Whether concurrent chemotherapy with radiotherapy (CRT) is effective for elderly patients with head and neck cancer is a controversial topic. This study aimed to analyze the effectiveness of CRT vs. radiation therapy (RT) among elderly patients in Japan.
Methods
Data from the Head and Neck Cancer Registry of Japan were extracted and analyzed. Patients with locally advanced squamous cell carcinoma of the oropharynx, hypopharynx, or larynx who received definitive CRT or RT between 2011 and 2014 were included.
Results
CRT was administered to 78% of the 1057 patients aged ≥ 70 years and 67% of the 555 patients aged ≥ 75 years. For the patients aged ≥ 75 years, the overall survival (OS) rate was significantly better in the CRT group than in the RT group (P < 0.05), while the progression-free survival (PFS) rate was not significantly different (P > 0.05). The add-on effect of CRT was significantly poor in elderly patients (P < 0.05), and it was not a significant factor in the multivariate analysis for patients aged ≥ 75 years. After propensity score matching, there were no significant differences in the OS and PFS rates between the patients aged ≥ 70 years and those aged ≥ 75 years (all, P > 0.05).
Conclusion
Although aggressive CRT is administered to elderly patients in Japan, its effectiveness is uncertain. Further prospective randomized trials are needed to verify whether CRT is superior to RT alone for elderly patients.
Patients who have undergone pelvic radiotherapy may live with low-grade chronic inflammation of the lower intestine 20 years after the treatment. This has been shown in a study by researchers at the University of Gothenburg.
Radiotherapy is often necessary to cure or slow down a cancer. Even though today’s radiotherapies feature a high level of precision, healthy tissue in and around the radiation field is still affected. This study highlights a previously unknown side effect of radiotherapy to the lower abdomen.
The mucous membrane of the large intestine is normally protected against contact with bacteria in feces by a thin barrier of mucus. In the current study, which was published in the journal eBioMedicine, researchers at the University of Gothenburg have shown that radiotherapy to the pelvic area affects this thin layer of mucus, allowing bacteria to come into contact with cells on the surface of the intestine. This could be a reason for the low-grade inflammation that the researchers also found in intestines that had been exposed to radiotherapy several years previously.
“It can be hard to detect low-grade inflammation,” says Sravani Devarakonda, a researcher at the University of Gothenburg’s Sahlgrenska Academy and lead author of the study. “This is the first time researchers have been able to show with certainty that this is happening in cancer survivors, a long time after pelvic radiotherapy has ended. We saw signs of low-grade inflammation as late as twenty years after radiotherapy.”
It is common for those who have received radiotherapy for cancer of the cervix, prostate, or rectum, for example, to experience intestinal symptoms many years after completing their treatment. The severity ranges from tenesmus (a feeling of not having emptied the bowels properly despite multiple toilet visits), to very frequent diarrhea (fifteen times a day or more).
The study is based on samples from 28 people, including 24 cancer survivors. Four of the subjects had not undergone radiotherapy and served as a control group. Among the subjects, the shortest time since radiotherapy was two years and the longest time was twenty years. The median was five years between the end of radiotherapy and intestinal biopsy.
The study was carried out in broad collaboration between clinical and basic science researchers at the University of Gothenburg, Sahlgrenska University Hospital and Karolinska Institutet. Responsible for the research cooperation is Cecilia Bull, an associate professor at the University of Gothenburg’s Sahlgrenska Academy. “Our study subjects included both patients who had received traditional radiotherapy and those who had the more targeted form, IMRT. We saw low-grade inflammation in both groups. The damage to the surrounding tissue can be limited by IMRT, but there are still long-term inflammatory changes,” she says.
The next step for the researchers will involve finding out whether this low-grade inflammation after radiotherapy causes some of the intestinal symptoms often seen in these cancer survivors and, if so, which symptoms are due to the inflammation.
Research is already being carried out to find ways of strengthening the intestines’ resistance to radiotherapy, so that long-term symptoms which affect quality of life can be alleviated or even prevented entirely. In an extensive study involving more than 300 patients, researchers are trying to strengthen the protective mucosal barrier by adding extra dietary fiber to the diet before beginning radiotherapy.
For individualized radiotherapy, high-precision delineation and characterisation of the tumour is critical. If highest radiation doses are delivered in a targeted fashion, the chance of tumour cell kill increases and tumour control probability is enhanced.
Precise delineation of the target in its anatomical/geometric and functional/biological aspects has long been a great dilemma for radiation oncologists. Traditionally, large margins were added to the tumour volume to account for uncertainties of tumour visualisation and target delineation. This results in a high risk of ‘collateral damage’ to healthy tissues – and in return the radiation dose to the tumour must be lowered, compromising the chance of tumour control. Technological progress has enabled advances in cross-sectional imaging, molecular imaging, and 3-D reconstruction. Introduction of CT was the first key development towards modern 3-D radiotherapy planning. Additional information from other imaging modalities such as magnetic resonance (MR) imaging, MR spectroscopy, or PET, has further improved the target volume definition process by providing better soft tissue contrast or physiologic information. Parallel innovations in radiation therapy technologies enable millimetre-precision with the introduction of stereotactic techniques and online 3-D image-guided radiation therapy (IGRT) based on linac-mounted Cone Beam CT systems. These parallel innovations have brought the fields of radiation oncology and radiology, which had drifted apart in the past decades, together on a novel level. Today, radiation oncologists are able not only to see the tumour but also treat the tumour with highest precision for each individual patient. However, despite 3-D CT-based planning, the definition of target volumes has still remained a highly subjective process, as shown by several ‘inter-user’ target volume definition studies. This is likely related to inherent uncertainties in tumour margin definition by anatomical imaging modalities that frequently do not adequately delineate the biologic/physiologic tumour target. PET as a functional imaging modality adds critically to the existing panel of imaging methods. PET provides physiological information of tissue and tumour metabolism. Increased FDG uptake indicates areas of higher glucose metabolism, which is characteristic of uncontrolled growth of tumour cells. However, PET alone lacks correlative anatomical information. Conversely, CT lacks this physiological information but provides superior definition of anatomical detail, tumour localisation and tissue density. The ‘marriage’ of the two modalities as a PET/CT provides combined imaging acquired at the same time without patient motion and is superior to either PET or CT imaging alone. This allows incorporation of biological, molecular, and pathophysiological parameters directly into the radiation therapy algorithms. Incorporating these principles has several aspects for the therapy algorithm, that all build on each other: Proper staging, anatomical and molecular target delineation for radiation therapy planning and image-guided treatment, treatment adaptation, and outcome prediction, and treatment adaptation based on outcome predictions during or after therapy (Fig. 1). Ample evidence has now accumulated that lung tumour delineation can be significantly refined by the use of PET/CT compared to CT alone, and impact treatment planning in half of patients. Improved delineation of the target volume by PET CT reduces the target volume in approximately one fourth of patients, especially for lesions masked by non-cancerous tissue (fibrosis or atelectasis), that is very challenging to differentiate from tumour by standard imaging. Reducing the target volume permits a decrease in the radiation dose to dose-limiting normal tissues (lung, spinal cord, oesophagus), and provides the opportunity to escalate the radiation dose for better tumour control. Conversely, an increase in the target volume based on PET/CT occurs in about one fourth of cases, where PET/CT identifies tumour involvement that is not evident by CT alone. Integrating PET-CT into the radiation therapy planning process has the potential to reduce risk for inadequate coverage of the tumour within the radiation ports (‘geographic misses’), and reduces inter-user variability in target definition. The higher precision in delineating tumour extent, and excluding non-cancerous tissues, open the door to dose escalation to the tumour while omitting large margins or ‘elective’ target volumes. Radiobiologic modelling studies of such dose escalation in stage N2-3 lung cancer have estimated an increase in tumour control probability by 13-18% – surpassing the gains achievable by many adjuvant therapies. Similarly, in head and neck cancer, target delineation through PET/CT fusion has shown benefit. Initially used to assess tumour response and guide management of involved cervical lymph nodes after radiation therapy, the technique of co-registration has evolved to PET/CT-guided intensity-modulated radiation (IMRT). This enables selective intensification of the radiation dose (‘dose painting’) in tumour sub-regions that are most metabolically active or in hypoxic areas using 18F-MISO PET/CT as a hypoxia tracer. Now that PET/CT planning is becoming established in lung, head and neck cancer, other tumours, such as gastrointestinal, anal carcinoma, prostate carcinoma, lymphoma and gynaecologic tumours are also being studied. For example, at initial diagnosis of anal carcinoma, 15-39% of the inguinal lymph nodes are involved. In the future, PET may be used as a decision tool whether to include the inguinal nodes to the target volume or not (Fig. 2) However, the use of this new paradigm is not without challenge. Not all metabolically active areas within malignant lesions represent tumour. Inflammation and radiation-induced reactive changes can represent challenges. Although PET/CT has reduced inter-observer variability in tumour delineation and has further refined how we ‘see’ tumours in anatomical and metabolic aspects, the optimal use and the proper integration of this relative expensive technique into cancer therapy has to be further defined and long-term follow-up studies to assess the impact on ultimate therapy outcome have yet to be completed. This novel approach holds the promise to improve cancer care in many malignancies. Its effective implementation will bring us closer to a Personalised Radiation Medicine approach in cancer therapy.
Patients with cancer often question whether the risks and adverse effects associated with a specific treatment outweigh the benefits. This decision is highly personal and dependent on individual values and goals. Many patients value independence and quality of life over cancer recurrence and rely on physicians to recommend treatments that align with those goals.
Although radiotherapy after breast conserving surgery is usually well tolerated, adverse effects include telangiectasia, breast pain, induration, retraction, and rarely secondary cancers and ischemic cardiac disease. Some women at low risk for local recurrence may forego radiation therapy, but outcome studies are needed to predict the effect on recurrence risk.
Investigators of the prospective LUMINA cohort study examined the incidence of local recurrence associated with omitting radiotherapy following breast conserving surgery and endocrine therapy in a subset of 500 women with a new diagnosis of low-risk invasive breast cancer. The women were ≥55 years of age, had a primary tumor < 2 cm in diameter, negative axillary nodes, and luminal A breast cancer, which is the least proliferative and associated with the best prognosis.
At 5 years, the incidence of local recurrence associated with the omission of radiotherapy was 2.3% (90% confidence interval, 1.3 to 3.8). This rate will likely increase after longer follow up. In a recent study and a study published in 2013, 10-year recurrence rates approximated 10% in patients with early breast cancer who had omitted radiotherapy. Therefore, longer follow up of the Lumina study is needed to guide patient-physician conversations regarding long-term risks of foregoing radiotherapy, as many breast cancer survivors now live 20 to 30 years after treatment, even those diagnosed at a relatively older age. In the meanwhile, women with low-risk breast cancer who are aged 55 years and older can use these data to help inform decisions about whether to include radiotherapy in their treatment plan.
Patients with clinical stage T2N1 or T3N0–1 rectal cancers who are eligible for sphincter-sparing surgery might be able to avoid preoperative radiotherapy if given induction FOLFOX prior to surgery.
Total neoadjuvant therapy for patients with locally advanced rectal cancer — whereby chemoradiotherapy and chemotherapy are administered prior to surgery — offers the potential for enhanced treatment tolerance and delivery, improvements in pathologic response at surgery, and nonoperative management for colostomy candidates who achieve a clinical complete response. However, for patients with high- or mid-rectal cancers undergoing total mesorectal excision, the role of neoadjuvant radiotherapy has been increasingly questioned.
To test the concept of avoiding neoadjuvant radiotherapy in this setting, investigators conducted a multicenter, noninferiority, randomized, phase 3 trial (PROSPECT) involving 1128 patients with clinical stage T2N1 or T3N0–1 high- or mid-rectal cancer who were candidates for sphincter-sparing surgery. Most patients were male, half had T3N1 cancers, 91% had T3N0–1 cancers, and 64% had cancers 5 to 10 cm from the anal verge. Half of patients received conventional neoadjuvant chemoradiotherapy, surgery, and adjuvant chemotherapy. The other half received induction chemotherapy with 6 cycles of FOLFOX, and those with a ≥20% reduction in the primary tumor proceeded to surgery without radiotherapy and received adjuvant chemotherapy.
At 5 years, disease-free survival was noninferior with induction FOLFOX versus chemoradiotherapy (80.8% vs. 78.6%; hazard ratio, 0.92, P=0.005), meeting the primary endpoint. Rates of local recurrence were similar with FOLFOX or chemoradiotherapy (1.8% and 1.6%, respectively), as were 5-year overall survival (89.5% and 90.2%) and pathologic complete response (21.9% and 24.3%). Nearly 90% of patients treated with FOLFOX avoided radiotherapy; 9.1% required neoadjuvant chemoradiotherapy after FOLFOX, and 1.4% required postoperative chemoradiotherapy. No new safety signals were observed.
Comment
The large, well-conducted trial indicates that the vast majority of patients with clinical stage T2N1 or T3N0–1 rectal cancers who are eligible for sphincter-sparing surgery can avoid the use of preoperative radiotherapy if given induction FOLFOX. This trial will change practice. The use of radiotherapy preoperatively will increasingly be relegated to more advanced rectal cancers or to patients requiring a permanent colostomy.
Adenocarcinoma of the oesophagus and gastro-oesophageal junction represent a large burden of cancer death in the Western World with an increasing incidence. In the past two decades, the overall survival of patients on a potentially curative treatment pathway has more than doubled due to the addition of perioperative oncological therapies to surgery. However, patients often fail to respond to oncological treatment or struggle to complete their treatment after surgery. In this review, we discuss the current evidence for total neoadjuvant therapy and options for assessment of treatment response.
Background
Oesophageal cancer is the 14th most common cancer in the United Kingdom, with adenocarcinoma being the most common histological subtype, and it is the 7th most common cause of cancer death [1]. The overall benefit of preoperative or perioperative oncological therapy (chemotherapy or chemoradiotherapy) for oesophageal and junctional adenocarcinoma is widely recognised, most notably demonstrated by landmarks trials including OEO2, MAGIC, FLOT4 and CROSS with overall 5-year survival reaching 47% in CROSS, a large improvement from 17–23% for surgery alone [2,3,4,5]. In this review, we discuss the effect of neoadjuvant chemotherapy (nCT) and chemoradiotherapy (nCRT) on surgical resection margin, lymph node downstaging, and primary tumour pathological response and how this impacts survival. We also review the challenges of delivering perioperative therapy and discuss total neoadjuvant therapy as a potential novel treatment regimen for patients with resectable oesophageal cancer.
Total neoadjuvant therapy—is it possible in oesophageal cancer?
Total Neoadjuvant Therapy (TNT), where all oncological treatment is delivered before surgery, is beneficial in other cancer types. This experience should be exploited with regard to potential issues which could arise using the TNT approach for oesophageal cancer, such as increased toxicity and poorer tolerability of neoadjuvant therapy given the higher chemotherapy dose and subsequent failure of progression to surgery.
For example, TNT has gained prominence in the management of locally advanced rectal cancer and has now been incorporated into national rectal cancer guidelines [6]. A summary of key trials of TNT in rectal cancer is shown in Table 1. The RAPIDO trial included high-risk patients with T4 or N2 clinical staging or other high-risk factors, and patients in the TNT group received 6 cycles of CAPOX or FOLFOX4 chemotherapy following a short course of radiotherapy [7]. In the UNICANCER-PRODIGE 23 trial, patients with T3-T4 and N0 clinical disease were included, arguably less advanced disease than in RAPIDO [8]. This trial used the more aggressive FOLFIRINOX chemotherapy before nCRT and showed a better 3-year disease-free survival in the TNT group and the trial concluded that there was a lower toxicity rate in the TNT group despite using FOLFIRINOX. These trials did not show any improvement in overall survival with TNT, but two meta-analyses have supported the improved oncological outcomes using TNT and consensus has shifted in favour of TNT in locally advanced rectal cancer [9, 10]. As well as these trials, there are various other smaller studies of TNT in rectal cancer, which consistently show better tolerability, less toxicity, and higher rates of planned treatment completion when the TNT approach is used [11,12,13]. Furthermore, excellent results have been reported in Phase 2 trials of TNT for borderline resectable pancreatic adenocarcinoma, with 2-year progression-free and overall survival of 43% and 56%, respectively and a median PFS of 48.6 months in those undergoing resection with 2-year OS of 72% [14]. There is evidence to suggest that TNT enables the delivery of intended systemic therapy with a greater chance of pCR and without compromising on surgical resection in pancreatic adenocarcinoma [15]. A recent systematic review and meta-analysis suggest superior oncological and pathological outcomes with TNT compared to standard neoadjuvant therapy [16]. Phase III trials of TNT in pancreatic adenocarcinoma are currently ongoing [17].Table 1 A summary of key trials of total neoadjuvant therapy in rectal cancer.
Current evidence for TNT in oesophageal adenocarcinoma is limited to retrospective or small pilot study evidence but is promising and summarised in Table 2. Due to the non-randomised and largely retrospective nature of these studies, it is difficult to draw strong conclusions, however, there appears to be a consistently high disease-free and overall survival with intensified neoadjuvant regimens compared to standard of care. In addition, there are high rates of treatment completion and surgical resection as evidenced by in patients receiving FLOXFOX + CROSS [18]. Although there was an 80% grade 4 toxicity rate in the prospective study by Wo et al., the majority of this was due to subclinical lymphopenia. When patients with M1 nodal disease were excluded, 2-year progression-free survival was 78% in this study [19]. There are several ongoing trials of TNT or enhanced neoadjuvant therapy in patients with oesophageal or oesophagogastric junction adenocarcinoma. These are summarised in Table 3.Table 2 Current evidence for total neoadjuvant therapy oesophagogastric adenocarcinoma.
Full size tableTable 3 Ongoing trials of total neoadjuvant therapy in oesophageal or gastroesophageal junction adenocarcinoma.
The, albeit limited, existing evidence in oesophageal and junctional adenocarcinoma, as well as other solid tumours suggests a significant survival benefit for patients receiving TNT and allows more patients to complete all oncological therapy and surgery. Prospective, randomised controlled trials are needed to compare treatment modalities directly using the TNT approach in oesophageal cancer.
Total neoadjuvant therapy—assessing treatment response
If patients are to embark on a prolonged course of preoperative treatment, ideally it should be a precision medicine strategy with mechanisms in place for an as early as possible assessment of response and adaption of treatment accordingly. Again, rectal cancer might help us to address this problem. The OPRA trial compared surgical resection to a “watch-and-wait” approach following TNT in patients with locally advanced rectal cancer [20]. This trial used an extensive surveillance protocol with a combination of digital rectal examination, flexible sigmoidoscopy (every 4 months for the first 2 years, then 6 monthly), CEA, MRI, CT chest/abdomen/pelvis and colonoscopies at year 1 and year 5 and demonstrated that organ preservation is safe and achievable in half of patients. Findings from the International Watch & Wait Database emphasise the importance of endoscopic surveillance [21]. We can also look to oesophageal squamous cell carcinoma, for which definitive chemoradiotherapy (dCRT) is a treatment option. Surveillance after dCRT includes regular OGD and biopsies, EUS, CT scan and Fluorine 18 fluorodeoxyglucose (FDG) positron emission tomography (PET-CT) [22, 23]. The SANO trial is ongoing, which investigates the use of active surveillance in an organ-sparing “watch-and wait” approach for patients with oesophageal squamous cell and adenocarcinoma and utilises PET-CT, OGD with biopsies and EUS with FNA of suspicious nodes in its clinical response evaluation [24].
Generally, PET-CT has been shown to be a feasible and accurate modality for detecting response to neoadjuvant therapy in oesophageal cancer [25,26,27,28]. However, its accuracy in detecting non-response is questionable, with one study suggesting reliable detection of non-responders in gastric and Siewert II-III cancers [29], and another suggesting a lack of accuracy in detecting non-response in oesophageal cancer [30]. In the absence of a “one size fits all” endoscopic or radiological surveillance modality and a lack of reliable tumour markers in oesophageal adenocarcinoma, it may be that a multimodality approach is required to assess response, and more importantly, non-response to preoperative treatment. The burden of such an approach for patients and the health care system will need to be understood.
Circulating tumour DNA (ctDNA) is well established as a marker of minimal residual disease and correlates with recurrence and survival in patients undergoing neoadjuvant therapy for rectal cancer [31,32,33,34,35,36]. The use of ctDNA in oesophageal cancer is still being established. The prospective pilot study of TNT in oesophageal adenocarcinoma analysed ctDNA at various time points, including post-chemoradiotherapy and post-surgery [19]. Those with undetectable ctDNA post-chemoradiotherapy and post-operatively had significantly lower recurrence rates compared to those with detectable ctDNA at these time points (8% vs 75% post-CRT, p = 0.004; 0% vs 40% post-op, P = 0.045). ctDNA has been identified in other studies as a useful biomarker of recurrence and treatment response in oesophageal cancer [37,38,39]. This highlights the potential utility of ctDNA as a biomarker of response to treatment, a predictor of recurrence and its utility in planning adjuvant treatment where needed. It is essential that any future trials of TNT incorporate several modalities to monitor response to treatment such as PET-CT, endoscopic surveillance and ctDNA.
Surgical resection margin
The importance of complete surgical excision of oesophageal and gastroesophageal junction (GOJ) cancers is long established. The 3-year survival in those with a complete surgical resection (R0) in OEO2 was 42.4% compared to 18.0% and 8.6% in those with R1 and R2 resections, respectively [40]. Patients who undergo preoperative oncological therapy are more likely to have an R0 resection. This is particularly evident in regimens where all the therapy is delivered pre-operatively, for example, in the CROSS trial, those receiving preoperative chemoradiotherapy had an R0 rate of 92% compared with 69% in those having surgery alone [5]. Neoadjuvant chemoradiotherapy has been shown to deliver better local tumour control (R0 resection rate) than preoperative chemotherapy. In the Neo-AEGIS study, which compared neoadjuvant CRT (CROSS) with perioperative chemotherapy, R0 in the CROSS group was 95% compared to 82% in the perioperative chemotherapy group [41]. Similar results have been shown for R0 rate in the NeoRes I study, where chemoradiotherapy (R0=89%) and chemotherapy (R0=71%) were compared in the neoadjuvant setting alone in patients with T1-T3 disease[42]. However, there were comparable R0 rates between nCRT and nCT in the POET study (72% vs 69%), in patients with T3-T4 disease [43]. It should be noted that in these comparative studies older chemotherapy regimens were largely used in the chemotherapy arm rather than FLOT. The ESOPEC trial is currently ongoing, which directly compares FLOT and CROSS [44]. In the FLOT4 trial, where 83% of patients who received perioperative FLOT chemotherapy had T3/T4 disease and 78% had node-positive disease, there was an R0 resection rate of 92% in those with resected specimens [45]. The recent DANTE trial, in which 93% of patients completed pre-op FLOT cycles, had similarly high R0 rates of 91% in the FLOT arm and 92% in FLOT + atezolizumab [46]. Indirect comparison of the studies above is limited by significant differences in the study population, notably differences in histological type, disease location, disease stage, age, and performance status. This highlights the need for precise patient selection in clinical trials comparing treatment modalities.
From the available evidence, if the objective of preoperative treatment were solely to improve R0 resection rate both CROSS and FLOT offer comparable outcomes, but other important outcomes that have a profound impact on overall survival need to be considered.
Lymph node status, primary tumour pathological response and survival
Systemic disease control in patients with node-positive or micrometastatic disease is important for improving long-term outcomes in patients with oesophageal cancer [47,48,49,50,51,52,53,54,55]. A recent meta-analysis has highlighted the importance of lymph node downstaging after neoadjuvant therapy as a prognostic factor in oesophageal cancer, with those with ypN0 achieving a much-improved survival over those with positive nodes (ypN+) after neoadjuvant therapy [56]. The POET study demonstrated a significantly improved 3-year survival for patients with an R0 resection and ypN0 (64.2%) compared with those who had tumour in the resected lymph nodes (38.8%), P < 0.001 [43]. Other studies have demonstrated the benefit of ypN0 as a prognostic factor in surgery for oesophageal cancer [57], with one study showing response in the lymph nodes and primary tumour to independently improve disease-free survival [58]. Two studies have suggested that adequate lymph node response improves survival, even if there is little response in the primary tumour [59, 60]. Furthermore, lymph node status was the largest determinant of prognosis in a recent machine-learning model predicting long-term survival [61]. Although there is a survival benefit for ypN0 over those with positive lymph nodes in the resected specimen (ypN+), the greatest benefit is seen in those with natural N0 or in those in whom there is concomitant complete regression in the primary tumour (ypT0)[62]. This highlights the importance of adequate pathological response in both the primary tumour and the lymph nodes. Moreover, primary tumour pathological complete response (pCR) has demonstrated 5-year overall survival of 88% vs 39% in those with complete resection (R0) but residual tumour in the resected specimen [63]. In a separate study, pCR was demonstrated as an independent predictor of improved survival following neoadjuvant chemoradiotherapy [64]. However, the Neo-AEGIS study, which compared neoadjuvant chemoradiotherapy to mostly older ECX perioperative chemotherapy, demonstrated higher rates of pCR (16% vs 5%) and ypN0 (60.1% vs 44.5%) after nCRT compared to nCT but this did not translate into improved survival [41]. If the objective of preoperative treatment were solely to improve pCR in the primary tumour and lymph nodes, neoadjuvant chemoradiotherapy would be the clear treatment of choice. However, it is important to consider how this impacts disease-free and overall survival.
Adjuvant therapy
The evidence for adjuvant therapy alone is extremely limited in gastroesophageal adenocarcinoma and is restricted to trials in gastric and gastroesophageal junction adenocarcinoma [65, 66]. In oesophageal adenocarcinoma, specific benefit of adjuvant therapy has only been demonstrated within the context of perioperative chemotherapy. In a large retrospective analysis, patients who received adjuvant chemotherapy had improved median survival over those who did not receive adjuvant chemotherapy (62.7 months vs 50.4 months) [67]. Moreover, the benefit of completing all cycles of FLOT has been shown to improve overall survival, regardless of tumour regression [68]. Adjuvant chemotherapy is also associated with improved median overall survival (40 months vs 34 months) in patients who had preoperative chemoradiotherapy [69]. Other studies suggest that the benefit of adjuvant chemotherapy in this setting is greatest in node-positive disease [70, 71]. Indeed, in their subgroup analysis in patients receiving perioperative chemotherapy Rahman et al. [67] found that patients who had ypN0 had excellent survival outcomes, with no additional benefit from adjuvant chemotherapy whereas those with ypN+ had superior survival if they received adjuvant chemotherapy. The relative benefit of neoadjuvant over adjuvant therapy alone has been shown in patients with gastric cancer in the PRODIGY trial with increased 3-year PFS in those receiving nCT (66.3%) compared to adjuvant CT alone (60.2%) [72]. Retrospective studies also show survival benefit in those with gastro-oesophageal junction adenocarcinoma receiving nCRT over adjuvant CRT [73].
Adjuvant therapy following preoperative oncological therapy can improve survival outcomes for patients with oesophageal adenocarcinoma, particularly those with residual nodal disease and is part of the current standard of care. However, there are challenges in delivering adjuvant chemotherapy in patients who have undergone oesophagogastrectomy and there is some evidence to suggest a relative benefit of neoadjuvant therapy over adjuvant.
Current standard of care and its challenges
Although accepted as a standard of care, the perioperative approach of neoadjuvant chemotherapy followed by surgery and adjuvant chemotherapy thereafter is often hampered by failure to complete all chemotherapy cycles. In the FLOT4 trial, only 46% of patients completed all cycles using the perioperative approach [4]. Whereas, in regimens where all treatment is delivered pre-operatively there is a much higher rate of treatment completion without reducing the number of patients proceeding to surgery. An example is the CROSS trial, in which 95% of patients completed oncological treatment and 90% of patients underwent resection, albeit that the amount of chemotherapy delivered in this regimen is much less than in FLOT. However, in the FLOT4 trial, 90% of patients completed all preoperative chemotherapy, suggesting that preoperative treatment is better tolerated than postoperative treatment, in part due to the morbidity following oesophagogastrectomy. Timing of surgery after neoadjuvant therapy is also an important consideration. Patients undergoing nCRT have improved response after delayed surgery (>7–8 weeks after nCRT completion) but have higher 30-day mortality after surgery [74]. A large study of >2000 patients suggests that the optimal timing for surgery is 56 days after nCRT completion to balance increased pathological response with overall survival [75].
Both the perioperative FLOT chemotherapy regimen and the preoperative CROSS chemoradiotherapy regimen plus surgery are accepted standards of care for patients with resectable oesophageal adenocarcinoma and are currently being compared in the ESOPEC trial [44]. Although there is currently no directly comparable clinical evidence to suggest that either is superior to the other, CROSS (nCRT) and FLOT (perioperative chemotherapy) have different effects on the primary tumour and systemic disease. There is a higher rate of pCR with CROSS than preoperative chemotherapy. Due to its radiotherapy component, CROSS gives the opportunity to downstage primary tumours where there is a risk of R1 resection. However, CROSS delivers less systemic treatment than FLOT. As a result, there is a risk of systemic undertreatment in patients allocated to nCRT using CROSS. This has been demonstrated in a recent large cohort study of patients with oesophageal adenocarcinoma all achieving pCR (ypT0N0) after neoadjuvant therapy, which showed that 5-year recurrence-free survival was significantly better in the nCT group (87.1%) compared to nCRT (75.3%), notably with a greater prevalence of distant recurrence in the nCRT group, suggesting potential systemic undertreatment [55]. This has also been demonstrated in 10-year CROSS follow-up, in which CROSS reduced oesophageal cancer-related death by reducing locoregional recurrence but did not reduce the incidence of distant recurrence compared to surgery alone [76].
Regarding pCR in the primary tumour and lymph nodes (ypT0N0), it is important to consider how this translates to into long-term outcomes and the differential outcomes observed after different neoadjuvant regimens. It is evident that whilst achieving ypT0N0 is important, the modality used to achieve this is also important for survival outcomes. Although there were higher rates of ypT0 and ypN0 in those receiving nCRT compared to nCT (using older ECX chemotherapy rather than FLOT) in the NEO-AEGIS study, this did not translate into improved 3-year overall survival (56% vs 57%) [41]. There were similar results in NeoRes I, with higher pCR for nCRT than nCT (28% vs 9%) but similar 5-year OS (42.2% vs 39.6%) [42]. A recent retrospective study directly comparing FLOT vs CROSS shows similar 5-year overall survival in patients receiving FLOT and CROSS despite a higher pCR with CROSS [77]. Other recent smaller studies demonstrate similar survival patterns between CROSS and FLOT but show higher distant recurrence and postoperative respiratory failure with CROSS [78, 79]. Results from the ESOPEC Phase III trial are eagerly awaited [44]. A 2019 meta-analysis makes the conclusion that although the addition of radiotherapy to chemotherapy alone increases the chance of pCR and reduces the risk of locoregional failure, it does not reduce the risk of distant metastases or death [80].
These clinical observations support tumour biology relating to intra-patient heterogeneity. One study has shown discrepancy in genomic alterations between primary tumour and metastatic disease and highlights the limitations of using genetic alterations in biopsies of the primary tumour to guide treatment in other areas of the patient’s disease such as distant metastases [81]. Furthermore, intratumoural heterogeneity exists between tissue from superficial primary tumour, deep primary tumour, and lymph node metastases [82].
The main challenges for the current standards of care are non-completion of perioperative therapy in the context of FLOT, as well as a risk of systemic undertreatment in those receiving CROSS. Whilst pCR is seen as a marker of treatment success, studies comparing patients achieving pCR who received nCT or nCRT lead us to conclude that ypT0N0 does not always translate into the same outcomes in primary endpoints such as disease-free or overall survival between treatment modalities and should not be used as a surrogate primary endpoint. Future comparative randomised trials should focus not only on pCR but also on survival outcomes. By combining both modalities in the preoperative setting using a total neoadjuvant approach, for example using extended preoperative FLOT or a combination of preoperative FLOT plus CROSS, we may be able to achieve both optimal locoregional and systemic disease control, without compromising progression to surgery, enabling more patients to complete all intended treatment.
The role of immune checkpoint inhibitors
Immune checkpoint inhibitors remove the inhibitory signals of T-cell activation that enable tumour-reactive T cells to overcome regulatory mechanisms and mount an effective antitumour response [83]. Although their mechanism of action is different, there are synergies between chemotherapy and immunotherapy and it has been suggested that an effective strategy to harness such synergies is to give immune checkpoint inhibitors after the tumour mass has been optimally reduced with surgery and systemic chemotherapy in the setting of minimal residual disease, where the negative impact of tumour bulk on antitumour immune response is minimised [84]. In the context of TNT, this could theoretically enable best possible response to local and systemic therapy whilst engaging the immune response in the postoperative setting. The positive impact of postoperative checkpoint inhibitors has been demonstrated in the nCRT setting in the CHECKMATE 577 trial, in which patients with residual disease after surgery (ypT+ or ypN+) were randomised to receive adjuvant PD-1 inhibitor, nivolumab, or placebo [85]. Median disease-free survival was 22.4 months in the treatment vs 11 months in the placebo arm (HR 0.69, P < 0.001). These results have changed the paradigm of treatment for oesophageal cancer, giving us a fourth treatment modality in addition to chemotherapy, radiotherapy, and surgery to improve outcomes for patients with locally advanced, high-risk oesophageal cancer. It must be noted that quality of life scores were comparable between the placebo and treatment groups with an acceptable safety profile, which is important when considering patients who might have already received TNT and surgical resection for further treatment [86]. However, recent trial results have failed to show a benefit for the addition of immune checkpoint inhibitors to neoadjuvant and adjuvant chemotherapy. Final results are awaited but KEYNOTE-585 reports a higher pathological complete response rate from the addition of pembrolizumab to perioperative FLOT, but the event-free and overall survival endpoints were not met [87]. Similarly, ATTRACTION-5 reported no recurrence-free survival benefit from the addition of Nivolumab to adjuvant chemotherapy [88]. In both KEYNOTE-585 and ATTRACTION-5 the use of immune checkpoint inhibitors was in biomarker unselected patients, and it is relevant that in CHECKMATE577 a post hoc subgroup analysis indicated that disease-free survival benefit from adjuvant nivolumab was only demonstrated in PDL1 combined positive score (CPS) ≥5 patients and not seen in PDL1 CPS ≤5. In metastatic or advanced-stage unresectable gastroesophageal cancer patients a number of randomised trials have reported the benefit of the addition of immune checkpoint inhibitor to chemotherapy and tumour PDL1 CPS has demonstrated benefit as a biomarker to predict the quantum of benefit from the checkpoint inhibitor. In CHECKMATE 649, patients with metastatic, or unresectable oesophageal, junctional or gastric adenocarcinomas who were not known to be HER2 positive were enrolled regardless of PDL1 CPS result, but the co-primary endpoints were PFS and OS in patients with PDL1 CPS ≥5 where benefit was seen with the addition of nivolumab to oxaliplatin plus capecitabine or 5-FU (OS HR = 0.70 (95% CI 0.61, 0.81), PFS HR = 0.70 (95% CI 0.60, 0.81)) [89]. Similarly in KEYNOTE 859, in metastatic or advanced-stage unresectable gastroesophageal junctional or gastric adenocarcinomas OS and PFS benefit from the addition of pembrolizumab to platinum fluoropyrimidine chemotherapy was demonstrated recently in patients with PDL1 CPS ≥1 with a greater incremental benefit seen in those with PDL1 CPS ≥10 [90]. While KEYNOTE 590 demonstrated benefit of the addition of pembrolizumab to platinum fluoropyrimidine chemotherapy to all randomised patients with oesophageal cancer (squamous and adenocarcinoma) and Siewert type I junctional adenocarcinomas, but greater incremental benefit in those with PDL1 CPS ≥10 [91]. These trials demonstrating the survival benefit of checkpoint inhibitors in unresectable and metastatic gastro-oesophageal malignancy have established new standards of care in biomarker-selected patients with advanced-stage disease and underscore the importance of biomarker-directed use of immune checkpoint inhibitors. Together with the recent results from KEYNOTE-585 and ATTRACTION-5, and post hoc PDL1 CPS analysis from CHECKMATE 577 this suggests that biomarker section for immune checkpoint inhibitors is likely to be important in the neoadjuvant and adjuvant setting as well. This has important relevance for ongoing trials of immune checkpoint inhibitors in the curative setting, including those which incorporate perioperative FLOT such as MATERHORN (FLOT + durvalumab or placebo) (NCT04592913). Microsatellite instability-high (MSI-H) is present in 6–24% of resected gastroesophageal adenocarcinoma and is an established predictive biomarker for immune checkpoint inhibitors [92]. Encouraging results have been reported in non-randomised Phase 2 trials of perioperative immune checkpoint inhibitors without chemotherapy in MSI-H selected patients, for example, the NEONIPIGA trial has shown pCR rates of 59% in patients with MSI-high disease, but survival follow-up is limited at present and larger randomised studies are yet to be undertaken [93].
Overall, the role of immune checkpoint inhibitors in perioperative treatment of gastroesophageal adenocarcinomas is not yet established and emerging trial results highlight the importance of biomarker-directed use of these agents. This emphasises the importance of optimising the conventional perioperative treatments with chemotherapy and chemoradiotherapy for those patients who are immune checkpoint inhibitor biomarker negative and the incorporation of treatment with checkpoint inhibitors in a biomarker-directed manner into trials of TNT where patients have residual disease despite optimal local and systematic therapy.
Conclusion
In Summary, the addition of perioperative oncological therapies to surgery have greatly improved overall and progression-free survival in patients with oesophageal and junctional adenocarcinoma, achieving higher R0 resection rates and pathological response in the primary tumour and involved lymph nodes. However, more than 50% of patients do not complete all planned therapy if receiving perioperative chemotherapy. Furthermore, whilst pCR is important, intra-tumour heterogeneity impacts how this translates into long-term disease-free survival, and the impact of FLOT and CROSS on survival does not appear to be directly related to pCR alone. Total neoadjuvant therapy has shown promising results with high pCR rates together with impressive disease-free and overall survival in the retrospective setting. This warrants a randomised controlled trial of total neoadjuvant therapy approaches, incorporating methods of treatment response.
BACKGROUND: IMvigor130 demonstrated statistically significant investigator-assessed progression-free survival benefit with first-line atezolizumab plus platinum-based chemotherapy (group A) versus placebo plus platinum-based chemotherapy (group C) in patients with locally advanced or metastatic urothelial carcinoma. Overall survival was not improved in interim analyses. Here we report the final overall analysis for group A versus group C.
METHODS: In this global, partially blinded, randomised, controlled, phase 3 study, patients (aged =18 years) with previously untreated locally advanced or metastatic urothelial cancer and who had an Eastern Cooperative Oncology Group performance status of 0-2 were enrolled at 221 hospitals and oncology centres in 35 countries. Patients were randomly assigned (1:1:1), with a permuted block method (block size of six) and an interactive voice and web response system, stratified by PD-L1 status, Bajorin risk factor score, and investigator’s choice of platinum-based chemotherapy, to receive atezolizumab plus platinum-based chemotherapy (group A), atezolizumab monotherapy (group B), or placebo plus platinum-based chemotherapy (group C). Sponsors, investigators, and patients were masked to assignment to atezolizumab or placebo (ie, group A and group C) and atezolizumab monotherapy (group B) was open label. For groups A and C, all patients received gemcitabine (1000 mg/m2 intravenously; day 1 and day 8 of each 21-day cycle), plus investigator’s choice of carboplatin (area under curve 4·5 mg/mL per min or 5 mg/mL per min; intravenously) or cisplatin (70 mg/m2 intravenously), plus either atezolizumab (1200 mg intravenously) or placebo on day 1 of each cycle. Co-primary endpoints of the study were investigator-assessed progression-free survival and overall survival for group A versus group C in the intention-to-treat (ITT) population (ie, all randomised patients), and overall survival for group B versus group C, tested hierarchically. Final overall survival and updated safety outcomes (safety population; all patients who received any amount of any study treatment component) for group A versus group C are reported here. The final prespecified boundary for significance of the overall survival analysis was one-sided p=0·021. The trial is registered with ClinicalTrials.gov, NCT02807636, and is active but no longer recruiting.
FINDINGS: Between July 15, 2016, and July 20, 2018, 1213 patients were enrolled and randomly assigned to treatment, of whom 851 were assigned to group A (n=451) and group C (n=400). 338 (75%) patients in group A and 298 (75%) in group C were male, 113 (25%) in group A and 102 (25%) in group C were female, and 346 (77%) in group A and 304 (76%) in group C were White. At data cutoff (Aug 31, 2022), after a median follow up of 13·4 months (IQR 6·2-30·8), median overall survival was 16·1 months (95% CI 14·2-18·8; 336 deaths) in group A versus 13·4 months (12·0-15·3; 310 deaths) in group C (stratified hazard ratio 0·85 [95% CI 0·73-1·00]; one-sided p=0·023). The most common grade 3-4 treatment-related adverse events were anaemia (168 [37%] of 454 patients who received atezolizumab plus chemotherapy vs 133 [34%] of 389 who received placebo plus chemotherapy), neutropenia (167 [37%] vs 115 [30%]), decreased neutrophil count (98 [22%] vs 95 [24%]), thrombocytopenia (95 [21%] vs 70 [18%]), and decreased platelet count (92 [20%] vs 92 [24%]). Serious adverse events occurred in 243 (54%) patients who received atezolizumab plus chemotherapy and 196 (50%) patients who received placebo plus chemotherapy. Treatment-related deaths occurred in nine (2%; acute kidney injury, dyspnoea, hepatic failure, hepatitis, neutropenia, pneumonitis, respiratory failure, sepsis, and thrombocytopenia [n=1 each]) patients who received atezolizumab plus chemotherapy and four (1%; unexplained death, diarrhoea, febrile neutropenia, and toxic hepatitis [n=1 each]) who received placebo plus chemotherapy.
INTERPRETATION: Progression-free survival benefit with first-line combination of atezolizumab plus platinum-based chemotherapy did not translate into a significant improvement in overall survival in the ITT population of IMvigor130. Further research is needed to understand which patients might benefit from first-line combination treatment. No new safety signals were observed.
Precision radiotherapy refers to the ability to deliver radiation doses with sub-millimetre accuracy. It does not however consider individual variation in tumour or normal tissue response, failing to maximise tumour control and minimise toxicity. Combining precise delivery with personalised dosing, through analysis of cell-free DNA, would redefine precision in radiotherapy.
Introduction
Around 50% of cancer patients require radiotherapy at some point in their treatment. The probability of treatment success is dependent upon the dose delivered and the relative radio-sensitivity of the tumour. The maximum dose delivered is calculated to ensure that no more than 10% of patients suffer life-changing late radiotherapy toxicity with an additional 20% reporting toxicity that still has some impact on quality of life. The current “one dose fits all” approach to radiotherapy treatment contrasts with the ethos of precision oncology in other branches of cancer medicine, which increasingly harness the power of genetic and genomic analyses to stratify patient care, monitor tumour response and detect disease progression.
Liquid biopsy – the analysis of cell-free DNA (cfDNA) and other cellular components released from dying or damaged cells into the circulation or other bodily fluids – has utility because the cellular components carry the characteristics of the tissues from which they are derived. Circulating tumour-derived DNA (ctDNA) retains the genetic and epigenetic hallmarks of the originating tumour, including somatic mutation and DNA methylation. Attractive because it is minimally invasive and repeatable, liquid biopsy is gaining traction in early detection and diagnosis, patient stratification, detection of minimal residual disease and prediction of recurrence after primary treatment [1,2,3,4,5].
Analysis of cfDNA has been little applied to management of radiotherapy, especially dosing or scheduling. However, the ability to quantify ctDNA and to define cfDNA tissue-of-origin in real time have the potential both to permit assessment of tumour response to radiation during a course of radiotherapy treatment and, at the same time, to measure the extent of damage to healthy tissues surrounding the targeted tumour. These advances, technically possible, would allow truly personalised adjustment to radiotherapy dose per fraction or number of fractions, based on how the patient is responding to their treatment and would transform how radiotherapy is currently delivered.
Here, we review recent data that define the mechanism and timing of cfDNA release arising from tissue damage and cell death after exposure to ionising radiation and the extent to which this can be quantified and ascribed to tissue-of-origin. Finally, we consider the work still required to validate and clinically translate these observations to new precision in radiation therapy.
cfDNA release after exposure to ionising radiation
Cellular DNA is released into the circulation primarily from dividing, damaged or dying cells undergoing apoptosis or necrosis. In radiotherapy, ionising radiation causes direct and indirect DNA damage predominantly through single and double strand breaks [6]. If this damage cannot be corrected by cellular DNA repair mechanisms, cell death will occur by an interplay of apoptosis, necrosis, or mitotic catastrophe [7].
In one of the first studies investigating the kinetics of ctDNA release during radiotherapy, Lo et al. quantified Epstein-Barr virus (EBV) ctDNA in patients undergoing radiotherapy for nasopharyngeal cancer. Having observed that 2 out of 10 patients had a transient rise in circulating EBV DNA one week after initiation of radiotherapy, a further 5 patients were recruited, in whom EBV DNA levels were measured daily during the first week. All 5 patients exhibited a transient rise in EBV DNA in the first week of radiotherapy, followed by a fall [8]. More recently, in pre-clinical studies, Rostami et al measured ctDNA release following chemical induction of apoptosis and exposure to radiation in tumour cell lines and tumour xenograft mouse models. While there was little immediate ctDNA release after irradiation, a subset of irradiated cell lines demonstrated a rise in ctDNA after 72–96 h. Supporting this timeline, three of five irradiated xenograft mouse models also showed a delayed increase in ctDNA release between 96 and 144 h after irradiation. These findings led them to propose a model of cell death and DNA release whereby, in certain cell types, mitotic catastrophe predominates in the early response to irradiation exposure, with a peak in apoptosis and cfDNA release later at around 3–6 days following irradiation [7]. Similarly, Muhanna et al, studying a model of buccal cancer in rabbits, found an initial rise in ctDNA in the 1–3 days following initiation of radiation therapy followed by a consistent fall [9].
These studies suggest a pattern of release of ctDNA from tumour cells, in which damaged cells undergo a combination of immediate and delayed cell death, with an initial rise of ctDNA release into the circulation following exposure to radiation, and detectable ctDNA concentrations that subsequently fall as tumour bulk decreases.
Detection, characterisation and analysis of cfDNA
ctDNA in cancer patients usually constitutes a small, frequently tiny proportion of the total circulating cfDNA. In early-stage cancer, ctDNA generally accounts for less than 1% of total cfDNA and only in late-stage cancer and in a subset of high-secreting tumours, does the proportion of ctDNA rise above 1% [10,11,12]. Methods of ctDNA detection must therefore be sensitive and specific to be clinically useful.
Tumour-derived somatic mutation in cfDNA can be detected by targeted or genome-wide sequencing and by multiplex and allele-specific PCR. A range of methods have been developed to maximise sensitivity and specificity including barcoding, amplification, error correction and deep sequencing [11,12,13]. Such methods are necessary because of the low total concentration of cfDNA in the circulation, the often low fraction of cfDNA that is tumour-derived and the molecular heterogeneity across cancer types and of individual tumours. These methods have already been successfully deployed across a range of clinical cancer studies for treatment stratification, assessment of minimal residual disease and detection of disease progression following primary treatment [1,2,3,4,5, 14,15,16,17]. In addition, because each tissue in the body, including tumour tissues, carries its own unique DNA methylation profile and these tissue-specific methylation profiles are retained after release of cellular DNA into the circulation, DNA methylation analysis is now recognised as a powerful tool for determining the tissue origin(s) of DNA samples including tumour-derived cfDNA [18,19,20].
In virus-associated cancers, detection of viral cfDNA by droplet digital PCR (ddPCR) or sequencing has been used to screen for virus-associated tumours in healthy populations and for characterisation of viral status at diagnosis. In longitudinally collected samples post-treatment, cfDNA viral titre has been successfully used as a prognostic marker and early marker of disease progression. Such approaches have shown particular value in EBV-associated nasopharyngeal cancer and human papillomavirus (HPV)-associated oropharyngeal cancers [21,22,23,24].
Personalising radiotherapy
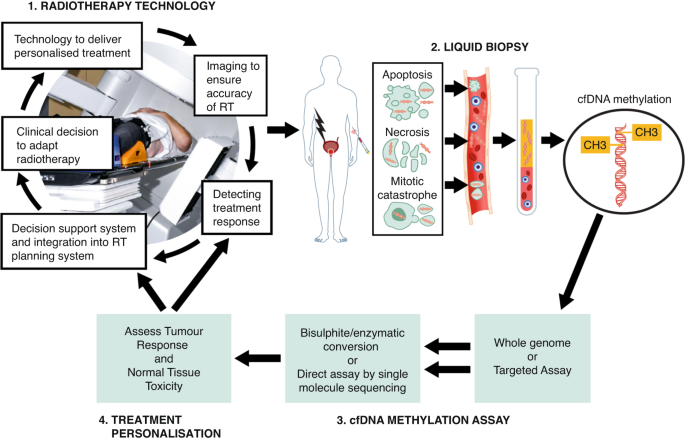
Advances in radiotherapy technology have improved the accuracy of radiation delivery to the tumour and clinical trials have refined dosing schedules with resultant improvements in outcomes, as reviewed elsewhere [6, 25, 26]. However, toxicity remains common, in part because of the absence of biomarkers of toxicity, such that once dosing has started, it continues till the end of the schedule unless severe acute symptomatic toxicity occurs. Further, despite known variation in inter-individual and tumour radiosensitivity, manifested at the germline and gene expression level [27,28,29], genetic methodologies have to date impacted little on cure rates or toxicity [26]. Recent advances in understanding the mechanisms and kinetics of ctDNA release from tumours and in the ability to define cfDNA tissue-of-origin suggest that liquid biopsy has the potential to change this (Fig. 1).
Fig. 1: Integration of liquid biopsy into a personalised, adaptive radiotherapy workflow.
In EBV-associated nasopharyngeal cancer, Lo et al. defined the kinetics of ctDNA release through measurement of EBV cfDNA [8], leading to the proposal of several groups that measurement of EBV viral load at the midpoint of radiotherapy treatment could be used as a basis for intensification or de-intensification of treatment, respectively, in those with an adverse or favourable cfDNA response [21, 23]. Similarly, Chera et al demonstrated that a favourable HPV clearance profile during chemoradiotherapy, defined as >95% clearance of circulating HPV cfDNA from a high HPV baseline copy number, was predictive of disease control in HPV-associated oropharyngeal cancer and could be the basis of trials to investigate de-intensification based on HPV clearance rate [22]. In non-virus associated cancers a number of recently published studies have demonstrated that the persistence of tumour-derived cfDNA following primary therapy, can predict those patients most likely to benefit from adjuvant therapy or subsequently relapse with early metastatic disease [4, 5, 30,31,32,33]. These results, some of which are primed for use in the clinic [3, 34], give optimism that the results in virus-associated cancers may also be applicable in non-virus associated cancers.
Of perhaps even greater novelty and applicability for radiotherapy would be the development of biomarkers of radiation-induced damage to tissues surrounding the targeted tumour. In the past five years, it has become clear that DNA methylation analysis has this capability. Extensive methylation atlases of healthy tissues and tumour types have been developed with the power to define the tissue composition of cfDNA samples and the ability to detect with high sensitivity the presence of DNA from a wide range of tissues and tumours, with demonstrated or potential application in the context of autoimmune disease, transplant rejection and early stage cancer [2, 18,19,20]. Showing promise for detecting damage to tissues surrounding the targeted tumour, methylation analysis has recently been reported to detect liver-derived cfDNA in patients undergoing radiotherapy treatment for right-sided but not left-sided breast cancer [35].
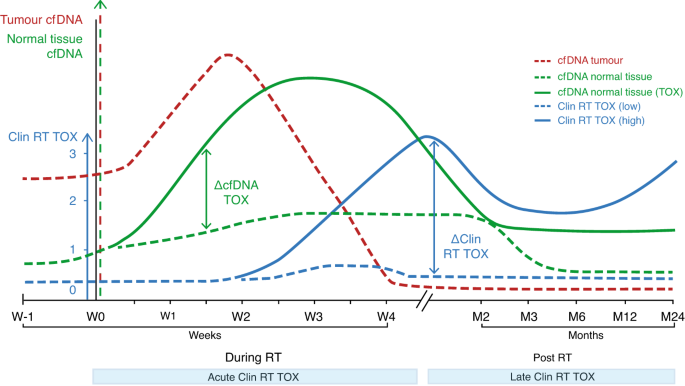
These proof-of-concept studies offer the prospect of direct tests both for tumour cell death and off-target tissue damage during radiotherapy treatments, as has also been noted in other recent reviews [10, 36]. Such tests could serve as biomarkers for adaptive radiotherapy regimes that guide treatment intensification or de-intensification based on the kinetics of clearance of circulating ctDNA and the presence or absence of cfDNA from healthy tissues surrounding the targeted tumour. However, the variable kinetics of cfDNA release in different cancer types and the currently incomplete knowledge of how different clinical radiotherapy fractionation protocols may impact on cfDNA release indicate that further study will be required to define the optimum timing of cfDNA assessment to impact effectively on radiotherapy outcomes (Fig. 2).
Fig. 2: Dynamics of cfDNA release in radiotherapy.
Validation and clinical translation
While evidence for the value of ctDNA analysis following primary treatment with surgery, chemotherapy and radiotherapy is accumulating rapidly, the use of cfDNA analysis to guide radiotherapy dosing and scheduling during treatment is at an early stage. The existing proof-of-concept studies need confirmation in further clinical studies for example on the kinetics of cfDNA release in different tumour types and with different radiotherapy protocols. Technical advances are also required, such as development of protocols to measure DNA methylation directly in real-time, as may now be achievable by single molecule sequencing [37,38,39]. However, given the data from pre-clinical models and virally-induced cancers which indicate that radiation damage to tissues leads to release of detectable cell-free DNA into the surrounding milieu, it is plausible that current liquid biopsy methods may be sufficiently sensitive to provide clinically useful biomarkers of real-time tumour response and damage to healthy tissues in radiotherapy management. The confirmation of these data, being sought in several labs worldwide, would allow intra-treatment analysis of cfDNA for personalised adaptative radiotherapy scheduling, enabling more effective tumour cell death while minimising healthy tissue toxicity. Such an advance would be transformative for precision management of radiation treatments for cancer.
the American Head and Neck Society Salivary Gland Section presented a multinational study of the clinical behavior of low and intermediate salivary tumors.1 In this large study, including 865 patients from 41 institutions in 5 different countries, the authors show that we could expect excellent outcomes after surgical treatment of these tumors. The cohort, overall, has a 5-year survival of 94%. Local, regional, and distant failures were all observed rarely. The estimate of any recurrence at 3 years was 6%. These are encouraging findings. These findings are even more significant, considering that 22% of patients had a positive margin after surgery and only 35% received adjuvant radiotherapy. Surgical extirpation results in long-term survival. Furthermore, this investigation focuses on elucidating the benefit and role of adjuvant radiotherapy in these tumors. When should we consider recommending adjuvant radiotherapy after tumor extirpation? Based on these findings, not very often. Radiotherapy was associated with improved outcomes in patients with positive margins, where the likelihood of local failure was diminished from 20% to 2%. However, when we analyze tumor extirpations with margins less than 1 mm, the addition of adjuvant radiotherapy was not associated with improved outcomes.
Question Can the combination of central nervous system (CNS) radiotherapy with pyrotinib and capecitabine improve CNS progression-free survival (PFS) in patients with ERBB2-positive breast cancer with brain metastases?
Findings In this phase 2 nonrandomized trial of 40 patients with ERBB2-positive breast cancer, the combination of CNS radiotherapy and pyrotinib plus capecitabine was associated with a 1-year CNS PFS rate of 74.9% and a median CNS PFS of 18.0 months, with an acceptable radiation necrosis rate.
Meaning The results of this trial suggest that there are potential benefits of combining radiotherapy with pyrotinib and capecitabine for patients with ERBB2-positive breast cancer with brain metastases, suggesting a promising novel treatment approach for this challenging clinical scenario.
Abstract
Importance The potential benefit of combining intracranial effective systemic therapy with radiotherapy for patients with breast cancer with brain metastases remains unclear.
Objective To assess the activity and safety of combining radiotherapy with pyrotinib and capecitabine in patients with ERBB2-positive breast cancer and brain metastases.
Design, Setting, and Participants This was a single-arm, single-center, phase 2 nonrandomized clinical trial with a safety run-in phase. Between January 2020 and August 2022, patients with ERBB2-positive breast cancer and brain metastases were enrolled. The data cutoff date was February 1, 2023.
Interventions Patients received either fractionated stereotactic radiotherapy or whole-brain radiotherapy. Treatment with pyrotinib (400 mg, once daily) and capecitabine (1000 mg/m2, twice daily, on days 1-14 of each 21-day cycle) was initiated from the first day of radiotherapy to the seventh day after the completion of radiotherapy and continued until disease progression or unacceptable toxic effects.
Main Outcomes and Measures The primary end point was 1-year central nervous system (CNS) progression-free survival (PFS) rate. Secondary end points included CNS objective response rate (ORR), PFS, overall survival (OS), safety, and changes in neurocognitive function.
Results A total of 40 female patients (median age, 50.5 years [IQR, 46-59 years]) were enrolled and received treatment, including 3 patients in safety run-in phase. With a median follow-up of 17.3 months (IQR, 10.3-26.9), the 1-year CNS PFS rate was 74.9% (95% CI, 61.9%-90.7%), and the median CNS PFS was 18.0 months (95% CI, 15.5 to not reached). The 1-year PFS rate was 66.9% (95% CI, 53.1%-84.2%), and the median PFS was 17.6 months (95% CI, 12.8-34.1). The CNS objective response rate was 85% (34 of 40). Median overall survival was not reached. The most common grade 3 or 4 treatment-related adverse event was diarrhea (7.5%). Asymptomatic radiation necrosis was identified in 4 of 67 lesions (6.0%) treated with fractionated stereotactic radiotherapy. Most patients maintained neurocognitive function, as evaluated by the Mini-Mental State Examination at different points.
Conclusions and Relevance The results of this trial suggest that radiotherapy combined with pyrotinib and capecitabine is associated with long intracranial survival benefit in patients with ERBB2-positive advanced breast cancer and brain metastases with an acceptable safety profile. This combination deserves further validation.