Scientists are testing a new device to help target cancer cells more accurately in ion radiotherapy of head and neck tumours, which could help limit the treatment’s side effects. It includes Timepix3, a small particle detector developed at CERN
Mária Martišíková (left), the project leader from Heidelberg University Hospital and German Cancer Research Center (DKFZ), and DKFZ researcher Laurent Kelleter. (Image: Heidelberg University Hospital / H.Schroeder).
Particle detectors like the ones used by physicists at CERN can have wide applications beyond fundamental research. Scientists from the German National Center for Tumor Diseases (NCT), the German Cancer Research Center (DKFZ), and the Heidelberg Ion Beam Therapy Center (HIT) at Heidelberg University Hospital are now testing a new imaging device supplied by the Czech company ADVACAM on its first patients. The device, which includes a small Timepix3 pixel detector developed at CERN, allows head and neck tumours to be closely monitored during ion radiotherapy, making them easier to target and thus helping limit the treatment’s side effects.
“One of the most advanced methods for treating head and neck tumours involves irradiation with ion beams. This has one unique feature: it can be precisely tailored to the depth inside the human head where the particles should have the maximal effect”, explains Mária Martišíková, the head of the DKFZ team.
Yet like other types of irradiation, ion radiation also has a drawback. The particle beams affect not only the tumour but also part of the healthy tissue around it. This is particularly challenging in the brain, where damage to the optic nerve or a patient’s memory are possible. Ideally, the irradiated area around the tumour should be as small as possible, and the dose to the tumour should be as high as possible. However, current technology does not allow for sufficiently precise targeting of the ions.
To complicate matters further, the situation inside a patient’s head can change during therapy. The x-ray computed tomography (CT) scan image taken before treatment is essentially used as a “map” to target the tumour with ion beams. But during therapy, the situation inside the skull may evolve. Until now, physicians lacked a reliable tool to alert them in case of a change in the brain.
The new ADVACAM device could help solve these issues, by improving the navigation of the ion beams inside the head by tracking the secondary particles that are created when ions pass through it.
“Our cameras can register every charged particle of secondary radiation emitted from the patient’s body. It’s like watching balls scattered by a billiard shot. If the balls bounce as expected according to the CT image, we can be sure we are targeting correctly. Otherwise, it’s clear that the ‘map’ no longer applies. Then it is necessary to replan the treatment,” describes Lukáš Marek from ADVACAM.
“We hope the new device will show us how often and where the tumour changes occur. It will allow us to reduce the overall irradiated volume of tissue, saving healthy tissue and reducing the side effects of radiotherapy. We will also be able to apply higher doses of radiation to the tumour” adds Martišíková.
The treatment can benefit enormously from the additional information obtained from the camera. In the first phase, data could lead to an interruption and replanning of the irradiation series when necessary. The ultimate goal is a system that can correct the path of the ion beam in real-time.
The Timepix3 chip developed at CERN is used in the new ADVACAM imaging device. (Image: CERN)
This device exemplifies successful knowledge transfer, showcasing how technology initially developed for detectors used in fundamental physics research can be applied in healthcare.
“When we started developing pixel detectors for the LHC we had one target in mind – to detect and image each particle interaction and thereby help physicists to unravel the secrets of Nature at high energies. The Timepix detectors were developed by the multidisciplinary Medipix Collaborations whose aims are to take the same technology to new fields. Many of those fields were completely unforeseen at the beginning and this application is a brilliant example of that,” says Michael Campbell, Spokesperson of the Medipix Collaborations.
Stereotactic body radiation therapy (SBRT) treatment is an emerging salvage modality for treating oligometastatic malignant lesions within the retroperitoneum. Appropriate planning target volume (PTV) margins are essential when delivering SBRT to effectively cover the target volume. Spine tracking uses bony spinal anatomy for localization during treatment delivery on robotic linear accelerator platforms. The aim of this study is to quantify the PTV margin needed when spine tracking is used for intrafraction motion tracking when treating retroperitoneal metastatic lesions with robotic SBRT.
Materials and Methods:
A single-institution chart review identified 16 patients with retroperitoneal tumors treated with SBRT over 19 courses in 103 fractions. Daily cone-beam CT images registered based on tumor positioning at the time of treatment were analyzed. Van Herk’s margin recipe was used to calculate the additional PTV margin required if spine tracking was used instead of daily tumor imaging. Patients’ tumors were stratified based on PTV proximity to the vertebral column (≤ 1 cm vs > 1 cm) and location within the retroperitoneum (superior vs inferior to renal artery), with descriptive statistics used to compare the differences of shifts based on location.
Results:
The additional margins calculated by Van Herk’s margin recipe to adequately cover the PTV within the 95% isodose surface for 90% of the entire patient cohort in the vertical, longitudinal, and lateral directions were 2.7, 2.8, and 2.8 mm, respectively. When tumors were stratified by proximity to the vertebral column, average longitudinal ( P < . 001) and total shifts ( P < . 001) were statistically significant.
Conclusion:
When treating retroperitoneal tumors with robotic SBRT, a minimum isometric margin expansion of 5 mm when creating the PTV is recommended if spine tracking is used for intrafraction motion assessment. Target volumes adjacent to the vertebral column may have PTV margins decreased to 4 mm without compromise in target coverage.
Introduction
Oligometastatic disease (OMD) is defined as a distinct cancer state in patients with a low metastatic disease burden in which a curative treatment is possible. 1A frequent location for OMD recurrence after local therapy for cancers of the lower abdomen and pelvis is the retroperitoneal lymph nodes. These nodal basins are comprised of the para-aortic, aortocaval, and paracaval lymph nodes. 2While some retroperitoneal recurrences are amenable to surgical salvage, many patients are either medically fragile and thus poor operative candidates or have a recurrent disease that is technically unresectable.
Stereotactic body radiation therapy (SBRT) has emerged as an attractive nonsurgical salvage option for recurrent tumors in the retroperitoneal region even in the setting of prior radiation therapy treatment. 3An increasing body of evidence suggests that incorporation of SBRT into metastasis-directed therapy of OMD improves patients’ oncological outcomes across a variety of histopathologies. 4 – 9Local control after SBRT in patients with limited OMD within the retroperitoneum has been estimated to be between 75% and 90% with favorable toxicity profiles. 10 – 12
SBRT is predicated on administering large doses of radiation therapy in a limited number of fractions, resulting in a high biologically effective dose delivery to target tissues. In an effort to minimize normal tissue toxicity, SBRT attempts to achieve highly conformal dose distributions with rapid dose falloff. 13An important step in the treatment process for SBRT is the determination of margin size when expanding from either the gross target volume (GTV) or internal target volume (ITV) to the planning target volume (PTV). Appropriate setup margins should account for both systematic errors that influence all fractions of treatment, such as inaccuracies of mechanical equipment and photon beam dosimetry, and random errors such as daily patient setup changes that generally influence only a single fraction. 14If a chosen PTV margin is too small, the GTV or ITV will not fall within the prescription isodose line during the entire treatment delivery, which may underdose the target. Conversely, if a selected setup margin is made exceedingly large, more normal tissue will be unnecessarily irradiated.
SBRT may be delivered across a variety of radiation therapy treatment platforms with diverse image guidance capabilities. The CyberKnife (Accuray Inc.) is a robotic radiation therapy delivery platform that utilizes 2 ceiling-mounted kV x-ray imaging sources with corresponding in-floor image detectors positioned at 45° such that the generated beams intersect orthogonally at an imaging center. 15While the CyberKnife was initially designed as a radiosurgical platform, it is commonly used to treat extracranial sites of diseases, including tumors within the spine, lung, pancreas, liver, and prostate. 16 – 20Target tracking can be accomplished using the CyberKnife platform through multiple methods depending on the site of treatment; however, all utilize the 2 ceiling-mounted kV x-ray imaging sources. While bony anatomy is readily discernible with kV imaging, soft-tissue delineation is suboptimal, thus making direct target tracking unfeasible for many extracranial treatment sites. In place of direct target tracking, adjacent bony structures such as the spine may be used. With this method of tracking, the spine is monitored during treatment and delivery may be interrupted to allow for patient repositioning if necessary. Alternatively, fiducial tracking, which may be used with or without respiratory motion tracking, utilizes small radiopaque markers implanted within or near the tumor and serves as target surrogates identifiable by the kV x-ray imaging sources.
While multiple institutions have previously utilized robotic linear accelerator platforms to deliver SBRT to oligometastatic retroperitoneal lesions, significant variability exists across published literature with respect to treatment planning and delivery. 21 – 26While historically PTV margin determination has been largely institutionally defined, modern cooperative protocols investigating the use of SBRT for ablation of systemic OMD allow between 2 and 5 mm PTV margin additions depending on the site of the disease, immobilization technique used, and institutional setup accuracy. 27 – 29However, there are no prior reports guiding appropriate PTV margin selection when treating retroperitoneal tumors with robotic stereotactic radiation therapy. Thus, the aim of this study is to quantify the PTV margin needed when spine tracking is used for intrafraction motion tracking when treating retroperitoneal metastatic lesions with robotic SBRT.
Materials and Methods
A single-institution chart review was performed that identified consecutive patients > 18 years of age treated with linear accelerator-based SBRT for a single site of retroperitoneal OMD between 2015 and 2023. Patients with multiple courses of SBRT were included if they received treatment at an additional site of retroperitoneal disease > 6 months after their first course of treatment. The retroperitoneal lymph nodes were defined inferiorly at the level of the aortic or inferior vena caval bifurcation and superiorly to the diaphragmatic crura encompassing the para-aortic, aortocaval, and paracaval nodal basins. This study was determined to be exempted by the University of Louisville Institutional Review Board (IRB #22.0219).
To simulate the CyberKnife’s spine-tracking system, daily cone-beam CT (CBCT) images acquired using conventional linear accelerator onboard imaging systems at the time of SBRT treatment were rigidly registered to the treatment planning CT scan, aligned to the patient’s visible disease, and analyzed. Each CBCT was reviewed in Offline Review software (Aria, Varian). A region of interest, including the spine adjacent to the treatment volume but excluding as much soft tissue as possible, was delineated. Rigid registrations were reperformed within Offline Review using the region of interest and a bone intensity window and level so that the position of the spine on the CBCT was aligned to its position on the planning CT as close as possible to emulate the CyberKnife’s spine-tracking system. Per-patient and per-fraction shifts from the treatment position were recorded. Similar methodologies have previously been described and published by our group in a patient cohort receiving lung SBRT. 30
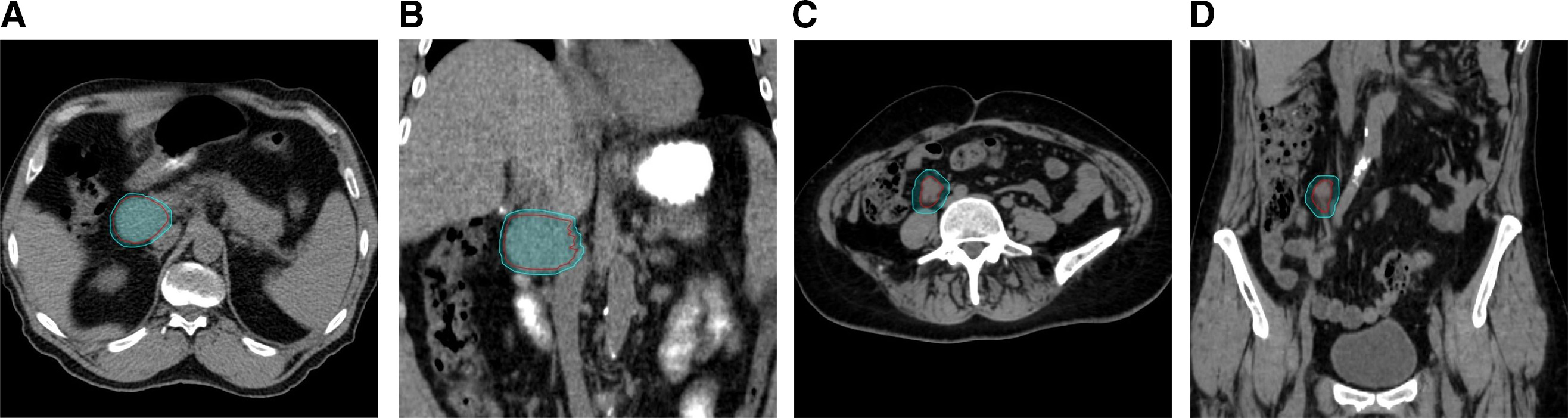
Patients’ tumors were stratified and compared based on proximity to the vertebral column (≤ 1 cm vs > 1 cm) and location within the retroperitoneum (superior vs inferior location to the renal artery). Stratification of tumor location by proximity to the vertebral column using a distance cutoff of 1 cm was selected based on previously published phantom modeling evaluating the use of spine tracking for abdominal tumors showing smaller dose differentials and higher gamma analysis passing rates using acceptance criteria of dose difference and distance-to-agreement of 5%/5 mm at a distance of 1 cm from reference vertebrae. 31The renal artery was chosen to stratify superior vs inferior retroperitoneal tumor locations within the abdomen given its readily identifiable nature on CBCT imaging and was used as a surrogate for target proximity to the diaphragm. Tumors were considered superior to the renal artery if the treatment isocenter was superior to the last slice of either the left or right renal artery, whichever was more superior. Examples of the different types of tumor classifications are demonstrated in Figure 1 .
After chart review completion, per-patient mean shifts and standard deviations were used to calculate group systematic and random standard deviations. Using Van Herk’s margin recipe, additional margins that would adequately treat the patient population if spine tracking were used instead of direct daily tumor imaging by other image guidance techniques were obtained. 32 , 33Van Herk’s recipe calculates the additional margin in the vertical, longitudinal, and lateral directions for each of the tumor classifications using the following formula: 2.5∑ + 0.7σ, where ∑ is the group systematic standard deviation (standard deviation of the per-patient mean shifts) and σ is the group random standard deviation (standard deviation of the per-patient standard deviation of shifts). Formula coefficients of 2.5 and 0.7 were chosen such that the margin would adequately cover the GTV/ITV within the 95% three-dimensional isodose surface for 90% of the patient cohort. With this method, normal probability distributions were assumed for this patient cohort and different sources of error (eg, target delineation inaccuracies, setup error, organ motion) were inferred to be statistically independent. Student t -test was used to determine whether there was any statistical significance to the difference in shift values based on location. The significance level was set at P ≤ 0.02 in alignment with prior investigations by our group. 30Tumor size and absolute shift dimensions across all fractions were compared using the Pearson rank correlation coefficient. Statistical analysis and graphical illustrations were performed in Excel (Microsoft).
Results
Baseline patient characteristics are listed in Table 1 . A total of 16 patients with a single site of retroperitoneal OMD were treated over 19 courses in 103 fractions with SBRT between January 2015 and January 2023 and included for analysis. Genitourinary and gynecological histologies comprised a majority of the patient cohort (63%), with gastrointestinal (25%) and other (12%) histologies comprising a minority. Also, 7 treatment courses had PTVs of ≤ 15 cm 3 (37%) compared with 4 with PTVs of 15-30 cm 3 (21%) and 8 with PTVs of > 30 cm 3 (42%), respectively. A total of 9 courses (48%) had PTV distances located ≤ 1 cm from the vertebral column compared with 10 (52%) > 1 cm. When stratified by tumor location within the retroperitoneum with respect to the renal arteries, 10 courses (52%) had superior retroperitoneal tumor classifications compared with 9 (48%) with inferior tumors. Motion management in the form of a four-dimensional CT (4DCT) scan obtained at the time of CT simulation and an ITV approach was utilized in a total of 12 courses (63%) vs 7 (37%) without. Of the 12 courses where a 4DCT was obtained, 8 were classified as a superior tumor location within the retroperitoneum in relation to the renal arteries, with mean tumor motion in the superior/inferior dimensions of 4.1 mm (range, 2.0-6.1 mm) vs a mean tumor motion of 1.9 mm (range, 0-3.0 mm) for lesions classified as located inferiorly within the retroperitoneum.Table 1.
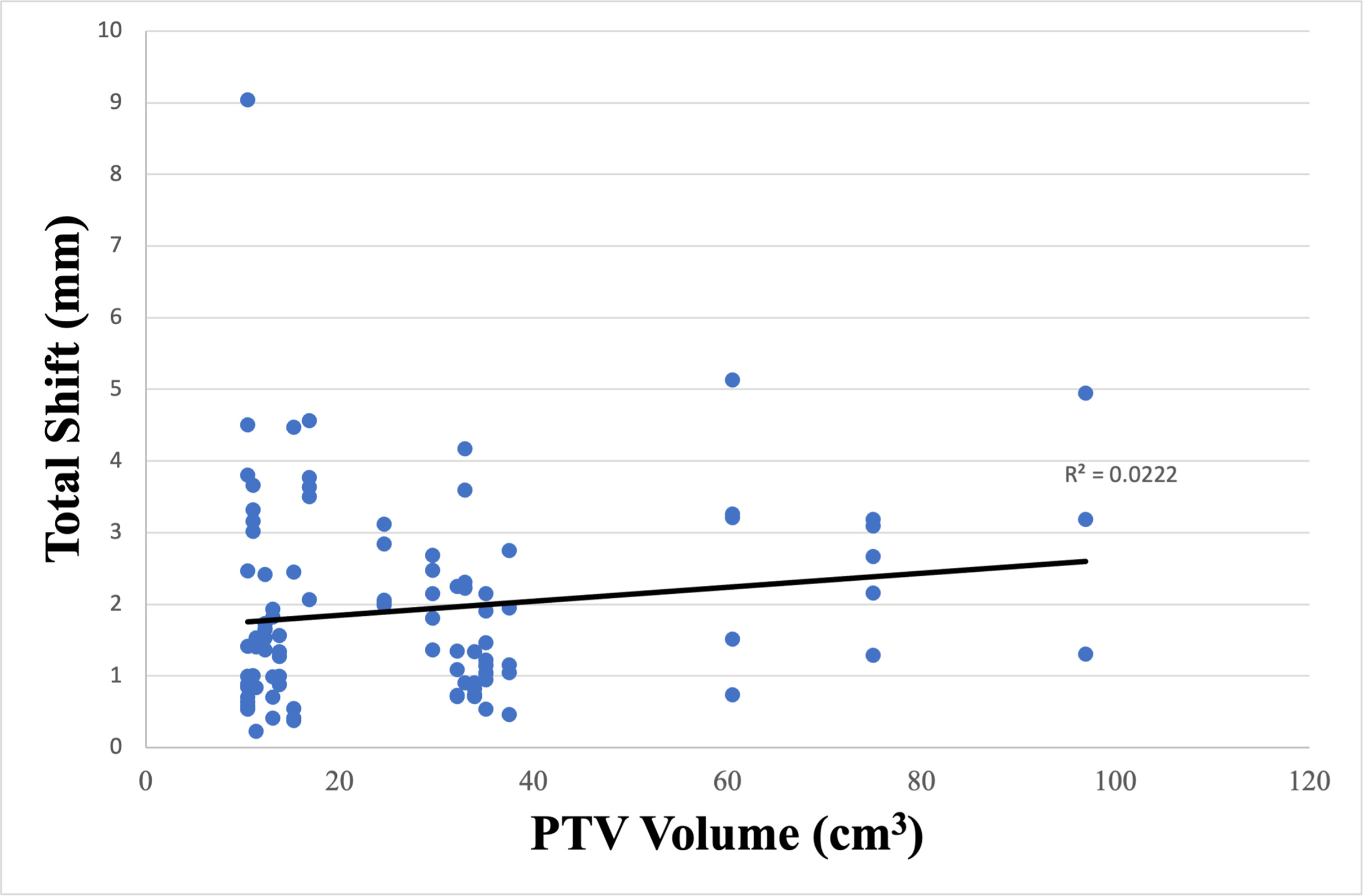
The additional margins calculated by Van Herk’s margin recipe to adequately cover the PTV within the 95% isodose surface for 90% of the entire cohort in the vertical, longitudinal, and lateral directions were 2.7, 2.8, and 2.8 mm, respectively, and shown in Table 2 . The absolute shifts for CBCTs with the maximum total shift based on stratification between tumor location within the retroperitoneum (superior vs inferior) and PTV proximity to the vertebral column (≤ 1 cm vs > 1 cm) are listed in Tables 3 and 4 . Additional analysis was performed to determine the significance of tumor location within the retroperitoneum and proximity to the vertebral column on both unidirectional and total shifts. When stratified by proximity to the vertebral column, only the average longitudinal ( P < .001) and total shifts ( P < .001) were statistically significant and are highlighted in Table 4 . Further analysis was performed to identify any additional factors other than tumor location and proximity to the vertebral column that would affect shifts. The absolute shifts for each tumor were plotted as a function of PTV ( Figure 2 ). No correlation between the magnitude of the shift and PTV size was suggested ( R 2 = .0222).Table 2.
Additional Planning Target Volume Margin Needed Across the Entire Patient Cohort
Vertical (mm)
Longitudinal (mm)
Lateral (mm)
Group systematic standard deviation
.9
.8
.9
Group random standard deviation
.8
1.1
.8
Additional margin
2.7
2.8
2.8
Table 3.
Additional Margin (in mm) Needed When Stratified by Superior vs Inferior Retroperitoneal Classification Using Van Herk’s Margin Recipe With P Values Calculated Using Student t -Test
Classification
Vertical (mm)
Longitudinal (mm)
Lateral (mm)
Total Shift (mm)
Group systematic standard deviation
Superior
.7
.7
.8
.8
Inferior
1.0
1.0
1.0
1.2
Group random standard deviation
Superior
.7
.9
.7
.8
Inferior
1.0
1.3
1.0
1.2
Additional margin
Superior
2.2
2.3
2.4
2.5
Inferior
3.2
3.4
3.3
3.9
P values
–
.073
.474
.598
.834
Table 4.
Additional Margin (in mm) Needed When Stratified by Proximity to Spine (≤ 1 cm vs > 1 cm) Using Van Herk’s Margin Recipe With P Values Calculated Using Student t -Test
Classification
Vertical (mm)
Longitudinal (mm)
Lateral (mm)
Total Shift (mm)
Group systematic standard deviation
≤1 cm
.6
.5
1.0
.6
>1 cm
.8
.9
.8
1.0
Group random standard deviation
≤1 cm
.5
.8
.9
.8
>1 cm
.9
1.4
.7
1.2
Additional margin
≤1 cm
1.9
1.8
3.1
2.1
>1 cm
2.7
3.3
2.5
3.4
P values
–
.056
<.001
.340
<.001
When stratified by location within the retroperitoneum, isometric PTV expansions of 3, 4, and 5 mm would have encompassed 82%, 94%, and 100% of the maximum total shifts for lesions superior to the renal artery vs 78%, 94%, and 98% for lesions inferior. Isometric PTV expansions of 3, 4, and 5 mm would have encompassed 55%, 76%, and 86% of the maximum total shifts for lesions > 1 cm from the vertebral column vs 94%, 100%, and 100% for lesions ≤ 1 cm and shown in Table 5 .Table 5.
Isometric PTV Expansions Accounting for Maximum Total Shifts
Classification
3 mm
4 mm
5 mm
Location (superior vs inferior)
Superior (n = 49)
40 (82%)
46 (94%)
49 (100%)
Inferior (n = 54)
42 (78%)
51 (94%)
53 (98%)
Spine PTV distance (≤ 1 cm vs > 1 cm)
≤1 cm (n = 54)
51 (94%)
54 (100%)
54 (100%)
> 1 cm (n = 49)
27 (55%)
37 (76%)
42 (86%)
Abbreviation: PTV, planning target volume.
Discussion
When utilizing robotic radiation therapy delivery platforms to treat retroperitoneal tumors, target tracking may be performed using either fiducial marker tracking or spine tracking. Fiducial tracking within tumors enables sub-millimeter level of tracking accuracy for small target displacements and is often considered the gold standard for target tracking with robotic radiation therapy delivery platforms. 34However, fiducial marker implantation is not always feasible due to patient medical comorbidities or tumor anatomic location precluding safe implantation. Additional limitations of fiducial tracking are the requirement of at least 3 implanted fiducials to support 6 degrees of freedom (DOF) corrections and added procedural costs. 35
Alternatively, intrafraction target tracking using surrogate structures, such as the spine, may be used. Spine tracking allows monitoring of a reference vertebra without the requirement of fiducial implantation using 6-DOF spatial information. A limitation of using spine tracking as a surrogate for the location of a retroperitoneal tumor is that it assumes the location of the tumor relative to the spine is constant from the time of simulation throughout the duration of treatment. However, treatment uncertainties may be introduced if the distance between the tumor and spine changes between simulation and treatment or if tumor motion patterns vary over time. As a result, an increased setup margin may be necessary, depending on the treatment site, to account for such sources of error. Selection of appropriately sized PTV margins is imperative when delivering high dose per fraction treatment with SBRT. When determining a PTV margin, radiation therapy departments must consider available image guidance within their clinic to ensure accurate dose delivery to target volumes.
Prior to this investigation, within our department, there was no standardized PTV margin addition when robotically treating retroperitoneal metastases with spine tracking. In this study, we found that minimum isometric PTV expansions of 3, 4, and 5 mm would have encompassed 55%, 76%, and 86% of the maximum total shifts for lesions >1 cm from the vertebral column vs 94%, 100%, and 100% for lesions ≤1 cm. Thus, our findings have informed our clinical PTV margin selection when treating with this modality for target lesions adjacent to the spine.
In the context of current literature, there is significant variability in treatment planning and delivery across institutions when treating retroperitoneal metastatic disease with robotic SBRT with spine tracking. Napieralska et al retrospectively reported the use of robotic SBRT using spine tracking to treat prostate cancer recurrences in 18 patients with a total of 31 metastatic lymph nodes located in the retroperitoneal region. 26Treatment doses and fractionation schedules varied, and an isometric GTV to PTV margin expansion of 5 and 4 mm was used in 28 and 3 lesions, respectively. Loi et al retrospectively reviewed 91 patients undergoing robotic SBRT for oligometastatic retroperitoneal failure without fiducial marker placement for pelvic, para-aortic, and upper abdominal lymph node failures. 25An isotropic PTV margin was used and varied between 2 and 5 mm around the GTV, with a median margin of 3 mm selected. Jereczek-Fossa et al analyzed 94 patients receiving robotic SBRT to 124 isolated prostate cancer lymph nodal recurrences in both pelvic and extra-pelvic lymph nodes using spine tracking without fiducial marker placement. 21A 2 mm margin was added to the GTV to obtain the PTV.
Limitations of this retrospective analysis include a small heterogeneous patient cohort treated at a single institution by multiple radiation oncologists over a period of 8 years. During this time, there was no institutionally defined PTV margin added to target volumes receiving SBRT to retroperitoneal sites nor were margins routinely isometric, introducing additional heterogeneity to this study cohort. Further, for purposes of this study, factors influencing group random and systemic errors were assumed to be constant across the entire patient cohort over time. Van Herk’s margin recipe assumes the sample population and sources of introduced error are normally distributed across a given study population. 32However, patient setup errors may not follow a normal distribution if collected over a short period of time in a small sample size. 36
Additionally, motion management was only assessed in a total of 12 treatment courses (63%) of our cohort. It has been reported that the diaphragmatic motion of abdominal lesions may reach 40 mm even during shallow respiration cycles. 37Van Herk’s margin recipe attempts to calculate the necessary additional PTV margin to ensure adequate dose coverage to a defined clinical target volume (CTV), which includes both gross disease in addition to subclinical microscopic disease. When utilizing SBRT, the generation of a CTV from a GTV or ITV is often omitted. Additionally, when using a 4DCT to generate an ITV, internal target motion is accounted for within treatment volumes, thus reducing the potential source of both systematic and random errors. Within this study population, a 4DCT/ITV approach was utilized in a total of 12 of 19 courses when delivering SBRT. At our institution, when treating extrathoracic sites of disease with SBRT, use of 4DCT imaging at the time of CT simulation is left to the discretion of the treating radiation oncologist. Thus, a large portion of this study cohort without known internal target motion may underestimate this potential source of error. However, even when using a 4DCT, further treatment uncertainties may arise from interfraction and intrafraction changes of organ motion, motion from unpredictable respiratory cycles, as well as variations between the imaging and treatment sessions.
We identified no significant differences in unidirectional and total shifts when tumors were stratified based on superior or inferior location to the renal arteries. The renal artery was chosen to stratify superior vs inferior retroperitoneal tumor locations within the abdomen given its readily identifiable nature on CBCT imaging. However, this is an unvalidated surrogate for target proximity to the diaphragm and respiratory cycle tumor motion. Within the contexts of this study, use of this landmark for such purposes should be viewed as hypothesis generating and requires additional validation.
Chan et al suggested that when robotic SBRT for lung cancers is delivered with spine tracking, unless effective means are employed to reduce tumor motion, caution should be undertaken when treating tumors with motion of more than 10 mm due to temporal dose variations from considerable intrafractional target motion. 38Technical discussions regarding Accuray’s Xsight Spine Tracking system utilized by our clinic are beyond the scope of this report but are explained further in detail by Ho et al. 39Future directions of study for this topic by our group include analyzing dosimetric variables for both organs at risk (OARs) and targets when utilizing the additional calculated Van Herk’s margins when treating retroperitoneal sites of disease with robotic SBRT.
Lastly, clinical judgment should be deferred to the treating physician for PTV margin selection in close collaboration with medical physics and dosimetry and performed on a per-patient basis accounting for the size of the treated lesion and proximity to OARs. Nonisometric PTV expansions are also appropriate and frequently used in clinical practice, which varies based on the treating institution. When selecting a setup margin, clinicians must weigh the likelihood of increased treatment-related morbidity from higher integral dose to adjacent normal structures for larger setup margins vs potential target underdosing if smaller margins are used.
Conclusions
When treating retroperitoneal tumors with robotic SBRT, an isometric PTV margin expansion of 5 mm is recommended if spine tracking is used for intrafraction motion assessment. Target volumes located near the vertebral column may have PTV margins decreased to 4 mm without compromising target coverage. Additional factors such as target motion, dose per fraction size, and institutional quality assurance should be considered for patient-specific PTV margin expansions.
RedHill Biopharma Ltd. announced the publication of data showing that opaganib, an investigational new drug, protects against radiation-induced lung inflammation and fibrosis in an in vivo mouse model of lung damage following exposure to ionizing radiation, demonstrating its potential use as a medical countermeasure against nuclear irradiation and in cancer radiotherapy. Data from multiple experiments was published in the International Journal of Molecular Sciences.
Radiation-induced inflammation is known to occur in two phases – in an initial inflammatory response immediately after irradiation and in a delayed response that can occur weeks later. As such, one of the experiments looked specifically at longer-term survival with two treatment windows: 1-3 days post-radiation and 31-45 days post-radiation. The opaganib group treated both during the initial and delayed phases of inflammation demonstrated a highly statistically significant improvement in survival at Day 180 (60% survival compared with 10% for controls, p=0.008). Thus, treating with opaganib during both initial and delayed phases of inflammation provided the greatest improvement in survival.
“The data, when looked at collectively across multiple experiments, demonstrate that opaganib significantly improved long-term survival associated with reduced lung fibrosis, suppression of granulocyte infiltration, and reduced expression of IL-6 and TNFα in an in vivo model of lung damage following exposure to ionizing radiation,” said Dr. Lynn W. Maines, lead author of the publication and VP of Research at Apogee Biotechnology Corporation, RedHill’s development partner for opaganib. “These data further demonstrate that sphingolipid metabolism is a critical regulator of fibrogenesis, and specifically show that opaganib suppresses radiation-induced pulmonary inflammation and fibrosis.”
Opaganib is being tested as a potential treatment for Acute Radiation Syndrome (ARS), following selection by the US government National Institutes of Health’s (NIH) Radiation and Nuclear Countermeasures Program (RNCP) for its radiation medical countermeasures Product Development Program. Opaganib was also recently selected for inclusion into the BARDA/NIH Chemical Countermeasures screening program for Sulfur Mustard exposure. Opaganib, a novel, oral, small molecule pill with a five-year shelf-life, is easy to administer and distribute, supporting potential central government stockpiling for use as a medical countermeasure in the event of mass casualty nuclear radiation incidents or Sulfur Mustard attack, if approved by the US Food and Drug Administration (FDA).
Whether concurrent chemotherapy with radiotherapy (CRT) is effective for elderly patients with head and neck cancer is a controversial topic. This study aimed to analyze the effectiveness of CRT vs. radiation therapy (RT) among elderly patients in Japan.
Methods
Data from the Head and Neck Cancer Registry of Japan were extracted and analyzed. Patients with locally advanced squamous cell carcinoma of the oropharynx, hypopharynx, or larynx who received definitive CRT or RT between 2011 and 2014 were included.
Results
CRT was administered to 78% of the 1057 patients aged ≥ 70 years and 67% of the 555 patients aged ≥ 75 years. For the patients aged ≥ 75 years, the overall survival (OS) rate was significantly better in the CRT group than in the RT group (P < 0.05), while the progression-free survival (PFS) rate was not significantly different (P > 0.05). The add-on effect of CRT was significantly poor in elderly patients (P < 0.05), and it was not a significant factor in the multivariate analysis for patients aged ≥ 75 years. After propensity score matching, there were no significant differences in the OS and PFS rates between the patients aged ≥ 70 years and those aged ≥ 75 years (all, P > 0.05).
Conclusion
Although aggressive CRT is administered to elderly patients in Japan, its effectiveness is uncertain. Further prospective randomized trials are needed to verify whether CRT is superior to RT alone for elderly patients.
Ultra-high-dose-rate radiation treatment found safe and effective for pain relief in small trial of patients with metastatic cancer
SAN ANTONIO
FLASH radiation treatment – which delivers therapeutic doses of radiation in a fraction of a second – may hold promise as a potential treatment for tough-to-kill tumors, a first-in-human study in a small number of people with bone cancer suggests. The technology, previously tested in animals, was shown to be as safe and appeared to be as effective as conventional radiation without causing unexpected side effects. Findings of the FAST-01 trial (NCT04592887) will be presented today at the American Society for Radiation Oncology (ASTRO) Annual Meeting.
“Our study shows FLASH radiotherapy with protons is a practical modality to reduce pain,” said Emily C. Daugherty, MD, lead author of the study and an assistant professor of clinical radiation oncology at the University of Cincinnati Cancer Center. “It deserves further exploration because of its potential to decrease the side effects associated with conventional radiation treatments.”
FLASH radiotherapy (RT) delivers radiation at dose rates that are more than 300 times higher than those used in conventional radiation treatments. This induces a phenomenon known as the FLASH effect, which reduces the harm that may occur to normal tissue surrounding a tumor during conventional radiation therapy, while still killing the cancer cells at the tumor site.
“Because FLASH radiotherapy is given at ultra-high dose-rates, it appears to cause less normal tissue injury. This offers the possibility of delivering larger doses of radiation – which could result in higher cure rates for patients with resistant tumors – without increasing side effects,” said John Breneman, MD, FASTRO, principal investigator on the trial and a professor of radiation oncology and neurosurgery at the University of Cincinnati Cancer Center.
Most early research on FLASH RT used electron beams to deliver the radiation, but these beams don’t penetrate very deep into tissue, limiting its applicability for this treatment approach. Using proton beams for ultra-high dose-rate radiation allows for penetration sufficient to reach tumor locations in most people. While pre-clinical trials with animals suggested FLASH-RT could safely deliver high doses of radiation with fewer harmful side effects, prior to the FAST-01 trial, the treatment had never been tested under a clinical trial in humans.
In this study, ultra-high-dose-rate radiation was delivered to 10 patients, ages 27-81 years, each with one to three painful bone metastases in their extremities. Treatments were delivered to a cumulative 12 metastatic sites in patients’ arms and legs. Patients were given 8 Gy of radiation in a single fraction, delivered at ≥40 Gy per second via a FLASH-enabled proton therapy system. Pain, use of pain medications and adverse events were measured on the day of treatment, 15 days following treatment, and at one, two and three months following treatment. Researchers continued measuring these results every two months for up to 13 months. The median follow-up was 4.8 months.
Researchers chose patients who would have received conventional radiation therapy at the same dose as they were given with FLASH RT. “We used the exact same regimen, but with FLASH dose-rate radiation. The patient experience is the same as it would have been receiving conventional radiation, only the treatment delivery process is shorter,” said Dr. Daugherty.
Following FLASH RT, seven of the 10 patients experienced complete or partial pain relief. Of the 12 treated sites, pain was relieved completely for six sites and partially for two additional sites. Temporary pain flares occurred in four of the 12 sites treated.
Side effects from treatment were mild. Four patients experienced mild skin hyperpigmentation (darkening skin tone), one experienced skin discoloration, two experienced mild limb edema (swelling or puffiness), two experienced pruritis (itchy skin), one experienced fatigue, one experienced erythema (reddening of the skin) and one experienced extremity pain.
Each FLASH treatment takes about 3/10 of a second, Dr. Daugherty explained. Following treatment, “both pain relief and side effects were in-line with what might have happened with conventional radiation. We did not see any unexpected additional toxicity with the substantially shorter treatment.”
FLASH RT would potentially be most useful in treating hard-to-kill cancers in the brain, lungs or gastrointestinal area, where healthy tissue surrounding tumors is particularly vulnerable to radiation exposure, said Dr. Breneman. However, clinical trials in these sites cannot be authorized until studies show ultra-high dose-rate radiation is safe and effective in other, less-sensitive areas. The FDA limited its approval for this study to adults with bone metastases in their arms and legs, areas at much lower risk should complications arise.
“From a practical standpoint, this is not the type of cancer that FLASH is designed to treat, but we need human data to see if there are any unexpected side effects. Treating arms and legs is not as risky as treating someone’s brain or lungs,” said Dr. Breneman, who he also serves as medical director of the Cincinnati Children’s/UC Medical Center Proton Therapy Center.
Ultimately, FLASH RT could also be useful in treating pediatric cancers, since children are more sensitive to the side effects of radiation therapy, he said. But much more research needs to be done before that can occur.
Researchers don’t fully understand why FLASH RT kills tumors with fewer side effects than conventional radiation and further research is needed to determine the biological mechanisms driving the FLASH effect, said Dr. Daugherty.
Next, the research team will test the safety and efficacy of FLASH RT with patients who have metastases closer to the lungs and heart. The FAST-02 trial (NCT05524064) is currently enrolling adult patients with thoracic bone metastases.
Ultra-high dose rate (FLASH) radiotherapy is a new way of treating tumours caused by cancer. Higher doses of radiotherapy are associated with trauma to the healthy tissue surrounding the tumour, whereas FLASH radiotherapy demonstrates a sparing effect of the healthy tissues without compromising the anti-tumour action. Dr Kristoffer Petersson at the Oxford Institute for Radiation Oncology, University of Oxford, along with collaborators Joseph D. Wilson, Ester M. Hammond and Geoff S. Higgins, review the available data on FLASH radiotherapy and its clinical potential in the treatment of cancer.
One in every two people in the UK born after 1960 is estimated to be diagnosed with some form of cancer during their lifetime. Radiotherapy (a non-invasive radiation treatment which damages and kills tumour cells) forms part of the treatment in 30-50% of these cases. Unfortunately, radiotherapy also damages the healthy tissue surrounding the tumour. Treatment success is dependent on delivering a high enough dose of radiation to destroy the tumour cells without causing severe trauma to the surrounding tissues. FLASH radiotherapy (FLASH-RT) is a new technique, involving treatment of tumours at ultra-high dose rates which actually reduces the trauma to normal tissue around the tumour, whilst equalling the anti-tumour effect of conventional dose rate radiotherapy (CONV-RT). However, very little is known about the mechanisms behind the FLASH effect.
Kristoffer Petersson and his colleagues at the Oxford Institute of Radiation Oncology, aim to better understand these mechanisms in the hope of bringing us closer to a successful implementation of FLASH technology in our radiotherapy clinics.
Ultra-high dose rate (FLASH) radiotherapy is a new way of treating tumours caused by cancer.
Tissue toxicity It was first noted in the 1960s that non-cancerous cells exposed to ultra-high dose rates of radiotherapy were more likely to be viable than those exposed to conventional dose rates. This has been more recently supported by studies in mice, one of which demonstrated much less lung damage in the chests of mice treated with FLASH-RT compared to those treated with CONV-RT. In another study, mice exposed to whole brain irradiation at conventional dose rates performed much worse in recognition tests compared to those treated at ultra-high dose rates. Radiation-induced skin reactions can include reddening and breakdown and have been shown to be much reduced in rodents being treated with FLASH-RT compared to CONV-RT. FLASH-RT also compared favourably in one study comparing the skin reaction of a mini-pig to different dose rates of radiotherapy. Another study involving treatment of nasal cancer in cats with FLASH-RT showed complete remission of tumours with minimal trauma to surrounding tissues.
Researching the FLASH effect is of value to establish how it can be used in a clinical scenario to treat cancer patients.
Anti-tumour response Many studies demonstrate that in addition to reducing tissue toxicity, FLASH-RT also produces the same tumour response as CONV-RT. One such study compared mice with breast cancer and head and neck carcinoma grafts which had been exposed to either FLASH-RT or CONV-RT; there was no difference in treatment success between the two methods. In another study, mice were inoculated with cancer cells into their lungs, then later irradiated and CT-scanned to measure tumour size. The tumours of the mice treated with FLASH-RT were smaller than those treated with CONV-RT. There is therefore some evidence that FLASH-RT may even produce a superior anti-tumour response to CONV-RT.
Influencing factors There are multiple factors that could influence the FLASH effect, including dose rate, total dose, pulse rate, fractionation, and modality of radiation. The dose rate needed for the FLASH effect may also vary depending on the affected tissue and the delivery method. Many studies vary in the total dose of radiation used, or use doses unattainable in clinical scenarios, which complicate the findings. The source of the radiation is also a factor, as the FLASH effect has been mostly observed following the use of electron linear accelerators. More recently, the FLASH effect has also been seen following the use of proton and X-ray radiation. Pulsing the radiation at a high frequency can induce a FLASH effect, at a suitable dose-per-pulse. Further study is needed to confirm the key parameters for inducing the FLASH effect, as there are so many variables at play.
Kristoffer Petersson’s research lab aims to identify the mechanisms behind FLASH radiation, with a view to finding the optimum way of implementing the technique in clinical practice.
Oxygen depletion Exactly why the FLASH effect occurs is not yet fully understood but has been hypothesised. Hypoxic tissues (tissues that are deprived of oxygen) are more resistant to radiation (and therefore less likely to become damaged) than well-oxygenated tissues. It is therefore thought that the difference in tissue toxicity between FLASH-RT and CONV-RT may be due to the level of hypoxia at ultra-high dose rates and subsequent radioresistance transferred to the irradiated tissue.
Immune modification Another proposed theory for the FLASH effect is a modified immune response − as it involves a shorter treatment time, less lymphocytes (white blood cells involved in the immune system) are affected by the radiation. One study reported less immune system activation in mice following FLASH-RT compared to CONV-RT. It should be noted that it is unclear if any immune response following FLASH-RT is contributing to the FLASH effect or caused by it. Other biological responses such as DNA damage and inflammation could also be contributing, and more studies are needed for clarification.
Clinical applications Ultimately, researching the FLASH effect is of value to establish how it can be used in a clinical scenario to treat cancer patients. It could be used in the clinic to allow for an increase of total dose in the treatment of tumours resistant to radiation that are currently associated with worse patient outcomes, as a higher dose could be used without the associated surrounding tissue toxicity of CONV-RT. It could also be used in situations where radiotherapy offers good tumour control but is associated with tissue toxicity as the same dose could be administered but with less toxicity than that of CONV-RT. The clinical viability of FLASH-RT in practice is complicated by inconsistencies, lack of clarity and limitations in the various studies performed. Some also do not have a control group irradiated with CONV-RT for comparison.
FLASH radiotherapy demonstrates a sparing effect of the healthy tissues without compromising on anti-tumour action.
One human patient has been treated with FLASH-RT. He had an aggressive form of lymphoma and had previously been treated with CONV-RT which caused severe reactions to the skin surrounding the cancerous lesions and took months to heal. One lesion was successfully treated with FLASH-RT and had only mild redness and inflammation around the area treated. Although a promising outcome, this study only involved one patient and therefore allowed for limited comparison between the two methods of radiotherapy.
Electron linear accelerators have been the source of the radiation in most studies demonstrating a FLASH effect. Clinical linear accelerators can be modified to deliver FLASH-RT with electrons, which would allow for the translation into clinical trials. A limitation of this is the depth of tissue which can be treated, which is restricted to a few centimetres with these electron beams. A solution would be to use higher energy electron beams, which can have improved depth penetration. Using electromagnets, the beam can theoretically be focused to the volume of tumour, resulting in dose-to-target conformity with a single beam, comparable to that of modern X-ray techniques. A single beam delivery such as this may prove essential in producing the FLASH effect; however, these beams are currently exclusive to research accelerators which are either very great in size or associated with low pulse rate, small beam size, and stability issues.
The FLASH effect offers superior tissue protection in comparison to CONV-RT without compromising on tumour treatment.
One recent study demonstrated that X-ray tubes could potentially be used in FLASH-RT studies. These are small, relatively cheap and available in clinical practice. They are also limited by depth penetration to a few millimetres of tissue and only have a small beam size. Synchrotrons are a type of particle accelerator which are another potential source and have similar beam energies as X-ray tubes, as well as the possibility of using spatially fractionated ultra-high dose rate microbeam radiation therapy (MRT). The combination of MRT and the FLASH effect have been shown to achieve superior clinical effects in small animal models compared to conventional X-ray or CONV-RT dose rates in a range of cancers. Synchrotrons are of limited availability due to being very large and expensive.
PHASER (Pluridirectional High-energy Agile Scanning Electronic Radiotherapy) is another concept for using FLASH-RT in the clinic. Part of this is a technique involving image-guidance. Image-guidance techniques are necessary for clinical FLASH-RT treatment of deep tumours, regardless of the delivery mode used. The PHASER concept is still in development and relies on further advances in technology. A clinically available method of treating deep-seated tumours with FLASH-RT is to use proton beams, although they are both costly and sizeable. Clinical proton beams have good depth penetration and can produce accurate dose distributions with single or few beams. These are likely to be used in future clinical trials in FLASH-RT.
The FLASH effect offers superior tissue protection in comparison to CONV-RT without compromising on tumour treatment. It has been studied across various species and now a single human case has been documented. While its mechanism of action is likely to involve oxygen depletion, it is not fully understood and therefore requires further study. The doses required to achieve the FLASH effect make it unsuitable for many clinical cases. Furthermore, the availability of radiation sources capable of producing suitable beams for treatment of both superficial and deep tumours is a limiting factor in clinical trials. If further study yields more understanding of the biological mechanisms of the FLASH effect, it may be possible to achieve it at lower doses, increasing its clinical viability.
What are the next steps in understanding more about the biological mechanisms of FLASH-RT?
There are many studies that still need to be performed for us to better understand the biological mechanisms responsible for the highly beneficial FLASH sparing effect. In Oxford, we aim to perform real time oxygen concentration measurements in cells and in mice during FLASH irradiation, in order to verify (or discard) oxygen depletion as a main explanation of the effect. Most FLASH studies to date have been in vivo studies. For a better understanding of the biological mechanisms of FLASH-RT, several more specific in vitro studies are needed, for example investigating levels of DNA damage and DNA damage response.
There may be a faster, less-painful way to use radiation against cancer.
The first-in-human trial of FLASH radiotherapy found the experimental treatment to be safe and effective — suggesting that there may be a faster, less painful way to use radiation against cancer.
The status quo: Radiation therapy is a common cancer treatment that uses high doses of radiation to kill or slow the growth of cancer cells. Usually, this is done by aiming a beam of radiation directly at a tumor for a few minutes. This part of the process is painless, like getting an X-ray.
Patients typically undergo daily treatments five days a week for several weeks, and including setup time, a treatment usually takes about 15 to 30 minutes.
With traditional radiation therapy, dosages may have to be limited to avoid painful side effects.
The challenge: By shrinking a tumor, radiation therapy can not only fight cancer, but also potentially relieve patients’ pain or other symptoms caused by it. But the beam of radiation can damage healthy tissue near the tumor, too, causing pain and other side effects.
To minimize these adverse effects, doctors have to limit the radiation dosage, which may reduce how effective the treatment is at fighting the cancer.
“[FLASH radiotherapy] offers the possibility of delivering larger doses of radiation, which could result in higher cure rates.”JOHN BRENEMAN
The FLASH effect: FLASH radiotherapy is a promising alternative to traditional radiation therapy.
It delivers a dose of radiation that’s over 300 times higher than traditional radiation therapy in just a fraction of a second. This induces something called the “FLASH effect” — a not-entirely-understood phenomenon in which the radiation still attacks the tumor, but doesn’t harm surrounding tissue.
“This offers the possibility of delivering larger doses of radiation — which could result in higher cure rates for patients with resistant tumors — without increasing side effects,” said John Breneman, principal investigator of the new trial.
In animal studies, FLASH radiotherapy has been shown to be safe and just as effective as traditional radiation therapy without causing unexpected side effects. Now, a University of Cincinnati-led team has shared the results of FAST-01, the first-in-human trial of the treatment.
One FLASH radiotherapy treatment lasts just 0.3 seconds.
The trial: The primary goal of the trial was to prove that FLASH radiotherapy is safe for people and has a feasible workflow. A secondary goal was to determine its efficacy by measuring how much pain relief it provided patients.
The trial included 10 patients with painful cancerous growths in the bones of their arms or legs. Each received one FLASH radiotherapy treatment — lasting just 0.3 seconds — at the site(s) of their cancer.
Their pain, use of pain meds, and adverse effects were measured the day they received the therapy, 15 days later, and one, two, and three months after treatment.
“We did not see any unexpected additional toxicity with the substantially shorter treatment.”EMILY C. DAUGHERTY
The results: Patients’ average time on the table was just 15.8 minutes per treated site — demonstrating that the workflow is feasible — and of the 12 total cancer sites treated, pain was fully relieved in six and partially relieved in two others.
“[B]oth pain relief and side effects were in-line with what might have happened with conventional radiation,” said lead author Emily C. Daugherty. “We did not see any unexpected additional toxicity with the substantially shorter treatment.”
Looking ahead: Ultimately, the researchers believe FLASH radiotherapy would be most useful for treating cancers in the brain, lungs, or gastrointestinal area, as the tissues around those tumors are particularly vulnerable to damage from traditional radiation therapy.
It could also be useful for treating cancers in children, who are more sensitive to the side effects of radiation therapy.
Since the limb treatments didn’t produce any unexpected side effects in people, they’ve begun enrolling patients in FAST-02, a trial that will target cancerous growths in the bones of the thorax, which surround the heart and lungs.
Dr. Deb Schrag is a gastrointestinal oncologist at MSK and Chair of the Department of Medicine. A clinical trial she led shows that people diagnosed with locally advanced rectal cancer can be safely treated without radiation therapy. The new method reduces side effects that can lessen quality of life.
Even a successful treatment can be improved, to give patients more options, including fewer side effects.
Radiation-Free Rectal Cancer Treatment Clinical Trial Results
The trial involved more than 1,100 people with locally advanced rectal cancer, meaning it had not spread to other organs. After five years, the research found that people who received a type of chemotherapy regimen called FOLFOX alone before surgery did just as well as those who underwent both chemotherapy and radiation before surgery. Skipping radiation could mean improvements in patients’ quality of life, including the preservation of fertility, sexual function, and more.
Dr. Schrag says: “There are around 47,000 people diagnosed with rectal cancer every year. We believe around 20,000 of them — who have stage 2 or 3 cancer — could benefit from this approach that can spare them from having to get radiation in addition to chemotherapy and surgery.”
Side Effects From Standard Treatment for Rectal Cancer
Typically, a person diagnosed with rectal cancer will receive radiation to the pelvic area given together with 5FU chemotherapy, either intravenously (in the vein) or orally (in the mouth). This strategy is known as chemoradiation and is sometimes referred to as 5FUCRT. The next steps are surgery to remove the tumor and, usually, more chemotherapy to keep the cancer from coming back in a distant organ.
“We’ve used chemoradiation since 1990 because it’s been remarkably effective at reducing the rate of local recurrences in the pelvis,” Dr. Schrag says. “This is critical because pelvic recurrence of rectal cancer is difficult to treat and causes much suffering. Since 2004, we have given the chemoradiation before surgery.”
But Dr. Schrag and colleagues wondered if they could get the same outcomes without subjecting patients to the side effects radiation often causes in such a complex region of human anatomy.
The rectum is the last six inches of the digestive system. It sits inside the pelvis, which is a crowded neighborhood of bone and tightly packed organs. Radiating this area can damage reproductive organs, cause infertility, and lead to early menopause in women, among other side effects.
“My colleagues and I began seeing more young women with rectal cancer who were devastated — not just because they had cancer but because the standard treatment we had to offer them would mean that they would not be able to carry a pregnancy to term,” Dr. Schrag says. “That was one of the big reasons we looked for a way to help patients and to see if we could achieve favorable outcomes without the uniform application of radiation.”
Dr. Schrag believes these issues are particularly urgent today because a growing number of people are diagnosed with rectal cancer at young ages — when fertility concerns are especially important. MSK is a leader in trying to find out why rectal cancer is rising among younger adults and established the first center in the world devoted to their specific needs: the Center for Young Onset Colorectal and Gastrointestinal Cancer.
People facing rectal cancer, Dr. Schrag says, are often concerned about other long-term consequences of radiation, which can impair (damage or weaken) bowel and sexual function.
There are also concerns about radiation and bone marrow, which makes blood. “Most of your bone marrow is made in the pelvic bones. When you radiate those bones, the bone marrow resilience can be impaired,” she says. That’s important, she adds, because “if the cancer comes back, it’s more difficult to give you chemotherapy if your bone marrow reserve is impaired.”
The PROSPECT Clinical Trial for Rectal Cancer: Replacing 5FUCRT With FOLFOX
Dr. Schrag and colleagues decided to turn the standard-of-care treatment on its head to address concerns about side effects.
The seed for the clinical trial idea started to sprout during MSK Colorectal Service meetings, where specialists from across disciplines discuss complex cases of rectal cancer. “MSK colorectal surgeon Martin Weiser, MD; gastrointestinal oncologist Leonard Saltz, MD; radiologist Marc Gollub, MD, and I launched a pilot trial to test the effectiveness of the idea,” Dr. Schrag says. “It was a small study of just 30 patients, but it enabled us to persuade our colleagues nationally to test the approach in a randomized trial.”
The chemotherapy regimen that is usually given after surgery for rectal cancer is called FOLFOX, which includes the drugs 5-fluorouracil (5FU), oxaliplatin, and leucovorin. Preliminary research showed that giving FOLFOX before surgery could also have good results, which Dr. Schrag confirmed in a pilot trial.
She hypothesized that giving FOLFOX alone before surgery — without radiation — could provide patients with the same good outcomes as the standard of care.
The trial, named PROSPECT, had two arms. One arm used FOLFOX chemotherapy before surgery and only used radiation if the response to FOLFOX alone was not sufficient (this happened for less than 10% of patients). The other arm used chemoradiation before surgery.
More than 1,100 patients were evenly split between the two arms, with patients participating at medical centers around the U.S. and Canada.
After five years, the results were clear: The patients who received only FOLFOX before surgery did just as well as the patients who received chemoradiation. Major endpoints, including disease-free survival, overall survival, and the rate of cancer recurrence, were nearly identical between the two methods.
The new method showed other benefits. For instance, the number of patients who needed a temporary ostomy was lower when radiation was not used. An ostomy is a surgically created hole in the abdomen (belly) that allows waste to be transported to a pouch outside the body. Ostomies are usually temporary for patients with rectal cancer that has not spread, but finding that fewer patients needed them at all after treatment with the new method was a definite improvement in quality of life.
Radiation for Rectal Cancer May Still Be Necessary for Some
Dr. Schrag is careful to point out that while the new method offers patients and doctors another option, in some cases radiation before surgery is still preferred. “In about 10% of cases, the person did not respond well enough to the FOLFOX regimen, and we administered chemoradiation,” she says.
Also, FOLFOX chemotherapy alone before surgery requires longer rounds of treatment, which can mean more side effects initially, including neuropathy of the hands — numbness or sharp pain.
Chemotherapy and surgery do have side effects, Dr. Schrag says, but this study found that patients with rectal cancer have options that don’t involve radiation. “Particularly for people concerned about radiation affecting their fertility,” she adds, “the new FOLFOX regimen presents an alternative.”
A Patient’s Successful Treatment Without Radiation Therapy
Having treatment options was important to Marc Scarduffa. He felt healthy and symptom-free when he underwent his first colonoscopy at age 50. (At the time, 50 was the recommended age to begin colorectal screening. It has since been lowered to 45 for people at average risk.)
Marc was stunned when the test revealed a stage 3 rectal cancer tumor. Marc had spent much of his career leading government relations for a major pharmaceutical company and was well-versed in medical issues. “I started at another hospital, but I insisted on MSK because it’s the gold standard.”
At MSK, Marc was cared for by Drs. Saltz and Weiser. Marc says their compassion and concern for his quality of life immediately reassured him. “I had been planning a big 50th birthday party in Italy, and Dr. Saltz said: ‘Go and enjoy it. We’ll start when you come back.’ That made such a difference, to spend time with family and friends.”
On Marc’s return, Drs. Saltz and Weiser told him about the clinical trial of treatment without radiation. “I had heard from several people about side effects they endured with radiation,” Marc says. “I was very happy to have an opportunity to not get radiation and instead just have FOLFOX and surgery.”
For Marc, the chemotherapy had only minor side effects. “Most people didn’t know I had cancer,” he says. “I was very enthusiastic about not having to lose my hair to radiation, and I continued to travel often for work.” After recovering from surgery, Marc returned to health and says the clinical trial was definitely the right option for his care.
“I’m such a big fan of MSK, and I’ve told several other people facing cancer to go there. I felt a real bond with my doctors.”
Radiation-Free Rectal Cancer Treatment Can Help Patients in Rural Areas
The new method may also benefit patients who face challenges of geography in addition to their cancer diagnosis.
“If you live in Idaho or Montana or many other rural parts of America, you may be many hours away from anywhere you can receive radiation treatment,” Dr. Schrag says. Chemoradiation requires 28 daily visits over five and a half weeks. In comparison, FOLFOX requires about six visits over 12 weeks. “For some people, the schedule and convenience are important.”
That benefit is magnified globally, because radiation treatment facilities are scarce in some countries, Dr. Schrag says. “In some parts of the world, access to radiation is very limited. Chemotherapy may be a more accessible alternative.”
Collaboration Is Key to Breakthrough Discoveries
This research was funded by the National Cancer Institute, a federal effort that is part of the National Institutes of Health. “These are your taxpayer dollars at work,” Dr. Schrag says. “This is the kind of work that only the government will fund because there is no commercial sponsor.”
Making use of those resources to accomplish the PROSPECT trial was possible “because of strong leadership from different disciplines,” she adds. “Management of rectal cancer is a team sport.”
The PROSPECT team included Dr. Weiser (Colorectal Surgery); Ellen Hollywood, RNP (Nursing); Dr. Saltz (Medical Oncology); Dr. Karyn Goodman (Radiation Oncology, now at Mount Sinai); Dr. Gollub (Radiology); and Jinru Shia, MD (Pathology).
Dr. Schrag says her deepest thanks go to the courageous patients who participated in the trial. “It’s not easy to say to a patient, ‘Let’s try treating you by omitting a treatment that has been used for over two decades,’ ” she says. “My hope is that this treatment approach will give people with rectal cancer and their doctors a new option. At MSK, our mission is to keep pushing the boundaries to make meaningful differences for our patients.”
More than a million European children undergo a CT scan each year. Ionizing radiation at moderate (> 100 mGy) to high (> 1 Gy) doses is a recognized risk factor for malignant hematopathies. The risk associated with exposure to low doses (< 100 mGy), typically delivered during a CT scan in children or adolescents, is unknown.
Previous studies assessed the risk for malignant hematopathies related to ionizing radiation from CT scans in young patients. Some showed an increased risk for leukemia with repeated scans, but confounding factors resulted in a lack of statistical power or biases in some cases. The EPI-CT study, coordinated by the International Agency for Research on Cancer, aimed to evaluate the cancer risk among children and adolescents after exposure to low doses of ionizing radiation during CT scans.
A European Cohort
A recent article presents an assessment of observed malignant hematopathies following CT scan. The authors followed a multinational European cohort of 948,174 patients who had a CT scan before age 22 years. Ionizing radiation doses to the bone marrow were evaluated based on the scanned body region, patient characteristics, scan year, and the technical parameters of the machine. The analysis involved 876,771 patients who underwent 1,331,896 scans (an average of 1.52 per patient) and were followed for at least 2 years after the first scan.
In total, 790 malignant hematopathies were diagnosed, including 578 lymphoid hematopathies and 203 myeloid hematopathies and acute leukemias. The average follow-up period was 7.8 years. At the time of diagnosis, 51% of patients were under the age of 20 years, and 88.5% were under the age of 30 years. There was an association between cumulative dose and the observed malignant hematopathy, with an observed rate of 1.96 per 100 mGy (790 cases).
This rate corresponds to a 16% increased rate per scan (for a dose observed per scan of 8 mGy). A higher rate for any type of malignant hematopathy was observed for doses > 10 mGy, with an observed rate of 2.66 for doses > 50 mGy, compared with doses < 5 mGy.
The rate of malignant hematopathy increased with older age at the time of radiation exposure, particularly for lymphoid observations. The rate in the 5- to 9-year age group and the > 10-year age group was, respectively, two times and three to four times higher than that in the < 5-year age group. The rate decreased over time, with the highest observed rate between 2 and 5 years after ionizing radiation exposure and the lowest after 10 years.
CT Scans Must Be Warranted
This study, which involved nearly a million patients, has higher statistical power than previous studies, despite missing or approximate data (including that related to actually delivered doses). An association was shown between cumulative dose to the bone marrow and the risk of developing malignant hematopathy, both lymphoid and myeloid, with an increased risk even at low doses (10-15 mGy).
The results suggest that for every 10,000 children examined today (with a dose per scan of 8 mGy), 1-2 could develop a radiation-related malignant hematopathy in the next 12 years (1.4 cases). This study confirms the higher risk for cancer at low radiation doses and emphasizes the importance of justifying each pediatric CT scan and optimizing delivered doses. It is important to recall that an MRI or ultrasound can sometimes be an adequate substitute for a CT scan.
Nearly half of all cancer patients undergo radiation therapy as part of their care. Ionizing radiation, or the emission of high-energy waves or particles, works as a therapy by damaging a cancer cell’s DNA. It’s an effective tool for killing cancer cells because they are generally much less adept at DNA repair compared to healthy cells. Damaging specific parts of DNA prevents cancer cells from reproducing, effectively killing them.
A major limitation of radiation therapy is the damage it may cause as it passes through healthy organs to get to tumors located deep in the body. The need to protect healthy organs limits the dose of radiation that can be delivered to cancerous tissue, thereby reducing the chance of successful treatment.
Overcoming this challenge has long been a mission for medical physicists and radiation oncologists like us. Improvements to radiotherapy will enable clinicians to not only better control tumors overall, but also open the door for more favorable outcomes in patients with cancers that are more resistant to radiation.
Fundamentals of radiation therapy
At the heart of radiation therapy lies the fundamental principle that cancer cells are more susceptible to radiation than healthy cells. However, there are exceptions. Sometimes resistance to radiation in cancer cells may be comparable or even greater than that of their neighboring cells.
When tumors lie close to vital organs that are highly sensitive to radiation, such as the brain or the bowels, it significantly limits the amount of radiation that can be delivered. In cases where tumors are significantly less sensitive to radiation than the organs surrounding it, radiotherapy may not be the best choice. Radiation therapy involves directing strong beams of energy to kill cancer cells.
Patient immobilization is another key aspect to reducing toxicity from radiation. Patients need to be completely motionless during treatments to ensure that the beam of radiation mainly targets tumors and not the healthy tissues surrounding them. If a patient moves during treatment, it can mean the radiation beam is partly or even entirely missing the cancer target. This scenario both underdoses the cancer and increases the risk of harming healthy tissue.
There are a few common types of radiotherapy that deliver radiation in different ways:
External beam radiation therapy
External beam radiation involves directing radiation from an outside source to a single part of the body.
Linear accelerators, commonly referred to as LINACs, are currently the most common technology used in radiation treatments. These machines generate beams of high-energy electrons and X-rays that can be aimed at cancer tissue with precision. The high energy of these beams allows in-depth penetration into the body to reach tumors.
Another form of radiotherapy is proton beam therapy, or PBT, which directs protons instead of X-rays at tumors. Currently, PBT is only available at a limited number of locations. It is typically recommended for specific populations such as pediatric patients because, unlike X-rays, it has an adjustable range that minimizes the effects of radiation on organs beyond the target area, potentially reducing toxicity.
Image-guided radiation therapy
In the early 2000s, researchers incorporated CT scanners into LINACs. This enabled real-time imaging of the patient’s anatomy just before or during treatment. By acting as the eyes of the care team, imaging reduced uncertainty about the location of tumors and improved the precision and accuracy of radiation therapy.
Newer linear accelerators are now incorporating MRIs, which significantly improve visualization of patient anatomy and tumors, further advancing treatment precision and accuracy.
Patients need to stay still during radiotherapy to ensure the beam stays on course.
Researchers are also adding positron emission tomography, or PET, scanners that provide information about the metabolic function of tumors. This advance makes it possible to increase the radiation dose specifically at the most active areas of tumors.
Adaptive therapy
An emerging approach to radiation therapy called adaptive therapy uses imaging to dynamically adjust treatment as the tumor or its positioning changes each day.
In conventional radiation therapy, patients receive the same treatment plan across multiple treatment sessions. However, adaptive therapy may apply several adjustments or lead to a completely new treatment plan in order to address changes to the tumor’s condition over the course of treatment.
Historically, the concept of adaptive therapy was more theoretical than practical. It faced many challenges, including a lack of suitable imaging technologies. Additionally, creating a treatment plan involves heavy computational work and collaboration among various specialties within a care team. The fact that the process needs to be repeated multiple times renders adaptive therapy particularly resource-intensive and time-consuming. However, researchers are looking into ways to use artificial intelligence to automate some of these steps to make this approach more practical.
Brachytherapy
Brachytherapy – stemming from the Greek word “brachys,” meaning “short” – is another widely used method in radiation therapy. It involves placing a radioactive source called a seed near or directly inside a tumor or affected area, reducing the distance from the radiation source to its target.
In contrast to external beam radiation therapy, where radiation often must pass through healthy tissue to reach cancer cells, brachytherapy applies radiation directly to the tumor. This technique is particularly advantageous for certain cancer types that are accessible through noninvasive or minimally invasive procedures, such as skin cancers, gynecological tumors and genitourinary tumors.
By placing the radioactive source inside the body, brachytherapy can target tumors more directly than external beam radiotherapy. Cancer Research UK/Wikimedia Commons, CC BY-SA
The conventional approach to brachytherapy involved using needles to place or inject radioactive seeds inside or adjacent to the cancerous tissue. These seeds would remain in the body either temporarily or permanently, with the goal of irradiating the area at a low dose over a long period of time.
An increasingly popular form of brachytherapy called high-dose rate brachytherapy involves using a tube to guide a more highly radioactive seed directly to the affected tissue before removing it after a few minutes. The seed emits a high dose of radiation in a short period of time, which enables clinicians to treat patients quickly in an outpatient setting.
Future of radiation therapy
Radiation therapy is continually evolving to more effectively and precisely treat cancer.
For example, a technique that delivers radiation at an ultra-high rate called FLASH-RT has shown promise in its ability to increase dosages without excessive toxicity. Researchers are also exploring treatments using ions heavier than protons to more effectively damage DNA in cancer cells and enhance the efficacy of radiation therapy.
Advances in the field hint at a future of more personalized radiation therapy, highlighting the fusion of technology and medical expertise in the fight against cancer.













{kind=link}