Fortunately, most thyroid cancers are indolent and their treatment is de-escalating. What was once uniformly managed with total thyroidectomy, adjuvant radioactive iodine, and thyrotropin suppression is now individualized, involving less or even no surgery—for the right patients. Matching the right treatment to the right cancer biology for the right patient is fundamental to providing the best care. Discerning thyroid tumor biology, however, currently depends on characteristics of disease presentation (eg, extent) and pathologic information obtained after surgery. When considering innovative surgery-free treatment strategies, such as radiofrequency ablation (RFA), an intrinsic question remains: how, without surgery, can we obtain the best and most comprehensive information about thyroid tumor biology?
Li and colleagues1 reported their retrospective and single-center experience of using RFA to treat 1613 patients with T1a (1 cm or less, intrathyroidal; 88% of cohort) or T1b (more than 1 cm and 2 cm or less, intrathyroidal; 12% of cohort) low-risk, differentiated thyroid carcinoma who were ineligible or refused either surgery or active surveillance. Over an average 5-year follow up, local tumor progression occurred in 4% of patients, of whom 39% had persistent disease, primarily occurring with larger or multifocal carcinomas in a subcapsular location, and 86% required RFA retreatment. Carcinomas with BRAF V600E mutations were up to 6 times more likely to develop local tumor progression, though the finding did not achieve statistical significance.
Could a more comprehensive molecular profile improve patient selection for RFA? Over the last 3 decades, significant strides in understanding the biology of thyroid carcinoma, especially its molecular underpinnings, have been made. Though the current study reported BRAF V600E status, this somatic abnormality is only 1 mutational feature of thyroid carcinomas.2 Studies increasingly report the connection of molecular profiling results with thyroid tumor biology and outcomes,3,4 offering important prognostic information from a fine-needle biopsy alone and, thus, perfectly suited to improve patient selection for nonoperative strategies. The use of molecular profiling for prognosis is common in other cancers5,6 and its application routinely guides clinical care of breast cancer7—why should thyroid cancer care lag behind?
The authors1 should be commended for their large series, which moves the field toward a better understanding of the safety of RFA for small thyroid carcinomas. Like active surveillance, RFA may be another possible nonoperative option for patients who desire further treatment of small (less than 1 cm) thyroid cancers. Avoiding surgery is a welcome change in a disease process where opportunities to de-escalate care are important, but it is still unclear whether RFA is a patient-centered, cost-effective alternative. Though future comparative studies are necessary, molecular profiling should be considered to optimize risk stratification and individualize treatment. For now, we must ask ourselves whether RFA is a solution that has yet to find its problem.
It’s “critically important” for clinicians to recognize that not all patients with hypothyroidism are fully treated with levothyroxine (LT4) and some may need combination treatment with triiodothyronine (LT3) despite normal levels of thyroid stimulating hormone (TSH), according to thyroid expert Antonio C. Bianco, MD, PhD.
Speaking to a crowded room at the recent American Association of Clinical Endocrinology (AACE) Annual Meeting 2022, Bianco summarized the history of thyroid replacement treatment, the emerging data focusing on the subset of patients remaining symptomatic on levothyroxine, and how the clinical guidelines have evolved from stating that LT4 is the one and only treatment to now acknowledging that some patients may need combination therapy.
“Treatment with LT4 will leave residual symptoms in about 10%-20% of the patients. Before planning a thyroid surgery, this issue should be discussed with patients. We used to tell patients that LT4 treatment resolves all symptoms, but this is not true for all. For those…who remain symptomatic while on LT4, physicians should attempt combination therapy,” Bianco told Medscape Medical News.
The acknowledgement, he said, is “critically important because patients are greatly aggravated by the fact that physicians are satisfied with a normal serum TSH and yet they do not feel well. This comes out in every survey we and others have done.” Common residual symptoms include weight gain, fatigue, and “brain fog,” which clinicians sometimes dismiss as psychological, he noted.
However, Bianco cautioned that before attempting combination therapy, it’s important to make sure that patients don’t have other comorbidities that could explain the residual symptoms, including perimenopause/menopause, obesity, vitamin B deficiency, anemia, or other autoimmune diseases.
Bianco is professor of medicine at the University of Chicago and author of more than 80 publications on the thyroid as well as an upcoming book.
Doctors Follow Guidelines…
Asked for comment, session moderator Alex Tessnow, MD, of the University of Texas Southwestern Medical Center, Southlake, told Medscape Medical News: “I agree with him entirely. I think the biggest challenge we have now is lack of data. It’s amazing how common hypothyroidism is. Almost 20% of women over age 65 have an elevated TSH.”
“Levothyroxine is the number one prescribed drug in the country. And of all those trials, only three have more than one hundred patients in them. That’s how unstudied this topic is. We really need to know more.”
Among the reasons the topic remains controversial, Tessnow said, are that “for years the guidelines said levothyroxine is the first choice. Doctors don’t want to deviate from the guidelines.”
And he noted that some doctors “may be fearful of LT3 being so potent and short-acting and potentially causing cardiac arrhythmias.”
“Levothyroxine is so long-acting it’s easy to give. Often patients have to take LT3 more than once a day on an empty stomach. There’s no combination pill as of now.”
Bianco noted that two investigational slow-release LT3 molecules are currently in the pipeline and could alleviate some of these concerns.
Trials Should Focus on Those Not Doing Well on Levothyroxine Alone
Tessnow and Bianco both noted that most of the studies that have failed to show a benefit of combination LT4+LT3 treatment have included overall populations with hypothyroidism rather than focusing just on those who remain asymptomatic with LT4.
“It is possible that those individuals most likely to benefit from combination therapy may not yet have been included in trials in sufficient numbers in order to provide adequate power for detecting a response,” Bianco said.
Tessnow agreed: “The sheer number of people who are doing fine on levothyroxine are going to cover up the potential benefit the combination would give those who are most symptomatic. We need to focus our studies on those patients”.
In fact, this research gap was among the conclusions from an expert consensus statement published in March 2021, following a joint conference of the American Thyroid Association (ATA), the British Thyroid Association (BTA), and the European Thyroid Association (ETA). Bianco was one of the statement’s authors.
This “acknowledges that the previous clinical trials were not adequately designed,” says Bianco, adding, “there is a need for new clinical trials.”
Many Patient Reports Document Dissatisfaction With LT4 Treatment
Numerous patient-generated publications have documented residual symptoms with LT4 treatment alone, including higher levels of symptoms on questionnaires, deficits in neurocognitive functioning, impact on psychological well-being, and “brain fog,” as reported by Medscape Medical News and published in December 2021, and notably, a study from Bianco’s group in 2018, which found “prominent dissatisfaction” with their treatment and their physicians.
“Some changed physicians five to ten times. We concluded there was a significant burden of unsuccessfully resolved symptoms among patients with hypothyroidism,” Bianco said during his talk.
“Some say patient preference isn’t a clinical outcome, but we have to consider it…To not listen to the patient in what they prefer is unfair and just gives them more reason to be mad at us,” he added.
History and Physiology: Why LT4 Is Used But May Not Be Enough for SomeTreatment of hypothyroidism using implantation of a sheep’s entire thyroid gland was first described in 1890, followed by subcutaneous injections of sheep’s thyroid extract. A short time later, thyroid extract by mouth was introduced. In 1965, a study demonstrated efficacy of a 3.5:1 mixture of synthetic LT4 and LT3.The shift to LT4 monotherapy happened in 1970, with a study published in the Journal of Clinical Investigation showing that T4 was converted to T3 in humans, “which all interpreted as ‘no need to use thyroid extract,’ then LT4 became the standard of care,” Bianco said.He then explained the physiologic basis for why some patients may not fare well with LT4 alone.TSH in the normal range doesn’t mean T3 and T4 are normal. “The thyroid is hard-wired to preserve serum T3,” he said.But once the patient develops hypothyroidism, the thyroid no longer responds to TSH, and serum T3 is only maintained via conversion of T4 to T3. Although LT4 is used to normalize serum TSH levels, that occurs before serum T3 is normalized, resulting in lower serum T3 levels and relatively higher serum T4 levels.The lower T3 level with normal serum TSH explains the residual symptoms, Bianco explained. “Thus, by adding small amounts of LT3 to the regimen with LT4 we can normalize serum TSH but with normal serum T4 and T3 levels,” he said.So why do most patients report feeling fine with LT4 alone? “We do not have the answer to this question. Multiple factors could explain it, including genetics,” he told Medscape Medical News.
How Can Combination Therapy Be Given Safely?
The 2012 guidance from the ETA provided specific information for how combination therapy should be prescribed by reducing LT4 and replacing a small amount with LT3 in order to keep TSH within normal range.
For example, if the patient is taking 100 µg/day of LT4, drop that to 87.5 µg/day and add 5 µg/day of LT3. Similarly, 200 µg/day of LT4 should be dropped to 175 µg/day and 10 µg/day of LT3 added.
Patients should undergo enhanced follow-up, with measurement of serum T3 at baseline and 3 hours after LT3.
This approach should be avoided in patients with cardiac conditions or concomitant use of other medications that could potentiate the effects.
Indeed, while there has been concern about cardiac effects of LT3, trials following nearly 1000 patients for as long as 1 year have shown that the addition of LT3 only minimally affects serum TSH, heart rate, or blood pressure. Bone turnover markers remained within normal range in two studies.
Another large study published in 2016 also showed no long-term effects of LT3 on cardiovascular disease outcomes or fractures, although there was increased use of antipsychotic medications.
“Given the new safety data, physicians could be more liberal with this form of therapy as they treat patients with residual symptoms,” he concluded.
Tissue accumulation of advanced glycation end products (AGEs) is associated with the presence of hypercortisolism, suggesting a potential future noninvasive method to assist in the diagnosis of Cushing syndrome, new research suggests.
Tissue accumulation of AGEs — harmful compounds formed by glycation of macromolecules — has been implicated in aging, diabetes, and cardiovascular disease. Now, in a new single-center prospective study, a group of 208 patients with endogenous hypercortisolism was found to have significantly higher median tissue AGE levels than 103 reference subjects without hypercortisolism.
The findings were presented at the American Association of Clinical Endocrinology Annual Meeting 2023 by Rashi Sandooja, MD, an endocrinology fellow at the Mayo Clinic, Rochester, Minnesota.
“Diagnosis of endogenous hypercortisolism can be quite challenging. Often patients can have nonspecific symptoms with biochemical testing being equivocal. In these situations, new biomarkers of hypercortisolism such as AGE measurement could potentially be useful,” Sandooja told Medscape Medical News.
“After proper validation, it could help clinicians in cases which may not be straightforward and could serve as an additional” instrument in the toolkit to reach a conclusive diagnosis, she added.
Asked to comment, session moderator Anupam Kotwal, MD, told Medscape Medical News: “I think it’s very exciting data…I envision its use in mild autonomous cortisol secretion, where there are not a lot of overt Cushing features but they may have a small adrenal mass…It might be used to guide care when there’s not a clear-cut answer.”
However, he cautioned that more validation is needed to determine the correlates of AGEs by different etiologies and magnitudes of cortisol excess.
Moreover, “Skin can become thin in hypercortisolism, so is [the reader device] just detecting it more with skin testing? I think a blood test for validation would be a very good next step,” added Kotwal, who is an assistant professor in the Division of Diabetes, Endocrinology and Metabolism at the University of Nebraska, Omaha.
A brain bleed (brain hemorrhage) can be life-threatening and may cause significant long-term complications.
A brain bleed (brain hemorrhage) occurs when blood vessels in the brain are damaged, such as by a head injury, problems with blood clotting and/or damage to the blood vessels in the brain, or a ruptured brain aneurysm. Bleeding in the brain increases pressure on brain tissue and can lead to serious complications.
There are several types of brain bleeds, all of which can cause significant complications and can be life-threatening. While most people who experience a brain bleed will live, they usually experience problems with memory, speech, or movement, depending on the location of the brain bleed.
A brain bleed can be life-threatening when blood enters the fluid-filled space around the brain (the subarachnoid space), in what is called a subarachnoid hemorrhage. When blood flows into the subarachnoid space it can spread quickly and put pressure on the entire brain so even parts of the brain that aren’t close to the bleeding blood vessel can be damaged.
Left untreated, a subarachnoid hemorrhage can lead to unconsciousness and life-threatening complications such as an irregular heartbeat and respiratory arrest. It can cause brain damage that may result in long-term or permanent problems such as speech difficulty or paralysis.
When a brain bleed occurs within the brain tissue, it’s called an intracerebral hemorrhage (a brain hemorrhage) and the blood presses against the tissue from the inside and against other blood vessels in that area causing the surrounding brain tissue to die. Depending on the function of that part of the brain, problems with vision, speech, movement, or sensation can occur. It can also lead to life-threatening complications.
Blood can also leak into the small gaps between the meninges (membranes covering the brain) in a subdural hematoma or between the meninges and the skull in an epidural hematoma. These conditions can also cause brain damage.
What Are Symptoms of a Brain Bleed?
Symptoms of a brain bleed (brain hemorrhage) vary depending on the location and severity of the bleeding and the amount of brain tissue is affected. Symptoms can develop suddenly or gradually over time. It’s important to seek medical attention immediately if a brain bleed is suspected.
Cocaine and other illicit drugs can weaken blood vessels
Some prescription drugs can also increase the risk of a brain hemorrhage
Blood vessel abnormalities, or arteriovenous malformations (AV)
A rare cause of brain bleeds
A group of blood vessels in the brain does not form correctly before birth and can cause leaking arteries or veins
How Is a Brain Bleed Diagnosed?
A rapid diagnosis of a brain bleed (brain hemorrhage) is needed to get prompt and proper treatment. The cause of a brain bleed is not always apparent when a patient arrives at an emergency room unless there is obvious head trauma. Patients who are conscious may be asked to describe their symptoms.
Brain bleeds (brain hemorrhages) may be treated surgically or nonsurgically, depending on the cause, severity, and location of the brain bleed, and the patient’s overall health.
Early treatment is aimed at stabilizing the patient in the intensive care unit (ICU) and includes:
A procedure to drill a hole into the skull that allows excess blood to drain
Craniotomy
An incision through the scalp is made and a special saw is used to remove a piece of the skull to allow the brain to expand and relieve the pressure created by the bleeding
External ventricular drain
A catheter is placed into the cavities (ventricles) of the brain to relieve pressure and decompress the cerebrospinal fluid
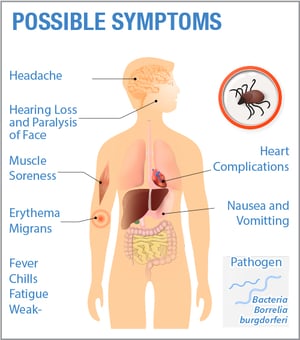
Lyme disease symptoms are wide-ranging, with more than a hundred different symptoms recorded. Symptoms can also change over time, as the bacteria spreads throughout the body. To make things more confusing, Lyme disease symptoms will also vary from patient-to-patient.
Lyme disease can mimic hundreds of other conditions since its symptoms mirror many medical problems such as multiple sclerosis, arthritis, chronic fatigue syndrome or lupus, and is sometimes known as “The Great Imitator” because of this. Click here for a more complete list of possible symptoms.
Symptoms can play a key role in diagnosing Lyme disease. Due to the lack of an accurate diagnostic test, many patients are diagnosed based on a combination symptoms and diagnostic testing. This makes it extremely important for patients to keep track of all the symptoms they experience, to share with their healthcare provider.
When do Lyme disease symptoms appear? Learn about the Stages of Lyme disease:
Lyme disease symptoms can vary based on stage of the disease (early, late, post-treatment, or chronic) and if other tick-borne infections are present and can change over time.
Symptoms in acute Lyme disease
Acute Lyme disease (aka: early localized LD) occurs days to weeks after the initial tick bite and infection, in which the bacteria have not yet spread from the site of infection in the skin.
The most common symptoms in acute (aka: early localized) Lyme disease are the ones people are most familiar with, because they are symptoms often shared with other illnesses; however, it’s important to recognize that they could indicate Lyme, and you should see a Lyme-treating physician right away.
Erythema migrans (AIR-ih-THEEM-ah MY-grans) rash or EM rash. This rash begins at the site of the tick bite about a week after the bite, and gradually expands. Note: The center of the rash may clear, giving the rash the appearance of a “bulls-eye.” Rashes may take on many different shapes and not all rashes will have a bulls-eye appearance. There can be multiple rashes on the body. While a rash is characteristic of Lyme disease, many people will not develop a rash at all.
Fever
Fatigue
Aches
Chills
Swollen lymph nodes
Other flu-like symptoms
Symptoms in early disseminated Lyme disease
Early disseminated Lyme disease occurs days to months after infection, in which the bacteria have begun to spread. There is a wide range of possible symptoms at this stage, including:
Severe headaches and neck stiffness
Arthritis, especially in the knees or other large joints
Muscle aches and pains
Heart palpitations or shortness of breath (Lyme carditis)
Facial paralysis on one or both sides (also known as Bell’s palsy)
Numbness or tingling in the hands or feet
Extreme fatigue
Symptoms in late stage Lyme disease
Late stage Lyme disease, which can include post-treatment, chronic, and neurological, occurs months to years after infection, in which the bacteria have spread throughout the body.
The symptoms of late disseminated disease are similar to those of early disseminated disease, but may be more extensive, more severe, and longer lasting. Late symptoms may also include:
neurologic features including vertigo or dizziness,
difficulty sleeping
mental fogginess
difficulty following conversations
difficulty processing information
Some common questions …
When should you see a doctor for Lyme disease?
As soon as you have visual proof of a tick bite (remember to save the tick and send in for testing) or you suspect Lyme disease based on the symptoms listed above, consult a Lyme treating physician. The sooner treatment is started after a tick bite, the more effective it is.
Do symptoms of Lyme disease come and go? Is it OK to stop treatment if symptoms disappear?
No. The absence of symptoms does not mean the disease is gone. It’s important to consult with your doctor even if symptoms disappear.
How long do Lyme disease symptoms last? Do you ever get rid of Lyme disease? What if symptoms persist after treatment?
It’s important to remember that up to 20% of those diagnosed and treated early will continue to have symptoms. This means that even if you have undergone treatment, you could still have Lyme disease. Keep track of all symptoms and share with your healthcare provider.
It remains unclear why some patients, despite antibiotic treatment, continue to experience symptoms of Lyme disease. Possible explanations include persistence of antibiotic-tolerant bacteria, autoimmunity triggered by prior infection with the Lyme bacteria, or perhaps co-infection with other tick-borne pathogens. These mechanisms of chronic disease are not mutually exclusive.
What if you suspect Lyme disease and have never been diagnosed or treated?
If you suspect Lyme disease, even though you don’t recall a tick bite or a rash, it’s important to consult with a Lyme physician right away. Untreated, Lyme disease can spread to other parts of your body for several months to years after infection, causing arthritis and nervous system problems.

 Lyme disease can mimic hundreds of other conditions since its symptoms mirror many medical problems such as multiple sclerosis, arthritis, chronic fatigue syndrome or lupus, and is sometimes known as “The Great Imitator” because of this.
Lyme disease can mimic hundreds of other conditions since its symptoms mirror many medical problems such as multiple sclerosis, arthritis, chronic fatigue syndrome or lupus, and is sometimes known as “The Great Imitator” because of this.  The most common symptoms in acute (aka: early localized) Lyme disease are the ones people are most familiar with, because they are symptoms often shared with other illnesses; however, it’s important to recognize that they could indicate Lyme, and you should see a Lyme-treating physician right away.
The most common symptoms in acute (aka: early localized) Lyme disease are the ones people are most familiar with, because they are symptoms often shared with other illnesses; however, it’s important to recognize that they could indicate Lyme, and you should see a Lyme-treating physician right away.