Nearly half of all cancer patients undergo radiation therapy as part of their care. Ionizing radiation, or the emission of high-energy waves or particles, works as a therapy by damaging a cancer cell’s DNA. It’s an effective tool for killing cancer cells because they are generally much less adept at DNA repair compared to healthy cells. Damaging specific parts of DNA prevents cancer cells from reproducing, effectively killing them.
A major limitation of radiation therapy is the damage it may cause as it passes through healthy organs to get to tumors located deep in the body. The need to protect healthy organs limits the dose of radiation that can be delivered to cancerous tissue, thereby reducing the chance of successful treatment.
Overcoming this challenge has long been a mission for medical physicists and radiation oncologists like us. Improvements to radiotherapy will enable clinicians to not only better control tumors overall, but also open the door for more favorable outcomes in patients with cancers that are more resistant to radiation.
Fundamentals of radiation therapy
At the heart of radiation therapy lies the fundamental principle that cancer cells are more susceptible to radiation than healthy cells. However, there are exceptions. Sometimes resistance to radiation in cancer cells may be comparable or even greater than that of their neighboring cells.
When tumors lie close to vital organs that are highly sensitive to radiation, such as the brain or the bowels, it significantly limits the amount of radiation that can be delivered. In cases where tumors are significantly less sensitive to radiation than the organs surrounding it, radiotherapy may not be the best choice. Radiation therapy involves directing strong beams of energy to kill cancer cells.
Patient immobilization is another key aspect to reducing toxicity from radiation. Patients need to be completely motionless during treatments to ensure that the beam of radiation mainly targets tumors and not the healthy tissues surrounding them. If a patient moves during treatment, it can mean the radiation beam is partly or even entirely missing the cancer target. This scenario both underdoses the cancer and increases the risk of harming healthy tissue.
There are a few common types of radiotherapy that deliver radiation in different ways:
External beam radiation therapy
External beam radiation involves directing radiation from an outside source to a single part of the body.
Linear accelerators, commonly referred to as LINACs, are currently the most common technology used in radiation treatments. These machines generate beams of high-energy electrons and X-rays that can be aimed at cancer tissue with precision. The high energy of these beams allows in-depth penetration into the body to reach tumors.
Another form of radiotherapy is proton beam therapy, or PBT, which directs protons instead of X-rays at tumors. Currently, PBT is only available at a limited number of locations. It is typically recommended for specific populations such as pediatric patients because, unlike X-rays, it has an adjustable range that minimizes the effects of radiation on organs beyond the target area, potentially reducing toxicity.
Image-guided radiation therapy
In the early 2000s, researchers incorporated CT scanners into LINACs. This enabled real-time imaging of the patient’s anatomy just before or during treatment. By acting as the eyes of the care team, imaging reduced uncertainty about the location of tumors and improved the precision and accuracy of radiation therapy.
Newer linear accelerators are now incorporating MRIs, which significantly improve visualization of patient anatomy and tumors, further advancing treatment precision and accuracy.
Patients need to stay still during radiotherapy to ensure the beam stays on course.
Researchers are also adding positron emission tomography, or PET, scanners that provide information about the metabolic function of tumors. This advance makes it possible to increase the radiation dose specifically at the most active areas of tumors.
Adaptive therapy
An emerging approach to radiation therapy called adaptive therapy uses imaging to dynamically adjust treatment as the tumor or its positioning changes each day.
In conventional radiation therapy, patients receive the same treatment plan across multiple treatment sessions. However, adaptive therapy may apply several adjustments or lead to a completely new treatment plan in order to address changes to the tumor’s condition over the course of treatment.
Historically, the concept of adaptive therapy was more theoretical than practical. It faced many challenges, including a lack of suitable imaging technologies. Additionally, creating a treatment plan involves heavy computational work and collaboration among various specialties within a care team. The fact that the process needs to be repeated multiple times renders adaptive therapy particularly resource-intensive and time-consuming. However, researchers are looking into ways to use artificial intelligence to automate some of these steps to make this approach more practical.
Brachytherapy
Brachytherapy – stemming from the Greek word “brachys,” meaning “short” – is another widely used method in radiation therapy. It involves placing a radioactive source called a seed near or directly inside a tumor or affected area, reducing the distance from the radiation source to its target.
In contrast to external beam radiation therapy, where radiation often must pass through healthy tissue to reach cancer cells, brachytherapy applies radiation directly to the tumor. This technique is particularly advantageous for certain cancer types that are accessible through noninvasive or minimally invasive procedures, such as skin cancers, gynecological tumors and genitourinary tumors.
By placing the radioactive source inside the body, brachytherapy can target tumors more directly than external beam radiotherapy. Cancer Research UK/Wikimedia Commons, CC BY-SA
The conventional approach to brachytherapy involved using needles to place or inject radioactive seeds inside or adjacent to the cancerous tissue. These seeds would remain in the body either temporarily or permanently, with the goal of irradiating the area at a low dose over a long period of time.
An increasingly popular form of brachytherapy called high-dose rate brachytherapy involves using a tube to guide a more highly radioactive seed directly to the affected tissue before removing it after a few minutes. The seed emits a high dose of radiation in a short period of time, which enables clinicians to treat patients quickly in an outpatient setting.
Future of radiation therapy
Radiation therapy is continually evolving to more effectively and precisely treat cancer.
For example, a technique that delivers radiation at an ultra-high rate called FLASH-RT has shown promise in its ability to increase dosages without excessive toxicity. Researchers are also exploring treatments using ions heavier than protons to more effectively damage DNA in cancer cells and enhance the efficacy of radiation therapy.
Advances in the field hint at a future of more personalized radiation therapy, highlighting the fusion of technology and medical expertise in the fight against cancer.
The past two decades have brought a sea change in the way many types of cancer are treated. Targeted therapies shut down specific proteins in cancer cells that help them grow, divide, and spread. Immunotherapies stimulate or suppress the body’s immune system to help fight cancer. But long-used treatments — surgery, chemotherapy, and radiation therapy — remain the backbone of treatment for most cancers.
Radiation therapy was first used to treat cancer more than 100 years ago. About half of all cancer patients still receive it at some point during their treatment. And until recently, most radiation therapy was given much as it was 100 years ago, by delivering beams of radiation from outside the body to kill tumors inside the body.
Though effective, external radiation can also cause collateral damage. Even with modern radiation therapy equipment, “you have to [hit] normal tissue to get to a tumor,” said Charles Kunos, M.D., Ph.D., of NCI’s Cancer Therapy Evaluation Program (CTEP). The resulting side effects of radiation therapy depend on the area of the body treated but can include loss of taste, skin changes, hair loss, diarrhea, and sexual problems.
Now, researchers are developing a new class of drugs called radiopharmaceuticals, which deliver radiation therapy directly and specifically to cancer cells. The last several years have seen an explosion of research and clinical trials testing new radiopharmaceuticals.
These studies have suggested that targeting radiation therapy at the cellular level has the potential to reduce the risk of both short- and long-term side effects of treatment while at the same time enabling even tiny deposits of cancer cells to be killed throughout the body.
“I think they’re going to transform radiation oncology in the next 10 to 15 years,” Dr. Kunos said.
Building on a Natural Affinity
Delivering radiation directly to cells isn’t itself a new approach. One such therapy, called radioactive iodine, has been used to treat some types of thyroid cancer since the 1940s. Iodine naturally accumulates in thyroid cells. A radioactive version of the element can be produced in the lab. When ingested (as a pill or a liquid), it accumulates in and kills cancer cells left over after thyroid surgery.
A similar natural affinity was later exploited to develop drugs to treat cancer that has spread to the bones, such as radium 223 dichloride (Xofigo), which was approved in 2013 to treat metastatic prostate cancer. When cancer cells grow in the bone, they cause the bone tissue they invade to break down. The body then attempts to repair this damage by replacing that bone—a process called bone turnover.
The radioactive element radium “looks like a calcium molecule, so it gets incorporated into areas of the body where bone turnover is highest,” such as areas where cancer is growing, Dr. Kunos explained. The radium is then able to kill nearby cancer cells.
These radioactive compounds all travel to cancer cells without any help. Researchers wondered whether it would be possible to engineer new radioactive molecules that specifically target other cancers.
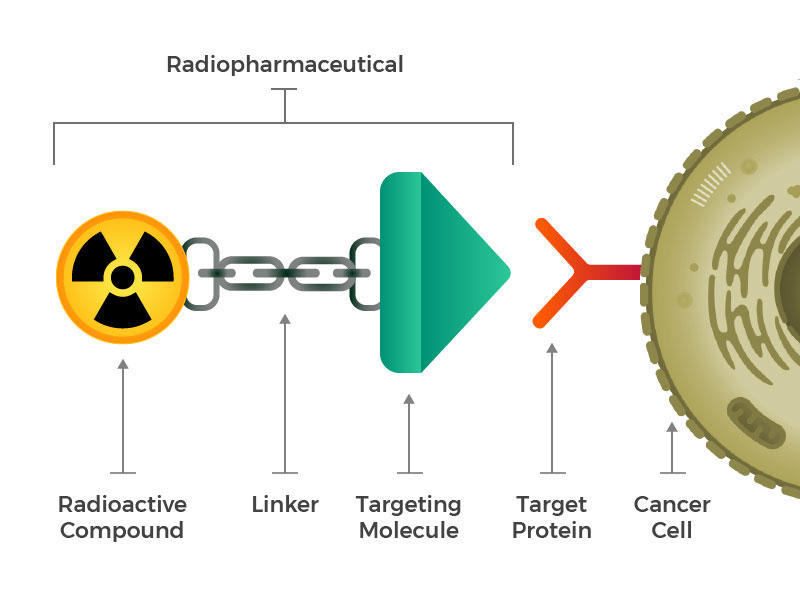
They envisioned engineered radiopharmaceuticals that consist of three main building blocks: a radioactive molecule, a targeting molecule (that recognizes and latches specifically onto cancer cells), and a linker that joins the two. Such compounds could be injected, infused, inhaled, or ingested, and then make their way into the bloodstream.
The idea of linking a cancer-targeting molecule with a molecule that kills cancer cells is not new either. For example, several drugs called antibody–drug conjugates, in which an antibody that binds to specific cancer cells is linked to a toxic drug, have been approved for treating cancer.
But efforts to create such drugs have met with limited success, Dr. Kunos explained, because it isn’t enough that toxins be brought close to a cancer cell. The toxins have to be taken inside and stay inside the cells long enough to cause damage. Many cancer cells have or develop mechanisms to simply pump toxins right back out before that can happen.
Radiopharmaceuticals also work best when the drugs can get inside cells. But that’s not necessary for them to be effective. Once a radiopharmaceutical has stuck to a cancer cell, the radioactive compound naturally breaks down. This decay releases energy that damages the DNA of nearby cells. And when a cell’s DNA is irreparably damaged, that cell dies. Cancer cells are particularly sensitive to radiation-induced DNA damage.
Depending on the type of radioactive compound used, the resulting energy can penetrate the cell bound to the radiopharmaceutical as well as about 10 to 30 cells surrounding that cell. This increases the number of cancer cells that can be killed with a single radiopharmaceutical molecule.
By the mid-2010s, the Food and Drug Administration (FDA) had approved two radiopharmaceuticals that target molecules on certain B cells to treat some people with non-Hodgkin lymphoma, a type of blood cancer. But these drugs were never widely adopted. Few doctors treating patients with lymphoma were trained to administer these types of radioactive compounds. And the radiopharmaceuticals faced competition from newer, nonradioactive drugs.
“This showed that solid tumors can also be targeted this way,” with a radiopharmaceutical built from scratch, he said. In this case, the targets are certain hormone receptors found in abundance on the surface of NET cells.
Lutetium Lu 177-dotatate was better at slowing NET growth than any previous drug tested, explained Aman Chauhan, M.D., of the University of Kentucky, who is leading several new clinical trials of the drug. “This was a huge step forward for our field,” he said.
Adapting Drugs from Imaging Compounds
Researchers are now designing and testing radiopharmaceuticals for a range of cancers as diverse as melanoma, lung cancer, colorectal cancer, and leukemia, said Dr. Capala. Any tumor that has a targetable molecule on the surface of its cells and a good blood supply—sufficient to deliver drugs—could potentially be treated with radiopharmaceuticals, added Dr. Chauhan.
Many of these newer drugs are re-engineered versions of existing compounds used for nuclear imaging. Nuclear imaging tests, such as positron emission tomography (PET), sometimes use weakly radioactive compounds linked to molecules that bind to specific targets on the surface of cancer cells. Specialized cameras can then reveal even tiny deposits of cancer cells, helping to measure the spread of cancer through the body.
Researchers have now repurposed these targeting molecules to carry more potent radioactive compounds, or isotopes, instead—ones that could kill cancer cells instead of simply helping visualize them.
Prostate cancer has been an early testing ground for this repurposing. A protein called PSMA is found in large amounts—and almost exclusively—on prostate cells. By fusing a molecule that binds to PSMA to a radioactive compound used in PET scan imaging, scientists have been able to visualize tiny deposits of prostate cancer that are too small to be detected by conventional imaging.
Several radiopharmaceutical treatments that target PSMA are now being tested in clinical trials.
Most prostate cancers are very sensitive to radiation, and external radiation is commonly used to treat the disease, explained Frank Lin, M.D., of NCI’s Center for Cancer Research, who is leading a clinical trial of one PSMA-targeting radiopharmaceutical at the NIH Clinical Center.
Most men who receive radiation as their initial treatment won’t experience a recurrence of their cancer. But if they do, it sometimes spreads throughout the body, with many small deposits of cancer cells in many organs, he explained.
“When the tumor has spread like that, you can’t really do external-beam radiation anymore, because external radiation can only be focused on and treat a small part of your body at a time,” Dr. Lin said.
Having a radiopharmaceutical that targets PSMA is a better way to give radiation in these cases, because it can be infused directly into the blood stream and circulate widely, attaching to prostate cancer cells that have spread throughout the body, he explained.
And a big advantage of having imaging and treatment molecules that use the same target is that imaging can then give doctors a sneak preview of whether the treatment is likely to work, added Dr. Lin.
For example, in Dr. Lin’s trial, men must have a PET scan with the imaging version of the compound before treatment. If the imaging compound finds its way to the cancer cells and is detected on the PET scan, then the researchers can assume that the corresponding radiopharmaceutical treatment will hit its target.
“This complementary development of diagnostics hand-in-hand with drug therapies makes this field so much more exciting,” said Dr. Chauhan. “This way we can know we’re delivering the therapy right to the tumor cells.”
Moving to Combination Therapies
While radiopharmaceuticals have shown promise in early studies, they are also, as is the case with other types of cancer drugs, unlikely to wipe out a tumor on their own.
For example, lutetium Lu 177-dotatate more than doubled the number of people who had their neuroendocrine tumors shrink after treatment, but that number was still modest: about 17%, up from 7% without the drug, explained Dr. Chauhan.
“There is still significant room for improvement,” he said.
Using radiopharmaceuticals in combination with other therapies may be one way to drive that improvement. Some researchers are now testing radiopharmaceuticals combined with radiation sensitizers—drugs that make cancer cells even more vulnerable to radiation. For example, Dr. Chauhan is leading a clinical trial of lutetium Lu 177-dotatate combined with a radiation sensitizer called triapine, which blocks cells from producing the compounds needed for DNA repair after radiation-induced damage.
In another trial, Dr. Lin is testing lutetium Lu 177-dotatate with a type of drug called a PARP inhibitor. These drugs, which are already approved to treat some types of breast, ovarian, and other cancers, block the process of DNA repair itself. “So the radiation would cause the DNA damage, and the PARP inhibitor would prevent the tumor cells from healing their DNA after the radiation,” he explained.
Other researchers are combining radiopharmaceuticals with immunotherapies to try to boost the effectiveness of these drugs. “Recent studies have shown that radiopharmaceuticals can make tumors more responsive to immunotherapy,” said Dr. Capala.
Many tumors are “cold” tumors, he explained, in that immune cells do not recognize them, or don’t work properly in the microenvironment around tumors, he explained.
But when radiation kills cancer cells, proteins and DNA from those cells can spill into the bloodstream for immune cells to see, which may allow the immune cells to recognize and kill other cancer cells throughout the body. Radiation therapy may also make the tumor microenvironment more hospitable to immune cells, added Dr. Capala.
“But there’s data suggesting that [immunotherapy] works better if each tumor, each metastasis, is exposed to radiation. So radiopharmaceutical therapy has an advantage there, in that once it’s in the body it reaches all metastases,” Dr. Capala explained.
It may even make sense to combine radiopharmaceuticals with external radiation, as long as careful treatment planning can ensure a safe overall radiation dose, added Dr. Capala. “External radiation therapy is very good at targeting large tumors, and then you could combine it with radiopharmaceutical therapy to target metastases,” he said.
Challenges and Cautions
The field of radiopharmaceuticals is still in its early days. One challenge the approach will need to overcome before it can be used more widely is the shortage of doctors trained to administer such drugs.
“The number of nuclear medicine physicians in the US is small,” said Dr. Lin, who has training in both nuclear medicine and medical oncology. “And I think we only train maybe 70 or 80 new people a year.”
So far, this workforce shortage has kept radiopharmaceuticals from living up to their true potential as a personalized treatment, explained Dr. Capala. That potential reflects the fact that, unlike with other types of cancer drugs, doctors can use imaging to measure exactly how much of a radiopharmaceutical has reached a tumor, almost in real time, and adjust the dose accordingly.
But this type of treatment planning requires multidisciplinary expertise that isn’t widely available and has left people using radiopharmaceuticals more as “radioactive chemotherapy,” with a one-size-fits-all dose, he added. “This means that many patients aren’t [yet] getting optimal treatment,” said Dr. Capala.
Long-term safety studies are also needed, added Dr. Chauhan. People treated with external radiation therapy may experience some side effects, called late effects—such as the development of second cancers—months or years after treatment. Although research to date has not shown a high rate of late effects from radiopharmaceutical treatment, “these are very new agents, and we have to continue to be cautious and monitor them,” he said.
Smoothing Collaborations
Because these drugs are relatively new, even with the trials underway, “we’re just scratching the surface of drug development for radiopharmaceuticals,” Dr. Chauhan said.
In 2019, to further boost trials of promising new radiopharmaceuticals, NCI launched the Radiopharmaceutical Development Initiative (RDI) to speed promising new drugs into clinical testing.
One thing NCI hopes to achieve with the RDI is to broker more trials using combinations of drugs produced by different pharmaceutical companies that might not collaborate otherwise, explained Dr. Kunos, who is leading the initiative. Concerns about intellectual property and a lack of trust can stop such projects before they start, Dr. Kunos explained.
“These types of collaborations would not necessarily happen unless NCI was the honest broker in the middle,” he said. Right now, only about 2% of early-phase trials supported by NCI are testing radiopharmaceuticals, but with the RDI this may grow exponentially in the coming years, he added.
“We’re not going to eliminate machines or other techniques that we use in radiation therapy,” Dr. Kunos said. “But with their targeted nature, we think radiopharmaceuticals are going to transform how we use radiation.”
NRG Oncology Phase III clinical trial, NRG-GY018, evaluating pembrolizumab in combination with standard of care chemotherapy (carboplatin and paclitaxel) met its primary endpoint of progression free survival (PFS) for the treatment of patients with stage III-IV or recurrent endometrial carcinoma, regardless of mismatch repair status. A pre-specified interim analysis, conducted by an independent Data Monitoring Committee, demonstrates that pembrolizumab in combination with chemotherapy has a statistically significant and clinically meaningful improvement in PFS compared with chemotherapy alone in both study cohorts, mismatch repair deficient (dMMR) and mismatch repair proficient (pMMR). The full results of this trial will be presented at an upcoming scientific conference.
NRG-GY018, a randomized, blinded, placebo-controlled study, accrued 819 women with stage III-IV or recurrent endometrial cancer. Two independent cohorts were evaluated, patients with endometrial cancers that are dMMR and patients with endometrial cancers that are pMMR. Patients were randomly assigned to receive pembrolizumab combined with carboplatin and paclitaxel (for a planned six, 3-week cycles), followed by pembrolizumab maintenance (for up to fourteen, 6 week cycles) or placebo combined with carboplatin and paclitaxel, followed by placebo maintenance.
Patients with advanced stage or recurrent endometrial cancer, the most common type of gynecologic cancer in the U.S., face a poor prognosis with limited treatment options. This is particularly notable in patients who progress after prior platinum-based adjuvant therapy with disease not amenable to curative surgery or radiation. In this study, pembrolizumab in combination with carboplatin and paclitaxel resulted in a statistically significant and clinically meaningful improvement in PFS in both the dMMR and pMMR study populations. We look forward to presenting these exciting findings at an upcoming scientific congress.”
Ramez Eskander, MD, of the University of California San Diego Moores Cancer Center and the Principal Investigator of the NRG-GY018 trial
This project was supported by the NRG Oncology Operations grant U10CA180868 and the NRG Oncology SDMC grant U10CA180822 from the National Cancer Institute (NCI), part of the National Institutes of Health and conducted by the NCI National Clinical Trials Network. Funding and support were also received from Merck & Co., Inc. through a Cooperative Research and Developmental Agreement with NCI. NRG-GY018 was conducted with funding supplemental to the CRADA from Merck in an Agreement between Merck and The GOG Foundation d/b/a NRG Oncology Philadelphia East.
For women who have a lumpectomy or breast-conserving surgery, radiation is a standard element in treatment. And we know from classic studies from the National Surgical Adjuvant Breast and Bowel Project (NSABP) and others that women who have a mastectomy actually have the exact same survival as women who have a lumpectomy, provided that the women who have a lumpectomy additionally receive radiation treatment.[1] The question that arises frequently for older women, typically defined as age 65 or 70 or older, is whether it essential to include radiation therapy? And there have been two studies that have looked at the possibility of omitting radiation treatment in older women with estrogen receptor (ER)–positive breast cancer after lumpectomy.
The first study, from Cancer and Leukemia Group B (CALGB), was led by Kevin Hughes and compared endocrine therapy alone versus endocrine therapy plus radiation treatment.[2,3]It showed that radiation therapy had no impact on long-term survival. However, women who had radiation treatment did have a lower risk of in-breast recurrence. It went to about 2%, with women who did not have radiation having about a 10% or 12% risk of in-breast recurrence. Again, that’s not overall survival, but it does lower the risk of an event within the breast over the next decade.
The PRIME II study was a European-based study that also asked a question, can women with ER-positive breast cancer omit radiation after lumpectomy if they are older? And fundamentally, the PRIME II study reached the same conclusion, that there was no impact on overall survival amongst older women, but there was a small decrease in the risk of in-breast recurrence.[4]
So what do we actually do in clinic? For many older women, particularly 75 years and older, I think it’s very comfortable to say that they may omit radiation therapy. The risk of in-breast recurrence is generally low, and there will be no impact on survival. For very vigorous women in their late 60s, early 70s, I think you can also point to these data and say that radiation therapy may lower their risk of in-breast recurrence. And since radiation is generally well tolerated, it can be a good option for such women who have a life expectancy well beyond 10 years. Finally, it’s important to remember that these studies assume that the patient will be taking antiestrogen adjuvant therapy. If there is a reason to believe that the patient will not be taking tamoxifen or an aromatase inhibitor or other appropriate endocrine treatment, then you can’t rely on the endocrine therapy to control in-breast recurrence, and those women should receive radiation treatment after lumpectomy.
Men with early stage testicular cancer can safely receive one course of chemotherapy or radiotherapy after surgery without it having a long-term effect on their sperm count, according to a study published in the leading cancer journal Annals of Oncology [1] on February 25.
Although it is known already that several rounds of chemotherapy or high doses of radiotherapy given to men with more advanced testicular cancer can reduce sperm count and concentration, it has been unclear whether a single cycle of chemotherapy or radiotherapy would have a similar effect in men with stage I disease.
Dr, Kristina Weibring, a cancer doctor at the Hospital in Stockholm, Sweden, who led the study, said: “We wanted to examine in more detail if postoperative treatment, given to decrease the risk of recurrence after the removal of the tumorous testicle, would affect the sperm count and sperm concentration long term in testicular cancer patients with no spread of the disease. To our knowledge, no such study has been done before.
“This is important to find out, since treatment with one course of postoperative chemotherapy has been shown to decrease the risk of relapse substantially, thereby reducing the number of patients having to be treated with several courses of chemotherapy.”
Testicular cancer is the most common cancer in young men between the ages of 15 and 40. When it is diagnosed, all patients have the testicle containing the tumour removed, a surgical procedure called orchiectomy.
In this study, 182 men aged between 18 and 50, diagnosed with stage I testicular cancer and who had had an orchiectomy within the past five years, took part in the study between 2001 and 2006. They were treated either in Stockholm or Lund. After surgery, they received radiotherapy (14 fractions of 1.8 Gy each, up to a total dose of 25 Gy) or one course of chemotherapy, or were managed by surveillance, meaning there was no postoperative treatment. They provided semen samples after orchiectomy but before further treatment, and then six months, one year, two years, three years and five years thereafter. From 2006 onward, radiotherapy was no longer used as a standard treatment in Sweden because of the risk of causing secondary cancer.
“We found no clinically significant detrimental long-term effect in either total sperm number or sperm concentration, irrespective of the type of postoperative treatment received,” said Dr Weibring. “Among men who received radiotherapy, there was a distinct decrease in average sperm number and concentration six months after treatment, though not in those who received chemotherapy. However, sperm number and concentration recovered in the radiotherapy group after six months, and continued to increase in all groups up to five years after treatment.
“I am very excited to see these results as I wasn’t expecting sperm to recover so well after postoperative treatment. I didn’t expect as negative an effect as if the patient had received many courses of chemotherapy, since it is much more toxic, but I was not sure how much the sperm would be affected by one course.
“With the results of this study we can give the patients more adequate information on potential side effects from postoperative treatment. Testicular cancer patients are often young men wanting to father children at some point, and we find, in many cases, that the patients are afraid of the potential risk of infertility caused by chemotherapeutic treatment. These findings should provide some reassurance to them.”
A well-known problem for men diagnosed with testicular cancer is an impaired ability to create sperm. A condition called testicular dysgenesis syndrome, characterized by poor semen quality among other things, may play a role in this and is also associated with a higher risk of developing testicular cancer. In addition, the orchiectomy and the cancer itself may also affect sperm quality. The removal of one testicle does not necessarily affect a man’s sperm count and concentration as the remaining testicle can compensate.
Dr Weibring concluded: “Our results are promising but more studies are needed, and we still recommend sperm banking before orchiectomy as a number of patients may have low sperm counts at the time of diagnosis that persists after postoperative treatment. In addition, the type of testicular cancer and whether or not it will need further treatments are unknown factors before the orchiectomy. Assisted reproductive measures may be necessary for these patients regardless of any treatment given.”
Editor-in-chief of Annals of Oncology, Professor Fabrice André, Professor in the Department of Medical Oncology, Institut Gustave Roussy, Villejuif, France, commented: “This study, together with other research efforts, explores the paths to recovering a normal life after cancer. The finding that one course of chemotherapy has minimal impact on sperm count offers hope for thousands of patients worldwide, but we all must keep in mind that these data are preliminary and will require validation before we can use them in clinics. The next step will be to establish how to predict the toxic effects on sperm count of different chemotherapy regimens.”
REFERENCE
[1] “Sperm count in Swedish clinical stage I testicular cancer patients following adjuvant treatment”, by Kristina Weibring et al. Annals of Oncology. doi:10.1093/annonc/mdz017
The research was supported by grants from the Swedish Government Funding for Clinical Research, the Swedish Cancer Society, Gunnar Nilsson’s Cancer Fund, Malmo University Hospital Foundation for Cancer Research and Foundation for Urological Research, and King Gustaf V’s Jubilee Fund for Cancer Research.
Lead author Dr. Amar Kishan, assistant professor of radiation oncology at the David Geffen School of Medicine at UCLA and researcher at the UCLA Jonsson Comprehensive Cancer Center.
A new UCLA-led study shows that men with low- or intermediate-risk prostate cancer can safely undergo higher doses of radiation over a significantly shorter period of time and still have the same, successful outcomes as from a much longer course of treatment.
This type of radiation, known as stereotactic body radiotherapy, is a form of external beam radiation therapy and reduces the duration of treatment from 45 days to four to five days. The approach has been in use since 2000, but has not yet been widely adopted because of concerns over how safe and effective this approach would be in the long term.
“Most men with low- or intermediate-risk prostate cancer undergo conventional radiation, which requires them to come in daily for treatment and takes an average of nine weeks to complete,” said lead author Dr. Amar Kishan, assistant professor of radiation oncology at the David Geffen School of Medicine at UCLA and researcher at the UCLA Jonsson Comprehensive Cancer Center. “That can be very burdensome on a patient and be a huge interruption in their life. With the improvements being made to modern technology, we’ve found that using stereotactic body radiotherapy, which has a higher dose of radiation, can safely and effectively be done in a much shorter timeframe without additional toxicity or compromising any chance of a cure.”
The UCLA research team analyzed data from 2,142 men with low- or intermediate-risk prostate cancer across multiple institutions who were treated with stereotactic body radiotherapy for prostate cancer between 2000 and 2012.
The men were followed for a median of 6.9 years. Just over half of the men had low-risk disease (53 percent), 32 percent had less aggressive intermediate-risk disease and 12 percent had a more aggressive form of intermediate-risk disease.
The recurrence rate for men with low-risk disease was 4.5 percent, the recurrence rate for the less aggressive intermediate-risk was 8.6 percent, and the recurrence rate for the more aggressive intermediate-risk group was 14.9 percent. Overall, the recurrence rate for intermediate-risk disease was 10.2 percent. These are essentially identical to rates following more conventional forms of radiation, which are about 4 percent to 5 percent for low-risk disease and 10 percent to 15 percent for intermediate-risk disease.
“What is remarkable about this very large study is how favorably stereotactic body radiotherapy compares to all other forms of radiation treatments, both in terms of effectiveness and side effects,” said senior author Dr. Christopher King, professor of radiation oncology and scientist at the UCLA cancer center. “With such long-term follow-up data, we can now offer this approach to patients with full confidence.”
The research team at UCLA had previously found that stereotactic body radiation therapy was more cost effective because of the fewer treatments involved. Other research has also suggested psychological benefits such as less regret about undergoing treatment. The current study now provides long-term data regarding the safety and clinical efficacy of this approach.
Kishan said the data show that the majority of the men followed are free of prostate cancer seven years after treatment. He added that there was no evidence that this therapy caused worse toxicity in the long term. “In fact,” Kishan said, “we not only confirm that this method is both safe and effective, but we provide significant evidence that this could be a viable treatment option for men with low- and intermediate-risk of prostate cancer.”
Breast cancer is the leading cause of cancer deaths in women in the U.S. Survival is better when breast cancer is diagnosed while still local, and 60.8% of women in the U.S. are diagnosed at this stage. In this group of patients, 5-year survival is 98.5%, according to data from the Surveillance, Epidemiology, and End Results (SEER) Program.1 In these cases, surgical treatment with lumpectomy or mastectomy is often followed by radiation therapy.
In fact, a recent meta-analysis of 22 randomized trials provided additional support for the use of postmastectomy radiation in decreasing the rate of mortality related to recurrent cancer and breast cancer in women found to have 1 to 3 positive lymph nodes during mastectomy and axillary dissection.2 As a result of this and other studies, the need to understand the long-term effects of radiation therapy has become more urgent. One of the most important questions is: Does radiotherapy to the chest increase the incidence of ischemic heart disease (IHD)?
The dose of radiation to the breast and heart is now considerably lower than it has been in the past.3 Nonetheless, when malignancies of the right breast are treated with radiation, the heart is typically exposed to a dose of approximately 1 to 2 Gy. Heart exposure is higher for disease of the left breast, of course, and may run up to 10 Gy.4
A recent study assessed how the dose of radiation a woman receives during breast cancer treatment affects her subsequent risk of IHD.
Darby and colleagues performed a case-control study of major coronary events in women who received external beam radiotherapy for invasive breast cancer.4 Major coronary events were defined as myocardial infarction, coronary revascularization, and death from IHD. Their study, recently published in the New England Journal of Medicine (NEJM), included 2168 women who received radiotherapy for breast cancer from 1958 to 2001 in Sweden and Denmark. Of these, 963 women had major coronary events, and 1205 did not and served as controls. Radiation doses to the whole heart and to the left anterior descending artery were estimated based on radiotherapy records.
Mean radiation dose to the heart was 4.9 Gy (range, 0.03 to 27.72). The rate of cardiovascular events increased by 7.4% for each increment of 1 Gy (95% CI, 2.9 to 14.5;P<.001), with no threshold below which there was no risk. This deleterious effect on the heart started within the first 5 years after therapy and continued for at least 20 years. The presence of cardiac risk factors increased the absolute rate of cardiac outcomes but didn’t affect the proportional increase in the rate of major coronary events per Gy.
None of the women in the study received the cardiotoxic chemotherapeutic agents taxanes or trastuzumab, and very few received anthracyclines, thus minimizing these confounders for ischemic outcomes.
Though radiation delivery techniques have improved considerably in recent decades, the incidental exposure of radiation to the heart is always of concern, and strategies to minimize radiation should be exercised whenever possible. Despite this, as Fei-Fei Liu, MD, Professor of Radiation Oncology at the University of Toronto, stated in an editorial that accompanied the Darby article, “It is important to reassure women with breast cancer that with the use of current technologies, the cardiac dose can be decreased considerably, and cardiac risk factors can be better managed.”
Investigator Sarah C. Darby, PhD, of the Clinical Trial Service Unit at the University of Oxford, England, says that “One thing that our studies have shown rather clearly is that any radiation-related risk probably multiplies the risk that a woman already has. Therefore, women who are already at increased risk of heart disease are likely to be at the greatest risk.”
Dr. Darby and her colleagues provided an example of this in the NEJM article:
In a 50-year-old woman with no cardiac risk factors at baseline, a 3-Gy dose of radiation to the heart would increase her risk of fatal IHD at age 80 from 1.9% to 2.4% (0.5 percentage points) and her risk of having at least 1 acute coronary event from 4.5% to 5.4% (0.9 percentage points).
In a 50-year-old woman with at least 1 cardiac risk factor, a 3-Gy dose of radiation would increase her risk of fatal IHD at age 80 from 3.4% to 4.1% (0.7 percentage points) and her risk of having at least 1 acute coronary event by then by 1.7 percentage points.
In their conclusions, Dr. Darby’s team wrote that because the percentage increase in IHD risk per unit increase in the mean radiation dose to the heart was similar in women with and without cardiac risk factors, one could assume that absolute risk increase at a specific dose was larger for women with preexisting cardiac risk factors.
“Therefore, clinicians may wish to consider cardiac dose and cardiac risk factors as well as tumor control when making decisions about the use of radiotherapy for breast cancer,” they wrote.
Significant decreases in the dose exposure to the heart can be achieved by changing the patient’s position (from supine to prone, for example) and the field in which the radiotherapy is delivered.3,5 Silvia C. Formenti, MD, chair of the Department of Radiation Oncology at NYU Langone Medical Center, in New York City, commented, “There are ways to limit dose radiation to the heart beyond what was available in the Darby study.”
Dr. Darby adds, “Published studies of tangential radiation, without irradiation of the internal mammary chain, indicate that for patients treated in the prone position, the heart is usually receiving about 1 to 2 Gy. This is similar to the heart dose delivered to patients treated in the supine position with breathing control. It remains to be seen which of these 2 methods will become more popular with oncologists.”
“Clearly,” she continues, “modern radiotherapy planning systems, including patient-specific CT scans, have the potential to increase the ability of radiation oncologists to control the dose to the heart more precisely than has been possible in the past.”
As these issues are sorted out, Dr. Darby urges clinicians to stay focused: “Remember that the most important thing is to cover the target tissue adequately. Compromising on coverage of the target tissue in order to reduce the dose to the heart is likely to be a risky practice,” she says.
Breast cancer is the leading cause of cancer deaths in women in the U.S. Survival is better when breast cancer is diagnosed while still local, and 60.8% of women in the U.S. are diagnosed at this stage. In this group of patients, 5-year survival is 98.5%, according to data from the Surveillance, Epidemiology, and End Results (SEER) Program.1 In these cases, surgical treatment with lumpectomy or mastectomy is often followed by radiation therapy.
In fact, a recent meta-analysis of 22 randomized trials provided additional support for the use of postmastectomy radiation in decreasing the rate of mortality related to recurrent cancer and breast cancer in women found to have 1 to 3 positive lymph nodes during mastectomy and axillary dissection.2 As a result of this and other studies, the need to understand the long-term effects of radiation therapy has become more urgent. One of the most important questions is: Does radiotherapy to the chest increase the incidence of ischemic heart disease (IHD)?
The dose of radiation to the breast and heart is now considerably lower than it has been in the past.3 Nonetheless, when malignancies of the right breast are treated with radiation, the heart is typically exposed to a dose of approximately 1 to 2 Gy. Heart exposure is higher for disease of the left breast, of course, and may run up to 10 Gy.4
A recent study assessed how the dose of radiation a woman receives during breast cancer treatment affects her subsequent risk of IHD.
Darby and colleagues performed a case-control study of major coronary events in women who received external beam radiotherapy for invasive breast cancer.4 Major coronary events were defined as myocardial infarction, coronary revascularization, and death from IHD. Their study, recently published in the New England Journal of Medicine (NEJM), included 2168 women who received radiotherapy for breast cancer from 1958 to 2001 in Sweden and Denmark. Of these, 963 women had major coronary events, and 1205 did not and served as controls. Radiation doses to the whole heart and to the left anterior descending artery were estimated based on radiotherapy records.
Mean radiation dose to the heart was 4.9 Gy (range, 0.03 to 27.72). The rate of cardiovascular events increased by 7.4% for each increment of 1 Gy (95% CI, 2.9 to 14.5;P<.001), with no threshold below which there was no risk. This deleterious effect on the heart started within the first 5 years after therapy and continued for at least 20 years. The presence of cardiac risk factors increased the absolute rate of cardiac outcomes but didn’t affect the proportional increase in the rate of major coronary events per Gy.
None of the women in the study received the cardiotoxic chemotherapeutic agents taxanes or trastuzumab, and very few received anthracyclines, thus minimizing these confounders for ischemic outcomes.
Though radiation delivery techniques have improved considerably in recent decades, the incidental exposure of radiation to the heart is always of concern, and strategies to minimize radiation should be exercised whenever possible. Despite this, as Fei-Fei Liu, MD, Professor of Radiation Oncology at the University of Toronto, stated in an editorial that accompanied the Darby article, “It is important to reassure women with breast cancer that with the use of current technologies, the cardiac dose can be decreased considerably, and cardiac risk factors can be better managed.”
Investigator Sarah C. Darby, PhD, of the Clinical Trial Service Unit at the University of Oxford, England, says that “One thing that our studies have shown rather clearly is that any radiation-related risk probably multiplies the risk that a woman already has. Therefore, women who are already at increased risk of heart disease are likely to be at the greatest risk.”
Dr. Darby and her colleagues provided an example of this in the NEJM article:
In a 50-year-old woman with no cardiac risk factors at baseline, a 3-Gy dose of radiation to the heart would increase her risk of fatal IHD at age 80 from 1.9% to 2.4% (0.5 percentage points) and her risk of having at least 1 acute coronary event from 4.5% to 5.4% (0.9 percentage points).
In a 50-year-old woman with at least 1 cardiac risk factor, a 3-Gy dose of radiation would increase her risk of fatal IHD at age 80 from 3.4% to 4.1% (0.7 percentage points) and her risk of having at least 1 acute coronary event by then by 1.7 percentage points.
In their conclusions, Dr. Darby’s team wrote that because the percentage increase in IHD risk per unit increase in the mean radiation dose to the heart was similar in women with and without cardiac risk factors, one could assume that absolute risk increase at a specific dose was larger for women with preexisting cardiac risk factors.
“Therefore, clinicians may wish to consider cardiac dose and cardiac risk factors as well as tumor control when making decisions about the use of radiotherapy for breast cancer,” they wrote.
Significant decreases in the dose exposure to the heart can be achieved by changing the patient’s position (from supine to prone, for example) and the field in which the radiotherapy is delivered.3,5 Silvia C. Formenti, MD, chair of the Department of Radiation Oncology at NYU Langone Medical Center, in New York City, commented, “There are ways to limit dose radiation to the heart beyond what was available in the Darby study.”
Dr. Darby adds, “Published studies of tangential radiation, without irradiation of the internal mammary chain, indicate that for patients treated in the prone position, the heart is usually receiving about 1 to 2 Gy. This is similar to the heart dose delivered to patients treated in the supine position with breathing control. It remains to be seen which of these 2 methods will become more popular with oncologists.”
“Clearly,” she continues, “modern radiotherapy planning systems, including patient-specific CT scans, have the potential to increase the ability of radiation oncologists to control the dose to the heart more precisely than has been possible in the past.”
As these issues are sorted out, Dr. Darby urges clinicians to stay focused: “Remember that the most important thing is to cover the target tissue adequately. Compromising on coverage of the target tissue in order to reduce the dose to the heart is likely to be a risky practice,” she says.
Following on the heels of recent revelations that x-ray mammography may be contributing to an epidemic of future radiation-induced breast cancers, in a new article titled, “Radiation Treatment Generates Therapy Resistant Cancer Stem Cells From Aggressive Breast Cancer Cells,” published in the journal Cancer July 1st, 2012, researchers from the Department of Radiation Oncology at the UCLA Jonsson Comprehensive Cancer Center report that radiation treatment actually drives breast cancer cells into greater malignancy.
The researchers found that even when radiation kills half of the tumor cells treated, the surviving cells which are resistant to treatment, known as induced breast cancer stem cells (iBCSCs), were up to 30 times more likely to form tumors than the nonirradiated breast cancer cells. In other words, the radiation treatment regresses the total population of cancer cells, generating the false appearance that the treatment is working, but actually increases the ratio of highly malignant to benign cells within that tumor, eventually leading to the iatrogenic (treatment-induced) death of the patient.
Last month, a related study published in the journal Stem Cells titled, “Radiation-induced reprogramming of breast cells,” found that ionizing radiation reprogrammed less malignant (more differentiated) breast cancer cells into iBCSCs, helping to explain why conventional treatment actually enriches the tumor population with higher levels of treatment-resistant cells. [i]
A growing body of research now indicts conventional cancer treatment with chemotherapy and radiation as a major contributing cause of cancer patient mortality. The primary reason for this is the fact that cancer stem cells, which are almost exclusively resistant to conventional treatment, are not being targeted, but to the contrary, are encouraged to thrive when exposed to chemotherapy and radiotherapy.
In order to understand how conventional treatment drives the cancer into greater malignancy, we must first understand what cancer is….
What Are Cancer Stem Cells, And Why Are They Resistant To Treatment?
Tumors are actually highly organized assemblages of cells, which are surprisingly well-coordinated for cells that are supposed to be the result of strictly random mutation. They are capable of building their own blood supply (angiogenesis), are able to defend themselves by silencing cancer-suppression genes, secreting corrosive enzymes to move freely throughout the body, alter their metabolism to live in low oxygen and acidic environments, and know how to remove their own surface-receptor proteins to escape detection by white blood cells. In a previous article titled “Is Cancer An Ancient Survival Program Unmasked?” we delved deeper into this emerging view of cancer as an evolutionary throw-back and not a byproduct of strictly random mutation.
Because tumors are not simply the result of one or more mutated cells “going rogue” and producing exact clones of itself (multi-mutational and clonal hypotheses), but are a diverse group of cells having radically different phenotypal characteristics, chemotherapy and radiation will affect each cell type differently.
Tumors are composed of a wide range of cells, many of which are entirely benign.
The most deadly cell type within a tumor or blood cancer, known as cancer stem cells (CSCs),has the ability to give rise to all the cell types found within that cancer.
They are capable of dividing by mitosis to form either two stem cells (increasing the size of the stem population), or one daughter cell that goes on to differentiate into a variety of cell types, and one daughter cell that retains stem-cell properties.
This means CSCs are tumorigenic (tumor-forming) and should be the primary target of cancer treatment because they are capable of both initiating and sustaining cancer. They are also increasingly recognized to be the cause of relapse and metastasis following conventional treatment.
CSCs are exceptionally resistant to conventional treatment for the following reasons
CSCs account for less than 1 in 10,000 cells within a particular cancer, making them difficult to destroy without destroying the vast majority of other cells comprising the tumor.[ii]
CSCs are slow to replicate, making them less likely to be destroyed by chemotherapy and radiation treatments that target cells which are more rapidly dividing.
Conventional chemotherapies target differentiated and differentiating cells, which form the bulk of the tumor, but these are unable to generate new cells like the CSCs which are undifferentiated.
The existence of CSCs explains why conventional cancer treatment has completely missed the boat when it comes to targeting the root cause of tumors. One reason for this is because existing cancer treatments have mostly been developed in animal models where the goal is to shrink a tumor. Because mice are most often used and their life spans do not exceed two years, tumor relapse is very difficult, if not impossible to study.
The first round of chemotherapy never kills the entire tumor, but only a percentage. This phenomenon is called the fractional kill. The goal is to use repeated treatment cycles (usually six) to regress the tumor population down to zero, without killing the patient.
What normally occurs is that the treatment selectively kills the less harmful populations of cells (daughter cells), increasing the ratio of CSCs to benign and/or less malignant cells. This is not unlike what happens when antibiotics are used to treat certain infections. The drug may wipe out 99.9% of the target bacteria, but .1% have or develop resistance to the agent, enabling the .1% to come back even stronger with time.
The antibiotic, also, kills the other beneficial bacteria that help the body fight infection naturally, in the same way that chemotherapy kills the patient’s immune system (white blood cells and bone marrow), ultimately supporting the underlying conditions making disease recurrence more likely.
The reality is that the chemotherapy, even though it has reduced the tumor volume, by increasing the ratio of CSCs to benign daughter cells, has actually made the cancer more malignant.
Radiotherapy has also been shown to increase cancer stem cells in the prostate, ultimately resulting in cancer recurrence and worsened prognosis.[iii] Cancer stem cells may also explain why castration therapy often fails in prostate cancer treatment.[iv]
Non-Toxic Natural Substances Which Target and Kill CSCs
Natural compounds have been shown to exhibit three properties which make them suitable alternatives to conventional chemotherapy and radiotherapy:
High margin of safety: Relative to chemotherapy agents such as 5-fluorouracil natural compounds are two orders of magnitude safer
Selective Cytotoxicity: The ability to target only those cells that are cancerous and not healthy cells
CSCs Targeting: The ability to target the cancer stem cells within a tumor population.
The primary reason why these substances are not used in conventional treatment is because they are not patentable, nor profitable. Sadly, the criteria for drug selection are not safety, effectiveness, accessibility and affordability. If this were so, natural compounds would form an integral part of the standard of care in modern cancer treatment.
Research indicates that the following compounds (along with common dietary sources) have the ability to target CSCs:
Additional research found on the GreenMedInfo.com Multidrug Resistance page indicate over 50 compounds inhibit multidrug resistance cancers in experimental models.
[i] Radiation-induced reprogramming of breast cancer cells. Stem Cells. 2012 May ;30(5):833-44. PMID: 22489015
[ii] Human acute myeloid leukemia is organized as a hierarchy that originates from a primitive hematopoietic cell. Nat Med. 1997 Jul ;3(7):730-7. PMID: 9212098
[iii] Long-term recovery of irradiated prostate cancer increases cancer stem cells. Prostate. 2012 Apr 18. Epub 2012 Apr 18. PMID: 22513891
[iv] Stem-Like Cells with Luminal Progenitor Phenotype Survive Castration in Human Prostate Cancer. Stem Cells. 2012 Mar 21. Epub 2012 Mar 21. PMID: 22438320








{kind=link}