Research led by the Centre for Targeted Protein Degradation (CeTPD) in the University of Dundee identified a breakthrough class of molecular glue that could pave the way for a new generation of drugs to target cancers and neurodegenerative diseases. The researchers collaborated with the research group of Georg Winter, PhD, at the Research Center for Molecular Medicine (CEMM) of the Austrian Academy of Sciences in Vienna, and have defined a new class of so-called “intramolecular bivalent glue,” which binds proteins that would otherwise stay apart.
“Targeted protein degradation is a pharmacological modality that is based on the induced proximity of an E3 ubiquitin ligase and a target protein to promote target ubiquitination and proteasomal degradation,” wrote the researchers. “This has been achieved either via proteolysis-targeting chimeras (PROTACs)—bifunctional compounds composed of two separate moieties that individually bind the target and E3 ligase, or via molecular glues that monovalently bind either the ligase or the target. Here, using orthogonal genetic screening, biophysical characterization, and structural reconstitution, we investigate the mechanism of action of bifunctional degraders of BRD2 and BRD4, termed intramolecular bivalent glues (IBGs), and find that instead of connecting target and ligase in trans as PROTACs do, they simultaneously engage and connect two adjacent domains of the target protein in cis.”
“These findings have major implications for the entire pharmaceutical industry engaged in targeted protein degraders,” said Alessio Ciulli, PhD, director of Dundee’s CeTPD.
“This is particularly true for the development of drugs that target cancer, neurodegenerative diseases, and many more illnesses driven by proteins that have always been considered undruggable.
“The glue that we have been able to define is special because it first attaches itself to one protein in two places—not just one—and then recruits the second protein, effectively sandwiching the two proteins together. We have only been able to identify this using our Targeted Protein Degradation technology and have identified a vulnerability that can be exploited by the design of new drugs that could potentially transform treatment for cancer patients, and those with other untreatable diseases.”
Targeted protein degradation (TPD) is an emerging field of drug development for treating diseases that involves redirecting protein recycling systems in our cells to destroy disease-causing proteins.
Working with collaborators at CEMM, the Goethe University of Frankfurt, and Eisai, the Japanese pharmaceutical company, the Dundee team has been able to reveal a novel mechanism of molecular gluing, different from those previously known.
The new mechanism binds to two sides of the target protein instead of just one, prompting a rearrangement of the whole protein and stabilizing its previously unknown interaction with the E3 ligase. The team was able to visualize, for the first time, the precise mechanism by which their compounds work and bring together the target proteins to one of these E3 ligases. Because the molecules have two heads, which latch on to two different regions within the same target protein, these have been coined intramolecular bivalent glues.
“The impact of what we have revealed here cannot be underestimated,” added Ciulli.
“This will cause a ripple effect throughout the pharmaceutical industry and has the potential to transform how we view drug development.”
In June, approximately 100 researchers attended a workshop on the campus of the National Institutes of Health (NIH) in Bethesda, MD, about an important but underappreciated side effect of some treatments for cancer: heart problems.
Certain cancer treatments can damage the heart and the cardiovascular system. These side effects, including high blood pressure, abnormal heart rhythms, and heart failure, can be caused or exacerbated by chemotherapy and radiation therapy, as well as by newer forms of cancer treatment, such as targeted therapies and immunotherapies.
“Cancer therapies affect a number of organs and organ systems, including the heart,” said Saro Armenian, D.O., M.P.H., at the meeting. Dr. Armenian, who treats children with cancer at City of Hope Comprehensive Cancer Center, noted that when a patient develops cardiac side effects during treatment, a doctor may modify the dose of a therapy or stop the therapy altogether.
Some cardiac side effects, however, go undetected for years or even decades after a patient’s treatment has ended. “Patients diagnosed with cancer are living longer today than in the past, and many of these survivors are living long enough to develop late cardiovascular effects,” said Lori Minasian, M.D., deputy director of NCI’s Division of Cancer Prevention, in an interview.
In recent years, Dr. Minasian continued, researchers have begun systematically to document the longer-term cardiovascular side effects of cancer treatments, also known as cardiotoxicities.
At the workshop on improving outcomes in treatment-related cardiotoxicity, participants from government, academia, and the private sector identified gaps in current knowledge and discussed priorities for future research. NCI and the National Heart, Lung, and Blood Institute (NHLBI) cosponsored the meeting.
Investigating a Range of Treatment-Related Cardiac Side Effects
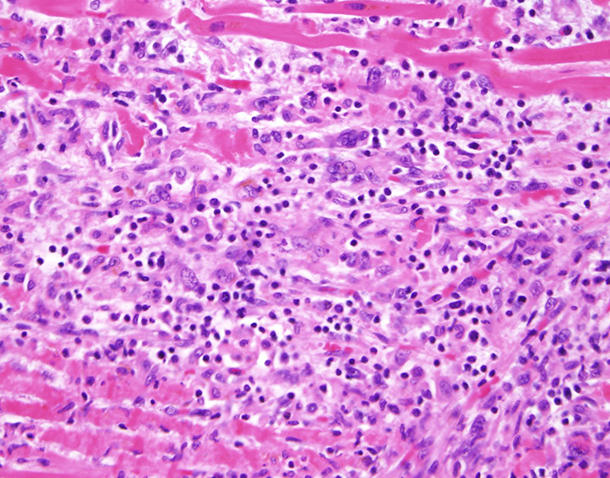
Heart tissue from a patient treated with an immune checkpoint inhibitor showing T cells (blue dots) invading muscle fibers in the heart.Credit: Dr. Javid Moslehi, Vanderbilt University
The workshop highlighted a challenge for the field, which is known as cardio-oncology: identifying and investigating cardiac side effects that are associated with a rapidly changing landscape of cancer treatments and combinations of therapies.
For example, as more and more immunotherapies have entered the clinic in recent years, researchers have begun to detect specific cardiac side effects that can occur during treatment with some of these agents.
“In a small but significant number of patients, there is a fatal outcome from immune checkpoint inhibitors that is directly related to the heart,” said Javid Moslehi, M.D., who directs the Cardio-Oncology Program at Vanderbilt-Ingram Cancer Center and led the study. (Other studies have estimated that the incidence of myocarditis in patients receiving checkpoint inhibitors is around 1%.)
While research on myocarditis from checkpoint inhibitors has “created a buzz,” many other cancer therapies can cause cardiovascular adverse events, he noted.
“We’re not paying enough attention to the other forms of cardiovascular toxicities from cancer drugs beyond doxorubicin,” Dr. Moslehi continued, referring to the commonly used chemotherapy drug that has been the focus of much cardiotoxicity research over the past decade. “We need to have a broader perspective.”
Susan Dent, M.D., who codirects Cardio-Oncology at Duke University, agreed. Doctors and patients, she noted, need information about the potential cardiac side effects of cancer drugs when these agents enter the clinic.
“We don’t want to wait until a decade has passed and then design a study to learn about the cardiotoxicities associated with a cancer drug,” she said.
Sharing Stories of Patients Who Died Prematurely
To illustrate the serious nature of cardiotoxicities and to put a human face on the issue, several speakers at the workshop shared the stories of individuals who died prematurely of heart problems related to cancer therapies, including Ellen Stovall.
A prominent advocate for cancer survivors who served on an NCI advisory board, Stovall had been treated for three different cancers over many years. Some of the therapies led to chronic health problems, and about 2 years ago, at the age of 69, Stovall died suddenly. The cause of her death was complications of cardiovascular disease related to her cancer treatments.
Another example discussed at the meeting was a woman who developed heart disease related to treatments for multiple cancers that led to emergency triple-bypass surgery. She died at age 47.
“We cannot cure patients of one cancer, only to have them develop a second cancer and treatment-related cardiac problems that result in a triple bypass” before age 50, Dr. Dent commented.
Studies Needed to Inform Clinical Decisions
More research is also needed to help inform clinical decisions about cancer treatments and cardiac side effects. “Oncologists and cardiologists want to be able to implement evidence-based guidelines for patient care, but more studies are needed,” said Dr. Minasian.
Chau Dang, M.D., a medical oncologist at Memorial Sloan Kettering Cancer Center, summarized the critical questions as “who, when, and how.” That is, who should be monitored for cardiovascular problems, when should they be monitored, and how should they be monitored?
The workshop included discussions of biomarkers of cardiac or cardiovascular damage, such as troponin, which is a complex of proteins that is released when heart muscle is damaged. These biomarkers were developed for patients with heart disease rather than for patients with cancer who may experience treatment-induced cardiac side effects.
As a result, it’s not clear whether biomarkers of cardiovascular damage could be used to assess the risk of cardiac side effects or to monitor cardiovascular health in patients being treated for cancer or in long-term survivors. “We don’t know if the patterns of injury from anti-cancer drugs are the same as the patterns of injury of de novo heart disease,” said Dr. Minasian.
Nonetheless, several speakers emphasized the need to establish the usefulness of biomarkers for assessing whether patients are experiencing cardiovascular damage from cancer therapies and how such biomarkers should be used, particularly given the existence of other tests, such as imaging tests.
“Right now, it’s not clear which combinations of biomarker and imaging tests should be used for which patients and when,” said Dr. Dent.
Understanding How Cancer Therapies Harm the Cardiovascular System
AartiAsnani, M.D., a cardiologist in the Cardio-Oncology Program at Beth Israel Deaconess Medical Center, said in an interview, “What we have now are broad and relatively nonspecific biomarkers of cardiac injury.”
She noted that developing new biomarkers will require “a deeper understanding of the mechanisms of cardiotoxicity as well as larger randomized clinical trials for validation.”
At the workshop, several participants also stressed the importance of learning more about how cancer treatments may harm the cardiovascular system. This information could be used to develop much-needed research tools, such as better ways to predict which patients are at risk of developing cardiac side effects as well as strategies for reducing this risk, Dr. Dent noted.
“Each cancer drug causes different cardiovascular issues through different mechanisms,” said Dr. Moslehi. “To move forward, we need to know the nature of the cardiovascular toxicity.”
Large clinical trials that follow patients over time would allow researchers to gain insights into how and when longer-term cardiac side effects develop, Dr. Armenian noted.
One Example: Cardiac Side Effects and Breast Cancer
Over the past decade, breast cancer has been a focus of research on cardiac side effects, in part because certain treatments for the disease are known to cause these side effects.
Based on this evidence, the American Heart Association recently issued a rare scientific statement on cardiovascular disease and breast cancerExit Disclaimer. For some breast cancer survivors—older individuals in particular—the risk of dying from cardiovascular disease may exceed the risk of dying from cancer, the authors of the statement noted.
Dawn L. Hershman, M.D., who studies breast cancer at the Herbert Irving Comprehensive Cancer Center at Columbia University Medical Center, agreed. “The reality is we’ve made a huge amount of progress in treating breast cancer, and today women diagnosed with early-stage breast cancer are more likely to die of cardiac disease than of cancer,” she said in an interview.
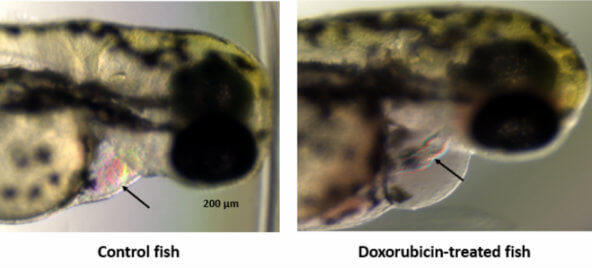
Researchers are using zebrafish to study how the cancer drug doxorubicin affects the heart. Normal fish (left) and a fish that developed cardiomyopathy after treatment with doxorubicin (right).Credit: Dr. Aarti Asnani, Beth Israel Deaconess Medical Center
“A big part of the problem is that cardiac and vascular risk factors are not always well managed in patients with cancer,” she explained. “When a woman is diagnosed with breast cancer, her adherence to treatments for other health conditions often goes down, such as the management of cholesterol or keeping diabetes under control.”
The dual risks of cancer and heart disease in cancer survivors have created a challenge for both oncologists and cardiologists, noted Dr. Minasian. “The question is, can we manage the risk of both diseases to help people live healthy and productive lives?” she said.
The goal, she explained, is to understand a patient’s risk of cardiovascular disease when cancer is diagnosed and then to manage that risk throughout the treatment for cancer and beyond. If a patient already has cardiovascular disease, then the disease would be managed along with the cancer, Dr. Minasian added.
Increasing Awareness of Cardiac Side Effects
With an aging US population and continued advances being made in cancer care, some researchers warned that cardiotoxicities are likely to become a larger concern in the coming decades.
Yet, several speakers noted that many of their colleagues in cardiology and oncology were generally unfamiliar with the cardiac side effects of cancer treatments.
“We need to engage all members of the health care team, including doctors, pharmacists, and nurses, to convey the importance of cardiovascular health in cancer survivors,” said Dr. Dent
Patients and survivors need to be informed as well, added Dr. Minasian, noting that collaboration among researchers will be critical to making progress against cardiotoxicities. “We need cardiologists and oncologists to work together to answer basic questions about cardiotoxicities that neither group could answer working alone,” she said.
Surgeons Help Patients Get the Treatments They Need
Some hospitals and cancer centers have developed multidisciplinary teams to facilitate the treatment of patients with cancer while mitigating the risk of cardiac side effects.
At the University of Texas MD Anderson Cancer Center, for example, Cezar A. Iliescu, M.D., is part of a new field known as interventional cardio-oncology. These physicians and researchers specialize in complex procedures that allow patients who have both cancer and heart disease to receive the cancer treatments they need.
“We’re able to do any cardiovascular procedure that patients with cancer—including frail patients—need, irrespective of their comorbidities,” said Dr. Iliescu. “We can say with strong confidence that the patient will not die from cardiovascular disease.”
The MD Anderson researchers have been publishing their results, including a review of the clinical management of acute coronary syndrome in patients with cancer.
“There are not a lot of data out there on how to manage the care of these types of patients, so we want to share our experience,” said Dr. Iliescu. “This is a very interesting and dynamic field.”
Nutrient acquisition and metabolism pathways are altered in cancer cells to meet bioenergetic and biosynthetic demands. A major regulator of cellular metabolism and energy homeostasis, in normal and cancer cells, is AMP-activated protein kinase (AMPK). AMPK influences cell growth via its modulation of the mechanistic target of Rapamycin (mTOR) pathway, specifically, by inhibiting mTOR complex mTORC1, which facilitates cell proliferation, and by activating mTORC2 and cell survival. Given its conflicting roles, the effects of AMPK activation in cancer can be counter intuitive. Prior to the establishment of cancer, AMPK acts as a tumor suppressor. However, following the onset of cancer, AMPK has been shown to either suppress or promote cancer, depending on cell type or state.
Methods
To unravel the controversial roles of AMPK in cancer, we developed a computational model to simulate the effects of pharmacological maneuvers that target key metabolic signalling nodes, with a specific focus on AMPK, mTORC, and their modulators. Specifically, we constructed an ordinary differential equation-based mechanistic model of AMPK-mTORC signaling, and parametrized the model based on existing experimental data.
Results
Model simulations were conducted to yield the following predictions: (i) increasing AMPK activity has opposite effects on mTORC depending on the nutrient availability; (ii) indirect inhibition of AMPK activity through inhibition of sirtuin 1 (SIRT1) only has an effect on mTORC activity under conditions of low nutrient availability; (iii) the balance between cell proliferation and survival exhibits an intricate dependence on DEP domain-containing mTOR-interacting protein (DEPTOR) abundance and AMPK activity; (iv) simultaneous direct inhibition of mTORC2 and activation of AMPK is a potential strategy for suppressing both cell survival and proliferation.
Conclusions
Taken together, model simulations clarify the competing effects and the roles of key metabolic signalling pathways in tumorigenesis, which may yield insights on innovative therapeutic strategies.
Discussion
As a cellular energy sensor, AMPK is activated in response to conditions that deplete cellular energy levels, such as nutrient starvation (especially glucose), hypoxia, and exposure to toxins that inhibit the mitochondrial respiratory chain complex [50]. Thus, AMPK plays a key role in coordinating metabolic pathways and in balancing nutrient supply with energy demand. Because of the favorable physiological outcomes of AMPK activation on metabolism, AMPK is believed to have therapeutic importance for treating obesity, type 2 diabetes, non-alcoholic fatty liver disease, and cardiovascular disease [51].
A number of roles have been hypothesized for AMPK in tumorigenesis, both as a promoter and a suppressor. A potential role for AMPK in limiting tumorigenesis is supported by its activation at low ATP by LKB1 [20], which is a tumor suppressor gene that is mutationally inactivated in a number of cancers. Administration of AMPK activators has demonstrated anti-tumorigenesis effects in culture and mice, and in some genetic contexts [52,53,54]. Activated AMPK phosphorylates downstream targets that activate catabolic pathways, while switching off anabolic pathways and other ATP-consuming processes. As a result, AMPK not only promotes ATP synthesis but also restricts cell growth and proliferation in an attempt to restore energy homeostasis and maintain cell viability. However, a conflicting role for AMPK emerges as it is found to promote cell survival under nutrient-poor conditions. This effect is particularly relevant for cancer cells, which are often challenged with insufficient nutrients in the microenvironments to support their needs. Thus, AMPK is also hypothesized to play a pro-tumorigenic role and its presence may be essential to sustain the rapid growth of some cancer populations. Indeed, findings in cancer cell lines and orthotopic xenografts [27] suggest that AMPK is required for some tumor cells to survive under metabolic stress [45, 55].
Is AMPK beneficial or malevolent in cancer? More specifically, does AMPK promote or limit cancer cell proliferation and survival? This question is challenging to answer due to the complexity of the signalling pathways that regulate cell growth, which involve many positive and negative feedback loops. To attain insights into the synergy among these processes, and to unravel the effect of activating or inhibiting AMPK under different cellular microenvironments, we have developed the present computational model. To interrogate the effect of AMPK activation on cancer cell population, we applied the model to assess the effect on mTORC1, the activation of which promotes cell proliferation, and mTORC2, the activation of which favors cell survival [29]. Model simulations (Fig. 4) suggest that under nutrient-poor conditions, AMPK activation may have an overall pro-tumorigenic role by facilitating cellular survival and hence the growth of cancer. In contrast, with sufficient nutrient availability, the anti-proliferation effect of AMPK dominates, and AMPK acts as a tumor suppressor. Taken together, whether AMPK is pro- or anti-tumorigenic depends, in part, on the nutrient level of the microenvironments of the cancer cells.
Model prediction is consistent with findings in a study by Saito et al. [56], which investigated the extent to which AMPK is critical in achieving metabolic homeostasis in leukemia-initiating cells. They observed that AMPK deletion caused a drastic loss in leukemia cells in the bone marrow, a nutrient-poor environment, but that effect is substantially attenuated in leukemia cells in the spleen, where nutrients are relatively plentiful [56]. These findings have potentially groundbreaking implications in cancer therapies. Before the onset of cancer, there was clearly no concern regarding the effect of AMPK on cancer cell survival. Hence, the health impacts of AMPK activators such as metformin are clearly positive. But in established cancers, AMPK can be a double-edged sword [57]. In most cancers, the affected organs (e.g., spleen) are well perfused and cancer cells have access to sufficient nutrients; under these conditions, AMPK opposes cancer growth and proliferation. But in some cancers, the microenvironments are nutrient-poor (e.g., bone marrow leukemia), and cancer cells are more dependent on AMPK activity. In that case, the activation of AMPK would increase the viability of the tumor cells and thereby potentially decrease survival of the patient. Thus, in cancers such as bone marrow leukemia, it would be an AMPK inhibitor rather than an activator that might be therapeutically useful.
Because AMPK inhibitors are not widely available, we conducted simulations to explore alternative approaches to reduce cancer cell population. We considered indirect AMPK inhibition via the inhibition of SIRT1, which is required for AMPK activation [24]. However, while SIRT1 inhibition influences mTORC1 and mTORC2 activation levels, those effects are insignificant when nutrients are scarce (Fig. 5). Given that this is the cell microenvironment in which AMPK inhibition may limit cancer cell population growth (Fig. 4), what are the alternative means of simultaneously suppressing mTORC1 and mTORC2, if not via SIRT1 inhibition? The predicted negligible effect of SIRT1 inhibition may be attributable to the significant but insufficiently large impact on AMPK activation. With a 90% reduction in SIRT1 abundance, the model predicts less than 50% reduction in AMPK activation under nutrient deprivation, due to the opposing effect from the mTORC1-ULK1-AMPK feedback loop (see Fig. 1). In contrast, when AMPK is much more strongly inhibited, the model predicts significant changes in mTORC1 and mTORC2 (Fig. 4A). An implication of these results is that, if one seeks to combat a cancer whose growth is known to be promoted by AMPK activation, indirect inhibition of AMPK may not be sufficient due to the many compensatory feedback loops in the network. Direct AMPK inhibition may be required. Compound C is available as an AMPK inhibitor and has been demonstrated as a tumor suppressor for certain cancer types [58]. However, due to its toxicity Compound C is currently limited to laboratory applications. Similarly, the specificity of another AMPK inhibitor SBI-0206965 has been questioned [59]. Hence, cancer research may benefit from enhanced effort in the development of a clinically usable AMPK inhibitor.
The complexity of AMPK’s role as a target in anti-cancer therapy is due, in large part, to its activation of mTORC2, which enhances cell survival [29]. This fact points to the potential of mTORC2 inhibitors in cancer treatment. Indeed, selective mTORC2 inhibition has shown promise in blocking breast cancer cell growth and survival and in slowing the migration and metastasis of melanoma cells [60]. However, given the many protein-protein interactions, inhibition of mTORC2 inevitably affects mTORC1 activity, possibly with detrimental outcomes. Furthermore, excessive inhibition of mTORC2 may overly suppress AKT, which is essential in the translocation of GLUT4, and lead to insulin insensitivity [61]. Our simulations indicate that if a mTORC2 inhibitor is used in an anti-cancer therapy, its effect in combating the progression of cancer will be enhanced by combining it with an AMPK activator (Fig. 7).
Another notable protein that modulates mTOR signalling is DEPTOR, which associates with both mTORC1 and mTORC2 and physically interacts with the FAT domain.
mTOR through its PDZ domain [62]. The role of DEPTOR as a tumor suppressor is consistent with its low expression revealed in a number of human cancers, including pancreas [14], esophageal squamous cell carcinoma [15], lungs [18], and breast cancer [16]. The role of DEPTOR in inhibiting tumor progression may be attributed to its ability to repress cell migration, which is necessary in metastasis and cancer progression. Supportive evidence is provided by the significantly reduced DEPTOR expression reported on the invasive front of endometrial cancer tissues. Consistency with the multifaceted nature of most aspects of cancer, DEPTOR has been reported to be overexpressed in multiple myeloma cells [12], which suggests a role of oncogene rather than tumor suppressor. Whether and how DEPTOR might promote metastasis in specific contexts awaits clarification in future studies. Our model simulations suggest that the relative effect of DEPTOR on cancer cell proliferation and survival depends on its expression level and other factors, including metabolic stress and AMPK activation level (Fig. 6).
Given the complexity of the signalling network, the effect of a single perturbation is often difficult to second guess. The cascading effects and feedback response can be fully explored using the present model. For example, the DEPTOR simulations suggest that with adequate nutrients, administering either a DEPTOR activator or inhibitor can shift cell fate away from proliferation in favor of cell survival; but in nutrient deprivation, DEPTOR inhibition may introduce oscillations in mTORC (Fig. 6). Another potentially impactful application of the model lies in the exploration of drug-drug interactions. In the mTORC2 inhibitor and AMPK activator simulations, the model predicts that when co-administered, these drugs may effectively limit the cancer population and the effect of both drugs on the system is not additive and is difficult to predict without a mathematical model.
Trialling more cancer drugs on children could help children like Grace in the future, her mum says
Children with cancer could be missing out on potentially life-saving drugs because EU regulations allow drug companies to opt out of running trials in children, cancer experts say.
Since 2012, 62% of approved EU cancer drugs were not tested on under-18s.
But cancer scientists say the rules should be changed so that adult cancer drugs have to be tested on children.
They are also calling for the age limit for adult clinical trials to be lowered to include teenagers.
Who is saying all this?
The Institute of Cancer Research in London, cancer hospital the Royal Marsden and parents of children who have died from cancer say nowhere near enough cancer medicines are being trialled in children or licensed for use in children.
A consultation is currently running on the future of EU rules on clinical trials, which means there is a chance they could be changed.
What happened to Grace?
Grace Kelly was four years old when she died from a very aggressive tumour in her kidney, just three weeks after she had been diagnosed, in 2014.
Her mother, Jennifer, who is a GP, believes the regulations should be tightened to allow more tests of cancer drugs on children to take place.
“There could have been a treatment for her out there, but we were told at her diagnosis that her cancer was [terminal],” she says.
She says huge progress could be made in treating rare cancers if the rules were changed.
“They are not looking at the children right now,” she says.
Image Grace had started school a month before she was diagnosed with cancer
Why can drug companies opt out of trials in children?
The rules, called the EU Paediatric Regulation, which were set up in 2007, allow drug companies to be granted a waiver by the European Medicines Agency (EMA) when it comes to trialling cancer drugs on children.
This usually happens if the drug in question targets a cancer such as lung cancer that does not affect or is very rare in children.
But cancer researchers and charities say the way a drug works may mean it could be effective in children – even if it does not seem to be relevant.
Cancer medicines are changing, and they are often designed to treat many different types of cancer, which may have the same genetic target, rather than just one.
So they want fewer waivers to be issued and more trials on children to take place.
Why do drug companies want to avoid carrying out trials in children?
It is not that they do not want to carry out the trials and help cure childhood cancers – it is more that they want to make sure the trials are worthwhile.
Not all cancer drugs will be relevant or safe for children.
Creating cancer drugs is an expensive process and developing treatments for children, in whom cancers are rare, is a financial challenge for many manufacturers.
That is why it has been suggested that greater economic incentives are needed for companies to run trials in children.
Are drug trials on children really complex?
Doctors have to be very careful when treating children with cancer, of course.
They will always follow up closely after drugs are given – but children with cancer are capable of being treated just like adults, often with the same drug doses.
What difference could tightening the rules make?
Prof Paul Workman, from the Institute of Cancer Research, says children are missing out on innovative cancer treatments now common in adults.
As a result, he wants the regulations to be updated so that children with cancer – even if it is rare or terminal – get the best possible treatment with the latest medicines.
Prof Louis Chesler, honorary consultant in paediatric oncology at the Royal Marsden NHS Foundation Trusts, says access to cancer medicines has improved in recent years and more cancer drugs are being developed – but there are still improvements that could be made.
“Is there any reason why adult cancer trials can’t lower their age limits to 16, or even 12?” he asks.
And he adds: “Everyone realises this is a challenge, but more incentives are needed for drug companies to make a return and to speed up the development of drugs.”
For decades, surgery, radiation and chemotherapy have been the three staple treatments against cancer. But clinical trials over the past five years have shown that harnessing the body’s immune response—which evolved to fend off harmful bacteria and viruses, among other things—presents a new treatment alternative. In fact, for some types of cancer, clinical trials of immunotherapy have reported complete remission in 90 percent of cases. The April issue of Scientific American highlights these emerging therapies, but we have covered the growing promise of immunotherapy for quite a while. In this special digital package, we have pulled together other recent Scientific American articles about different types of immunotherapy that tell you even more about this exciting next generation of cancer treatment.
CONTENTS
The Cancer Defense
Against cancer, new enhancements to the body’s own immune system are looking like lifesavers
By Karen Weintraub on April 1, 2016
What Gene Therapy Needs Now: A Good Off Switch
Researchers are developing molecular switches that can inactivate transplanted genes, paving the way for safer gene therapies. First up—immunotherapies for cancer
By Jim Kozubek on January 1, 2016
Can Viruses Treat Cancer?
For some cancer patients, viruses engineered to zero in on tumor cells work like a wonder drug. The task now is to build on this success
By Douglas J. Mahoney, David F. Stojdl, Gordon Laird on November 1, 2014
New Drugs Free the Immune System to Fight Cancer
By releasing the brakes that tumor cells place on the immune system, researchers are developing a new generation of more powerful treatments against malignancy
By Jedd D. Wolchok on May 1, 2014
A New Ally against Cancer: Vaccines
The FDA recently okayed the first therapeutic cancer vaccine, and other drugs that enlist the immune system against tumors are under study
Here’s what happens when you take away a cancer cell’s fuel.
Cancer cells are cells that cheat death – rather than growing old and dying, as healthy cells do, they continue to grow and divide, changing their metabolism to continue proliferating throughout the body. It’s that proliferation of malignant cells that gives rise to cancers and tumours, and the challenge for medical researchers is to prevent this abnormal behaviour from occurring.
One way cancer cells fuel their growth and expansion is by increasing their glucose intake, and researchers are now looking at the possibility of shutting this down to combat their spread. A recent study has identified the PARP 14 protein as being responsible for the additional glucose production, and it’s overproduced in virtually every human cancer, but isn’t found in normal, healthy cells.
Genetic and molecular tests have shown that reducing PARP 14 levels in cancer cells literally starves them to death, as the UK-based team describes over at The Conversation. What’s more, scientists have discovered that the level of PARP 14 also influences the chance of patients surviving cancer, and this could help doctors identify the aggressiveness of a particular cancer ahead of time and adjust the treatment accordingly.
While a PARP 14-inhibiting drug is still a long way from becoming a reality at the moment, the findings have the potential to make a huge difference in cancer treatments once the necessary development and testing has been completed. Unlike chemotherapy and radiotherapy techniques, a PARP 14 blocker would only affect the cancerous cells, so treatment would be much kinder to the patient’s body.
The authors of the study, published in Nature Communications, believe that processes like chemotherapy would still be necessary, but a drug that targets the protein that cancerous cells rely on would make these cells much more vulnerable to chemo – as a result, doses could be lowered or programs could be shortened.
Glucose is so important to cancer cells because it not only gives them energy, it also guards against the molecules that cause natural cell death. If that glucose is removed, the cancer cells have their guard down. But it’s not quite as simple as cutting out sugar from your diet, because cancer cells adapt to find alternative fuel sources to build up glucose levels.
Researchers need to first design a drug that blocks or reduces PARP 14, and then make sure it’s safe and effective for humans, but our understanding of how cancer spreads – and how it can be stopped – is growing all the time, and the PARP 14 discovery could be one of the most important finds yet. “If we can find a way of stopping this over production of PARP 14 we can cure cancer,” says one of the team, Salvatore Papa from the University of London.


 Trialling more cancer drugs on children could help children like Grace in the future, her mum says
Trialling more cancer drugs on children could help children like Grace in the future, her mum says


