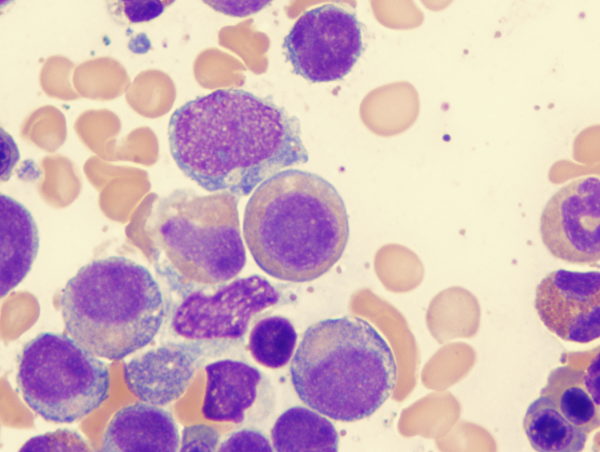
A 47-year-old man presented to the hospital with a 2-day history of weakness and fever. His blood pressure was 64/47 mm Hg, heart rate 110 beats per minute, and temperature 39.0°C. On physical examination, the patient had swelling and redness of the left thigh, which aroused concern about the presence of an abscess. Laboratory studies showed pancytopenia and extreme elevation of the d-dimer level. Promyelocytic blast cells with intracellular Auer rods — needle-shaped cytoplasmic structures specific for myeloid neoplasms — were seen on a peripheral-blood smear. Owing to concern about acute promyelocytic leukemia and sepsis, the patient was admitted to the intensive care unit. Induction chemotherapy with all-trans retinoic acid and prednisolone was initiated. A bone marrow biopsy showed promyelocytes with abundant intracellular Auer rods in formations that resembled bundles of sticks (arrows). Genetic analysis for chromosomal translocation identified a PML–RARA fusion gene. A diagnosis of acute promyelocytic leukemia was confirmed. Two days after the start of treatment, differentiation syndrome developed. The hospital course was further complicated by the presence of disseminated intravascular coagulation and Staphylococcus aureus bacteremia with leg abscesses. After molecular complete remission had been attained, consolidation chemotherapy that included arsenic trioxide was administered. On hospital day 72, the patient was discharged.
A new clinical trial showed that personalized treatment durations based on blood tests greatly enhance survival and remission in CLL, marking a major advancement in leukemia therapy.
Personalized therapy enhances survival rates for patients with CLL leukemia.
A phase III trial conducted by the University of Leeds discovered that personalized treatment for the most prevalent type of adult leukemia extends patient survival and maintains remission.
This significant research was recently published in the New England Journal of Medicine and highlighted at the 65th American Society of Hematology (ASH) Annual Meeting and Exposition in San Diego.
The data shows that the duration of therapy can be individualized for each patient by using regular blood tests to monitor their response. In the trial, this approach resulted in significant improvements in both progression-free and overall survival in patients with previously untreated chronic lymphocytic leukemia (CLL). The effect was stronger among patients with poorer outcomes to standard treatments, such as those with some genetic mutations.
Personalized Treatment Approach and Its Efficacy
Adult patients were given a combination of cancer growth-blocking drugs over varied durations depending on how rapidly their disease responded.
The trial found that this approach significantly improved progression-free and overall survival compared to the standard treatment for CLL, with more than 19 in 20 patients in remission three years after starting treatment.
The study, named FLAIR, is a phase III randomized controlled trial for untreated CLL, taking place in more than 100 hospitals across the UK. It was funded by Cancer Research UK, Janssen Research & Development, LLC, and AbbVie Pharmaceutical Research and Development.
Lead author Peter Hillmen, Professor of Experimental Haematology in the University of Leeds’ School of Medicine, and Honorary Consultant Haematologist at Leeds Teaching Hospitals NHS Trust, said: “Our findings show that, for this group of patients, the treatment is very effective at tackling their disease and is well tolerated by them. This means that patients on our trial had better outcomes while also enjoying a better quality of life during their treatment. Most patients treated with the new combination have no detectable leukemia in their blood or bone marrow by the end of treatment which is better than with previous treatments and is very encouraging.”
Research Findings and Future Implications
Dr Iain Foulkes, Executive Director of Research and Innovation at Cancer Research UK, said: “We are delighted to see these results from the FLAIR trial which show the importance and effectiveness of tailoring cancer treatment to the individual patient. Not only this, but the trial has found a way to do so without requiring frequent bone marrow tests which are more invasive and can be painful.
“The collaborative effort that went into this trial – involving researchers, healthcare professionals, funders and dedicated patients and their families – point to a new standard of care which could see real progress made against leukemia.”
Chronic lymphocytic leukemia is a type of cancer that affects the blood and bone marrow. It cannot usually be cured but can be managed with treatment. More than nine in 10 people are aged 55 and over when they are diagnosed.
Current treatments include chemotherapy, immunotherapy, or cancer growth blockers.
The FLAIR trial tested cancer growth blockers called Ibrutinib and Venetoclax (I+V). Also known by the brand names Imbruvica and Venclexta, these are usually administered either continuously or for the same fixed duration rather than tailored to each patient’s response. This means that many patients may stop treatment too early and don’t get the full potential benefit from their therapy or continue therapy for longer than necessary. This could lead to a greater chance of relapse of their leukemia and/or of treatment side effects.
FLAIR researchers aimed to discover whether it was possible to personalize I+V treatment duration for patients based on regular blood sampling and/or bone marrows, and whether this was as effective or better than standard treatment (FCR).
This regular blood and bone marrow monitoring gave researchers a more up-to-date picture of how patients were responding to I+V, and meant that the duration of I+V treatment could be tailored accordingly to each patient. In addition, it was found that basing the duration of treatment on less invasive, quicker blood samples was just as effective as using bone marrows, which can be painful and sometimes require sedation.
Trial Design and Results
FLAIR was launched in 2014, recruiting 1,509 patients with CLL. They were randomized to four treatment groups, each receiving a different treatment.
This part of the FLAIR trial compared two of the groups, placing 260 patients on I+V and 263 on the standard treatment, known as FCR. Almost three-quarters were male, which was to be expected as CLL occurs more frequently in males. The average age was 62, and just over a third had advanced disease.
At the end of this stage of the trial, 87 patients had seen their disease progress, 75 of which were on FCR, and 12 on I+V.
To date, 34 of these patients have died during the trial. Of these, 25 were treated with FCR and only nine with I+V.
The patients on I+V underwent blood tests and bone marrows to monitor their response to treatment. The technique used is known as measurable residual disease (MRD) which allows clinicians to see the number of remaining cancer cells. The number of cells may be so small that the patient is asymptomatic. An MRD positive test result means that there are remaining cancer cells.
The research team now hopes that this more personalized therapy approach, guided by blood test monitoring will be adopted as a new standard of care for patients needing first-line CLL treatment.
Professor Hillmen said: “The results of the FLAIR Trial, led by the Leeds Cancer Research UK Clinical Trials Unit at the University of Leeds, are exceptional and herald a change in the way chronic lymphocytic leukemia will be treated. FLAIR has been a huge collaborative effort over the last decade by the UK’s leading CLL specialists and by the hematology teams in over 100 hospitals throughout the UK. The participation of patient groups, individual patients, and their families was critical to delivering such progress, particularly through the challenges of the pandemic.”
The trial was co-ordinated by the Leeds Cancer Research UK Clinical Trials Unit at the University of Leeds. Deputy Director Professor David Cairns said: “The vision of the Leeds Cancer Research UK CTU is to improve the length and quality of survival for cancer patients on a worldwide scale. Our strategy to do this is to ensure that we build evidence to identify the correct treatment, for the correct duration, for the correct patient. FLAIR is a trial well aligned with our strategy, and reflects team science including clinicians, laboratory scientists, methodologies, and operational experts working together to deliver important trial results. None of this would be achieved without the selfless commitment of trial participants who contribute their time and data.”
Surprising treatment breakthroughs in recent years
There have been surprising breakthroughs in the treatment of leukemia in recent years. (Shutterstock)
Leukemia is a term that scares many people. It is commonly known as blood cancer and is a malignant disease involving the blood system. But is leukemia truly incurable and fatal? How has leukemia’s treatment method and its effectiveness progressed in recent years?
The Epoch Times interviewed Michael Andreeff, a professor of medicine in the Department of Leukemia, Division of Cancer Medicine at the University of Texas MD Anderson Cancer Center in Houston, Texas, regarding the above questions. This article is written and organized based on the content of the interview.
Classification and Diagnosis Methods of Leukemia
Leukemia can be divided into two groups, chronic and acute, and it can be further divided into lymphocytic leukemia and myelogenous leukemia according to its cell of origin.
Therefore, in general, there are four main types of leukemia: chronic lymphocytic leukemia (CLL), acute lymphocytic leukemia (ALL), chronic myelogenous leukemia (CML), and acute myelogenous leukemia (AML).
The causes and gene mutations of these four types of leukemia are all different—they are not related to one another and have great differences, and their treatment and prognosis are also completely different.
The symptoms of leukemia are not distinct. Patients may feel tired or bleed for no apparent reason. It may not be discovered until a doctor checks the blood counts and finds that they are not normal.
A blood count measures the number of three types of cells in the blood: red blood cells (which contain hemoglobin) that carry oxygen, white blood cells that protect against infection, and platelets that stop bleeding.
White blood cells and red blood cells in the blood. (Shutterstock)
Leukemia patients may have at least three or four abnormalities in their blood count.
For example, their hemoglobin levels may be low, which can cause the patients to feel tired because there is not enough oxygen in the blood.
Their white blood cell count may also be too low or too high. Low white blood cell counts indicate that patients do not have enough cells to fight infection and are prone to fevers, which require prompt treatment and can be fatal. On the other hand, an influx of abnormal leukemia cells produced by the bone marrow and released into the blood can cause a high white blood cell count.
The platelet count may also be low. Some patients have very low platelet levels, leading to spontaneous bleeding without trauma.
Blood count results alone are not enough to diagnose leukemia; a bone marrow test is also needed. Bone marrow tests can only determine the type of leukemia, but special tests (such as ones that look for mutated genes and abnormal chromosomes, immunophenotyping, etcetera) can also be performed. These special tests are conducted because there are many immunotherapies and gene-targeted therapies for leukemia.
Chemotherapy Can Cause Leukemia
Because we know so little about its causes, there is currently no feasible or complete way to prevent it, but we do know some of the risk factors that may lead to leukemia.
These days, most cancer patients are treated with chemotherapy. A study found that patients who received chemotherapy for other cancers had a higher chance of developing leukemia in the future, and this is related to Clonal Hematopoiesis of Indeterminate Significance, or CHIP cells.
As people age, a small number of cells in the blood begin to turn abnormal and develop genetic mutations, but these cells are not abnormal enough to cause leukemia or other cancers. These are called CHIP cells.
In such context, chemotherapy treatments for breast, ovarian, lung, and other cancers may transform CHIP cells into a preleukemic state, which may develop into leukemia in the future.
For instance, myelodysplastic syndrome (MDS) is a precursor to acute myelogenous leukemia (AML), and MDS is often seen in patients receiving chemotherapy for solid tumors.
Myelodysplastic syndromes are a group of disorders caused by abnormal production of blood cells in the bone marrow. (Shutterstock)
As it seems patients who received chemotherapy for other cancers also have an increased risk of developing leukemia in the future, the current research trend is to replace chemotherapy with other methods, such as immunotherapy.
Exposure to benzene has also been linked to acute myelogenous leukemia. Found in solvents used to wash and degrease machine parts, as well as in some glues used to treat such parts, benzene has been associated with a risk of leukemia.
Radiation can also cause leukemia. Eight years after the atomic bombing of Hiroshima, the number of confirmed cases of chronic myelogenous leukemia in the Hiroshima area reached its peak. It can be inferred that radiation-induced leukemia may take eight years or even longer to develop.
X-rays and radiation used for medical diagnosis can also be a problem. Hence, while CT scans are useful, they should only be done when necessary.
Additionally, certain lawn fertilizers have been linked to the development of chronic lymphocytic leukemia or lymphoma.
Most Cases of Chronic Myelogenous Leukemia Can Be Completely Cured
Among the four types of leukemia mentioned above, chronic myelogenous leukemia (CML) has made the most progress and has the best treatment effectiveness.
Chromosomal abnormalities have long been noted in the leukemia cells of most CML patients. Such abnormalities were first discovered in Philadelphia, Pennsylvania, hence the name the “Philadelphia chromosome.”
It was not until 1982 that the gene mutation caused by the Philadelphia chromosome was discovered, and the mutation was confirmed to be a single-gene mutation. The first-generation drug targeting the abnormal gene was introduced in 2001 after extensive scientific research and clinical trials, and it instantly changed the three-and-a-half-year average life expectancy of CML patients at the time.
Since then, the survival rate of CML patients has greatly increased, and today, the treatment success rate of the targeted therapy is almost 100 percent, which is simply a dream result.
Gene mutations caused by the Philadelphia chromosome also exist in the leukemia cells of some ALL patients. The treatment success rate of such patients after receiving the targeted therapy is also very high.
High Survival Rate for Chronic Lymphocytic Leukemia, Many Patients Remain Disease-Free in Remission
Another type of leukemia with a long survival period is chronic lymphocytic leukemia (CLL), which is mainly seen in the elderly, with the average age of patients being 70 years old. It is more common in Western countries and less common in Asian countries.
Symptoms of CLL include swollen lymph nodes in the neck, armpit, or groin, and an enlarged spleen. In addition, patients may have very high white blood cell counts. Doctors generally do not start treatment as long as the patient is in good condition.
However, the approach is changing, and more doctors are considering early intervention for CLL. This is because the longer the waiting period, the more chromosomal and other molecular abnormalities become present in the patient’s leukemia cells.
Currently, CLL can be treated with methods like chemotherapy and gene-targeted therapy. Chemotherapy has significantly improved the survival rate of patients, while gene-targeted therapy is effective for almost all CLL patients.
It takes a longer observation period to determine whether a patient is completely cured, as CLL is inherently a slow-evolving chronic disease.
Doctors tend to be conservative and will not claim that a patient is completely cured. However, CLL patients are expected to have a long life expectancy. Most CLL patients can stay in a leukemia-free remission state, and many of them will recover. Relapsed patients now have access to alternative medicines, which were not available 10 years ago.
The Deadliest Leukemia Can Be Treated With Arsenic, With a Cure Rate of 90 Percent
There is an extremely critical and dangerous subtype of acute myelogenous leukemia (AML) called acute promyelocytic leukemia (APL).
In addition to abnormal white blood cells in the body, APL patients also have coagulation disorders. If left untreated, the patient usually bleeds to death within a few weeks, or even overnight.
As a result, the early mortality rate of APL patients was up to 30 percent, and the overall survival rate was only 30 percent. This type of leukemia is also the most difficult to treat.
Worse, these patients do not experience early warning symptoms, and they often say, “I’ve never been sick.” However, the leukemia had been developing in their body for years; it simply did not cause symptoms until later on.
Surprisingly, the drugs developed (pdf) to save the lives of APL patients are a form of the vitamin, all-trans retinoic acid (ATRA), and the highly toxic substance arsenic trioxide (commonly known as arsenic).
After clinical verification, all-trans retinoic acid and arsenic have become the standard drugs for treating APL all over the world, and they have indeed achieved the effect of stopping bleeding and saving patients’ lives.
The cure rate of APL has reached 80 to 90 percent worldwide, and the effectiveness of the disease’s treatment can only be described as miraculous.
APL only accounts for 15 percent of the total number of AML patients, and great progress has been made in the treatment of the remaining AML patients.
Different AML patients have mainly relied on two kinds of drug treatment for more than 50 years, and the cure rate is only about 20 to 25 percent. However, 10 new drugs have been approved by the FDA in the past three years, and the response rate of elderly AML patients to treatment has reached nearly 90 percent. Many patients are expected to be cured, though the exact results are still being observed.
CAR-T Cell Therapy for Acute Lymphocytic Leukemia Is a Huge Progress
The treatment of acute lymphocytic leukemia (ALL) still requires many sessions of chemotherapy, but it can be tolerated by children’s bodies and the cure rate is close to 90 percent, which is amazing.
Treatment outcomes in adults with ALL are significantly worse than in children, but high remission rates can still be achieved. Patients in remission usually remain in good health, and there is no trace of leukemia on microscopic or molecular testing.
In addition to chemotherapy, immunotherapy is an essential treatment method for ALL. One of the commonly used immune drugs is a monoclonal antibody that can be mass-produced. The antibody recognizes and binds to protein antigens on the cell surface, ultimately destroying the leukemia cells. Immunotherapy has significantly reduced the relapse and mortality rate of ALL patients.
Natural killer cells kill cancer cells. (Shutterstock)
Another emerging cancer treatment involves collecting a patient’s normal white blood cells, genetically modifying them, and then returning them to the patient. These cells, called CAR-T cells, kill leukemia cells.
This treatment method for ALL has been approved by the FDA. It has been clinically proven that CAR-T cell therapy is effective in about half of ALL patients who do not respond to any other treatment, which is a huge improvement.
Except for Some Types, the Cure Rate of Leukemia Is Increasing Year by Year
Generally speaking, the cure rate of leukemia patients is increasing year by year, and a significant change in the survival curve can be seen every five years; some types of leukemia even reach a 90 percent cure rate. However, it is undeniable that the cure rate for some types of leukemia remains extremely low.
For example, a type of leukemia with a mutation in the P53 gene barely responds to any current treatments.
Even with drugs available, there is one big problem in leukemia treatment, and that is high drug prices. For example, a targeted drug for CML costs $100,000 per year in the United States.
It takes an average of 20 years and a huge amount of capital for a drug to go from development to animal testing, to three phases of clinical trials, and eventually to FDA approval. Most people cannot afford such expensive drugs. Some patients have no choice but to travel to other countries in search of cheap generic drugs.
However, it is possible to access free medicine in the United States.
During the clinical trial phase of a drug (which usually lasts several years), patients participating in the trial are given free medication, including other standard drugs used in combination.
Drug companies sometimes also provide free access to many drugs that have been approved by the FDA. While many patients can still obtain free drugs even if their insurance company does not cover their costs, this requires the cooperation of a professional team to fight for the patients’ access.
Is It Worth Participating in a Clinical Trial for the Treatment of Leukemia?
Many people think that participating in clinical trials and using new drugs that have not been approved by the FDA is tantamount to treating themselves as guinea pigs, but this is not the case.
“Patients will not die from the use of new drugs, only from cancer,” Andreeff said.
A lot of preliminary work is required before any new drug can enter large-scale clinical trials. A team of experts consisting of chemists, pharmaceutical chemists, and doctors works in the laboratory for years prior to a drug receiving approval. Every new clinical trial needs to be approved by the FDA before it can start, and there are many safeguards under the supervision of the FDA.
Furthermore, doctors recommend experimental new drugs only when they think patients will benefit from them.
Even if patients do not experience substantial therapeutic responses after participating in clinical trials, or the experimental new drug is not approved by the FDA in the end, participating in such clinical trials may prolong patients’ lives.
Statistics have shown that patients participating in clinical trials live longer than those receiving standard treatment elsewhere.
In specialized cancer centers with abundant information and resources, some cancer specialists have access to information about new drugs, and they already know the effectiveness of those drugs long before the FDA approves them. Even after new drugs are approved by the FDA, it may take a while before oncologists can start using them.
As a doctor who works at a large specialized cancer center, Andreeff believes that it is best for patients to start treatment at one of these cancer centers, or at least consult the specialists there for a second opinion, so as not to miss out on treatment options that may be right for them.
MD Anderson researchers presenting key advances in multiple leukemias at ASH 2022
MD Anderson News Release December 12, 2022
Researchers from The University of Texas MD Anderson Cancer Center are presenting compelling findings from three clinical trials at the 2022 American Society of Hematology (ASH) Annual Meeting. These oral presentations highlight encouraging results to advance the use of targeted therapies and novel combinations in multiple types of leukemia, including high-risk and newly diagnosed acute myeloid leukemia (AML) in older and younger patients and Philadelphia chromosome-positive acute lymphoblastic leukemia (ALL). More information on all ASH Annual Meeting content from MD Anderson can be found at MDAnderson.org/ASH.
Older or high-risk patients with newly diagnosed AML respond well to triplet therapy (Abstract 61) Researchers observed encouraging response rates in older or high-risk patients with newly diagnosed acute myeloid leukemia (AML) who were treated with the triplet combination therapy of azacitidine, venetoclax and magrolimab on a Phase Ib/II trial. The newly diagnosed cohort had an 80% overall response rate (ORR), and the median overall survival (OS) was not yet reached at a median follow-up of 9.2 months. Naval Daver, M.D., associate professor of Leukemia, presented study results Dec. 10.
“We are encouraged by the promising evidence of this triplet therapy as a treatment option for older or unfit patients with AML,” Daver said. “We will continue to expand the trial to include more patients, and we have initiated an international Phase III randomized study evaluating the triplet therapy versus the doublet azacitidine-venetoclax. If the study is positive, it could establish a new frontline standard of care for these patients.”
About 50-55% of patients with AML are considered older or unfit for intensive chemotherapy. Frontline treatment with azacitidine and venetoclax achieves response rates of 65-70% in newly diagnosed patients, but most patients will relapse and those with TP53 mutations continue to have poor outcomes, with median OS of less than six months. Magrolimab is an anti-CD47 antibody that works to block the “don’t eat me signal” on leukemia cells. In a previous trial, it demonstrated efficacy with azacitidine in newly diagnosed AML, with an especially encouraging signal of response and survival in frontline TP53-mutated AML.
The current trial enrolled 74 patients across two cohorts. The first cohort enrolled 45 frontline patients aged 75 or older with documented comorbidities that made them ineligible for intensive therapy or with adverse risk factors and/or a TP53 mutation, regardless of age. This cohort included 27 patients with a TP53 mutation and 14 without. The second cohort enrolled 29 patients with relapsed/refractory (R/R) disease.
All patients who received at least one dose of any of the three study drugs were included for response and adverse events. Eighteen patients experienced greater than grade 3 anemia, and the most common non-hematologic side effects were febrile neutropenia, pneumonia, hyperbilirubinemia, transaminitis, creatine elevation and hypokalemia.
In the newly diagnosed cohort, the ORR in patients with and without TP53 mutations was 74% and 93%, respectively. Median OS was not yet reached for either group of patients. Responses in patients with R/R disease with prior venetoclax treatment were modest, and the cohort was closed for futility. Patients with R/R disease without venetoclax exposure still are being enrolled.
The study was funded by Gilead. Daver has served in an advisory role for Gilead. A complete list of collaborating authors can be found within the abstract here.
Chemotherapy-free regimen ponatinib plus blinatumomab effective in patients with newly diagnosed Ph+ ALL (Abstract 213) The chemotherapy-free regimen of ponatinib and blinatumomab achieved high response rates and reduced the need for an allogeneic stem cell transplant for patients with recently diagnosed Philadelphia chromosome-positive (Ph+) acute lymphoblastic leukemia (ALL), according to results from a Phase II trial. One of the lead investigators, Nicholas Short, M.D., assistant professor of Leukemia, presented the findings Dec. 10.
“Traditionally, Ph+ ALL responds poorly to standard chemotherapy and is high-risk for relapse, so these survival results and reduced need for a stem cell transplant are very encouraging,” Short said. “Not only does this regimen appear to be a safe and effective chemotherapy-free option, but it also seems to overcome the historical need for transplant in these patients.”
Patients with Ph+ ALL have historically had poor long-term survival rates. Researchers have found adding tyrosine kinase inhibitors (TKIs), such as ponatinib, to chemotherapy can drastically improve survival. Ponatinib is a third-generation TKI that targets BCR-ABL1 and is traditionally used to treat certain types of chronic myeloid leukemia. Blinatumomab is a CD3-CD19 bispecific antibody that is effective as a single agent in relapsed or refractory Ph+ ALL.
The trial enrolled 40 patients with newly diagnosed Ph+ ALL. Patients with uncontrolled cardiovascular disease or clinically significant central nervous system comorbidities were excluded from the study. The average age of participants was 56 years old.
Of the patients that were evaluable for a hematologic response, 96% had a complete remission or complete remission with incomplete count recovery. Among the 38 patients who were evaluable for complete molecular response (CMR), 68% achieved CMR after one treatment cycle and 87% achieved CMR during the trial period. Molecular responses were rapid, with a majority of patients achieving CMR in the peripheral blood within two weeks of therapy. Only one patient underwent stem cell transplant in first remission.
At a median follow-up of 15 months, event-free and estimated overall survival was 95%. These encouraging outcomes were observed despite the very low rate of transplant in the study. The treatment was well tolerated, and most toxicities were grade 1-2 and consistent with known side effects of the two agents.
The study was funded by Amgen and Takeda Oncology. Short has served in a consulting or advisory role for Takeda Oncology. A complete list of collaborating authors can be found within the abstract here.
Venetoclax with CLIA highly effective in younger patients with newly diagnosed AML, high-risk MDS (Abstract709) The latest results of a Phase II study evaluating the addition of venetoclax to the intensive chemotherapy treatment of cladribine, idarubicin and cytarabine (CLIA) as a frontline therapy demonstrated high rates of disease control and remissions in younger patients with newly diagnosed AML and high-risk myelodysplastic syndrome (MDS). In the study, 96% of patients responded to treatment and 90% had no measurable disease detected in a bone marrow sample. Patrick Reville, M.D., instructor of Leukemia, presented updated results and longer-term follow-up data Dec. 12.
“Venetoclax has been a breakthrough for AML patients that are ineligible for intensive therapy. This data continues to demonstrate the benefit of including venetoclax with the CLIA induction regimen,” Reville said. “This regimen is leading to unprecedented response and measurable residual disease-negativity rates. As we continue to follow participants, we are encouraged by their long-term outcomes and survival.”
The single-center, single-arm trial enrolled 67 patients with a median age of 48. Sixty patients had AML and four patients had high-risk MDS. In addition, three patients had a mixed-phenotype acute leukemia (MPAL).
The composite complete response rate was 96% across all patients and 100% for patients with both MDS and MPAL with a myeloid predominant clone. Most patients went on to receive a subsequent allogeneic stem cell transplant (alloSCT), including 70% of those who responded to treatment.
Encouragingly, with a median follow-up of just over two years, the median duration of response, event-free survival and overall survival have not yet been reached. At 12 months, the estimated event-free survival rate is 70% and the estimated overall survival rate is 86%. Seventy-four percent of responding patients are estimated to have an ongoing response at 12 months.
The most common non-hematologic adverse event that participants experienced was febrile neutropenia, which was managed. Researchers continue to follow patients and study this treatment regimen as a safe and effective induction treatment strategy for this patient population.
Young adults who received radioactive iodine therapy for differentiated thyroid cancer were at 92% increased risk for leukemia and 23% increased risk for any solid malignancies vs. those who did not receive radioactive iodine therapy.
Among solid cancers, researchers observed elevated risk for uterine, breast, lung and salivary gland cancers; solid malignancy risks increased with greater time since thyroid cancer diagnosis.
Young adults receiving radioactive iodine therapy for differentiated thyroid cancer had a higher risk for any solid cancer, breast cancer or uterine cancer compared with those who did not have radioactive iodine therapy. Data were derived from Pasqual E, et al. OR-14. Presented at: American Thyroid Association Annual Meeting; Sept. 30-Oct. 3, 2021 (virtual meeting).
“Our results reinforce the notion that treatment decisions regarding the use of radioactive iodine therapy should consider the balance of risks and benefits for individual patients with differentiated thyroid cancer,” Cari Kitahara, PhD, a senior investigator in the division of cancer epidemiology and genetics, radiation epidemiology branch, of the NIH’s National Cancer Institute, told Healio. “This is especially important for younger patients who are much more vulnerable to the carcinogenic effects of ionizing radiation compared with older adults, and patients diagnosed with differentiated thyroid cancers with low risk of recurrence.”
Elisa Pasqual
Incidence of differentiated thyroid cancer (DTC) has increased in the U.S. since the 1970s, becoming the second most common cancer in adolescents and young adults, Elisa Pasqual, MD, PhD, a postdoctoral fellow in the division of cancer epidemiology and genetics at the NCI, said during a presentation at the American Thyroid Association annual meeting. In parallel, the use of radioactive iodine (RAI) treatment also increased, including for young patients.
Researchers analyzed data from nine U.S. Surveillance, Epidemiology and End Results cancer registries (1975-2017) to estimate RRs for solid and hematopoietic malignancies associated with RAI therapy (yes vs. no/unknown) among patients diagnosed with nonmetastatic DTC before age 45 years, using Poisson regression analyses among 27,050 5-year survivors and 32,171 2-year survivors, respectively.
Cari Kitahara
During a maximum follow-up of 43 years, RAI therapy was associated with an increased risk for solid cancers (RR= 1.23; 95% CI 1.11-1.37), particularly more than 20 years after DTC diagnosis (RR = 1.47; 95% CI 1.24-1.74). Researchers observed a similar pattern for breast cancer, the most common second cancer, with an overall RR of 1.18 (95% CI, 0.99-1.4) and an RR of 1.46 more than 20 years after RAI therapy (95% CI, 1.1-1.95). Risk was also elevated for uterine cancer (RR = 1.55; 95% CI, 1.03-2.32) and leukemia (RR = 1.92; 95% CI, 1.04-3.56). The researchers also observed nonsignificant increased risks for cancers of the salivary gland and lung.
Researchers estimated that 6% of solid and 14% of hematologic malignancies that occurred among pediatric and young adult DTC survivors during 1975-2017 at least 1 year after RAI therapy may be attributable to RAI.
“Previous studies have consistently linked radioactive iodine therapy for thyroid cancer with an increased risk of leukemia about 2 years after exposure,” Pasqual told Healio. “Quantifying the risks of solid cancers after radioactive iodine therapy has been more challenging, and results have been inconsistent. We know from the radiation epidemiology and radiobiology literature that the effects of radiation on solid cancer development are not observable for at least 5 to 10 years. Also, surprisingly, there has been limited focus on second cancer risks in young thyroid cancer patients, even though younger individuals are more susceptible to the late effects of radiation and have a longer average life expectancy over which these effects might develop.”
Kitahara said the focus on young patients with thyroid cancer and long-term follow-up were important features of the study that allowed researchers to quantify the risks of RAI-associated second cancers more precisely compared with previous studies.
“Future research should determine whether the risks of second cancers after radioactive iodine therapy are dose-dependent,” Kitahara told Healio. “If radioactive iodine therapy for thyroid cancer indeed causes an increased risk of second primary malignancies, then we should expect higher doses to yield higher risks. This research also would help to determine whether lower doses of radioactive iodine could be considered for patients who would otherwise benefit from this treatment.”
Researchers at Salk University have completed a study that’s revealed how the nucleus acts on its contents in order to influence gene expression. They discovered that nuclear core components regulate the expression of cell identity genes through the interaction with super-enhancers. Salk Professor, Martin Hetzer, comments “Our research shows that, far from being a passive enclosure as many biologists have thought, the nuclear membrane is an active regulatory structure.”
The team discovered two particular proteins are actively associated with the parts of DNA known to trigger the expression of genes. By better understanding the way in which these proteins function, scientists gain a better insight into diseases that are linked to dysfunctional nuclear membrane components including heart disease, leukemia and some aging disorders such as progeria. The first author of the paper and a Salk staff scientist, Arkaitz Ibarra said, “Discovering that key regulatory regions of the genome are positioned at nuclear pores was very unexpected.”
Salk scientists discover that nuclear pore components regulate the expression of cell identity genes through functional interactions with super-enhancers. In the image, a super-enhancer driven cell identity gene (red dot) localizes in close proximity to the nuclear envelope (green) in the nucleus of human primary lung fibroblasts (blue).
Next, the team studied a human bone cancer cell line to see which areas of DNA interacted with nucleoporins. They pinpointed where two nucleoporins (Nup153 and Nup93) came in contact with the genome and looked into which genes were being affected and how. It was found that Nup153 and Nup93 both interacted with super-enhancers that are vital in determining cell identity and driving gene expression. Hetzer says, “People have thought the nuclear membrane is just a protective barrier, which is maybe the reason why it evolved in the first place. And it’s such an important area because so far, every membrane protein that has been studied and found to be mutated or mislocalized seems to cause a human disease.”
Dr. Paul Spagnuolo is a researcher and assistant professor in Ontario, Canada at the University of Waterloo’s School of Pharmacy. Today, we think of pharmacy schools as being mostly funded by large prescription drug pushing pharmaceutical companies, but Dr. Spagnuolo’s methodology is quite different. His undergraduate and master degrees were focused on the biological compounds and healing potential located inside real, clean foods, not biologically engineered chemical combinations. More specifically, as reported by Uwaterloo.ca, Dr. Spagnuolo and his team generate detailed research in order to discover the “potential anti-cancer treatment applications of nutraceuticals i.e., food-derived bioactive compounds.”
Researcher Spagnuolo takes the phrase, “Let food be your medicine,” very seriously.
As Natural News reports, Spagnuolo caused quite a stir when he discovered a link between a particular “lipid found naturally in avocados” and the ability of this specific lipid to target and combat potent leukemia stem cells. It is these stem calls that “drive” a blood disease called acute myeloid leukemia (AML.) Working with this avocado lipid on a molecular level, Spagnuolo created a compound he called Avocatin B. As reported by the University of Waterloo, his research confirmed that this powerful avocado derivative doesn’t damage any healthy cells, but instead goes after the “root of the disease – leukemia stem cells.” His extensive work to discover and isolate Avocatin B was also recognized by the American Society of Nutrition who honored Dr. Spagnuolo’s achievement by giving him their Mead Johnson award.
Chemotherapy, radiation, bone marrow transplant or avocados?
In the United States, according to Cancer.net, just under 20,000 people , at any age, will be diagnosed with acute myeloid leukemia (AML) this year. As one might expect, Cancer.org reports that typical treatment for AML is two different phases of chemotherapy. It may take a number of years for Spagnuolo’s new discovery to be made available as an actual treatment option for AML, but work and experimentation is continuing so that clinical trials can be instituted. When these clinical trials do get started, patients diagnosed with AML will have the opportunity to experiment with this non- toxic alternative.
Avocados also have many other important nutrition benefits.
Healthynews24.com reports that the benefits from eating avocados are vast. A medium size fruit can provide at least half the fiber you need daily. Avocados will provide potassium, help regulate your blood sugar and provide Vitamin B. There are two specific nutrients found in avocados – lutein and zeaxanthin that may help protect your eyesight. Avocados are known to be anti-inflammatory, provide Vitamin E and K and even have an antioxidant called glutathione which has been associated with keeping one younger looking. The fats found in avocado can also be beneficial for skin and the complexion. That full feeling you get from eating avocados might assist in weight loss efforts. Add the newly discovered anti-cancer properties of this delicious green fleshy fruit, and you have a bevy of healthy reasons to add avocados as a staple on your family’s grocery list.
As few as one diet soda daily may increase the risk for leukemia in men and women, and for multiple myeloma and non-Hodgkin lymphoma in men, according to new results from the longest-ever running study on aspartame as a carcinogen in humans. Importantly, this is the most comprehensive, long-term study ever completed on this topic, so it holds more weight than other past studies which appeared to show no risk. And disturbingly, it may also open the door for further similar findings on other cancers in future studies.
The most thorough study yet on aspartame – Over two million person-years
For this study, researchers prospectively analyzed data from the Nurses’ Health Study and the Health Professionals Follow-Up Study for a 22-year period. A total of 77,218 women and 47,810 men were included in the analysis, for a total of 2,278,396 person-years of data. Apart from sheer size, what makes this study superior to other past studies is the thoroughness with which aspartame intake was assessed. Every two years, participants were given a detailed dietary questionnaire, and their diets were reassessed every four years. Previous studies which found no link to cancer only ever assessed participants’ aspartame intake at one point in time, which could be a major weakness affecting their accuracy.
One diet soda a day increases leukemia, multiple myeloma and non-Hodgkin lymphomas
The combined results of this new study showed that just one 12-fl oz. can (355 ml) of diet soda daily leads to:
– 42 percent higher leukemia risk in men and women (pooled analysis) – 102 percent higher multiple myeloma risk (in men only) – 31 percent higher non-Hodgkin lymphoma risk (in men only)
These results were based on multi-variable relative risk models, all in comparison to participants who drank no diet soda. It is unknown why only men drinking higher amounts of diet soda showed increased risk for multiple myeloma and non-Hodgkin lymphoma. Note that diet soda is the largest dietary source of aspartame (by far) in the U.S. Every year, Americans consume about 5,250 tons of aspartame in total, of which about 86 percent (4,500 tons) is found in diet sodas.
Confirmation of previous high quality research on animals
This new study shows the importance of the quality of research. Most of the past studies showing no link between aspartame and cancer have been criticized for being too short in duration and too inaccurate in assessing long-term aspartame intake. This new study solves both of those issues. The fact that it also shows a positive link to cancer should come as no surprise, because a previous best-in-class research study done on animals (900 rats over their entire natural lifetimes) showed strikingly similar results back in 2006: aspartame significantly increased the risk for lymphomas and leukemia in both males and females. More worrying is the follow on mega-study, which started aspartame exposure of the rats at the fetal stage. Increased lymphoma and leukemia risks were confirmed, and this time the female rats also showed significantly increased breast (mammary) cancer rates. This raises a critical question: will future, high-quality studies uncover links to the other cancers in which aspartame has been implicated (brain, breast, prostate, etc.)?
There is now more reason than ever to completely avoid aspartame in our daily diet. For those who are tempted to go back to sugary sodas as a “healthy” alternative, this study had a surprise finding: men consuming one or more sugar-sweetened sodas daily saw a 66 percent increase in non-Hodgkin lymphoma (even worse than for diet soda). Perhaps the healthiest soda is no soda at all.
As few as one diet soda daily may increase the risk for leukemia in men and women, and for multiple myeloma and non-Hodgkin lymphoma in men, according to new results from the longest-ever running study on aspartame as a carcinogen in humans. Importantly, this is the most comprehensive, long-term study ever completed on this topic, so it holds more weight than other past studies which appeared to show no risk. And disturbingly, it may also open the door for further similar findings on other cancers in future studies.
The most thorough study yet on aspartame – Over two million person-years
For this study, researchers prospectively analyzed data from the Nurses’ Health Study and the Health Professionals Follow-Up Study for a 22-year period. A total of 77,218 women and 47,810 men were included in the analysis, for a total of 2,278,396 person-years of data. Apart from sheer size, what makes this study superior to other past studies is the thoroughness with which aspartame intake was assessed. Every two years, participants were given a detailed dietary questionnaire, and their diets were reassessed every four years. Previous studies which found no link to cancer only ever assessed participants’ aspartame intake at one point in time, which could be a major weakness affecting their accuracy.
One diet soda a day increases leukemia, multiple myeloma and non-Hodgkin lymphomas
The combined results of this new study showed that just one 12-fl oz. can (355 ml) of diet soda daily leads to:
– 42 percent higher leukemia risk in men and women (pooled analysis) – 102 percent higher multiple myeloma risk (in men only) – 31 percent higher non-Hodgkin lymphoma risk (in men only)
These results were based on multi-variable relative risk models, all in comparison to participants who drank no diet soda. It is unknown why only men drinking higher amounts of diet soda showed increased risk for multiple myeloma and non-Hodgkin lymphoma. Note that diet soda is the largest dietary source of aspartame (by far) in the U.S. Every year, Americans consume about 5,250 tons of aspartame in total, of which about 86 percent (4,500 tons) is found in diet sodas.
Confirmation of previous high quality research on animals
This new study shows the importance of the quality of research. Most of the past studies showing no link between aspartame and cancer have been criticized for being too short in duration and too inaccurate in assessing long-term aspartame intake. This new study solves both of those issues. The fact that it also shows a positive link to cancer should come as no surprise, because a previous best-in-class research study done on animals (900 rats over their entire natural lifetimes) showed strikingly similar results back in 2006: aspartame significantly increased the risk for lymphomas and leukemia in both males and females. More worrying is the follow on mega-study, which started aspartame exposure of the rats at the fetal stage. Increased lymphoma and leukemia risks were confirmed, and this time the female rats also showed significantly increased breast (mammary) cancer rates. This raises a critical question: will future, high-quality studies uncover links to the other cancers in which aspartame has been implicated (brain, breast, prostate, etc.)?
There is now more reason than ever to completely avoid aspartame in our daily diet. For those who are tempted to go back to sugary sodas as a “healthy” alternative, this study had a surprise finding: men consuming one or more sugar-sweetened sodas daily saw a 66 percent increase in non-Hodgkin lymphoma (even worse than for diet soda). Perhaps the healthiest soda is no soda at all.
People residing at higher latitudes, with lower sunlight or ultraviolet B (UVB) exposure and greater prevalence of vitamin D deficiency, are at least two times at greater risk of developing leukemia than equatorial populations.
People residing at higher latitudes, with lower sunlight or ultraviolet B (UVB) exposure and greater prevalence of vitamin D deficiency, are at least two times at greater risk of developing leukemia than equatorial populations.
These results suggest that much of the burden of leukemia worldwide is due to the epidemic of vitamin D deficiency we are experiencing in winter in populations distant from the equator.
According to the American Cancer Society, 54,270 cases and 24,450 deaths from leukemia occur in the United States alone each year. There is no known way to prevent most types of leukemia, though some types may be prevented by avoiding high doses of ionizing radiation, exposure to the chemical benzene, smoking and certain types of chemotherapy.
Leukemia rates were highest in countries relatively closer to the poles, such as Australia, New Zealand, Chile, Ireland, Canada and the United States. They were lowest in countries closer to the equator, such as Bolivia, Samoa, Madagascar and Nigeria.













{kind=link}