You already know a lack of iron can drag you down.
But experts say numerous vitamin and mineral deficiencies can contribute to fatigue. If left unchecked, the same deficiencies that make it hard to keep your head up can lead to long-term health consequences – from brittle bones to impaired brain function.
“Fatigue can be like an early warning sign of potentially more severe problems down the road if you don’t recognize and treat the problem causing the fatigue,” says Dr. Anthony Komaroff, a professor of medicine at Harvard Medical School and a senior physician at Brigham and Women’s Hospital in Boston. “You need to explore all possible explanations for your fatigue.” That goes for ongoing feelings of exhaustion to concerns about muscle fatigue being more pronounced or prolonged than might be expected from physical activity.
Some of the most common causes of fatigue – and easiest things to test for – involve deficiencies in three minerals and two vitamins, Komaroff says. After iron comes lack of magnesium, potassium, vitamin B12 and folic acid. “All of them can be corrected by giving supplements of the missing minerals or the missing vitamins,” he says, or through dietary changes.
“More serious problems than just the fatigue can develop from these vitamin and mineral deficiencies,” Komaroff says. “For example, vitamin B12 deficiency, if it goes on long enough, undiagnosed and untreated, can lead to permanent damage of the brain and the spinal cord that can affect people’s ability to move, walk and think clearly.”
Even the mundane can become imperiling – such as untreated anemia from iron deficiency. “Iron is needed to build hemoglobin, which is what is inside the red blood cell,” Komaroff explains. “It carries oxygen, which is a critical source of energy to every cell in the body.”
Anemia often occurs in women as a result of blood loss due to menstruation, though it can affect women of any age as well as men. In mild cases, it can escape detection. But as iron deficiency becomes more severe – and if left uncorrected – symptoms can escalate to include severe fatigue, headache, chest pain and increased heart rate. Besides iron, vitamin B12 or a folic acid deficiency can also lead to anemia.
One factor that may be largely to blame for vitamin deficiencies is a national obsession with restrictive diets, according to Jessica Crandall, a Denver-based registered dietitian nutritionist and a spokeswoman for the Academy of Nutrition and Dietetics. “Most Americans are engaging in some kind of fad diet throughout their life, and when they do that, they are cutting out food groups, [which] can cause repercussions, such as nutrient deficiencies,” Crandall says.
A big sandwich might make you sluggish; but, she says, cutting out carbohydrates – the centerpiece of several popular diets – has left many feeling like they’re forever out to lunch.
“I’ve seen a serious rise in people cutting out carbohydrates from their diet, whether it be they’re following an Atkins or South Beach or Paleo-type of diet,” Crandall says. “When you cut carbohydrates out of your diet, you essentially are restricting a lot of the B vitamins as well as essential nutrients to provide your brain’s energy it needs to function.” Low-carb consumption, and resulting deficiencies – including in vitamin B12, which is already not absorbed well by women over age 50 – can cause brain fog or mental fatigue as well as physical exhaustion, she says.
“So we know we need to make sure we’re getting B12, whether that be from fortification, supplementation or our primary source, which would be our food groups,” Crandall says. She recommends eating a variety of foods and consulting a registered dietitian if considering food restrictions to lose weight. That’s in addition to reviewing lab tests with your physician to unearth any potential deficiencies.
Haphazard calorie cutting and meal timing, including skipping meals, can also contribute to vitamin and mineral deficiencies, as well as fatigue, she says. “I always encourage my clients to eat within the first hour of waking up to better kind of fuel their metabolisms and get their brain and body functioning,” Crandall says.
Whether a vitamin or mineral deficiency is contributing to tiredness, experts say it’s always worth exploring the cause from a health and wellness standpoint. There’s no shortage of potential culprits for fatigue from lifestyle issues, such as lack of sleep and not exercising enough, to more insidious causes, including underlying heart disease.
Felicia Stoler, a registered dietitian nutritionist and exercise physiologist in private practice in Red Bank, New Jersey, recommends that those experiencing chronic fatigue see a doctor to rule out medical causes. The type of fatigue matters, too, in pinpointing if or how a vitamin or mineral deficiency may contribute. While iron, for example, might cause an overall feeling of tiredness, a lack of potassium and magnesium can contribute to muscle aches and cause a person to feel sore and weak, Stoler says.
She, too, typically starts with diet to address mineral and vitamin deficiencies that can trigger fatigue, from recommending more meat, fish, fruit – such as cantaloupe, bananas and apricots – plus potatoes, turnips and other veggies to deliver magnesium; to cashews and peanuts, whole-grain products, fish, poultry and eggs to offset a zinc deficiency, which can also cause fatigue.
“I add supplements as needed,” she says, most commonly for vitamin D deficiencies, which can also invite fatigue and hurt bone health in the long term, increasing the risk for osteoporosis.
Stoler says it’s important to heed vitamin and mineral deficiencies, including those that might contribute to fatigue, and to be mindful of the broader implications. “If you think about why we even started looking at adequate intake levels and dietary guideline levels,” she says, “it’s really preventing … illnesses or disease associated with deficiencies.”
Portable sensors and artificial intelligence are helping researchers decode animal communication—and begin to talk back to nonhumans.
Algorithms have revealed complex communication among Egyptian fruit bats. Analysis of audio and video recordings showed that the bats argue over food, distinguish between genders and use individual “signature calls” as names.
In the 1970s a young gorilla known as Koko drew worldwide attention with her ability to use human sign language. But skeptics maintain that Koko and other animals that “learned” to speak (including chimpanzees and dolphins) could not truly understand what they were “saying”—and that trying to make other species use human language, in which symbols represent things that may not be physically present, is futile.
“There’s one set of researchers that’s keen on finding out whether animals can engage in symbolic communication and another set that says, ‘That is anthropomorphizing. We need to … understand nonhuman communication on its own terms,’” says Karen Bakker, a professor at the University of British Columbia and a fellow at the Harvard Radcliffe Institute for Advanced Study. Now scientists are using advanced sensors and artificial intelligence technology to observe and decode how a broad range of species, including plants, already share information with their own communication methods. This field of “digital bioacoustics” is the subject of Bakker’s new book The Sounds of Life: How Digital Technology Is Bringing Us Closer to the Worlds of Animals and Plants.
Scientific American spoke with Bakker about how technology can help humans communicate with creatures such as bats and honeybees—and how these conversations are forcing us to rethink our relationship with other species.
[An edited transcript of the interview follows.]
Can you give us a brief history of humans attempting to communicate with animals?
There were numerous attempts in the mid-20th century to try to teach human language to nonhumans, primates such as Koko. And those efforts were somewhat controversial. Looking back, one view we have now (that may not have been so prevalent then) is that we were too anthropocentric in our approaches. The desire then was to assess nonhuman intelligence by teaching nonhumans to speak like we do—when in fact we should have been thinking about their abilities to engage in complex communication on their own terms, in their own embodied way, in their own worldview. One of the terms used in the book is the notion of umwelt, which is this notion of the lived experience of organisms. If we are attentive to the umwelt of another organism, we wouldn’t expect a honeybee to speak human language, but we would become very interested in the fascinating language of honeybees, which is vibrational and positional. It’s sensitive to nuances such as the polarization of sunlight that we can’t even begin to convey with our bodies. And that is where the science is today. The field of digital bioacoustics—which is accelerating exponentially and unveiling fascinating findings about communication across the tree of life—is now approaching these animals and not asking, “Can they speak like humans?” but “Can they communicate complex information to one another? How are they doing so? What is significant to them?” And I would say that’s a more biocentric approach or at the very least it’s less anthropocentric.
Taking a bigger view, I think it’s also important to acknowledge that listening to nature, “deep listening,” has a long and venerable tradition. It’s an ancient art that is still practiced in an unmediated form. There are long-standing Indigenous traditions of deep listening that are deeply attuned to nonhuman sounds. So if we combine digital listening—which is opening up vast new worlds of nonhuman sound and decoding that sound with artificial intelligence—with deep listening, I believe that we are on the brink of two important discoveries. The first is language in nonhumans. And that’s a very controversial statement, which we can dig into. And the second is: I believe we’re at the brink of interspecies communication.
What sort of technology is enabling these breakthroughs?
Digital bioacoustics relies on very small, portable, lightweight digital recorders, which are like miniature microphones that scientists are installing everywhere from the Arctic to the Amazon. You can put these microphones on the backs of turtles or whales. You can put them deep in the ocean, [put them] on the highest mountaintop, attach them to birds. And they can record sound continuously, 24/7, in remote places where scientists cannot easily reach, even in the dark and without the disruption that comes from introducing human observers in an ecosystem.
That instrumentation creates a data deluge, and that is where artificial intelligence comes in—because the same natural language processing algorithms that we are using to such great effect in tools such as Google Translate can also be used to detect patterns in nonhuman communication.
What’s an example of these communication patterns?
In the bat chapter where I discuss the research of Yossi Yovel, there’s a particular study in which he monitored [nearly two] dozen Egyptian fruit bats for two and a half months and recorded … [their] vocalizations. His team then adapted a voice recognition program to analyze [15,000 of] the sounds, and the algorithm correlated specific sounds with specific social interactions captured via videos—such as when two bats fought over food. Using this, the researchers were able to classify the majority of bats’ sounds. That is how Yovel and other researchers such as Gerry Carter have been able to determine that bats have much more complex language than we previously understood. Bats argue over food; they actually distinguish between genders when they communicate with one another; they have individual names, or “signature calls.” Mother bats speak to their babies in an equivalent of “motherese.” But whereas human mothers raise the pitch of their voices when talking to babies, mother bats lower the pitch—which elicits a babble response in the babies that learn to “speak” specific words or referential signals as they grow up. So bats engage in vocal learning.
That’s a great example of how deep learning is able to derive these patterns from [this] instrumentation, all of these sensors and microphones, and reveal to us something that we could not access with the naked human ear. Because most of bat communication is in the ultrasonic, above our hearing range, and because bats speak much faster than we do, we have to slow it down to listen to it, as well as reduce the frequency. So we cannot listen like a bat, but our computers can. And the next insight is, of course, that our computers can also speak back to the bat. [The software produces] specific patterns and uses those to communicate back to the bat colony or to the beehive, and that is what researchers are now doing.
How are researchers talking to bees?
The honeybee research is fascinating. A [researcher] named Tim Landgraf studies bee communication, which, as I mentioned earlier, is vibrational and positional. When honeybees “speak” to one another, it’s their body movements, as well as the sounds, that matter. Now computers, and particularly deep-learning algorithms, are able to follow this because you can use computer vision, combined with natural language processing. They have now perfected these algorithms to the point where they’re actually able to track individual bees, and they’re able to determine what impact the communication of an individual might have on another bee. From that emerges the ability to decode honeybee language. We found that they have specific signals. [Researchers have given these signals] funny names. [Bees] toot; they quack. There’s a “hush” or “stop” signal, a whooping “danger” signal. They’ve got piping [signals related to swarming] and begging and shaking signals, and those all direct collective and individual behavior.
The next step for Landgraf was to encode this information into a robot that he called RoboBee. Eventually, after seven or eight prototypes, Landgraf came up with a “bee” that could enter the hive, and it would essentially emit commands that the honeybees would obey. So Landgraf’s honeybee robot can tell the other bees to stop, and they do. It can also do something more complicated, which is the very famous waggle dance—it’s the communication pattern they use to convey the location of a nectar source to other honeybees. This is a very easy experiment to run, in a way, because you put a nectar source in a place where no honeybees from the hive have visited, you then instruct the robot to tell the honeybees where the nectar source is, and then you check whether the bees fly there successfully. And indeed they do. This result only happened once, and scientists are not sure why it worked or how to replicate it. But it is still an astounding result.*
This raises a lot of philosophical and ethical questions. You could imagine such a system being used to protect honeybees—you could tell honeybees to fly to safe nectar sources and not polluted ones that had, let’s say, high levels of pesticides. You could also imagine this could be a tool to domesticate a previously wild species that we have only imperfectly domesticated or to attempt to control the behavior of other wild species. And the insights about the level of sophistication and the degree of complex communication in nonhumans raises some very important philosophical questions about the uniqueness of language as a human capacity.
What impact is this technology having on our understanding of the natural world?
The invention of digital bioacoustics is analogous to the invention of the microscope. When [Dutch scientist Antonie] van Leeuwenhoek started looking through his microscopes, he discovered the microbial world…, and that laid the foundation for countless future breakthroughs. So the microscope enabled humans to see anew with both our eyes and our imaginations. The analogy here is that digital bioacoustics, combined with artificial intelligence, is like a planetary-scale hearing aid that enables us to listen anew with both our prosthetically enhanced ears and our imagination. This is slowly opening our minds not only to the wonderful sounds that nonhumans make but to a fundamental set of questions about the so-called divide between humans and nonhumans, our relationship to other species. And [it’s] also opening up new ways to think about conservation and our relationship to the planet. It’s pretty profound.
Viruses have evolved with humans for millions of years, so it’s no surprise they’ve evolved tricks to evade our natural, or innate, immune responses. Unfortunately, it’s often unclear what these tricks are. But now, thanks to researchers at the University of North Carolina (UNC) School of Medicine, one of these tricks has been revealed. It is particular to gammaherpesviruses, which include Kaposi sarcoma-associated herpesvirus (KSHV) and Epstein-Barr virus (EBV).
These viruses, which are DNA viruses, have been linked to several cancers and establish lifelong latency in the human population. According to the UNC researchers, these viruses use a human protein called barrier-to-autointegration factor 1, or BAF, to evade our innate immune response, allowing the viruses to spread and cause disease.
The researchers suggest that BAF and related proteins could prove to be valuable therapeutic targets. Indeed, if these targets can be engaged, it may be possible to prevent virus-instigated cancers such as Kaposi sarcoma, non-Hodgkin lymphoma, Hodgkin lymphoma, multicentric Castleman disease, nasopharyngeal carcinoma, and gastric cancer.
“We report that barrier-to-autointegration factor 1 (BAF)-mediated suppression of the cGAS-STING signaling pathway is necessary for reactivation of KSHV and EBV,” the article’s authors wrote. “We demonstrate a role for BAF in destabilizing cGAS expression and show that inhibiting BAF expression in latently infected, reactivating, or uninfected cells leads to increased type I interferon-mediated antiviral responses and decreased viral replication. Furthermore, BAF overexpression resulted in decreased cGAS expression at the protein level.”
The research was led by Blossom Damania, PhD, the Boshamer distinguished professor of microbiology and immunology and member of the Lineberger Comprehensive Cancer Center. She stated, “Viruses are in a constant battle with the cellular immune system, which includes the protein cyclic GMP-AMP synthase, or cGAS, which binds to viral DNA and sounds the alarm to trigger immune responses and fight the viral invaders. We’ve discovered that KSHV and EBV use a different host cell protein, BAF, to prevent cGAS from sounding the alarm.”
In the case of KSHV and EBV, the expression of BAF is increased upon infection, suggesting that these viruses take advantage of this host protein to blunt the immune response to infection. In a series of experiments, Damania’s laboratory found that BAF contributes to the degradation of the cGAS DNA sensor. With less cGAS protein available in the infected cell to detect DNA, the cells mount weaker immune responses, which allows these two viruses to replicate and spread more efficiently.
“BAF enables EBV and KSHV to reactivate from latency, replicate, and make more of themselves,” said first author Grant Broussard, a graduate student in the genetics and molecular biology curriculum at UNC Lineberger. “Our study highlights the prominent role that DNA detection pathways like the cGAS pathway play in controlling viral infection.”
He stressed that disrupting BAF activity with targeted therapies could reduce its immunosuppressive effects, thus restricting replication of these viruses to prevent the spread of disease.
Damania, who is a Leukemia and Lymphoma Society scholar and a Burroughs Wellcome Fund investigator in infectious diseases, added, “Preventing lytic replication will prevent transmission of these viruses and also reduce the global cancer burden associated with these two viruses.”
Consuming tree nuts such as macadamia nuts may have cardiovascular benefits.
A new study suggests that tree nuts may reduce certain risk factors for cardiovascular disease by modifying the metabolism of L-tryptophan, an amino acid.
In a controlled parallel trial, people with obesity or overweight who snacked on tree nuts as part of a 24-week weight loss and weight maintenance program experienced increased levels of serotonin, which can enhance mood.
Tree nuts are rich in nutrients, and eating them instead of other snacks was not associated with gaining weight.
The authors of a new study recently established a link between the consumption of tree nuts — almonds, cashews, hazelnuts, macadamia, pecans, pistachios, and walnuts — and a reduction in blood pressure, an important risk factor for cardiovascular disease (CVD). They’ve just published a new study that may explain the connection.
The researchers found that tree nuts increased levels of cardio-protective L-tryptophan metabolites in plasma and stool samples collected from study participants.
The study was a randomized, controlled, parallel study that involved 131 people with obesity or overweight over the course of a 24-week weight loss and weight maintenance program.
The diet of all participants included a daily 1.5-ounce snack. Of the 95 people who completed the study, 39 individuals snacked on pretzels as a control, while 56 other people ate tree-nut snacks of the same caloric value instead. At the end of the study period, the researchers analyzed fecal and blood plasma samples from each participant to ascertain the effects of their different snacks.
People who ate tree nuts experienced significant increases in levels of blood serotonin at week 12 (60.9%), and week 24 (82.2%), compared to their baseline levels. Those who ate pretzels experienced an increase in blood serotonin levels during the maintenance phase of the study, between weeks 12 and 24.
Tryptophan is the body’s only precursor of serotonin, which is credited with supporting a range of body functions, including mood, sleep, and digestion.
The research was funded by the International Tree Nut Council Nutrition Research & Education Foundation, along with the U.S. Department of Defense, VA Merit Review, and VA Career Development Award.
According to the Institute of Food Technologists (IFT), Americans eat 2.7 snacks a day, with an increasing number of young adults consuming as many as five or more.
Children get about 27% of their daily calorie intake from snacks, according to Harvard’s T.H. Chan School of Public Health.
Snacking can lead to unwanted weight gain, and unhealthy snacks often wind up replacing more nutritious foods in one’s daily diet.
Tree nuts contain substantial amounts of tryptophan, which is an essential amino acid that helps support growth and overall health.
Tryptophan is metabolized via three pathways, the kynurenine and serotonin pathways in body cells, and via the indole pathway in gut bacteria.
Disrupted tryptophan metabolism has been linked to metabolic diseases, including obesity and CVD.
The study’s corresponding author, Dr. Zhaoping Li, said the new study at least partially answers the question posed by her group’s earlier research: “One of the possible mechanisms is through [a] change of tryptophan metabolism.”
Dr. Li said in a press release issued by the International Tree Nut Council Nutrition Research & Education Foundation:
“We discovered some new associations between tryptophan metabolites and blood pressure, heart rate, and satiety in overweight/obese subjects, suggesting a broader impact of tryptophan metabolism in overall health, including cardiovascular health.”
“Gut microbiome and their metabolites can contribute to the regulation of our metabolism and mood,” she told Medical News Today.
There are other reasons the study makes sense, said Michelle Routhenstein, cardiology dietitian and preventive cardiology nutritionist at EntirelyNourished:
“[The authors’ interpretation of t]his study’s findings that tree nuts encourage CVD protective tryptophan metabolites and heart health makes sense due to its ability to help reduce inflammation, one of the main causes for atherosclerosis and heart disease.”
Dr. Li explained the connection between eating and emotions.
“Emotional eating is a significant factor [that contributes] to obesity. Nuts may improve mood through an increase of serotonin that is one of the key neurotransmitters to regulate mood,” she said.
The researchers were surprised to find an increase in serotonin levels in the tree nut group during the weight loss and maintenance sections of the study. Only the tree-nut group experienced increased levels of fecal serotonin.
By the end of the study, both groups had higher blood serotonin levels.
The authors speculate this final increase in blood serotonin for all participants may be evidence of the body’s response to weight loss.
“An increase in serotonin levels may be beneficial for people who are overweight or obese trying to achieve weight loss because of its role in energy expenditure and appetite suppression,” Routhenstein also noted.
“One and one-half ounces of tree nuts or peanuts provides [greater than] 10% of the adult male recommended dietary allowance for protein, iron, magnesium, phosphorus, zinc, copper, thiamin, and vitamin E. In addition, 1.5 oz (42 g) of tree nuts provides [greater than] 10% of the adult male RDA for vitamin B-6 and selenium.”
By way of example, Routhenstein listed some significant nutrients associated with a few tree nuts:
Pistachios contain phytosterols, potassium, and carotenoids that promote good blood vessel health and blood lipids.
Brazil nuts contain selenium, which helps combat oxidative stress and boost heart health and immune health.
Pecans are rich in copper, which helps with blood sugar metabolism and may help maintain a healthy thyroid gland.
Almonds are high in antioxidants, fiber, and protein. A single Brazil nut delivers 100% of the recommended daily amount of selenium. Although nuts are rich in energy, concerns about them being linked to weight gain appear unwarranted. Studies have shown that higher nut intake is associated with reductions in body weight and body fat, suggesting they do not contribute to weight gain.
A 48-year-old white man presented with a 4-week history of itchy lesions on the skin of his upper back and shoulders. The patient’s medical history included ulcerative colitis and a seizure disorder. In addition, Hodgkin’s lymphoma had been diagnosed three months earlier, for which the patient was receiving doxorubicin, bleomycin, vinblastine and dacarbazine chemotherapy. The lesions appeared during the patient’s fourth cycle of chemotherapy, after having received 64 units of bleomycin in total.
On examination, the patient had crisscrossing flagellate hyperpigmentation over his shoulders and neck (Figure 1A), and a red, raised lesion was developing on the back of his right wrist (Figure 1B). The patient reported linear reddish marks, similar to the one on his wrist, having preceded some of the hyperpigmented streaks. Histopathology of both lesions showed superficial perivascular dermatitis with eosinophils and minimal changes at the vacuolar interface, likely representing the same disease process, with features suggesting a drug-induced reaction.
(A) Crisscrossing flagellate hyperpigmentation over the shoulders and neck of a 48-year-old man receiving bleomycin for Hodgkin’s lymphoma. (B) The patient also presented with a linear, urticarial, eczematous lesion on his wrist.
Bleomycin is a glycopeptide antineoplastic antibiotic agent used in chemotherapy for Hodgkin’s lymphoma, squamous cell carcinoma and testicular cancer. The drug is metabolized by bleomycin hydrolase, but it has been shown to have adverse effects in tissues with relatively low levels of this enzyme, such as the lungs and skin.1,2 Minor trauma to the skin, such as pressure over bony prominences and scratching, is thought to increase blood flow and cause local accumulation of bleomycin.3 Flagellate dermatitis and subsequent hyperpigmentation in the skin is fairly common among patients receiving bleomycin, with reported incidence between 8% and 22%.3 Flagellate dermatitis is not typically associated with the other medications our patient was receiving.
Various topical and systemic therapies have been tried, but treatment mostly involves management of symptoms to limit trauma to the skin. The lesions typically resolve within six months after the withdrawal of bleomycin.4 After treatment with fluocinonide ointment and withdrawal of bleomycin, signs of active inflammation resolved, and our patient’s hyperpigmentation was lightened at a follow-up appointment five weeks later.
The Dying with Dignity commission of the Quebec National Assembly has issued its report after two years of public hearings, consultations with experts and visits to countries where there is now some experience with a range of options on ways of dying.1 The commission and the Charest government deserve equal praise for their thoughtful report and their courage in addressing this controversial topic. The principal theme of the report holds that palliative care has come of age and is adequate to meet the needs of most dying people; however, it is underprovided, particularly in remote and rural areas.2 A second important theme concerns “l’aide médicale à mourir” — medical assistance to die. On this subject, the report calls for a change in thinking, arguing that there will still be cases where suffering is great, irreversible and unrelievable, such that the only option is actively helping a person to die.
The recommendation is based on two legal considerations. First, the civil code recognizes the right of adult patients to make medical decisions concerning their care, even if refusing or stopping treatment may result in their death. Second, both the Quebec and Canadian charters of rights and freedoms enshrine the rights to personal dignity and integrity. These rights imply a respect for self-determination and a person’s physical and psychological well-being. These are powerful arguments and suggest that an individual should be able to make life’s important decisions in a free and unconditional way, including deciding when the struggle to stay alive should end. However, this line of reasoning only supports an individual’s right to end his or her own life.
Proponents of “dying with medical assistance” must argue that a patient’s rights invoke a corresponding medical duty to provide the means if a patient cannot, and it follows that this should be done in a safe and expert way. Hence, the act of assisting death would need to move from the context of being criminal to being part of the continuum of end-of-life care.
Many physicians and patients will find this a shocking prospect to consider. If their views are to prevail, they will need to argue why there should be limits to a person’s autonomy. Human dignity may imply certain rights and freedoms, but conflicts among people’s rights are hard to resolve. Frail, dependent patients often feel a burden to their families or caregivers, and the unspoken possibility of a quick resolution to their predicament may complicate an already stressful situation. Removing the legal barrier to ending another’s life may ensure the self-dignity of those who wish to die, but may distress and remove the self-dignity of more people who wish to live.
Others will welcome this report as heralding a needed change in the way we perceive life and its ending. They will need to argue why patient autonomy trumps other considerations and why we should prepare to embrace euthanasia as routine. Proponents of euthanasia cannot assume that the practice will be restricted to extreme cases of untreatable suffering; they should be prepared to accept the implications of unrestricted choice, or a patient’s “right to die.” For example, in Belgium, where euthanasia has been legal since 2002,3 half of all nonsudden deaths are the result of some decision to hasten the end of life; 4% of these deaths are defined as euthanasia, and 11% involve continuous deep sedation or rendering the person unconscious until he or she dies.3
If Quebec chooses to proceed with the report’s recommendations, those who disagree will have to acknowledge that society’s values have become more pluralistic. However, any change in the law must safeguard both health care workers and patients from possible abuses in its application.4
Public consultation in Quebec is only the first step. A change to the criminal code will need more national dialogue and action from federal lawmakers. Change should not be the result of one provincial Supreme Court decision (www.courts.gov.bc.ca/jdb-txt/SC/12/08/2012BCSC0886.htm). Issues such as who is expert at providing this new option, how it will be provided, and how to assist patients who do not fit the criteria or families who disagree with the patient’s choice will be debated in a brave new future.
The ethics of euthanasia are a familiar debate in Canada; one that may have been theoretical until recently, because of the tacit assumption that doctors do not kill people. In Quebec, the debate is moving from theory toward practice. Which way will legislation go? Will the rest of Canada follow? Those who care about the answers to these questions must speak up now, and with conviction.
Carbohydrates are found in breads, cereals and other grains, fruit, vegetables and milk. They’re also in ultra-processed fast foods, cakes, chips and soft drinks.
These days, low-carb diets are promoted as a weight-loss solution, to beat heart disease and as better for diabetes. But how do these claims match up with the latest research?
A new review of the evidence found long-term low-carb dieters lost just under a kilo more weight than other dieters. However the review concluded there was no evidence low-carb diets have any additional health benefits.
In fact, if you’re on a low-carb diet, you’ll need to pay closer attention to what you eat to make sure you get enough essential vitamins, minerals, dietary fibre and other phytonutrients.
What Did the Reviewers Investigate?
The Cochrane review included 61 randomised controlled trials (the highest level of evidence) with almost 7,000 adults with excess body weight. About 1,800 had type 2 diabetes. People in the healthy weight range were not included.
The reviewers compared weight-loss diets that varied in carbohydrate content:
lower carbohydrate diets. This included very low-carb or ketogenic diets (less than 50g of carbs a day or less than 10% of your total energy from carbs) and low-carb diets (50-150g of carbs per a day, or less than 45% of total energy from carbs)
“balanced” carbohydrate diets (150+ grams of carbs a day, or 45-65% of your total energy from carbs).
Here’s an example comparing how a very low-carb, low-carb and balanced carb one-day meal plan might look. The portion sizes differ between the meals to keep the total kilojoules about the same. Note, the reviewers grouped the first two low carb diet categories together. Author provided
What Did They Find?
The reviewers found that among adults with excess body weight (but who didn’t have type 2 diabetes), those following lower-carb diets for 3-8.5 months lost, on average, one kilogram more weight than those on balanced carb diets.
However, when they ensured restrictions in energy intake were the same in both groups, by providing the food or meal plans, the difference was about half a kilogram.
In longer-term weight-loss interventions lasting one to two years, the average difference in weight-loss between those on low-carb versus balanced carb diets was just under one kilogram.
There isn’t a great different in weight-loss outcomes between those on low-carb diets and those on balanced carb diets.
The average weight lost by groups on any weight-reducing diet varied greatly across the trials from less than one kilogram in some, up to about 13kg in others.
The studies in adults with type 2 diabetes found greater initial weight loss on low-carb diets compared to balanced carb diets: 1.3kg over three to six months. However, in longer interventions that lasted between one to two years, there was no difference.
In the small group of studies that included a maintenance period at the end of the weight-loss intervention, there were no differences in weight-loss in adults either with or without type 2 diabetes.
There were no significant differences in other health measures, including blood pressure, cholesterol, blood sugar control or risk of constipation. And they found no important clinical differences in results based on the extent of participants’ carb restriction.
Overall, the review shows that whether you prefer a lower carb or a balanced carb eating pattern, both can work for weight loss.
Nutrients to Monitor on a Low-Carb Diet
Carbohydrate is a macronutrient. Your body uses it to produce energy to fuel your muscles, brain, lungs and other vital processes.
Healthy foods with carbs – breads, cereals and other grains, fruit, vegetables and milk – are packed with other important nutrients, especially dietary fibre, thiamine, calcium and folate.
Without careful planning, a low-carb diet could also be lower in these nutrients. So how can you ensure you’re consuming enough? Here’s what to look out for – and some lower- and higher-carb options.
Dietary fibre is needed to keep your bowel function regular and promote growth of healthy bacteria in your colon.
Lower carb sources: green leafy vegetables, avocado, broccoli, peanuts
Higher carb sources: wholemeal bread (Australian bread-making flour is fortified with folic acid), fortified wholegrain cereals, brown rice, oranges.
Ultimately, if you love carbs and want to lose weight, you can. Plan to lower your kilojoule and carb intake by not eating ultra-processed, energy-dense, nutrient-poor (junk) foods, while still eating carbohydrates from healthy foods.
This antibiotic contributes to rising problems with antibiotic-resistant bacteria, kidney stones and psychotic episodes; data demonstrates it increases your risk of a fatal heart condition. I’ll share how to avoid this risk.
STORY AT-A-GLANCE
Fluoroquinolones, long associated with Achilles tendonitis and rupture, have been demonstrated to increase your risk of aortic dissection (a tear in the wall of the major artery, allowing blood to flow between the layers) or aortic rupture, which can lead to death
Even though “black-box” warnings are now attached to them, fluoroquinolones are still often prescribed for upper respiratory infections or urinary tract infections
Antibiotic use can trigger a permanent change in your gut microbiome, which accounts for nearly 80% of your immune system function, so it is important to use antibiotics only when absolutely necessary
You may reduce your risk of bacterial and viral infections by supporting your immune system through simple lifestyle measures, such as quality sleep, fermented foods, regular exercise and optimizing your vitamin D level
Research shows your body’s microbiome has nearly 39 trillion bacteria.[[1] During early years, your family, dietary intake and environmental exposure contribute to the variety in your microbiome, influencing your lifelong health. Everyday activities such as brushing your teeth, eating, kissing someone or handling a family pet also affect your microbiome.
This composition may be as distinct to you as a fingerprint and plays an enormous role in disease prevention, and influences the function of your skin, lungs, breast and liver.[2] Harmful bacteria can trigger illness and disease, which is frequently treated with antibiotics. Of the 10 most commonly prescribed, two are from the antibiotic class of fluoroquinolones.[3]
The Food and Drug Administration (FDA) first added a boxed warning to fluoroquinolones in 2008, due to the increased risk for tendinitis and tendon rupture.[4] Boxed warnings, also referred to as black box warnings, appear on prescription drug labels designed to call attention to serious or life-threatening risks.[5]
An additional warning was added in 2011 for those suffering from myasthenia gravis, and updates were included in 2013 describing irreversible peripheral neuropathy.[6] In 2018, the FDA warned fluoroquinolone antibiotics may increase the occurrence of ruptures or tears in the aorta.[7] And, in January 2022, the FDA decided:[8]
“We have determined that fluoroquinolones should be reserved for use in patients with no other treatment options for acute bacterial sinusitis, or ABS, acute bacterial exacerbation of chronic bronchitis (ABECB), and uncomplicated UTI because the risks generally outweighs the benefits.
For some serious bacterial infections the benefits of fluoroquinolones outweigh the risks, and it is appropriate for them to remain available as a therapeutic option.”
Yet, despite these warnings, researchers found in April 2022 that fluoroquinolones are still among the most-prescribed antibiotics around the world.[9] They concluded that some health care workers may have an “unsatisfactory knowledge” of the safety profiles and risks of these drugs, and that more education on adverse reactions to fluoroquinolones may be needed.
FDA Warning Links Fluoroquinolones With Aortic Damage
The aorta is the main artery in your body supplying oxygenated blood to your circulatory system. The artery comes from the left side of your heart and runs down the front of your backbone. The review by the FDA found fluoroquinolone antibiotics increase the risk of tears in the aorta, also called aortic dissections, or ruptures of an aortic aneurysm, leading to excessive bleeding and death.
The findings occurred when antibiotics were given by mouth or through an injection. This led the FDA to caution against the use of fluoroquinolone antibiotics in those at risk, unless there are no other treatment options available.
Specifically, the antibiotic should not be used in those who are at risk for, or have a current, aortic aneurysm, such as those suffering peripheral atherosclerotic vascular disease, hypertension and specific genetic conditions such as Ehlers-Danlos syndrome or Marfan syndrome.[10]
Findings were pulled from four published observational studies, which taken together demonstrated a consistent association between aortic dissection or rupture and fluoroquinolone use. The underlying mechanism could not be determined from those studies.
Some of the commonly used fluoroquinolones include ciprofloxacin (Cipro), levofloxacin (Levaquin), gemifloxacin (Factive) and moxifloxacin (Avelox). These are prescribed to treat upper respiratory and urinary tract infections. In a statement, the FDA warns:[11]
“Fluoroquinolones should not be used in patients at increased risk unless there are no other treatment options available.
Health care professionals should avoid prescribing fluoroquinolone antibiotics to patients who have an aortic aneurysm or are at risk for an aortic aneurysm, such as patients with peripheral atherosclerotic vascular diseases, hypertension, certain genetic conditions such as Marfan syndrome and Ehlers-Danlos syndrome, and elderly patients.”
Upper Respiratory Infections Are Often Viral
Viruses commonly trigger upper respiratory infections (URIs) with symptoms of runny nose, cough, low grade fever, sore throat and difficulty sleeping. URIs represent the most common acute illness in the outpatient setting, often related to the common cold, which is typically a mild, self-limited inflammation of the mucous membranes in the airways.[12]
Bacterial illness may follow a viral illness as a secondary infection, and commonly includes symptoms persisting longer than 14 days with a fever higher than one might typically expect from a virus. Oftentimes, the fever gets worse a few days into the illness rather than improving.[13]
Unfortunately, one of the more common reasons fluoroquinolones are prescribed is for upper respiratory infections, ordinarily triggered by a virus. According to the U.S. Centers for Disease Control and Prevention (CDC),[14] the highest number of community antibiotic prescriptions are written in the southeastern states.
Fluoroquinolones ranked No. 4 in the highest number of prescriptions written per 1,000 people in the CDC’s outpatient antibiotic prescription index in 2016. Because providers were still opting for fluroquinolones more than they should for respiratory infections such as pneumonia, the CDC reported in 2021 that an expert panel had recommended the use of these drugs for this purpose be lowered by 90%.[15]
Bacterial and viral infections are dissimilar in important respects related to the organism’s structure and the way they respond to medications. Although both are too small to be seen with the naked eye, the largest virus is actually smaller than the smallest bacteria.[16] Unlike the more complex bacteria, viruses cannot survive without a host and only reproduce by attaching themselves to other cells. Also, unlike bacteria, most viruses are specific in the cells they attack.
The differences in the structure and complexity of the organism have an impact on the type of medication that may be effective against it. Viral infections are not affected by antibiotics such as fluoroquinolones. In fact, using antibiotics for viral infections only contributes to the rising number of antibiotic-resistant infections.
Fluoroquinolones Linked to Multiple Health Concerns
Fluoroquinolone antibiotics have been associated with Achilles tendon ruptures and damage for over a decade. Other severe adverse events, such as retinal detachments as well as aortic aneurysms, may also be associated with other systems requiring collagen formation.[17] This may also explain, at least in part, how the drug increases your risk of aortic rupture or dissection, as collagen[18] lines your arteries and veins to allow for stretch as the heart pumps blood.[19]
Subsequently, in July 2022 the FDA mandated another warning, “alerting physicians to the increased risk of tendonitis and tendon rupture associated with their use.”[20] According to Dr. Renata Albrecht, who heads the FDA’s Division of Special Pathogen and Transplant Products, “Achilles’ ruptures associated with fluoroquinolones are three to four times more frequent than ruptures among people not taking these drugs.[21]
So, if you are taking these antibiotics, you should seek immediate medical care if you experience soreness or inflammation in muscles or tendons. You should also not exercise while your joints are affected.
The drugs are also powerful iron chelating agents that may trigger epigenetic changes through the loss of agents requiring iron as a cofactor. As noted in one study, this may also explain the classic renal toxicity associated with the antibiotics:[22]
“At sub-millimolar concentrations, these antibiotics inhibited jumonji domain histone demethylases, TET DNA demethylases and collagen prolyl 4-hydroxylases, leading to accumulation of methylated histones and DNA and inhibition of proline hydroxylation in collagen, respectively. These effects may explain fluoroquinolone-induced nephrotoxicity and tendinopathy.”
A recent study[23] has linked the use of fluoroquinolones to the rising number of children and adults affected by kidney stones. The odds of stones increased 1.5 times with the use of fluoroquinolones and exposure within 3 to 12 months was associated with greater risk. It appeared children and adolescents were particularly susceptible.
Reactions can be bodywide, impacting your central nervous system and musculoskeletal, visual and renal systems, sometimes simultaneously. Among the serious reactions reported are:[24]
Memory impairment
Delirium
Agitation
Disorientation
Retinal detachment[25]
Hearing loss and/or tinnitus[26]
Disturbance in attention
Kidney stones
Kidney failure[27]
Hypoglycemia leading to coma
Aortic rupture or dissection
Tendon rupture or dissection
More Psychiatric Side Effects Than You Might Imagine
Researchers recommend further study to understand the pathogenesis caused by antibiotics in order to treat antibiotic-associated diseases through the mitigation of the intestinal environment — restoring it to its original state.[28]
Further research has demonstrated an imbalance in gut microbiome caused by antibiotics can negatively affect health in a number of ways and for long periods of time.[29] If your physician prescribes one of these dangerous antibiotics, ask to use another one. It would be unusual a fluoroquinolone would be the only antibiotic that could be used to treat your infection.
Remember, these dangerous antibiotics should be used as a last resort only. If it is necessary, be sure to carefully read the package insert and all the warnings, and seek medical attention the moment you notice a side effect.
The late Dr. David Flockhart, who served as professor of medicine and chief of clinical pharmacology at Indiana University School of Medicine, and who before his death was considered one of the leading experts in fluoroquinolone side effects, said in 2012 that “as many as one-third of patients taking a fluoroquinolone will experience some sort of psychiatric side effect.”[30]
But the thing is, Flockhart had tried to call attention to these drugs over 10 years earlier, in 2001, when he decried Ciprio specifically, as he tried to stress just how dangerous fluoroquinolones are:[31]
“Cipro is basically a big gun whose benefits outweigh its risks in certain circumstances. But the bigger the gun you use, the more damage you can expect as collateral.”
Antibiotics Trigger Permanent Changes to Your Gut Microbiome
The health of your gut microbiome is a game changer. It has become increasingly apparent in recent years that the composition of your gut microbiome plays an enormous role in your health and disease prevention. Cancer and many other health conditions have been traced back to the influence of gut microbes, including obesity, depression, Parkinson’s and allergies, just to name a few.
Since your gut is the main residence of your immune system,[32] disrupting your gut microbiome automatically disrupt your immune function, which can have far-reaching consequences. One way antibiotics can promote disease is by creating an oxygen-rich environment in your intestines, favoring the growth of pathogenic bacteria.
Beneficial microbes grow in an anaerobic (no oxygen) environment, while pathogenic bacteria need oxygen to survive.[33] Data suggest even one course of antibiotics can negatively alter your microbiome for up to one year, which is why it’s crucial to use antibiotics only when it is absolutely necessary.[34]
However, Dr. Martin Blaser with the Langone Medical Center at New York University argues the impact of antibiotics on gut bacteria may be permanent. In an editorial in Nature he writes:[35]
“Early evidence from my lab and others hint that, sometimes, our friendly flora never fully recover. These long-term changes to the beneficial bacteria within people’s bodies may even increase our susceptibility to infections and disease.
Overuse of antibiotics could be fueling the dramatic increase in conditions such as obesity, Type 1 diabetes, inflammatory bowel disease, allergies and asthma, which have more than doubled in many populations.”
Support Your Health and Your Gut
The stronger your immune system, the less chance any microbe will have of gaining a foothold in your body. Below are some basic strategies for supporting your immune system and preventing illness.
Optimize your diet — Avoid foods that tax your immune system, such as trans fats, fried foods, processed foods, sugars and grains. Seek to reduce your net carbohydrate (sugar, grains, fructose) and protein intake, replacing them with high-quality healthy fats.
Balance your gut flora — One of the best ways to support your gut is by incorporating naturally fermented foods into your diet, working up to 4 to 6 ounces per day. You may take a high-quality probiotic supplement, but fermented foods tend to offer the greatest benefit.
Exercise regularly — Exercise improves the circulation of immune cells in your blood, creating a more efficient system at locating and eliminating pathogens in your body. Make sure your fitness plan incorporates weight training, high-intensity exercises, stretching and core work.
Get plenty of restorative sleep — Research shows sleep deprivation has the same effect on your immune system as physical stress or disease, which is why you may feel ill after a sleepless night.
Reduce stress — High levels of stress hormones can diminish your immunity, so be sure you’re implementing some sort of stress management. Meditation, prayer, yoga and Emotional Freedom Techniques (EFT) are all excellent strategies for managing stress, but you’ll have to find what works best for you.
Optimize vitamin D levels — Studies show inadequate vitamin D can increase your risk for MRSA and other infections. Your best source of vitamin D is through sensible sun exposure. Monitor your vitamin D level to confirm they’re in a therapeutic range of 60 to 80 ng/mL. If you can’t get UV exposure, consider taking an oral vitamin D3 supplement, in conjunction with magnesium and vitamin K2 (MK-7).
In addition to the lifestyle measures listed above, there are natural agents that are naturally antibacterial, including the following:
Vitamin C — Vitamin C’s role in preventing and treating infectious disease is well established. Intravenous vitamin C is an option, but if you don’t have access to a practitioner who can administer it, liposomal vitamin C is the most potent oral form. For more information on vitamin C, listen to my interview with Dr. Ronald Hunninghake (hyperlinked above), an internationally recognized vitamin C expert.
Garlic — Garlic is a powerful antibacterial, antiviral and antifungal. It can stimulate your immune system, help wounds heal and kill antibiotic-resistant bacteria. For highest potency, the garlic should be eaten fresh and raw (chopped or smashed.)
Olive leaf extract — In vitro studies show olive leaf extract is effective against Klebsiella, a gram-negative bacteria, inhibiting its replication, in addition to being toxic to other pathogenic microbes.
Manuka honey — Manuka honey, made from the flowers and pollen of the Manuka bush, has been shown to be more effective than antibiotics in the treatment of serious, hard-to-heal skin infections. Clinical trials have found Manuka honey can effectively eradicate more than 250 clinical strains of bacteria, including resistant varieties such as MRSA.
Tea tree oil — Tea tree oil is a natural antiseptic proven to kill many bacterial strains.[36]
Colloidal silver — Colloidal silver has been regarded as an effective natural antibiotic for centuries, and recent research shows it can even help eradicate antibiotic-resistant pathogens. If you are interested in this treatment, make sure you read the latest guidelines for safe usage of colloidal silver as there are risks with using it improperly.
Following 2 consecutive years of decline, total suicides in the U.S. rose from nearly 46,000 in 2020 to just over 48,000 in 2021, researchers wrote in Morbidity and Mortality Weekly Report.
The report noted that suicide rates in this timespan increased the most among American Indian or Alaskan Native individuals, while the greatest decrease in suicide rates was among white individuals.
U.S. suicide rates had declined for 2 years, but increased from 2020 to 2021.
“Research indicates that suicide is preventable through a comprehensive public health approach that relies on data to drive decision-making, multisectoral partnerships to expand reach, and implementation and evaluation of multiple culturally relevant prevention strategies,” Deborah M. Stone, ScD, of the CDC’s National Center for Injury Prevention and Control, and colleagues wrote. “CDC’s Suicide Prevention Resource for Action supports states and communities to prioritize interventions with the best available evidence that can save lives.”
Stone and colleagues analyzed changes in racial and ethnic suicide rates from 2018 to 2021 National Vital Statistics System multiple cause-of-death mortality files. Researchers calculated 95% CIs with the direct method and the 2000 U.S. standard population. Included Hispanic individuals could be of any race, and those with unknown ethnicity were excluded from race and ethnicity groups but were included in the overall total.
The researchers reported that suicide rates were highest among non-Hispanic American Indian or Alaskan Native individuals at 28.1 per 100,000 overall. This group experienced the highest relative percentage change from 2018 to 2021 at 22.3 to 28.1 per 100,000 (26% increase).
Rates also increased significantly among non-Hispanic Black individuals, from 7.3 to 8.7 per 100,000 (19.2% increase) and among Hispanic individuals, from 7.4 to 7.9 per 100,000 (6.8% increase) from 2018 to 2021. Non-Hispanic white individuals showed the greatest overall decline in suicide rates, from 18.1 to 17.4 (3.9% decline).
Suicide rates of Black individuals aged 10 to 24 years increased significantly, from 8.2 to 11.2 (36.6% increase). Overall, suicide rates increased among those aged 25 to 44 years at 5%, American Indian or Alaskan Native at 33.7%, Black at 22.9%, Hispanic at 19.4% and non-Hispanic multiracial at 20.6% from 2018 to 2021.
The researchers reported that overall, suicide rates of individuals aged 45 to 64 years decreased significantly at –12.4%, among non-Hispanic Asian at –15.9%, Hispanic at –9.3% and white at –11.5%. Suicide rates of individuals aged at least 65 years showed no significant changes.
“Significant increases among young Black persons aged 10 to 24 years and across multiple racial and ethnic populations aged 25 to 44 years raise particular concern,” Stone and colleagues wrote. “Suicide is a complex problem related to multiple risk factors such as relationship, job or school, and financial problems, as well as mental illness, substance use, social isolation, historical trauma, barriers to health care and easy access to lethal means of suicide among persons at risk.”
It sounds counterintuitive. However, there are many reasons why there is a lack of study, including this cancer’s aggressive nature, poor survival rate, and the great differences in how it presents across countries and even between sexes.
Esophageal cancer is not as common in the United States. However, a 2022 analysis presented at a conference found that from 2012 to 2019, the rate of esophageal cancer for people ages 45 to 64 almost doubled, based on 5 million people’s data in Florida.
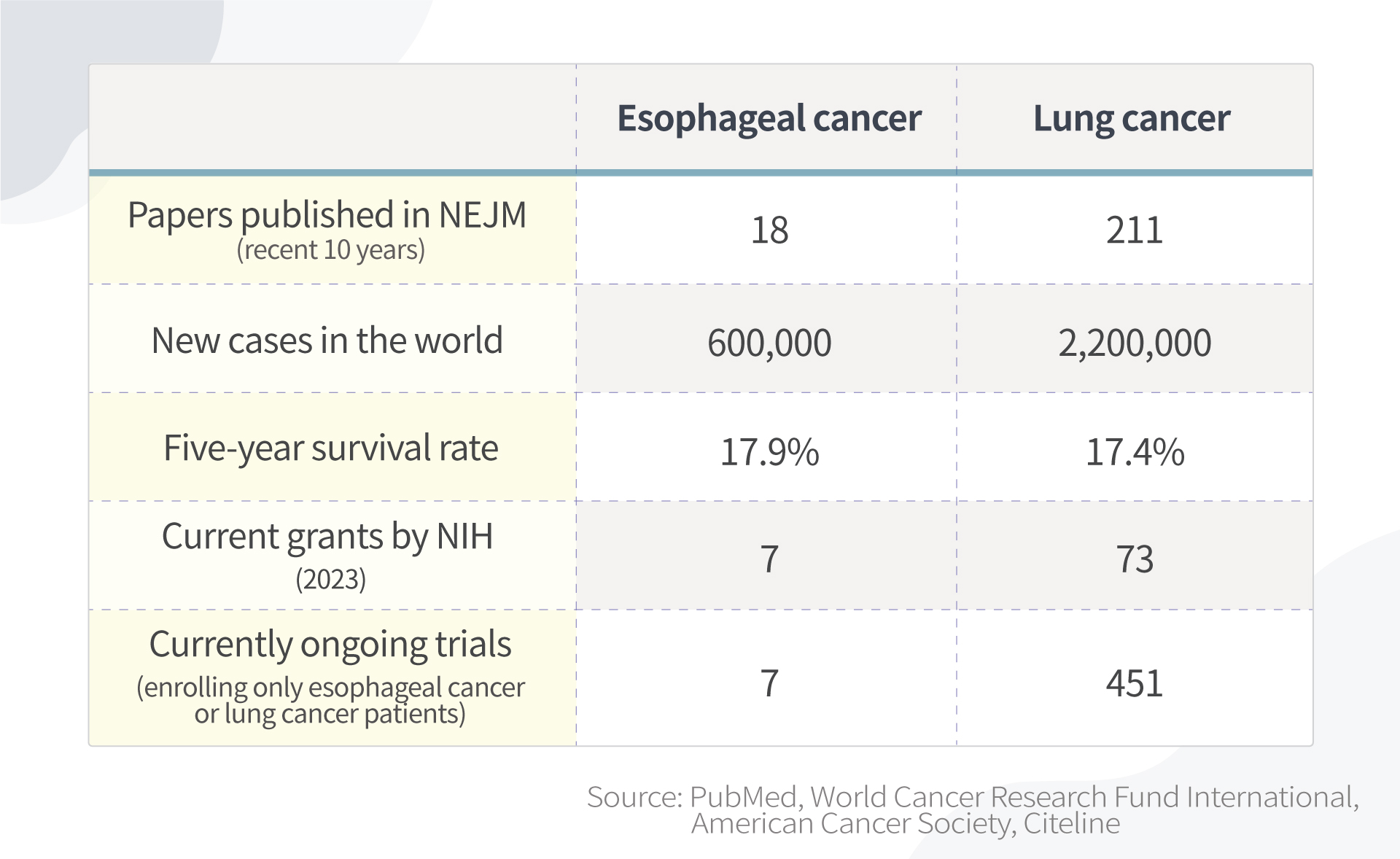
Esophageal Cancer Is One of the Least Studied Common Cancers, 3 Reasons
By searching publications in the New England Journal of Medicine, the world’s leading medical journal, studies in esophageal cancer are far fewer than those in lung cancer.
Studies in esophageal cancer are far fewer than those in lung cancer. Information accessed February 2023.
There are multiple reasons for this:
1. Incidence rates are relatively low in the United States
The majority of esophageal cancer cases are outside of the United States. Esophageal cancer makes up only about 1 percent of cancer cases in the United States.
The National Institutes of Health (NIH) is the world’s largest public funder of biomedical research. However, because esophageal cancer is so uncommon in the United States, it is difficult to be granted funding from institutions like NIH to research it.
Also, because there aren’t many esophageal cancer patients in the United States, there is less motivation for pharmaceutical companies to develop new drugs targeting esophageal cancer.
2. Presents differently between sexes and among races, but root causes unknown
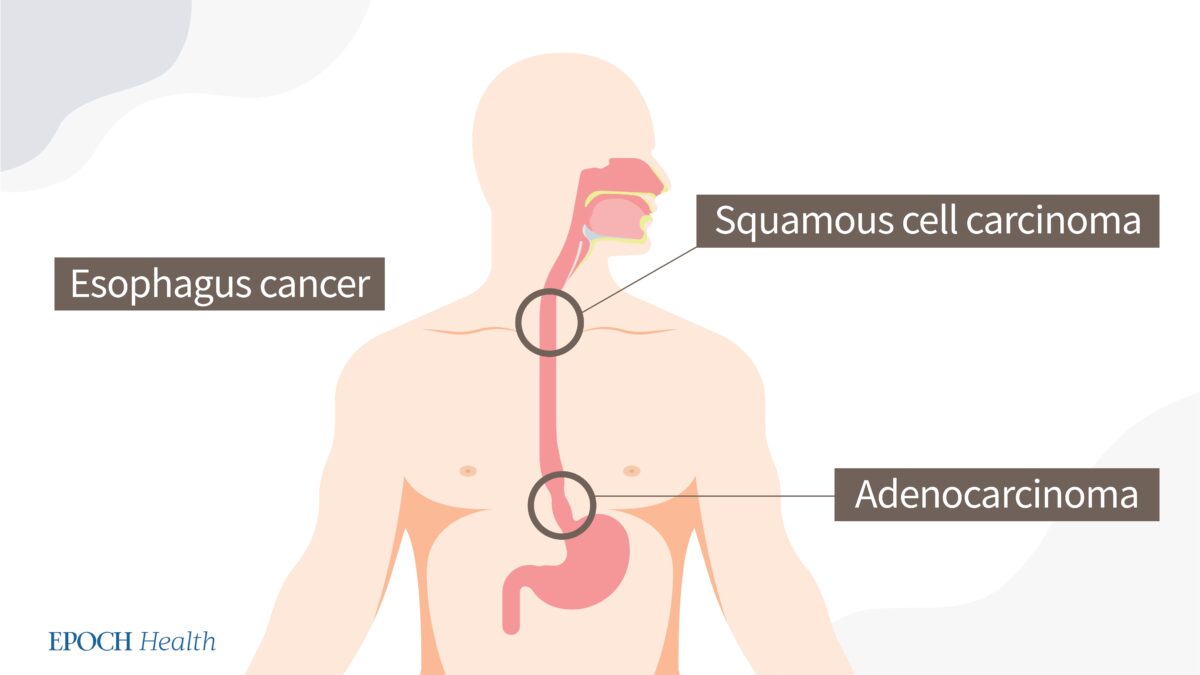
Most esophageal cancers can be classified as one of two types: adenocarcinoma or squamous cell carcinoma.
Squamous cell carcinoma is the predominant histological type worldwide. This form mainly occurs in the “Asian Esophageal Cancer Belt,” which includes China.
However, in countries like the United States, Australia, the UK, and Western Europe, adenocarcinoma incidence is higher.
Two types of esophageal cancers. (The Epoch Times)
Similar to other cancer types, esophageal cancer exhibits sex disparities in occurrence. The incidence of esophageal adenocarcinoma is about eight times higher (pdf) in men than in women. Sex is known to be an independent prognostic marker for squamous cell carcinoma but not for adenocarcinoma, with survival rates being higher in women.
Esophageal cancer affects races differently, as well. While nonwhite patients were more likely to develop squamous cell cancer or a tumor in the middle esophagus, white patients were more likely to develop adenocarcinoma or a tumor in the lower esophagus. The root causes for these differences are still unknown.
Esophageal cancer is very complicated and differs across sex, race, region, and socioeconomic status. Thus, as the number of patients in the United States is limited, and with so many factors to consider, it is hard to get statistically significant results.
3. High death rate
On average, according to a paper published in the World Journal of Gastroenterology, about 40 to 45 percent of patients die within a year after diagnosis, so it is hard to recruit patients for studies if they are too sick. This contributes to a limited number of eligible patients.
Can Esophageal Cancer Be Identified Early?
The deadliness of cancer depends on when it is found. If esophageal cancer is found while it is still localized, the patient has a 46 percent chance of survival for five more years. If it is found while it is regional, that chance drops to 26 percent, and if found while distant, only 5 percent of patients will survive five more years.
Localized means that the cancer is growing only in the esophagus.
Regional means that the cancer has spread to nearby lymph nodes or tissues.
Distant means that the cancer has spread to organs or lymph nodes away from the main tumor.
Unfortunately, in the earliest stages when it’s easiest to treat, esophageal cancer has very few symptoms. Therefore, it is called a silent killer.
Can screening be done? In the United States, screening for esophageal cancer is not recommended, partially because the incidence is low; therefore, for society overall, it is not cost-effective at lowering risk.
Will There Be a Sharp Increase in Esophageal Cancer in the US?
The researchers who presented their findings at the 2022 Digestive Disease Week conference argue that more middle-aged persons should be checked for esophageal cancer in light of their study, as esophageal cancer may be increasing among middle-aged people.
That being said, the study’s findings should be analyzed with caution, as the study only included adults residing in Florida, meaning it’s not wholly representative of the population of the United States. For instance, the increase might be due to Florida’s growing population (it has grown by 14.6 percent in the last decade and growth accelerated during the pandemic). Florida’s late-night eating habits may also influence the increase; Miami is a late-night eating town compared to the rest of the country. More on this later.
What Are Common Risk Factors of Esophageal Cancer?
As mentioned, nearly half of the patients die within a year once they are diagnosed—which is why prevention is very important.
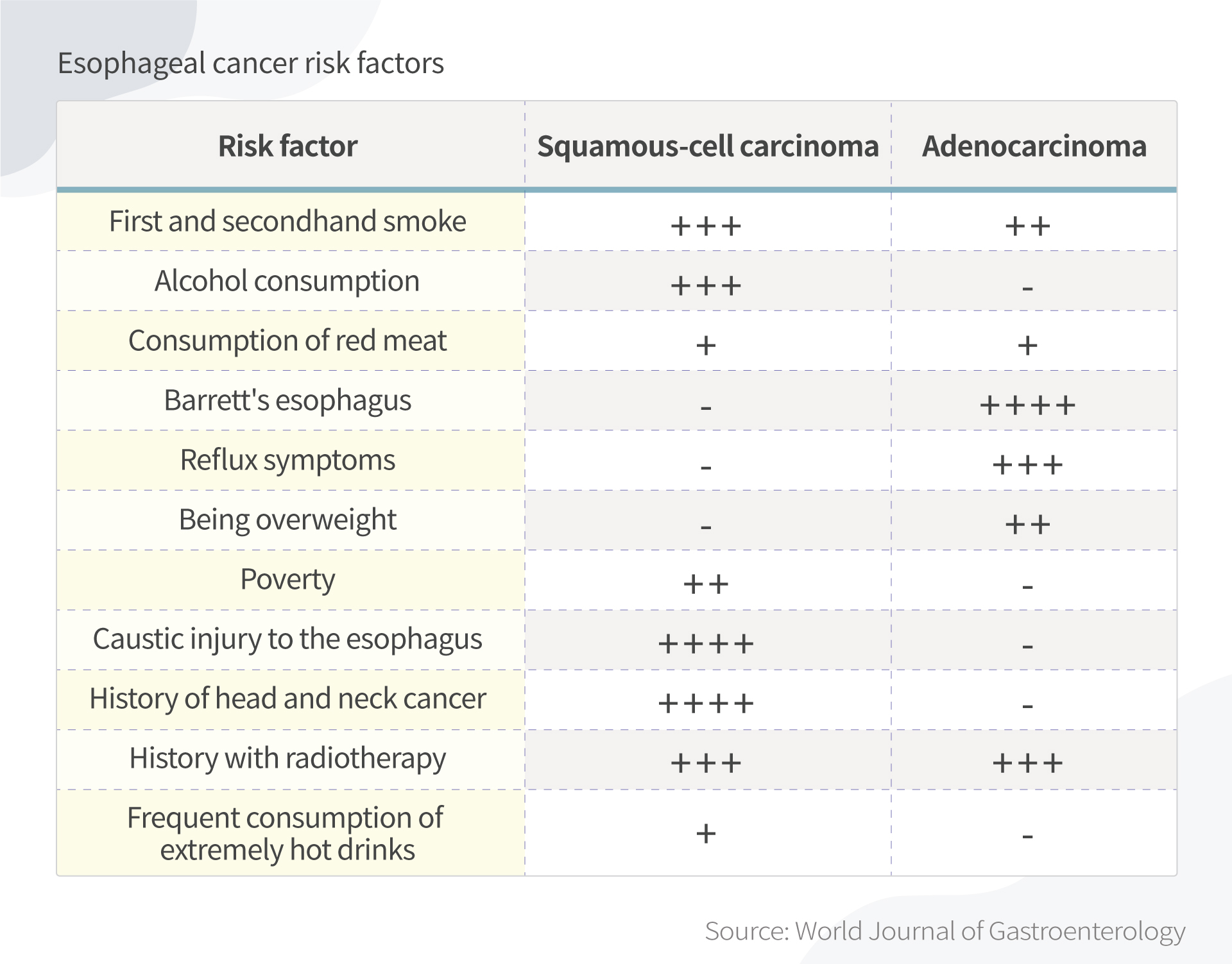
Smoking, alcohol, obesity, drinking hot tea, red meat consumption, poor oral health, low intake of fresh fruit and vegetables, and low socioeconomic status have all been associated with a higher risk of esophageal cancer, according to the World Journal of Gastroenterology paper.
Risk factors of adenocarcinoma and squamous cell carcinoma. (The Epoch Times)
5 Ways to Prevent Esophageal Cancer
There are a few things that you can do now to lower your chance of developing esophageal cancer.
1. Avoid eating late
When you eat late at night and then lie down, the contents of your stomach press harder against the lower esophageal sphincter. This can trigger gastroesophageal reflux disease (GERD), or acid reflux. Some ways to avoid this include:
Waiting two to three hours after eating to go to bed.
Not snacking late at night.
Eating larger meals earlier in the day. Try to make your last meal small.
Many people love to have late-night dinners and drinks, especially while on vacation. Although having to restrain yourself from delicious food at night might be hard, it is rewarding to control your weight and prevent other diseases beyond esophageal cancer.
2. Avoid hot foods and liquids
Different people have different eating habits. I hear discussions about why Chinese people like drinking hot water. It can be relaxing and soothing. However, drinking very hot beverages may be associated with esophageal cancer risk.
Thermal irritation has long been known to be a risk factor. Back in the 1930s, after reviewing clinical records of 771 cases of esophageal cancer, New York physician W.L. Watson wrote that “thermal irritation is probably the most constant factor predisposing to the cancer of the esophagus.” This prevalence could explain why a large proportion of all cases of esophageal cancer affects populations in which drinking tea, coffee, or maté, or eating hot foods is common.
Decades later, this conclusion is supported by multiple studies. More recently, the World Health Organization, a 2018 Chinese study, and a 2019 Iranian study all hinted at the connection.
It should be noted that some studies used a temperature greater than which most people would normally drink liquids. Still, drink liquids at a reasonable temperature.
3. Avoid smoke and alcohol
Drinking alcohol and smoking are major risk factors for esophageal cancer, especially in Western populations, as established by many retrospective studies.
The observed association between smoking and adenocarcinoma risk is weaker than that for squamous cell carcinoma, while the effect of alcohol on adenocarcinoma is uncertain.
Notably, any level of alcohol consumption increases esophageal cancer risk. The more a person drinks, the higher their risk. Compared to no alcohol consumption, heavy drinking leads to a five-fold increased risk.
4. Beware of Barrett’s esophagus
One of my studies on esophageal cancer started with a patient with a family history of esophageal cancer. He originally had Barrett’s esophagus and later developed esophageal cancer.
Barrett’s esophagus—which usually results from acid reflux—is recognized as a risk factor for esophageal cancer. Acid reflux damages the esophagus, resulting in the lining thickening and turning red. Between 5 and 8 percent of persons with acid reflux develop cancer.
The sole indicator still effective for determining whether people are at an elevated risk of developing cancer is the presence of precancerous cells (dysplasia) in Barrett’s esophagus.
But don’t worry. The diagnosis of Barrett’s esophagus should not be a reason for alarm. If it coincides with high-grade dysplasia, your doctor might recommend a minimally invasive esophagectomy.
Furthermore, recent research (pdf) has shown that under the right conditions, Barrett’s esophagus can be made to regress after endoscopic ablative therapy.
5. Boost your immune system
Before I started my research in gastrointestinal cancer, I worked at a Chinese medicine hospital and heard a story from my supervisor about his friend, who happened to be my previous neighbor. He had developed esophageal cancer at a young age and was hopeless. He then took ginseng and had a fever for days. He lost consciousness and after he woke up, he was cancer free.
I am not encouraging readers to take ginseng to prevent esophageal cancer without consulting Chinese medicine doctors. Plus, different ginseng has different effects.
Takeaway
According to the study using electronic health records in Florida, esophageal cancer is on the rise among middle-aged Americans. Since this is a deadly cancer that is hard to diagnose early, be aware of any early signs, such as difficulty swallowing (dysphagia), weight loss without known reasons, chest pain, pressure or burning in your esophagus, and talk to your doctors as early as you can.
The most important thing you can do today is to have a healthy lifestyle and a positive outlook, get rid of bad habits, and manage stress to ensure you have a good immune system.











{kind=link}