Ibogaine is currently among the buzziest psychedelics, promising to upend the landscape of mental health care and support. First discovered to curb addiction in the 1960s, the drug was declared an illegal substance by the 1970s. Now, ibogaine is making a comeback not only for treating addiction but anxiety, depression, and now traumatic brain injuries.
In a study published Friday in the journal Nature Medicine, military veterans with mostly mild traumatic brain injuries underwent a combination treatment of magnesium and ibogaine in Mexico, where the psychedelic is legal. One month following their treatment, the individuals reported feeling immense relief from symptoms associated with post-traumatic stress disorder (PTSD), anxiety, and depression, as well as improved cognition.
“No other drug has ever been able to alleviate the functional and neuropsychiatric symptoms of traumatic brain injury,” Nolan Williams, an associate professor of psychiatry and behavioral sciences at Stanford University School of Medicine, who led the study, said in a press release. “The results are dramatic, and we intend to study this compound further.”
“Living in a blizzard”
Ibogaine is a naturally occurring compound found in the roots of a shrub called Tabernanthe iboga, which is native to Central Africa and has been used for centuries for ceremonial practices.
Ibogaine acts as a stimulant in small doses but is a powerful psychedelic in large doses. What it does in the brain, however, isn’t well understood. Studies in rats show that ibogaine may increase proteins that encourage neuroplasticity, which could explain how it helps the brain rewire itself, overcoming seemingly hard-set neural patterns of addiction.
While ibogaine isn’t legal in the U.S., that hasn’t deterred a growing number of individuals from flocking to clinics in Mexico (where the substance is unregulated) seeking treatment for addiction and other mental health issues.
“There were a handful of veterans who had gone to this clinic in Mexico and were reporting anecdotally that they had great improvements in all kinds of areas of their lives after taking ibogaine,” Williams said. “Our goal was to characterize those improvements with structured clinical and neurobiological assessments.”
To do this, Williams and his colleagues at Stanford recruited 30 military veterans who had been in special operations with a history of traumatic brain injuries — a condition causing other mental health issues like PTSD, depression, and anxiety — and repeated blast or combat exposures. The participants first underwent neuro- and psychological evaluations at Stanford and, a few days later, traveled by themselves to the Ambio Treatment Clinic located in Tijuana, Mexico.
At the clinic, the group took an oral dose of ibogaine paired with an intravenous drip of magnesium to prevent any side effects to the heart and cardiovascular system, which the psychedelic is known to do. Participants also participated in some wellness activities while at the clinic, such as reiki, meditation, yoga, and massage. They were then re-evaluated at Stanford four to five days and one month after the ibogaine treatment.
The results were significant. The average disability score for the participants before the treatment was equivalent to mild to moderate disability. This changed to no disability on the one-month follow-up. The veterans also reported, on average, an 88 percent reduction in symptoms associated with PTSD, 87 percent for depression, and 81 percent in anxiety relative to before the ibogaine treatment. They also did much better on their cognitive tests with respect to overall concentration, information processing, memory, and impulse control.
“Before the treatment, I was living life in a blizzard with zero visibility and a cold, hopeless, listless feeling,” Sean, a 51-year-old veteran from Arizona with six combat deployments who participated in the study, said in the press release. “After ibogaine, the storm lifted.”
A new frontier
These findings complement other studies involving military veterans that, similarly, have found ibogaine vastly improved cognitive impairment, PTSD, anxiety, and depression.
In light of the promising research thus far, pharmaceutical companies are already gearing up to develop drugs from ibogaine. German-based atai Life Sciences made an ibogaine formulation to treat opioid-use disorder that completed an early phase clinical trial in the U.K. At the University of California, San Francisco, researchers developed an antidepressant that mimics ibogaine’s impact on the protein that transports the neurotransmitter serotonin.
Since this study was purely observational, Williams and his colleagues are interested in expanding their research to include brain imaging to see exactly what sort of structural changes or otherwise are going on. The researchers believe ibogaine could be a veritable game-changer not just for traumatic brain injuries but a whole laundry list of neurological and psychiatric conditions.
“In addition to treating [traumatic brain injury], I think this may emerge as a broader neuro-rehab drug,” Williams said. “I think it targets a whole host of different brain areas and can help us better understand how to treat other forms of PTSD, anxiety, and depression that aren’t necessarily linked to TBI.”
A brain imaging study led by a team at Duke University has shown that adults with posttraumatic stress disorder (PTSD) have smaller cerebellums, suggesting that this part of the brain may represent a target for continued research into PTSD, and potentially the development of new therapeutic approaches.
“The differences were largely within the posterior lobe, where a lot of the more cognitive functions attributed to the cerebellum seem to localize, as well as the vermis, which is linked to a lot of emotional processing functions,” said Ashley Huggins, PhD, who is first author of the team’s published study in Molecular Psychiatry, and who helped to carry out the work as a postdoctoral researcher at Duke in the lab of psychiatrist Raj Morey, MD.
The findings have prompted Huggins, who is now an assistant professor of psychology at the University of Arizona, to start looking for what comes first, a smaller cerebellum that might make people more susceptible to PTSD, or trauma-induced PTSD that leads to cerebellum shrinkage. Huggins also hopes the results will encourage others to consider the cerebellum as an important medical target for those with PTSD. “If we know what areas are implicated, then we can start to focus interventions like brain stimulation on the cerebellum and potentially improve treatment outcomes.”
Huggins and colleagues for the Enhancing NeuroImaging Genetics through Meta-Analysis (ENIGMA)-Psychiatric Genomics Consortium (PGC) PTSD workgroup reported on their finding in a paper titled “Smaller total and subregional cerebellar volumes in posttraumatic stress disorder: a mega-analysis by the ENIGMAPGC PTSD workgroup.” In their report the authors concluded, “Although the appreciation of the cerebellum for its contributions to cognitive and affective function is relatively recent, the current results bolster a growing literature confirming the cerebellum is not exclusively devoted to motor function and may, in fact, have unique relevance to psychiatric conditions including PTSD … The insights from the current study have revealed a novel treatment target that may be leveraged to improve treatment outcomes for PTSD.”
PTSD is a psychiatric disorder brought about by experiencing or witnessing a traumatic event, such as a car accident, sexual abuse, or military combat. Though most people who endure a traumatic experience are spared from the disorder, “… nearly 10% of trauma survivors develop chronic symptoms of posttraumatic stress disorder (PTSD), a debilitating psychiatric condition characterized by a constellation of symptoms including intrusive memories, avoidance, hypervigilance, and negative changes in mood and cognition,” the team explained.
Researchers have identified several brain regions involved in PTSD, including the almond-shaped amygdala that regulates fear, and the hippocampus, a critical hub for processing memories and routing them throughout the brain.
The grapefruit-sized cerebellum—the name is Latin for “little brain”—by contrast, has received less attention for its role in PTSD. “It’s a really complex area,” Huggins said. In fact, while the cerebellum makes up just 10% of the brain’s total volume but packs in more than half of the brain’s 86 billion nerve cells.
The cerebellum is best known for its role in coordinating balance and choreographing complex movements, like walking or dancing. But there is much more to it than that. The cerebellum can influence emotion and memory, which are impacted by PTSD. “If you look at how densely populated with neurons it is relative to the rest of the brain, it’s not that surprising that it does a lot more than balance and movement,” Huggins noted. The authors pointed out that the cerebellum shares connections with areas of the brain including the prefrontal and limbic areas, “strongly suggesting that it participates in processes beyond motor coordination that may be highly relevant of PTSD,” they noted. The cerebellum is also connected widely with stress-related regions of the brain, such as with the amygdala and hippocampus, which may make it especially vulnerable to traumatic stress, “… potentially leading to the development of PTSD symptoms by disrupting typical brain-mediated stress responses via cerebro-cerebellar circuits,” the team continued. But also, they added, “A growing body of structural and functional magnetic resonance imaging studies has begun to examine the role of the cerebellum in PTSD.”
Researchers have recently observed changes to the size of the tightly-packed cerebellum in PTSD. Most of that research, however, is limited by either a small dataset (fewer than 100 participants), broad anatomical boundaries, or a sole focus on certain patient populations, such as veterans or sexual assault victims with PTSD. And what isn’t known is whether a smaller cerebellum predisposes a person to PTSD or PTSD shrinks the brain region.
To help address these limitations in previous work Morey, along with over 40 other research groups that are part of the data-sharing consortium, pooled together their brain imaging scans to study PTSD as broadly and universally as possible.
They focused on images from 4,215 adult MRI scans, about a third of whom had been diagnosed with PTSD. And even with automated software to analyze the thousands of brain scans, Huggins manually spot-checked every image to make sure that the boundaries drawn around the cerebellum and its many subregions were accurate. “I spent a lot of time looking at cerebellums,” Huggins said.
The result of this thorough methodology was the consistent finding, that the cerebellums of PTSD patients were about two percent smaller than those of control individuals. And zooming in to specific areas within the cerebellum that influence emotion and memory, Huggins found similar cerebellar reductions in people with PTSD. “We found subregional specificity linking PTSD to smaller volumes in the posterior cerebellum, vermis, and flocculonodular cerebellum,” the team noted.
The results in addition indicated that the worse PTSD was for a person, the smaller was their cerebellum. “Focusing purely on a yes-or-no categorical diagnosis doesn’t always give us the clearest picture,” Huggins said. “When we looked at PTSD severity, people who had more severe forms of the disorder had an even smaller cerebellar volume.”
Noting limitations of their study, the authors further concluded in their report, “Overall, these findings argue for a critical role of the cerebellum in the pathophysiology of PTSD, bolstering support for the region’s contributions to processes beyond vestibulomotor function.”
The researchers suggest the results are an important first step at looking at how and where PTSD affects the brain. There are more than 600,000 combinations of symptoms that can lead to a PTSD diagnosis, Huggins explained. Figuring out if different PTSD symptom combinations have different impacts on the brain will also be important to keep in mind.
For now, the researchers hope that their work will raise recognition of the cerebellum as an important driver of complex behavior and processes beyond gait and balance, as well as point to this brain region as a potential target for new and current treatments for people with PTSD. “The cerebellum appears to play an important role in higher-order cognitive and emotional processes, far beyond its historical association with vestibulomotor function,” they wrote. “Further examination of the cerebellum in trauma-related psychopathology will help to clarify how cerebellar structure and function may disrupt cognitive and affective processes at the center of translational models for PTSD.”
Huggins added, “While there are good treatments that work for people with PTSD, we know they don’t work for everyone. If we can better understand what’s going on in the brain, then we can try to incorporate that information to come up with more effective treatments that are longer lasting and work for more people.” And as the authors pointed out, “Further examination of the cerebellum in trauma-related psychopathology will help to clarify how cerebellar structure and function may disrupt cognitive and affective processes at the center of translational models for PTSD.”
In the past few years, at more than a dozen research centers across the globe, adults suffering from post-traumatic stress disorder (PTSD) took MDMA (3,4-methylenedioxymethamphetamine)—the psychedelic commonly known as ecstasy. In cozy rooms with soft light and calming music, individual participants worked through trauma with therapists. Half of the participants took MDMA. The others swallowed placebo pills.
Despite some promising clinical results, researchers still don’t know how psychedelics such as psilocybin (magic mushrooms) cause trips, or whether these trips influence therapeutic outcomes. Image credit: Shutterstock/24K-Production.
After three such sessions, and additional therapy, many of the 100-plus participants improved, according to the report, published last September (1). In the absence of MDMA and through therapy alone, more than 46% of individuals no longer met the criteria for PTSD. For those who took MDMA, it was more than 71%.
Sign up for PNAS alerts.
Get alerts for new articles, or get an alert when an article is cited.
The study is the latest in a series of clinical trials suggesting that MDMA may safely treat PTSD in many patients. In December, the treatment regimen’s developer, MAPS Public Benefit Corporation, became the first company to request Food and Drug Administration approval for a psychedelic drug.
More and more evidence suggests that psychedelics, such as MDMA, LSD (lysergic acid diethylamide), psilocybin (commonly known as magic mushrooms), and DMT (N,N-dimethyltryptamine; the active ingredient in ayahuasca), can be useful tools—in conjunction with psychotherapy—for easing difficult-to-treat mental health conditions. But as these once-villainized drugs come closer to mainstream medicine, a question remains: How do they work? “We need to know so much more,” says neuroscientist Jennifer Mitchell of the University of California, San Francisco, lead author of the MDMA study.
Scientists don’t know how psychedelics improve mental health or why a patient’s environment seems to influence the effect. They also don’t fully understand what triggers the psychedelic experience commonly known as a “trip”—and they’re unsure whether this trip is necessary for overcoming symptoms.
Researchers and clinicians don’t actually need those answers to administer psychedelics safely. But revealing how psychedelics function could help pharmacologists design more effective treatments. “The drugs work super well for some people, but not as well for other people,” Mitchell says. “I’d like to know how to maximize the therapeutic benefit of the drug. And I’d like to know how to reach those people that right now are unreachable.”
Searching for answers, neuroscientists are probing the effects of psychedelics from the molecular level to the entire brain. Ultimately, they’ll need to investigate aspects of drug use that are rarely explored in detail—how individual differences and even the setting interact with these drugs to shape the psychedelic journey and longer-term healing.
Changing Perspectives
Classic psychedelics share a key feature: They have an impact on serotonin receptors in the brain. Serotonin, a chemical messenger that helps neurons communicate, is especially important for regulating mood. Psilocin (a molecule metabolized from psilocybin), DMT, and LSD stimulate neurons by activating many of the same receptors as serotonin. MDMA, a different form of psychedelic, causes a massive release of the brain’s own serotonin, which then activates receptors.
Serotonin does, of course, activate its own receptors. And common antidepressants increase the amount of serotonin available to stimulate receptors. Yet, somehow, psychedelics acting on this same system can cause dramatic effects, such as hallucinations or waves of empathy. And, it seems in some cases, healing, which can persist long after the immediate effects of the drugs have worn off. Ingrained patterns, such as compulsive substance use or constant negative thinking, can be “upended, interrupted, and really blown apart by these psychedelics,” says psychopharmacologist Albert Garcia-Romeu of Johns Hopkins University (JHU) School of Medicine in Baltimore, Maryland.
Researchers recognized this therapeutic potential in the 1950s and ‘60s, when tens of thousands of volunteers participated in psychedelics studies (2). By today’s standards, the research lacked scientific rigor. By the 1970s, governments cracked down on psychedelic drug use due to safety concerns, and the studies came to an end. Research ramped up again in the 1990s, spurred, in part, by new tools for brain imaging (2). Today, such treatments are moving through clinical trials for many mental health conditions, including substance abuse disorders (3), eating disorders (4), and depression (5).
The current treatments aren’t for everyone, cautions Garcia-Romeu. Studies exclude people with conditions that could make a psychedelic experience risky, such as those with a history of psychosis. But from the data available, psychedelics seem to be safe and potentially effective for a number of conditions, he says. And, yet, exactly why these drugs work, often with effects persisting weeks or months after a single dose, remains unknown.
Dendrites (green) branch out from a rat neuron in a cell culture plate after exposure to ibogaine, a psychedelic. Two proteins in the neuron’s cytoskeleton are labeled in blue and magenta. Image credit: Andras Domokos (Olson Lab, University of California, Davis, California).
On Target
Many investigating this mystery start from the beginning—the moment that a psychedelic enters the brain and triggers the serotonin receptor known as 5-HT2A. This receptor seems to be necessary for a trip. When scientists block it in mice or humans, the psychoactive drug effects disappear (6). (Researchers, of course, don’t know whether mice trip the way humans do, nor how their environs affect the experience. But mice do a telltale head twitch when under the influence of psychedelics.)
There’s good reason to suspect that this receptor also underlies the therapeutic benefits of psychedelics. Some researchers believe that some psychological conditions occur because environmental or genetic factors cause neurons in the brain’s prefrontal cortex to atrophy, diminishing this executive brain region’s ability to regulate motivation, fear, and reward (7).
In animal models, common antidepressant drugs, if taken continuously, prompt neurons to branch and establish new synapses with other neurons (8). “They just do this very slowly and on a timescale that correlates with their clinical efficacy,” says chemical neuroscientist David Olson, director of the University of California, Davis Institute for Psychedelics and Neurotherapeutics.
In 2018, Olson reported that psychedelics also cause neurons to branch in the prefrontal cortex of animal models, but at a rapid clip (7). “You see those neurons grow back within 24 hours,” he says. “The other thing that is really remarkable is that the effects last for a very long time.” Other drugs that do not act through serotonin 2A receptors, such as cocaine, can also cause neuron branching, but not necessarily as rapidly, robustly, or as targeted to the specific brain regions where this growth could alleviate depression, says Olson. In February 2023, Olson published findings that could help explain why psychedelics cause neurons to quickly branch in the prefrontal cortex (9). In this brain region, a large portion of 5-HT2A receptors are located inside neurons. The purpose of those seemingly sequestered receptors is unknown, as the neuron’s membrane blocks serotonin from reaching them. But psychedelics can pass through the membrane (9).
Working with rat neurons in cell culture plates, Olson’s team found that activating internal receptors with DMT or psilocin triggers neurons to rapidly branch and form new synapses. When researchers helped serotonin reach the inner receptors by using an electrical current to open holes in the cell membrane, they again saw speedy branching. “The location of the 5-HT2A receptor matters,” Olson says.
Relief Without the Trip
Other receptors may matter, too. In addition to activating serotonin 5-HT2A, each psychedelic targets a suite of other receptors (10). LSD, for example, activates additional serotonin receptors, as well as several dopamine receptors (11). And a single receptor could trigger several cellular pathways within the neuron, depending on the compound that activates it. These variations might explain why some compounds that activate the 5-HT2A receptor cause hallucinations, while others do not, says Jason Wallach, a pharmacologist and medicinal chemist at Saint Joseph’s University in Philadelphia, Pennsylvania.
“All of a sudden, there is no big boss man in this brain governing the show.”
—Robin Carhart-Harris
Wallach and his team are incrementally tweaking psychedelic compounds to make them more specific to particular receptors and cellular pathways. In doing so, Wallach hopes to identify more effective drugs, including some that trigger healing without the trip. He and colleagues recently found, for example, that they can control whether a 5-HT2A-triggering molecule causes head twitches in mice by adjusting its ability to activate one cellular pathway over another—potentially opening the door to finding ways to modulate these drugs (12) “There’s a big debate in the field whether or not the psychoactive effects are necessary,” Garcia-Romeu says. “Myself and others feel that those experiences that happen when people are under the influence are actually an important part of the process.”
Researchers often report links between treatment success and the mystical nature of psychedelic experiences. In a 2015 pilot study, Garcia-Romeu and colleagues found that 12 of 15 cigarette smokers who took psilocybin along with therapy to break their addiction were smoke-free 6 months after treatment (13). The more intensely mystical they rated their experience, the larger their decrease in cigarette cravings reported at the 6-month check-in.
But these are only correlations. It’s possible that isolating the individual neural circuits involved could decouple the trip from other effects. By tweaking the chemical structures of different psychedelics, Olson identified several compounds that, at least in mice, cause neurons to branch without triggering those telltale head twitches (14, 15). His biotech startup, the Boston-based Delix Therapeutics, is now conducting a Phase 1 clinical trial of one of these drugs in the Netherlands. The participants are healthy volunteers, but the aim is ultimately to treat major depressive disorder and treatment-resistant depression (16). “A single clinical trial may not give us a definitive answer,” Olson says. “We may not know for many, many years because it is all about what patient population, what disease indication.”
Olson and Wallach both expect that, for some health conditions, a psychedelic experience could help patients. Wallach speculates that when treating depression, for example, a trip might prove useful. “[People] often talk about meaningful transformative personal insights they have had during the psychedelic experience,” Wallach says, and “how that influenced their outlook and perspective in their everyday life.” Such testimonials are prompting him and his team to make fully psychedelic compounds. But for a condition less tied to one’s mental outlook, such as cluster headaches (17), Wallach questions whether the psychedelic experience is critical. “In that case”, he says, “I think it is hard to make an argument that it’s anything more than just this physiological effect.”
One huge benefit of using psychedelics without prompting hallucinations would be scalability. “To administer [psychedelics] safely, you have to give them under the supervision of a healthcare professional,” Olson says. “That dramatically increases the complexity of the treatment, as well as the cost.”
A Whole-Brain Response
Other researchers are zooming out to study how the brain as a whole changes during a psychedelic trip. One leading theory: Psychedelics temporarily topple the brain’s usual hierarchy (18).
This idea rests on a longstanding cognitive science theory, which holds that the brain’s executive control regions, including the prefrontal cortex, create expectations about surroundings and that these expectations dominate our perceptions. Input from other regions, including the visual and auditory cortices, carries less weight in the grand calculation that yields one’s impression of the world.
The psychedelics theory known as the “relaxed beliefs under psychedelics (REBUS) and the anarchic brain model” posits that a brain under the influence of psychedelics gives less weight to executive control, while allowing more input from elsewhere. “All of a sudden, there is no big boss man in this brain governing the show,” says neuroscientist Robin Carhart-Harris of the University of California, San Francisco, a developer of the theory. This change in command might explain the sensory experience of a trip.
In one recent study, altered brain activity did appear to track with that subjective experience. Carhart-Harris and colleagues monitored the brains of 20 healthy adults before, during, and immediately following DMT use (19). While under the influence of the psychedelic, the brain’s waves of electrical activity, captured by electroencephalogram (EEG), were more irregular, indicating a greater complexity of brain activity, which the researchers theorized could stem from information flowing more freely. The level of complexity for each participant also correlated with the individual’s own ratings of the intensity of the psychedelic experience.
Brain imaging data from the same study, captured via functional MRI (fMRI), suggest that a brain under the influence of DMT breaks down typical brain networks and opens up communication between networks. For example, Carhart-Harris’ team found that, on DMT, the default mode network—a brain network known to remain active during self-reflection and daydreaming—communicated less within itself and more with other brain regions, mirroring similar results from his studies of psilocybin (20) and LSD (21). If the temporary reorganization of the brain’s hierarchy allows for greater flexibility in thought patterns that, with therapy, can be shaped into a more positive outlook over time, Carhart-Harris and others theorize that the REBUS model might also explain mental health improvements lasting for weeks or even months after the psychedelic experience (5, 22).
But the model itself is still a matter of debate in the neuroscience community (23). And researchers don’t know yet whether such lasting cognitive changes are related to physiological brain changes during a trip, such as the branching neurons witnessed in animal models.
Psychedelic treatment rooms, like this one at the University of California San Francisco’s Neuroscape center, are intended to be cozy, calming spaces. How such environs affect treatment efficacy is still a matter of some debate. Image credit: Jennifer Mitchell (University of California, San Francisco, California).
Enduring Change
Even as researchers continue to explore the neural mechanisms of psychedelic healing, neuroscientists are studying which changes in mental processes underlie reductions in symptoms. JHU researchers, for example, found that patients with major depressive disorder improved their scores in tests of cognitive flexibility—the ability to switch focus between tasks—even 4 weeks after psilocybin treatment (24). But this study found no correlation between improved cognitive flexibility and reduced symptoms.
“You have to tailor these experiences in a way that we are just not accustomed to doing for other sorts of Western medicine. If the environment feels unsafe or threatening, the experience can go very dark very quickly.”
—Jennifer Mitchell
Cognitive neuroscientist Ceyda Sayalı, of JHU’s Center for Psychedelic and Consciousness Research, is also looking at changes in another measure: cognitive effort avoidance. Everyone avoids cognitive effort sometimes—like using a precalculated tip rather than doing the math, Sayalı says. “For people with major depressive disorder, anxiety, or similar mental illnesses, this kind of effort-avoidance behavior can be very pathological.”
In her previous work with healthy participants, cognitive task seekers were better at reducing activity in their default mode networks (dialing down that daydreaming function), while, at the same time, increasing activity in the frontal parietal network, a necessity for task completion (25). Sayalı is now enrolling patients diagnosed with both major depressive disorder and alcohol use disorder in a study that will combine simple number tasks and fMRI imaging to test whether cognitive effort—and the networks that support it—improves a week after psilocybin use.
If these measures do improve, that still would not explain the underlying reason for the persistent change. One challenge in tying the drugs’ effects to their neural substrates is limited funding. The present wave of psychedelic research has been supported in large part by nonprofits and private donors rather than government grants or large pharmaceutical companies (22). Without substantial financial support, clinical trials are often small and lack neural imaging. Complicating matters, even some of the larger, most high-profile studies, including the recent MDMA trials, have been criticized for methodological flaws, such as failing to truly blind the studies (26–29).
A Personalized Approach
Even if psychedelics can be effective, it’s clear that they don’t work for everyone. Researchers are beginning to explore differences among patients that could predict success. “Everyone has a slightly different organization of their brain,” says neuropsychologist Katrin Preller of the Psychiatric University Hospital Zurich in Switzerland. She’s testing how differences in the way brain networks synch up could predict patient outcomes.
The microbiome, too, may impact psychedelic therapy, in part because bacteria in the gut could influence how the body metabolizes these drugs (30). Garcia-Romeu and colleagues are analyzing how gut microbiome composition influences treatment results.
And then there’s genetics. Some people lack a working version of a gene that codes for an enzyme that metabolizes LSD, for example. For these individuals, trips are longer and more intense, according to a 2021 report by researchers at University Hospital Basel in Switzerland (31).
Increasingly, researchers are taking this sort of personalized medicine approach to many drugs—not just the mind-altering sort. But the psychedelics field has long catered to the individual because of two major additional variables: set and setting.
“Set” is the mindset that someone brings to treatment. “Setting” is the environment where the drug is administered, including everything from music to throw pillows. “You have to tailor these experiences in a way that we are just not accustomed to doing for other sorts of Western medicine,” Mitchell says. “If the environment feels unsafe or threatening, the experience can go very dark very quickly.”
This experiential nature of psychedelics complicates clinical trials. It’s hard to truly “blind” studies. Patients typically know whether they’ve taken a psychedelic, even when researchers offer a lower dose or a nonpsychedelic drug as a placebo (32). So expectations of healing could change people’s outlooks and lead researchers to overestimate the drug’s direct effects. The environment where the drug is administered, which includes the therapists being present, could also sway treatment outcomes in ways that differ between clinics, or even between patients in the same clinic.
Aiming to make these factors more transparent, researchers from Imperial College London recently called on over 70 psychedelics researchers, study participants, and therapists to recommend components of setting that should be reported in clinical trials. The consensus, shared in late summer 2023 at a set and setting workshop in the Netherlands, includes a long list of variables, from whether therapists gave participants verbal instructions to whether flowers were in the room.
The importance of the vast majority of these variables, however, has not been tested experimentally. Instead, therapists rely on their own experience and the shared wisdom of their craft. But that wisdom may not always hold up to scientific scrutiny.
Western classical music, for example, is a standard choice for ambience setting in psychedelics treatments. In a pilot study of psilocybin use for smoking cessation, Garcia-Romeu and colleagues swapped the Western classical soundtrack for one that included instruments such as gongs and a didgeridoo in one of a patient’s two sessions. They then let patients choose between the two soundtracks in a third session. Six of 10 patients selected the non-Western music. And there was no statistically significant difference in treatment outcomes (33).
Mitchell worries that results from recent clinical trials will convince people that the drugs are safe anywhere, when, in reality, researchers are still figuring out under what conditions they actually help. All of this work also continues to take place in the shadow of a complicated history. The psychedelics research community is still recovering from when these drugs lost favor in the 1970s, Mitchell says. Credible, safe treatments, she says, will only come through sound experimental approaches that “evaluate exactly when and how and if and why the drugs are effective.”
Posttraumatic stress disorder (PTSD) is characterized by a persistent maladaptive reaction after exposure to severe psychological trauma. Traumatic events that may precipitate PTSD include violent personal assaults, natural and human-made disasters, and exposure to military combat or warfare. There is a growing body of evidence for associations of PTSD with major risk factors for cardiovascular disease (CVD), such as hypertension and diabetes, as well as with major CVD outcomes, such as myocardial infarction and heart failure. However, it is unclear whether these associations are causal or confounded. Furthermore, the biological and behavioral mechanisms underlying these associations are poorly understood. Here, the available evidence on the association of PTSD with CVD from population, basic, and genomic research as well as from clinical and translational research are reviewed, seeking to identify major research gaps, barriers, and opportunities in knowledge acquisition and technology as well as research tools to support and accelerate critical research for near-term and longer-term translational research directions. Large-scale, well-designed prospective studies, capturing diverse and high-risk populations, are warranted that include uniform phenotyping of PTSD as well as broad assessment of biological and behavioral risk factors and CVD outcomes. Available evidence from functional brain imaging studies demonstrates that PTSD pathophysiology includes changes in specific anatomical brain regions and circuits, and studies of immune system function in individuals with PTSD suggest its association with enhanced immune inflammatory activity. However, establishment of animal models and human tissue biobanks is also warranted to elucidate the potential causal connection of PTSD-induced brain changes and/or inflammation with CVD pathophysiology. Emerging large-scale genome-wide association studies of PTSD will provide an opportunity to conduct mendelian randomization studies that test hypotheses regarding the presence, magnitude, and direction of causal associations between PTSD and CVD outcomes. By identifying research gaps in epidemiology and genomics, animal, and human translational research, opportunities to better justify and design future interventional trials are highlighted that may test whether treatment of PTSD or underlying neurobiological or immune dysregulation may improve or prevent CVD risk or outcomes.
Summary: Ibogaine, a plant-based psychoactive drug combined with magnesium, effectively reduces PTSD, anxiety, and depression in veterans with traumatic brain injuries (TBI). The study, involving 30 U.S. special forces veterans, showed significant and lasting improvements in mental health and functioning post-treatment.
Ibogaine’s potential extends beyond TBI, offering hope for broader applications in neuropsychiatric conditions like PTSD and depression. The drug’s safety profile and positive results suggest a promising avenue for veterans’ mental health treatment.
Key Fact:
Ibogaine, in combination with magnesium, leads to significant and lasting improvements in veterans’ mental health and functioning.
This research offers hope for treating traumatic brain injuries (TBI) and broader neuropsychiatric conditions such as PTSD and depression.
Ibogaine’s safety profile and effectiveness suggest potential benefits for veterans’ mental health treatment.
Source: Stanford
For military veterans, many of the deepest wounds of war are invisible: Traumatic brain injuries resulting from head trauma or blast explosions are a leading cause of post-traumatic stress disorder, anxiety, depression and suicide among veterans. Few treatments have been effective at diminishing the long-term effects of TBI, leaving many veterans feeling hopeless.
Now, Stanford researchers have discovered that the plant-based psychoactive drug ibogaine, when combined with magnesium to protect the heart, safely and effectively reduces PTSD, anxiety and depression and improves functioning in veterans with TBI.
Their new study, to be published online Jan. 5 in Nature Medicine, includes detailed data on 30 veterans of U.S. special forces.
“No other drug has ever been able to alleviate the functional and neuropsychiatric symptoms of traumatic brain injury,” said Nolan Williams, MD, an associate professor of psychiatry and behavioral sciences. “The results are dramatic, and we intend to study this compound further.”
Alternative options
Traumatic brain injury is defined as a disruption in the normal functioning of the brain resulting from external forces — such as explosions, vehicle collisions or other bodily impacts. The trauma associated with TBI can lead to changes in the function and/or structure of the brain, which, in turn, contributes to neuropsychiatric symptoms.
Hundreds of thousands of troops serving in Afghanistan and Iraq have sustained TBIs in recent decades, and these injuries are suspected of playing a role in the high rates of depression and suicide seen among military veterans. With mainstream treatment options not fully effective for some veterans, researchers have sought therapeutic alternatives.
Ibogaine is a naturally occurring compound found in the roots of the African shrub iboga, and it has been used for centuries in spiritual and healing ceremonies.
More recently, it has gained interest from the medical and scientific communities for its potential to treat opioid and cocaine addiction, and research has suggested that it increases signaling of several important molecules within the brain, some of which have been linked to drug addiction and depression.
Since 1970 ibogaine has been designated as a Schedule I drug, preventing its use within the U.S., but clinics in both Canada and Mexico offer legal ibogaine treatments.
“There were a handful of veterans who had gone to this clinic in Mexico and were reporting anecdotally that they had great improvements in all kinds of areas of their lives after taking ibogaine,” Williams said. “Our goal was to characterize those improvements with structured clinical and neurobiological assessments.”
Capturing ‘before and after’
Williams and his colleagues at Stanford teamed up with VETS, Inc., a foundation that helps facilitate psychedelic-assisted therapies for veterans. With support from VETS, 30 special operations veterans with a history of TBI and repeated blast exposures, almost all of whom were experiencing clinically severe psychiatric symptoms and functional disabilities, had independently scheduled themselves for treatment with magnesium and ibogaine at a clinic in Mexico.
Before the treatment, Stanford researchers gauged the participants’ levels of PTSD, anxiety, depression and functioning based on a combination of self-reported questionnaires and clinician-administered assessments.
Participants then traveled to a clinic in Mexico run by Ambio Life Sciences, where under medical monitoring they received oral ibogaine along with magnesium to help prevent heart complications that have been associated with ibogaine. The veterans then returned to Stanford for post-treatment assessments.
“These men were incredibly intelligent, high-performing individuals who experienced life-altering functional disability from TBI during their time in combat,” Williams said. “They were all willing to try most anything that they thought might help them get their lives back.”
At the beginning of the study, participants were experiencing clinically significant levels of disability as measured by the World Health Organization Disability Assessment Scale 2.0, which assesses disability in six functional domains, including cognition, mobility, self-care, getting along, life activities and community participation. In addition, 23 met the criteria for PTSD, 14 for an anxiety disorder and 15 for alcohol use disorder. In their lifetimes, 19 participants had been suicidal and seven had attempted suicide.
Life-changing results
On average, treatment with ibogaine immediately led to significant improvements in functioning, PTSD, depression and anxiety. Moreover, those effects persisted until at least one month after treatment — the endpoint of the study.
Before treatment, the veterans had an average disability rating of 30.2 on the disability assessment scale, equivalent to mild to moderate disability. One month after treatment, that rating improved to 5.1, indicating no disability.
Similarly, one month after treatment participants experienced average reductions of 88% in PTSD symptoms, 87% in depression symptoms and 81% in anxiety symptoms relative to how they were before ibogaine treatment. Formal cognitive testing also revealed improvements in participants’ concentration, information processing, memory and impulsivity.
“I wasn’t willing to admit I was dealing with any TBI challenges. I just thought I’d had my bell rung a few times — until the day I forgot my wife’s name,” said Craig, a 52-year-old study participant from Colorado who served 27 years in the U.S. Navy.
“Since [ibogaine treatment], my cognitive function has been fully restored. This has resulted in advancement at work and vastly improved my ability to talk to my children and wife.”
“Before the treatment, I was living life in a blizzard with zero visibility and a cold, hopeless, listless feeling,” said Sean, a 51-year-old veteran from Arizona with six combat deployments who participated in the study and says ibogaine saved his life. “After ibogaine, the storm lifted.”
Importantly, there were no serious side effects of ibogaine and no instances of the heart problems that have occasionally been linked to ibogaine. During treatment, veterans reported only typical symptoms such as headaches and nausea.
Lessons for PTSD, depression and anxiety
Williams and his team are planning further analysis of additional data collected on the veterans but not included in the current study, including brain scans that could help reveal how ibogaine led to improvements in cognition. They also hope to launch future studies to further understand how the drug might be used to treat TBI.
However, they think ibogaine’s drastic effects on TBI also suggest that it holds broader therapeutic potential for other neuropsychiatric conditions.
“In addition to treating TBI, I think this may emerge as a broader neuro-rehab drug,” Williams said. “I think it targets a whole host of different brain areas and can help us better understand how to treat other forms of PTSD, anxiety and depression that aren’t necessarily linked to TBI.”
Traumatic brain injuries (TBIs) resulting from head trauma or blast explosions are a leading cause of post-traumatic stress disorder, anxiety, depression, and suicide among military veterans. Few treatments have been effective at diminishing the long-term effects of TBI, leaving many veterans feeling hopeless.
Researchers at Stanford School of Medicine have now reported the results of a clinical trial demonstrating that the plant-based psychoactive drug ibogaine, when combined with magnesium to protect the heart, safely and effectively reduced PTSD, anxiety and depression, and improved functioning in veterans with TBI.
“No other drug has ever been able to alleviate the functional and neuropsychiatric symptoms of traumatic brain injury,” said research lead Nolan Williams, MD, an associate professor of psychiatry and behavioral sciences. “The results are dramatic, and we intend to study this compound further.” Williams and colleagues at Stanford, and at Palo Alto University, Veterans Affairs Palo Alto Health Care System, and at Ambio Life Sciences, reported on the trial results in Nature Medicine, in a paper titled “Magnesium–ibogaine therapy in veterans with traumatic brain injuries.” In their paper, the researchers concluded “This is possibly the first study to report evidence for a single treatment with a drug that can improve chronic disability related to repeated TBI from combat/blast exposures.”
Traumatic brain injury is defined as a disruption in the normal functioning of the brain resulting from external forces—such as explosions, vehicle collisions or other bodily impacts. The trauma associated with TBI can lead to changes in the function and/or structure of the brain, which, in turn, contributes to neuropsychiatric symptoms. “Traumatic brain injury (TBI) is a leading cause of disability,” the authors wrote. “Sequelae can include functional impairments and psychiatric syndromes such as post-traumatic stress disorder (PTSD), depression and anxiety … The sequelae of TBI may also include both subjective and objective changes in memory, attention, processing speed and executive functions that can substantially impact quality of life.”
For military veterans, including special operations forces (SOFs) and special operations veterans (SOVs), TBIs are suspected of playing a role in the high rates of depression and suicide, and with mainstream treatment options not fully effective for some veterans, researchers have sought therapeutic alternatives. “Given this substantial burden of ongoing disability and suicide risk in SOVs, additional treatment options are needed,” the investigators noted.
Ibogaine is a naturally occurring compound found in the roots of the African shrub Tabernanthe iboga, and it has been used for centuries in spiritual and healing ceremonies. More recently, it has gained interest from the medical and scientific communities for its potential to treat opioid and cocaine addiction, and research has suggested that it increases signaling of several important molecules within the brain, some of which have been linked to drug addiction and depression. Since 1970 ibogaine has been designated as a Schedule I drug, preventing its use within the U.S., “Such legal restrictions have limited research, as have concerns related to neuro- and cardiotoxicity,” the authors continued, although clinics in both Canada and Mexico offer legal ibogaine treatments.
“There were a handful of veterans who had gone to this clinic in Mexico and were reporting anecdotally that they had great improvements in all kinds of areas of their lives after taking ibogaine,” Williams said. “Our goal was to characterize those improvements with structured clinical and neurobiological assessments.”
For their study Williams and his colleagues at Stanford teamed up with VETS, a foundation that helps facilitate psychedelic-assisted therapies for veterans, to undertake a prospective study examining the safety and efficacy of the Magnesium–Ibogaine: the Stanford Traumatic Injury to the CNS (MISTIC) protocol in SOVs.
The study involved 30 SOVs with a history of TBI and repeated blast exposures, almost all of whom were experiencing clinically severe psychiatric symptoms and functional disabilities, had independently scheduled themselves for treatment with magnesium and ibogaine at a clinic in Mexico.
Before the treatment, the participants’ levels of PTSD, anxiety, depression and functioning were gauged, based on a combination of self-reported questionnaires and clinician-administered assessments. Participants then traveled to a clinic in Mexico run by Ambio Life Sciences, where under medical monitoring they received oral ibogaine along with magnesium to help prevent heart complications that have been associated with the drug. The veterans then returned to Stanford for post-treatment assessments.
At the beginning of the study, participants were experiencing clinically significant levels of disability as measured by the World Health Organization Disability Assessment Scale 2.0, which assesses disability in six functional domains, including cognition, mobility, self-care, getting along, life activities and community participation. In addition, 23 met the criteria for PTSD, 14 for an anxiety disorder and 15 for alcohol use disorder. In their lifetimes, 19 participants had been suicidal and seven had attempted suicide.
“These men were incredibly intelligent, high-performing individuals who experienced life-altering functional disability from TBI during their time in combat,” Williams said. “They were all willing to try most anything that they thought might help them get their lives back.”
The trial results indicated that on average, treatment with ibogaine immediately led to significant improvements in functioning, PTSD, depression and anxiety. The effects persisted until at least one month after treatment—the endpoint of the study. Before treatment, the veterans had an average disability rating of 30.2 on the disability assessment scale, equivalent to mild to moderate disability. One month after treatment, that rating improved to 5.1, indicating no disability. Similarly, one month after treatment participants experienced average reductions of 88% in PTSD symptoms, 87% in depression symptoms and 81% in anxiety symptoms relative to how they were before ibogaine treatment. “After MISTIC, participants showed a remarkable reduction in these symptoms with large effect sizes (Cohen’s d > 2 on clinician-rated psychiatric assessments) and the benefits were sustained at the 1-month follow-up,” the authors wrote.
Formal cognitive testing also revealed improvements in participants’ concentration, information processing, memory and impulsivity…“Neuropsychological testing (NPT) revealed areas of improvement after treatment, particularly in processing speed and executive function, without any detrimental changes observed.”
During treatment, veterans reported typical symptoms such as headaches and nausea, but there were no serious side effects associated with ibogaine treatment, and no instances of the heart problems.
Noting limitations of their study, and the need for additional trials to replicate their findings, particularly in non-mild TBI cases, the investigates concluded, “In summary, our study provides initial evidence to suggest that MISTIC could be a powerful therapeutic for the transdiagnostic psychiatric symptoms that can emerge after TBI and repeated exposure to blasts and combat, including suicidality… Importantly, our results indicate that ibogaine can be administered safely.”
The research team is now planning further analysis of additional data collected on the veterans but not included in the reported study, including brain scans that could help reveal how ibogaine led to improvements in cognition. They also hope to launch studies in the future that will provide additional understanding into how the drug might be used to treat TBI.
The drastic effects of ibogaine on TBI may also suggest that the drug holds broader therapeutic potential for other neuropsychiatric conditions. The authors stated, “Although outside the context of TBI and veterans, our findings are consistent with previous studies suggesting benefits of treatment with psychedelic substances across several psychiatric disorders.” Williams added, “In addition to treating TBI, I think this may emerge as a broader neuro-rehab drug. I think it targets a whole host of different brain areas and can help us better understand how to treat other forms of PTSD, anxiety and depression that aren’t necessarily linked to TBI.”
Psychedelics made their mark this year—not as counterculture party drugs, but as a new paradigm in mental health therapy.
In June, Australia became the first country to greenlight MDMA, popularly known as molly or ecstasy, and psilocybin, the active ingredient in magic mushrooms, to treat post-traumatic stress disorder (PTSD) and depression.
MDMA also inched closer to approval in the US for PTSD, thanks to positive results from a large multi-site, double-blind, randomized trial—the gold standard for testing drug safety and efficacy.
Meanwhile, psilocybin gained steam as a treatment for severe depression. A randomized, placebo-controlled trial in 104 adults found that a single dose of magic mushrooms dampened the symptoms of depression when combined with psychological support. The effects lasted at least six weeks with minimal side effects. Clinical trials are in the works to explore whether psilocybin and its derivatives can help patients cope with chronic lower back pain, tackle depression in bipolar disorder, and ease mental struggles in end-of-life care.
This year also saw magic mushrooms for therapy move ahead. Registered clinics in Oregon have already begun psilocybin treatments in patients with mental health disorders ranging from obsessive-compulsive disorders to PTSD—even though the drug isn’t federally approved and remains illegal.
In 2022, Oregon became the first state to legalize psilocybin therapy with strict regulations: The mushrooms are carefully controlled for potency and quality and need to be taken under supervision. The guidelines offer a blueprint for other states—such as Colorado, which also decriminalized psilocybin for potential therapeutic use.
Yet one glaring problem remains. Despite promising clinical results, no one knows exactly how psychedelic drugs work in the brain. Examining their actions on brain cells isn’t just an academic curiosity. It could give rise to variants that maintain antidepressant properties without the high. And because hallucinogens substantially alter our perception of the world, they could be powerful tools for investigating the neurobiology behind consciousness.
Lucy in the Sky With Brain Cells
Mind-altering drugs are “fabulously dirty,” in that they act on multiple targets across the brain, with each activating different types of neurons in diverse regions.
However, they share similarities. For example, most psychoactive drugs regulate serotonin, a brain chemical involved in mood, appetite, memory, and attention.
This year, scientists found another common theme—psychedelics seem to “reset” the brain to a more youthful state, at least in mice. Like humans, mice have an adolescent critical period, during which their brains are highly malleable and can easily rewire neural circuits, but the window closes after adulthood.
An earlier study showed that MDMA reopens the critical window in adult mice, so that they change their “personality.” Mice raised alone are often introverted and prefer to keep to themselves in adulthood. A dose of MDMA increased their willingness to snuggle with other mice—essentially, they learned to associate socializing with happiness, concluded the study.
It’s not that surprising. MDMA is well-known to promote empathy and bonding. The new study, by the same team, extended their early results to four psychedelics that don’t trigger fuzzy feelings—LSD, ketamine, psilocybin, and ibogaine. Similar to MDMA, adult mice raised alone changed their usual preference for solitude when treated with any of the drugs. Because habits are hard to change in adulthood—for mice and men—the drugs may have reopened the critical period, allowing the brain to more easily rewire neural connections based on new experiences.
People with depression often have rigid neural networks that lock them into non-stop ruminations and dark thoughts. Psychedelics could potentially be a “master key” that helps brain networks regain their fluidity and flexibility.
Surprisingly, despite vastly different chemical structures, all the tested psychedelics activated a brain protein called brain-derived neurotrophic factor. A nutrient for brain cells, the protein helped brain regions involved in memory and mood give birth to new neurons. It also restored damaged neural branches, so neurons could better connect into functional networks.
Classic antidepressants such as Prozac also activate the protein, but psychedelics are far more effective. It could be why they rapidly relieve depressive symptoms within hours, whereas conventional alternatives often take months.
That said, being high all the time is hardly practical.
Another study suggests that it might be possible to separate a drug’s mind-bending and mood-boosting effects. By studying brain networks in mice tripping on LSD, the researchers pinpointed a key hub for the drug’s anti-depressant effects. Genetically deleting the protein hub reduced anti-depressant effects, but kept the high (on acid, mice bob their heads nonstop as if jamming to the Grateful Dead). The results suggest it may be possible to develop LSD variants that skirt unwanted hallucinations but keep their rapid antidepressant properties.
These are just early results. But psychedelic research is gaining a new ally—artificial intelligence. Algorithms that predict protein structure, combined with rational drug design, could generate psychedelics that retain their psychiatric benefits without the high.
Machine learning could also further help decipher their effects on brain activity. For example, a collaboration between McGill University in Canada, the Broad Institute at Harvard and MIT, and other institutions is using AI to explore how hallucinogens alter different chemical systems in the brain.
The method is outside-the-box: The study designed an algorithm that analyzed 6,850 “trip reports” from people who took a range of 27 different drugs and cataloged their subjective experiences in everyday language. The AI extracted commonly used words for any given substance and linked them to brain chemical systems across brain regions that are likely affected by that particular drug. In other words, the AI reliably translated real-world experiences into potential chemical changes in the brain for researchers to explore. A similar tool could link drug-induced changes in consciousness to different brain regions.
A Regulatory Sea Change
Despite growing enthusiasm, hallucinogens and empathogens—such as MDMA—remain federally illegal. The Drug Enforcement Agency classifies them as Schedule I, meaning the agency considers them drugs without known medical uses and high risk of abuse.
However, federal regulators are gradually warming up to their potential.
In June, the Food and Drug Administration released draft guidance on how to conduct clinical trials using psychedelic drugs—giving the field a tentative nod. The agency has already approved a version of ketamine for treatment-resistant depression and granted MDMA and psilocybin breakthrough therapy status to accelerate their development. Even Congress is on board. This year, it passed bills allowing the Department of Veteran Affairs to study psychedelics for veterans’ mental health.
Acceptance is also growing across society. A small poll by the UC Berkeley Center for the Science of Psychedelics found over 60 percent of 1,500 surveyed participants supported legalizing psychedelics for therapy, as long as they’re regulated.
This year was a landmark year for psychedelic therapy. While promising, the results are still early. Given the drugs’ tumultuous history, researchers and practitioners are carefully moving forward with guidelines on best therapeutic practices (such as what to do when a patient suffers a bad trip). With at least 260 registered clinical trials in the works, next year is poised to continue psychedelic drugs’ foray into mental health.
A new trial finds that LSD might have the potential to treat anxiety. microgen/Getty Images
MindMed, a biotech company specializing in psychedelic-inspired medicines, has revealed promising results from its MM-120 drug candidate in the treatment of Generalized Anxiety Disorder (GAD).
The results from a recent clinical trial showed that the MM-120 — a hallucinogen better known as LSD — could become a potential new treatment for GAD, a condition that affects millions of people worldwide.
The trial highlight that the drug candidate, particularly at the 100 µg dose, demonstrated effectiveness, significantly reducing anxiety symptoms.
Generalized anxiety disorder (GAD) is characterized by persistent and excessive worry or nervousness about everyday life, frequently causing disruptions in daily tasks and personal connections.
Potential treatments include psychotherapy, medication, and lifestyle adjustments.
GAD, categorized as an anxiety disorder, is prevalent, affecting 3.1% of the United States population in a given year, equivalent to 6.8 million adults. It is more frequently diagnosed in women.
Coping with anxiety can present difficulties, but like other anxiety disorders, GAD is eminently manageable and responsive to treatment.
Mind Medicine (MindMed) Inc., a clinical-stage biopharmaceutical company specializing in innovative treatments for brain health conditions, has just released promising findings from its Phase 2b clinical trial involving MM-120 (lysergide d-tartrate) for generalized anxiety disorder (GAD).
Dr. Daniel Karlin, chief medical officer of MindMed, explained the key findings to Medical News Today:
“MindMed conducted this study with participation from 198 patients, all of whom suffered with a primary psychiatric diagnosis of generalized anxiety disorder (GAD), across 20 clinical sites in the United States.”
“Participants were divided into 5 study arms; each arm received a single dose of a lysergide-based drug candidate, called MM-120 (lysergide d-tartrate), or a placebo,” Dr. Karlin continued.
“Among the four groups that received a dose of MM-120, doses were 25, 50, 100, or 200 µg of MM-120. Importantly, no form of additional therapy was given to any participant. The study design evaluated the stand-alone effects of the drug candidate, MM-120,” he further explained.
“The data available to us at this time show that patients experienced meaningful and lasting symptom reduction. Four weeks following a single dose of MM-120, 78% of participants who received either a 100 or 200 µg dose measured as having a clinically significant response to the drug. 50% of participants who received the 100 µg dose were considered to be in clinical remission at Week 4, meaning that the patient no longer suffered from clinically significant symptoms of GAD.” — Dr. Daniel Karlin
The research results have yet to be published in a peer-reviewed journal; however, the company plans to submit the study for publication soon.
Heather Tarbet, Ph.D., vice president of research & development at Amani Ag, told MNT that “this research presents several compelling implications, especially in mitigating the challenges associated with psychedelic therapy.”
“The study demonstrates the tolerability of MM-120, which shortens psychedelic effects while preserving the therapeutic benefits. This approach could alleviate safety and logistical concerns, thereby making psychedelic therapies more accessible and widely accepted among diverse patient groups.” — Dr. Heather Tarbet
Dr. Tarbet noted that “the study’s insights could inspire progress in the broader field of psychedelic research, potentially enhancing treatments for various complex mental health conditions.”
“Moreover, by altering LSD to lessen its intensity and duration, these treatments could gain broader acceptance among patients, healthcare providers, and regulatory authorities, paving the way for wider adoption in medical practice,” she said.
The preliminary findings from early-phase studies should be corroborated and validated through real-world evidence. This process ensures the reliability and applicability of the trial results.
Dr. Walker Porterfield of Clarity Hyperbarics urged caution about making definitive conclusions, telling MNT that “although on the surface this trial seems to be quite beneficial to patients[experiencing] Generalized Anxiety Disorder (GAD), I see some potential issues.”
Dr. Porterfield highlighted the sample size and trial duration, saying, “the trial was a very small group for a very short duration (198 participants and only four weeks long).”
In addition, Dr. Porterfield noted there was also improvement for patients who were part of the placebo group (31% compared to 78% in the active group).”
Considering this, it’s reasonable to infer that some of the favorable outcomes could be attributed to a placebo-like response. Further studies will need to be completed to assess the actual effectiveness of the medication.
Dr. Karlin told MNT that “MindMed has evaluated the effects of MM-120 in study participants through 12 weeks post-dosing and are currently awaiting those data.”
“We expect to share [more] of that data in the first quarter of 2024. We intend to present the full study results at a scientific conference next year. MindMed also plans to hold an ‘End of Phase 2’ meeting with the FDA in the first half of 2024,” he said.
“Pending the outcome of that meeting, we expect to initiate Phase 3 clinical trials in the second half of 2024,” he added.
“Patients and individuals impacted by GAD largely have been left behind in recent decades; the last approval of a new GAD treatment came in 2004. The most widely prescribed treatments for the disorder often fail to stimulate significant or long-lasting improvement, while exposing patients to side effects that can range from unpleasant to unbearable.” — Dr. Daniel Karlin
Dr. Karlin explained that “the strong, rapid, and durable clinical activity observed following a single dose of MM-120 is extremely promising for patients who are underserved by current treatment options.”
“The data from this study represents a major step forward in our goal to bring a paradigm-shifting treatment to the millions of people impacted by this debilitating condition,” he said.
Stellate ganglion blocks appear to reset the sympathetic nervous system and deliver powerful results for those suffering with PTSD.
A stellate ganglion procedure performed at Joy Wellness Partners.
For most of his life, Isaiah Heller has oscillated between panic and prescriptions, alcohol, and marijuana to numb difficult emotions and a mind that “moved at 100 miles a second.”
The U.S. Army veteran tried to take his own life twice. He couldn’t keep a job, and his driver’s license was once revoked after he suffered a trauma-induced seizure disorder. He attempted—but walked out of—cognitive processing therapy, a specialized clinical treatment to reframe past events and gain emotional freedom.
Heller suffered from shame and trauma due to experiences in foster care, a near-death hate crime assault as a young teen, and sexual abuse in the military. But his silent suffering echoed in the walls of his own home with night terrors, paranoia, and his inability to be present—psychological symptoms that bled into the lives of his wife and children.
And then, one day, these symptoms came to a grinding halt; his nervous system relaxed like a rubber band that loses tension. He was miraculously present and at peace when he walked out of the Joy Wellness Partners clinic after getting his first stellate ganglion block (SGB).
“It was almost like the weight of the universe lifted up off my body. It was such a euphoric feeling,” he said. “I am getting time back in my life because I’m enjoying the moment.”
Trauma isn’t rare. Heller is among the 6 percent of the population that experiences post-traumatic stress disorder (PTSD)—about 12 million adults in a given year. At some point in their lifetime, half of all adults will have trauma, a shocking event witnessed or that happens to them.
SGBs are simple procedures that take minutes, involving an anesthetic injected into the stellate ganglion, a bundle of nerves in the cervical spinal column associated with the sympathetic nervous system.
Guided by sonogram imagery, a physician inserts a small needle of medicine that temporarily dulls this starburst of nerves connecting the body to the brain. The block lasts for about eight to 10 hours with a similar mechanism as an epidural, which blocks sensation from the belly button to the upper thighs for pregnant women in labor.
It’s a well-established procedure anesthesiologists have used for a century for pain. A case report of PTSD in 1990 inspired its “off-label” use for trauma.
In most cases, SGBs offer instantaneous relief to burdened nervous systems that have become stuck in “fight-or-flight.” But rocky reviews and murkiness over its mechanism have stalled wide acceptance of the procedure. Research hasn’t pinpointed why it doesn’t reboot everyone’s nervous systems. Also, among those who enjoy its benefits, the longevity of the reset varies extensively. It may last a decade or only a few months, with no foreknowledge on factors that make it more effective.
“Certain people just don’t respond to the block, and we don’t know why,” Dr. Eugene Lipov, pain specialist and early pioneer of the procedure, told The Epoch Times. Lipov—the chief medical officer for Stella clinics across the United States, Australia, and Israel that offer the procedure—said his research includes looking into genetic and other explanations for differences in patient response.
How SGB Works
It’s theorized that the reason SGBs work is because they reset the nervous system to its state before the trauma. The sympathetic nervous system is a component of the autonomic nervous system that’s designed to unite the brain and body for effortless, instantaneous responses to threats, whether physical or emotional.
Dr. Frank Ochberg, a pioneer in trauma science, has petitioned for years to reclassify PTSD as post-traumatic stress injury (PTSI) because improved brain scans now reveal that trauma can be healed, boosting the validity of biological interventions such as SGB. He argues a change in name could remove the stigma attached to trauma and better allow the injured to seek help.
One simple theory is that SGB works by calming the nervous system. The cervical sympathetic trunk is the link between the body and the brain, holding polysynaptic neurological connections from the stellate ganglion leading to the amygdala, the part of the brain associated with anxiety and trauma.
Another hypothesis is the injection could be suppressing nerve growth factor, which lowers norepinephrine and mutes physiological symptoms like rapid heart rate, shallow breathing, sweaty palms, and brain fog. The activation of the fight-or-flight system elevates norepinephrine in the brain, a neurotransmitter that leads to arousal, selective attention, and vigilance.
Those with PTSD have high levels of norepinephrine in their cerebrospinal fluid. High norepinephrine symptoms are associated with sleep dysfunction, impulsivity, anxiety, depression, and sexual dysfunction.
Finally, additional evidence indicates SGB might work as a sedative due to the reduction in norepinephrine. The nervous system then “boots up” back at baseline.
Assessing Risks and Side Effects
Until the development of fluoroscopy, SGBs were performed by using vertebrae as landmarks to guide the injection. Now, sonograms are used for the procedure, which lowers many risks by helping doctors guide the needle to the anterior lateral C6 vertebrae and allowing them to watch the administration of medication using dye.
Risks associated with SBG include a small chance of infection. There are very rare occurrences of the injection hitting a blood vessel and forming a hematoma, which is why it’s not done on those taking blood thinners. Temporary side effects such as droopy eyes or a hoarse voice are common.
Prevalent, but rarely a significant problem, is the rush of emotions and memories that happens after the procedure. Heller believes the effect is what enabled him to talk about his trauma and process it in healthy ways. He re-entered therapy, this time successfully. Eight weeks in, he told his wife about the sexual abuse.
“That was a breakthrough for me, and I never thought I was ever going to get there. It doesn’t affect me anymore,” Heller said. “It’s crazy what you can do when you’re in the right phase of mind.”
Lives Changed
The number of clinics specializing in SGBs is growing, as are non-profit organizations that offset costs. A mix of studies and proponents claim a success rate claim of about 75–90 percent. But while some patients rave about the results, it isn’t always a one-and-done fix.
Dave Conley, U.S. Navy veteran and founder of One More Day Inc., is a pragmatic advocate. Focused on the prevention of veteran and military suicide, One More Day helps connect veterans to The Stellate Institute, run by veteran physicians Drs. Sean Mulvaney and James Lynch, among other providers.
“You’ve got to still put the work in,” said Conley, who had an SGB followed by two weeks of intensive PTSD therapy in 2022. He lost four friends to suicide after they returned from serving. After his own attempt at taking his life, he started the organization and then a podcast.
Conley’s nightmares eased up significantly after his SGB. He said the procedure stirs a lot of excitement, but people should be wary of false hope. Many need a follow-up procedure, oftentimes because of re-exposure to new trauma or intense triggers.
Heller opted for two follow-up procedures after a car accident introduced new stress. His experiences overall have motivated him—to find a job he loves, dig into his school work, and enjoy every moment with his three children.
“People that say they want to change, they act on it. I’ve worked for everything I’ve gotten,” Heller said. “This is my life, and it’s amazing.”
That tenacity to stick with therapy is a key component of the SGB success story, Conley said. He was ready to quit after three days, but by the second week, it all began to click.
A randomized study of 113 active military personnel published in 2019 in JAMA found a significant improvement in symptoms in the group that had SGB. The author wrote that the procedure buoys therapy for patients with barriers to cognitive-based therapies because of concentration and hyperarousal issues, which can affect the brain’s ability to function normally.
“Specifically, encoding and retrieving memories or integrating new learning becomes very challenging,” wrote Kristine L. Rae Olmsted, a behavioral epidemiologist whose focus is military mental health. “As a psychologist who has deeply collaborated with physicians who provide SGB, I have observed that many of the insights discussed prior to SGB have been more easily applied following the procedure.”
Broader Reach
Conley believes the use of this novel trauma treatment could expand dramatically, though SGBs haven’t garnered sweeping support from governmental agencies. Doctors have spent years seeking more veteran access to SGBs, but legislation to expand the treatment option—the Treat PTSD Act—died in committee during the last two congressional sessions.
The bill would require the Department of Veterans Affairs and the Department of Defense to provide SGBs for qualified military and veterans, as well as updating clinical practice guidelines to include it as a PTSD treatment option. Support has come from both sides of the aisle.
There’s another hiccup in SGB’s history. A study published in 2016 Regional Anesthesia and Pain Medicine—a double-blind, randomized controlled trial—concluded there’s no evidence to support SGB for PTSD. The study, authored by Dr. Steven Hanling who didn’t reply to a request for an interview, “did not demonstrate any appreciable difference between SGB and sham treatment on psychological or pain outcomes.”
However, a Department of Defense analysis that looked at this study and the 2019 JAMA study noted that the 2016 study “had a number of methodological limitations, including high attrition, absence of key outcomes, and deviance from commonly used administration techniques for SGB.” The 2016 study also had a smaller sample size of 42 participants while the 2019 study that found evidence of efficacy had 113 participants.
The 2019 study also had its own issues, including a lack of blinding of treating physicians, meaning they knew which patients got the real treatment. There was also a possible unblinding of participants due to side effects of SBG, meaning some patients may have figured out if they got the real treatment or the sham treatment.
Proponents have questioned the reliability of the 2016 study in light of other evidence, including an analysis published in 2021 of 205 patients that showed 90 percent responded positively to the procedure. Of the 20 who didn’t receive a reset, 10 had the procedure done on the other side of their neck, and nine of those patients had a favorable outcome.
Lipov admits the limited acceptance of SGB could simply be because it’s a “weird concept,” a disruptive use of technology that doesn’t fit medical training and thinking. His career pivoted to focus on it only because of his own observations of its efficacy.
Patients who want an SGB must pay out-of-pocket, which can limit the market size for interested physicians. But the treatment may also rub up against the pharmaceutical industry, which sells billions of dollars in drugs used for PTSD and anxiety disorders.
“The main problem it’s not accepted I think is there’s no pharmaceutical dollar behind it,” Lipov said. “There’s no patent on the drug, and the distribution process is a complex undertaking.”
A stellate ganglion procedure performed at Joy Wellness Partners. A stellate ganglion procedure performed at Joy Wellness Partners. A stellate ganglion procedure performed at Joy Wellness Partners.
Summary: Often considered dangerous, mind-altering drugs, researchers are turning to the study of psychedelic therapies as a potential to treat an array of psychiatric conditions including depression and PTSD.
Source: Stanford
It was 1985 and John Lawn had seen enough.
In Boston nightclubs and Dallas bars, MDMA—better known by its street name, ecstasy—had become an enormously popular recreational drug. It had also terrified the Reagan administration, which was in the midst of its historic War on Drugs.
Lawn, the administrator of the Drug Enforcement Administration at the time, acted quickly. Despite the outcry of medical professionals pointing to the range of MDMA’s clinical uses, Lawn classified the drug as Schedule 1, one of many to be banned in a backlash against psychedelics like LSD and psilocybin. The message was clear: these drugs were dangerous, immoral, and medically useless.
Nearly four decades later, researchers at Stanford’s Wu Tsai Neurosciences Institute are at the forefront of a seismic shift that’s putting a spotlight on a once taboo field. Scientists are starting to take seriously what Lawn’s DEA long ago dismissed: that the mind-expanding properties of these demonized “party drugs” might be clinically valuable after all.
It’s an exciting time for a reborn field. Early clinical trials suggest MDMA may help patients with PTSD confront their traumatic memories. In other early studies, ketamine has reduced suicidal thoughts and other symptoms in patients with clinical depression.
Psilocybin too may be able to help people with intractable depression, decreasing symptoms in some patients for a year or more, though the data here are still limited. And many other studies and trials are ongoing in the field.
This recent pivot toward psychedelic drugs has been described by some as a “psychedelic revolution” in psychiatry, if not a “miracle cure” for mental health disorders in general. But many of the basic mechanisms of these drugs remain poorly understood, in a field of medicine that has barely begun to recover from decades of government-enforced stigmatization.
“There are a lot of questions that need answering,” said Robert Malenka, the Pritzker Professor of Psychiatry and Behavioral Sciences at Stanford and a Wu Tsai Neurosciences Institute deputy director, who studies the mechanisms that drive MDMA’s therapeutic properties. “We’re still concerned about the evidence that these drugs will be therapeutically useful—and if they are, how to best use them therapeutically.”
Partly because of these big unknowns, psychedelic medicine has struggled to shake off the same fears first expressed by Lawn’s DEA. For some potentially addictive compounds like MDMA, abuse potential remains a charged question, and broader ethical concerns surrounding the vulnerable state that many psychedelics produce remain at play for other substances.
To pull this 1960s-era field into the present, psychedelic researchers are going back to basics. They’re working to untangle the mechanisms behind these drugs’ properties—from their therapeutic effects to their abuse potential. By understanding how these drugs work, researchers hope to design better and safer treatments that come with all the benefits of psychedelics, and few of the downsides.
The wild world of psychedelics
Warped colors and fantastical images are familiar hallmarks of “classical” psychedelics, including hallucinogens like LSD and psilocybin. But the new “psychedelic revolution” actually involves several different families of drugs—some of which, like MDMA and ketamine, are not technically psychedelics at all.
MDMA is an example of an entactogen, a batch of compounds that alter social perceptions and amplify empathy. Take one of these drugs, and you’ll start feeling more connected to those around you, whether it be your fellow partygoers, your therapist, or even your significant other, as some therapists have found helpful in bridging fractured relationships.
Meanwhile, ketamine is an example of a dissociative anesthetic, which acts by distancing users from reality. Such drugs can place patients in a dream-like state of sensory deprivation where even your sense of self fades away.
For researchers, the goal is to understand—from a mechanistic standpoint—why only certain drugs work for some disorders and not for others, isolate those effective drug mechanisms, and focus research efforts around those mechanisms to develop far more targeted, disorder-specific treatments.
Scientists are now beginning to tease out the brain mechanisms behind the distinctive mind-altering properties of these different drug families, a critical step in turning them into mainstream treatments.
Classic psychedelics seem to work by binding to the serotonin 2a receptor, one of the 15 specialized receptor molecules the serotonin system uses to coordinate brain activity. Entactogens and dissociative anesthetics don’t directly act on this receptor, which is why they “feel” different from hallucinogens.
Research into these compounds is even murkier: while early studies into MDMA have implicated serotonin in the drug’s effects, it’s only one chemical in a mixed bag of neurotransmitters and hormones. Meanwhile, ketamine has been tenuously linked to a specific receptor in the brain’s glutamate system.
“We need more research using the same rigorous methods applied to many other promising compounds for mental illnesses. By studying both efficacy and mechanisms, we can be more precise in developing better treatments with fewer side effects,” said Carolyn Rodriguez, a professor of psychiatry and behavioral sciences who co-authored a July 2022 position statement by the American Psychiatric Association on the mental health uses of psychedelics and empathogens.
Rodriguez, who directs the Stanford Translational Therapeutics Lab, is leading studies on the mechanisms underlying ketamine’s effects, a crucial component of her work on ketamine as a potential therapy for OCD.
Previously, Rodriguez has demonstrated ketamine’s ability to reduce the compulsive behaviors characteristic of OCD. Her study on ketamine’s mechanism of action aims to better understand how ketamine helps OCD patients—one stepping stone toward a targeted OCD treatment.
Another key question is how these drugs change the brain itself to produce their unique mental states. Karl Deisseroth, the D. H. Chen Professor of bioengineering and of psychiatry and behavioral sciences at Stanford and a Howard Hughes Medical Institute investigator, has studied how ketamine alters brain dynamics to produce the characteristic “dissociative” state that appears to help some patients with depression and other disorders.
In a 2020 study, the Deisseroth lab linked these dissociative states to a specific rhythm of activity in particular circuits in the mouse brain. When the team artificially reproduced this rhythm in normal mice, they found they could directly trigger dissociation, even without ketamine.
Don’t trip? Or maybe do
Psychedelic therapy isn’t as simple as just taking a drug such as LSD, ketamine, or MDMA and waiting for your depression to go away. It unfolds over several preparatory sessions, each dedicated to pinning down how and when to enter the psychedelic experience.
When the drug arrives, it’s accompanied by ambient music and a pair of eye shades. The patient pops the pill, sits back, and lets the drug get to work on their brain. Lastly comes the therapist-aided process of integration, where the patient takes what they’ve experienced and tries to fit it back into their life.
“It’s a big, holistic process,” said Boris Heifets, an anesthesiologist and neuroscientist at the Wu Tsai Neurosciences Institute who has previously worked alongside Malenka to study the mechanisms of MDMA. “These drugs are more like ‘catalysts’ than they are treatments.”
The downside of this holistic approach, according to Malenka, is that psychedelic therapy is hard to regulate. In part, this is because psychedelic therapy often requires far more oversight than traditional therapy. For instance, because psychedelic drugs put patients in an altered, vulnerable state, each individual is normally accompanied by at least one and often two therapists for the sake of safety. This makes psychedelic therapy not only expensive, but tricky to scale up.
“The FDA has never had to evaluate a treatment that involves both a drug treatment and a psychotherapeutic intervention,” Malenka said. “Everybody’s very interested in seeing how federal agencies and states regulate the distribution of these substances as therapeutics.”
The ideal psychedelic treatment would drastically streamline this therapeutic process, reducing psychedelic therapy to nothing more than a simple, safe-to-use pill. It’s a tremendously difficult—and thus far elusive—goal.
At the heart of the matter is the “trip,” or the acutely brain-altering experience that characterizes these psychedelic drugs. Many researchers think that the process of consciously undergoing this experience is deeply intertwined with the therapeutic properties of drugs like LSD and MDMA.
“There’s this suspicion that the therapeutic part might come from the process of mixing things up and jumbling your rigid way of thinking,” Heifets said. “You can call it a realignment of your values, or a perspective change.”
One example might be found in MDMA. Patients with PTSD typically experience intense anguish in response to trauma-related triggers, yet MDMA’s brain-altering properties reduce these fear barriers while also producing a shift in perspective: one that allows patients to confront their trauma while remaining grounded in the present.
At the same time, MDMA’s ability to aid social interaction can greatly increase the emotional rapport between patient and therapist, further supporting the patient in working through their disorder.
But the question remains: do the clinical benefits of psychedelics always require patients to undergo these profound, and sometimes grueling, drug-induced experiences? It would certainly be much simpler for researchers—and speed the pace of progress for patients—if the benefits of psychedelics could be achieved without the trip.
Heifets, an anesthesiologist, has used general anesthesia to better investigate this question. By placing patients under anesthesia, he aims to test whether it’s possible to get the benefits of psychedelic drugs without actively experiencing the “trip”—suggesting that these drugs are operating on some deeper, more mechanistic level.
“What we’re studying is what would happen if we eliminated all external sensory input—if we made sure that patients were unaware of the drug’s effect on their brain by making them unconscious,” Heifets said. “Would we still get that therapeutic effect?”
Currently, researchers are working to develop this approach in ketamine trials, with the potential for future applications in other compounds. From what researchers have seen so far, however, there has not been compelling evidence that these drugs can work without the holistic process of preparation, “trip” and integration.
Still, a solution without the “trip” remains the white whale (something obsessively pursued but difficult to achieve) of psychedelic medicine.
“We’re talking about designing drugs that have the same therapeutic efficacy, without the possible side effects, without the potential for bad stuff to happen,” Malenka said. “If that’s possible, that would be wonderful.”
Want to understand addiction? Look to evolution
It might not be possible to get the therapeutic benefit without the “trip,” but it might be possible to get the “trip” without one of the key risks—namely, addiction.
Addiction is a particularly vexing problem in non-classical psychedelic drugs like MDMA and ketamine, which trigger the release of dopamine, the neurotransmitter linked to addictive behavior. But is this same addiction mechanism responsible for the drugs’ therapeutic benefit?
For Malenka, the key to understanding these drugs’ addictive potential lies in understanding the ancient circuits they alter. The pleasure of socializing with other human beings is a core drive for our species, burned into our neural circuitry by their evolutionary value to human survival.
“What in the brain tells us that a social interaction is fun and rewarding?” Malenka said. “Why is it that, for most people, it’s more fun to go out to dinner with friends than eat by yourself?”
The Malenka lab’s research explores how these mechanisms get hijacked by drugs of abuse, including potentially beneficial ones like MDMA. Researchers had already established that MDMA’s addictive potential came from its ability to stimulate the release of dopamine, a neurotransmitter involved in reward and motivation that plays a role in most forms of addiction.
Early clinical trials suggest MDMA may help patients with PTSD confront their traumatic memories.
But in a series of studies, Malenka and Heifets—then a researcher in Malenka’s group—wanted to find out if MDMA’s therapeutic, empathy-boosting abilities might involve a different brain pathway, making it possible to separate out its positive effects from its abuse liability.
One leading possibility was the brain’s serotonin system, which can play a role in stabilizing feelings of well-being and happiness—the basis for MDMA’s therapeutic use. To test this question, the Malenka lab separately blocked MDMA’s ability to release either serotonin or dopamine in mice.
Normally, MDMA dramatically boosts rodents’ social drives, much like in humans. But inhibiting serotonin prevented this effect—strong evidence for a link between this neurotransmitter and the drug’s prosocial effects. In contrast, inhibiting dopamine had virtually no influence on animals’ sociability.
“This was compelling evidence that it might be possible to design a version of MDMA that elevates sociability through the serotonin system while greatly reducing or eliminating the regular drug’s addictive downsides,” Malenka said.
This mechanistic separation between therapeutics and abuse might not be possible in all drugs, however. While scientists are still working on these varied psychedelic compounds, the risk looms that abuse potential might come as an inseparable side effect of treatment.
“It’s hard to make categorical statements about abuse liability,” Heifets said. “Every drug is different, so at least when it comes to addiction, you have to talk about each like its own animal.”
The future of psychedelic treatment
With the field of psychedelics booming, researchers are operating in a high-stakes environment. On the one hand, it’s never been a better time to study these compounds: the Food and Drug Administration (FDA) has indicated their intent to approve both MDMA and psilocybin as mental health treatments in the next two years, according to a federal letter made public only weeks ago. Yet others fear that the excitement surrounding these compounds has gone too far, and that these potential treatments might be more hype than substance.
The obstacles are clear. According to Malenka, the risk that widespread medical legalization of these substances might lead to rampant misuse, could threaten the future of psychedelic medicine altogether.
“As soon as something bad happens, the pendulum will swing the other way,” he said. “We don’t want to return to the early 70s, where some individuals and communities used these substances inappropriately and bad things happened.”
It remains to be seen how regulators will scale up and facilitate this pipeline from lab breakthrough to mainstream treatment. But many researchers are excited to get their hands on a new set of tools to help treat mental disorders that have long resisted conventional forms of treatment. If these drugs deliver on their promised benefit, a new era for psychiatric medicine might be at hand—and all it took was for us to finally open our minds to the possibilities.








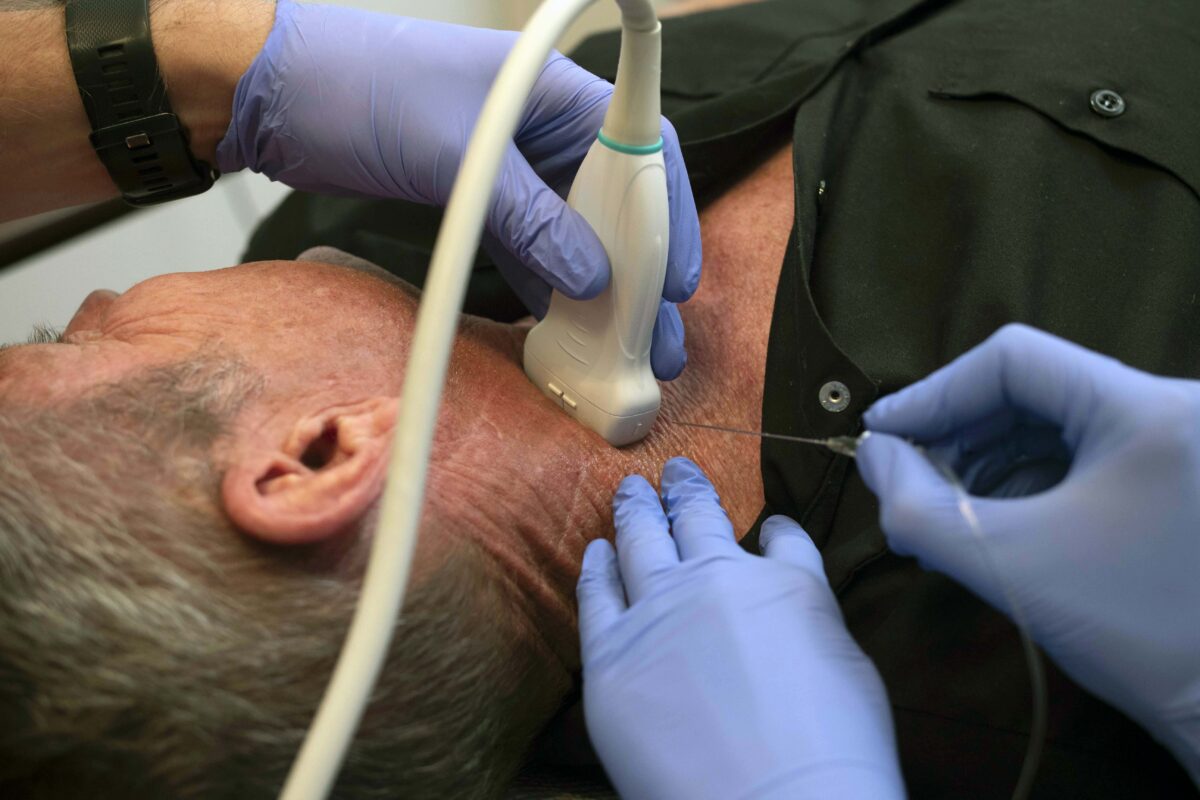




{kind=link}