The golden age of antibiotic discovery from the ’50s and ’60s lies far behind us and antibiotic resistance is slowly becoming an enormous problem. Will artificial intelligence be able to save us from a world without working antibiotics?
Antibiotic resistance is slowly becoming an enormous problem in the medical world, will artificial intelligence be able to save us from a world without working antibiotics?
The golden age of antibiotic discovery from the ’50s and ’60s lies far behind us. Back then, countless new classes of antibiotics were discovered in rapid succession. Sadly though, since then, hardly any new types of antibiotics have been found while antibiotic resistance is slowly becoming an immense problem.
Without the development of new and stronger antibiotics, an era where small injuries and ordinary infections can kill, and where complex procedures such as chemotherapy and surgery become too risky, is a genuine possibility. The world health organization even stated that antibiotic resistance even endangers the world as we know it as it can lead to huge epidemics if we are not careful.
Taking all of the above into consideration, the more it becomes clear how critical a recent discovery of a potent antibiotic by MIT researchers actually is. They identified the new antibiotic using artificial intelligence, machine learning to be precise. The drug was able to kill many of the most problematic disease-causing bacteria in laboratory testing. Incredibly enough, it was even able to kill off several strains that are immune to all known current antibiotics.
The scientists used a computer program designed to pick out possible antibiotics that eliminate bacteria using mechanisms than differ from those of currently existing drugs. Amazingly the program is able to scan over a hundred million chemical compositions per day!
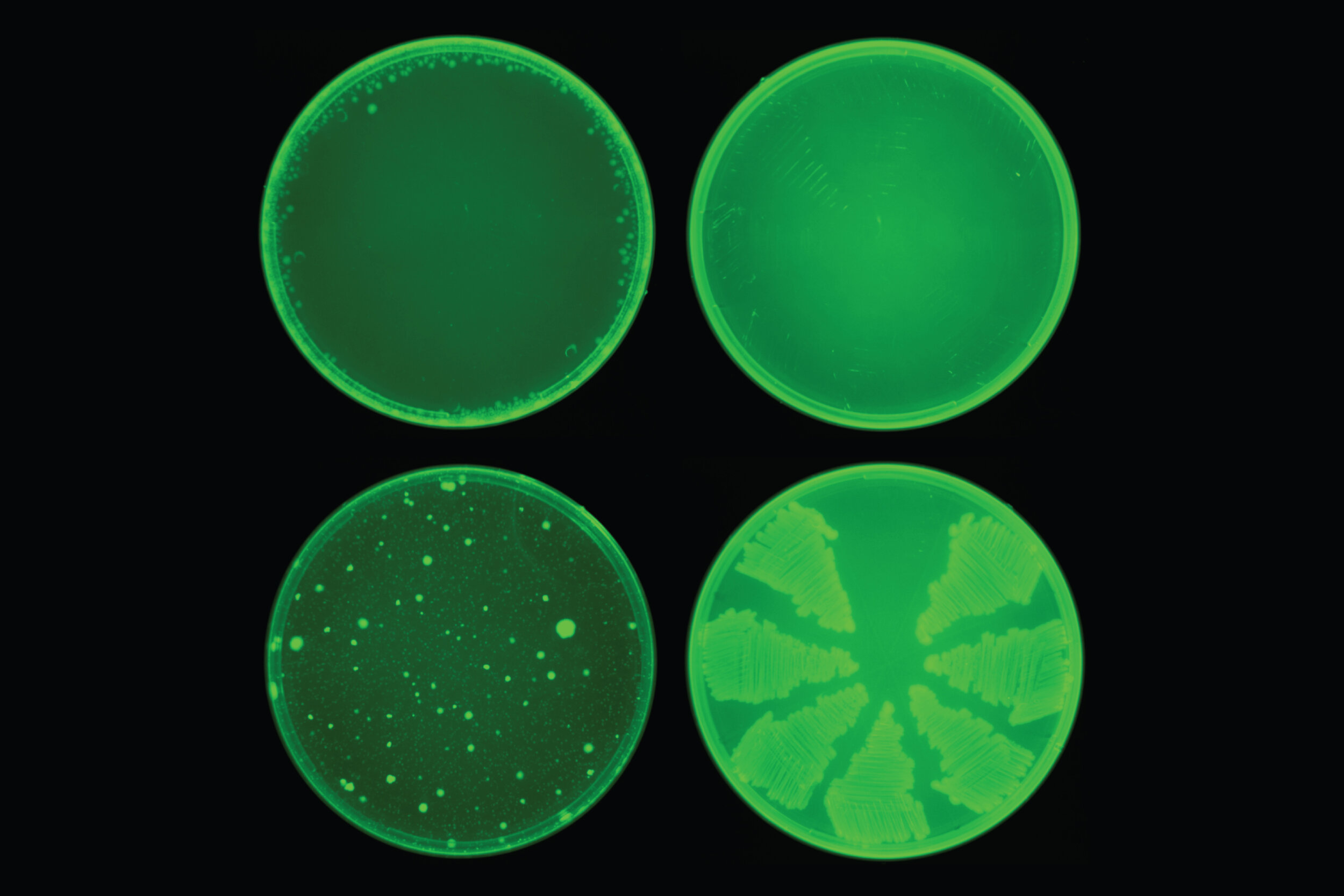
MIT scientist employed a machine-learning algorithm to detect a drug called halicin. It is capable of eliminating many strains of bacteria. Halicin (top row) prevented the development of antibiotic resistance in E. coli, while ciprofloxacin (bottom row) did not.
James Collins, one of the researchers and MIT Professor of medical engineering and science, stated that their goal was to create a platform that would enable them to harness the power of artificial intelligence to usher in a new age of antibiotic drug development. Their approach uncovered a marvelous molecule that is arguably one of the most potent antibiotics that has ever been discovered.
Amazingly, the antibiotic mentioned above was not the only antibiotic the researchers found. It turns out they identified several other promising antibiotic candidates as well. The scientists plan to further test these candidates in the future. As if that isn’t enough, the computer model is also believed to be capable of designing new drugs based on what it has discovered about chemical compositions that facilitate drugs to eliminate bacteria.
Industrial factory farms routinely use antibiotics, which cause unnatural growth by altering the animals’ gut microbiome. Some of those gut bacteria become antibiotic-resistant — leading the contaminated meat to become a source of drug-resistant infections.
Story at a glance:
An estimated 35,000 Americans die each year from drug-resistant infections. Globally, the death toll attributed to drug-resistant infections is thought to be around 4.95 million annually.
When animals are given antibiotics, it causes unnatural growth by altering their gut microbiome. In the process, some of those gut bacteria become antibiotic-resistant. Contaminated meat can then become a source of drug-resistant infections.
Between 2015 and 2017, antibiotic use in U.S. food animals declined by 42%, but the downward trend didn’t last. In the years between 2017 and 2022, antibiotic use increased by 12%, with 4.3% of that rise occurring in 2022 alone. Other data show the number of animals raised in 2022 was lower than in 2021, so more antibiotics were used in a smaller number of animals.
Antibiotics are also massively overused in human medicine and have risks besides the promotion of drug resistance. Fluoroquinolones have been shown to increase your risk of aortic rupture, which can lead to death. Several oral antibiotics have also been linked to the development of kidney stones, inflammatory bowel disease (IBD) and colorectal cancer.
Natural antimicrobials that do not appear to promote drug resistance include garlic, ginger, echinacea, goldenseal, myrrh oil, thyme oil, oregano oil, clove extract, olive leaf extract and colloidal silver.
Antibiotic-resistant infections are a vastly underestimated health threat. An estimated 35,000 Americans die each year from drug-resistant infections.
Globally, the death toll attributed to drug-resistant infections could be as high as 4.95 million annually, and it’s only getting worse.
Agriculture has played a central role in this trend. As of 2020, 69% of the U.S. antibiotic supply was bought up by the meat industry, and most of these antibiotics are given to animals that aren’t sick; rather, they’re used for prophylactic and/or growth promotion purposes.
When animals are given antibiotics, it causes unnatural growth by altering their gut microbiome. In the process, some of those gut bacteria become antibiotic-resistant.
Antibiotic ban lowers antibiotic-resistant infections in humans
Governments have tried to tackle the growing problem of antibiotic resistance for decades. The European Union (EU) led the way by banning the use of antibiotics for growth promotion purposes in 2006.
In 2013, the U.S. Food and Drug Administration issued guidance that called on farmers to voluntarily begin to phase out the use of medically important antibiotics in livestock production.
In 2017, the World Health Organization urged farmers to stop the routine use of antibiotics “to promote growth and prevent disease in healthy animals” to preserve the effectiveness of antibiotics used in human medicine.
That same year, the U.S. government also tightened federal rules to prevent the use of antibiotics for growth promotion.
A year later, in 2018, California became the first U.S. state to ban the routine preventive use of antibiotics in food-animal production, as well as any antibiotic use without a veterinarian’s prescription — a decision later confirmed to have had a beneficial impact, reducing the prevalence of extended-spectrum cephalosporin-resistant E. coli in the human population by 7.1% in the following three years.
Conversely, in the United Kingdom (U.K.) — the only European country where antibiotics are still allowed to be used prophylactically in food animals — U.K. Health Security Agency data show the prevalence of serious antibiotic-resistant infections rose by 2.2% between 2020 and 2021.
In January 2022, the EU further restricted the use of agricultural antibiotics, banning “all forms of routine use in farming, including preventative group treatments.”
Antibiotic use is going in the wrong direction
Between 2015 and 2017, antibiotic use in the U.S. declined by 42%, but the downward trend didn’t last. In the years between 2017 and 2022, antibiotic use increased by 12%; 4.3% of that rise occurred in 2022 alone.
“The Food and Drug Administration data show sales of medically important antimicrobials approved for use in farm animals rose 4.3% to 6.25 million kilograms in 2022.
“The 2022 figure is a significant decrease on the 8.36 million kilograms sold in 2016, the earliest year shown in the data. But the 2022 figure is higher than all other years since 2016, indicating a more recent trend in the wrong direction.
“Thomas Van Boeckel, an expert in global antimicrobial usage and resistance in farm animals, fish and humans, says the upward swing indicates that ‘unlike some European and Asian countries … the U.S. is clearly not on a trend that shows its commitment to sustainably reduce antimicrobial use in animals.’
“The data, he adds, shows the problem is ‘mostly a pig and cattle issue’ and reveals ‘a dependence’ by the livestock sector on antibiotics that has ‘potential consequences on the continued development of resistance.’ …
“According to FACT’s Steven Roach, a closer look at the data suggests sales may be even higher. ‘If you look at the more detailed biomass data … it shows that animal numbers were down in 2022 compared to 2021 so when corrected for biomass the [medically important antimicrobial] sales increases are even larger.’”
Antibiotics pose hidden health risks
Antibiotics are also massively overused in human medicine, which also contributes to the development of drug resistance. Antibiotic misuse and overuse also put your health at risk in other ways.
For example, fluoroquinolones have been shown to increase your risk of aortic dissection (a tear in the wall of the major artery, allowing blood to flow between the layers) or aortic rupture, which can lead to death.
Even though these antibiotics carry a “black-box” warning, fluoroquinolones are still often prescribed for upper respiratory infections and urinary tract infections (UTIs).
As noted by the authors, the lack of understanding of the risk profile of this class of antibiotics is putting patients at risk, and there’s “a dire need” to initiate educational campaigns among healthcare professionals to prevent unnecessary harm to patients.
The association is most pronounced among younger children and, with the exception of broad-spectrum penicillin, this risk remains statistically significant for up to five years after exposure.
According to research presented at the Digestive Disease Week conference held in San Diego, California, in May 2022, the use of antibiotics was associated with a 64% increased risk of developing IBD, and the risk increased with additional doses.
Compared with those who had taken no antibiotics in the previous five years, the risk of IBD in those who received five or more antibiotic prescriptions increased by 236%.
And, while all classes of antibiotics were associated with increased IBD risk, fluoroquinolones again took the lead, having the strongest association.
Considering their many risks, I advise using antibiotics only as a last resort. The good news is many natural plant-based remedies will help kill bacteria without the risk of building resistance, including the following.
Garlic — Garlic has been used to fight bacterial and parasitical infections for centuries. According to a 2014 review, garlic has been proven effective against “a plethora of gram-positive, gram-negative, and acid-fast bacteria,” including but not limited to Salmonella, E. coli, Klebsiella, Clostridium and Vancomycin-resistant enterococcus.
Importantly, garlic “exerts a differential inhibition between beneficial intestinal microflora and potentially harmful enterobacteria,” meaning it inhibits bad bacteria while leaving good bacteria alone.
Ginger — A 2020 study demonstrated that ginger essential oil was effective against E. coli and S. aureus, two bacteria involved in periodontal infections.
Another study found a 10% ginger extract effectively killed Streptococcus mutans, Candida albicans and Enterococcus faecalis, which are also implicated in the causation of oral infections. More than a dozen other bacteria are also vulnerable to its effects, as are a number of biofilms.
Ginger is not suitable for children under age 2, and adults should not take more than 4 grams of ginger per day. Pregnant women are advised to cap their intake at 1 gram per day.
Echinacea — According to Mount Sinai Hospital, echinacea extract may be used to treat “urinary tract infections, vaginal yeast (candida) infections, ear infections (also known as otitis media), athlete’s foot, sinusitis, hay fever (also called allergic rhinitis), as well as slow-healing wounds.”
As a general recommendation for infection, take it three times a day for a maximum of 10 days.
Goldenseal — One of the main constituents of goldenseal is berberine, known for its potent antibacterial properties. Berberine primarily kills gram-positive bacteria, including methicillin-resistant Staphylococcus aureus, or MRSA.
According to Mount Sinai, goldenseal is not recommended for pregnant or breastfeeding women, and those with high blood pressure, liver disease or heart disease should discuss its use with their medical provider, as it can interfere with medications prescribed for these conditions.
Potential adverse effects include irritation of the skin, mouth, throat and vagina, and increased sensitivity to sunlight.
Myrrh oil — When an antibiotic fails to kill off all the bacteria, you can end up with nongrowing bacterial persister cells. While these persisters do not undergo genetic change to make them resistant to antibiotics, they often end up forming biofilms and are a major cause of chronic low-grade infections.
This is where myrrh oil really shines, as research shows it preferentially kills off these nongrowing persister cells and does so without the risk of promoting resistance. Other research suggests it may be useful in the treatment of gingivitis, treatment-resistant trichomoniasis vaginalis (a sexually transmitted disease) and Lyme disease.
Thyme (including thyme essential oil) — Thyme oil has antibacterial, antibiofilm, antiviral, antifungal and antiseptic properties. However, make sure you’re using either standardized thyme preparations or essential oils that meet the requirements of national pharmacopeias.
What you’re looking for in thyme preparations are minimum thymol and carvacrol contents of 40%. In essential oils, you want 37 to 55% thymol and 0.5 to 5.5% carvacrol.
Oregano oil — Oregano oil has shown effectiveness against bacteria such as Streptococcus mutans, which causes dental cavities, as well as 11 different multidrug-resistant bacteria, including MRSA, and their biofilms. Tests have confirmed that repeated use of oregano oil does not lead to resistance, which makes it a useful remedy in the treatment of wounds.
Clove extract — Research has shown ethanolic clove extract provides broad-spectrum inhibition against both gram-negative and gram-positive UTI-causing pathogens such as Proteus mirabilis, Staphylococcus epidermidis, S. aureus, E. coli and K. pneumoniae.
Olive leaf extract — Olive leaf extract has been shown to be effective against bacteria such as Klebsiella, Staphylococcus aureus, E. coli and Salmonella.
Colloidal silver — Colloidal silver has been regarded as an effective natural antibiotic for centuries, and research suggests it can even help eradicate multidrug-resistant gram-positive and gram-negative bacteria.
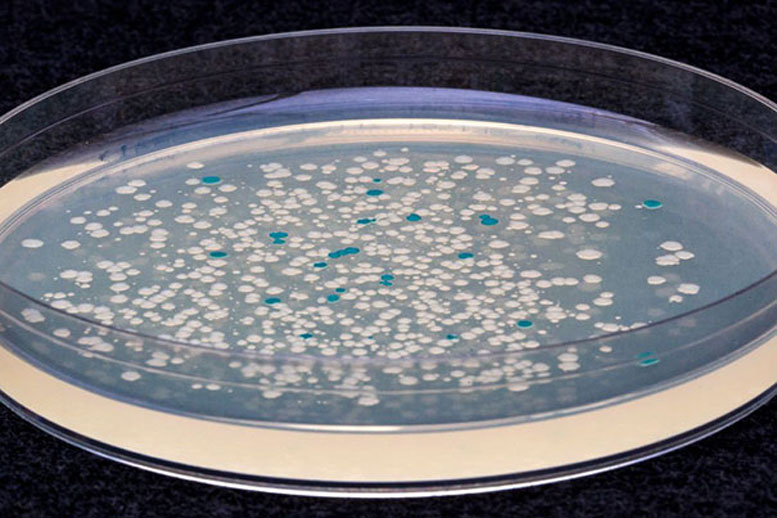
Colonies of engineered E. coli bacteria that were actively dividing at the time ATC was added turn blue when grown on a medium containing lactose, while those that were not dividing when ATC was added remain white. Credit: Wyss Institute at Harvard University
Scientists at the Wyss Institute used synthetic biology techniques to discover that bacteria respond to antibiotics very differently — exactly opposite, in fact — inside the body than on a petri dish, suggesting that some of our current assumptions about antibiotics may be incorrect.
Bacterial infections are the No. 1 cause of death in hospital patients in the U.S., and antibiotic-resistant bacteria are on the rise, causing tens of thousands of deaths every year. Understanding exactly how antibiotics work, or don’t, is crucial for developing alternative treatment strategies, both to target new “superbugs” and to make existing drugs more effective against their targets.
“The image most clinicians have is that antibiotics work by killing actively dividing bacteria, and nondividing bacteria are the ones that resist treatment and cause infections to persist. I wanted to know whether that’s actually true — does the proportion of dividing bacteria change over the course of an infection, and how do antibiotics impact that?” said Laura Certain, a clinical fellow at the Wyss Institute and Massachusetts General Hospital, the first author of the study published in the August 31 issue of Cell Host & Microbe.
“Synthetic biology is widely used to engineer bacteria so that they produce useful products or diagnose diseases, and we used that same approach to create a microbiology tool that can tell us how bacteria are behaving in the body,” she said.
Certain and her colleagues used a genetically engineered strain of E. coli that was created in the lab of Wyss core faculty member Pamela Silver a few years ago. The bacteria have a genetic “toggle switch” encoded into their DNA that changes from the “off” to the “on” position when the bacteria are exposed to a chemical called anhydrotetracycline (ATC). When the switch is turned on, a genetic change happens that allows the bacteria to digest the sugar lactose, which bacteria whose switches remain off cannot do. The key to this system is that the toggle switch can only be flipped if the bacteria are actively dividing when ATC is added; nondividing bacteria’s switches will stay off, even when ATC is present. Thus, the toggle switch offers a snapshot in time that can indicate whether bacteria were active or dormant at the moment of ATC exposure.
Bacterial studies are often carried out in vitro, but infections happen in the complex environment of living bodies, which are quite different from a petri dish. To evaluate their bacteria in vivo, the researchers implanted a small plastic rod into the legs of mice and inoculated their engineered bacterial strain into the legs to imitate the chronic bacterial infections that commonly arise in humans when medical devices and artificial joints are implanted. They then injected the mice with ATC at different times throughout the course of the infection to flip the toggle switch in any dividing bacterial cells to the “on” position.
When they extracted bacteria from the mice and grew them on a special lactose-containing medium, they found that all the bacteria were actively dividing for the first 24 hours, but by the fourth day that fraction dropped to about half and remained constant for the rest of the infection, indicating that the number of bacteria being killed by the body was balanced by new bacteria being created via cell division. This result differed from the in vitro response, in which all the bacteria stopped dividing once they reached the carrying capacity of their environment.
Next, the scientists tested the bacteria’s response to antibiotics in vivo by allowing the infection to progress for two weeks, then injecting the mice with the antibiotic levofloxacin. When they analyzed the extracted bacteria, they found that while the total amount of bacteria in the mice decreased, the proportion of the surviving bacteria that were actively dividing actually increased. This outcome was in direct opposition to antibiotics observed in vitro, which killed more dividing cells than nondividing cells. The researchers screened the bacterial colonies for antibiotic resistance, and did not find any evidence that the bacteria had evolved to better withstand the killing effects of the levofloxacin, confirming that the antibiotic was still effective.
“There are several possible reasons why we saw a higher proportion of dividing bacteria in the presence of an antibiotic,” said Certain. “We find it most likely that dormant cells are switching into an active state in order to ‘fill the gaps’ that arise when antibiotics reduce the overall bacterial population. If bacteria continue to actively divide throughout an infection, as our study suggests, they should be susceptible to antibiotics.”
Indeed, the researchers were able to cure the infection with a higher dose of the antibiotic, indicating that, contrary to conventional assumptions about bacterial infections, there is no fixed population of dormant, antibiotic-tolerant cells in this chronic infection model.
“If an antibiotic isn’t working, we should focus on finding ways to deliver more of it to the infection site or identifying other tolerance mechanisms that might be at play, rather than assuming that a bastion of nondividing bacteria is the culprit,” said the corresponding author and Wyss core faculty member Jim Collins, who is also the Termeer Professor of Medical Engineering & Science and a professor of biological engineering at the Massachusetts Institute of Technology.
MIT chemical engineers have devised a way to encapsulate probiotics so that they can be delivered along with antibiotics to kill multiple strains of bacteria. Credit: Ryan Allen
In the fight against drug-resistant bacteria, MIT researchers have enlisted the help of beneficial bacteria known as probiotics.
In a new study, the researchers showed that by delivering a combination of antibiotic drugs and probiotics, they could eradicate two strains of drug-resistant bacteria that often infect wounds. To achieve this, they encapsulated the probiotic bacteria in a protective shell of alginate, a biocompatible material that prevents the probiotics from being killed by the antibiotic.
“There are so many bacteria now that are resistant to antibiotics, which is a serious problem for human health. We think one way to treat them is by encapsulating a live probiotic and letting it do its job,” says Ana Jaklenec, a research scientist at MIT’s Koch Institute for Integrative Cancer Research and one of the senior authors of the study.
If shown to be successful in future tests in animals and humans, the probiotic/antibiotic combination could be incorporated into dressings for wounds, where it could help heal infected chronic wounds, the researchers say.
Robert Langer, the David H. Koch Institute Professor and a member of the Koch Institute, is also a senior author of the paper, which appears in the journal Advanced Materials on October 17. Zhihao Li, a former MIT visiting scientist, is the study’s lead author.
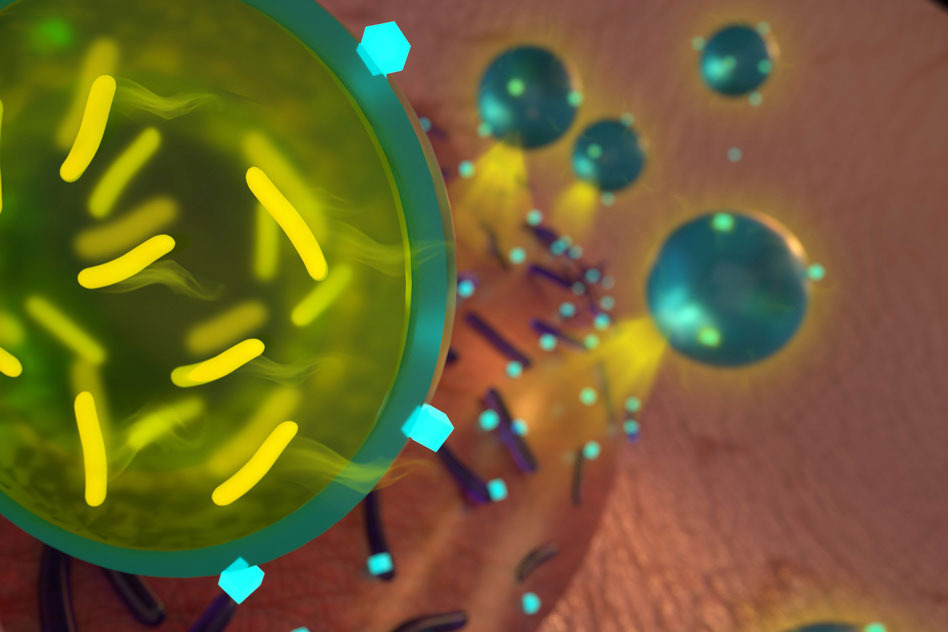
At left, spheres of alginate with probiotics encapsulated inside. At right, a close-up of a single sphere, with probiotic bacteria labeled in green. Courtesy of the researchers
Bacteria wars
The human body contains trillions of bacterial cells, many of which are beneficial. In some cases, these bacteria help fend off infection by secreting antimicrobial peptides and other compounds that kill pathogenic strains of bacteria. Others outcompete harmful strains by taking up nutrients and other critical resources.
Scientists have previously tested the idea of applying probiotics to chronic wounds, and they’ve had some success in studies of patients with burns, Li says. However, the probiotic strains usually can’t combat all of the bacteria that would be found in an infected wound. Combining these strains with traditional antibiotics would help to kill more of the pathogenic bacteria, but the antibiotic would likely also kill off the probiotic bacteria.
The MIT team devised a way to get around this problem by encapsulating the probiotic bacteria so that they would not be affected by the antibiotic. They chose alginate in part because it is already used in dressings for chronic wounds, where it helps to absorb secretions and keep the wound dry. Additionally, the researchers also found that alginate is a component of the biofilms that clusters of bacteria form to protect themselves from antibiotics.
“We looked into the molecular components of biofilms and we found that for Pseudomonas infection, alginate is very important for its resistance against antibiotics,” Li says. “However, so far no one has used this ability to protect good bacteria from antibiotics.”
For this study, the researchers chose to encapsulate a type of commercially available probiotic known as Bio-K+, which consists of three strains of Lactobacillus bacteria. These strains are known to kill methicillin-resistant Staphylococcus aureus (MRSA). The exact mechanism by which they do this is not known, but one possibility is that the pathogens are susceptible to lactic acid produced by the probiotics. Another possibility is that the probiotics secrete antimicrobial peptides or other proteins that kill the pathogens or disrupt their ability to form biofilms.
The researchers delivered the encapsulated probiotics along with an antibiotic called tobramycin, which they chose among other tested antibiotics because it effectively kills Pseudomonas aeruginosa, another strain commonly found in wound infections. When MRSA and Pseudomonas aeruginosa growing in a lab dish were exposed to the combination of encapsulated Bio-K+ and tobramycin, all of the pathogenic bacteria were wiped out.
“It was quite a drastic effect,” Jaklenec says. “It completely eradicated the bacteria.”
When they tried the same experiment with nonencapsulated probiotics, the probiotics were killed by the antibiotics, allowing the MRSA bacteria to survive.
“When we just used one component, either antibiotics or probiotics, they couldn’t eradicate all the pathogens. That’s something which can be very important in clinical settings where you have wounds with different bacteria, and antibiotics are not enough to kill all the bacteria,” Li says.
Better wound healing
The researchers envision that this approach could be used to develop new types of bandages or other wound dressings embedded with antibiotics and alginate-encapsulated probiotics. Before that can happen, they plan to further test the approach in animals and possibly in humans.
“The good thing about alginate is it’s FDA-approved, and the probiotic we use is approved as well,” Li says. “I think probiotics can be something that may revolutionize wound treatment in the future. With our work, we have expanded the application possibilities of probiotics.”
In a study published in 2016, the researchers demonstrated that coating probiotics with layers of alginate and another polysaccharide called chitosan could protect them from being broken down in the gastrointestinal tract. This could help researchers develop ways to treat disease or improve digestion with orally delivered probiotics. Another potential application is using these probiotics to replenish the gut microbiome after treatment with antibiotics, which can wipe out beneficial bacteria at the same time that they clear up an infection.
Sometimes the therapeutic effects of honey surpass even those of medication.
In this series, we will explore the good and bad sweeteners, uncover the unexpected outcomes of cutting out sugar, and discover the ultimate way to achieve this.
Honey is a sweet food and medicine that nature has gifted us. Its history of medicinal use can be traced back 8,000 years. Sometimes, the therapeutic effects of honey surpass even those of medications, particularly its outstanding antibacterial and antiviral properties.
Honey’s Antibacterial Properties Are Superior to Antibiotics’
“Bacteria quickly learn how to fight off the effects of the antibiotic drugs, but they don’t have honey resistance,” Nural Cokcetin, a research fellow at the Australian Institute for Microbiology and Infection in the science faculty at the University of Technology Sydney, said in an interview with The Epoch Times.
Honey has been used to treat skin problems and wound infections for thousands of years. For instance, ancient Greeks and Egyptians would apply honey topically to the skin to treat wounds and burns. Honey’s effectiveness in treating wounds and eczema was also documented in Persian traditional medicine. Interestingly, the concept of microorganisms such as bacteria and fungi causing wound infections during those historical periods might not have even been known.
The broad-spectrum antibacterial activity of honey has been increasingly recognized and substantiated. In recent years, the prevalence of wound infections caused by antibiotic-resistant bacteria has become a major global health care challenge. Honey can disrupt biofilms that are formed by these resistant bacteria and sometimes penetrate the biofilm structure to eliminate the embedded bacteria. An article published in the journal of the American Society for Microbiology in 2020 reported no documented cases of bacteria developing resistance to honey.
In clinical settings, medical-grade honey has been utilized in various ways. It’s formulated into topical ointments, dressings, and bandages for the treatment of postoperative wound infections, burns, necrotizing fasciitis, nonhealing wounds, boils, venous ulcers, diabetic foot ulcers, eczema, psoriasis, and dandruff. Additionally, it has proven effective in both preventing and treating infections caused by multidrug-resistant microorganisms.
In vitro studies have shown that honey can kill Helicobacter pylori. Furthermore, oral consumption of honey can reduce the duration of bacterial diarrhea.
The antibacterial properties of honey originate from its inherent characteristics and a diverse array of components derived from both nectar-producing plants and bees themselves. (Africa Studio/Shutterstock)
Key Antimicrobial Components
The antibacterial properties of honey originate from its inherent characteristics and a diverse array of components derived from both nectar-producing plants and bees themselves. Additionally, some of these components are formed during the maturation process of honey.
High Viscosity and pH
Honey has a high sugar content, reaching up to 82.5 percent. As a result, it has a viscous and syrupy consistency, exhibiting hygroscopic properties (ability to absorb moisture) and high osmolarity. Bacteria that come into contact with honey undergo dehydration and ultimately perish.
Honey is acidic due to its various organic acids, with a pH value ranging from 3.2 to 4.5. Bacteria can’t survive in honey; their optimal pH typically ranges between 6.5 and 7.5.
Primary Antibacterial Agent: Hydrogen Peroxide
An important enzyme in honey derived from bees facilitates the oxidation of glucose, resulting in the production of hydrogen peroxide.
Hydrogen peroxide is an effective bactericidal agent that can inhibit and kill microorganisms.
Interestingly, water is necessary to induce honey’s hydrogen peroxide production. The maximum level of hydrogen peroxide can be obtained by diluting honey to a concentration of 30 to 50 percent, according to a paper in the International Journal of Microbiology.
Bee defensin-1 is another natural antibacterial component in honey originating from the honeybee’s hypopharyngeal gland.
Bee defensin-1 is an antimicrobial peptide that can kill various bacteria and microorganisms. Specifically, the defensin protein has been shown to create pores within the bacterial cell membrane, leading to cell death.
Additionally, bee defensin-1 can aid in wound healing by stimulating keratinocytes, the most common type of skin cell.
Unique Antibacterial Component in Manuka Honey: Methylglyoxal
Manuka honey is often mentioned in studies regarding the antibacterial effects of various kinds of honey. As a globally recognized honey with high antibacterial potency, it possesses a unique natural component called methylglyoxal (MGO).
After honeybees gather nectar from the flowers of manuka trees, a natural substance that’s found in the trees undergoes spontaneous dehydration, leading to the formation of MGO in the honey.
“The more of [methylglyoxal] there is, the more antibacterial that honey is,” Dee Carter, a professor from the School of Life and Environmental Sciences at the University of Sydney, told The Epoch Times.
MGO exhibits remarkable antibacterial properties by itself. It can alter the structure of bacterial fimbriae and flagella (appendages), and induce damage to their cell membranes, ultimately resulting in cell death.
However, this substance is sensitive to heat. Heating manuka honey to 98.6 degrees F (37 degrees C) can increase the levels of MGO, but heating it to 122 degrees F (50 degrees C) results in the loss of MGO.
Manuka honey possesses a unique compound derived from the manuka tree called methylglyoxal (MGO), which is an antibacterial compound not found in other types of honey.
Honey’s Antiviral Properties May Reduce COVID-19 Complications
Honey not only possesses antibacterial properties but also exhibits antiviral effects, which help protect the body and boost the immune system. Many individuals find relief from symptoms of cold and respiratory illnesses by consuming honey water, and there’s a valid basis for this remedy.
Combats Influenza and COVID-19
MGO can inhibit the growth of enveloped viruses, including the virus that causes COVID-19.
According to a study published in the Eurasian Journal of Medicine and Oncology in 2020, computer simulations revealed that multiple compounds found in honey can bind to the protease of SARS‑CoV‑2, effectively inhibiting its replication.
MGO in manuka honey can also inhibit the replication of influenza viruses, including drug-resistant strains.
Currently, scientists are researching the potential of MGO for managing and treating COVID-19.
Boosts the Immune System
Honey can activate several immune cells, enabling them to eliminate viruses effectively. For example, oligosaccharides that are present in honey can enhance the activity of natural killer cells. Additionally, certain immune cells can “remember” specific viruses during the antiviral response, offering future protection against the same viral invasions.
Honey can promote the proliferative activity of immune cells, thus increasing their quantity.
Promotes Autophagy
Honey can promote autophagy, which is crucial in combating deadly viruses such as SARS‑CoV‑2, which causes COVID-19. It’s an internal cellular process that involves the degradation and metabolism of cells, allowing for the removal and recycling of unwanted or damaged cells and impurities. This process contributes to the generation of healthier cells and promotes recovery.
Honey’s Anti-Inflammatory and Gut-Health Benefits
Inflammation is a common occurrence in bacterial or viral infections. Left unchecked, it can significantly harm the body, potentially leading to life-threatening complications.
Moreover, honey has been suggested to have a dual role in inflammation control: It can downregulate anti-inflammatory factors, thereby reducing inflammation damage, and stimulating the production of inflammatory mediators, promoting wound healing.
In one of Ms. Cokcetin’s studies, honey could reduce inflammation levels in the intestines. She attributes this effect to the abundant presence of phenolic compounds found in honey.
She explained that honey also contains oligosaccharides and polysaccharides, which are complex sugars. These compounds serve as prebiotics, supporting the growth of beneficial bacteria in the gut and inhibiting the growth of harmful bacteria. Additionally, consuming honey promotes the production of short-chain fatty acids in the intestines.
Choosing Honey With Potent Properties
Generally, raw and darker honey varieties tend to have more robust efficacy.
Commercially available honey found on supermarket shelves differs from raw honey sold by beekeepers or at bazaars, as it’s generally pasteurized. Research has shown that heat processing can lower the antioxidant capacity of honey by 33.4 percent. Alternatively, you can also choose honey processed using high-pressure techniques.
Honey comes in a diverse range of colors, from light yellow to amber, dark red, and even nearly black. These colors reflect the varying composition of honey, such as polyphenols, minerals, and pollen. Numerous studies suggest that dark-colored honey generally contains higher levels of phenolic compounds and exhibits more potent activity.
To obtain manuka honey with exceptional antibacterial properties, it’s recommended to opt for pure honey sourced from New Zealand and Australia.
The manuka tree is exclusive to specific New Zealand and Australian regions, and its annual yield is limited. Certain products labeled as manuka honey may contain blends of other honey types, potentially affecting the honey’s properties. Furthermore, some of these products may even include low-quality ingredients such as sucrose.
Opting for single-origin honey sourced exclusively from the manuka tree and checking for its Unique Manuka Factor (UMF) rating is recommended. A higher UMF rating indicates higher levels of substances related to MGO. Some honey products also specify the amount of MGO in milligrams per kilogram.
However, manuka honey with a higher UMF rating may have a strong flavor that some people find pungent.
Ms. Cokcetin recalled that when she began her research on the antibacterial properties of honey, a professor she worked with said, “We’ve already got this great gift from nature that is a solution to superbugs; we just have to figure out how it works and why it works the way it does.”
In a phase III trial, the addition of oral clarithromycin to beta-lactam antibiotic treatment improved the clinical response of people with community-acquired pneumonia who had systemic inflammatory response syndrome, findings that support existing guidelines.
In the study, the proportion of patients meeting the primary composite endpoint after 72 hours of treatment — fulfilling criteria for both respiratory symptom improvement and an early dampening of the inflammatory burden — reached 68% of those randomized to clarithromycin atop standard care and 38% of those receiving beta-lactam antibiotics alone (OR 3.40, 95% CI 2.06-5.63), reported Evangelos Giamarellos-Bourboulis, MD, of the National and Kapodistrian University of Athens, Greece, and coauthors.
Additionally, the combination of antibiotics significantly reduced the risk for subsequent organ dysfunction, prevented development of new sepsis, and shortened the time to hospital discharge, according to the double-blind ACCESS trial published in Lancet Respiratory Medicineopens in a new tab or window.
“Our results suggest that clarithromycin should be added to the management of hospitalized patients with community-acquired pneumonia to alleviate the inflammatory burden and to achieve early clinical benefit,” the group wrote.
Serious treatment-emergent adverse events (TEAEs) out to 90 days occurred in similar numbers between groups (43% vs 53%; OR 1.46, 95% CI 0.89-2.35).
Time-to-event curves suggested most of the benefit of the macrolide occurred in the first 8 days. The investigators added that they had indirect evidence of clarithromycin having a strong effect at the level of immune function — given that the clarithromycin group produced more tumour necrosis factor-α and less interleukin-10 in response to lipopolysaccharide stimulation than patients in the placebo group at day 4 — though cautioned that the antibiotic should still be used with caution to avoid emergence of resistance.
“Perhaps the most intriguing aspect of the study was the attempt to assess how clarithromycin modified immune response,” commented Grant Waterer, MD, PhD, of the University of Western Australia and Royal Perth Hospital.
“If impairment in early downregulation of pro-inflammatory responses is beneficial, this has fundamental implications for our understanding of the pathobiology of severe sepsis. Because most of the trend to benefit in mortality with clarithromycin was observed in the first 6-7 days, primary sepsis was probably driving mortality, not a reduction in secondary infections,” he wrote in an invited commentopens in a new tab or window.
In any case, ACCESS filled the need for a good randomized trial on combining beta-lactam antibiotics and macrolides for community-acquired pneumonia, a practice that has already been recommended by American and European guidelines alike.
ACCESS was conducted at multiple public hospitals within Greece from 2021 to 2023.
Investigators sought adults requiring hospital admission who were experiencing two or more community-acquired pneumonia-related symptoms such as cough, dyspnoea, pleuritic chest pain, or purulent sputum expectoration. Participants were ineligible if they had any history of contact with the hospital environment or with healthcare facilities during the preceding 90 days.
Patients also needed to exhibit two or more criteria for systemic inflammatory response syndrome, have a total Sequential Organ Failure Assessment (SOFA) score of at least 2, and have a procalcitonin concentration of at least 0.25 ng/mL.
A total of 278 patients were enrolled in the trial and randomized to standard care with or without oral clarithromycin (500 mg tablets every 12 hours for a week). Over 60% of the patient population were men, and all of the patients were white.
Individual components of the primary endpoint all favored the clarithromycin group over controls:
Decreases in respiratory symptom severity scores of at least 50% from baseline: 72% vs 48% (OR 2.83, 95% CI 1.70-4.70)
Decrease of 30% or more in SOFA score: 68% vs 41% (OR 3.10, 95% CI 1.88-5.11)
Favorable change in procalcitonin kinetics: 69% vs 54% (OR 1.86, 95% CI 1.12-3.06)
None of the TEAEs were found to be related to the study treatments. The most common events were septic shock, anemia, and SARS-CoV-2 infection, all of which were numerically more frequent among placebo patients.
As for the trial’s limitations, researchers noted that there was a heavy inflammatory burden among the patients enrolled and that the pathogen was ultimately found in 55% of the patient population, distinguishing ACCESS from other studies.
“Questions undoubtedly remain over the role of macrolides in community-acquired pneumonia,” Waterer wrote. “The threshold of severity for mandatory use is unclear and further studies are needed at lower thresholds, acknowledging that many patients with mild community-acquired pneumonia will have good outcomes regardless of the therapy chosen.”
Molecular “smart tweezers” that can select specific bacteria from a microbiome have been developed by researchers at the Icahn School of Medicine at Mount Sinai. Their technique, mEnrich-seq, exploits the natural signals that bacterial DNA uses to differentiate from each other.
Using this approach, the researchers can distinguish specific bacteria from the many types in a given microbiome. Once bacteria are “plucked out,” researchers can assemble their genomes and study them. The Icahn team’s paper appears in Nature Methods.
“Imagine you’re a scientist who needs to study one particular type of bacteria in a complex environment. It’s like trying to find a needle in a large haystack,” said Gang Fang, PhD, of Icahn’s Genetics and Genomic Sciences department and the study’s senior author. “mEnrich-seq essentially gives researchers a ‘smart tweezer’ to pick up the needle they’re interested in.”
Studies suggest microbiomes play a crucial role in human health. Imbalance of the normal gut microbiota, for example, have been linked with conditions including inflammatory bowel disease, irritable bowel syndrome, obesity, type 2 diabetes, and allergies. Meanwhile, the vaginal microbiome seems to impact sexual and reproductive health.
However, in many microbiome applications, the focus is on studying specific types of bacteria in a sample, rather than looking at each type present. For example, when studying infectious diseases, researchers might only be interested in a few harmful gut bacteria, but these are mixed in with many others.
The mEnrich-seq strategy thus addresses a critical technology gap. Previously, researchers would need to isolate specific bacterial strains from a given sample using culture media for the specific bacterium—a time-consuming process that works for some bacteria, but not others. In contrast, mEnrich-seq can directly recover the genome(s) of bacteria of interest from the microbiome sample without culturing.
Its developers point out that mEnrich-seq offers various opportunities:
A more economical approach to microbiome research, particularly in large-scale studies where resources may be limited.
It can focus on a wide range of bacteria, making it a versatile tool for both research and clinical applications.
By enabling more targeted research, mEnrich-seq could accelerate the development of new diagnostic tools and treatments.
“One of the most exciting aspects of mEnrich-seq is its potential to uncover previously missed details, like antibiotic resistance genes that traditional sequencing methods couldn’t detect due to a lack of sensitivity,” Fang added. “This could be a significant step forward in combating the global issue of antibiotic resistance.”
As one of three applications described in this study, the authors used mEnrich-seq to directly reconstruct pathogenic E. coli genomes from urine samples from patients with urinary tract infections, which allowed the comprehensive analysis of the antibiotic resistance genes in each genome.
In another application, the authors used mEnrich-seq to selectively construct the genomes of Akkermansia muciniphila, a bacterium that has been shown to have benefits in obesity and diabetes, among several other diseases, as well as a response to cancer immunotherapy.
Looking ahead, the team aims to refine the method to improve its efficiency further and to expand its range of applications. Collaborations with clinicians and health care professionals are also in the pipeline to validate the method’s utility in real-world settings.
Researchers are studying how extreme weather and rising temperatures can encourage the spread of drug-resistant infections.
Flooding in Bangladesh in 2020 compromised the safety of water supplies. Credit: Zabed Hasnain Chowdhury/SOPA Images/LightRocket via Getty
In 2021, microbiologist Adwoa Padiki Nartey caught a bacterial infection and her tonsils started to swell. She’d had the same symptoms the year before; both illnesses occurred during one of two annual rainy seasons in Ghana’s capital, Accra, where she lives. In these seasons, she knew, high humidity and moisture spur microbial growth. Doctors prescribed antibiotics but, unlike before, the drugs didn’t work. The bacteria had become resistant.
Over two weeks, her tonsils became increasingly inflamed. “It was painful to drink. Painful to eat. I could barely speak,” says Padiki Nartey, who researches antibiotic resistance at the University of Ghana in Accra. “I was worried.”
To her relief, a final combination of two types of antibiotic worked. Otherwise, the infection could have killed her, she says. “That’s pretty scary.”The fight against antimicrobial resistance
The episode demonstrates how two major threats to human health — climate change and the spread of antibiotic resistance — can intersect. Climate change has led to more frequent heavy rainfall in Ghana, Padiki Nartey says. Those conditions, in turn, encourage bacterial growth, including that of antibiotic-resistant microbes. Flooding also spreads antibiotic-resistant bacteria from sewage systems into people’s homes and drinking water, she adds.
Although researchers have some understanding of how climate change will exacerbate the rise in antibiotic resistance, scientists are now digging into the mechanisms and exploring how large the effect could be, says Pamela Yeh, an evolutionary biologist at the University of California, Los Angeles. “Climate change and antibiotic resistance are two of the biggest health issues of our time,” she says. “Researchers are starting to look at how they link up.”
Climbing resistance
Drug-dodging bacteria are on the rise. In 2020, human blood infections caused by antibiotic-resistant Neisseria gonorrhoea, Escherichia coli and Salmonella bacteria became at least 15% more common than in 2017, according to a report published by the World Health Organization (WHO) in 2022. We are hurtling towards a world where scraping your knee, giving birth or having a simple surgical procedure could kill you, says Yeh. “It’s incredibly frightening,” she says.
The key problem is that antibiotics are often overused or misused to fight infections in people, other animals and plants. Bacteria can develop resistance to drugs through DNA mutations that alter the bacterial cell wall such that antibiotics can’t work, or that confer abilities to break down antibiotics or pump them out of cells. Strains that become resistant can also share antibiotic-resistance genes with other bacteria. If the wrong antibiotics are given to treat infections, or if the right drugs are taken at insufficient doses to kill the microorganisms, then the microbes have more time to multiply and to evolve or spread resistance.
But as in Ghana, changing weather conditions that help bacteria thrive also play a part. And disasters stemming from extreme weather events such as floods, droughts, hurricanes and wildfires can exacerbate the issue because they often reduce access to clean water, leading to unsanitary conditions. When injuries and infections start to rise, more people use antibiotics, in turn pushing up the likelihood of resistance developing.
In a study1 published last October, microbiologist Rita Colwell at the University of Maryland in College Park and her colleagues showed that a deadly hurricane had led to a spike in harmful species of antibiotic-resistant Vibrio bacteria — including a flesh-eating species — in waters off the coast of Florida. The high winds whipped up nutrients from marine sediments that the bacteria thrive on, says Colwell.
Temperature changes
Beyond the physical damage caused by extreme weather, researchers are exploring how rising temperatures that result from climate change might influence antibiotic resistance. In November 2022, microbiologist Lianping Yang at Sun Yat-sen University in Guangzhou, China, and his colleagues reported on the prevalence of three bacteria behind antibiotic-resistant hospital infections that are often severe and can be deadly: Acinetobacter baumannii, Klebsiella pneumoniae and Pseudomonas aeruginosa2.
The researchers looked for links between temperature and antibiotic resistance by comparing bacterial data — collected from people treated in hospitals in 28 provinces and regions across China — with information on average air temperatures in cities in the same regions. The team corrected for factors that could affect rates of drug resistance, including the level of antibiotic consumption, average humidity, yearly rainfall and population density.
They found that, for every 1 °C increase in average air temperature, there was a 14% increase in the proportion of samples containing K. pneumoniae that were resistant to a type of antibiotic called carbapenems. These drugs are usually reserved for treating bacteria that are resistant to all other antibiotics.
Yang and his colleagues also linked a 1 °C increase in average air temperature to a 6% increase in the proportion of samples containing carbapenem-resistant P. aeruginosa. But temperature did not significantly affect the prevalence of drug-resistant A. baumannii.
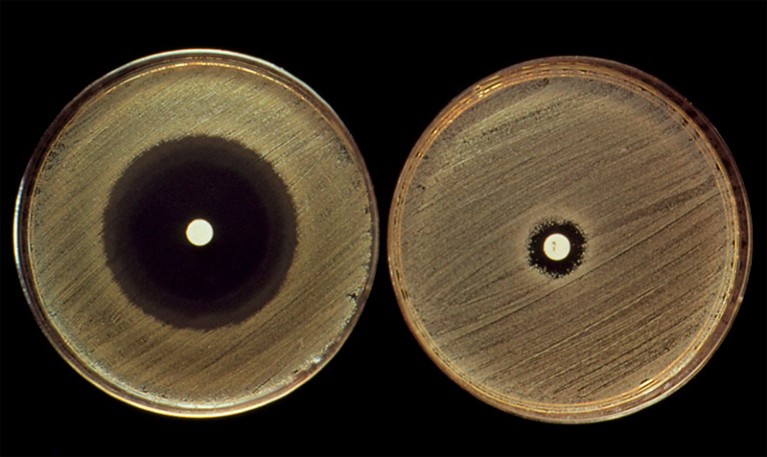
Widely used antibiotics such as penicillin (in white spots) can have very different effects on related bacterial strains (opaque growths).Credit: John Durham/SPL
These findings support studies from 2018 and 2020 by microbiologist Derek MacFadden at the University of Ottawa and his colleagues3,4. The team found that increased average minimum temperatures were linked to higher rates of antibiotic resistance across 41 states in the United States3 and 28 countries in Europe4. However, the studies do not show a causal link between temperature and antibiotic resistance, says Yang.
One way that gradual increases in average air temperature could be driving up antibiotic resistance is by increasing the growth rate of bacteria, speeding up their evolution, says MacFadden. There is also evidence that bacteria can share genes — including elements that confer antibiotic resistance — more easily in warm conditions than in cold ones5.
Extreme conditions
Another idea is that very high temperatures — which are experienced more often as the globe warms, even though average temperatures rise only slightly — might induce genetic changes in bacteria that help them to resist antibiotics, says Yang.
In a 2018 study, Yeh and her colleagues exposed E. coli, which grew best at 41 °C, either to a temperature of 44 °C or to a range of 12 antibiotics (deliberately given at low doses to inhibit but not kill all the bacteria)6. The researchers tracked how the bacteria responded to these stressors, and found that patterns of gene expression changed in similar ways for both temperature and antibiotic type. In both cases, bacteria responded to the stress by producing more ‘heat-shock’ proteins. These help other proteins to fold correctly and apparently also help bacteria to survive antibiotic attack, says Yeh. “We sometimes call antibiotics that mimic [the effects of] hot conditions ‘hot’ drugs,” she says.
When E. coli was exposed to temperatures as low as 22 °C, the microbes ramped up ‘cold-shock’ proteins — again helping them to produce the proteins needed for survival. Some ‘cold’ antibiotics, such as tetracycline, altered bacterial gene activity in a similar way.COP28 climate summit signals the end of fossil fuels — but is it enough?
The findings suggest that bacteria that have evolved in extremely hot or cold conditions might be more resistant to certain antibiotics, Yeh says. But in a study that is yet to be published, Yeh’s team found that exposure to high temperatures sometimes makes bacteria less resistant to ‘hot’ antibiotics, highlighting that the links between temperature and resistance are likely to be complex, she says.
Extreme temperatures could also contribute to antibiotic resistance by changing how people interact with each other, says MacFadden.
In South Korea, “when we reach the highest temperatures, people tend to stay inside”, says microbiologist Soojin Jang at the Pasteur Institute Korea in Seongnam. Bacteria tend to spread particularly easily between people who are in close contact with each other indoors, she says. That could help to spread resistant strains, and — because more bacteria are multiplying in more people — increase the chance that resistance will emerge.
Over the past year, Jang and her team have been tracking the presence of antibiotic-resistance genes in bacterial samples collected from public toilets, trains and buses. The researchers hope to continue this over the next decade and compare rates of antibiotic resistance with factors such as local air temperature and social behaviour. This could help to reveal how climate change is affecting the spread of resistance, says Jang.
Tackling resistance
Surveillance such as Jang’s could be allied with climate and weather data to help track or predict the spread of antibiotic-resistant bacteria, says Colwell. In a study published last February, she and her colleagues used factors including temperature and rainfall data from satellites to predict when and where cholera outbreaks — caused by the waterborne bacteria Vibrio cholerae — would occur7. Their machine-learning model predicted the risk of cholera outbreaks in various regions across Yemen with an average accuracy of 72%, and up to four weeks in advance.
Combining weather data with surveillance for antibiotic-resistance genes by monitoring waste water could improve forecasts for areas that are at a high risk of antibiotic resistance, Colwell says. It’s an approach her team is working on.
Hurricane Ian caused flooding in the streets of Fort Myers, Florida, in 2022.Credit: Pedro Portal/Miami Herald/Tribune News Service via Getty
Besides improving surveillance, researchers already know what’s needed to reduce the spread of antibiotic-resistant bacteria: improving access to clean water and sanitary facilities, and raising awareness of how to use antibiotics appropriately.
Some efforts have been successful. In Lebanon, for instance, clinician and infectious-disease researcher Souha Kanj says a programme that she and her colleagues started at the American University of Beirut in 2018 educated physicians on how to reduce the use of carbapanem antibiotics in their hospital. In 2020, the proportion of A. baumannii infections that were carbapenem-resistant had fallen to 63%, from 81% at the start of the programme8.
Padiki Nartey, meanwhile, is among those trying to develop new ways to kill drug-resistant bacteria. One particularly promising approach is to use viruses called phages, which infect bacteria, but not human cells.
Global action
Researchers seeking to stem the rise of antibiotic resistance could also learn lessons from climate-change politics, says Steven Hoffman, an international lawyer and health-policy researcher at York University in Toronto, who is also at the Public Health Agency of Canada. Such global threats don’t respect national borders, says microbiologist Saffiatou Darboe at the University of the Gambia in Serrekunda. So, drawing parallels with climate change, countries should agree a global treaty to tackle the issue, Hoffman says.
But stronger action is needed, says Hoffman. In a 2022 study9, he and his colleagues called for a treaty to tackle drug-resistant pathogens — equivalent to the 2015 Paris climate agreement. He wants countries to articulate a single unifying goal, such as a 35% reduction in drug-resistant infections by 2035, and hopes that they will make progress on this when they convene at a UN meeting on antimicrobial resistance in September. The meeting is only the second time that the issue has been the subject of a UN General Assembly.
Growth of bacterial cultures in Petri dishes [Sylvia Suter, University Hospital Basel]
Clinical bacteriology relies on the ability to identify cultured isolates. However, unknown isolates are common in hospital settings. Now, researchers at the University of Basel, have established a new study algorithm—NOVA (Novel Organism Verification and Analysis)—to analyze bacterial isolates that cannot otherwise be characterized using conventional identification procedures.
The team, which has been collecting and analyzing patient samples containing unknown bacterial isolates since 2014, have discovered more than thirty new species of bacteria, some of which are associated with clinically relevant infections.
In this work, the researchers led by Daniel Goldenberger, PhD, at the University of Basel, analyzed 61 unknown bacterial pathogens found in blood or tissue samples from patients with a wide range of medical conditions. Conventional laboratory methods, such as mass spectroscopy or sequencing a small part of the bacterial genome, had failed to produce results for all these isolates. Researchers sequenced the complete genome of the bacteria.
Out of 61 analyzed bacteria, 35 represent potentially novel species. And 27 of 35 strains were isolated from deep tissue specimens or blood cultures. The authors noted that, “Corynebacterium sp. (n = 6) and Schaalia sp. (n = 5) were the predominant genera. Two strains each were identified within the genera Anaerococcus, Clostridium, Desulfovibrio, and Peptoniphilus, and one new species was detected within Citrobacter, Dermabacter, Helcococcus, Lancefieldella, Neisseria, Ochrobactrum (Brucella), Paenibacillus, Pantoea, Porphyromonas, Pseudoclavibacter, Pseudomonas, Psychrobacter, Pusillimonas, Rothia, Sneathia, and Tessaracoccus.”
Most of the newly identified species belong to the Corynebacterium and Schaalia genera, both gram-positive bacilli. “Many species in these two genera are found in the natural human skin microbiome and the mucosa. This is why they are frequently underestimated, and research into them is sparse,” explained Goldenberger. They can, however, cause infections when they enter into the bloodstream—due to a tumor, for example.
The researchers classified the remaining 26 strains as hard to identify. An evaluation of the patient data showed that seven out of the 35 new strains were clinically relevant, meaning that they can cause bacterial infections in humans. “Such direct links between newly identified species of bacteria and their clinical relevance have rarely been published in the past,” said Goldenberger.
One of the hard-to-identify pathogens might be clinically relevant, too. It was found in the inflamed thumb of a patient after a dog bite. A Canadian research group also recently isolated this bacterium from wounds caused by dog or cat bites. “This has led us to assume that it is an emerging pathogen which we need to monitor,” said Goldenberger. The Canadian researchers appropriately named the bacterium Vandammella animalimorsus (animal bite Vandammella) in 2022.
Naming their new species is the next item on the Basel team’s to-do list, too. They are working closely with Peter Vandamme, a professor from the University of Ghent and a specialist in bacteria classification. Two of the bacteria have been named already. One is Pseudoclavibacter triregionum—referring to Basel’s location near the borders of Switzerland, France, and Germany.
Researchers report that a new type of antibiotic has proved its mettle against a deadly superbug.
Acinetobacter baumannii, a bacteria that goes by the nickname CRAB when it becomes antibiotic-resistant, can trigger serious infections in the lungs, urinary tract and blood, according to the U.S. Centers for Disease Control and Prevention. Unfortunately, it’s resistant to a class of powerful broad-spectrum antibiotics called carbapenems.
Now, in a study published Jan. 3 in the journal Nature, researchers from Harvard University and the pharmaceutical company Hoffmann-La Roche discovered that a new type of antibiotic, zosurabalpin, can kill A. baumannii.
Zosurabalpin employs a unique method of action, researcher Dr. Kenneth Bradley, global head of infectious disease discovery with Roche Pharma Research and Early Development, told CNN.
“This is a novel approach, both in terms of the compound itself but as well as the mechanism by which it kills bacteria,” he explained. A. baumannii is a Gram-negative bacteria, meaning it is protected by both inner and outer membranes, making it difficult to attack.
In this study, the scientists first tried to identify and then fine-tune a molecule that could cross those double membranes and eliminate the bacteria.
After years of improving the potency and safety of a number of compounds, the researchers chose one modified molecule.
How does it work? Zosurabalpin prevents the movement of large molecules called lipopolysaccharides to the outer membrane of the bacteria, where they keep the protective membrane intact. This causes the molecules to accumulate inside the bacteria’s cell to the point where the cell becomes so toxic that it dies.
In the study, zosurabalpin worked against more than 100 CRAB samples. It also reduced the levels of bacteria in mice with CRAB-induced pneumonia and prevented the death of mice with sepsis triggered by the bacteria.
Zosurabalpin is now being tested in phase 1 clinical trials, to assess its safety in humans, the researchers told CNN.
Still, the public health threat of antimicrobial resistance remains a huge problem globally due to a lack of effective treatments, Dr. Michael Lobritz, worldwide leader of infectious diseases at Roche Pharma Research and Early Development, told CNN.
In the United States, there are more than 2.8 million antimicrobial-resistant infections each year. More than 35,000 people die as a result, according to the CDC’s 2019 Antibiotic Resistance Threats Report.
Even though zosurabalpin is years away from human use, it’s an extremely promising development, Dr. César de la Fuente, presidential assistant professor at the University of Pennsylvania, told CNN.
“I think from an academic perspective, it is exciting to see a new type of molecule that kills bacteria in a different way,” de la Fuente said. “We certainly need new out-of-the-box ways of thinking about antibiotic discovery, and I think this is a good example of that.”
The only drawback to the discovery is that the modified molecule will work only against the specific bacteria it is designed to kill, the researchers noted.
However, de la Fuente said this new method could turn out to be better than many broad-spectrum antibiotics.
“For decades, we’ve been obsessed with creating or discovering broad-spectrum antibiotics that kill everything,” he noted. “Why not try to come up with specific, more targeted antibiotics that only target the pathogen that is causing the infection and not all the other things that might be good for us?”









 By Robin Foster HealthDay Reporter
By Robin Foster HealthDay Reporter
{kind=link}
{kind=link}