An investigational, point-of-care rectal expulsion device may help determine whether patients with chronic constipation will improve with pelvic floor physical therapy, according to data presented at Digestive Disease Week 2022.
“[Rectal expulsion device (RED)] was specifically designed to simplify and pull the tertiary care paradigm of anorectal function testing downstream to any general gastroenterologists’ medical office for patients with chronic constipation,” Eric D. Shah, MD,MBA, assistant professor at Dartmouth College Geisel School of Medicine and Dartmouth-Hitchcock Medical Center in New Hampshire, told Healio.
From May 2020 to June 2021, Shah and colleagues enrolled patients who were referred to general gastroenterology, met Rome IV criteria for functional constipation and failed fiber/laxatives for more than 2 weeks. Thirty-nine patients were included in the feasibility phase to develop use-case protocol, 60 were enrolled in the subsequent blinded validation phase and 52 patients (mean age, 46.9 years; 94.2% women) were included in the intention-to-treat analysis.
Participants were evaluated after insertion of the single-use, self-inflating RED, with time to expel measured in a left lateral position. Patients who failed to expel RED within 120 seconds then attempted to expel the device in a seated position.
All patients participated in pelvic floor physical therapy, and at 12 weeks investigators measured outcomes, which included global clinical response (Patient Assessment of Constipation Symptoms score reduction > 0.75 vs. baseline), improvement in health-related quality-of-life (HRQoL; Patient Assessment of Constipation-Quality of Life score reduction > 1) and complete spontaneous bowel movement frequency (CSBM).
Results showed RED predicted clinical response [generalized area under the curve (gAUC) = 0.67; 95% CI, 0.58-0.76], HRQoL response (gAUC = 0.67; 95% CI, 0.58-0.77) and CSBM response (gAUC = 0.63; 95% CI, 0.57-0.71) in the left lateral position. An abnormal RED in this position, defined as expulsion within 5 seconds or after more than 120 seconds, predicted 48.9% clinical response to physical therapy vs. 8.9% with normal RED.
According to researchers, adding a subsequent seated maneuver strengthened the predicted clinical response (71.1% among patients retaining RED > 13 seconds).
“We demonstrated that RED appears capable of predicting patient outcomes with pelvic floor physical therapy delivered in the community, thereby allowing gastroenterologists to rapidly triage care for patients with chronic constipation and help patients break the cycle of ineffective, rotating fiber and laxatives,” Shah said.
A history of COVID-19 nearly doubled the odds of having very short sleep, according to results from a large U.S. study presented at SLEEP 2022.
“Few studies have focused on factors associated with sleep quantity and quality,” Marie-Rachelle Narcisse, PhD, lead study author and assistant professor at the University of Arkansas for Medical Sciences Northwest, said.
Further, she added, no studies have been conducted on a large, nationally representative sample of the U.S. population nor have any been multidimensional.
Before the COVID-19 pandemic, 24% of Americans had insomnia, Narcisse said. Now, 40% are affected, prompting The Sleep Foundation to coin the terms “coronasomnia” and “COVID-somnia.”
Narcisse and colleagues used data from the 2020 National Health Interview Survey to examine the association between past COVID-19 diagnosis and sleep health among 17,713 adults. Participants were asked about sleep quantity (the number of hours of sleep in a 24-hour period) and sleep quality (trouble falling or staying asleep).
According to Narcisse, 4.2% of study participants had a positive COVID-19 diagnosis and of these, 3.1% had very short sleep (4 hours or less), 24.2% had short sleep (5-6 hours), 59.9% had healthy sleep (7-8 hours) and 12.8% had long sleep (9 hours or more).
The study also showed that 37.0% had trouble falling asleep some days, 10.9% had trouble most days, and 6.5% every day. In addition, 33.7% had trouble staying asleep some days, 13.9% most days and 6.6% every day.
“A history of COVID-19 almost doubled the odds of having very short sleep — less than 5 hours,” Narcisse said. “However, there were no significant associations between a past diagnosis of COVID-19 and other sleep quantity categories and trouble falling and staying asleep.”
“It is important for health care professionals to consider a history of COVID-19 when addressing sleep deprivation in their patients,” she concluded.
The FDA has extended the approval of Dupixent to include children aged 6 months to 5 years with moderate to severe atopic dermatitis, Regeneron Pharmaceuticals and Sanofi announced in a press release.
“We’ve had Dupixent now for the past few years, but there are many children who are under 6 who are also suffering from atopic dermatitis,” Amy S. Paller, MD, primary investigator at Northwestern University’s Skin Disease Research Center, told Healio. “It’s been great to have some new studies come out that show it’s just as efficacious and that the safety is the same.”
The FDA has extended the approval of Dupixent to include children aged 6 months to 5 years with moderate to severe atopic dermatitis.
The approval was based on phase 3 data that found 200 mg or 300 mg of Dupixent (dupilumab), based on body weight, plus low-potency topical corticosteroids resulted in clear or almost clear skin in 28% of patients, compared with 4% of those treated with placebo. Overall disease severity improved by at least 75% in 53% of patients, compared with 11% of placebo-treated patients and a clinically meaningful reduction in itch was achieved in 48% of those treated with Dupixent, compared with 9% of those treated with placebo.
Amy S. Paller
Dupixent is the first biologic approved to treat atopic dermatitis in individuals from infancy to adulthood.
“Until today, treatment options in the U.S. for infants and children under the age of 6 suffering from moderate to severe atopic dermatitis have been limited to topical steroids — which may be associated with significant safety risks when used long-term. This has left patients and their caregivers in desperate need of medicines that can better address the chronic, long-term nature of the disease,” Naimish Patel, MD, senior vice president and head of global development in immunology and inflammation at Sanofi, said in the release. “These young people, and their families, often struggle to cope with the significant impact itch can have not only on the body, but on many other facets of daily life. This approval means that Dupixent, with its well-established safety and efficacy profile, is now available to some of the youngest people living with this disease.”
The drug’s safety profile in this younger age group was similar to the safety profile in the 6 years and older group, with hand, foot and mouth disease and skin papilloma being the most common treatment emergent adverse events recorded.
“We are not seeing any new red flags, and that means we have a systemic that even though it is injectable, it doesn’t need any lab testing. Safety is what speaks volumes to those of us who treat pediatric patients and certainly to the families of those patients,” Paller said.
The use of H1 or H2 antihistamines may mitigate some side effects of peanut oral immunotherapy, but they did not influence quality of life, according to a study published in TheJournal of Allergy and Clinical Immunology: In Practice.
Future trials should explore safer approaches to food allergy treatment that improve quality of life, Derek K. Chu, MD, PhD, of the department of medicine at McMaster University in Hamilton, Ontario, Canada, and colleagues wrote.
Source: Adobe Stock
The randomized, three-arm, parallel-design, placebo-controlled Peanut Immunotherapy Starting in Canada, Evaluation and DiScovery, or PISCES, trial involved 43 patients (mean age, 7.8 years; age range, 5 to 11 years; 65% boys) with peanut allergy being treated with OIT at Hamilton Health Sciences’ McMaster Children’s Hospital.
Researchers assigned 10 patients to “double placebo” with placebo OIT and placebo premedication, 16 to peanut OIT with placebo premedication and 17 to peanut OIT with antihistamine premedication.
The patients assigned to antihistamine premedication before their OIT received 2.5 mg of desloratadine, a second-generation H1 antihistamine, in 5 ml by mouth once a day or 75 mg of ranitidine, an H2 blocker, in 5 ml by mouth twice a day.
The risk for experiencing at least one adverse event was higher among those treated with OIT vs. the double-placebo group, whether they received OIT with antihistamines (HR = 3.75; 95% CI, 2.79-4.72) or with placebo (HR = 4.62; 95% CI, 3.61-5.62).
However, premedication with antihistamines before peanut OIT reduced the number of moderate or severe adverse events compared with OIT without antihistamines (1.9 vs. 4.2 events per patient; incidence rate ratio [IRR] = 0.46; 95% CI, 0.24-0.89).
Still, both OIT groups saw increases in their rates of moderate or severe adverse events compared with the double-placebo group at 0.9 events each (OIT without antihistamines, IRR = 4.65; 95% CI, 2.02-10.73; OIT with antihistamines, IRR = 2.16; 95% CI, 1.01-4.6).
According to the researchers, reductions in urticaria drove these differences, with fewer events per patient on peanut OIT with antihistamines (0.6 vs. 2.1; IRR = 0.28; 95% CI, 0.1-0.8) and on double placebo (0.7 vs. 2.1; IRR = 3.04; 95% CI, 1.17-7.88) compared with patients on peanut OIT without antihistamines.
The participants on peanut OIT with antihistamines experienced numerically, but not significantly, fewer abdominal pain events than those on OIT without antihistamines (2.6 vs. 4.6; IRR = 0.61; 95% CI; 0.27-1.37), with both OIT groups experiencing more events than the 0.8 observed in the double-placebo group.
Additionally, the antihistamine premedication increased incidence of neuropsychiatric events, primarily tiredness and dizziness, compared with placebo premedication (3.35 vs. 1.06; IRR = 3.16; 95% CI, 1.84-5.42).
After 12 months, mean quality-of-life scores were 4.36 (standard deviation [SD], 1.1) for the participants on peanut OIT and antihistamines, 3.28 (SD, 0.99) for those on peanut OIT and a placebo, and 3.63 (SD, 0.62) for those in the double-placebo group, which suggested small or no differences between the groups. Reviews of specific scores pertaining to emotional impact, food anxiety and social and dietary limitations yielded similar results.
These results suggest that adverse events caused by OIT are not the only factors impacting quality of life, the researchers wrote. Also, they continued, antihistamines do not have enough of an impact on adverse events to significantly improve quality of life.
Although antihistamines do not increase the costs of oral immunotherapy, their addition to an already complex regimen should be weighed against their modest benefits and their potential for adverse effects, according to the researchers.
Future research should investigate safer food allergy treatment approaches that improve patient and family quality of life, the researchers concluded, noting that the OUtMATCH study will explore the use of omalizumab (Xolair; Genentech, Novartis) with peanut oral immunotherapy.
These results are not too surprising. However, I have not used antihistamines as part of an OIT treatment protocol, as I have not wanted it to become a “crutch” or mask symptoms. Ultimately, we want patients to consume foods and doses safely without the need of other medications. I have used antihistamines in conjunction with OIT for other reasons such as environmental allergies or eczema, but they were used for that purpose and not OIT.
One interesting finding in the study was that concurrent treatment with antihistamines reduced moderate to severe but not mild OIT-induced adverse events, and yet it did not lead to important improvements in quality of life. Further, there were additional adverse effects such as sedation and dizziness in the antihistamine group.
Overall, it does not seem that adding antihistamines moved the needle much. I also think the quality-of-life assessments and conclusions were not thorough. First, there was no indication of what quality-of-life measures were accounted for. Second, they only did a baseline assessment and then another assessment 4 weeks after the desensitization. This does not allow much time for the participants to really understand the difference that OIT may have made. Third, the maximum doses achieved in this study imply that the patient would not have been allowed to free-eat foods after OIT. If this is the case, then that would likely affect quality-of-life scores. So, I think these aspects should be more carefully evaluated before drawing conclusions.
I think this study shows that OIT can be performed without antihistamines and that they are not needed as part of a protocol. Rather, they can be used to control concurrent allergic disorders such as environmental allergies or eczema.
Further research is needed into quality-of-life assessments with varying maintenance doses of OIT and after patients have been in maintenance for a longer period and incorporating foods more regularly into their diets. Also, as the article suggests, similar research with biologics may show different results as well.
Douglas H. Jones, MD
Cofounder of Global Food Therapy
Cofounder and President of Food Allergy Support Team
Director of Rocky Mountain Allergy at Tanner Clinic
Healio Allergy/Asthma Peer Perspective Board Member
Diabetes technology continued to advance in 2020, and the pace of change is accelerating.
Even with unprecedented shifts in health care delivery brought on by the COVID-19 pandemic, the FDA this year cleared expanded indications for a smart insulin pen, a next-generation continuous glucose monitor and an interoperable insulin pump, allowing a customized automated insulin delivery system. In December 2019, the FDA authorized marketing of the Tandem Diabetes Care Control-IQ interoperable, automated insulin dosing algorithm, the first dosing controller that can be used with other interoperable diabetes devices. The move has been praised by experts as part of a new era of diabetes technology.
“As someone who has worked in the field of diabetes for many years, we don’t usually talk about game changers every year. But this year, we are,” Robert Gabbay, MD, PhD, FACP, chief scientific and medical officer for the American Diabetes Association, told Endocrine Today. “This is lessening the burden of having diabetes. That is a goal we are all striving for. It is challenging to have diabetes, and we ask more and more of our patients. To have technology where we are actually asking less of them, wow.”
“Game changing” diabetes technology is allowing physicians to ask for less effort from their patients with diabetes, according to Robert Gabbay, MD, PhD, FACP.
The latest iterations of popular diabetes devices — smaller and longer-wearing sensors for CGM, “smarter” insulin delivery systems and advanced decision-support tools using artificial intelligence technology — are likely to be rolled out with greater frequency as the pace of change quickens. The ongoing COVID-19 pandemic, which pushed an almost overnight reliance on telehealth for care, only served to underscore the importance of advanced technology, according to experts; endocrinologists, in particular, now look to diabetes devices more than ever before to help patients manage glucose levels and guide decision-making.
“Things in diabetes technology are now moving like smartphones — every September, you expect to see a new iPhone — and in the diabetes field, that is going to be the expectation, that you see something new,” Viral Shah, MD, associate professor of medicine and pediatrics at the Barbara Davis Center for Diabetes and the School of Medicine at the University of Colorado Anschutz Medical Campus, told Endocrine Today. “People never imagined that things would move this fast. To say there will be something new every year, that is a huge change, and it is a move in the right direction.”
Hybrid closed-loop advancements
In January, Tandem Diabetes Care announced the commercial launch of its t:slim X2 insulin pump with Control-IQ technology, which combines the Dexcom G6 CGM with an insulin pump to regulate insulin levels with little user effort. It is the first system that adjusts basal insulin levels and delivers automatic bolus doses to prevent hyperglycemia or hypoglycemia.
In June, the FDA cleared an expanded pediatric indication for the t:slim X2 interoperable insulin pump, lowering its indicated age for use by children from 14 years to 6 years.
“The first big splash this year was the approval of Control-IQ, which came out in December 2019,” Carol J. Levy, MD, CDCES, clinical director of the Mount Sinai Diabetes Center and investigator in the NIH-sponsored study, told Endocrine Today. “That offered many new clinical features. The Medtronic 670G was a great initial device to be released, but this system is incrementally more robust for several reasons. No. 1, no finger-stick calibrations are required to make sure the device works appropriately. No. 2, the system provides automated correction doses when needed during the day. No. 3, the system allows the entry of sleep/wake cycles to maximize glucose control at different times of day. And No. 4, the system allows for extended bolusing for higher-fat meals, improving meal dosing flexibility for some patients.”
In September, the FDA approved the Medtronic MiniMed 770G system, a next-generation hybrid closed-loop insulin delivery system for children aged 2 to 6 years with type 1 diabetes. The 770G system, which builds on the success of Medtronic’s 670G, is intended to automatically monitor glucose and provide appropriate basal insulin doses with little or no input from users or their caregivers; it is the first legally marketed device that can automatically adjust insulin delivery based on CGM for a young pediatric population.
Viral Shah
Medtronic is launching the 770G first as a separate device, with plans to release the full-featured 780G in the U.S. Medtronic secured a CE mark for the 780G in Europe in June. In the U.S., the 780G is for investigational use only.
In the FLAIR study, the first randomized, crossover study to a compare the MiniMed 780G with the 670G, adolescents and young adults with type 1 diabetes reported a greater reduction in daytime hyperglycemia and greater ease of use with the next-generation model. The findings, presented at the ADA Scientific Sessions in June, showed participants’ time spent with glucose levels above 180 mg/dL fell from a mean of 42% at baseline to 34% and 37%, respectively, when using the 780G and the 670G, for a difference of three percentage points (P < .001).
Within the cohort, 56 participants received the 780G for 12 weeks and 57 participants received the MiniMed 670G for 12 weeks, before switching to the other device.
Percentage of time in range, defined as a blood glucose levels between 70 mg/dL and 180 mg/dL, increased from a baseline level of 57% to 67% with the advanced hybrid closed-loop and 63% with the 670G. The number of participants achieving the international time-in-range consensus target of greater than 70% went up nearly threefold from baseline when using the advanced hybrid closed-loop compared with increasing almost twofold when using the 670G.
“Each one of these systems offers different advantages, and each one is improving with each generation,” Bruce A. Buckingham, MD, emeritus professor of pediatrics and endocrinology at Stanford Children’s Health Center, Stanford University, and the Lucile Salter Packard Children’s Hospital, told Endocrine Today. “The new MiniMed system is a nicely aggressive system. It has a glucose target down to 100 mg/dL. If the active insulin time is set to 2 hours, a lot of people achieve close to 80% time in range. When that is available with a nonadjunctive sensor, and there is Bluetooth connectivity so parents can have remote monitoring, that is a significant advance.”
Buckingham presented pilot study results at the ADA Scientific Sessions this year from the Omnipod 5/Horizon automated insulin delivery system (Insulet), which employs a tubeless, on-body waterproof pump with an embedded algorithm. The pump receives communication by Bluetooth from a Dexcom continuous glucose sensor. The algorithm has customizable glycemic targets from 110 mg/dL to 150 mg/dL, which can be programmed to vary throughout the day. Users experienced a blood glucose level less than 70 mg/dL less than 1% of the time and had a mean time in range 70mg/dL to 180 mg/dL more than 70% of the time. A pivotal multicenter study for submission to the FDA has now been completed, Buckingham said.
“We use the pod for a lot of children, particularly younger children, since it is waterproof, is not ‘tethered’ and has an automatic inserter, so the child never sees and insertion needle,” Buckingham said.
Bruce A. Buckingham
Work on a bionic pancreas is also moving forward. In December 2019, the FDA granted breakthrough device designation to Beta Bionics’ investigational iLet bionic pancreas system. iLet is a pocket-sized, wearable medical device designed to autonomously control glucose levels with on-body wear similar to an insulin pump, according to the company. Unlike insulin pump therapy, however, the investigational system is designed for users to enter only their body weight for the bionic pancreas to initialize therapy, with no need to count carbohydrates, set insulin delivery rates or deliver bolus insulin for meals or corrections.
The bionic pancreas is designed to function as three medical devices in one. It can be configured as an insulin-only bionic pancreas, a glucagon-only bionic pancreas or a bihormonal bionic pancreas using insulin and glucagon.
“Right now, we are limited in where we can set targets for blood glucose levels and how to individualize those targets,” Laura M. Nally, MD, FAAP, a pediatric endocrinologist and instructor of pediatrics in the division of pediatric endocrinology at Yale University School of Medicine, told Endocrine Today. “With diabetes, your settings need much more fine-tuning than what we are currently able to do. That is why many people move to the do-it-yourself [closed-loop insulin delivery] world, because you can individualize targets for exercise, menstrual cycles, sick days, etc. The next step for these hybrid closed-loop systems is to learn what your needs are and respond without the person with diabetes intervening.”
Next-gen CGM, sensors
Six personal CGM options are currently available in the U.S. from four companies: Abbott’s Freestyle Libre Flash CGM, Dexcom’s G5 and G6, Medtronic’s Guardian Connect and Guardian 3, and the Eversense implantable CGM (Senseonics).
In September, Abbott announced its next-generation FreeStyle Libre 3 received a European CE mark. The newest CGM features the smallest, thinnest CGM sensor — the size of two stacked pennies, according to Abbott — as well as a more environmentally sustainable system design and the longest-lasting, self-applied CGM available at 14 days (vs. 10 days with other CGMs). The newest device will be priced the same as previous generations, according to Abbott.
“I look forward to when the Libre 3 makes it to the U.S., as well as the other devices now in development from other companies,” Levy said. “Glucose sensors have different bells and different whistles for different patients. Maybe a patient wants a device that isn’t beeping a lot, like the Libre 2. Maybe they want something private that goes directly to their phone, so they pick Dexcom. Maybe they prefer something implantable, so they select Eversense. There is also the Medtronic sensor that is compatible with the Medtronic pump. The Libre is now compatible with smartphones, too. These are all exciting steps allowing us to engage more patients to use this technology. If something does not work for them, now we have the opportunity to offer them two or three other devices.”
Carol J. Levy
Dexcom’s next-generation G7 sensor is also in development. In February, Dexcom and Insulet announced a global commercialization agreement to combine current and future Dexcom CGMs with Insulet’s Omnipod Horizon system for automated insulin delivery, currently in pivotal trials, according to a press release. Under the terms of the nonexclusive agreement, the Omnipod Horizon automated insulin delivery system will use sensor values from the Dexcom G6 and next-generation G7 CGM, once available, to predict glucose levels and automatically adjust the insulin dose required for optimal glucose management.
“The future of CGM — as with many things in technology — is to get smaller and last longer,” Buckingham said. “The G7 will be a much smaller sensor and disposable. There is a new sensor we are just beginning to start clinical studies on that will last 16 days with nonadjunctive use, with a new company. Medtronic getting to nonadjunctive use is also a great plus.”
Future of tech
The latest advancements — along with the pace of change — has researchers excited for what may come next.
Buckingham said technology that can recognize when a person is eating a meal could further alleviate diabetes burden. At Stanford, Buckingham and colleagues are leading a pilot study to examine whether the Klue app is effective in detecting missed or late meal boluses in patients with type 1 diabetes. The app is programmed onto an Apple Watch and will detect potential missed boluses from hand motion. It will send text alerts to the user asking if they have taken their insulin.
“We’ve done studies with Klue and an Apple Watch worn on the dominant hand, which would recognize eating with about three gestures of moving hand to mouth,” Buckingham said. “It was about 95% accurate, with only two or three false positives per week. It even distinguished drinking from eating or shaving or brushing teeth. We found the hand gestures preceded the rise in glucose by about 12 to 18 minute, so if these hand motions could trigger a pre-meal bolus, even before the glucose rises, then there is a double confirmation of meals, and meal announcements may not be needed. This may get us to full closed loop.”
Levy said people with diabetes can expect devices that do even more to reduce patient burden in the coming years.
“Specifically, customization for specific patient populations,” Levy said. “Older adults, pregnant women — how can we meet these patients where they are and provide them with customized care to meet their glucose targets? One patient may decide they want a 100 mg/dL target instead of 110 or 120 mg/dL. Or a patient may decide they want a target of 140 mg/dL or 150 mg/dL. For pregnancy, the glucose targets are even more stringent. Soon that will be an option. The ability to meet these patients at their clinical status, as well as at their desired glucose target, is important.”
Access for everyone
Laura M. Nally
Talk of a bionic pancreas, a fully closed-loop insulin delivery system and personalized medicine with diabetes devices is exciting; however, such advancements will not be available in the immediate future, Gabbay said.
“Those are long-term goals, and they are wonderful goals,” Gabbay said. “What excites me is increasing access to the devices that already work, particularly with where this country is right now and some of the challenges we have with racial inequities in society. The ADA has taken this on with #HealthEquityNow, where we made a strong commitment to address this issue. Our patient bill of rights includes access to technology. We are in the process of establishing some big partnerships around that.”
Diabetes technology making its way beyond the endocrinologist is also important for increasing access, Gabbay said.
“That is the only way we will reach the number of people who will benefit from it,” Gabbay said. “As endocrinologists, we only see a small percentage of the people with diabetes. If we are the only ones using technology, then that is not the answer. There will be a big learning curve, and the ADA has an initiative around time in range. We must raise awareness among people with diabetes and providers in the primary care setting.”
Insurance plans must also expand access to diabetes technology, Nally said.
“Medicaid programs are different from state to state,” Nally said. “In Connecticut, Omnipods are covered under state health insurance, but they were not covered in California. Here in Connecticut, we have difficulty getting the Freestyle Libre covered, which was a problem I didn’t have when I worked in California. Each state is a little bit different, which makes it harder for the clinician to prescribe the device that will best serve the needs of the patient. It can be frustrating for the patient because it is too expensive to buy these devices out of pocket.”
Cost remains the major barrier preventing access, Shah said.
“On one side, I am excited about next-generation technology, but on the other side, patients are abandoning the technology or not initiating it because they cannot afford it,” Shah said. “You can have a great system, but if the patient cannot afford the technology, it does not matter. Yes, I want to see smaller, smarter devices, but I also want to see affordable devices, too. This is a problem that we are seeing right now. With COVID-19, people have lost jobs and are on Medicaid — Medicaid does not cover CGM. A lot of things are moving in the right direction, but what I want to see are affordable, low-cost devices so everyone can benefit. That is the bottom line.”
Adolescents’ risk for developing type 1 diabetes rose with increasing BMI, according to data presented at the American Diabetes Association Scientific Sessions and simultaneously published in Diabetologia.
“There were previous reports on the association between obesity and type 1 diabetes in previous cohorts that included mostly children,” Gilad Twig, MD, PhD, a resident in the department of internal medicine at Sheba Medical Center in Tel Aviv, Israel, told Healio. “We were somewhat surprised to see that the association persisted in adolescents who were perfectly healthy — apart from having abnormal weight — without apparent risk factors for type 1 diabetes.”
Teens in the 75th percentile or higher of BMI have a greater risk of developing type 1 diabetes as adults than those below the 50th percentile of BMI. Data were derived from Zucker I, et al. 1263-P. Presented at: American Diabetes Association Scientific Sessions; June 3-7, 2022; New Orleans (hybrid meeting).
Twig and colleagues conducted a retrospective cohort study of adolescents aged 16 to 19 years who underwent a medical examination prior to military conscription in Israel from January 1996 to December 2016. Data from participants were linked to the Israeli National Diabetes registry. BMI was calculated using height and weight measured at baseline. Participants were placed into age- and sex-matched percentiles based on criteria from the CDC. Participants in the 85th to 94th percentile of BMI were considered to have overweight, and obesity was defined as the 95th percentile or higher.
There were 834,050 men and 592,312 women included in the study. Over a median follow-up of 11.2 years, there were 777 incident type 1 diabetes cases during 15,819,750 person-years, for an incidence rate of 4.9 cases per 100,000 person-years.
The risk for type 1 diabetes gradually increased with higher BMI. In multivariable analysis, adolescents in the 75th to 84th percentile of BMI (adjusted HR = 1.41; 95% CI, 1.11-1.78), with overweight (aHR = 1.54; 95% CI, 1.23-1.94) and with obesity (aHR = 2.05; 95% CI, 1.58-2.66), had an increased risk for type 1 diabetes compared with those in the fifth to 49th percentile of BMI.
“For adolescents with obesity, the risk for type 1 diabetes was approximately doubled,” Twig said. “It is important to remember that in our study, we grouped all those with obesity in the group regardless of obesity severity. Therefore, it is likely that for adolescents with more severe forms of obesity, the actual risk for developing type 1 diabetes is even higher.”
Each 5-unit increase in BMI was associated with a 35% increase in risk for developing type 1 diabetes (aHR = 1.35; 95% CI, 1.24-1.47) and each 1 standard deviation increase in BMI increased the risk for developing type 1 diabetes by 25% (aHR = 1.25; 95% CI, 1.17-1.32).
Twig said future research is planned to identify more risk factors for incident type 1 diabetes in the same cohort.
“We are, in particular, planning to better identify the characteristics of adolescents in whom excessive weight may have a more emphasized role in the development of type 1 diabetes,” Twig said.
Adults and children with type 1 diabetes who used an insulin-only bionic pancreas had reduced HbA1c without increasing hypoglycemia and other improved metrics compared with standard of care, researchers reported.
The Insulin-Only Bionic Pancreas Pivotal Trial achieved key primary and secondary endpoints in adults and children with type 1 diabetes, according to data presented during a mini-symposium at the American Diabetes Association Scientific Sessions.
Source: Adobe Stock
The iLet bionic pancreas (Beta Bionics) is a pocket-sized, wearable, investigational device designed to autonomously determine and deliver insulin doses to control blood glucose levels for people with diabetes. It is designed to be worn like an insulin pump; however, users would enter only their body weight to initialize therapy and would not set any insulin parameters. The device is designed to automatically titrate and infuse insulin without requiring the user to count carbohydrates, set insulin-to-carbohydrate ratios, set insulin basal rates, set correction factors or determine bolus insulin for meals or corrections, according to a company release.
This is a “fairly new and different concept in automation,” Greg Forlenza, MD, associate professor of pediatrics at the Barbara Davis Center for Diabetes at the University of Colorado Anschutz Medical Campus, said during a presentation.
Large, diverse trial
The pivotal trial was designed to evaluate safety and efficacy of the iLet bionic pancreas compared with current standard of care for insulin-treated diabetes over 13 weeks.
“This is the largest randomized controlled trial ever conducted to evaluate the safety and efficacy of an automated insulin delivery system,” Steven J. Russell, MD, PhD, associate professor of medicine at Harvard Medical School and Massachusetts General Hospital, said during the presentation.
The study population consisted of 440 adults and children aged 6 years and older with type 1 diabetes at 16 U.S. sites.
“This randomized trial included a more diverse population of adults with type 1 diabetes than previous pivotal studies of hybrid closed-loop systems with respect to minority representation, method of insulin delivery and HbA1c levels,” Davida Kruger, MSN, APN-BC, nurse practitioner at Henry Ford Health System, said here.
Participants were randomly assigned to the bionic pancreas or to continue their standard of care from January to July 2021. Seventy-seven percent of participants were non-Hispanic white, 10% non-Hispanic Black, 9% Hispanic or Latino and 4% other. The standard of care group was comprised of about one-third on automated insulin delivery systems, one-third on insulin pump therapy with continuous glucose monitoring and one-third on multiple daily injection therapy with CGM, Forlenza said.
The primary outcome was HbA1c at 13 weeks.
Primary analysis results
The primary analysis compared outcomes with the bionic pancreas, using insulin lispro (Humalog, Novo Nordisk) or insulin aspart (NovoLog, Novo Nordisk), with standard of care in 326 adults and children. The remaining 114 adults used the bionic pancreas with rapid-acting insulin (Fiasp, Novo Nordisk).
At 13 weeks, the following outcomes were improved over standard of care:
Significant reduction in HbA1c: At 13 weeks, mean HbA1c was reduced by 0.5% in the bionic pancreas group vs. standard of care (P < .001). In those with baseline HbA1c higher than 7%, the mean HbA1c reduction was 0.7% for the bionic pancreas group vs. standard of care (P < .001).
No increase in hypoglycemia: Those who used the bionic pancreas did not experience any significant increase in average time spent with CGM values less than 54 mg/dL over 13 weeks compared with standard of care (P < .001 for noninferiority).
Increased time in range: Those who used the bionic pancreas had an average of 2.6 hours more time in range (70-180 mg/dL) per day over 13 weeks vs. standard of care (P < .001).
Additional analyses
Kruger reported results from 161 adults using insulin aspart or lispro. In this cohort, mean HbA1c decreased from 7.6% at baseline to 7.1% at 13 weeks in the bionic pancreas group vs. 7.5% in the standard of care group (P < .001). Moreover, HbA1c improvement greater than 0.5% at 13 weeks occurred in 43% of the bionic pancreas group vs. 17% of the standard of care group (P < .001) and greater than 1% in 23% vs. 4%, respectively (P < .001). Greater improvements occurred in those with higher baseline HbA1c levels, Kruger said.
Time in range improved after just 1 day of use of the bionic pancreas, Kruger said. At 13 weeks, those assigned the bionic pancreas spent 11% more time in range (2.6 hours per day) compared with standard of care (P < .001). The researchers reported no difference in time spent below 54 mg/dL.
Seven severe hypoglycemia events were reported in the bionic pancreas group (25.5 per 100 person-years) and two in the standard of care group (14.2 per 100 person-years). No diabetic ketoacidosis events occurred. Thirty hyperglycemia adverse events associated with infusion set failures occurred in the bionic pancreas group (failure rate = 0.9 for 3,203 infusion sets), according to the presentation.
Laurel H. Messer, PhD, presented results from 165 children using insulin aspart or lispro. In the pediatric cohort, mean HbA1c decreased from 8.1% at baseline to 7.5% at 13 weeks in the bionic pancreas group and remained steady at 7.8% in the standard of care group (P < .001). HbA1c improvement greater than 0.5% at 13 weeks occurred in 51% of the bionic pancreas group vs. 17% of the standard of care group (P < .001) and greater than 1% in 29% vs. 6%, respectively (P < .001). As in adults, greater improvements in HbA1c occurred in those with higher levels at baseline.
At 13 weeks, those assigned the bionic pancreas spent 10% more time in range (2.4 hours per day) compared with standard of care (P < .001). Again, there was no difference in time spent with glucose below 54 mg/dL, Messer said.
Laurel H. Messer
Three severe hypoglycemia events were reported in the bionic pancreas group (10.4 per 100 person-years) and one in the standard of care group (7.3 per 100 person-years). No DKA events occurred. There were 30 hyperglycemia adverse events associated with infusion set failures in the bionic pancreas group (failure rate = 3% for 3,420 infusion sets), according to the presentation.
In these analyses, Kruger said the benefits of the bionic pancreas were “more prominent in multiple daily injection users without having a pre-randomization run-in period to initiate pump use, and the benefit was seen across race/ethnicity and socioeconomic status subgroups.”
In another analysis, Russell highlighted a comparison of the bionic pancreas using rapid-acting insulin aspart (n = 114 adults) compared with standard of care (n = 54 adults) and compared with the bionic pancreas using insulin aspart or insulin lispro (n = 107 adults).
“Compared with standard care, HbA1c was improved with the bionic pancreas using fast-acting insulin aspart without increasing CGM-measured hypoglycemia,” Russell said.
At 13 weeks, mean HbA1c decreased from 7.8% to 7.1% in the rapid-acting insulin aspart group and from 7.6% to 7.1% in the insulin aspart/lispro group (P < .001 for both).
“Compared with the bionic pancreas using insulin aspart or lispro, there was no difference in HbA1c, no difference in mean glucose, a 2% difference in mean time in range due to differences during the daytime, an increase in the proportion with time in range greater than 70% and no significant difference in the proportion with an increase in time in range by 5% or more or 10% or more,” Russell said.
In other results, there were no differences between the groups across nine patient-reported outcome surveys, according to Russell.
Jill Weissberg-Benchell, PhD, CDCES, with Ann and Robert H. Lurie Children’s Hospital of Chicago, reported additional patient-reported outcomes. Adults using the bionic pancreas cited reduced diabetes distress, improved fear of hypoglycemia and improved well-being. Among pediatric patients using the device, distress at baseline was associated with a steeper decrease in HbA1c compared with the standard of care group, Weissberg-Benchell said. Parents of the children in the study also reported satisfaction and acceptability of the bionic pancreas, she said.
Taken together, “Compared to a challenging standard of care, the bionic pancreas reduced HbA1c by a clinically significant margin (0.5%) overall and in subgroups; did not increase hypoglycemia; increased time in range by 2.4 to 3.1 hours per day; decreased mean glucose, time above 180 mg/dL and above 250 mg/dL; gave reasonable control of glycemia without CGM input; and autonomously produced and updated an open-loop regimen that gave reasonable control of glycemia,” Russell said.
Building civility, respect and inclusion into the cardiology workplace is essential, especially in an era where burnout is so high, a speaker said at the National Lipid Association Scientific Sessions.
Cardiology Today Editorial Board Member Laxmi Mehta, MD, FACC, FAHA, FNLA, professor of medicine, vice chair of wellness in the department of internal medicine and section director of preventive cardiology and women’s cardiovascular health at The Ohio State University, gave a presentation on how to define and identify physician burnout, how to relate contributors to burnout with discrimination and how to respond to microaggressions.
Mehta is professor of medicine, vice chair of wellness in the department of internal medicine and section director of preventive cardiology and women’s cardiovascular health at The Ohio State University.
Dealing with burnout
The signs of burnout include physical and emotional exhaustion manifested in chronic fatigue, insomnia, impaired concentration, reduced attention span, increased illness, loss of appetite, anxiety and depression; cynicism and detachment manifested in loss of enjoyment, pessimism, isolation and detachment; and ineffectiveness manifested in apathy, hopelessness, irritability, lack of productivity and poor performance, Mehta said.
In a 2019 American College of Cardiology survey, the prevalence of burnout among cardiologists was 26.8%, with 49.5% identifying themselves as stressed and only 23.7% saying they enjoyed work, she said.
Compared with those without burnout, those with it were less likely to be married, to feel satisfied with family life, to say they feel treated fairly at their job or valued in their profession and to say they feel their contributions matter, and more likely to say their family responsibilities hinder their ability to work, to be less satisfied with achieving professional goals, to be less satisfied with their financial compensation, to report experiencing discrimination and to recommend cardiology as a career, she said.
In a 2021 paper published in the Journal of the American College of Cardiology, 29% of cardiologists reported experiencing emotional harassment, 4% reported experiencing sexual harassment and 30% reported experiencing discrimination, while 79% reported adverse effects on professional activities as a result of these issues, Mehta said.
Addressing uncivil workplace behaviors
The four main components of uncivil workplace behaviors are bias, discrimination, bullying and harassment (BDBH), Mehta said, noting that components of programs that have successfully reduced them include subject-matter expertise; structures, resources and funds dedicated to addressing those issues; a strategic plan with comprehensive assessments; and organizational and leadership commitment to reducing BDBH.
“Individuals should ensure freedom from BDBH in their own personal behaviors and actions and assist others by practicing allyship and upstander behaviors, and by supporting institutional efforts,” Mehta said. “Individuals should work toward establishing a culture and climate of respect, including elimination of harassment and bullying. The workforce must have, and be able to use, the necessary skills and tools to achieve those goals.”
Moreover, she said, organizations should incorporate assessments of respect and civility into performance reviews, rewarding those who have worked toward reducing BDBH, should have robust training programs about BDBH and should have mechanisms for confidential reporting and investigation of incidents without retribution.
“The framework for a just culture matches the level of response to the degree of the behavioral problem,” she said.
Handling microaggressions
Microaggressions are common in the cardiology workplace, are often caused by implicit bias and “may have the same negative effect on individuals as overt racism and sexism,” Mehta said during the presentation.
“Microaggressions are more prevalent in environments where BDBH is also prevalent and where workforce diversity and inclusivity are low,” she said. “Long-term strategies for reducing microaggressions must include increasing organizational diversity, equity, inclusion and belonging.”
She said the best way to respond to microaggressions is to use the ACTION framework, which stands for Ask clarifying questions, Curiosity instead of judgment, Tell the facts you observed, Intention vs. impact, Own your thoughts/share your reactions and Next steps.
“For professional fulfillment, assessment is key,” she said. “Burnout is the metric and well-being is the goal. Cardiovascular organizations and individuals are responsible for ensuring a safe, supportive and respectful workplace environment.”
Summary: Researchers have uncovered a neural circuit that involves spinal neurons and a signaling pathway that is responsible for how burning pain is sensed.
Source: Case Western Reserve
The world has changed since 1664, when French philosopher and scientist Rene Descartes first claimed the brain was responsible for feeling the sensation of pain.
However, a key question remains: How exactly does the human brain feel pain? Specifically, thermal pain—like that experienced when touching an open flame or a hot pan while cooking.
A team of researchers in the neurosciences department at the Case Western Reserve University School of Medicine think they’ve found an answer—that a neural circuit involving spinal neurons and a signaling pathway––are responsible for how burning pain is sensed.
They believe their discovery, published recently in the journal Neuron, could lead to more effective treatment for chronic, pathological pain—such as shooting, stabbing and burning pain—because it may involve the same signaling pathway.
“We know that heat, cold, pressure and itching stimulations to our skin result in appropriate feelings in the brain. However, the neurons encoding the heat signals in the spinal cord were unclear,” said Hongsheng Wang, study lead author and a postdoctoral fellow at the School of Medicine.
“Our study identified a group of interneurons in the spinal cord required for heat sensation. We also found a signaling pathway contributes to heat hypersensitivity caused by inflammation or nerve injuries.”
The study
The brain controls everything we do, from our perception of the world around us to how we move our bodies and experience sensations. The process involves neurons, which are cells that act as messengers to transmit information between the brain and nervous system. The neurons send information through complex circuits throughout the body.
The research team looked at neurons in the spinal cord and their role in thermal pain by analyzing mouse models and their response to heated plates. During this process, the team identified the activation of a “novel,” or newly discovered, class of spinal cord neurons (called ErbB4+) that process heat signals to the spinal cord.
The team wanted to look further into whether these neurons specifically are responsible for thermal pain. There are several ways to test this, including destroying the ErbB4+ neurons.
The brain controls everything we do, from our perception of the world around us to how we move our bodies and experience sensations. Credit: The Researcher
The researchers expressed a toxin specifically targeting the ErbB4+ neurons. Once the neurons were destroyed, the response to heat pain was impaired. This demonstrated that ErbB4+ neurons are specifically tied to how thermal pain is sensed and, when destroyed, pain is not felt less.
They also examined the role of neuregulin 1 (NRG1), a protein involved in many cellular functions. They found that NRG1 and its receptor tyrosine kinase ErbB4 (often referred to as the NRG1 signaling) is also involved in the sensation of thermal pain.
The findings
“Pain is a sensation we have all experienced. For most of us, pain is temporary,” said Lin Mei, professor and chair of the Department of Neurosciences at the School of Medicine and study corresponding author.
“However, for patients with pathological pain, the pain experience is unending, with little hope for relief. Scientists have long believed it’s a result of dysfunctional neuronal activity.”
Mei said their study showed that pathological pain can be reduced by injecting an ErbB4+ inhibitor or an NRG1 neutralizing peptide.
The application of these discoveries may go beyond the therapeutic treatment of pathological pain.
“Both NRG1 and ErbB4 are risk genes of many brain disorders including major depression and schizophrenia,” Mei said.
“Further studies are warranted to show if the mechanism of heat pain and pathological pain also plays a role in different types of pain experienced by those who have brain disorders.”
Abstract
A novel spinal neuron connection for heat sensation
Highlights
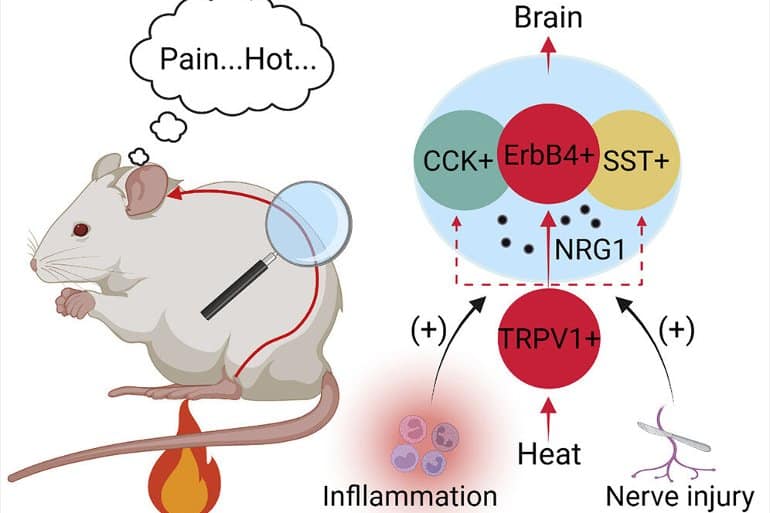
Spinal ErbB4+ neurons are activated by heat and synapsed by TRPV1+ nociceptors
Heat sensation is reduced by ErbB4+ neuron ablation or inhibition
Augmented effect on heat sensation by inhibiting ErbB4+, SST+, and CCK+ neurons together
NRG1-ErbB4 signaling promotes heat sensation and hypersensitivity
Summary
Heat perception enables acute avoidance responses to prevent tissue damage and maintain body thermal homeostasis. Unlike other modalities, how heat signals are processed in the spinal cord remains unclear.
By single-cell gene profiling, we identified ErbB4, a transmembrane tyrosine kinase, as a novel marker of heat-sensitive spinal neurons in mice. Ablating spinal ErbB4+ neurons attenuates heat sensation.
These neurons receive monosynaptic inputs from TRPV1+ nociceptors and form excitatory synapses onto target neurons. Activation of ErbB4+ neurons enhances the heat response, while inhibition reduces the heat response.
We showed that heat sensation is regulated by NRG1, an activator of ErbB4, and it involves dynamic activity of the tyrosine kinase that promotes glutamatergic transmission.
Evidence indicates that the NRG1-ErbB4 signaling is also engaged in hypersensitivity of pathological pain.
Together, these results identify a spinal neuron connection consisting of ErbB4+ neurons for heat sensation and reveal a regulatory mechanism by the NRG1-ErbB4 signaling.
Summary: Researchers say women tend to feel less stressed on weekends when they usually have more “down time”.
Source: Binghamton University
Women feel less stressed on weekends, when there is more downtime, according to new research from Binghamton University, State University of New York.
Lina Begdache, assistant professor of health and wellness studies at Binghamton University, researches the different determinants of mental distress.
In a recent study, her team investigated the role of diet quality, time of the week and physical fitness on the stress hormone cortisol and how they relate to mood (short-term changes in mental status) and mental distress (typically longer-term mental distress).
A total of 336 records from 48 college students were analyzed. Students recorded their dietary intake for three days, and completed two different mood questionnaires on a Wednesday (a peak weekday) and a Saturday (a downtime day).
Researchers found that during a peak weekday, individuals who experience a negative affect are more likely to experience mental distress, but the likelihood of these emotions remaining high subsides during downtime (e.g. weekends). This suggests that those experiencing high levels of mental distress need to consider taking a break.
“This is important because it is known that women have twice the risk of mental distress such as anxiety and depression when compared to men,” said Begdache.
“Women tend to juggle several responsibilities and multitask because their brain is wired to do so, but obviously, this adds to their mental distress. Therefore, knowing that taking frequent breaks may improve their mental well-being may ward off the need to resort to medications.”
Researchers found that during a peak weekday, individuals who experience a negative affect are more likely to experience mental distress, but the likelihood of these emotions remaining high subsides during downtime (e.g. weekends). Image is in the public domain
Begdache said that planning some downtime might help women better manage their stress.
“I know myself, as a woman who juggles many responsibilities, that it is sometimes easier said than done, but by making a conscious effort to experience some downtime, many times we could be successful,” said Begdache. “Delegation of tasks or building priorities sometimes helps.”
The researchers also found that physically fit individuals are more likely to relax faster, so including some physical activity in their daily routine could add to their mental improvement.
Begdache and her team have another manuscript under review looking at the impact of exercise frequency on mental health during weekdays and weekends and comparing it to the different stages of COVID-19: before, during the pandemic and after the ease of restrictions.
Also contributing to this research were Saloumeh Sadeghzadeh, assistant professor in the School of Management; graduate student Paul Pearlmutter; undergraduate students Gia Derose and Pragna Krishnamurthy; and Ahyeon Koh, assistant professor of biomedical engineering.