A research team at the Leibniz Institute for Natural Product Research and Infection Biology – Hans Knöll Institute (Leibniz-HKI) in Jena, Germany has developed a new method to produce complex natural products in amoebae. These polyketides include various antibiotics but also olivetolic acid, a precursor of the herbal active ingredient tetrahydrocannabinol (THC).
Polyketides are natural products with a wide range of therapeutic applications. Among them are dietary supplements, various antibiotics such as erythromycin, and one of the key cannabinoid precursors: Olivetolic acid. It is needed for the synthesis of tetrahydrocannabinol (THC). The medical use of this psychoactive substance is being intensely researched, and it is already being used to provide relief for patients with neurological diseases and pain, among other things.
THC is a natural ingredient in the cannabis plant. “However, isolating THC in its pure form from the abundance of substances is very complex,” says Falk Hillmann, head of the junior research group “Evolution of Microbial Interactions” at Leibniz-HKI and coleader of the study. Chemical synthesis of THC on the other hand is expensive and the yield is low. That’s why he and a team are researching how such plant substances can be efficiently produced biotechnologically.
“So far, bacteria such as Escherichia coli or the yeast Saccharomyces cerevisiae are mainly used, but neither of them are native producers of natural products,” explains Vito Valiante, head of the cooperating junior research group “Biobricks of Microbial Natural Product Syntheses” at the Leibniz-HKI. Accordingly, a large number of genetic modifications is necessary to enable synthesis in these classic model organisms. The research team is thus looking for alternatives. One promising candidate is the amoeba Dictyostelium discoideum, which already possesses numerous biosynthetic genes for the production of natural products such as polyketides. “Taking a closer look at the genes, we noticed that some show a high similarity to plant biosynthetic genes,” said first author Christin Reimer, who is working on the topic for her PhD.
To test how well D. discoideum is suited as a chassis organism for biotechnological production, the researchers first had the amoeba produce the food supplement resveratrol, also a polyketide. Afterward they incorporated the plant enzyme that produces the THC precursor olivetolic acid into the amoeba’s genome. However, the addition of chemical precursors was still necessary to enable the synthesis.
To circumvent this, the researchers took advantage of the amoeba’s natural properties and combined the plant enzyme with an amoebic enzyme. “The amoeba is able to produce the required precursor, a hexane unit, directly on site,” Hillmann explains. Thus, the research team succeeded in producing a functional inter-kingdom hybrid enzyme that produces olivetolic acid without any further additives.
“Through our research, we have shown that the amoeba Dictyostelium can be used as a biotechnological production platform for polyketide-based natural products,” says Reimer. The researchers already filed a patent for the process, and are striving to improve it on an ongoing basis. “Our next goal is to insert the two enzymes that are still missing in order to be able to produce the final product THC in the amoebae,” Hillmann says.
Moreover, a team from the Bio Pilot Plant at the Leibniz-HKI was also involved in the research. Johann Kufs, joint first author of the study alongside Reimer, is in charge of developing and optimizing the synthesis process for industrial application.
The side effects of cancer therapy continue to cause significant health and cost burden to the patient, their friends and family, and governments. A major barrier in the way in which these side effects are managed is the highly siloed mentality that results in a fragmented approach to symptom control. Increasingly, it is appreciated that many symptoms are manifestations of common underlying pathobiology, with changes in the gastrointestinal environment a key driver for many symptom sequelae. Breakdown of the mucosal barrier (mucositis) is a common and early side effect of many anti-cancer agents, known to contribute (in part) to a range of highly burdensome symptoms such as diarrhoea, nausea, vomiting, infection, malnutrition, fatigue, depression, and insomnia. Here, we outline a rationale for how, based on its already documented effects on the gastrointestinal microenvironment, medicinal cannabis could be used to control mucositis and prevent the constellation of symptoms with which it is associated. We will provide a brief update on the current state of evidence on medicinal cannabis in cancer care and outline the potential benefits (and challenges) of using medicinal cannabis during active cancer therapy.
Despite the excitement that surrounds newer, more targeted agents, the reality for most people with advanced cancer is that chemotherapy will be used, and it will cause a degree of collateral damage to healthy tissues [1]. Clinically, this damage presents as a broad variety of diverse, individualised, and highly dynamic symptoms and side effects. Rarely do these side effects occur in isolation; instead, they present as clusters of related symptoms that are united by common underlying mechanisms, as well as physical and psychosocial/behavioural determinants [2]. With increased accessibility of “big”, real-world data, these symptom clusters have been documented and characterised with greater precision [3]. This has prompted new initiatives to identify early drivers of chronic treatment-related morbidity, with the goal of halting the self-perpetuating nature of inter-related symptom clusters.
Of the many documented side effects of chemotherapy, the breakdown of the mucosal barrier of the gastrointestinal tract (“mucositis”) is one of the earliest and most common. Mucositis is initiated by rapid and extensive DNA damage in highly proliferative stem cells throughout the gastrointestinal mucosa [4]. The resulting apoptosis and inflammation degrades the mucosa, leading to the formation of ulcerative lesions in the mouth, oesophagus, intestines and rectum which severely impair functional capacity. This dysfunction can lead to taste changes, dysphagia, pain and malabsorption; each of which drive anorexia, malnutrition and dehydration [5]. On a cellular level, these breaches in the protective mucosa create an inhospitable environment for resident gut bacteria, leading to loss of commensal species and their protective metabolites including short-chain fatty acids (SCFAs). These changes further weaken the mucosal barrier and permit unrestricted communication between the underlying immune system and luminal compounds (e.g., danger signals). This results in profound local and systemic inflammation which leads to numerous extraintestinal consequences such as fever (“febrile mucositis”) [6], cognitive impairment [7, 8] and fatigue [9]. As such, the destructive changes in the gastrointestinal microenvironment position mucositis as a catalyst for a range of secondary complications, and a key player in a range of symptom clusters.
Despite the impact of mucositis on patients and the healthcare system, it remains without effective intervention, and its range of secondary symptoms/consequences are managed reactively and in isolation [10]. Given the body of evidence that now suggests many symptoms and treatment consequences may be influenced by mucositis, there is an opportunity to control mucositis to mitigate the constellation of impactful symptoms with which it is associated. This review aims to outline a rationale for how, based on its already documented effects on the gastrointestinal microenvironment, medicinal cannabis could be used to control mucositis and prevent its associated symptom cluster. We will provide a brief update on the current state of evidence on medicinal cannabis in cancer care and outline the potential benefits (and challenges) of using medicinal cannabis during active cancer therapy.
Medicinal cannabis: illicit drug, plant, or medicine?
Cannabis has been used medicinally for over 3000 years, primarily for its analgesic properties. The predominant phytocannabinoids in cannabis by amount are Δ9-tetrahydrocannabinol (Δ9-THC or THC) and cannabidiol (CBD), with mainstay medicinal cannabis (MC) preparations containing either or both of these compounds in varying ratios as the active ingredients, either as isolates or whole extracts. However, there remains a vast phytochemical complexity to cannabis aside from just THC and CBD, whereby whole extracts may contain over one hundred different minor phytocannabinoids and terpenes, all of which may vary in their relative expression across a number of cannabis chemotypes and displaying variable retention via different extraction processes [11, 12]. Many of these compounds have been shown to exhibit selective bioactivities that may interact with the efficacy of THC and CBD in MC preparations and may be considerations particularly where full-spectrum botanical extracts are concerned, oft described through the popular term ‘entourage effect’ applied to medicinal cannabis [13, 14]. However, their contribution to the efficacy of most conventional MC formulations where THC and CBD predominate may only be marginal, with a paucity of investigative studies on these cannabis phytochemicals compared to THC and CBD.
Today, over 40 countries have legalised MC, with different access pathways depending on jurisdictional legislation [15]. Despite significant variation across jurisdictions, the medicinal use of cannabis is guided by the formulation (oil, sprays, tablets and flowers). Typically, MC requires prescription for a pre-defined indication or with clear clinical justification for why a certain condition may respond positively to MC. This ambiguity often results in lengthy and administratively burdensome reporting requirements; hence, MC use continues to be a challenging medico-legal entity. The combination of its often high cost, clinician hesitancy and logistic difficulties for supply compared to relative ease of access in the community, is a major driver of why people continue to self-medicate with uncontrolled and non-standardised cannabis products.
Canada was one of the first countries to introduce a MC access programme in 1999. Between 2015 and 2019, the number of registered MC patients in Canada increased from 40,000 to nearly 400,000, an increase attributed to several policy changes that have gradually broadened access to a variety of medicinal cannabis formulations. In December 2015, the first cannabis oil product was launched in the Canadian market and in 2016, the Access to Cannabis for Medicinal Purposes Regulations allowed patients to grow cannabis for personal use [16].
The United States was another early adopter of medicinal cannabis, starting with state-level legalisation in California in 1996. Now, as of February 2023, medicinal cannabis has been legalised in 37 states, 3 territories, and the District of Columbia [17]. In February 2019, Thailand became the first and only nation in Southeast Asia to legalise medicinal cannabis, offering three different categories of cannabis-based products: medicinal-grade cannabis-based medicines, Thai traditional medicine products that contain cannabis as the active ingredient, and folk medicine products prepared by registered folk healers [18].
In 2016, cannabis was rescheduled in Australia to enable access for medicinal purposes. Currently, the majority of cannabis products are classified as “unapproved” therapeutic goods, with two exceptions: Sativex (nabiximols), an oromucosal spray containing equivalent amounts of THC and CBD, and Epidyolex (also known as Epidiolex), a CBD solution with a concentration of 100 mg/mL (Therapeutic Goods Administration, 2020a). The situation in the UK is similar; even though medicinal cannabis was legalised in 2018, it remains challenging for patients to obtain access, with only a limited number of National Health Service prescriptions issued to date [19]. Medicinal products that meet safety, quality and efficacy standards are registered on the Australian Register of Therapeutic Goods (ARTG), however additional pathways such as Special Access Schemes (SAS) and an Authorised Prescriber (AP) scheme facilitate patient access to “unapproved” therapeutic goods, including many other types of MC products currently. This scheme is being increasingly adopted in Australia, with the MC Therapeutic Goods Administration (TGA) dashboard showing an increase in AP applications and a levelling off of SAS-B approvals in the last 2 years.
The “endocannabinoidome” and its relevance to chemotherapy symptoms and side effects
The endocannabinoidome or, in its broader sense, the endocannabinoid system (ECS), is an endogenous network of receptors, enzymes, transporters and ligands, that has largely been recognised for its role in regulating of neurotransmitter release [20]. However, this original concept of the ECS is gradually being replaced by an increasingly sophisticated and complex network capable of regulating numerous biological pathways and functions across a range of organ systems. The interactions that exist within the ECS are critical to central nervous system development, synaptic plasticity and the homeostatic maintenance of cognitive, behavioural, emotional, developmental and physiological processes [20, 21]. These diverse mechanisms are mediated by endogenous cannabinoids which are produced on demand, both physiologically and patho-physiologically, from membrane lipids and are metabolised by fatty acid amide hydrolase (FAAH) and monoacylglycerol lipase (MAGL), respectively [22]. They include the main known endocannabinoids, N-arachidonoylethanolamine (AEA) or anandamide and 2-arachidonoylglycerol (2-AG) produced by phospholipid precursors through activity-dependent activation of specific phospholipase enzymes; N-acyl-phosphatidylethanolamine-selective phosphodiesterase and phospholipase C subsequent production of diacylglycerol via diacylglycerol lipase, respectively [20]. The broadly termed acylethanolamines and acylglycerols interact to a variable extent with cannabinoid receptors including the well-described CB1 and CB2 receptors (CNR1/CNR2) as well as other G-protein-coupled receptors such as GPR55, GPR18, GPR3, GPR6, GPR12, transient receptor potential channels such as TRP vanilloids TRPV1 to TRPV4, TRP ankyrin TRPA1, TRP M member TRPM8 and peroxisome proliferator-activated receptors such as PPAR2, and PPARγ [23]. Although there are diverse receptors with which endocannabinoids interact, CNR1 and CNR2 are functionally characterised both physiologically and with respect to ECS dysfunction.
CNR1 is a G-protein-coupled receptor that is highly abundant within the peripheral and central nervous system, largely present on axon terminals and pre-terminal axon segments [24] (Fig. 1). It is highly abundant in medium spiny neurons in both the dorsal and ventral striatum, and is particularly high on the direct pathway axons as they enter the globus pallidus heading towards the substantia nigra [25]. However, the expression of CNR1 is increasingly diverse, with a range of immune cells (including glia) now understood to express CNR1 [26,27,28] as well as the more immunologically abundant, CNR2. Indeed, there remains debate about the expression of CNR2 which has historically been considered to be mainly expressed in the periphery [29]. Although emerging evidence suggests it is expressed on sensory nerve terminals and microglia in the brain [30].
Fig. 1: Simplified scheme representing the expression pattern of the main cannabinoid receptors, CNR1 and CNR2.
Although not the only components of cannabis, the most commonly studied and clinically utilised components, THC and CBD, are highly lipid soluble and have a poor bioavailability when inhaled (10–35%) or orally ingested and 11–45% [31,32,33]. When THC is consumed by inhalation or mucosal sprays, it is absorbed through the lungs into the bloodstream and concentrations in the plasma will typically peak in less than 10 min [31] and when it is orally congested, concentrations may peak at ~2 h. THC is distributed into well vascularises organs as well as the brain. THC and CBD are highly protein-bound and has a half-life of 25–36 and 18–32 h, respectively [31, 34], with some of the metabolites (THCCOOH) having a very long half-life up to 52 h [35]. Chronic users have much longer half-lives.
THC undergoes extensive first-pass metabolism in the liver by cytochrome P450 (CYP 450) isozymes; these enzymes are also responsible for the metabolism of many anti-cancer drugs and several other commonly used co-medication and are known to cause large inter-individual variability in plasma concentrations for majority of clinically used medications [36]. Therefore, it is particularly important to investigate any potential drug–drug interactions to avoid toxicity or therapeutic failure for any of the medications. THC primarily is metabolised via oxidation by CYP2C9, CYP2C19 and CYP3A4 into several metabolites with 11‐hydroxy‐THC (11‐OH‐THC) and 11‐carboxy‐THC (11‐COOH‐THC) being the most abundant [34, 37]. 11-OH-THC is metabolised by the UGT1A9 and UGT1A10 enzymes and 11-COOH-THC is metabolised mostly by the UGT1A3 and UGT2B7enzyme [34, 35]. CBD is also metabolised in the liver via mostly CYP3A4, CYP2C19 and CYP2C9 and other CYPs to a lesser degree via hydroxylation to form metabolites, 7-OH-CBD and 7-COOH-CBD, which is then undergoes glucuronidation by UGT1A9 and UGT2B7 [31, 34]. The remaining THC, CBD and metabolites can be taken up by fat tissue before it is redistributed into the circulation. More than 65% of THC and CBD will be excreted in faeces and ~20% in the urine [35, 37]. Metabolites excreted in urine have been observed to vary up to fivefold between individuals when drug administration was controlled, demonstrating the variability in metabolism [35].
Inter-individual differences in pharmacogenomics, pharmacokinetics and pharmacodynamics may explain contradictory outcomes from previous studies and accounting for such differences will provide an opportunity for personalised medicine where efficacy can be maximised, and toxicity minimised for various conditions or diseases [38].
Reflecting the breadth of cells upon which ECS receptors are expressed, the ECS regulates a number of critical functions that are well-known to contribute to the side effects of chemotherapy. Most notable is its psychotropic properties, modulating mood, anxiety, cognition, appetite, sleep and pain [39, 40]; all of which are well-documented to be negatively impacted by chemotherapy [1]. Peripheral CB1 expression is also implicated in gastrointestinal inflammation, mucosal defences and gastric motility [41,42,43,44], and thus by extension diarrhoea and constipation, due to its expression on presynaptic cell of sympathetic motor neurons innervating visceral organs leading to reduced noradrenalin release [45]. Further to this, given the immunomodulatory capacity of the ECS, its ability to influence numerous symptoms and side effects of chemotherapy of which many are underpinned by aberrant inflammation, is vast. It is for these reasons that medicinal cannabis, and strategies to augment the ECS, have gained considerable momentum for their potential benefits in people with cancer.
Medicinal cannabis use in cancer care: what is the evidence?
Cannabis use in people with cancer is not uncommon, although it remains difficult to determine exact prevalence due to heterogeneous results published across numerous studies with varied designs. In a study published in 2018, 43% of respondents (at a Canadian cancer centre) reported using “illicit” cannabis for a variety of symptoms and side effects of their treatment [46]. This is similar to a large population-based analysis from 2005 to 2014 in the US, which showed 40.3% of the 826 respondents with cancer having used cannabis in the last 12 months [47]. However, in a larger survey of more than 200,000 people, results indicated that less than 10% of people were using cannabis [48]. Irrespective of self-reported cannabis use, there is a high degree of interest in its potential benefits during cancer care, with 80% of healthcare professionals reporting that they have engaged in conversations with their patients about cannabis [49]. Unfortunately, less than 30% feel equipped to guide their patients citing a lack of clear evidence on its safety and efficacy [49]. This uncertainty undoubtedly stems from the inadequate and highly variable evidence base for cannabis in cancer care, which is dominated by largely observational studies that are subject to inherent biases, powerful placebo effects and diverse confounders, leading to a high rate of false positives [50,51,52]. Similarly, of the limited number of randomised control trials, few are considered high quality and they remain near impossible to compare/synthesise due to inherent differences in design, outcome measures and cannabis products/doses/delivery/formulations used [50]. This has prevented replication and meta-analyses, and the resulting evidence base is therefore inconsistent and largely uninformative.
Although challenging to compare studies, a large number of systematic reviews have been conducted in an attempt to synthesise data and determine its efficacy in symptom control. Notably, there have been few that have been able to perform meta-analysis, reflecting the heterogeneity of available data. The most recent review of cannabis in cancer care reviewed 42 studies (19 randomised, 23 non-randomised), focused on people with cancer receiving palliative care [53]. Among these studies, pain was the most commonly investigated symptom, with highly variable effects reported across the studies. This aligns with a recent systematic review and meta-analysis which investigated the effect of cannabis for pain management in people with cancer, which was unable to form any conclusive recommendation [54]. Accordingly, recent guidelines from the Multinational Association for Supportive Care in Cancer (MASCC) do not recommend the use of cannabinoids for cancer pain, although, it is unclear how this relates to chemotherapy-induced pain which is diverse in its origins [52].
While pain has dominated the landscape for cannabis research in cancer care, emerging evidence exists for its role in chemotherapy-induced nausea and vomiting (CINV), anorexia, cachexia, sleep disturbance and psychological symptoms (depression/anxiety). Doppen and colleagues reviewed the evidence for CINV, reporting generally positive effects across multiple studies using various assessment tools [53]. This is consistent with recommendations from MASCC, which show THC and nabilone are both effective in controlling CINV, however, no more effective than current antiemetic medications [55]. Despite these positive findings, MASCC was unable to form any guideline due to insufficient, high-quality evidence. This is echoed by the American Society for Clinical Oncology (ASCO) who question the quality of current evidence [56]. Despite the lack of clinical recommendation from MASCC and ASCO, it appears that there is discordance between published clinical trial data and anecdotal reports of patient preferences, which tend to favour cannabis over existing antiemetic strategies, even when adverse effects were higher [57, 58].
MASCC maintains a similar stance with respect to anorexia and cachexia, with limited evidence available to inform relevant guidelines. Doppen et al. reviewed 15 studies for cannabis and appetite, with both objective and self-reported benefits reported for nabinol and Marinol, however, several studies reported no or inconsistent effects [53]. Given the heterogeneity in data and approaches, it remains difficult to draw robust conclusions despite the popularised effects of cannabis on appetite stimulation. Similarly, for psychological effects (e.g., on sleep, anxiety, depression), MASCC were unable to make any recommendations with most studies investigating these outcomes as secondary analyses with inconsistent data across studies [51].
While the systematic review by Doppen et al. has provided insight on the current state of evidence regarding cannabis use in cancer care, it has been scrutinised for its methodology and over-simplification of data as “positive” and “negative” effects based on the null hypothesis significance test [50, 53]. As cautioned by Davis and Soni (2022), our approach to cannabis research should be guided by effect sizes that are deemed clinically significant, rather than statistically significant [50]. Furthermore, they highlight the need to be more holistic in our assessment of cannabis for symptom management, avoiding excessively large studies designed with highly restrictive outcomes guided by narrow-minded criteria [50]. With this in mind, and the growing appreciation for symptom clusters in people undergoing chemotherapy, there is a clear rationale to prioritise trial designs that address clusters of related symptoms, rather than single symptoms, to deliver meaningful impacts to the participant’s physical or psychosocial well-being. Critical to these approaches is the inclusion of consumers in cannabis research, to ensure research methodologies are informed by, and consistent with, consumers behaviours and preferences. In line with ensuring consumer engagement, trials should include relevant patient reported outcome measures (PROMs) to ultimately determine if cannabis has a meaningful impact on people with cancer.
Gastrointestinal effects of cannabis: can they be adapted to control mucositis?
Cannabinoids, including both CBD and THC, are increasingly documented for their capacity to modulate gastrointestinal function, owing to the immense control that the ECS has on gastrointestinal homeostasis. Both CNR1 and CNR2 are present in the gastrointestinal tract, largely on enteric nerves and the epithelium, but also on enteroendocrine cells and immune cells [42]. This network of ECS receptors controls gastric motility, and as such, it is now understood that variants in the genes encoding for CNR1 are implicated in diseases characterised by altered motility including irritable bowel syndrome (IBS), particularly diarrhoea-predominant [59]. Both CNR1 and CNR2 are expressed in the gut at medium to high degrees, respectively. Accordingly, it has been shown that agonists of the cannabinoid receptors (CNR1 and CNR2) [60, 61], as well as targeting endocannabinoid degradation [62], minimises experimental colitis and associated visceral hypersensitivity [63]. Furthermore, preclinical investigations have shown that potent agonists of CNR1 (without central nervous system effects) and CNR2 have been shown to control increased gastrointestinal motility caused by stress [64] and inflammation [44]. Similarly, inhibition of anti-diacylglycerol lipase (DAGL) and fatty acid amide hydrolase (FAAH)—two enzymes critical in endocannabinoid metabolism—has been shown to normalise transit time in the context of opioid-induced constipation [65]. Of particular interest to changes in the gastrointestinal microenvironment associated with mucositis is the ability of CNR2 activation [66] and FAAH inhibition [67] to control accelerated gastrointestinal motility induced by lipopolysaccharide—a bacterial product that is causally implicated in chemotherapy-induced diarrhoea.
In addition to its effect on gastrointestinal motility, which has clear applications in controlling chemotherapy-induced diarrhoea, the ECS exerts potent immunomodulatory effects in the gastrointestinal tract controlling intestinal inflammation [41]. Both synthetic CB receptor agonists and endocannabinoids have been shown to impair cellular and humoral immunity by reducing inflammatory cell recruitment, inducing T-cell apoptosis and suppressing the production of numerous pro-inflammatory cytokines and chemokines (e.g., TNF-α, IL-1β, IL-2, IL-6, IL-17, IFN-γ, CCL2 or CXCL10) [41, 68]. Therapeutically, both exogenous administration of cannabis and preventing endocannabinoid degradation by inhibiting FAAH have been shown to reduce colitis [60,61,62,63, 69]. In fact, FAAH inhibition and CB receptor activation have shown efficacy in mouse models of colitis and FAAH knockout mice are less susceptible to experimentally induced colitis compared to wild-type mice [69]. The ability of endocannabinoids (or exogenous cannabis products) to accelerate wound healing in the gut points to their ability to promote intestinal/mucosal barrier function, that is, the bonding of intestinal epithelial cells to create a uniform and restrictive barrier. This mechanism has been confirmed in vitro, with cannabinoids improving or maintaining paracellular permeability (i.e., leakiness) and tight junction protein expression in Caco-2 cells treated with Clostridium difficile toxin A and other barrier-directed insults (e.g., cytokines, EDTA) [41, 70]. These mucoprotective effects have also been reported preclinically, with cannabinoids reported to decrease intestinal permeability (and increase regulatory T-cell recruitment) in experimental colitis induced by dextran sulfate sodium (DSS) [41]. It has also been suggested that cannabinoids can modulate secretory processes in the intestinal epithelium which, when dysregulated, lead to altered osmotic forces and potentially diarrhoea [71,72,73,74].
An emerging area of interest with respect to the gastrointestinal microenvironment is the interaction between the ECS, cannabis and the gut microbiota [43, 75, 76]. The gut microbiota is a collection of micro-organisms (bacteria, viruses and fungi) that reside in the gastrointestinal lumen and mucosal niches, regulating host physiology and immune function. Importantly, these beneficial host-directed effects are best achieved when there is high microbial diversity and enrichment for commensal microbes. Chemotherapy indirectly impacts the diversity and composition of the gut microbiota, through the destruction of their mucosal niches and oxidative stress [77]. As such, a highly dysbiotic microbiota is a hallmark trait of chemotherapy, and an event documented to drive a range of adverse effects including fever, infection, diarrhoea, cachexia, weight loss, anxiety, cognitive impairment, cardiotoxicity and fatigue. Although a relatively new concept, emerging data suggests an interaction between the ECS and the gut microbiota. Most recently, cannabis extracts (CN1, CN2, CN6) were shown to increase microbial diversity and richness in a mouse model of metabolic disease whilst promoting enrichment of microbial taxa associated with health [78]. Further suggesting an ECS-microbiota interaction is the finding that germ-free mice (mice without a microbiota) are deficient in a number of ECS components, including the CNR1 [79]. A microbial taxa of particular interest is Akkermansia muciniphila, a mucus-degrading microbe implicated in gut inflammation [80] and chemotherapy side effects [81, 82]. This microbe is reportedly elevated in response to CNR1 antagonism with the compound SR141716A, although this was only demonstrated in obese mice [76, 83]. Despite this emerging evidence, it is unclear if medicinal cannabis influences the gut microbiota and if this mechanism underpins/delivers meaningful impacts for the host.
Collectively, this body of evidence strongly demonstrates the profound control that the ECS exerts on gastrointestinal function, regulating motility, barrier function and repair, immune function, secretion and potentially the microbiota. These data underscore the potential mucoprotective effects of exogenous cannabinoid administration or augmentation of the ECS. In the context of cancer care, this therefore supports strategies targeting ECS (via direct cannabinoid administration or inhibition of degradation) to control mucositis and promote a more resilient gastrointestinal microenvironment. Despite the scientific strength of this rationale, and the prevalence of mucositis (occurs in ~60% of patients treated with standard chemotherapy), there have been few attempts to explore the mucoprotective properties of medicinal cannabis in cancer care [55]. This may reflect the complexities of using/investigating medicinal cannabis during active cancer treatment.
Using medicinal cannabis during active cancer treatment: precautions, challenges and potential benefits
To minimise both the depth and duration of mucositis, supporting the gastrointestinal microenvironment and controlling the constellation of symptoms with which mucositis is associated, medicinal cannabis should be used during active chemotherapy treatment. Of course, this raises some concerns regarding the possibility of adverse drug interactions with anti-cancer therapies and potential loss of anti-tumour efficacy. There has been limited investigation of how cannabis influences the anti-tumour efficacy of cancer treatment. Cannabis has been investigated for its effect on the pharmacokinetics of irinotecan and docetaxel, with no effects observed [84]. On the other hand, two recently reported observational studies indicate a negative impact of cannabinoids on immune checkpoint inhibitors (ICI) related cancer outcomes [85, 86]. Bar-Sela et al. highlighted in a prospective study that the concomitant use of prescribed cannabis was associated with lower response rates (39% vs 59%), median time to progression (3.4 months vs 13.1 months) and median overall survival (6.4 months vs 28.5 months) when compared to ICI therapy alone [85]. Another retrospective observational study from the same research group reported inferior outcomes for cannabinoid use along with nivolumab (an ICI) when compared to nivolumab among selected solid cancers [86]. While some evidence suggests that cannabis may impair the anti-tumour efficacy of immunotherapy [87, 88], recent evidence suggests cannabis may actually have a synergistic effect with immunotherapy. This has been shown both preclinically and clinically, with median survival in CT26 tumour-bearing mice treated with THC and an anti-PD1 antibody having significantly higher overall survival compared to controls [89]. Authors also reported higher overall survival (numerical, failed to reach statistical significance) in 201 people with non-small cell lung cancer undergoing monotherapy with pembrolizumab who used medicinal cannabis. Although this does not confirm a synergistic effect, it does indicate no detrimental effect. The only study in which a definite synergy has been identified was preclinical, where a combination of cannabigerol and anti-PD-1 resulted in enhanced tumour clearance and increased survival compared to monotherapy in tumour-bearing mice [90]. Given the evidence from low quality clinical trials, well conducted trials are required to assess the efficacy of cannabinoids as anti-cancer therapeutics either alone or in combination with other systemic cancer therapies.
In the context of chemotherapy, although there is no concrete evidence that suggests cannabis may impair its anti-tumour efficacy, given the increasing evidence for immune-mediated mechanisms enhancing chemoefficacy [91], this risk cannot be ignored and should be appropriately built into studies investigating medicinal cannabis in combination with standard chemotherapy. Although it remains exclusively experimental and prone to inflation, there is a growing body of evidence that suggests medicinal cannabis may in fact be a beneficial adjunct to standard chemotherapy, capable of inducing cell death or controlling proliferation by inducing endoplasmic reticulum (ER) stress [92, 93], proteosome inhibition [94], upregulation of matrix metalloproteinases [95] and reactive oxygen species activation [96]. In line with these findings, several studies have outlined the potential for cannabinoids to be used as anti-cancer agents either on their own or in combination with other systemic cancer therapies or radiotherapy [97, 98]. A recent review summarised the anti-cancer effects of cannabinoids to be mediated through multiple pathways including anti-proliferative, pro-apoptotic, pro-autophagy, anti-invasion and metastasis, anti-angiogenesis, and immunomodulation [99]. However, it is important to note that the majority of these findings have only been explored in vitro or in preclinical (animal) models and are subject to inflation in the public domain. As a result, these benefits have not been robustly translated into the clinical setting.
Three human clinical trials reported the results on the role of cannabinoids on patients with recurrent glioma [100,101,102]. Guzman et al. demonstrated that only two of nine patients with recurrent Glioblastoma (GBM) had reduced tumour proliferation when treated with intracranial Δ9-THC alone as monotherapy [100]. Another trial that combined Nabiximols (a mixture of plant-derived THC, CBD and non-cannabinoid compounds) with temozolomide (N = 27) resulted in a numerically higher 2-year overall survival (50% vs 22%, P = 0.13) when compared to placebo/TMZ [101]. Schloss et al. compared two different doses of THC/CBD combination as adjunct to standard treatment of recurrent high-grade gliomas (N = 88) and demonstrated an improved quality of life and an imaging-assessed tumour response in 11% while 34% had stable disease when compared to historical controls [102]. These clinical trials highlight that a small proportion of people with recurrent GBM may benefit from cannabinoids, however, there are no available predictive biomarkers that may identify responders and non-responders.
In addition to the impact on anti-tumour efficacy, the other main risk associated with medicinal cannabis use in parallel to active treatment is drug–drug interactions. Given the predominant role of MC for pain control in cancer care, its interaction with other analgesics is of interest. Evidence suggests that cannabis may in fact enhance opioid-induced analgesia, with synergistic analgesia observed when opioid/cannabinoid ligands are co-administered. In animal studies, either morphine or codeine produces synergistic antinociception when combined with THC [103,104,105,106], and similar synergies have been documented in humans [107]. However, these benefits must be taken in light of evidence that suggests this combination may increase tolerance to both forms of analgesia and increase the risk of “drug-liking” effects [88, 108]. There is also evidence to suggest drug–drug interactions between CBD and the non-steroidal anti-inflammatory, naproxen, although this is limited to in vitro evidence [109]. However, both CBD and THC are metabolised by CYP2C9, suggesting the possibility of impaired drug clearance [109] or renal/liver toxicity. However, there are no data to suggest CBD and THC cause renal/liver toxicity, and in fact there is data to suggest hepatoprotective effects [110] and prevention of cisplatin-induced renal toxicity [111]. However safety profiles of MC in the context of cancer care remains superficially addressed, underscoring the importance of regular renal and liver function tests, appropriately titrated dosing, and studies with co-primary endpoints that address efficacy and safety [88]. These studies should also endeavour to capture the patient experience with respect to milder adverse events such as dry mouth and fatigue/somnolence, given their association with both cancer therapy and MC.
While medicinal cannabis use during active chemotherapy presents some challenges, if approached carefully, there are a number of benefits that can be achieved. These benefits largely relate to the ability to control multiple symptoms early in their aetiology, rather than therapeutically targeting single symptoms that may have developed and persisted well after treatment ends. This holistic approach to controlling multiple symptoms is in line with recent suggestions by the MASCC, and also aligns with the scientific evidence that underpins the clinical phenomenon of symptom clustering [112,113,114].
We have outlined a clear rationale for how medicinal cannabis products, or augmentation of the ECS, modulates gastrointestinal function and exerts mucoprotective effects. It is therefore well positioned to target numerous mechanisms known to be involved in mucositis pathobiology and symptomatology. Given the documented role of mucositis and associated changes in the gastrointestinal microenvironment (e.g. gut microbiota dysbiosis) driving a range of intestinal and extraintestinal symptoms, medicinal cannabis in the active stages of chemotherapy may deliver broad-reaching benefits. This is particularly compelling when considering that medicinal cannabis, and the ECS, will likely have paralleled effects on these associated symptoms. For example, mucositis can cause taste changes and pain, leading to reduced oral intake (anorexia) and therefore clinically impactful weight loss. As such, targeting mucositis with cannabis, whilst simultaneously promoting food enjoyment and behaviours, will likely deliver meaningful impacts of weight maintenance and nutritional status. Similarly, diarrhoea and pain due to mucositis is anecdotally thought to cause sleep disturbances [115]. Again, by addressing a biological cause and providing symptomatic relief, the potential for meaningful impacts on patient quality of life is enhanced. This same framework can be applied to numerous, interacting consequences of mucositis and associated symptoms (Fig. 2).
Fig. 2: The centrality of gastrointestinal mucositis to infectious (orange), gastrointestinal (green) and neuropsychological (purple) symptoms commonly reported in people with advanced cancer undergoing chemotherapy.
By approaching symptom management in this manner, the magnitude of benefit is likely to be larger, and thus the health and well-being of people undergoing chemotherapy better maintained. This will deliver knock-on effects to patients, ensuring they remain in the workforce, thus reducing personal financial toxicity, and remain willing/capable of receiving their intended chemotherapy dosing ensuring optimal tumour response and progression-free/overall survival. This indirect effect on treatment efficacy is significant and should not be disregarded. For example, in a recent review of 874 women with advanced breast cancer, chemotherapy dose reductions of >15% significantly increased the risk of mortality [116]. Similarly, a reduction in total cumulative dose of neoadjuvant FEC-D (where it is <85% of intended dosing) decreased the length of survival in women with breast cancer [117]. Similar effects have been reported in ovarian cancer and colon cancer [118,119,120].
When considering the causes of dose reductions or modifications, adverse effects (i.e., side effects) are the most common cause, accounting for 82% of all dose reductions in a recent audit of 584 people undergoing adjuvant chemotherapy for stage III colon cancer [119]. As such, the provision of proactive supportive care that tackles symptom clusters at multiple points in their aetiology and progression is critical. In fact, the provision of supportive care early in symptom aetiology is recommended, with evidence illustrating both quality of life and survival benefits when this approach is adopted [121]. Furthermore, by addressing multiple symptoms concurrently, or targeting common underlying mechanisms of multiple symptoms, polypharmacy (5+ medications) can be reduced. More than 80% of people with advanced care report polypharmacy [122]. This approach is fragmented and places substantial burden on the patient who must navigate multiple medications, increasing their risk of adverse drug interactions and medical misadventure [123]. With recent calls to address the fragmented approach to supportive cancer care and symptom control [124], the ability of MC to transcend multiple symptoms is compelling and advantageous.
In considering how MC can be used to deliver substantive impacts for people undergoing chemotherapy, a number of practical matters must be carefully considered. Firstly, there are a range of cannabis extracts that are available for consumption in a variety of formulations ranging from dry leaves/buds which can be smoked or vaporised, to highly purified and processed isolates [125, 126]. Typically, the more readily accessible cannabis products are in the community, the lower the degree of purification and quality assurance. In light of high rates of self-reported use [16, 46, 48], this underscores the need to deliver evidence that (if shown to be beneficial) will ensure patients can access MC in more appropriate and safe formulations.
Cannabis is commonly available as an oil, which contains or is enriched for CBD and THC, typically in combination with many other cannabinoids and phytochemicals (e.g., terpenes) at varying proportions. Oils are a convenient method of administration and can be directly administered to the oral cavity for rapid mucosal absorption, however, they do require a degree of dexterity and are prone to inaccurate dosing as people typically administer their dose as a number of “drops” [88]. Similarly, sublingual or oral–mucosal sprays can be used. While direct application to the oral mucosa is a common and easy method of administration, it is important to consider how factors like oral mucositis may influence tolerance, as some sprays are prepared in an ethanol diluent which would be painful to apply to an ulcerated oral cavity. Similarly, it is unclear how oral mucositis impacts the rate of absorption. Oils can also be encapsulated for ingestion; however, this method of administration must be considered in the context of dysphagia and nausea/vomiting, which may impact the patient’s ability to swallow a capsule, or intestinal mucositis which may also influence the rate of absorption [127]. This underscores the need to conduct appropriate pharmacokinetic studies to understand how these unique factors associated with cancer, in particular active chemotherapy, impact the uptake and efficacy of cannabis. Further to this, there is evidence that suggests the presence of high-fat food impacts the bioavailability of cannabis, and thus this should be carefully considered in the design of capsules and other formulation strategies [32, 128]. Importantly, these methods of administration result in different clinical effects, particularly with respect to the timing and duration of the response [88]. These should be considered when selecting the time of administration (i.e., time of day) and the symptom or side effect(s) of interest.
In addition to the method of administration, the selection of specific cannabinoids and their relevant doses is critical. This decision needs to be guided by the specific symptom or side effect(s) of interest, with a clear scientific rationale for their use. When considering the MC intervention of interest, it is also important to acknowledge and respect the complexity of medicinal cannabis as an entire entity (i.e., a whole plant) in which the combination of numerous active compounds work cooperatively to elicit benefit. As such, while using synthesised isolates may be attractive from a pharmacological perspective, evidence suggests that the synergy of numerous cannabis compounds, a process referred to as the “entourage effect”, outweighs the benefits that can be gained from a single isolate or molecule.
In the context of mucositis and its constellation of symptoms, the use of CBD and THC (with other cannabinoids and compounds such as terpenes) is likely to be best positioned to deliver meaningful benefits based on their unique yet synergistic effects [13, 129]. Of note, CBD is documented to counteract the undesirable psychotropic effects of THC [130] and may therefore improve adherence. This synergy is in addition to the ability of these compounds to address different but related symptoms. For example, CBD is hypothesised to control self-perpetuating inflammatory pathways that ultimately dictate the depth and duration of mucosal injury to deliver clinically meaningful benefits [62, 131,132,133]. In parallel, THC has the capacity to provide complementary effects to control anxiety, promote food intake/appetite and sleep quality [134,135,136,137]. However, it cannot be ignored that while THC provides potential benefits for the patient, it certainly introduces additional medico-legal complexity, with many countries enforcing strict no-tolerance laws with respect to operating heavy machinery or driving motor vehicles. This may negatively impact patient well-being by impacting their employment prospects, or ability to live independently. It also poses challenges for patients that may have caring duties. Further advice regarding dosing has been summarised by Cyr and colleagues [88].
The future of medicinal cannabis
The field of MC has been and continues to be difficult to navigate, reflecting the legislative challenges, variations in formulations and complexities of this emerging pharmacotherapy [33, 34, 38, 138]. To understand how to appropriately use this plant and its individual components in a therapeutic manner and avoid toxicity, well-designed in vitro and in vivo clinical pharmacology studies are required, particularly due to individual differences [138, 139]. Understanding the clinical pharmacology involved with MC will take the ‘guesswork’ out of the current largely uncontrolled and uncertain approach, which could provide the long wanting ‘safeguard’ for many vulnerable [140] individuals who are not benefiting from current practices and already suffering from poor quality of life due to undergoing cytotoxic chemotherapy and/or many other unpleasant conditions.
It is well-known that there are many cannabis species producing hundreds of compounds of which more than 100 chemicals are known as phytocannabinoids, with THC, CBD, terpenes and flavonoids being mostly abundant [31, 34]. Therefore, in order to provide this ‘safeguard’ with MC therapy, there are two key elements that need to be addressed. The first being, understanding the molecular mechanisms behind both the therapeutic and adverse effects of the various compounds within MC, and the second being, understanding the pharmacogenomics, pharmacokinetics and pharmacodynamics of the various products and formulations between individuals [34, 38, 139].
To achieve this, well-established genetic approaches should be adopted in the field of MC to facilitate precision medicine (‘selecting right drug’) [38, 139] and pharmacokinetic-guided approaches to facilitate precision dosing (‘selecting the right dose’) [31, 34, 141]. For the latter, specifically, exposure-response studies via therapeutic drug monitoring or pharmacogenomics may enable individualised therapy [38, 139], similar to how it has been done for anti-cancer therapeutics [142]. In addition, to provide true individualised or personalised dosing, population pharmacokinetic–pharmacodynamic (POP-PK/PD) models need to be developed to better understand how the population and individuals respond to these compounds, and which covariates (e.g., age, weight, gender, genotype, comedications, etc.) drive any variability in the pharmacokinetics and thus responses [140].
It has been well-documented that clinical trials are limited and of the available data, it is clear that varied design has resulted in the inability to compare and establish conclusive evidence. However, with personalised medicine currently in its peak in many research areas, such as antimicrobials, and anti-cancer drugs [143], it is an ideal time to build on current research and investigate which compounds should be isolated or combined in the appropriate formulations and administered to truly enable personalised MC therapy [34, 38, 139]. This will lead to a better understanding how exactly these compounds exert their effects and how this knowledge can be utilised to treat conditions such as mucositis which in turn has the potential to reduce symptom clustering and an array of treatments which cause additional challenges (polypharmacy, drug–drug interactions, adverse effects, poor quality of life and financial burden) for both the individuals and the healthcare systems. The need and opportunity to investigate how MC therapy can be personalised for individuals suffering from mucositis and other conditions is evident and brings on an exciting future for MC research.
While trial data remain inconclusive, it is likely that individual factors that dictate tolerance and efficacy have contributed to the variable and often contradictory results observed. For example, previous cannabis use is associated with lower anxiety after THC. Similarly genomic factors have been shown to predict the efficacy and tolerability of CBD. In a recent genomic study of patients with treatment-resistant epilepsy, single-nucleotide polymorphisms in certain genes were identified which were associated with a lower response and greater side effects of CBD [141]. The study also revealed genetic variants that were related to the likelihood of CBD-associated diarrhoea [141]. These findings present an opportunity for personalised pharmacogenomics-guided strategies for precise MC treatment that could be particularly advantageous for patients undergoing chemotherapy, already at risk of gastrointestinal side effects such as diarrhoea [141]. Understanding these factors will be critical in optimising the safe and effective use of cannabis in medical practice.
Conclusions
Soon after the discovery of its chemical structure and ability to obtain various compounds from the plant in the late 1900s, as well as the description of the cannabinoid receptors and the endocannabinoid system in the 1990s, cannabis use for medical purposes has increased significantly with a steep rise in the last few years [31, 144]. It is evident that the majority of this use results from illegal access, however, this has been recognised and laws are in a fast-changing phase with several products approved and several others on a registered unapproved list. This provides new opportunities for users and prescribers to access MC products in a legal manner. In cancer care, self-reported cannabis use is prevalent, however, the evidence base is lacking due to inconsistencies in study design and outcomes. Moving forward, it is critical that research efforts integrate appropriate pharmacokinetic and mechanistic sub-studies to understand cannabis biology in the context of cancer and investigate its efficacy in a more holistic sense by considering its impact on clusters of related symptoms. In the context of mucositis, this is a compelling approach given the numerous symptoms that occur secondary to mucosal barrier injury and the already documented benefits medicinal cannabis has on gastrointestinal physiology, inflammation, and dysfunction.
A two-part research study suggests that frequent cannabis is a risk factor for coronary artery disease (CAD).
In the first part, in an observational study, daily cannabis use was associated with 34% higher odds for CAD compared with never-users in a large population-based US cohort. Less frequent use was not associated with increased odds for CAD.
In the second part, people with a genetic susceptibility to cannabis use disorder or severe cannabis dependency had an increased risk for CAD compared with other people.
Ishan Paranjpe, MD, the study’s lead author, reported these results in a press briefing and will present the study at the upcoming American College of Cardiology (ACC) Scientific Session/World Congress of Cardiology (WCC) 2023.
Dr Ishan Paranjpe
“A couple of takeaway points are that daily cannabis use, but not less frequent cannabis use was associated with CAD” in the large population-based cohort, said Paranjpe, a resident physician at Stanford University, California, during the press conference.
“This analysis was adjusted for several possible confounders including age, sex at birth, [body mass index (BMI)], race, education, cigarette use, hypertension, high cholesterol, and diabetes,” he noted, and even after accounting for these risk factors, the association with heart disease remained.
“And the next thing, using Mendelian randomization, we sort of implied that there might be a causal relationship between cannabis and heart disease. Importantly this effect is independent of alcohol and cigarette use.
“The notion that cannabis is completely benign is probably wrong, and there might be certain risk of certain cardiovascular effects of cannabis we should be more on the lookout for,” Paranjpe said in an interview with theheart.org | Medscape Cardiology.
“Our main conclusion was that prevalent CAD is associated with cannabis consumption,” he added. “Other mechanistic work published in Cell, has also shown that cannabis causes vascular inflammation that may lead to CAD.
“Thus, there is growing evidence from both laboratory and population studies that cannabis consumption may be harmful for cardiovascular health,” he said. “However, we still need more work on whether it affects the risk of incident cardiovascular events (ie, stroke, heart attack) in patient[s] with existing CAD.”
ASCVD Risk
Invited to comment, Robert L. Page II, PharmD, chair of the writing group for the American Heart Association’s scientific statement Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, published in 2020, said, “this adds to our hypothesis that if you are using marijuana over a longer period, greater exposure, you’re going to see an increase in the risk” for atherosclerotic cardiovascular disease (ASCVD).
“We’re seeing this increased risk for ASCVD in young adults between ages 18 to 40 — people who think that they’re invincible,” Page, a professor at the University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences, Aurora, Colorado, who was not involved with this research, told theheart.org | Medscape Cardiology in an interview.
“The bottom line is that the risk that they are seeing is what has also been documented in other observational studies, and it adds fuel to the fire. We need to be paying close attention to this,” he said.
“Primary care [clinicians], cardiologists, need to address this, particularly in younger adults — because that’s where you’re seeing the highest amount of use.”
“All of Us” Observational Study
In the first part of the study, the researchers analyzed data from the “All of Us” cohort comprising adults age 18 and older from 340 inpatient and outpatient sites across the United States.
They identified 57,958 individuals who replied to a questionnaire asking about cannabis use (medicinal or recreational and whether it was edible or used by smoking or vaping) over the past 3 months.
There were 39,678 never-users, 8749 who used it once or twice, 2075 who used it monthly, 2720 who used it weekly, and 4736 who used it daily.
Of these, 3506 individuals had CAD, based on medical records.
Only daily users had a significantly higher risk for CAD compared with never-users (odds ratio [OR], 1.34; P = .001) after adjusting for age, sex, hypertension, hyperlipidemia, type 2 diabetes, BMI, education, insurance status, and cigarette use.
The median age for daily users was 41, whereas the median age for never-users was 59.
GWAS Analyses
The researchers then performed a Mendelian randomization analysis based on genome-wide association studies (GWAS) of cannabis use disorder and of CAD.
“Cannabis use disorder is a psychiatric diagnosis of severe cannabis dependency, equivalent to ‘alcohol use disorder’ for alcohol consumption,” Paranjpe explained. “The exact definition involves frequent use leading to significant dependence (but does not specify how often it is used).”
The GWAS data for cannabis use disorder came from a recent meta-analysis of three cohorts: the Psychiatric Genomics Consortium Substance Use Disorders working group, iPSYCH, and deCODE.
The GWAS statistics for CAD were obtained from the CARDIoGRAMplusC4D Consortium.
Cannabis use disorder was associated with significantly increased odds for CAD (OR, 1.05; P = .001), which remained after adjusting for both cigarette and alcohol use (OR, 1.04; P = 1.07).
Summary: A study of 42 runners reveals that using cannabis before exercise can boost mood and enjoyment. The study shows that both THC and CBD can enhance exercise experience, with CBD even outperforming THC in some aspects.
However, THC can make exercise feel more effortful due to increased heart rate. While cannabis may improve enjoyment, it’s not considered a performance-enhancing drug, and its use should be approached with caution.
Key Facts:
Cannabis, both THC and CBD, can enhance the enjoyment and mood during exercise, potentially making it more enjoyable.
CBD, in particular, showed significant benefits in enhancing exercise experience without the impairment associated with THC.
THC can increase heart rate, making exercise feel more challenging, and it’s not recommended for performance enhancement.
Source: University of Colorado
A bit of weed before a workout can boost motivation and make exercise more enjoyable. But if performance is the goal, it may be best to skip that joint.
That’s the takeaway of the first ever study to examine how legal, commercially available cannabis shapes how exercise feels.
The study of 42 runners, published Dec. 26 in the journal Sports Medicine, comes almost exactly 10 years after Colorado became the first state to commence legal sales of recreational marijuana, at a time when cannabis-users increasingly report mixing it with workouts.
“The bottom-line finding is that cannabis before exercise seems to increase positive mood and enjoyment during exercise, whether you use THC or CBD. But THC products specifically may make exercise feel more effortful,” said first author Laurel Gibson, a research fellow with the University of Colorado Boulder’s Center for Health and Addiction: Neuroscience, Genes and Environment (CU Change).
The findings, and previous research by the team, seem to defy long-held stereotypes that associate cannabis with “couch-lock” and instead raise an intriguing question: Could the plant play a role in getting people moving?
“We have an epidemic of sedentary lifestyle in this country, and we need new tools to try to get people to move their bodies in ways that are enjoyable,” said senior author Angela Bryan, a professor of psychology and neuroscience and co-director of CU Change. “If cannabis is one of those tools, we need to explore it, keeping in mind both the harms and the benefits.”
‘A first-of-a-kind study’
In one previous survey of cannabis users, Bryan’s research group found that a whopping 80% had used before or shortly after exercise. Yet very little research has been done at the intersection of the two.
For the study, Bryan and Gibson recruited 42 Boulder-area volunteers who already run while using cannabis.
After a baseline session, in which the researchers took fitness measurements and survey data, they assigned participants to go to a dispensary and pick up either a designated flower strain that contained mostly cannabidiol (CBD) or a Tetrahydrocannabinol (THC) -dominant strain.
THC and CBD are active ingredients in cannabis, with THC known to be more intoxicating.
On one follow-up visit, volunteers ran on a treadmill at a moderate pace for 30 minutes, answering questions periodically to assess how motivated they felt, how much they were enjoying themselves, how hard the workout felt, how quickly time seemed to pass and their pain levels.
On another visit, they repeated this test after using cannabis.
Federal law prohibits the possession or distribution of marijuana on college campuses, so the runners used it at home, before being picked up in a mobile laboratory, a.k.a the ‘CannaVan,’ and brought to the lab.
The runners also wore a safety belt on the treadmill.
‘Not a performance-enhancing drug’
Across the board, participants reported greater enjoyment and more intense euphoria, or ‘runner’s high,’ when exercising after using cannabis.
Surpisingly, this heightened mood was even greater in the CBD group than in the THC group, suggesting athletes may be able to get some of the benefits to mood without the impairment that can come with THC.
Participants in the THC group also reported that the same intensity of running felt significantly harder during the cannabis run than the sober run.
This may be because THC increases heart rate, Bryan said.
In a previous study conducted remotely, she and Gibson found that while runners felt more enjoyment under the influence of cannabis, they ran 31 seconds per mile slower.
“It is pretty clear from our research that cannabis is not a performance enhancing drug,” said Bryan.
Notably, numerous elite athletes—including U.S. sprinter Sha’Carri Richardson— have been prohibited from competing in recent years after testing positive for cannabis.
An NCAA committee recently recommended that it be removed from its list of banned substances.
A different kind of runner’s high
Why does cannabis make exercise feel better?
While natural, pain-killing endorphins have long been credited with the famous “runner’s high,” newer research suggests that this is a myth: Instead, naturally produced brain chemicals known as endogenous cannabinoids are likely at play, kicking in after an extended period of exercise to produce euphoria and alertness.
“The reality is, some people will never experience the runner’s high,” Gibson notes.
By consuming CBD or THC, cannabinoids which bind to the same receptors as the cannabinoids our brain makes naturally, athletes might be able to tap into that high with a shorter workout or enhance it during a long one, she said.
Athletes considering using cannabis should be aware that it can come with risks — including dizziness and loss of balance— and it’s not for everyone.
For someone gunning for a fast 5k or marathon PR, it doesn’t really make sense to use beforehand, Bryan said.
But for an ultrarunner just trying to get through the grind of a double-digit training run, it might.
As a public health researcher, Bryan is most interested in how it could potentially impact those who struggle to exercise at all, either because they can’t get motivated, it hurts, or they just don’t like it.
“Is there a world where taking a low-dose gummie before they go for that walk might help? It’s too early to make broad recommendations but it’s worth exploring,” she said.
Why do people mix weed and workouts?
When researchers asked study participants, here’s what they said:
90.5% It increases enjoyment
69% It decreases pain
59.5% It increases focus
57.1% It increases motivation
45.2% It makes time go by faster
28.6% It improves performance
Abstract
Acute Effects of Ad Libitum Use of Commercially Available Cannabis Products on the Subjective Experience of Aerobic Exercise: A Crossover Study
Objective
The present study aimed to examine the acute effects of legal-market cannabis on regular cannabis users’ subjective responses to exercise in a controlled laboratory environment.
Background
Given the stereotype that cannabis is associated with extreme sedentary behavior, there are concerns that cannabis legalization may exacerbate the US physical inactivity epidemic. However, despite these concerns, recent years have seen considerable public interest in the use of cannabis concurrently with exercise (e.g., running).
Methods
The present study compared participants’ experiences of exercise without cannabis to their experiences of exercise after acute ad libitum use of one of two commercially available cannabis flower products: a Δ9-tetrahydrocannabinol-dominant or a cannabidiol-dominant product. Participants (N = 42) were regular cannabis users between the ages of 21 and 39 years (mean = 30.81 years, standard deviation = 4.72 years).
Results
Although participants reported a more positive affect (p < 0.001), enjoyment (p < 0.001), and runner’s high symptoms (p < 0.001) during their cannabis (vs non-cannabis) exercise appointment, they also reported more exertion (p = 0.04). Pain levels were very low and did not differ between appointments (p = 0.45). Effects appeared to depend, in part, on cannabinoid content; there was a larger difference in enjoyment (p = 0.02), and a smaller difference in exertion (p = 0.02), between the cannabis and non-cannabis exercise appointments among participants in the cannabidiol (vs Δ9-tetrahydrocannabinol) condition.
Conclusions
To our knowledge, this is the first study to investigate the acute effects of commercially available cannabis on subjective responses to exercise in a laboratory environment. Our findings suggest that, among regular cannabis users who use cannabis in combination with exercise, cannabis use prior to exercise may lead to increases in both positive and negative aspects of the subjective exercise experience. Research using diverse samples, exercise modalities, and methodologies (e.g., placebo-controlled trials) is needed to establish the generalizability of these findings.
Although recreational and medicinal marijuana (cannabis) is increasingly available across the U.S., public and professional awareness that cannabis use may adversely affect brain health is critical, according to the American Heart Association’s first scientific statement on the subject.
Animal studies indicate that marijuana’s psychoactive component, THC, may lead to behavioral and cognitive abnormalities, particularly if exposure occurs prenatally or during adolescence.
However, studies in humans have had mixed results, with some suggesting a higher risk of cognitive impairment due to marijuana use and further research needed on exact consequences.
The statement outlines the latest research and the need for future studies to address several open questions about how marijuana may impact brain health.
Embargoed until 6 a.m. CT / 7 a.m. ET Thursday, Feb 10, 2022
DALLAS, Feb. 10, 2022 — Despite the perception that marijuana is harmless, there is some scientific evidence challenging that belief, and there are many unanswered questions about its impact on brain health, according to a new American Heart Association scientific statement published today in the Association’s journal Stroke. This scientific statement will be presented and discussed during a symposium at the Association’s International Stroke Conference in New Orleans, today at 7 a.m. CT/ 8 a.m. ET. An American Heart Association scientific statement is an expert analysis of current research and may inform future clinical practice guidelines.
“There’s a lot of uncertainty in the medical community about the health effects of marijuana. This scientific statement is intended to guide health care professionals in having a balanced and intentional discussion with patients about the potential known and unknown effects of marijuana on brain health,” said writing group Chair Fernando D. Testai, M.D., Ph.D., FAHA, a professor of neurology and rehabilitation at the University of Illinois at Chicago.
This is the Association’s first scientific statement on cannabis and brain health, following a statement on marijuana and cardiovascular health, published in August 2020. Both statements are important since marijuana use in the U.S. is increasing, particularly among adolescents and young adults, with about one-third of 12th graders and nearly half of college students reporting marijuana use in 2018. In addition, the use of marijuana medicinally and/or recreationally has been legalized or decriminalized in many states across the U.S. in the past 2 decades, and the concentration of tetrahydrocannabinol (THC, the psychoactive component in marijuana) in cannabis products has increased significantly, from about 4% in 1995 to 15% in 2018.
The most studied chemicals in cannabis are THC and CBD. THC is the compound in marijuana that gives the sensation of being high. CBD (cannabidiol) has antioxidant and anti-inflammatory properties but does not have psychoactive effects. The potential therapeutic benefits of CBD continue to be investigated in clinical trials.
The U.S. Drug Enforcement Agency (DEA) and the Food and Drug Administration (FDA) classify cannabis as a Schedule I controlled substance, on par with heroin and LSD, for having a “high potential for abuse and little to no medical benefit.” In contrast, CBD is legal when derived from hemp, which is the same species of plant as cannabis and contains less than 0.3% THC.
To fully understand the potential impact of marijuana, it’s important to know that the human body naturally produces compounds called endocannabinoids that are similar to those in marijuana. Endocannabinoids are involved in the regulation of many body processes throughout life (including learning, memory, pain control and sleep), and the action of endocannabinoids is essential to prenatal brain development and to brain maturation during adolescence.
Endocannabinoids, as well as THC, can attach to neurons in the brain through molecules called cannabinoid receptors. When THC activates cannabinoid receptors in the brain, it can disrupt the normal actions of endocannabinoids. “These receptors are highly concentrated in brain areas related to cognition,” said Testai.
According to the statement, previous animal studies (in rodents) indicate that prolonged exposure to THC disrupts memory and learning, and impacts brain development and maturation in specific ways if exposed at certain stages of life:
During prenatal life, an important time for brain development, THC disrupts the normal signaling pathways of the endocannabinoid system and may alter the offspring’s thinking, emotional behavior and response to stress.
During adolescence, an important time for brain maturation, THC changes the structure and function of brain circuits, particularly in areas involved in cognition, emotional regulation and social behavior (such as the prefrontal cortex and hippocampus).
“Data obtained in these animal studies demonstrate that disruption of endocannabinoid pathways leads to behavioral and cognitive abnormalities, such as poorer memory and learning ability and a heightened sensitivity to stress. Also, there may be vital life periods – gestation and adolescence – when the brain may be particularly vulnerable to the impact of THC,” Testai said.
While the exact timing and amount of marijuana exposure are more easily controlled in animal studies, as well as controlling the animals’ social and environmental conditions, human research studies cannot replicate similar strict parameters. Thus, results from existing studies in humans have been mixed, yet raise similar concerns about the impact of marijuana exposure on brain health. Among the studies in humans summarized in the scientific statement, the findings included:
While actively using marijuana, people demonstrated worse scores on driving road tests when using THC-dominant marijuana, compared to when they were using CBD-dominant marijuana or no marijuana.
In young adults who were followed for 25 years as part of a heart disease research project, scores on verbal memory tests declined in correlation to more years of self-reported exposure to marijuana.
There were more psychological problems and poorer cognitive function in children (average age 9) whose mothers reported using marijuana during pregnancy.
Marijuana use during adolescence has been associated with thinning in an area of the brain involved in cognition (the prefrontal cortex), with greater exposure to marijuana associated with more thinning. However, other studies detected no difference.
Structural changes in the brain were visible in some studies comparing marijuana users and non-users. Specifically, there was thinning of brain areas important in orchestrating thoughts and actions, or decreased volume in an area of the brain important for memory. Other studies that compared cognitive testing and brain imaging found no differences between marijuana users and non-users.
Cannabis users were found to have an increased risk of clot-caused stroke, with one study finding 17% more and another finding 24% more strokes among cannabis users.
The statement also highlights numerous open questions on the impact of cannabis on brain health, including:
Does marijuana’s impact on brain health differ depending on the person’s age?
How does marijuana interact with other substances such as prescription medications? This is a particular concern in elderly people who may be using multiple medications such as blood thinners, antiarrhythmia or anticonvulsant medications to treat other chronic health conditions.
Do the effects of marijuana differ whether it is used recreationally or prescribed for the treatment of a specific medical condition?
How much marijuana is too much? In older research studies conducted when marijuana was illegal in all U.S. states, there may have been significant under-reporting of how frequently marijuana was used.
Do different types of marijuana (such as higher THC levels or synthetic cannabinoids) impact the brain differently?
Are there differences in brain health depending on whether marijuana is smoked or consumed in an edible product?
“Our understanding of the effects of marijuana on the brain is imperfect, and human research in this area is a work in progress. Still, the results of recent animal studies challenge the widely accepted idea that cannabinoids are harmless and call for caution when using marijuana, particularly while pregnant or during adolescence,” said Testai.
This scientific statement was prepared by the volunteer writing group on behalf of the American Heart Association’s Stroke Brain Health Science Subcommittee of the Stroke Council; the Council on Arteriosclerosis, Thrombosis and Vascular Biology; the Council on Cardiovascular and Stroke Nursing; the Council on Lifestyle and Cardiometabolic Health; and the Council on Peripheral Vascular Disease. The American Academy of Neurology has affirmed this scientific statement as an educational tool for neurologists.
American Heart Association scientific statements promote greater awareness about cardiovascular diseases and stroke issues and help facilitate informed health care decisions. Scientific statements outline what is currently known about a topic and what areas need additional research. While scientific statements inform the development of guidelines, they do not make treatment recommendations. American Heart Association guidelines provide the Association’s official clinical practice recommendations.
Co-authors are Philip B. Gorelick, M.D., M.P.H.; Hugo J. Aparicio, M.D., M.P.H.; Francesca M. Filbey, Ph.D.; Raul Gonzalez, Ph.D.; Rebecca F. Gottesman, M.D., Ph.D.; Miriam Melis, Ph.D.; Mariann R. Piano, R.N., Ph.D.; Tiziana Rubino, Ph.D.; and Sarah Y. Song, M.D. Authors’ disclosures are listed in the manuscript.
The Association receives funding primarily from individuals. Foundations and corporations (including pharmaceutical, device manufacturers and other companies) also make donations and fund specific Association programs and events. The Association has strict policies to prevent these relationships from influencing the science content. Revenues from pharmaceutical and biotech companies, device manufacturers and health insurance providers and the Association’s overall financial information are available here.
A cancer diagnosis is both devastating and terrifying. Patients are almost always directed towards conventional cancer treatments like surgery, chemotherapy and radiation, and are made to feel that any other, more “natural” treatments are not only ineffective but dangerous.
The truth is, however, that mainstream cancer treatments wreak havoc on the body, leaving it defenseless against disease and breaking it down at the exact time when it needs to be as strong as possible. With its less than impressive success rate of between 2 and 4 percent, along with its devastating effects on the body, it is unsurprising that three out of every four doctors say they would refuse chemotherapy as a treatment option if they themselves became ill.
While doctors like to promote the idea that there are no treatments scientifically proven to work besides the usual surgery/chemotherapy/radiation regimen, the truth is there is a strong body of evidence that many natural, non-invasive treatments are effective in the fight against cancer. One of the most well-researched and solidly proven of all these natural medicines is cannabis.
The miraculous power of cannabinoids
As noted by Dr. Mark Sircus, writing for Green Med Info, there is no confusion about whether marijuana is an effective cancer treatment. Cannabis has been scientifically proven to kill cancer cells without the devastating and body weakening effects of conventional cancer treatments.
The marijuana plant contains about 113 powerful chemical compounds known as cannabinoids. The most well-known of these compounds are tetrahydrocannabinol (THC) – the chemical that induces marijuana’s “high” – and cannabidiol – a non-psychoactive compound which has been extensively studied as a cure for many diseases.
The power of the elements: Discover Colloidal Silver Mouthwash with quality, natural ingredients like Sangre de Drago sap, black walnut hulls, menthol crystals and more. Zero artificial sweeteners, colors or alcohol. Learn more at the Health Ranger Store and help support this news site.
These and other cannabinoids are what make marijuana such a potent anti-cancer treatment, as reported by Green Med Info:
Cannabinoids are found to exert their anti-cancer effects in a number of ways and in a variety of tissues.
Triggering cell death, through a mechanism called apoptosis
Stopping cells from dividing
Preventing new blood vessels from growing into tumors
Reducing the chances of cancer cells spreading through the body, by stopping cells from moving or invading neighboring tissue
Speeding up the cell’s internal ‘waste disposal machine’ – a process known as autophagy – which can lead to cell death
All these effects are thought to be caused by cannabinoids locking onto the CB1 and CB2 cannabinoid receptors. Almost daily we are seeing new or confirming evidence that Cannibinoids can be used to great benefit in cancer treatment of many types.
Scientific studies published in a host of peer-reviewed journals have confirmed marijuana’s powerful ability to fight breast, lung, ovarian, pancreatic, prostate and other cancers.
Scientists are calling for more studies to be done on humans after studying the cancer-fighting effects of chemicals in the drug.
Studies suggest chemicals called phytocannabinoids could stop cancer cells multiplying and spreading, block the blood supply to tumors, and reduce cancer’s ability to survive chemotherapy. …
The new research review admits cannabis has ‘anti-cancer effects’ and says more research needs to be done in real patients to confirm the findings.
It takes real courage to receive a cancer diagnosis and decide not to follow mainstream advice but seek alternative treatments. But even for those who choose to receive conventional cancer treatments like radiation and chemotherapy, cannabis can still be an important part of their overall wellness plan. As Dr. Sircus admonishes, “Every cancer patient and every oncologist should put medical marijuana on their treatment maps.”
Patients with treatment-resistant epilepsy can develop a tolerance to cannabis-based therapy, a finding that may have implications for long-term management, new research suggests.
Dr Shimrit Uliel-Sibony
“Physicians should be aware that tolerance may occur,” study investigator Shimrit Uliel-Sibony, MD, pediatric epileptologist, Dana-Dwek Children’s Hospital, Tel Aviv University, Israel, told Medscape Medical News.
“There’s this notion that cannabis is a great medicine, that it’s much better in terms of response rates than other interventions for patients with treatment-resistant epilepsy, but that may only be at the beginning,” she added.
Long-term exposure may produce a different picture. With time, efficacy may decrease, resulting in a need to increase the dose. This suggests the development of tolerance.
“We know marijuana may have cognitive consequences with long-term, chronic recreational use. I think we need to be a little more cautious on our expectations of this therapy,” said Uliel-Sibony.
The study was presented here at the American Epilepsy Society (AES) 72nd Annual Meeting 2018.
Few Long-term Data
In the recent past, many studies have suggested that medical cannabis is superior to traditional antiepileptic drugs (AEDs). Studies have reported dramatic improvement in seizure control, as well as a favorable safety profile.
However, said Uliel-Sibony, there is a need for data on long-term safety and efficacy. The long duration of treatment, the investigators note, “raises the possibility of withdrawal and tolerance.” Some animal studies suggest that prolonged exposure to tetrahydrocannabinol (THC), the psychoactive ingredient in cannabis, but not cannabidiol (CBD) leads to tolerance.
To assess the long-term efficacy of cannabinoids as well as the development of tolerance in the treatment of refractory epilepsy, the investigators conducted an observational, longitudinal study of pediatric and adult patients.
The analysis included 92 patients (59 males) ranging in age from 1 year to 37 years (mean age, 11.8 years). All had treatment-resistant epilepsy; two had Dravet syndrome; and three had Lennox-Gastaut syndrome (LGS). The remainder had other types of seizures and epilepsy syndromes.
All patients had experienced treatment failure with numerous drug therapies, and for some, use of the ketogenic diet or vagal nerve stimulation therapy was also ineffective. None had been previously treated with medical cannabis.
Participants were initially given a cannabis oil extract in which the ratio of CBD to THC was 20:1. That amount of THC has negligible psychoactive activity, noted Uliel-Sibony.
The patients had been receiving stable doses of AEDs for at least 4 weeks before study enrollment. All participants had at least 3 months of follow-up (mean follow-up, 20 months).
No “Honeymoon” Tolerance
Tolerance was defined as a 30% or greater reduction in response rate that continued for more than 3 months.
Patients in whom efficacy decreased during the first 3 months of treatments were not included. The intention was to exclude patients who showed short-lasting improvement that was possibly the result of the “honeymoon” effect.
The investigators found that about 29% of the study population experienced a reduction in seizures by 50% to 75%.
Of 84 patients included in the tolerance analysis, 25% developed tolerance, which was reported with an average dosage of 12.6 mg/kg/day.
This dosage is lower than in some studies that used more purified cannabis. There was some suggestion that combining CBD with a very small amount of TCH “enables use of a lower dose of CBD,” a phenomenon referred to as the entourage effect, said Uliel-Sibony.
None of the patients with Dravet syndrome or LGS developed tolerance, she added.
In an attempt to counteract tolerance, the CBD dose was increased. Using this approach, about 20% of the patients were able to achieve the same response rate as before the development of tolerance, but this was not the case for almost half of the cohort.
In some patients, tolerance was reversed by gradually reducing the CBD dose, waiting 2 to 3 weeks, and then restarting the medication at the same dose that achieved response.
The tolerance may be due to “receptor desensitization,” said Uliel-Sibony. “If we take patients off the medicine, the receptors become sensitive again.”
This new study used two similar CBD products that are available in Israel. There was no difference between the two products in terms of tolerance.
It is not clear whether the tolerance seen in the study was due to the presence of THC. The literature on the subject suggests that there is no tolerance to CBD, only to THC, she said.
But it may be a question of exposure. In this study, the mean time for tolerance to occur was 7.3 months.
“Tolerance is something that develops over time,” said Uliel-Sibony.
Having a small amount of THC in the product seems to have some positive side effects, she said. Parents reported that children showed improvements in sleep and appetite and that they were more alert.
Great Expectations
She noted that overall, the side effect profile for the formulation is superior to that reported in other studies that used a more purified formulation of CBD. Of the 87 patients included in the safety analysis, 51% experienced adverse reactions.
Uliel-Sibony hopes to continue to follow the patients in the study for a longer period “to get a better picture” of tolerance, she said.
But she recognizes the challenges of following this patient population. Moreover, even if the number of seizures is reduced by half, for those patients who were having 10 seizures at the start of treatment, the condition is still not well controlled.
She believes expectations are high for cannabis-based therapy. She cited one study that showed that parents who relocated to Colorado just to access one of the early CBD treatments for epilepsy reported better response to the drug.
Families may be misled by some of the hype surrounding medical marijuana, said Uliel-Sibony. “Parents believe they’re giving their child something natural, something that isn’t really a chemical, but CBD is a medicine like any other.”
She noted that her study has limitations, including the fact that it is not randomized controlled trial.
For many , the idea of cannabis being used as an asthma treatment can feel a bit backwards. After all, one of the most common ways cannabis is ingested is by smoking, a method that would seem to be detrimental to those with asthma. However, recent studies have found that cannabis in any form (even smoked) can greatly benefit those suffering from the symptoms of asthma.
Can Marijuana Treat Asthma?
First let’s take a closer look at asthma and what it actually means to have it. Asthma is a fairly common lung disease that results in the narrowing of the airway passage. Due to this narrowing, those suffering from asthma frequently experience feeling out of breath, wheezing or uncontrollable coughing.
While treatment can be used to reduce the effects patients with asthma experience, there is currently no cure for the condition. Asthma attacks can come in many forms and can be triggered by a number of factors including allergies or exercise. While asthma doesn’t reduce your life expectancy, being caught in an intense asthma attack without the proper treatment can be fatal.
So how does a substance that can be smoked help treat asthma? The explanation can be found by examining where asthma begins. Asthma is a chronic inflammatory disease, while cannabis is known for its powerful anti-inflammatory effects. This means cannabis works in an opposite effect to other substances like tobacco and can actually help expand the lungs instead of constricting them.
Editor’s Note: A 2015 animal study in the Journal of Pharmacology and Experimental Therapeutics identified THC specifically as the active compound in cannabis that could benefit people suffering from asthma. They found that THC had anti-inflammatory and bronchodilator effects on airways (very similar to the effect Ventolin has on the lungs during an asthma attack). This is great news!
So how powerful can a cannabis treatment actually be? For those suffering from an asthma attack the results are practically instantaneous and are similar to the results found with some of the more common name brand inhalers.
If you or someone you know is suffering from asthma and would like to seek cannabis as a treatment option, be sure to check out your state’s list of qualifying medical conditions for medicinal cannabis to see if you are eligible for such a treatment option.
Other Ways to Treat Asthma Naturally
If you’re looking for more natural forms of asthma treatment, talk to your doctor about the following options:
Irecently opened a Snapchat from my best friend informing me that she had been fired from her job because she failed a drug test.
Jasmine does not do drugs — her idea of a wild night includes catching up on “Jane the Virgin” while sipping Moscato. I started to panic, thinking, “My best friend has totally gone off the deep end.” Some form of telepathy must have kicked in, because seconds later, I received a text assuring me everything was okay.
The job loss wasn’t a tragedy: Jasmine was already planning to submit her two weeks notice. We spent the next few minutes laughing about how dumb it was that she lost her job because of a poppy seed (during the harvesting process, poppy seeds absorb opium extract, which can cause your pee to test positive for morphine). After we hung up, I started to wonder: How long does it take before a drug is out of your system?
According to the US Anti-Doping Agency, it can take up to 48 hours for drugs like morphine and codeine to pass through your system. But what about marijuana? It seems like all the cool kids are doobie-ing it up these days.
Green Rush Daily explains that the most common way for an employer to track your marijuana usage is through a urine test. These tests don’t detect THC (the ingredient in weed that makes makes you feel high). Instead, urine tests look for THC-COOH, a derivative chemical your body produces after smoking or ingesting weed. THC-COOH stays in your system longer than THC, which explains why you might fail a drug test, even weeks after a smoke session.
The more you smoke, the longer it takes for marijuana to completely exit your body. Here’s a quick breakdown:
First time smokers usually test positive for marijuana for five to eight days after using.
If you smoke two to four times in a week, THC-COOH will remain in your urine for approximately 11–18 days.
Smokers that get high five to six times a week will test positive for over a month after smoking.
If you smoke weed every day, THC-COOH can remain in your urine for up to 77 days.
Some weed enthusiasts claim that drinking water and cranberry juice can help you pass a drug test. Unfortunately, consuming too many fluids can dilute your urine, which may compromise your test results.
Sorry, marijuana lovers; it’s hard to outsmart science. Even the best employees can be brought down by a poorly timed drug test. When it comes to your weed (and poppy seed) use, tread lightly.
In November 2016, Cannabis Science announced 2 new pharmaceutical developments in the form of cannabis skin patches for pain. Representatives claim the skin patch will be more effective than cannabis-based topical creams, pills, or injections due to its more accurate dosing (1).
Currently, the skin patches are not yet available and no official date has been given by Cannabis Science for clinical trials. Nevertheless, should research and development progress as expected, the cannabis skin patch could prove to be a much-needed new option for treating complicated chronic pain conditions including fibromyalgia and diabetic neuropathy.
Does Cannabis Work for Treating Pain?
The most common natural plant cannabinoids (phytocannabinoids) are: THC, cannabidiol (CBD), cannabigerol (CBG), cannabichromene (CBC), and cannabinol (CBN). While the majority of research and public attention has been directed at THC, the new skin patch development uses the CBD, otherwise known as cannabidiol(1).
Research shows that CBD has several beneficial properties, including (5):
anti-inflammatory
analgesic (pain relief)
greater antioxidant activity than vitamins C or E
neuroprotective
CBD is a non-euphoriant, and some research actually suggests that this particular cannabinoid reduces the effect of the other euphoriant cannabinoids, lessening their psychoactive effects including panic, anxiety, intoxication, and heart palpitations. In short, taking isolated CBD will not alter your state of mind like smoking or consuming marijuana would.
Cannabis Science CEO, Raymond Dabney states, “As more states nationwide legislate for the legalization of Cannabis and Cannabis derived medications, we here at Cannabis Science are focused on developing pharmaceutical formulations and applications to supply the huge growing demand expected over the coming few years.”
Thanks to a growing body of research exploring the medical uses of cannabis, and a cultural openness to medical marijuana use, the cannabis skin patch may soon be a real option available to those suffering from painful conditions like diabetic nerve damage and fibromyalgia.
Diabetic Neuropathy and Cannabis
Diabetic neuropathy is a group of nerve disorders associated with diabetes. While nerve damage can start at any point for those with diabetes, people who have had diabetes for 25 years or more or who have difficulty managing their blood sugar or blood pressure levels, have the highest risk (2).
Since nerve damage can occur in every organ system, symptoms can be varied. Some people with nerve damage won’t experience any noticeable symptoms at all. The 4 main types of diabetic nerve damage come with their own unique set of symptoms:
Diabetic Nerve Damage Symptoms
1. Peripheral Neuropathy: The most common type of neuropathy is peripheral neuropathy, which usually manifests in hands and feet as (2):
numbness
tingling
sharp pain
sensitivity to touch and temperature
2. Autonomic Neuropathy: This type of nerve damage affects the cardiovascular system, eyes, digestive tract, sex organs, urinary tract, and sweat glands. Symptoms include (2):
noticeable changes in digestion and bladder function
sexual dysfunction in both men and women
inability to manifest usual warning signs of low blood sugar
trouble seeing at night
profuse sweating
3. Proximal Neuropathy: Proximal neuropathy is localized in the legs. It’s associated with (2):
pain in legs, hips, thighs or bottom
noticeable weakness in leg muscles
4. Focal Neuropathy: This form of nerve damage can affect any nerve in the body (but most often in the head and arms), causing weakness and pain. Other symptoms include (2):
vision problems, aching around eyes
facial paralysis
acute pain in chest, stomach or abdominals
How Is Diabetic Nerve Damage Treated?
Conventionally, doctors will prescribe patients with diabetic nerve damage painkillers, anticonvulsants or antidepressants such as oxycodone, Ultram, amitriptyline, Cymbalta, or Lyrica. Additionally, they will work with the patient to help keep blood sugar levels balanced.
Should Cannabis Science’s skin patch go through clinical trials and be approved by the FDA, it would provide a more natural and effective way to manage pain from diabetic nerve damage without risk of addiction (a massive problem with opioid prescriptions).
Fibromyalgia and Cannabis
Fibromyalgia syndrome is a chronic condition often grouped together with arthritis, although it is not an arthritic condition. Fibromyalgia affects mostly women. A 2008 report estimated that about 5 million adult Americans suffer from fibromyalgia (4). Sufferers of fibromyalgia experience chronic non-localized pain, tenderness, and intense fatigue. Sometimes, fibromyalgia is accompanied by other symptoms including (3):
brain fog
headaches
morning stiffness
restless leg syndrome
painful menstrual cramps
irritable bowel syndrome
How is Fibromyalgia Treated?
Unfortunately, fibromyalgia can be tricky to treat; this is complicated by the fact that many medical providers are not familiar with fibromyalgia or its various treatments. The FDA has currently approved 3 drugs for fibromyalgia treatment: Duloxetine, Milnacipran, and Pregabalin.
The Cannabis Science skin patch might be a promising treatment option for many fibromyalgia patients, especially those for whom the 3 current drugs don’t have an effect. It would also provide a less risky solution than the current drugs, which come with their own long lists of side effects and long-term risks.
Help us spread awareness of this potential new treatment by sharing this article with your friends and family. We will continue to follow the development of the Cannabis Science skin patch and provide updates as new studies and trial information becomes available.
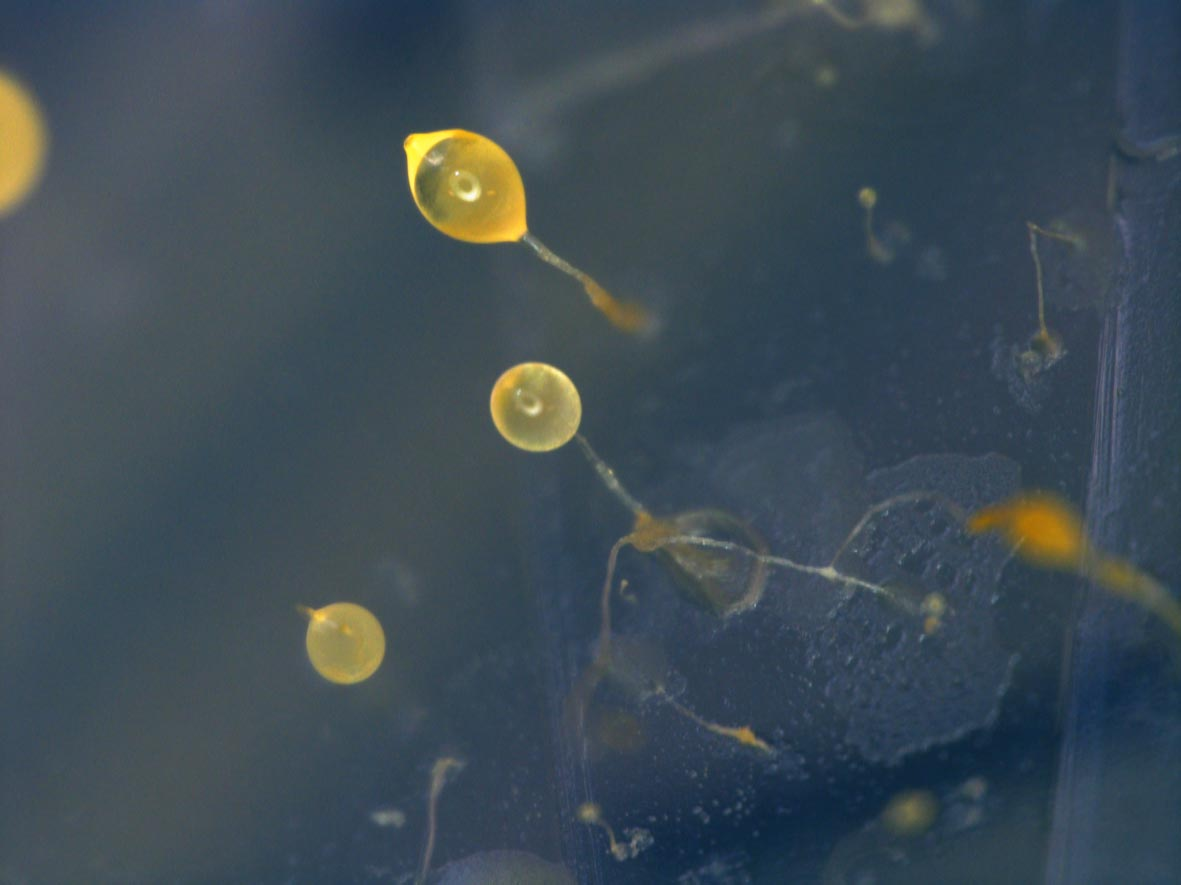

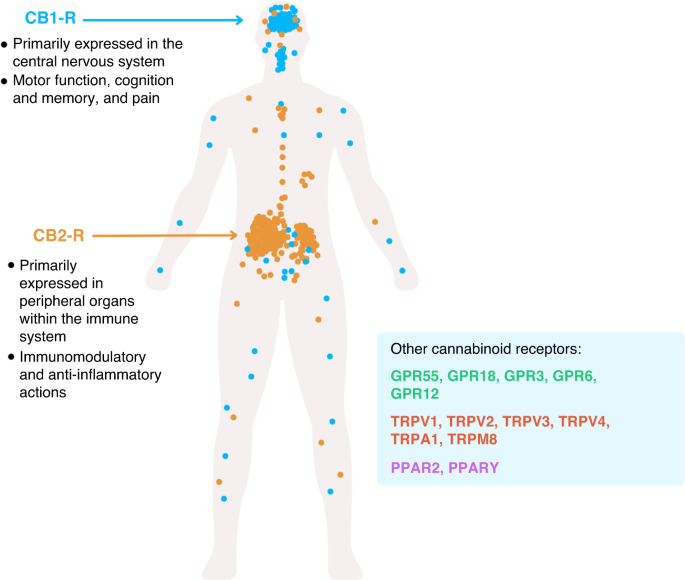
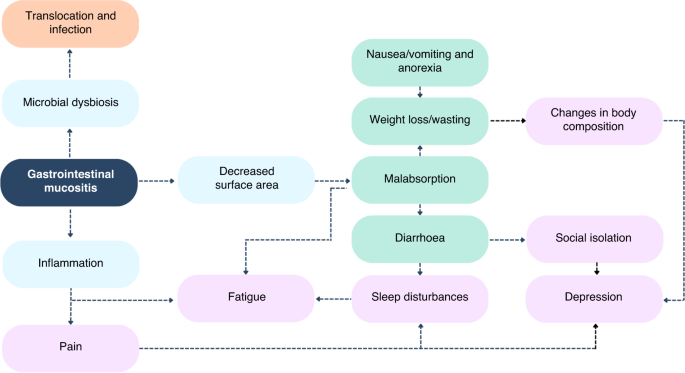






{kind=link}