Dr. Tsang suggests that diabetic patients should take sufficient vitamins B1, B6, and B12.
Diabetes was the seventh leading cause of death in the United States in 2019, based on 87,647 death certificates in which diabetes was listed as the underlying cause of death, according to the American Diabetes Association. In 2019, 37.3 million Americans, or 11.3 percent of the population, had diabetes.
The latest survey by the International Diabetes Federation found that 1 in 4 diabetic patients interviewed reported that they didn’t receive adequate information on the disease. As a result, many patients failed to care for complications properly, which seriously hindered their daily lives.
Diabetes Causes Peripheral Neuropathy
Diabetic patients are often unaware of the relationship between peripheral neuropathy and diabetes. Hence, they may misinterpret sensations of physical paralysis as part of aging. Since symptoms of diabetes are not always apparent in the early phases, by the time some patients seek medical treatment, the disease may have progressed substantially.
Endocrine and diabetes specialist practitioner Dr. Tsang Man-wo at United Christian Hospital points out that diabetes is the most common cause of peripheral neuropathy. The nerve fibers in the surrounding nervous system are damaged, causing peripheral nerve injuries or microvascular dysfunction due to elevated blood sugar levels.
Peripheral neuropathy can lead to multiple health risks, including sensory loss, muscle atrophy, and shakiness, increasing the risk of injury and making everyday activities a challenge. Diabetic patients are prone to other severe health conditions, such as skin ulcers and diabetes mellitus-induced foot amputation.
How to Prevent Peripheral Neuropathy?
Tsang suggests that the best way to prevent lesions or further deterioration by diabetes is to control blood sugar levels. In addition to blood sugar control, patients should maintain normal blood pressure and cholesterol levels, avoid smoking and consuming alcohol, and exercise regularly.
Moreover, patients should take sufficient vitamins B1, B6, and B12 to more effectively maintain the health of blood vessels and nervous systems.
Vitamin B1 deficiency affects the heart and feet, damages nerves, and likely causes beriberi, also known as thiamine deficiency. The lack of vitamin B6 affects the blood, brain, and signaling transduction of the nervous system. Vitamin B12 deficiency impacts the blood and nervous system regeneration, or worse, causes scurvy, malignant anemia, sensory loss, and dementia.
Metformin is a common drug for treating diabetes. However, high dosage and prolonged use, especially for three years or more, may affect vitamin B12 absorption in the intestines, resulting in peripheral neuralgia.
Tsang says that by increasing the intake of B vitamins, such as B1, B6, and B12, specifically for the nervous system, the symptoms of peripheral neuropathy can be relieved and prevented.
The doctor suggests that whenever patients encounter numbness in the limbs, particularly diabetics, they shouldn’t overlook the possibility of peripheral neuropathy and mistake it for arthritis or sciatica.
If we didn’t learn to manage our emotions when we were children, we will need to learn as adults
(Brittany Risher/Shutterstock)
At the office, your co-worker is always mumbling at their computer screen. At home, your partner left his socks on the floor—again. And now, one of your children has decided to take up singing off-key renditions of songs from “Frozen” as their new favorite activity.
These kinds of situations happen every day, and if you’re feeling irritated by them, you’re not alone.
With the ongoing global health crisis, many of us have been left feeling frustrated, overwhelmed, and irritated due to the absence of clear information and to doubts concerning vaccine requirements. The ongoing experience of these feelings can wreak havoc on our well-being.
Irritability and Its Common Signs
People might feel fine in one moment, but a small annoyance might set their feelings off in a different direction the next—creating a more sensitive response to stress.
Some common signs of irritability include:
Agitation, frustration, and annoyance
Confusion and difficulty concentrating
Difficulty making accommodations or changing plans
Excessive sweating
Fatigue
Increased breathing rate
Rapid heartbeat
Oversensitivity
Short temper
Tension
Irritability is often described as a trait. That differs from anger, which is an affective state, and from reactive aggression, which is a behavior.
Irritability is defined as being prone to anger. A series of recent studies explored the relationship between irritability and depression.
In 1917, Sigmund Freud, in one of his most important clinical works, “Mourning and Melancholia,” described melancholia as involving “self-directed hostility originally directed toward others,” underlying what he described as “the undoubtedly pleasurable self-torture of melancholy.”
Are Irritability and Anger Bad?
Many may ask, “Are irritability or anger bad emotions?” Modern psychologists would say “not necessarily.” Why? Scientists would say that anger is a natural, adaptive response to threats.
It inspires powerful aggressive feelings and behaviors to fight and defend oneself when one is attacked. One could say that a certain amount of anger is essential to survival.
Diseases Can Cause Irritability
Most people feel irritable from time to time. Some people feel irritable on a more regular basis.
It’s important to identify the source of irritability.
The extent to which physical things can cause psychological issues is often underestimated. In some cases, physical disease can cause irritability or anger as a side effect.
Several common psychological causes of irritability include stress, anxiety, and autism. Some mental health disorders have been associated with irritability, including, but not limited to, depression, bipolar disorder, and schizophrenia.
Not only can physical and psychological discomfort cause irritability or anger, but the constant flood of stress chemicals and associated metabolic changes that go with ongoing unmanaged anger can eventually cause harm to health, too.
Factors of Irritability: Why Are Some More Easily Irritated Than Others?
According to Dr. Jerry Deffenbacher, a psychologist who specializes in anger management, people who are easily irritated may have a lower tolerance for frustration, inconvenience, or annoyance.
Recent studies suggest that both genetic and environmental factors play a significant role in determining a person’s trait level of irritability.
The association between irritability and depression is somewhat explained by shared risk factors such as genetics, family history of depression, shared temperamental and personality characteristics, negative parenting styles, and socioeconomic factors.
Why Is Emotional Regulation So Important?
Knowing the cause, however, doesn’t mean that it’s OK to lash out at every person or object that’s irritating or annoying. In an article in Psychology Today, Dr. Gregg Henriques, a professor of psychology at James Madison University, describes all basic emotions as being adaptive or maladaptive.
Henriques made his viewpoint clear by quoting from Aristotle’s “Nicomachean Ethics”: “Anybody can become angry, that is easy; but to be angry with the right person, and to the right degree, and at the right time, and for the right purpose, and in the right way—that is not within everybody’s power; that is not easy.”
“Negative emotions,” according to Henriques, “are maladaptive if they are under-regulated, chronically accessible, have low thresholds, and lead to problematic behaviors that increase suffering and impairment.”
We can’t avoid being irritated, nor can we change others, but we can always learn to regulate or control our reactions. It’s a skill to be able to regulate emotions, which takes time to learn and improves with practice.
The benefits of emotional regulation come through acting assertively without being aggressive and can help one maintain healthy, peaceful relationships.
Emotions can be regulated through problem-solving, asserting oneself, and reappraisal of a situation, leading to mood improvement and better health, and, in the long run, can increase compassion and empathy for others.
Can Emotional Regulation Be Learned?
There are several good methods to learn how to regulate emotion.
The National Mental Health Association suggests that the three main approaches to regulating emotions are through expressing feelings, suppressing anger, and calming oneself. The healthiest way to express angry feelings is in an assertive, nonaggressive manner.
“To do this, you have to learn how to make clear what your needs are, and how to get them met, without hurting others. Being assertive doesn’t mean being pushy or demanding—it means being respectful of yourself and others.” the National Mental Health Association states.
Suppressing and redirecting anger, and calming oneself down, controls outward behavior as well as internal responses, helping to lower heart rate and regain calmness.
Tips for Practicing Emotional Regulation
Emotional regulation is one of the early skills learned as children, often from one’s family. And if those skills weren’t learned in youth, it’s never too late to start.
Try these techniques when feelings of anger arise:
Take a break: If you find yourself frustrated at work, or in a stressful environment, try taking a timeout or simply walk away from the situation for a few minutes.
Practice relaxation techniques: Relaxation is a skill that you can learn over time. When you recognize the early signs of irritation or tension, try some relaxation techniques to help improve your mood. Some techniques include breathing deeply from your diaphragm or repeating a calming word or phrase such as “relax” or “take it easy.”
Meditation or mindfulness practices can help you maintain calmness throughout your day. You might try the ancient technique of daily meditation or learn some breathing techniques and self-awareness strategies.
Reframe your thoughts: When you catch yourself dwelling on the unfairness of a situation or thinking about how much you dislike something, try to reframe it. Shifting negative thoughts to positive ones and your perception of a situation to an unbiased one may help you to feel less angry.
Share your thoughts and feelings. Talking with your family or other support systems may help you clarify problems, gain good advice, help provide different perspectives, and strengthen your relationships by building more effective communication skills.
Meditation and Self Regulation
Meditation has been scientifically proven to help reduce depression and addiction, enhance concentration and immune function, lower blood pressure, and suppress anxiety and insomnia.
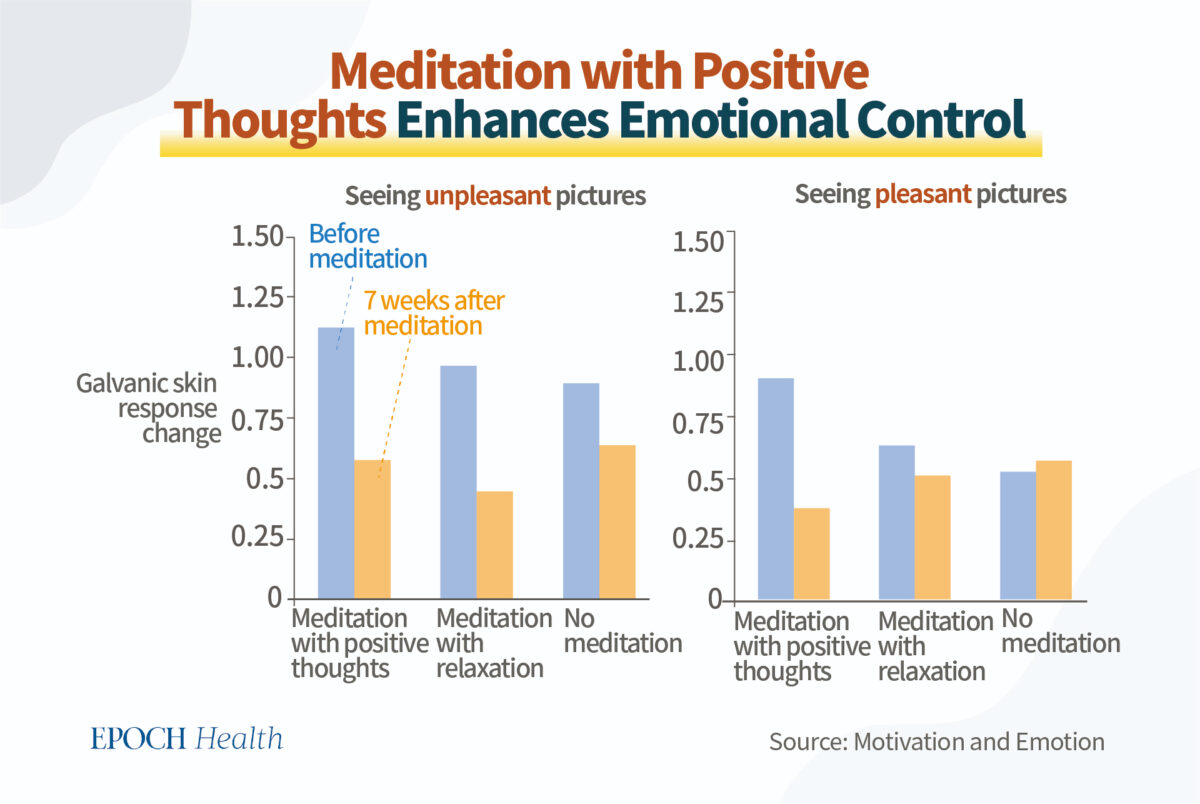
Scholars from the University of Minnesota and the University of Toronto in Canada published a study in the journal Motivation and Emotion.
The subjects were divided into three groups: meditation with positive thoughts, meditation with relaxation, and no meditation at all.
After seven weeks, it was found that both groups of meditators experienced a significant decrease in emotional fluctuations, with those who meditated with positive thoughts experiencing even greater emotional control.
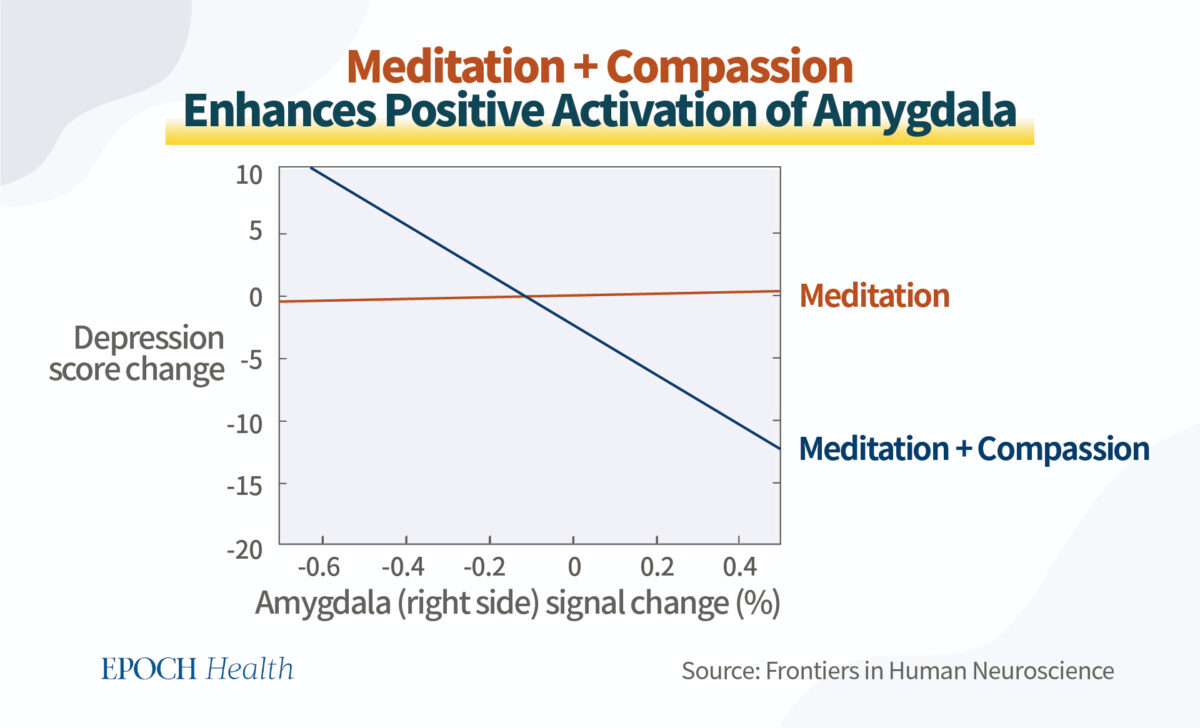
Emory University conducted a study showing that participants who added compassion to meditation had significantly lower depression scores and increased positive activation of the amygdala, a cluster of neurons that generates and regulates emotions.
The Effects of Gratitude, Positive Thinking, and Communication
According to Dr. Adam Borland, a psychologist practicing at the Center for Adult Behavioral Health at Cleveland Clinic, when it comes to emotional health, “it really comes down to gratitude.”
“It’s so easy to overlook the good things and focus on the bad things. Instead, take a step back and think, ‘What do I appreciate in this moment?’” he said.
Positive thinking and effective communication skills can also have a significant effect. Beyond easing irritation and improving emotional regulation, these abilities can improve overall work performance. And in learning to make intentional, sound decisions, our overall experience of life can improve as well.
Life will continue to have its hardships, disappointments, and losses, and the behaviors of others may still be unpredictable, but we can alter our thought processes and reactions to create a more mindful life. Our mind and body are connected, and through these practices, we can enhance our immunity to viruses and develop a better capacity to remain healthy during this pandemic.
Endogenous retroviruses account for up to 8 percent of human DNA.
The concept that microbes such as those in the gut and skin contribute to human health is not new. In fact, scientists have also discovered that hundreds of thousands of DNA fragments in the human body are derived from viruses; these fragments were embedded in the human body long ago and passed down from generation to generation; and these DNA fragments and the viruses from which they are derived are known as “endogenous retroviruses”.
What do these viral DNA do to the human body? It was not until recent years that people discovered that these foreign genetic materials may also play a role in boosting human immunity.
Yuanyu Jeng, a former attending physician at the Department of Infectious Disease of Taipei Veterans General Hospital, explained this topic in detail.
A Study in the Science Journal: Fragments of Viral DNA Protect Against Viral Infection
A study published in Science in October 2022 pointed out that a protein called Suppressyn can protect human cells from RD114 virus infection.
Suppressyn can be produced by the human body itself, but scientists have found through in-depth analysis that the DNA that produces Suppressyn in the human body was introduced by a virus. They believe that the process of virus invasion occurred in our ancestors. The virus can be passed from generation to generation since it infects germ cells, to begin with. So today, humans generally possess this viral gene.
Therefore, everyone is born with viral genes inherited from their ancestors. Studies have now found that about 8 percent of the genetic information in human DNA is composed of endogenous retroviruses.
How Does Retroviral Invasion Alter Cellular DNA?
The human body can produce ribonucleic acid (RNA) with reference to the genetic information of DNA, thereby producing the essential substance that constitutes the human body—proteins. “Transcription” refers to the process by which the human body makes RNA with reference to DNA.
Naturally, the DNA of the human body needs to be protected, so scientists used to believe that the process of transcribing DNA into RNA is unidirectional and irreversible.
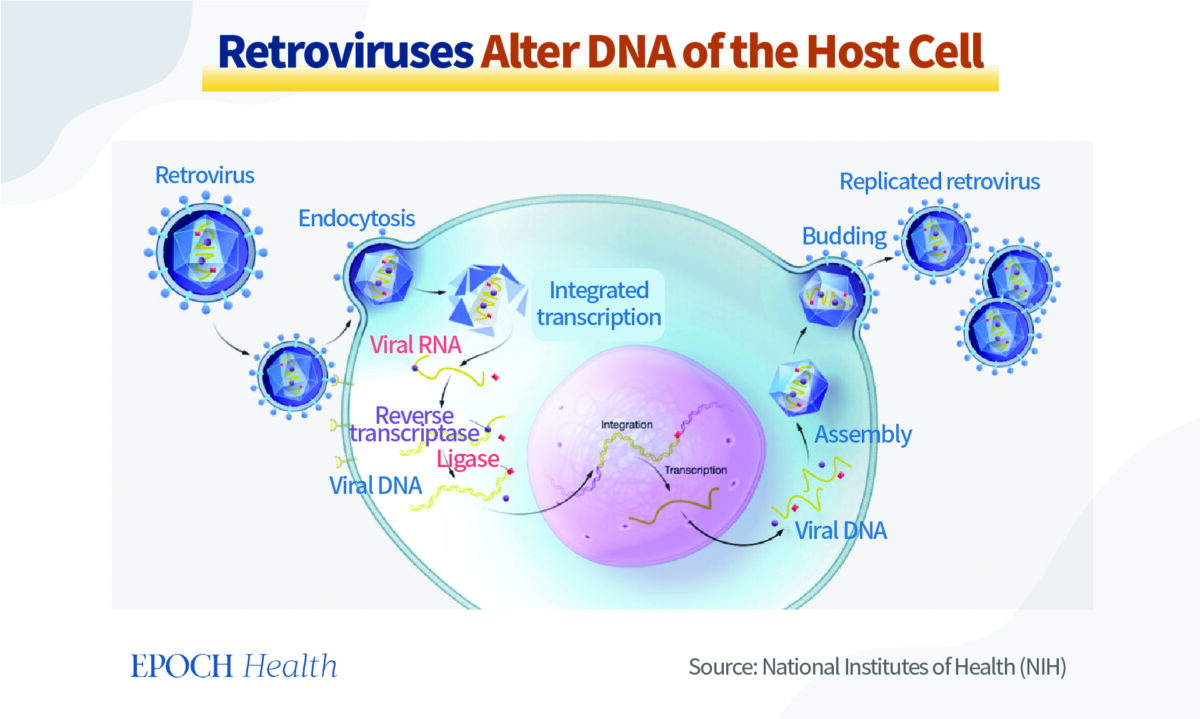
However, scientists were taken by surprise by the discovery of “retroviruses”, as these viruses can use human cells with reference to their own RNA, make DNA fragments with viruses, and place them in the DNA of cells. In other words, it is possible for the DNA in the cells of an organism to be invaded and altered.
Simply put, retroviruses can insert their own genetic information into the DNA of human cells, thereby changing their DNA.
The HIV virus that causes AIDS and the hepatitis B virus that causes hepatitis are common retroviruses.
Can Viruses That Alter Human DNA Turn People Into ‘Mutants’?
After the human DNA is altered, will people be transformed into “mutants”, “cyborgs” or “zombies” as seen in movies?
Of course not.
For example, the hepatitis B virus only alters liver cells, while HIV targets helper T cells. The DNA of other cells in the body is not altered. In other words, the DNA of the patient’s offspring will not be affected by the viruses.
However, if a retrovirus infects germ cells, such as spermatogonia or oogonia, and alters their DNA, the alterations can be passed on to the patient’s offspring and then passed down from generation to generation.
Thus, all of us are born with viral DNA that we inherited from our ancestors who were infected with the virus. They are named “endogenous” retroviruses, as the DNA information of these viruses is “naturally” present in our bodies.
Tracing back to the origin, the endogenous retroviral fragments in human DNA were acquired from external infection by our ancestors. Other animals, including pigs, monkeys, and orangutans, also contain endogenous retrovirus information in their DNA.
Can Viral Genes Inherited From Our Ancestors Still Cause Infection?
When it was first discovered that there were fragments of foreign viruses in human DNA, scientists thought that they might just be “fossils” left over from ancient viruses and were non-functional. Basically, humans or other animals survive after overcoming these viral infections, but they cannot get rid of the foreign DNA, so they remain in the DNA like “residues”.
Human endogenous retroviruses have not been found to be pathogenic or infectious, but it has been confirmed that human cells can produce a viral entity called human endogenous retrovirus K.
Although this is the only complete virus discovered so far, endogenous retroviruses actually account for up to 8 percent of human DNA; other parts of retroviruses, such as RNA fragments and protein particles, can also be made from human cells.
Looking at it from another perspective, in the process of entering human cells and passing on from generation to generation, some of the DNA of these viruses have become incomplete, some have become inactive, and some are even beneficial to humans.
Endogenous Retroviruses Have Both Good and Bad Effects on the Human Body
As an example, the body produces a protein called syncytin that stabilizes the placental structure. Without syncytin, pregnant women will experience placenta-related conditions and diseases, such as miscarriage, fetal growth restriction, and preeclampsia.
Studies have found that the gene that encodes syncytin is brought by an endogenous retrovirus, and syncytin has been a crucial stability factor for human reproduction.
However, some diseases, including multiple sclerosis, schizophrenia, and bipolar disorder, may be associated with syncytin abnormalities in the nervous system.
Studies also found that some other endogenous retroviral components may also be related to autoimmune diseases, including Type 1 diabetes and rheumatoid arthritis.
It is conceivable that the viral genes inherited by human beings were originally “invaders” to our ancestors. After being passed down from generation to generation, the immune system gradually tolerates the existence of these genes.
Then, is it possible for the immune system to regard these viral genes as foreign “invaders” and launch an attack, thereby causing autoimmune diseases? In this regard, current studies have found a preliminary association.
However, just like the principle of “mutual promotion and mutual restraint” taught by Taoism, there are always pros and cons to everything.
If the downside of a viral gene embedded in human DNA is autoimmune diseases, what is the upside? Well, it allows the immune system to respond earlier by simulating an environment in the body similar to a viral invasion.
Endogenous Retroviruses Use Ordinary Cells to Fight Viruses
Speaking of the benefits of endogenous retroviral genes to the human body, the aforementioned Science study has found that a protein derived from endogenous retroviral genes, Suppressyn, has antiviral properties.
The study also found that placental and embryonic stem cells have high levels of Suppressyn gene expression, which makes the Suppressyn protein. In other words, the human body already has the ability to fight against viruses when it is still in the embryonic stage, which was never thought of in the past.
So, how does Suppressyn fight viral infections?
The RD114 virus detected by the researchers is a common virus in feline species, such as domestic cats. The virus can bind to the ASCT2 receptor on the surface of human cells and infect the cells. Suppressyn can interfere with the binding process of RD114 virus and ASCT2 receptor, thus preventing the virus from infecting the cells.
Of course, Suppressyn’s antiviral properties are just an example. There are more than 100,000 DNA fragments of endogenous retroviruses in the human body, and they help the immune system to fight against viruses in more than one way.
For instance, virus invasion will stimulate the body to produce antibodies with high binding capacity. It is one of the functions of the acquired immune system.
Why is it called “acquired” immunity? This is because when the human body is exposed to a pathogen, the immune system needs to identify the characteristics of the pathogen before it can make antibodies through “acquired learning”. Hence, it takes time for the human body to make antibodies, and antibodies can only fight against one specific target.
However, after the virus invades the human body, it also produces a substance called double-stranded RNA, which can trigger and activate the innate immune system and enhance antiviral capabilities. The innate immune response has a broad effect as the process does not require the identification of specific characteristics of the virus. Innate immunity can quickly fight viral infections when acquired immunity fails.
Studies found that some cells will activate the endogenous retroviral genes, express double-stranded RNA, and call on the immune system to make a stronger response when foreign viruses invade. Such findings were seen in cell experiments with influenza A.
The endogenous retroviruses of human DNA also have other ways of fighting viruses, such as the “receptor interference” described below.
There are many complex steps in the process by which a virus invades a cell, replicates in large numbers, and then leaves the cell. Human cells can use the endogenous retroviral genes to produce a variety of virus-like components that can occupy the positions where viruses need to bind, such as the cellular entry receptors or the exit pathways. There are also components that can interfere with viral activity, such as the process of viral replication.
In fact, every cell in the human body has a complete set of DNA information, including DNA fragments of all endogenous retroviruses. In theory, many cells in the body have the potential to utilize these viral DNAs. This is equivalent to launching an “all-out anti-virus defense” with ordinary cells of the human body, instead of relying only on immune cells.
Endogenous Retroviruses May Be Useful in Detecting Cancer
Fragments of endogenous retroviruses in human DNA may have another application.
It has been found that cancer cells are particularly prone to activating the expression of these endogenous retroviral genes. It is uncertain whether the cells deteriorate and become cancerous because these genes are activated abnormally, or whether the cancer cells have these genes activated.
In any case, there is one more identifiable difference between cancer cells and normal cells that we may be able to utilize. This is because the expression products of these genes are ancient viral components, and on the basis of existing cancer immunotherapy, they can induce the immune system to target the endogenous retroviral genes that are activated in cancer cells. It is a promising approach to cancer treatment.
It’ll help you determine if a packaged food is healthy in less than 30 seconds. (Dreamstime/TNS)
Confused about what to look for on food labels? You’re not alone. In the past, the common starting places were often calories and total fat. Yet, those two values reveal very little about a food’s nutrient content and overall health value.
So, to get some insight on where to start, we polled more than 20 dietitians and asked them what they look at first on a label when grocery shopping. Surprisingly, the responses tended to be one of two things.
The Ingredient List
The overwhelming response isn’t a number, but rather the ingredient list. Bailee Hart, RD, shares that she’s looking for “a fairly short list of natural, whole-food and recognizable ingredients.” She also doesn’t waste time: “If there’s a long list of unrecognizable ingredients, I put it back before looking any further at the label.”
I got similar feedback from other dietitians, like Jennifer Hunt, RDN, LD, who shared that, while it may not be true for every food, “most often the quality of the ingredients trumps the macros and nutrients when I am checking out a product.”
What else are dietitians looking for in that list?
— The number of ingredients.“The fewer the better,” says Diane Norwood, M.S., RD, CDE, advice that I also received from many others. — The order of ingredients. Manufacturers are required to list ingredients in order of weight going from highest to lowest. Leanne Ray, M.S., RDN, says looking at where ingredients fall in the list “is a great way to get a quick sense of what makes up the bulk of a recipe.” — Added sugars. If it’s a sweetened food, then it’s important to identify the added sugar. The closer the added sugars are to the end of the list, the better, since those ingredients are in descending order. Looking for added sugars in foods that aren’t usually sweet (like pasta sauce or bread) can be a good way to decide between two similar products at the store.
The Fiber Content
If the ingredient list wasn’t the first thing dietitians said they looked at, then it was fiber. This makes sense, since most people don’t get enough fiber on a daily basis. But this is also because fiber content is often a good indicator of a food’s quality.
“Fiber content is a quick and easy way for consumers to get a clue to the nutrient density of a food,” explains chef and dietitian Michele Redmond, M.S., RDN, FAND. Redmond adds that looking at fiber amounts for carb-based foods “can help one to decide which food products offer the complex, slower-metabolizing carbohydrates associated with heart health, satiety, a healthy microbiome and other benefits.”
What else should you look for on a nutrition label?
Checking out the ingredient list and fiber content can take a lot of guesswork out of trying to choose healthier items, but where do you go from there? “Priorities for label reading really depend on health concerns,” says Bridget Swinney, M.S., RD. Carbohydrates may be the focus for those with diabetes, while sodium may be more important for those with high blood pressure. Also, a key element on that label to remember is serving size. As Jill Weisenberger, M.S., RDN, CDE, author of Prediabetes: A Complete Guide, points out, “Everything else on the Nutrition Facts panel is based on that.”
It’s one of the leading causes of disability, lost wages, and lowered productivity. It’s estimated that 8 out of 10 of us will experience it at least once in our lifetime. It’s chronic low back pain — and understanding the possible back pain causes, risk factors, and treatment options is essential for ensuring your spine stays as healthy as possible as you age.
What are the symptoms of chronic back pain, why is this broad health condition so common, and what can be done about it? Let’s look at the current research.
Majority of Factors Leading to Chronic Low Back Pain Are Preventable, Lifestyle-Related, According to Experts
Back pain symptoms include dull, throbbing, achy, and/or stiff pain anywhere in the spine, but usually in the lower back. If the underlying cause of your back pain — such as disc herniation, disc bulge, or spinal stenosis — involves compression of a nerve as it leaves the spinal column, then additional symptoms in the leg or arm can develop, too, including weakness, numbness, pain, and tingling.
No matter what specific back diagnosis you may have, here are the most common risk factors for developing it:
Advancing age (men between the ages of 30 and 50 are particularly at risk)
Genetics
Fitness level (you guessed it — less physically fit people and “weekend warriors” are more likely to have back pain)
Weight gain
Occupational factors, such as frequent heavy lifting, bending, pulling, pushing or even sitting
Stress, anxiety, and depression
Smoking
As for kids, heavy and improperly carried backpacks are the leading culprit.
Now, notice that except for the first two, all these risk factors are modifiable. This means keeping your spine healthy is largely within your control.
When It Comes to Low Back Pain, Conventional Medicine Often Falls Short — Here’s What the Research Recommends Instead
It didn’t surprise anyone when a new study in the British Journal of Sports Medicine concluded that physical inactivity is linked with an increased risk of severe COVID-19. But what happens if your back hurts so much that you can barely tolerate standing for longer than 5 to 10 minutes?
Unfortunately, many people assume that when they have chronic symptoms of low back pain, the only way out is to eventually go under the knife or take daily trips to the medicine cabinet. The problem is, these conventional approaches to chronic back pain aren’t always as effective as one would hope.
Take this, for example:
Recent reviews, including a 2016 paper in the Journal of Pain Research and a 2018 review in the Asian Spine Journal conclude that spinal surgery — including discectomies, decompression, and fusions — sometimes “fails to provide relief or provides only temporary relief of the patient’s pain.” In fact, this is so common that it’s earned its own clinically recognized name: failed back surgery syndrome (FBSS).
According to some data, nearly 1 in 3 spinal surgery patients have the same amount of pain — or even worse pain — 12 months after lumbar surgery. Overall, spinal surgery boasts about a 50 percent “success rate,” and revision surgeries fare even worse. Only about 30 percent, 15 percent, and 5 percent of people who undergo second, third, or fourth surgeries have “successful” outcomes.
And while medications may be helpful in some cases — especially in acute back pain or back pain related to cancer — the risks of long-term use of medication often outweigh the potential benefits. In fact, The U.S. Centers for Disease Control and Prevention (CDC) advises non-drug options as the first line of treatment for chronic pain conditions like back pain, according to the American Physical Therapy Association.
So, what might your drug-free, surgery-free back pain solution look like? Here are the top research-backed recommendations for treating and preventing this common condition:
Weight loss
Exercise (including aerobic, resistance, and aquatic activities)
Physical therapy
Cognitive-behavioral therapy and pain education
Alternative therapies, and especially acupuncture — which is proven to be at least “moderately” effective for chronic low back pain
The most important thing to do when you have chronic back pain? Stay active. Bedrest “is not recommended,” according to the National Institute of Neurological Disorders and Stroke.
Finally, an unbiased pathologist has taken a vaccine into the lab to demonstrate exactly what’s causing ‘the mystery of the rubbery clots.’
STORY AT-A-GLANCE
A recent laboratory investigation by The Highwire reveals the only consistent thing about the COVID shots are their inconsistency. There is no quality control. Some appear clear like saline, while others are loaded with contaminants
In August 2021, Japan rejected 1.63 million doses of Moderna’s mRNA shot due to contamination. Last year the European Medicines Agency (EMA) also expressed concern over vials that were only 50% to 55% pure
The vials also contain massively inconsistent amounts of polyethylene glycol (PEG). PEG can cause anaphylactic shock in some people. PEG also gets in the way of proper immune response
If you are unfortunate enough to get a vial that is loaded with PEG, your risk of adverse effects such as anaphylactic shock and dysregulated immune response is greater than if you get a vial with lower amounts
According to Dr. Ryan Cole, a pathologist, what looks like microchips or nanotechnology in the liquid are actually stacked cholesterol, sugar and salt crystals, and what has been described as parasites are stellate trikons, found on the bottom of leaves. They’re likely a contaminant picked up at some point during the lab investigation
December 12, 2022, The Highwire posted1 a fascinating and shocking lab investigation of the COVID shots. Del Bigtree begins by reviewing some of the many alleged findings by organizations looking at the shots using various technologies. For example, some claim to have found graphite in the vials, while others have discovered what looks like nanotechnology and parasites.
“Some of these we’ve addressed here and others we haven’t,” Bigtree says. “Part of it is I really don’t like addressing something that I don’t know where the information is coming from …
I do not trust experts just because they tell me they’re an expert. I want to see the science, I want to see the evidence, I want to see how it’s done … So, I reached out to Dr. Ryan Cole, a pathologist who has proved to me that he’s impeccable in the work that he does. He’s unbiased.
And I said, ‘Would you do me a favor? Can we get a hold of these vaccines? I want to come into the laboratory. I want to see it with my own eyes. Can we bring some cameras in and do a real investigation?’”
The Mystery of the Rubbery Clots
Cole agreed, and that taped investigation is what you see in the video above. Cole begins by showing what some of the white rubbery clots look like under the microscope, and slides showing the distribution of spike protein in various tissues.
A number of embalmers have reported pulling these stringy, stretchy objects out of deceased people who got the jab, and they’re different from anything they’ve ever seen before. Cole agrees that these clots are something brand-new.
Cole describes the white elastic clots as “an amyloid-type of material” induced by the spike protein, which is actually a glycoprotein. He cites a paper2 from August 2021 by Etheresia Pretorius and her team, in which she describes finding “persistent circulating plasma microclots that are resistant to fibrinolysis” in long-COVID patients and those who have received the COVID jab.
She refers to them as “anomalous amyloid microclots.” In summary, what she discovered was that even when she took the platelets out of the blood, once she added spike protein, the proteins still glommed together, forming masses, and processes that would normally break down a blood clot do not work on these amyloid-like depositions.
COVID Injections Under the Microscope
Cole then moves on to look at the COVID shots under a microscope. The first one is the Janssen shot, which has what looks like debris in it, including, potentially, a shard of glass. As noted by Cole, when manufacturing is ramped up to the current speeds at which these shots are produced, there’s really no purity guarantee.
As you may recall, in August 2021, Japan rejected 1.63 million doses of Moderna’s mRNA shot due to contamination. Last year the European Medicines Agency (EMA) also expressed concern over vials that were only 50% to 55% pure.
This impurity also means that you may be getting fragmented RNA, as opposed to complete RNA, which can have unforeseen consequences, as shortened RNA can end up producing incomplete proteins. Of the Pfizer vials, some also contained unidentifiable particles, some of which were stuck together.
That said, where others see nanotechnology — square objects that resemble microchips — Cole sees stacked cholesterol. So, while there’s debris (which is bad enough) he does not ascribe to theories that the shots include nanotech.
Some have also discovered what looks like parasites but, according to Cole, they are stellate trikons, found on the bottom of leaves. He suggests it’s an impurity that landed in the liquid or on the glass during the process of investigation. Bigtree summarized their findings:
“Generally speaking, as we looked at all the different vaccines, one of the conclusions that we came away with is, it’s just a hodgepodge. There were vaccines that seemed like they had no particles, almost nothing, there; almost like a saline shot. And then the [next] one would be just packed with all sorts of things. You just get this sense that the manufacturing is totally and completely inconsistent.”
Cole agreed:
“I agree 100%. Some are more concentrated, some were less, and that goes to the point, where are these being made? Is the FDA inspecting each facility? No. And these are being made around the world, and they were ramped up so quickly. It’s not good manufacturing process … And … this is a very unique, brand-new process which they’re using at a mass scale.”
COVID Shots Analyzed With Mass Spectronomy
The shots were also analyzed using mass spectronomy, which revealed the presence of metallic particles, including aluminum, silicon, magnesium, sodium chloride, calcium, titanium and iron. Cole cites research showing that some of these metals come from the needle used to extract the liquid from the vial, so they may or may not be part of the actual formula in the vial.
They also found massively inconsistent amounts of polyethylene glycol (PEG) in the different vials. PEG, which is what coats and protects the mRNA, is what causes anaphylactic shock in some people, as PEG sensitivity and allergies are common among the general public. Worse, however, is the fact that PEG also gets in the way of proper immune response.
“Poor, inconsistent manufacturing processes are resulting in wildly varying contents from one batch or vial to another.”
If you are unfortunate enough to get a vial that is loaded with PEG, your risk of adverse effects such as anaphylactic shock and dysregulated immune response is greater than if you get a vial with the appropriate amount, or less than what the recipe calls for. Again, it’s a sign of poor, inconsistent manufacturing processes resulting in wildly varying contents from one batch or vial to another. Notably, no graphene was found in any of the 100 vials tested. Cole explains:
“Those little flakes that we were seeing, those little lines and floating things, those are three things: cholesterol crystals — there’s a cholesterol cholesterin spike on some of these mass spec graphs — … salt and some sugars … So, at the end of the day, the mass spec showed that’s what it was.
These vials have lipid content. They have polyethylene glycol content in varying ratios. They have salts, they have sugars. They do have genetic material … and some lots had some contaminants …
There’s lipid nanoparticle and a gene sequence that makes your body make a foreign protein. Those two things are necessary and sufficient to cause harm. Sure, you want a pure product, but those are the two harmful things. The lipid nanoparticle is hyper-inflammatory and can be toxic.
When it was designed, it was made to be given once. Studies on giving it two, three, four times aren’t there in humans. So, the cumulative toxicity of the nanoparticle itself is concerning.
Even more concerning is [that] the more of this gene you get into your cells that continues to make a protein that has known countless side effects … that toxic spike protein. That’s what matters.”
The Show-Stopper
The real show-stopper is toward the end, where they take a drop of Bigtree’s blood, who is unjabbed, and then add a drop of the COVID “vaccine.” The slide containing nothing but his unjabbed blood looks perfectly normal, with nice doughnut-shaped cells.
The slides to which a drop of COVID “vaccine” was added show remarkable inconsistencies. On one slide, in the area touched by the liquid, the red blood cells looked like they’d evaporated. According to Cole, the cells were basically “de-hemoglobiated.”
The hemoglobin was just wiped out. As a result, the cells turned white, which makes it look as though they evaporated. “That just says that many of these vials are very, very irritating in their pre-mixture … It all goes back to purity and consistency of manufacturing,” Cole says. The blood cells were also clumping toward the outside of the drop, many were folding together and echinocytes were clearly visible. As explained by Cole:
“It instantly changed the pH of the interior. These are little blobs of protein on the membrane of the red cell, because the red cell has involuted … All these little fingers, that is not spike protein. That’s another myth.
But that’s fascinating, because that instantly changed the pH of the interior of the cell. And it caused a massive outflow of fluid from the interior of the cell causing all that cell membrane folding. That’s wild.
It was almost instantaneous, and it is everywhere. Those red cells are now nonfunctional red cells. Those aren’t going to carry a whit of oxygen. Now your body has to decide what to do and has an inflammatory reaction, because now it has to gobble those up.”
This Technology Must Be Stopped
In closing, Cole says:
“To go back to the key point — I want to drive this home — they’re going to try to do lipid nanoparticles plus influenza genes, plus RSV genes for all these other shots going forward. We already know that this was a failed ‘vaccine’ program. They have a technology that’s harmful. Human cells are meant to make human proteins. Human cells were not meant to make foreign toxic proteins.
Traditional vaccines don’t do that. Your body wants to make its own protein, not a flu protein, not an RSV protein, not any other viral protein, not SARS-CoV-2 protein. This platform is sufficiently proven to be dangerous that not only do the COVID shots need to be stopped, but the platform [as well] …
We see enough things going wrong already. I think that’s the message to humanity, to regulatory agencies, to government officials that are willing to step in and block regulatory corruption … Let’s stop these programs. Let’s continue to do proper science and not rush science.
You know that quote in the European Committee? ‘We were working at the speed of science.’ Good science isn’t rushed. And the Pfizer exec that just stepped down? [She said] ‘We were building the airplane while we were trying to fly it.’ Good grief. And she was proud of that. No, that’s not what you do to your fellow human beings. And that’s not what we do in medicine and safety.”
Bigtree adds:
“We stopped these gene programs multiple times. They’ve [been] stopped in their tracks because they were causing too much cancer. We’re having serious problems with this technology.
It has been stopped for all those reasons, so we should have been very concerned [about] using it as a vaccine. We certainly should not have rushed it. Instead we put it in front of a bunch of ‘kindergarteners’ that know nothing about what they’re looking at, and they approved it …
[T]here is something going wrong. And when we listen to Edward Dowd, insurance actuaries are going [under] because of the rise in all-cause mortality. All of this is happening, and they literally want to fast-track a system where they can just start banging these out [without] safety trials. This is a movie. This is a cartoon. How are real people acting like this? … These are critically damaging choices being made.”
Remedies that can help inhibit, neutralize and eliminate spike protein have also been identified by the World Health Council. Inhibitors that prevent the spike protein from binding to your cells include Prunella vulgaris, pine needle tea, emodin, neem, dandelion extract and the drug ivermectin. Dr. Pierre Kory, of FLCCC, believes ivermectin may be the best approach to bind the circulating spike protein.
Spike protein neutralizers, which prevent the spike from damaging cells, include N-acetylcysteine (NAC), glutathione, fennel tea, star anise tea, pine needle tea, St. John’s wort, comfrey tea and vitamin C.
Complex regional pain syndrome (CRPS) is a neuropathic pain disorder defined by the presence of distinct clinical features, including allodynia, hyperalgesia, sudomotor and vasomotor abnormalities, and trophic changes. The pain experienced is disproportionate to the degree of tissue injury and persists beyond the normal expected time for tissue healing. The pathophysiology is multifactorial and involves pain dysregulation in the sympathetic and central nervous systems, with likely genetic, inflammatory, and psychological contributions. There are two subtypes: type I, formerly known as reflex sympathetic dystrophy, and type II, formerly known as causalgia. Type I occurs in the absence of nerve trauma, while type II occurs in the setting of known nerve trauma. Clinically they are indistinguishable and follow a regional rather than dermatomal or peripheral nerve distribution. CPRS favors the distal extremities, though spread beyond the initially affected area commonly occurs in the proximal or contralateral limb. CRPS is further subdivided into “warm” versus “cold” and sympathetically-maintained versus sympathetically-independent, which may affect prognosis and treatment options. This activity describes the evaluation and management of complex regional pain syndrome and highlights the role of the interprofessional team in improving care for affected patients.
Objectives:
Outline the typical presentation of complex regional pain syndrome.
Describe the Budapest Criteria and their role in the diagnosis of complex regional pain syndrome.
Review the treatment options for complex regional pain syndrome.
Explain how careful planning and discussion amongst interprofessional team members involved in the care of patients with complex regional pain syndrome can help improve patient outcomes.
Complex Regional Pain Syndrome (CRPS) is a neuropathic pain disorder characterized by ongoing pain disproportionate to the degree of tissue injury and persists beyond the usual expected time for tissue healing. [1] Pain is accompanied by sensory, motor, and autonomic abnormalities. Such abnormalities include allodynia, hyperalgesia, sudomotor and vasomotor abnormalities, and trophic changes. Pain does not follow a particular dermatome or myotome but is rather regional. This disabling condition often develops after a trauma, fracture, or surgery.[2][3] But some spontaneous cases have also been reported.[4]
In the 16th century, Ambroise Paré reported cases with CRPS like symptoms for the first time which developed after phlebotomy.[5] In 1864, Silas Mitchell noted this syndrome after gunshot wounds. He used the term ‘causalgia’ to describe this syndrome in 1872. James A. Evans coined the term ‘reflex sympathetic dystrophy’ to describe a similar condition where he suspected sympathetically mediated pain in 1946. [6] Finally, in 1994, the International Association for the Study of Pain (IASP) named this condition ‘Complex Regional Pain Syndrome’ and proposed a diagnostic criterion. Due to low specificity, a widely accepted revised criterion was proposed in 2010 and is commonly referred to as the “Budapest Criteria.”[2][7]
CRPS has two subtypes: type I, formerly known as reflex sympathetic dystrophy, and type II, formerly known as causalgia. Type I occurs in the absence of nerve trauma, while type II occurs in the setting of known nerve trauma. Clinically they are indistinguishable and follow a regional rather than a dermatomal or peripheral nerve distribution and favor the distal extremities, though spread outside of the initially affected area commonly occurs to the proximal or contralateral limb.[6][8] CRPS is further subdivided into “warm” versus “cold,” and sympathetically-maintained (SMP) versus sympathetically-independent (SIP), which may affect prognosis and treatment options. [8]
CRPS not only impacts function, sleep, and activities of daily living but also takes a significant mental and psychosocial toll on the patient.[9][10][11] Its diverse spectrum of clinical presentation and lack of any clearly defined pathophysiology poses a challenge for optimal management of this disorder.
Evaluation
No definite pathophysiologic mechanism for CRPS has been identified yet. Therefore, no gold standard diagnostic test for CRPS exists.[8] The diagnosis is clinical and based on the widely accepted Budapest criteria. Compared to the previous IASP criteria, the Budapest criteria have similar sensitivity (0.99) but higher specificity (0.68).[7]
Motor/trophic: Evidence of decreased range of motion and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (hair, skin, nails).
D. Finally, there is no other diagnosis that better explains the signs and symptoms.
Various objective testing measures have been utilized to include thermography, triple-phase bone scan, and the quantitative sudomotor axon reflex test. While these studies provide further data, they are not necessary to make the diagnosis of CRPS. The diagnosis of CRPS is largely clinical and one of exclusion. The differential diagnosis includes small or large fiber sensorimotor neuropathy, cellulitis, erythromelalgia, vasculitis, vascular insufficiency, lymphedema, deep vein thrombosis, and Reynaud’s phenomenon. Diagnostic tests in CRPS are primarily aimed at screening for other potential differential diagnoses.
Although there is a possibility that patients with CRPS may improve spontaneously, considering the debilitating nature of this syndrome, it is prudent to institute aggressive management as soon as possible as a delay may result in an unfavorable outcome. Moreover, compared to chronic CRPS, early CRPS is less resistant to treatment and therefore has a better prognosis.[49] The goal of treatment is not only improvement in pain and discomfort but also functional restoration and prevention of disability. Therefore, the most optimal management would include an interprofessional approach including physical and occupational therapy, pharmacotherapy, behavioral therapy, and interventions.[6]
Physical and Occupational Therapy
Manual therapy and exercises are not the only CRPS treatments under this section. Other therapy modalities include transcutaneous electrical nerve stimulation, ultrasound, laser, pain education, mirror therapy, and graded motor imagery (GMI). Multiple mechanisms of action of physical therapy have been proposed with no clear definitive theory. Manual therapy and exercise improve range of motion, function and reduce disability through endorphin release as well as other central and peripheral analgesic mechanisms.[3][50] Pain education influences pain perception and behavior by improving understanding of pain pathophysiology in such patients.[3] Whereas mirror therapy and GMI remediate maladaptive cortical neuroplastic changes associated with chronic pain conditions like CRPS.[51]
A 2016 Cochrane review found that among the different physiotherapy modalities, mirror therapy and GMI may improve pain as well as function in CRPS. However, the quality of evidence was poor. Two clinical trials each for GMI and mirror therapy have demonstrated improvement of pain and function at 6 months. Very low-quality evidence was also found for improvement of impairment in CRPS with multimodal physiotherapy.[3]
Pharmacotherapy
Multiple pharmacotherapeutic agents are used in the management of CRPS. The commonly used therapeutic options in this category include anti-inflammatory medications, anticonvulsants, antidepressants, transdermal lidocaine, opioids, NMDA antagonists, and bisphosphonates. Using a multimodal pharmacologic regimen that combines several different classes may lead to superior outcomes.
Anti-inflammatory Medications
Oral corticosteroids and non-steroidal anti-inflammatory drugs (NSAIDs) have been used in CRPS as inflammation is thought to play a role in disease pathogenesis. Based on three trials that compared oral corticosteroids to placebo in CRPS, a 2013 Cochrane review concluded that oral steroids do not significantly reduce pain. This was supported by very low-quality evidence. The review also found that oral corticosteroids seem to improve composite pain scores.[52] Another study found that compared to piroxicam (NSAID), oral prednisone seemed to be more effective in improving composite CRPS scores in post-stroke patients.[53] A more recent study found that 2-month treatment with low-dose oral prednisone was safe and effective in post-stroke CRPS.[54]
Bisphosphonates
This class of medication is used routinely in bone-related problems as it inhibits osteoclastic activity. Several mechanisms of action of bisphosphonates in CRPS have been proposed. The more commonly accepted mechanisms include inhibition of bone marrow cell proliferation and migration as well as inflammation modulation.[55] A 2017 meta-analysis concluded that bisphosphonates seem to reduce pain in CRPS I.[56] A Cochrane review in 2013 found that low-quality evidence also seemed to suggest the same response in CRPS, more so in those with concomitant evidence of osteopenia or osteoporosis.[52]
Anticonvulsants and Antidepressants
Gabapentin is the most widely studied medication in this class. It works by inhibiting the alpha 2-delta subunit of voltage-gated calcium channels. Despite its widespread use in treating CRPS, very low-quality evidence suggests that gabapentin is ineffective in the treatment of CRPS I.[52] In 2016, a study compared amitriptyline and gabapentin for CRPS I and pediatric neuropathic pain. Both the medications were found to reduce pain intensity and disability significantly. However, no significant difference in effect was noted between the two.[57]
Opioids
The effectiveness of opioids has not been studied in CRPS, and therefore no evidence-based conclusions can be drawn.[41]
NMDA Antagonists
NMDA receptor antagonists like ketamine have been hypothesized to reverse central sensitization and maladaptive cortical neuroplastic changes in CRPS.[24] Low-quality evidence suggests that intravenous ketamine infusion may improve pain in CRPS for up to 4-11 weeks. [52][52] However, side effects and psychomimetic properties of ketamine have prevented widespread use.[24]
Behavioral Therapy
Elevated levels of catecholamines associated with depression can worsen CRPS by inducing central sensitization through adrenergic mechanisms. Reversal of this effect is one of the proposed mechanisms of action of psychotherapy in CRPS. Apart from case reports and case series, only one small trial has been done evaluating the efficacy of behavioral interventions in CRPS. Despite the lack of clear evidence supporting their use in CRPS, behavioral therapy has been recommended part of comprehensive treatment.[58]
Interventions
Sympathetic Blocks
Sympathetic hyperactivity is believed to be an underlying pathophysiologic mechanism of CRPS.[41] Therefore, lumbar sympathetic nerve blocks are routinely used in the treatment of lower extremity symptoms, and stellate ganglion sympathetic blocks are used for the management of upper extremity symptoms of this syndrome. A 2013 Cochrane review found that sympathetic blocks with local anesthetic were ineffective at reducing CRPS related pain, but the quality of evidence was low.[52] A more recent Cochrane review in 2016 failed to draw any definitive conclusions on the efficacy of such treatment in CRPS due to paucity of evidence.[59]
Spinal Cord Stimulation
Spinal cord stimulation (SCS) involves delivering electric stimulation to the dorsal column of the spinal cord by the placement of electrodes in the epidural space. The electrodes are usually connected to an implanted pulse generator to power the electrode, but some devices use an external pulse generator. Multiple mechanisms of action of SCS have been proposed, which include inhibition of nociceptive neural conduction in the spinal cord, adrenergic inhibition, vasodilation, and reversal of cortical maladaptive neuroplastic changes. A systematic review in 2017 studied the effectiveness of SCS in CRPS. The authors concluded that a high level of evidence supports the use of SCS for improvement of pain scores, quality of life as well as the perception of pain relief in CRPS.[59]
Dorsal Root Ganglion Stimulation
Targeting the dorsal root ganglion (DRG) instead of the spinal cord is a relatively new and novel neuromodulation modality for the management of chronic pain. This enables a more focused application of neurostimulation than traditional SCS. DRG stimulation was approved by United States Food and Drug Administration in 2016 for treatment of lower extremity pain in CRPS. A recent pooled analysis study concluded that DRG stimulation was safe and effective for CRPS with a 4.9-point mean reduction of pain intensity in CRPS-I.[60] The ACCURATE study compared SCS and DRG stimulation in 152 subjects with CRPS, and study results were published in 2017. This multicenter randomized trial found that DRG stimulation was more effective than traditional SCS in reducing pain and improving quality of life in CRPS.[61]
Bonica, in 1990 had proposed 3 stages of CRPS. Bruehl et al. studied the validity of stages in a series of 113 patients and found no significant difference in duration of symptoms among the stages. This research suggested that clear generalized disease stages don’t exist in CRPS.[62]
The prognosis of CRPS can be variable. Both spontaneous remission and refractory clinical presentation have been seen. But early treatment may improve the prognosis.
Dystonia, cognitive executive dysfunction, adrenal insufficiency, gastroparesis, and irritable bowel syndrome are a few of the complications associated with long-standing CRPS.
Oral supplementation of vitamin C has been hypothesized to lower the risk of development of CRPS after fractures due to its antioxidant properties. A meta-analysis of 3 trials in 2015 found that available evidence failed to demonstrate a definitive preventive role of vitamin C in CRPS development after distal radial fractures, although the level of evidence was low.[63] Another meta-analysis and systemic review in 2017 evaluated the efficacy of vitamin C in the prevention of CRPS development after wrist fractures. 500 mg vitamin C daily therapy for 50 days seemed to reduce the risk of CRPS at 1 year in this study.[64]
An interdisciplinary team approach to this problem is required to maximize recovery and limit disability. Social service, pharmacology, nursing, and physical therapy, along with early advanced pain management, are key to improved outcomes.
Pregabalin and Gabapentin are non-natural, branched chain amino acids. Both are chemical analogues of gama-aminobutyric acid (GABA); however, neither drug has activity in GABAergic neuronal systems. Both these drugs are efficacious in certain types of neural pain control.
Dosage: The treatment for neuropathic pain with Gabapentin is usually initially started with one dose of 300 mg per day.It can be given orally at a dose of 300-1200 mg 3 times per day. Maximum dose should be 3600 mg per day.
The suggested maximum therapeutic dose of Pregabalin in neuropathic pain associated with diabetic peripheral neuropathy is 300 mg per day; it can be initiated at a dose of 50 mg thrice a day. The dose of the drug can be increased up to 300 mg per day within a week of starting the treatment.
For neuropathic pain associated with spinal cord injury, the recommended therapeutic dose of Pregabalin should be 150 to 600 mg daily. The suggested starting dose is 75 mg twice per day. The dose might be increased to 150 mg twice/day within one week of starting treatment. In patients having suboptimal pain relief after 2 to 3 weeks of treatment with 150 mg twice daily, the dose might be increased up to 300 mg twice/day.[1]
Excretion: It is estimated that elimination half-life parameter for the two drugs are same. The elimination half-life for Gabapentin is estimated to be in the range of 5-7 hours, and that for Pregabalin is about 6.3 hours, indicating that both drugs can reach a steady state within 24-48 hours.
Adverse effects: Generally, Pregabalin and Gabapentin are well tolerated. Dizziness is the most frequently reported negative effect of Pregabalin, followed by somnolence, which accounts for the most frequent reason for treatment discontinuation. The negative effects of both the drugs are dose-dependent and are reversible.