Month: August 2022
MR May Detect Brain Changes Before Symptoms of Dementia Appear
According to a study in Radiology, an advanced MR technique shows promise in helping understand early structural changes in the brain before symptoms of dementia become apparent. The research indicates the structural integrity of the brain’s white matter, as measured with an advanced MR technique, is lower in cognitively normal people who carry a genetic mutation associated with Alzheimer’s disease than it is in non-carriers. Researchers said the findings show the promise of widely available imaging techniques in helping to understand early structural changes in the brain before symptoms of dementia become apparent.

People who carry the autosomal dominant Alzheimer disease (ADAD) mutation have a higher risk of Alzheimer’s disease. The mutation is linked to a buildup of abnormal protein called amyloid-beta in the brain that affects both the gray matter and the signal-carrying white matter.
“It’s thought that the amyloid deposition in the gray matter could disrupt its function, and as a result the white matter won’t function correctly or could even atrophy,” said study lead author Jeffrey W. Prescott, M.D., Ph.D., neuroradiologist at the MetroHealth Medical Center in Cleveland.
An earlier study by Dr. Prescott and colleagues on patients with sporadic Alzheimer’s disease, which comprises 99% of cases, found that white matter structural connectivity, as measured with the MR technique diffusion tensor imaging (DTI), degraded significantly as patients developed more amyloid burden.
“The current work extends these results by showing that similar findings are detectable in asymptomatic at-risk patients,” said Jeffrey R. Petrella, M.D., professor of radiology at Duke University and senior author on both studies.
In the new study, Dr. Prescott and colleagues used data from the Dominantly Inherited Alzheimer Network (DIAN) to compare ADAD mutation carriers with non-carriers to see if there were changes in structural connectivity that could be related to the mutation.
The study participants included 30 mutation carriers, mean age 34 years, and 38 non-carriers, mean age 37. The participants all had normal cognition when they underwent structural brain MR and DTI.
Analysis showed that mutation carriers had lower structural connectivity in the frontoparietal control network, which connects areas mainly in the parietal and frontal lobes, two regions known to be involved with Alzheimer’s disease. Among mutation carriers, there was a correlation between expected years until onset of symptoms and white matter structural connectivity in the frontoparietal control network, even when controlling for amyloid plaque burden.
“This suggests that DTI measures of network integrity may serve as a surrogate for the brain’s resilience to pathologic attack,” Dr. Petrella said.
“We used a network measurement called global efficiency, in which a decreased efficiency can be taken as a breakdown in the organization of the network,” Dr. Prescott added. “The results show that for mutation carriers, global efficiency would decrease significantly as they approach the estimated age of symptom onset.”
The study findings support a potential role for imaging-based identification of structural changes of the brain in people at genetic risk for early-onset Alzheimer’s disease in understanding how genes influence the disease process that leads to dementia.
“This shows the potential of MR as an evaluation tool in patients who are deemed at-risk for Alzheimer’s disease before they develop symptoms,” Dr. Prescott said. “Use of these advanced MR techniques could help further refine identification of at-risk patients and risk measurements.”
The findings also point to a role for imaging in studying therapeutic drugs to treat Alzheimer’s disease. While the majority of trials so far have been performed with patients who already have Alzheimer’s disease or cognitive impairment, earlier identification and treatment of patients at risk represents a more promising avenue for preventing or at least delaying the onset of dementia.”
“One potential clinical use of this study tool would be to add quantitative information to risk factors like family history and use that to help identify patients early, when they may benefit from treatment,” Dr. Prescott said. “But until we have an effective treatment, we will have to wait for that to be implemented.”
The researchers hope to do a follow-up using advanced imaging and updated data from the DIAN network to evaluate the progression of Alzheimer’s disease in the study participants.
Large International Study Reports Brain Complications in COVID-19 Patients
Approximately one in 100 patients hospitalized with COVID-19 will likely develop complications of the central nervous system, including stroke, hemorrhage, and other potentially fatal complications, according to the largest multi-institutional international study to date on brain complications of COVID-19. The study is being presented at RSNA 2021.

“Much has been written about the overall pulmonary problems related to COVID-19, but we do not often talk about the other organs that can be affected,” said study lead author Scott H. Faro, MD, FASFNR, professor of radiology and neurology and director of the Division of Neuroradiology/Head & Neck Imaging at Thomas Jefferson University in Philadelphia. “Our study shows that central nervous system complications represent a significant cause of morbidity and mortality in this devastating pandemic.”
Dr. Faro initiated the study after discovering that existing literature on central nervous system complications in hospitalized COVID-19 infected patients was based on a relatively small number of cases.
To derive a more complete picture, he and his colleagues analyzed nearly 40,000 cases of hospitalized COVID-19 positive patients from seven U.S. and four western European university hospitals. The patients had been admitted between September 2019 and June 2020. Their average age was 66 years old, and there were twice as many men as women.
The most common cause of admission was confusion and altered mental status, followed by fever. Many of the patients had comorbidities like hypertension, cardiac disease and diabetes.
There were 442 acute neuroimaging findings that were most likely associated with the viral infection. The overall incidence of central nervous system complications in this large patient group was 1.2%.
“Of all the inpatients who had imaging such as MRI or a CT scan of brain, the exam was positive approximately 10% of the time,” Dr. Faro said. “The incidence of 1.2%means that a little more than one in 100 patients admitted to the hospital with COVID-19 are going to have a brain problem of some sort.”
The most common complication was ischemic stroke, with an incidence of 6.2%, followed by intracranial hemorrhage (3.72%) and encephalitis (0.47%), an inflammation of the brain.
The researchers also discovered a small percentage of unusual findings, such as acute disseminating encephalomyelitis, an inflammation of the brain and spinal cord, and posterior reversible encephalopathy syndrome, a syndrome that mimics many of the symptoms of a stroke.
“It is important to know an accurate incidence of all the major central nervous system complications,” Dr. Faro said. “There should probably be a low threshold to order brain imaging for patients with COVID-19.”
Patients on Older Blood Thinners may be at Higher Risk for Brain Bleeding after Head Trauma
Patients taking older types of blood thinners or taking aspirin while on blood thinners may be at a higher risk of delayed brain bleeding and death following head trauma, according to a study presented at RSNA 2021. The three-year study of more than 1,000 patients found that the risk of delayed intracranial hemorrhage and death following head trauma was significantly higher for adults taking older blood thinning medications including clopidogrel (Plavix) and warfarin (Coumadin).

“The incidence of delayed posttraumatic intracranial hemorrhage in patients on different types of blood thinners with and without the addition of aspirin is not well established,” said Warren Chang, MD, neuroradiologist and director of research at the Imaging Institute of the Allegheny Health Network in Pennsylvania. “This is an active area of investigation, especially as novel blood thinners become more widely adopted.”
Intracranial hemorrhage occurs when blood vessels within the brain rupture, releasing blood into the brain tissue. In a delayed traumatic intracranial hemorrhage, bleeding in the brain occurs after the initial trauma, usually within 48 hours, after an initial negative head CT.
High blood pressure, head injury and the use of blood thinners are known causes of intracranial hemorrhage. As the population ages, the prevalence of patients taking blood thinners is increasing.
Adults taking blood thinners who suffer head trauma typically undergo CT imaging of the brain. However, the standard of care beyond initial imaging is not well defined. Some hospitals admit patients for observation and repeat CT imaging, while others may discharge a patient who does not have intracranial hemorrhage and is in stable condition.
“Different hospital networks have different strategies for repeat imaging of these patients,” Dr. Chang said.
In the retrospective analysis, researchers reviewed the records of all patients taking blood thinners who suffered head trauma and underwent CT imaging in the Allegheny Health Network between January 1, 2017, and January 1, 2020. Patients were included in the study if initial CT imaging was negative for intracranial hemorrhage and repeat imaging was subsequently performed. The final study group of 1,046 patients included 547 women and 499 men with an average age of 77.5.
Within the study group, 576 patients were taking one of the newer blood thinners, such as apixiban
(Eliquis), rivaroxaban (Xarelto) and dabigatran (Pradaxa), and 470 patients were taking warfarin, clopidogrel or another older medication.
Overall, there was 1.91% incidence (20 patients) of delayed hemorrhage and 0.3% mortality rate (3 patients). All deaths in the study group were among patients in the warfarin/clopidogrel/older blood thinner group.
Among the total study group, 345 patients were taking both blood thinners and aspirin. Of the 20 patients who suffered a delayed hemorrhage, 15 were taking an older type of blood thinner, and nine of the 15 were also taking aspirin.
“The rate of delayed hemorrhage was higher in patients taking older blood thinners compared to novel drugs, and significantly higher in patients taking aspirin in addition to the older medications,” Dr. Chang said.
Among the five patients taking novel blood thinners who experienced a delayed hemorrhage, four were also taking aspirin.
“Given the high volume of our trauma patients taking aspirin and anticoagulants, this study will help to guide our care of closed head injury patients in emergency medicine and support efforts to use imaging resources appropriately,” said Thomas Campbell, MD, MPH, the system chair for Emergency Medicine of the Allegheny Health Network.
Based on the findings, the study’s authors recommend follow-up CT for patients who had no initial intracranial hemorrhage from head trauma who are taking one of the older blood thinners and for patients who take any blood thinner along with aspirin. Unless there are external signs of trauma, follow-up CT is unnecessary for patients who only take one of the newer blood thinners and do not take aspirin.
“Taking any blood thinner concurrently with aspirin significantly increased the risk of delayed hemorrhage, while taking one of the novel medications without aspirin significantly reduced the risk,” Dr. Chang said.
“This study illustrates how innovative imaging can drive optimal patient care. In the end, I believe the recommendations of this work will save many lives,” said Bethany Casagranda, DO, chair of the Imaging Institute of the Allegheny Health Network.
Trauma Imaging in Pregnancy: A Review of the Evolving Appearance of the Placenta on CT and Mimics of Placental Injury








Blunt abdominopelvic trauma in pregnant patients can be a cause of great concern for both the mother and the fetus. The fetus should always undergo sonographic evaluation and monitoring to assess for signs of distress or demise.
Cross-sectional imaging should be used judiciously, as radiation emitted by computed tomography (CT) increases the risk of harm to the fetus and development of childhood cancers. Given the rarity with which CT is performed on pregnant patients, this manuscript will review the indications and risks of CT in pregnant trauma patients, the normal CT appearance and evolution of the placenta, physiologic findings of pregnancy on CT that may mimic placental injury, and commonly encountered pregnancy-related traumatic injuries.
Abdominopelvic trauma in pregnancy poses a clinical conundrum with respect to imaging in the emergency room. In pregnant trauma patients, various imaging modalities may be utilized to evaluate the mother and fetus. Radiography is the first line of imaging, used as a primary survey of the cervical spine, chest, and pelvis.1-3 The benefit of radiography is its ability to rapidly assess possible fractures and common thoracic trauma with relatively low radiation dose.
Ultrasound is used both to assess the fetus and to detect intra-abdominal and pericardial fluid in the mother, the latter as part of a focused assessment with sonography in trauma (FAST) scan.3 Fetal assessment should include evaluation of cardiac activity and examination for possible injuries. Performing FAST poses a challenge under these circumstances, owing to the distorted pelvic view from the gravid uterus; therefore, evaluating the pouch of Douglas for hemoperitoneum requires skill and experience. Moreover, potential hemorrhage from solid organ injury, amniotic fluid from uterine rupture, or both can make it difficult to distinguish the etiology of free intraperitoneal fluid with FAST.4
FAST is indicated in hemodynamically unstable pregnant patients, as it can efficiently determine the presence of intra-abdominal free fluid that requires exploratory laparotomy. FAST has an overall sensitivity of 61%–83% for detection of free fluid, although this varies by trimester.1 Serial FAST examinations raise overall sensitivity to 72%–93%.4 A study by Richards, et al, found that sensitivity and specificity of FAST was highest in the first trimester of pregnancy, and declined in the second or third trimester.13 Despite these findings, the negative predictive value of FAST remained relatively high (above 95%) regardless of gestational age.5 FAST is especially useful in the initial assessment of pregnancy trauma during the first trimester, particularly in hemodynamically unstable patients. In stable patients, on the other hand, FAST has limited sensitivity for detecting injuries that may require intervention.
Computed tomography is the preferred imaging modality for evaluating high-energy trauma, such as from a motor vehicle accident, in hemodynamically stable patients.2 Per the American College of Radiology (ACR) Appropriateness Criteria, single portal venous phase CT of the abdomen and pelvis with intravenous contrast is indicated in cases of life-threatening emergencies.6 Noncontrast CT is never indicated in these cases, owing to its low sensitivity for detecting solid-organ injuries. CT angiography (CTA) may be indicated in cases of unstable pelvic fractures with a high suspicion for arterial injury to help guide surgical or vascular intervention.6
Magnetic resonance imaging (MRI) is seldom used in the acute setting for initial evaluation of pregnant patients, owing to extended, and often delayed, acquisition time. In the setting of a stabilized patient who requires follow-up imaging, MRI may be useful in situations that require visualization of the spine and soft-tissue injuries. MRI is safe for use during pregnancy, as it presents no radiation to the fetus.7
Effects of Radiation on Pregnancy
In hemodynamically stable patients, contrast-enhanced CT (CECT) is indicated for assessment of suspected hollow- and solid-organ, vascular, and bony pelvic injuries.1,2 CECT is recommended by the ACR when the required information can only be acquired through the modality and when imaging may affect care management.3 In most cases, those two criteria are met in the setting of trauma in pregnancy.
Radiation exposure may affect the fetus in many ways; thus, CT should be used judiciously. For pregnant patients undergoing CT within the first two weeks of conception, the main risk is failure of blastocyst implantation.7 Beyond this point, the fetus is most vulnerable to radiation from the second through the twentieth weeks of gestation, when the fetus is rapidly developing; the primary concern is for teratogenesis.1,7 Therefore, CT should not be used during the first trimester except in life-threatening emergencies for which no other imaging modality is suitable.
The short-term risks of radiation exposure to a fetus include death, abnormal growth causing deformities, and intellectual underdevelopment.7 Long-term risks include a two-fold increased risk of fatal childhood cancer, from a baseline of 1 in 2000 to 1 in 1000.1,2 The expected exposure threshold for these risks to manifest is greater than 100 mGy of radiation; however, radiation doses do not exceed 50 mGy with any diagnostic imaging modality, including abdominopelvic CT.1,7 Hence, the radiation dose from imaging should not pose any of the aforementioned risks unless serial imaging is performed, which could exceed the radiation dose considered safe for fetal imaging.
CT Dose Reduction in Pregnancy
Although typical CT imaging doses do not exceed 50 mGy,1,4 caution should still be taken to keep radiation exposure to the fetus as low as reasonably achievable (ALARA) during these examinations. The most common method of reducing dose is to alter acquisition parameters by decreasing the milliamperage, kilovolt peak, and craniocaudal extent of acquisition.8 A wide pitch and narrow collimation can also help reduce the dose,8 as can employing a single-phase protocol if a multiphasic protocol is unnecessary. A lead shield may be used while obtaining CT images outside of the abdomen and pelvis; however, exposure to scattered radiation is minimal, as most of it is internal rather than external.8
Effects of Iodinated Intravenous Contrast on Fetal Development
Another aspect of CT imaging to consider during pregnancy is the use of iodinated contrast. While no teratogenic effects have been described following intravenous administration of iodinated contrast, iodine-based compounds can impact the thyroid gland of the fetus.7,9 The thyroid uses iodine to synthesize thyroid hormones; therefore, any iodine-containing drug should be used with caution during pregnancy due to the risk of iodine uptake leading to secondary hypothyroidism in the fetus. Congenital hypothyroidism occurs in 1 of every 4000 births; left untreated, the condition can lead to failure to thrive as well as mental and developmental impairments.9 The ACR recommends iodinated contrast media in pregnancy only when no acceptable alternative test is available, when the expected information to be obtained from the study is vital to the well-being of the mother and fetus, and when the referring physician deems it necessary based on their clinical judgement.9
Review of Cross-sectional Trauma Imaging in Pregnancy
Trauma is the leading cause of non-obstetrical maternal mortality and a significant cause of fetal loss.2 In the setting of trauma during pregnancy, there are two patients, the mother and the fetus, and the decision to use CT in these circumstances should consider the risks and benefits to both. In the acute setting, the primary concern for the treating physician should be for maternal benefit from early and accurate diagnosis. While the risk of radiation exposure to the fetus is of significant concern, the dose is low enough to pose no expected, tangible effects on the fetus. Given the infrequency with which cross-sectional imaging is performed during pregnancy, certain CT findings of normal physiologic changes may initially appear concerning to those unfamiliar with the normal appearance.
Normal Placental Appearance
The CT imaging appearance of a normal placenta will evolve with progression of pregnancy as follows:
First Trimester
Computed tomography should not be utilized to evaluate patients in their first trimester except under life-threatening circumstances. During this period, the placenta is almost indistinguishable from the myometrium, with a homogeneous appearance and indistinguishable smooth chorionic plates along the periphery of the uterine cavity.10,11 Depending on gestational age, the only indications of early pregnancy identifiable on CT may be endometrial thickening or a small, ovoid fluid collection representing a gestational sac.
Second Trimester
Throughout the second trimester, the placenta becomes heterogeneous in appearance and increases in attenuation relative to the myometrium.10 It is during the second trimester that placental cotyledons begin forming. These appear as multiple foci of low attenuation throughout the placenta (Figure 1).1,11 Chorionic plate indentations may begin appearing by the late second or third trimester as scattered, hypoattenuating indentations at the interface of the fetal surface of the placenta and the amniotic sac (Figure 1).1,10 Placental cotyledons and chorionic plate indentations share features with those of placental abruption, including hypoattenuation of placental tissue, although the lesion seen in placental abruption will involve the full placental thickness.
Third Trimester
By this period, the placenta appears increasingly heterogeneous, with better visualization of the venous lakes. Also referred to as placental lakes, venous lakes are located on the maternal side of the placenta and appear as patchy regions of hyperdense foci or placental enhancement on CECT owing to their rich venous supply (Figure 2).1,2 Given their appearance, these may be mistaken for regions of placental hemorrhage.
Mimics of Placental Injury
Given the evolving nature of the placenta, some its features on CT images can be misinterpreted as placental injury (Table 1).
Myometrial contractions typically appear hypoattenuating in comparison to the placenta. The angle of the hypoattenuation relative to the myometrium is the primary differentiator between injury and contractions; myometrial contractions tend to form obtuse angles with myometrial tissue, while injury such as abruption often forms acute angles.1,10
Chorionic plate indentations appear as scattered, low-attenuation, shallow, and wedge-shaped indentations along the fetal surface of the placenta (Figure 1).1,10 This is in contrast to placental abruption, which appears as full-thickness areas of low-attenuation or nonenhancement. Venous lakes may appear as areas of contrast blush on the maternal side of the placenta and can be mistaken for placental hemorrhage or abruption (Figure 2).1 Several retrospective and prospective studies have demonstrated that placental lakes are associated with increased placental thickness and do not confer any increased risk of gestational or placental complications.12,13
Wedge-shaped placental infarcts can appear as low-attenuation wedges along the periphery of the placenta as it matures and tend to have no clinical significance.10
During early pregnancy, subchorionic hemorrhages may also be visualized as low- to intermediate-density fluid immediately subjacent to the chorion; when small, they also tend to be clinically insignificant.1,10
Pregnancy-related Injuries
One of the most common pregnancy-related injuries during the second and third trimesters is placental abruption, which may occur in up to 50% of major traumas.1 Abruptions related to trauma have a high fetal mortality ranging from 67% to 75%.1 The diagnosis is primarily clinical, with signs and symptoms including abdominal pain, uterine contractions, and non-reassuring fetal heart rates. Ultrasound may be used to identify placental hematomas, but the modality has poor sensitivity compared to CT.6,10 Placental abruption on CT images appears as a full-thickness area of nonenhancing placenta that forms an acute angle with the myometrium (Figure 3).1,10
The most troubling traumatic obstetrical injury is uterine rupture, which occurs in 0.6% of all maternal injuries and carries a high risk of mortality for both the fetus and the mother.3 Patients typically present with hemodynamic instability, sudden severe abdominal pain, palpable fetal parts, and non-reassuring fetal heart rates. Imaging can help confirm diagnosis by showing endometrial or myometrial defects, intraperitoneal fetal parts, and possible extrauterine hematoma, for which urgent laparotomy is warranted.8
Other Modalities Used to Image Trauma During Pregnancy
Following CT imaging for initial assessment, follow-up sonography or MRI can be used during pregnancy to reduce the cumulative radiation dose that results from repeated CT examinations. Importantly, while ultrasound can assist in diagnosis, the modality is insensitive for placental abruption and a negative examination does not exclude this diagnosis.1,3 Ultrasound is preferred in fetal assessment, while MRI allows for improved soft-tissue evaluation and can be used to evaluate the pelvic anatomy and the fetus.
Conclusion
Given the high mortality rate of nonobstetrical trauma to both mother and fetus, CT should be utilized only after discussing the risks and benefits with the patient and care team. Computed tomography visualizes greater anatomic detail than does ultrasound, and it is superior to MRI with respect to availability and the time required for examination. The imaging appearance of the placenta evolves throughout pregnancy; not all radiologists may be aware of the expected CT findings of a normal placenta, as the modality is rarely used during pregnancy. Radiologists should be aware of the changing appearance of the normal placenta to avoid confusing these features with those of placental injury.
Subsequent ultrasound or MR imaging may be performed to further evaluate or monitor findings suspicious for uterine or placental injury.
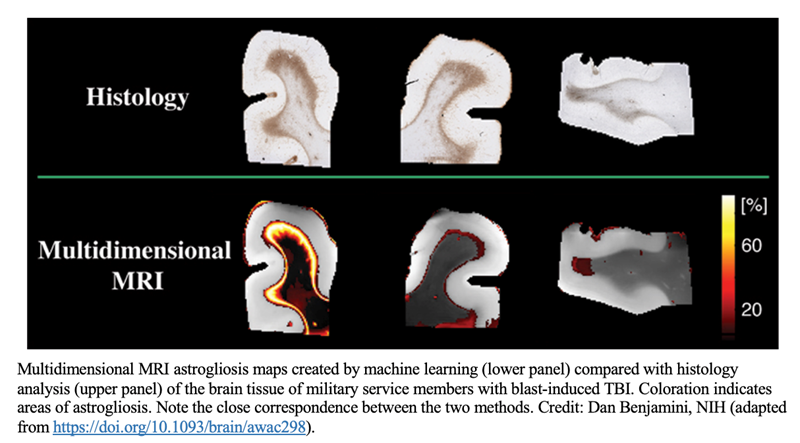
Multidimensional MRI Detects “Invisible” Brain Injury
A National Institutes of Health (NIH)-developed multidimensional MRI method can detect astrogliosis, a neuroinflammatory response that occurs in traumatic brain injury (TBI) and other neurological conditions, according to a study published in Brain. Researchers had previously established that the multidimensional MRI strategy can identify diffuse axonal injury—a microscopic brain injury that, like astrogliosis, cannot be detected by conventional radiological methods.
The two studies, conducted with postmortem human brain tissue, illustrate the potential of using multidimensional MRI with living humans to identify biomarkers for diseases and disorders previously considered radiologically invisible.
The multidimensional MRI method was developed in the laboratory of Peter Basser, PhD, at NIH’s Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). The studies were conducted through a collaboration between NIH, the Center for Neuroscience and Regenerative Medicine (CNRM), and the Henry M. Jackson Foundation for the Advancement of Military Medicine. They were led by Dan Benjamini, PhD, a former NICHD postdoctoral fellow in Dr Basser’s lab and CNRM staff scientist who is now a tenure-track investigator at NIH’s National Institute on Aging.
Conventional MRI methods lack the sensitivity to detect microscopic brain injuries such as axonal injury and astrogliosis. Diffuse axonal injury is a type of TBI that involves tearing of the brain’s white matter fibers when the brain shifts and rotates inside the skull. Astrogliosis is an abnormal increase in the number and size of reactive astrocytes that can occur in TBI, neurodegenerative diseases and disorders such as epilepsy and multiple sclerosis, aging-related diseases such as Alzheimer’s disease, and other neurological conditions.
MRI methods that can detect such microscopic changes would have potential research and clinical applications, including facilitating diagnosis of TBI, a major global public health concern.
To identify MRI biomarkers for astrogliosis, the researchers compared samples of postmortem brain tissue from seven military service members who had sustained TBI from blast exposure, which results in astrogliosis, and from seven people who had not. The researchers found that astrogliosis induces microscopic changes in the brain tissue that result in a distinct multidimensional MRI pattern. They then developed an approach to compare areas with and without astrogliosis in the same brain, allowing them to specifically map areas of astrogliosis. Their MRI results correlated well with findings from histology images—the current gold standard for detecting astrogliosis in tissue samples.
Their previous work to identify MRI biomarkers of diffuse axonal injury in human brain tissue samples followed a similar approach. Interestingly, they found that astrogliosis and axonal injury have opposite effects on certain parameters of their MRI spectra, suggesting that multidimensional MRI could be used to detect both conditions in the same brain.
If successfully adapted for use in live humans, this multidimensional MRI strategy could be applied to personalized diagnosis and therapy of TBI and other neurological conditions. It also would serve as a useful tool for neuroimaging studies of brain injury, disease, repair, and aging.
Additionally, the method can be used to identify other quantitative MRI biomarkers of injury or tissue damage. “In the past, finding potential MRI biomarkers was a shing expedition,” says NICHD’s Dr Basser. “Now we’re at least fishing with sonar.”
The scientists are now working to adapt their multidimensional MRI method to detect astrogliosis and other neurological diseases and disorders in people. In the future, they aim to conduct a small clinical study to validate the method.
In Trauma Cases, Use of Chest and Abdominopelvic CT has Increased
The national utilization of chest and abdominopelvic CT for trauma-related emergency department (ED) encounters increased between 2011 and 2018 in commercially insured patients—especially for single-encounter thoracabdominopelvic CT examinations and for minor injuries—as reported in the American Journal of Roentgenology (AJR).
“Given concerns of increased cost and incidental findings detection, further investigation is warranted to explore the potential benefit of single-encounter thoracabdominopelvic CT examinations in patients with minor injuries, as well as strategies to optimize order appropriateness,” wrote first author Ninad V Salastekar, MBBS, MPH, from the department of radiology and imaging sciences at Emory University School of Medicine.
Using national claims information extracted from the IBM MarketScan Commercial Database, Dr. Salastekar’s team identified trauma-related ED encounters via 2011–2018 MarketScan files. ED encounters were organized using the Injury Severity Score (minor, intermediate, major) via International Classification of Diseases codes, them assessed for chest CT, abdominopelvic CT, and single-encounter thoracoabdominopelvic CT examinations.
Ultimately, in commercially insured patients, national utilization of single-encounter thoracoabdominopelvic CT per 1,000 trauma-related ED encounters increased from 3.4 in 2011 to 9.8 in 2018 (adjusted incidence rate ratios, 1.16 per year). Additionally, rates rose from 1.1 to 4.6 (1.18) for minor, 6.4 to 16.4 (1.16) for intermediate, and 99.6 to 179.9 (1.08) for major injuries.
Because their retrospective study used national claims data from commercially insured patients—excluding the majority of Medicare- or Medicaid-eligible individuals, while entirely excluding the uninsured—“the findings may not generalize to such populations,” the authors of this AJR article cautioned.
Scientists use High-Resolution MRI to Create New Map of Young Human Brain Cortex
Using high-resolution MRI, scientists at the UNC School of Medicine have mapped the surface of the cortex of the young human brain with unprecedented resolution, revealing the development of key functional regions from two months before birth to two years after.

Published in the Proceedings of the National Academy of Sciences, the new cortical development mapping represents a valuable resource for further research on brain development and offers a powerful new approach to the study of brain-development conditions such as autism and schizophrenia.
“These results provide an important reference for exploring and understanding the dynamics of early brain development,” said study senior author Gang Li, PhD, associate professor of radiology at the UNC School of Medicine.
The study’s first author was Ying Huang, a PhD candidate in Li’s laboratory.
The cortex is a sheet of brain cells that wraps around much of the rest of the brain. The most evolutionarily advanced brain region, it is proportionately larger in humans than in other mammals, and is responsible for higher, distinctively human functions including language abilities and abstract reasoning.
The third trimester of pregnancy through the first two years of life is the most dynamic period in cortical development. The cortex thickens markedly during this interval, and grows at an even faster pace in terms of surface area, by forming complicated cortical folds.
Disruptions to cortical thickening and expansion in this phase have been linked to autism and schizophrenia. However, neuroscientists haven’t had as detailed an understanding of this developmental phase as they would like. In particular, they’ve had a need for more comprehensive, high-resolution mapping, across the fetal-to-toddler age range, that divides or “parcellates” the developing cortex into distinct regions with their own growth rates – especially surface area growth rates.
In the study, Li and colleagues performed just such a mapping. They first gathered a set of 1,037 high-quality magnetic resonance imaging (MRI) scans of infants in the third-trimester-to-two-year age interval. The scans came from two other research projects, the UNC/UMN Baby Connectome Project (BCP) and the Developing Human Connectome Project. The team analyzed the scan data using state-of-the-art, computer-based image-processing methods, essentially dividing the cortical surface into a virtual mesh containing thousands of tiny circular areas, and calculating the surface expansion rate for each of these areas.
The analysis didn’t start with assumptions about the locations of brain structures or functional regions, but this regionalization of the brain became evident anyway from the resulting maps, based solely on the different rates at which areas of the surface expanded. In all, the researchers defined 18 distinct regions, which they found correlated well with what is already known about the developing cortex’s functional regions.
“All these regions show dramatic expansion in surface area during this developmental window, with each region having a distinct trajectory,” Li said.
The maps revealed that each region tended to have the same developmental path as its counterpart in the cortex’s opposite hemisphere. Sex differences were apparent too. Even when controlling for sex differences in overall surface area – male brains having greater area – there remained differences in multiple regions. For example, the medial prefrontal region in the left hemisphere, which is believed to host important functions such as attention and working memory, became proportionately larger in males early in the second year of postnatal life.
The analysis also showed that the patterns of cortical surface area expansion in this early period of life were very different from the patterns of cortical thickness development, suggesting that these two measures of brain development involve distinct mechanisms.
All in all, Li said, the mapping provides fundamental new insights into brain development.
He and his team now plan to extend this approach with MRI scan datasets that start at earlier ages and end at older ones. They also hope eventually to study scan datasets covering children who have autism-spectrum or other neurodevelopmental conditions. Such analyses might offer not only clues to the origins of these conditions, but also the identification of early signs or biomarkers, which in the future could be used to administer early and more effective treatments.
FDA Authorizes Omicron-Targeted Booster Shots
Monovalent mRNA Booster shots no longer authorized as boosters in people 12 and up

The FDA on Wednesday authorized bivalent COVID-19 booster shots from Pfizer/BioNTech and Moderna that target the original strain along with the Omicron BA.4/BA.5 subvariants.
In an amendment to the emergency use authorizations (EUAs), both shots can be administered starting 2 months following a primary vaccination series or prior booster — in people 12 and up for Pfizer’s shot and in people 18 and up for Moderna’s vaccine.
“The FDA has been planning for the possibility that the composition of the COVID-19 vaccines would need to be modified to address circulating variants,” Peter Marks, MD, PhD, of FDA’s Center for Biologics Evaluation and Research, said in a statement. “We sought input from our outside experts on the inclusion of an omicron component in COVID-19 boosters to provide better protection against COVID-19. We have worked closely with the vaccine manufacturers to ensure the development of these updated boosters was done safely and efficiently.”
Of note, clinical data supporting the EUA amendment were derived from studies on bivalent vaccines that targeted the original Omicron strain, but the agency said it considers such data as “relevant and supportive” of the newer BA.4/BA.5-targeted vaccines.
Support for the vaccines’ efficacy came in the form of immunogenicity data. The studies for each vaccine involved about 600 fully vaccinated adults who had already received a booster shot as well. Immune responses to BA.1 were superior in individuals receiving either of the companies’ bivalent vaccines — which included components targeting the ancestral strain as well as Omicron BA.1 — compared to those that received the original monovalent boosters targeting only the original strain.
This rollout is “similar to situations we’ve done in the past with influenza strain changes … we don’t do clinical studies for them in the United States,” Marks said during a press briefing on Wednesday.
“To stave off serious outcomes and symptomatic disease, one needs to refresh the immune system with what is actually circulating,” he said. “BA.1 is no longer circulating.”
CDC’s variant proportions tracker shows that the BA.5 Omicron subvariant makes up 88.7% of cases in the U.S., while BA.4 makes up 3.6% and BA.4.6 makes up 7.5% of cases.
Prior research in individuals infected with BA.4 or BA.5 has demonstrated robust protection against a variety of other variants, including BA.1, Delta, and Beta, Marks noted.
“The hope here is that by increasing the amount of antibodies we have to that particular variant, we will restore the protection we had when these [vaccines] were launched — that is the goal here,” he said.
Safety data for Wednesday’s authorization were derived from studies on the BA.1-targeting bivalent vaccines in 800 adults 18 and up for Moderna’s shot and in 600 adults 55 and older for Pfizer’s. Commonly reported side effects for the vaccines included injection site pain, redness, and swelling, lymph node swelling in the arm of the injection, as well as chills, fever, fatigue, headache, muscle or joint pain, and nausea or vomiting.
“We are confident in the evidence supporting these authorizations,” he said.
Monovalent mRNA vaccines that target the original SARS-CoV-2 strain will no longer be authorized as boosters in people 12 and up, the agency said.
Marks said he expects the FDA will authorize bivalent boosters for children in the next month or two.
Before shots can go into arms, the CDC’s Advisory Committee on Immunization Practices (ACIP) will need to weigh in with their recommendation
Here’s What to Know About Fall COVID Boosters
Experts confident in safety, but questions remain about efficacy

The CDC’s Advisory Committee on Immunization Practices (ACIP) will weigh in on newly authorized fall COVID boosters this week, in a manner unprecedented during the pandemic — without data from human clinical trials.
While most experts agree that there are no safety concerns, and many support the FDA’s attempt to keep up with viral variants, others have pointed out gray areas and open questions when it comes to Omicron-targeting bivalent vaccines.
That includes whether boosters with components targeting Omicron would offer a significant advantage in terms of efficacy — particularly, protection against infection — over boosting against the ancestral strain of the virus alone.
Regulatory Recap
To recap, the regulatory process for fall boosters started earlier this summer. On June 28, the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) voted 19-2 to recommend the use of an Omicron-specific component in future boosters. Their review was based on human clinical trial data from a bivalent booster containing the ancestral strain and the BA.1 variant, showing sufficient levels of neutralizing antibodies after the fourth dose.
But most committee members voiced support for a bivalent vaccine that included the ancestral strain plus the BA.4/5 variants, even though data from a human clinical trial wouldn’t be available before fall.
That would make the authorization process for this and possibly future COVID boosters similar to that for annual influenza vaccines, which relies on immunogenicity data from mouse studies.
Indeed, Pfizer has presented data from a mouse study, showing that BA.4/5 monovalent and bivalent boosters sufficiently raised neutralizing antibody levels against all Omicron variants.
Pfizer and Moderna are both starting human clinical trials of BA.4/5 boosters this month — a 30-mcg dose for Pfizer and a 50-mcg dose for Moderna — but those won’t be concluded before shots likely start going into arms in the coming weeks.
The Unknowns
While proponents tout the positives of moving quickly, others have raised several concerns, including not knowing whether a BA.4/5 boost will offer better protection against infection than another boost with the ancestral strain.
Paul Offit, MD, of Children’s Hospital Philadelphia, who participated in the June 28 VRBPAC meeting, told MedPage Today that the human data on BA.1 boosters were “underwhelming.”
Depending on the company, he said, there was a 1.5-fold to 1.75-fold increase in neutralizing antibody titers in the group that got the bivalent vaccines, and that’s “not likely to be a clinically significant difference.”
That could be related to “imprinting,” Offit said, which is also referred to as “original antigenic sin.” The concept is that the immune system response is bolstered against the strain that a person was initially exposed to.
“You largely are hooked into that ancestral strain, so it’s hard to boost in a big way with BA.4/5 vaccines,” Offit said. “If I gave a monovalent BA.4/5 vaccine to a 10-year-old with no previous vaccination or natural infection, you’d see a dramatic increase in neutralizing antibodies.”
Offit maintains that boosters aren’t needed in healthy adult populations at all because T-cell responses are conserved and recipients are thus protected against severe disease. Boosters, he said, are beneficial in at-risk groups: older patients (above 70), those with chronic conditions, and the immunocompromised.
John Moore, PhD, professor of microbiology and immunology at Columbia University in New York City, noted that the Pfizer mouse study data actually suggested better results with a monovalent BA.4/5 booster. Thus, it’s not clear why a monovalent booster isn’t moving forward at this time, he said.
Moore added that recent modeling data — albeit, a preprint, and not clinical data — suggest there wouldn’t be much of a difference in outcomes if people received a booster of the ancestral strain versus the Omicron-targeted booster.
“A great deal of time, effort, and money have now gone into making new boosters that will be little better than what we already had available in large quantities,” Moore told MedPage Today in an email.
He added it would be a “mistake if the public was persuaded that the new boosters are a super strong shield against infection, and hence increased their risk and exposed themselves to more virus.”
Several experts also expressed concerns that if the public perceived that the bivalent boosters were problematic because they only have animal data behind them, hesitancy could increase. That’s troubling given that only about 30% of the U.S. population has taken a booster dose, they said.
Still others think FDA is on the right track. Robert “Chip” Schooley, MD, an infectious diseases expert at the University of California San Diego, told MedPage Today in an email, “I think the call was the right one.”
“Coronavirus-induced immunity (whether vaccine- or infection-driven) wanes quickly and we have a large number of unboosted and under-boosted people in the population and are poised for a recrudescence of infection as people go indoors for the winter,” Schooley said. “Thus, there is not time for a comparative trial with clinical efficacy endpoints before the need to roll vaccination out in anticipation of the winter surge.”
He said he would have liked to see a clinical trial “embedded in the fall rollout in which people were randomized to a ‘legacy’ vaccine or a new one with a subset of patients being studied for immunogenicity versus a range of variants and clinical outcomes in the full cohort” — but that he wouldn’t advocate “continuing with the legacy vaccine for the next 6 months, which is what would be required to do a properly controlled clinical trial.”
He concluded that COVID vaccines are “likely headed toward where flu vaccines have gone.”
That certainly seems to be a foregone conclusion, as Biden administration officials have already touted the value of Omicron-targeted bivalent boosters. White House COVID-19 Response Coordinator Ashish Jha, MD, MPH, called it the “first major upgrade of the vaccines … in the last two and a half years.”
CDC Director Rochelle Walensky, MD, MPH, told the podcast Conversations on Health Care that bivalent boosters “shouldn’t impact safety at all.”
If the country waits for human data, she said, “we would be using what I would consider to be a potentially outdated vaccine. … It’s best to use a vaccine that’s tailored to the variant we have right now.”
