the risks; but other experts, including Florida’s surgeon general Dr. Joseph Ladapo and Dr. Peter McCullough, argue the risks outweigh the benefits, at least for young, healthy people.
Patient after patient in stable remission are now suddenly experiencing an explosive relapse
Oncology doctors are sounding the alarm – the COVID boosters appear to be triggering metastasis. Patient after patient in stable remission are now suddenly experiencing an explosive relapse, triggering the appearance of new tumors just days or weeks after being forced to have a booster.
STORY AT-A-GLANCE
Cancer rates have increased since the introduction of the COVID shots and is now one of the top three leading causes of premature death among younger adults — a trend that in turn is driving down U.S. life expectancy
The leading causes of death in 2021 were heart disease and cancer, both of which are potential side effects of the COVID jabs
Dr. Angus Dalgleish, professor of oncology at St. George’s University of London, warns that COVID boosters may be causing aggressive metastatic cancers
Research shows SARS-CoV-2 spike protein obliterates 90% of the DNA repair mechanism in lymphocytes, a type of white blood cell that helps your body fight infection and chronic disease, including cancer
The COVID jab is less effective in lymphoma patients. Emory University researchers found only 68% of non-Hodgkin lymphoma and chronic lymphocytic leukemia developed neutralizing antibodies after the second dose, compared to 100% of healthy controls
Cancer rates have increased since the introduction of the COVID shots and is one of the top three leading causes of premature death among younger adults — a trend that in turn is driving down U.S. life expectancy.
In 2019, the average life span of Americans of all ethnicities was nearly 78.8 years.1 By the end of 2021, life expectancy had dropped to 76.42 — a loss of nearly three years, which is an astounding decline. The leading causes of death in 2021 were heart disease, cancer and COVID-19, all three of which were higher in 2021 than in 2020,3 and both heart disease and cancer are potential side effects of the COVID jabs.
COVID Boosters Are Triggering Metastatic Cancer
November 26, 2022, The Daily Sceptic published a letter4,5 to the editor of The BMJ, written by Dr. Angus Dalgleish, professor of oncology at St. George’s University of London, warning that COVID boosters may be causing aggressive metastatic cancers:
“COVID no longer needs a vaccine programme given the average age of death of COVID in the U.K. is 82 and from all other causes is 81 and falling,” Dalgleish writes.6“The link with clots, myocarditis, heart attacks and strokes is now well accepted, as is the link with myelitis and neuropathy …
However, there is now another reason to halt all vaccine programmes. As a practicing oncologist I am seeing people with stable disease rapidly progress after being forced to have a booster, usually so they can travel. Even within my own personal contacts I am seeing B cell-based disease after the boosters.
They describe being distinctly unwell a few days to weeks after the booster — one developing leukemia, two work colleagues Non-Hodgkin’s lymphoma, and an old friend who has felt like he has had Long COVID since receiving his booster and who, after getting severe bone pain, has been diagnosed as having multiple metastases from a rare B cell disorder.
I am experienced enough to know that these are not the coincidental anecdotes … The reports of innate immune suppression after mRNA for several weeks would fit, as all these patients to date have melanoma or B cell based cancers, which are very susceptible to immune control — and that is before the reports of suppressor gene suppression by mRNA in laboratory experiments. This must be aired and debated immediately.”
New Norm: Explosive Cancer Relapses
In a December 19, 2022, article7 in Conservative Woman, Dalgleish continues discussing the phenomenon of rapidly spreading cancers in patients who were in stable remission for years before receiving their COVID boosters. He notes that after his letter to The BMJ was published, several oncologists have contacted him to say they’re seeing the same thing in their own practices.
“Seeing the recurrence of these cancers after all this time naturally makes me wonder if there is a common cause?” he writes.8“I had previously noted that relapse in stable cancer is often associated with severe long-term stress, such as bankruptcy, divorce, etc.
However, I found that none of my patients had any such extra stress during this time, but they had all had booster vaccines and, indeed, a couple of them noted that they had a very bad reaction to the booster which they did not have to the first two injections.
I then noted that some of these patients were not having a normal pattern of relapse but rather an explosive relapse, with metastases occurring at the same time in several sites … Scientifically, I was reading reports that the booster was leading to a big excess of antibodies at the expense of the T-cell response and that this T-cell suppression could last for three weeks, if not more.
To me, this could be causal as the immune system is being asked to make an excessive response through the humoral inflammatory part of the immune response against a virus (the alpha-delta variant) which is no longer in existence in the community.
This exertion leads to immune exhaustion, which is why these patients are reporting up to a 50% greater increase in Omicron, or other variations, than the non-vaccinated.”
A Change of Heart and Mind
Interestingly, in mid-2021, the Daily Mail published an article in which Dalgleish encouraged people to get the COVID shot, especially younger individuals.9 Dalgleish explains that, at the time, there was an “overwhelming push by the government and the medical community … that this would be in everyone’s best interest.”
So, he caved to the narrative, even though he had concerns from the start. Now, however, the environment has changed and there’s really no need for these experimental shots anymore.
His concerns further grew when his son developed myocarditis “after having a jab he did not want but that he needed for work and travel purposes.” A friend of his son, who was in his early 30s, suffered a stroke after his jab, and a relative of a close colleague died from a heart attack at the age of 34 after hers.
“I began to be highly alarmed that it was the vaccines causing these symptoms,” Dalgleish writes,10“and that just as we had written11 … a genetically engineered virus had serious implications for vaccine design.
This paper, which was suppressed and therefore did not appear in print for many months, reported that the sequence of the virus was completely consistent with having been genetically engineered, with a furin cleavage site and six inserts at places that would make the virus very infectious, and the reason this had such tremendous implications for vaccine design was that 80% of these sequences had homology to human epitopes.
In particular, we had noticed a homology with platelet factor 4 and myelin. The former is also certainly associated with what is known as VITT (low platelets and clotting issues) and the latter associated with all the neurological problems, such as transverse myelitis, both of which are now recognized as side effects of the vaccine even by the MHRA [Medicines and Healthcare Products Regulatory Agency in the UK].”
Authorities Have Willfully Ignored All Warning Signals
Dalgleish says his team’s findings were eventually circulated among cabinet members and various medical committees, but everyone ignored them. As a result, many have been placed at unnecessary risk for serious injury and/or death.
As Dalgleish points out, young hearts over-express the ACE receptor that the virus was engineered to bind to. This binding with the ACE2 receptor is what “sets off the inflammatory response, which leads to myocarditis, pericarditis, stroke and deaths,” Dalgleish says.
This could explain the dramatic increase observed in deaths of young athletes who were jabbed: They simply have more ACE2 receptors that bind to the spike proteins created by the jab. Dalgleish continues:12
“When the facts change, or new facts emerge, the position of all those in authority directing mandates should change but unfortunately, they did not.
I tried desperately to point out that all the evidence that vaccines might have been useful in helping to curtail the pandemic was changing; that it was becoming very clear that there were highly significant side effects to the vaccine programme that Pfizer had gone to great lengths to cover up, and that it was only a court case in the US that led to them becoming available.
At this stage the whole vaccine programme should have been stopped but nobody seemed to want to address this, neither the Government, the medical authorities or the media.
Having written many articles for the Daily Mail arguing against lockdown and for it never to be used again, I was extremely keen to address my change of opinion on the vaccines and to warn people of their dangers particularly to younger people, and to point out there were no grounds at all for giving it to children.
Unfortunately, all my efforts and approaches to the mainstream media on this subject have been rejected. This, I believe, is something that will come back to haunt all those who introduced an Orwellian kind of suppression to the emerging truth, which labelled doctors trying to save their patients along the lines of ‘first do no harm’ as outcasts or villains.”
Scientific Proof COVID Jab Causes Cancer
Back in August 2022, The Exposé13 highlighted scientific evidence showing the COVID jabs can cause cancer of the ovaries, pancreas and breast, and that “a monumental cover-up is taking place to suppress the consequences … on women’s health.”
Research shows SARS-CoV-2 spike protein obliterates 90% of the DNA repair mechanism in lymphocytes, a type of white blood cells that help your body fight infection and chronic disease, including cancer.
The research in question was that of Jiang and Mei, who published a peer-reviewed article showing the SARS-CoV-2 spike protein obliterated the DNA repair mechanism in lymphocytes, a type of white blood cells that play an important role in your immune system. Lymphocytes help your body fight infection and chronic disease, including cancer. Professional data analyst Joel Smalley writes:14
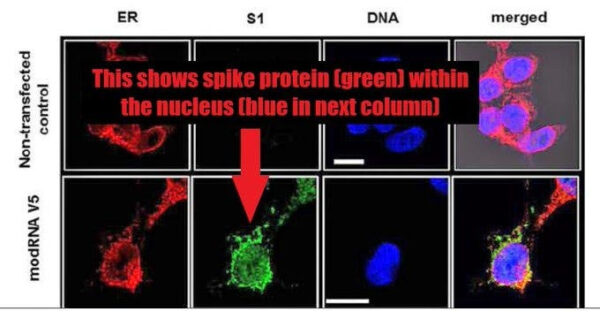
“The viral spike protein was so toxic to this pathway that it knocked 90% of it out. If the whole spike protein got into the nucleus (in the ovaries), and enough of it was produced and hung around long enough before the body was able to get rid of it all, it would cause cancer. Fortunately, in the case of natural infection, this is unlikely to occur.
Unfortunately, the experimental mRNA toxshot induces spike protein to be produced (the full-length spike exactly matching — amino acid for amino acid — the full length of the viral spike protein15) in and around the cell nucleus and is produced for at least 60 days and almost certainly longer.16
‘Fact checkers’ said the viral spike protein doesn’t get in the nucleus despite the expert scientists showing that it absolutely does. Public health authorities and regulators said the vaccinal spike protein doesn’t get in the nucleus despite the mRNA manufacturers submitting pictures of it doing so to them as part of their emergency use application …
Jiang and Mei, quite logically and reasonably, cautioned that the mRNA spike protein would likely have the same effect as the viral spike protein on p53 and therefore cause cancer … [The] Jiang and Mei paper was retracted due to spurious ‘expressions of concern’ (EOC) about the methods of the study despite them being standard practice …
Well, despite the retraction, the spike protein circulating in large quantities, in the direct vicinity of the cell nucleus, for elongated periods of time, still has the potential to induce cancer in those cells (ovary, pancreas, breast, prostate, lymph nodes). These cancers can take years to develop and so it’s possible that we don’t see much of a safety signal for 5 or 10 years.”
As noted by Smalley, one of the authors of the EOC that led to the retraction of the paper was Eric Freed, Ph.D., who heads up the U.S. National Institutes of Health’s Center for Cancer Research.
He’s been a tenured investigator with the National Institute of Allergy and Infectious Diseases (NIAID) and NIH since 2002,17 the very agencies that funded Moderna’s mRNA jab, yet this conflict of interest was not disclosed in the EOC.
A Not so Rare Cancer Case
At the end of September 2022, The Atlantic18 featured the story of Belgian immunologist Michel Goldman, 67, who in the spring of 2021 got his first and second COVID shot. In the fall that year, he was diagnosed with lymphoma, cancer of the immune system.
Mere weeks after his body scan and diagnosis, he got his first booster, thinking he needed it since he’d soon become immunocompromised by the chemotherapy. But the booster caused a rapid decline in his health.
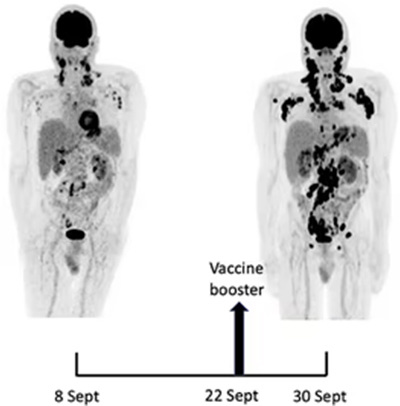
Another body scan at the end of September 2021, just three weeks after his first scan, revealed “a brand-new barrage of cancer lesions — so many spots that it looked like someone had set off fireworks inside Michel’s body,” Roxanne Khamsi writes:19
“More than that, the lesions were now prominent on both sides of the body, with new clusters blooming in Michel’s right armpit, and along the right side of his neck.
When Michel’s hematologist saw the scan, she told him to report directly to the nearest hospital pharmacy. He’d have to start on steroid pills right away, she told him. Such a swift progression for lymphoma in just three weeks was highly unusual, and he could not risk waiting a single day longer.
As he followed these instructions, Michel felt a gnawing worry that his COVID booster shot had somehow made him sicker. His brother [Serge, head of nuclear medicine at the hospital of the Université Libre de Bruxelles] was harboring a similar concern.
The asymmetrical cluster of cancerous nodes around Michel’s left armpit on the initial scan had already seemed ‘a bit disturbing,’ as his brother said; especially given that Michel’s first two doses of vaccine had been delivered on that side. Now he’d had a booster shot in the other arm, and the cancer’s asymmetry was flipped.
The brothers knew this might be just an eerie coincidence. But they couldn’t shake the feeling that Michel had experienced what would be a very rare yet life-threatening side effect of COVID vaccination.”20
T Cells Gone Berserk
Goldman, who was an early champion of the mRNA COVID shots, now “suspected that he was their unlucky victim,” Khamsi writes.21 He decided to go public about his cancer despite fears “anti-vaxxers” would use it to argue against the COVID jab. His concern for people who had the same type of cancer he had won out.
There are approximately 30 different subtypes of lymphoma. The kind Goldman had — angioimmunoblastic T-cell lymphoma — attacks follicular helper T cells, which play a crucial role in your body’s immune response to invading pathogens.
Helper T cells serve as a messenger between dendritic cells, which identify the pathogen, and B cells that make the appropriate antibodies. The mRNA COVID shots “are especially effective at generating that message, and spurring its passage through the helper T cells,” Khamsi writes.
This activation of helper T cells is part of what makes the COVID jabs work. But Goldman began to suspect that revving up those helper T cells might in some cases cause them to go berserk, resulting in tumors, or worsening of already existing ones.
Other Case Reports
Goldman was lucky. He lived to talk about it. Many others have not been so fortunate. And while he still believes he’s an “ultra-rare” case, he’s since received reports from other patients who suddenly developed angioimmunoblastic T-cell lymphoma after their shots. As reported by Khamsi:22
“Around the time of his February follow-up, Michel received a message from a doctor who had read his self-referential case report. The doctor’s mother had been diagnosed with the same subtype of lymphoma that Michel has following a COVID booster shot. More recently, he got an email from a woman whose sister had been vaccinated and received that diagnosis the following month.”
In August 2022, Frontiers in Medicine published a case report23 describing “rapid progression of marginal zone B-cell lymphoma” following the COVID jab. The 80-year-old Japanese woman featured in the report developed a noticeable tumor the very next day after her first shot. According to the authors:24
“Initially, we suspected head-and-neck benign lymphadenopathy as a side effect of vaccination. Nine weeks later, the number of swollen submandibular and parotid glands increased, and the lymph nodes further enlarged.
Finally, the right temporal mass was diagnosed as marginal zone B-cell lymphoma based on immunohistochemical and flow cytometry findings of biopsy specimens.
Our findings suggest that although 4-6 weeks of observation for lymph node inflammation after the second vaccination is recommended, malignancy should also be considered in the differential diagnosis of lymphadenopathy following vaccination.”
COVID Jab Is Far Less Effective in Lymphoma Patients
In May 2022, a single-center study25 at Emory University discovered that the humoral immune response in patients with non-Hodgkin lymphoma (NHL) or chronic lymphocytic leukemia (CLL) was significantly reduced after getting a COVID jab, compared to people who did not have either of those diagnoses.
Patients with NHL or CLL also didn’t have nearly the same antibody response to the shot. Only 68% of them developed neutralizing antibodies against SARS-CoV-2 after the second dose, compared to 100% of healthy controls. NHL/CLL patients who had undergone anti–CD20-directed therapies within one year of the first dose had the lowest antibody levels.
Data from the Defense Medical Epidemiology Database (DMED)26 — historically one of the most well-kept and most heavily-relied upon medical databases in the world — showed that, compared to the previous five-year averages, cancer among Department of Defense (DOD) personnel in 2021 skyrocketed.
Overall, cancers tripled among servicemen and their family members after the rollout of the COVID shots. Breast cancer went up 487%. Exploding cancer rates are also seen elsewhere. One of the first to warn that the shots might cause cancer was Dr. Ryan Cole, a pathologist who runs his own pathology lab.
He suspects the shots accelerate already existing cancers by way of immune dysregulation.27 He noticed that cancers that were previously well-controlled would suddenly grow out of control and rapidly lead to death once they got the COVID jab.
Swedish pathologist, researcher and senior physician at Lund’s University, Dr. Ute Kruger, has also observed an explosion in rapidly advancing cancers in the wake of the COVID shots. For example, she’s noticed:28,29
Cancer patients are getting younger — The largest increase is among 30- to 50-year-olds
Tumor sizes are dramatically larger — Historically, 3-centimeter tumors were commonly found at the time of cancer diagnosis. Now, the tumors they’re finding are regularly 4 to 12 centimeters, which suggests they’re growing at a much faster rate than normal
Multiple tumors in multiple organs are becoming more common
Recurrence and metastasis are increasing — Kruger points out that many of the cancer patients she’s seeing have been in remission for years, only to suddenly be beset with uncontrollable cancer growth and metastasis shortly after their COVID jab
These “turbo-cancers,” as Kruger calls them, cannot be explained by delayed cancer screenings due to lockdowns and other COVID restrictions, as those days are long gone. Patients, despite having access to medical screenings as in years past, are showing up with grossly exacerbated tumor growths, and she believes this is because the cancers are being “turbo-charged” by the mRNA jabs.
Disturbingly, as detailed in “How Cancer Deaths From the COVID Jabs Are Being Hidden,” analysis of U.S. Morbidity and Mortality Weekly Report (MMWR) data suggests the U.S. Centers for Disease Control and Prevention has been filtering out and redesignating cancer deaths as COVID deaths since April 2021 to eliminate the cancer signal. The signal is being hidden by swapping the underlying cause of death with main cause of death.
Unintended consequences potentially explain vaccine failure from the outset
(MattLphotography/Shutterstock)
One of the curious findings from the original randomized trials of mRNA vaccines was an explosive rate of early infection after the first injection as compared with placebo.
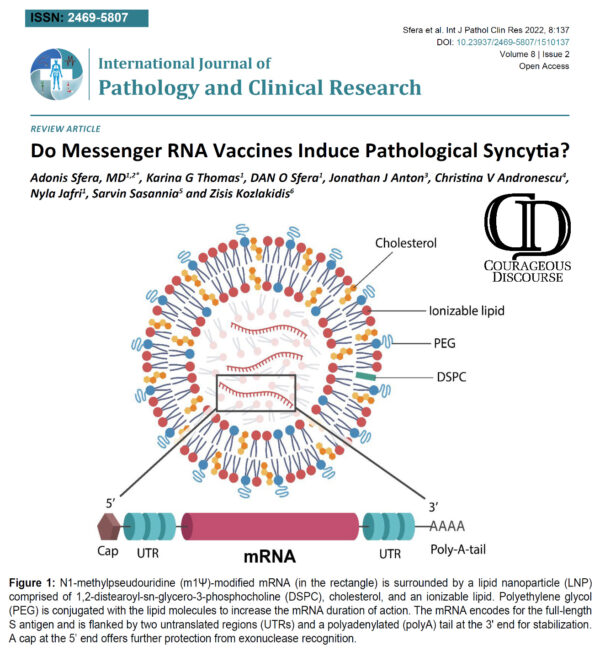
In a recent paper from Sfera et al, the description of pathological syncytia or fusion between immune cells is described: “The LNP technology, to put it simply, mimics viral envelopes with externalized phosphatidylserine (ePS), a universal “eat me” signal, that directs immune cells to engulf the particle.
Sfera A, Thomas KG, Sfera DO, Anton JJ, Andronescu CV, et al. (2022) Do Messenger RNA Vaccines Induce Pathological Syncytia?. Int J Pathol Clin Res 8:137. doi.org/10.23937/2469-5807/1510137
However, as ePS is also a potential “fuse me” signal, LNP may inadvertently facilitate the formation of pathological syncytia. Moreover, ePS may activate a disintegrin and metalloprotease 10 and 17 (ADAM10) (ADAM 17), master regulators of syncytia formation, contributing further to the unintended consequence of cell-cell fusion…
As mRNA vaccines are based on pre-fusion epitopes, the fusion pathology may be undeterred, allowing viral infection by syncytia formation to continue unabated. This is significant, as it could account for the reoccurrence of COVID-19 symptoms in fully vaccinated individuals.”
The authors point out that SARS-CoV-2 utilizes more than just the ACE2 receptor to gain entry into the fused cells and by overlooking this possibility, vaccine developers have made a blunder. This is further complicated by the choice of lipid nanoparticles and polyethylene glycol which facilitate entry into organs were syncytia as well as Spike protein will incite inflammation and immune system regulation.
Sfera also considers pregnancy: “Several studies demonstrated that SARS-CoV-2 can activate HERV-W, an ancestral gene that encodes for the physiological placental fusogen syncytin-1 responsible for the merger of trophoblasts during the early pregnancy. This suggests that the reproductive post-vaccine events may be triggered by the furin cleavage site pathology.” Such processes could occur in the gravid uterus and compound the bleeding and clotting risks of ill-advised vaccination is this special population.
In summary Sfera et al point out the following blind spots of well-funded DARPA consultants, BARDA funded academic researchers, and later by Pfizer and Moderna in mRNA vaccine development:
1) pathologic syncytia formation,
2) use of lipid nanoparticles with PEG,
3) failure to consider SARS-CoV-2 could use alternative points of cell entry other than ACE2 (metalloprotease pathway, antibody dependent enhancement, cell penetrating peptides, viroporins).
With billions of people rushed into indiscriminate mRNA vaccination, virologists and immunologists will be picking up the pieces of a failed vaccine campaign that has left so many at risk for more SARS-CoV-2 infections and progressive complications over the months and years to come.
Have you ever wanted to really understand how the immune system works? Or how the COVID-19 vaccine is different from natural immunity?
According to this cardiac surgeon, viral proteins can remain from a previous COVID infection, especially in your blood vessels, lungs and brain.
STORY AT-A-GLANCE
An international survey of 2,002 people found that people who had previously had COVID-19 experienced “significantly increased incidence and severity” of side effects after the COVID-19 vaccine
Dr. Hooman Noorchashm has repeatedly warned the FDA that “clear and present danger” exists for those who have had COVID-19 and subsequently get vaccinated
At issue are viral antigens that remain in the body after a person is naturally infected; the immune response reactivated by the COVID-19 vaccine may trigger inflammation in tissues where the viral antigens exist
The inner lining of blood vessels, the lungs and the brain may be particularly at risk of such inflammation and damage, which could lead to major thromboembolic complications
Noorchashm believes that people should be screened for SARS-CoV-2 viral proteins prior to COVID-19 vaccination, while vaccination should be delayed for people with symptomatic or asymptomatic COVID-19 infections, as well as those who have recently recovered from the virus
In their race to vaccinate the entire U.S. adult population, health officials are urging everyone to get a COVID shot, regardless of whether or not they’ve already been infected with SARS-CoV-2, the virus that causes COVID-19, and spending billions of dollars in taxpayer funded propaganda to convince people to get the vaccine.
This is an important distinction, however, with at least one scientist warning the U.S. Food and Drug Administration that “clear and present danger” exists for those who have had COVID-19 and subsequently get vaccinated.
That scientist — Dr. Hooman Noorchashm, a cardiac surgeon and patient advocate — warned the FDA that prescreening for SARS-CoV-2 viral proteins may reduce the risk of injuries and deaths following vaccination, as the vaccine may trigger an adverse immune response in those who have already been infected with the virus.[1]
Unfortunately, health agencies continue to assert that everyone should get vaccinated, even if they’ve already acquired natural immunity via previous infection.
CDC: Get Vaccinated Even if You’ve Had COVID
The U.S. Centers for Disease Control and Prevention admits that it’s rare to get sick again if you’ve already had COVID-19. Despite this, they say those who have recovered from COVID-19 should still get vaccinated:[2]
“You should be vaccinated regardless of whether you already had COVID-19. That’s because experts do not yet know how long you are protected from getting sick again after recovering from COVID-19. Even if you have already recovered from COVID-19, it is possible — although rare — that you could be infected with the virus that causes COVID-19 again.”
Your immune system is designed to work in response to exposure to an infectious agent. Upon recovery, you’re typically immune to that infectious agent. This is why, for instance, proof of prior diagnosis with chickenpox, measles and mumps is allowed instead of vaccination to enter most U.S. public schools[3] — once you’ve had the disease and recovered, you’re immune.
If you’ve had COVID-19, you have some level of immunity against the virus. It’s unknown how long it lasts, just as it’s unknown how long protection from the vaccine lasts. According to the Public Health Agency of Sweden:[4]
“If you have had COVID-19, you have some protection against reinfection. This means that you are less likely to become infected and seriously ill, and less likely to infect others if you are exposed to the virus again.
Over time, the protection that you get after an infection wanes and there is an increased risk of getting infected again. At present, we estimate that the protection after having had COVID-19 lasts at least six months from the time of infection.”
People With Prior COVID Have More Vaccination Side Effects
An international survey of 2,002 people who had received a first dose of COVID-19 vaccine found that people who had previously had COVID-19 experienced “significantly increased incidence and severity” of side effects after the COVID-19 vaccine.[5] Those who had previously had COVID-19 had a greater risk of experiencing any side effect, along with the following, specifically:
Fever
Breathlessness
Flu-like illness
Fatigue
Local reactions
Severe side effects leading to hospital care
The mRNA COVID-19 vaccines were linked to a higher incidence of side effects compared to the viral vector-based COVID-19 vaccines, but the mRNA side effects tended to be milder, local reactions. Systemic reactions, such as anaphylaxis, flu-like illness and breathlessness, were more likely to occur with the viral vector COVID-19 vaccines.
According to the researchers, the findings should prompt health officials to reevaluate their vaccination recommendations for people who’ve had COVID-19:[6]
“People with prior COVID-19 exposure were largely excluded from the vaccine trials and, as a result, the safety and reactogenicity of the vaccines in this population have not been previously fully evaluated. For the first time, this study demonstrates a significant association between prior COVID19 infection and a significantly higher incidence and severity of self-reported side effects after vaccination for COVID-19.
Consistently, compared to the first dose of the vaccine, we found an increased incidence and severity of self-reported side effects after the second dose, when recipients had been previously exposed to viral antigen.
In view of the rapidly accumulating data demonstrating that COVID-19 survivors generally have adequate natural immunity for at least 6 months, it may be appropriate to re-evaluate the recommendation for immediate vaccination of this group.”
Surgeon Warns of Immunological Dangers, Blood Clots
Noorchashm has written multiple letters to the FDA, warning them that people should be screened for SARS-CoV-2 viral proteins prior to COVID-19 vaccination. Without such screening, he wrote in one letter to the FDA, “this indiscriminate vaccination is a clear and present danger to a subset of the already infected.”[7]
He describes the case of 32-year-old Benjamin Goodman of New York, who died within one day of receiving the Johnson & Johnson COVID-19 vaccine. “There will be many more as we carelessly and indiscriminately vaccinate the already infected, millions a day … It is a near certainty,” he continued.[8] At issue are viral antigens that remain in the body after a person is naturally infected.
The immune response reactivated by the COVID-19 vaccine may trigger inflammation in tissues where the viral antigens are present. The inner lining of blood vessels, the lungs and the brain may be particularly at risk of such inflammation and damage.[9] According to Noorchashm:[10]
“Most pertinently, when viral antigens are present in the vascular endothelium, and especially in elderly and frail with cardiovascular disease, the antigen specific immune response incited by the vaccine is almost certain to do damage to the vascular endothelium.
Such vaccine directed endothelial inflammation is certain to cause blood clot formation with the potential for major thromboembolic complications, at least in a subset of such patients. If a majority of younger more robust patients might tolerate such vascular injury from a vaccine immune response, many elderly and frail patients with cardiovascular disease will not.”
What’s more, Noorchashm quotes one of his previous medical school professors, who said, “the eyes do not see what the mind does not know.” In the case of a vaccine-induced antigen specific immune response, which may trigger thromboembolic complications 10 to 20 days after vaccination, including in those who may already be elderly and frail, the reaction isn’t likely to be registered as a vaccine-related adverse event.
Immediately Delay Vaccination for These Key Groups
In his repeated letters to the FDA, Noorchashm suggests that the FDA “immediately and at the very minimum” delay COVID-19 vaccination for people with symptomatic or asymptomatic COVID-19 infections, as well as those who have recently recovered from the virus.
Because so many cases are asymptomatic, he recommends clinicians “actively screen as many patients with high cardiovascular risk as is reasonably possible, in order to detect the presence of SARS-CoV-2, prior to vaccinating them.”[11] As it stands, Noorchashm points out that by ignoring what he believes to be an imminent risk for a sizable minority of people, the FDA’s credibility, and that of the mass vaccination campaign in general, is at grave risk:[12]
“Can you imagine if the public, without having received any real warning from FDA, becomes aware of an increasing number of such vascular/thromboembolic complications? What do you suppose will happen to the level of ‘vaccine hesitancy’ then?
And, what kind of accountability do you think the public will demand from our experts and federal regulators — especially if they knew, or should have known, that this immunological danger might exist?
The aim of benefiting the majority of our public and saving the nation from this pandemic by quick and aggressive vaccination is an ethically sound one — but where we know of real or likely risks of harm and mortality, we ought to mitigate the risks to those in potential harm’s way.
So doing is the only reasonable, ethical, and likely legal option you can pursue as public health regulators — for in America, we no longer sacrifice the lives of minority subsets of people for the benefit of the majority.”
No Proof of Efficacy in People Who’ve Had COVID-19
In a high-profile report issued by the CDC’s Advisory Committee on Immunization Practices, 15 scientists stated that the Pfizer-BioNTech COVID-19 vaccine had “consistent high efficacy” of 92% or more among people with evidence of previous SARS-CoV-2 infection.[13]
But according to Rep. Thomas Massie, R-Ky, “That sentence is wrong. There is no efficacy demonstrated in the Pfizer trial among participants with evidence of previous SARS-CoV-2 infections and actually there’s no proof in the Moderna trial either.”[14] In France, the health body la Haute Autorité de Santé (HAS) does not recommend routinely vaccinating those who have already recovered from COVID-19, stating:[15]
“At this stage, there is no need to systematically vaccinate people who have already developed a symptomatic form of Covid-19 unless they wish to do so following a decision shared with the doctor and within a minimum period of time. 3 months from the onset of symptoms.”
When Massie realized that vaccination didn’t change the risk of infection among people who’ve had COVID-19, he was alarmed and contacted the CDC directly, recording his calls.
“It [the CDC report] says the exact opposite of what the data says. They’re giving people the impression that this vaccine will save your life, or save you from suffering, even if you’ve already had the virus and recovered, which has not been demonstrated in either the Pfizer or the Moderna trial,” Massey says in a “Full Measure” report.[16]
CDC Allows Misinformation to Continue
Massie spoke with multiple officials on numerous occasions, who acknowledged the misinformation and implied that it would be fixed.[17],[18] It wasn’t until Massie’s final call with the CDC, to deputy director Dr. Anne Schuchat, that it was acknowledged that a correction was necessary.
“As you note correctly, there is not sufficient analysis to show that in the subset of only the people with prior infection, there’s efficacy. So, you’re correct that that sentence is wrong and that we need to make a correction of it. I apologize for the delay,” Schuchat said. January 29, 2021, the CDC did finally issue a correction, which reads:[19]
“Consistent high efficacy (≥92%) was observed across age, sex, race, and ethnicity categories and among persons with underlying medical conditions. Efficacy was similarly high in a secondary analysis including participants both with or without evidence of previous SARS-CoV-2 infection.”
Instead of fixing the error, Massie believes the wording just phrases the mistake in a different way and still misleadingly suggests vaccination is effective for those previously infected.[20] Meanwhile, increasing numbers of breakthrough COVID-19 cases among the fully vaccinated are being reported, which the CDC has been reporting.
The CDC also changed recommendations on PCR tests for the fully vaccinated, which will further drive down the appearance of breakthrough cases by making them less likely to “test positive.”
PCR tests recommended by the WHO used to be set to 45 cycle thresholds (CTs),[21] yet the scientific consensus has long been that anything over 35 CTs renders the test useless,[22] as the accuracy will be extremely low, with false positives artificially driving up case numbers.
In April 2021, the CDC recommended the CT be lowered to 28, but only for people who are fully vaccinated.[23] Under this guidance, someone with a CT of 30 would not be considered to have COVID-19 if they were fully vaccinated, but if they were not, then their test would be “positive.”
This is beyond obvious that they are rigging the system to create data that fit their fake narrative, which is pushing the entire population to get a vaccine they don’t need.
The Big Lie — Natural Infection Isn’t Adequate
Why is it that the media continue to promote the fake narrative that natural immunity — the type acquired by getting infected by and recovering from a virus — isn’t as powerful or long-lasting as vaccine-acquired immunity?[24],[25]
Did they forget that COVID-19 vaccines aren’t intended to be a long-term solution, and have NEVER been shown to provide immunity benefits? The original warp speed test only showed reduced symptoms.
Pfizer’s CEO Albert Bourla exacerbated this charade by stating that not only will people need a third booster dose of COVID-19 vaccine within 12 months of being fully vaccinated, but annual vaccination will probably be necessary.[26]
Robust natural immunity has been demonstrated, however, for at least eight months after infection in more than 95% of people who have recovered from COVID-19.[27],[28] A Nature study also demonstrated robust natural immunity in people who recovered from SARS and SARS-CoV-2.[29]
There continue to be many unanswered questions surrounding COVID-19 vaccines, many of which most of the public has never heard of, such as imprinting and Th2 immunopathology.
That being said, if you or someone you love have received a COVID-19 vaccine and are experiencing side effects, be sure to report it. Children’s Health Defense (CHD) is calling on all who have suffered a side effect from a COVID-19 vaccine to do three things:[30]
Unintended consequences potentially explain vaccine failure from the outset
One of the curious findings from the original randomized trials of mRNA vaccines was an explosive rate of early infection after the first injection as compared with placebo.
In a recent paper from Sfera et al, the description of pathological syncytia or fusion between immune cells is described: “The LNP technology, to put it simply, mimics viral envelopes with externalized phosphatidylserine (ePS), a universal “eat me” signal, that directs immune cells to engulf the particle.
Sfera A, Thomas KG, Sfera DO, Anton JJ, Andronescu CV, et al. (2022) Do Messenger RNA Vaccines Induce Pathological Syncytia?. Int J Pathol Clin Res 8:137. doi.org/10.23937/2469-5807/1510137
However, as ePS is also a potential “fuse me” signal, LNP may inadvertently facilitate the formation of pathological syncytia. Moreover, ePS may activate a disintegrin and metalloprotease 10 and 17 (ADAM10) (ADAM 17), master regulators of syncytia formation, contributing further to the unintended consequence of cell-cell fusion…
As mRNA vaccines are based on pre-fusion epitopes, the fusion pathology may be undeterred, allowing viral infection by syncytia formation to continue unabated. This is significant, as it could account for the reoccurrence of COVID-19 symptoms in fully vaccinated individuals.”
The authors point out that SARS-CoV-2 utilizes more than just the ACE2 receptor to gain entry into the fused cells and by overlooking this possibility, vaccine developers have made a blunder. This is further complicated by the choice of lipid nanoparticles and polyethylene glycol which facilitate entry into organs were syncytia as well as Spike protein will incite inflammation and immune system regulation.
Sfera also considers pregnancy: “Several studies demonstrated that SARS-CoV-2 can activate HERV-W, an ancestral gene that encodes for the physiological placental fusogen syncytin-1 responsible for the merger of trophoblasts during the early pregnancy. This suggests that the reproductive post-vaccine events may be triggered by the furin cleavage site pathology.” Such processes could occur in the gravid uterus and compound the bleeding and clotting risks of ill-advised vaccination is this special population.
In summary Sfera et al point out the following blind spots of well-funded DARPA consultants, BARDA funded academic researchers, and later by Pfizer and Moderna in mRNA vaccine development:
1) pathologic syncytia formation,
2) use of lipid nanoparticles with PEG,
3) failure to consider SARS-CoV-2 could use alternative points of cell entry other than ACE2 (metalloprotease pathway, antibody dependent enhancement, cell penetrating peptides, viroporins).
With billions of people rushed into indiscriminate mRNA vaccination, virologists and immunologists will be picking up the pieces of a failed vaccine campaign that has left so many at risk for more SARS-CoV-2 infections and progressive complications over the months and years to come.
 Example individual model fits for the primary series (blue) and booster dose (orange) Anti-S trajectory data. Dashed lines for D1, D2, and D3 indicate timing of dose 1, dose 2, and dose 3, respectively. (B) Distribution of all individual half lives for primary series (blue) and booster dose (orange). (C) Individual Anti-S half life as a function of chronological age for primary series and booster dose, where a decreasing trend as a function of increased age is found. (D) Violin plots of Anti-S half lives and number of chronic morbidities. Points are plotted with a jitter function to display the density of individuals with each chronic morbidity count. (E) Parametric plot of chronic morbidity count and chronological age, where the size of each point corresponds to the number of data points at a given age with the same chronic morbidity count. The number of individuals within each chronic morbidity category are shown to the right of the plot. Credit: Scientific Reports (2024). DOI: 10.1038/s41598-024-58811-3")