Abstract
Objective
To study the association between maternal exposure to arsenic, cadmium, lead, manganese and mercury, time-to-pregnancy (TTP) and infertility.
Design
Pregnancy-based retrospective TTP cohort study.
Setting
Hospitals and clinics from ten cities across Canada.
Population
A total of 1784 pregnant women.
Methods
Concentrations of arsenic, cadmium, lead, manganese and mercury were measured in maternal whole blood during the first trimester of pregnancy as a proxy of preconception exposure. Discrete-time Cox proportional hazards models generated fecundability odds ratios (FOR) for the association between metals and TTP. Logistic regression generated odds ratios (OR) for the association between metals and infertility. Models were adjusted for maternal age, pre-pregnancy body mass index, education, income, recruitment site and plasma lipids.
Main Outcome Measures
TTP was self-reported as the number of months of unprotected intercourse to become pregnant. Infertility was defined as TTP longer than 12 months.
Results
A total of 1784 women were eligible for the analysis. Mean ± SD maternal age and gestational age at interview were 32.2 ± 5.0 years, and 11.6 ± 1.6 weeks, respectively. Exposure to arsenic, cadmium, manganese or mercury was not associated with TTP or infertility. Increments of one standard deviation of lead concentrations resulted in a shorter TTP (adjusted FOR 1.09, 95% CI 1.02–1.16); however, the association was not linear when exposure was modelled in tertiles.
Conclusion
Blood concentrations of metals at typical levels of exposure among Canadian pregnant women were not associated with TTP or infertility. Further studies are needed to assess the role of lead, if any, on TTP.
1 INTRODUCTION
Environmental exposure to metals is a public health concern given their wide dispersion in the environment and potential endocrine disruptive properties.1–3 An endocrine endpoint of interest in reproductive and environmental epidemiology is human fecundity given the increased rates of gynaecological conditions associated with impaired fecundity and possible association with exposure to endocrine-disrupting chemicals.4–7 There is evidence linking metals like arsenic, cadmium, lead and mercury to impaired ovarian function through oxidative stress.1, 2 In contrast, other metals like manganese, an essential trace element, may prevent oocyte damage through antioxidant properties.8–10
Although several environmental chemicals have been associated with decreased fecundability or a longer time-to-pregnancy (TTP),11–15 the impact of metals on TTP and infertility needs further investigation. The effect of lead is of particular interest, given its high toxicity at high levels of exposure in almost every organ. At current environmental levels of exposure, the most notable and strongest association observed with lead exposure is its detrimental effect on children’s neurological function.16, 17 The existing body of research exploring the relationship between female fecundity and lead exposure is limited, and the findings are inconclusive.18–21 Further investigation is warranted to provide a clearer understanding of a potential association.
Two previous cohort studies have investigated the effect of metals on TTP. The New York Angler Cohort, a prospective cohort study including 80 women, reported that higher pre-pregnancy levels of magnesium were associated with a shorter TTP and zinc exposure was associated with a longer TTP, but there was no association for arsenic, cadmium or lead.20 The Longitudinal Investigation of Fertility and the Environment (LIFE) study assessed the effects of environmental chemicals and human fecundity among 501 couples in Michigan and Texas.21 Male lead and female cadmium concentrations were associated with reduced fecundability. When jointly modelling couples’ exposures, only male lead concentration significantly reduced fecundability.21 The few studies that have assessed the impact of environmental metals exposure on infertility (i.e. inability to conceive after 12 months of unprotected intercourse) have reported associations with infertility at increased levels of cadmium or lead.22–24
This study aims to evaluate the association between selected metals (arsenic, cadmium, lead, manganese and mercury), TTP and infertility in participants from the Maternal–Infant Research on Environmental Chemicals (MIREC) study, a Canadian pregnancy and birth cohort.
RESULTS
A total of 1784 participants from the MIREC study met our eligibility criteria (Figure 1). The distribution of demographic and lifestyle characteristics of the study population and their association with TTP are presented in Table 1. Mean maternal age at interview was 32.2 ± 5.0 years and mean gestational age at the time of the blood sample was 11.6 ± 1.6 weeks (± SD). Participants in this study were mostly White, born in Canada, lifelong non cigarette smokers and had a normal pre-pregnancy BMI. Almost two-thirds had an undergraduate degree or higher, more than one-third reported a household income greater than Can$ 100 000, and over half had one previous pregnancy with a live birth.

TABLE 1. Characteristics of 1784 women from the MIREC study, 2008–2011, and association with time-to-pregnancy.
| n (%) | Time-to-pregnancy (months) | Crude FOR (95% CI) | ||
|---|---|---|---|---|
| Mean ± SD | Median (IQR) | |||
| Maternal age (years) | ||||
| ≤29 | 524 (29.4) | 3.8 ± 6.9 | 1 (1–4) | 1.00 |
| 30–34 | 650 (36.4) | 4.6 ± 7.4 | 2 (1–4) | 0.81 (0.70–0.94) |
| 35+ | 610 (34.2) | 7.0 ± 12.8 | 2 (1–6) | 0.62 (0.54–0.72) |
| Pre-pregnancy BMI (kg/m2) | ||||
| <24.9 | 1052 (59.0) | 4.8 ± 8.6 | 1 (1–4) | 1.00 |
| 25–29.9 | 362 (20.3) | 5.2 ± 10.7 | 1 (1–4) | 1.03 (0.89–1.21) |
| >30 | 245 (13.7) | 6.6 ± 11.1 | 1 (1–7) | 0.76 (0.64–0.91) |
| Missing | 125 (7.0) | 5.2 ± 10.6 | 1 (1–4) | 1.03 (0.82–1.31) |
| Education | ||||
| Some college or less | 281 (15.8) | 5.1 ± 9.8 | 1 (1–5) | 1.00 |
| College diploma | 378 (21.2) | 5.7 ± 10.2 | 2 (1–6) | 0.88 (0.73–1.08) |
| Undergraduate | 655 (36.7) | 5.5 ± 10.8 | 2 (1–5) | 0.96 (0.81–1.15) |
| Graduate (MSc, PhD) | 470 (26.3) | 4.4 ± 6.6 | 2 (1–4) | 1.02 (0.84–1.23) |
| Income (Can$) | ||||
| <Can$ 60 000 | 374 (21.0) | 4.0 ± 6.9 | 1 (1–4) | 1.00 |
| Can$ 60 001–Can $ 100 000 | 624 (35.0) | 5.4 ± 10.1 | 2 (1–5) | 0.81 (0.69–0.96) |
| >Can$ 100 000 | 702 (39.3) | 5.6 ± 10.2 | 2 (1–5) | 0.77 (0.66–0.91) |
| Missing | 84 (4.7) | 5.0 ± 10.7 | 2 (1–4) | 0.90 (0.66–1.22) |
| Country of birth | ||||
| Foreign | 336 (18.8) | 5.0 ± 8.0 | 2 (1–6) | 1.00 |
| Canada | 1448 (81.2) | 5.2 ± 9.9 | 2 (1–5) | 1.04 (0.90–1.21) |
| Race and ethnicity | ||||
| White | 1487 (83.4) | 5.1 ± 9.7 | 2 (1–5) | 1.00 |
| Not White | 297 (16.6) | 5.4 ± 8.9 | 2 (1–6) | 0.93 (0.79–1.08) |
| Maternal cigarette smoking | ||||
| Never | 1087 (60.9) | 5.1 ± 8.8 | 2 (1–5) | 1.00 |
| Former | 491 (27.5) | 5.3 ± 10.8 | 2 (1–4) | 1.06 (0.92–1.21) |
| Current | 206 (11.5) | 5.1 ± 10.2 | 2 (1–4) | 1.09 (0.90–1.32) |
| Parity | ||||
| Nulliparous | 850 (47.6) | 6.1 ± 11.3 | 2 (1–6) | 1.00 |
| Parous | 934 (52.4) | 4.4 ± 7.6 | 2 (1–4) | 1.19 (1.06–1.34) |
| Total plasma lipids (g/L) | ||||
| <5.60 | 537 (30.1) | 4.2 ± 7.8 | 2 (1–4) | 1.00 |
| 5.60–6.60 | 613 (34.4) | 5.0 ± 8.9 | 2 (1–5) | 0.86 (0.74–1.00) |
| >6.60 | 619 (34.7) | 6.2 ± 11.4 | 2 (1–6) | 0.75 (0.65–0.87) |
| Missing | 15 (0.8) | 6.5 ± 9.7 | 2 (1–6) | 0.62 (0.32–1.20) |
- Abbreviations: BMI, body mass index; CI, confidence interval; FOR, fecundity odds ratio; IQR, interquartile range; SD, standard deviation.
The cumulative conception rate was 44.8% at 1 month, 81.9% at 6 months and 90.8% at 12 months. Hence, the rate of infertility (TTP > 12 months) in this cohort was 9.2%. Maternal age, pre-pregnancy BMI, income, parity and total plasma lipids were associated with TTP (Table 1). Older women, with higher BMI, higher income or increased plasma lipids had decreased fecundability (longer TTP). Parous women had a shorter TTP. Education, country of birth, race and ethnicity, and cigarette smoking status were not associated with TTP (Table 1).
Most participants had detectable blood levels of all five metals (Table 2). Geometric means for arsenic, cadmium, lead, manganese and mercury were 0.73 μg/L, 0.21 μg/L, 0.62 μg/dL, 8.79 μg/L and 0.61 μg/L, respectively. TABLE 2. Whole blood concentrations of metals, MIREC study 2008–2011.
| LOD | n (%) < LOD | Median | Minimum | Maximum | GM (95% CI) | |
|---|---|---|---|---|---|---|
| Arsenic (μg/L) | 0.23 | 136 (7.62) | 0.83 | <LOD | 34.59 | 0.73 (0.71–0.76) |
| Cadmium (μg/L) | 0.04 | 47 (2.63) | 0.20 | <LOD | 5.5 | 0.21 (0.20–0.22) |
| Lead (μg/dL) | 0.10 | 0 (0) | 0.63 | 0.16 | 5.21 | 0.63 (0.61–0.64) |
| Manganese (μg/L) | 0.55 | 173 (9.70) | 8.79 | 2.03 | 29.12 | 8.80 (8.67–8.93) |
| Mercury (μg/L) | 0.12 | 153 (9.74) | 0.70 | <LOD | 10.03 | 0.61 (0.58–0.64) |
- Abbreviations: CI, confidence interval; GM, geometric mean; LOD, limit of detection.
In relation to TTP, increments of one SD increase in blood concentrations of arsenic, cadmium, manganese or mercury were not associated with TTP (Table 3). In the adjusted model, increments of one SD of lead concentrations resulted in a shorter TTP (adjusted FOR [aFOR] 1.09; 95% CI 1.02–1.16). When exposure was modelled as tertiles, no relationship was observed between arsenic, cadmium, manganese or mercury and TTP. For lead, relative to the first tertile, the second (aFOR 1.33; 95% CI 1.14–1.54) and third (aFOR 1.28; 95% CI 1.10–1.50) tertiles were associated with a shorter TTP (Table 3). TABLE 3. Fecundability odds ratios for the association between metals and time-to-pregnancy, MIREC study 2008–2011.
| Metals | Levels | n | Crude FOR (95% CI) | Adjusted FORa (95% CI) |
|---|---|---|---|---|
| Arsenic (μg/L) | log2As/SD | 1784 | 0.99 (0.94–1.05) | 1.02 (0.95–1.08) |
| <0.60 | 600 | 1.00 | 1.00 | |
| 0.60–1.05 | 596 | 0.93 (0.80–1.07) | 0.94 (0.81–1.10) | |
| >1.05 | 588 | 0.96 (0.83–1.11) | 0.99 (0.85–1.17) | |
| Cadmium (μg/L) | log2Cd/SD | 1784 | 1.02 (0.97–1.09) | 1.04 (0.97–1.12) |
| <0.15 | 568 | 1.00 | 1.00 | |
| 0.15–0.28 | 590 | 1.06 (0.92–1.23) | 1.10 (0.94–1.27) | |
| >0.28 | 626 | 1.06 (0.91–1.22) | 1.07 (0.91–1.26) | |
| Lead (μg/dL) | log2Pb/SD | 1784 | 1.06 (1.00–1.13) | 1.09 (1.02–1.16) |
| <0.50 | 575 | 1.00 | 1.00 | |
| 0.50–0.77 | 578 | 1.27 (1.10–1.48) | 1.33 (1.14–1.54) | |
| >0.77 | 631 | 1.24 (1.04–1.43) | 1.28 (1.10–1.50) | |
| Manganese (μg/L) | log2Mn/SD | 1784 | 1.02 (0.96–1.08) | 1.04 (0.98–1.10) |
| <7.69 | 640 | 1.00 | 1.00 | |
| 7.69–10.44 | 576 | 1.10 (0.96–1.28) | 1.12 (0.96–1.29) | |
| >10.44 | 568 | 1.11 (0.96–1.28) | 1.17 (1.01–1.35) | |
| Mercury (μg/L) | log2Hg/SD | 1784 | 0.94 (0.89–1.00) | 0.98 (0.92–1.05) |
| <0.42 | 594 | 1.00 | 1.00 | |
| 0.42–1.04 | 586 | 0.87 (0.75–1.00) | 0.92 (0.79–1.07) | |
| >1.04 | 604 | 0.87 (0.75–1.01) | 0.95 (0.81–1.11) |
- Note: FOR derived from Cox proportional hazards model modified for discrete time data with multiple imputation (m = 20) for missing covariate information.
- Abbreviations: CI, confidence interval; FOR, fecundity odds ratio.
- a Adjusted for maternal age, pre-pregnancy body mass index, education, income, country of birth, race and ethnicity, maternal cigarette smoking, plasma lipids and recruitment site.
In relation to infertility (TTP > 12 months), increments of one SD increase of blood concentrations of arsenic, cadmium, lead, manganese or mercury were not associated with infertility (Table 4). When modelled as tertiles, exposures to arsenic, cadmium or mercury were not associated with infertility. For lead, relative to the first tertile, the second tertile was associated with decreased odds of infertility (aOR 0.57; 95% CI 0.37–0.87), but not the third tertile (Table 4). For manganese, relative to the first tertile, no association was observed with the second tertile, but the third tertile was associated with decreased odds of infertility (aOR 0.64; 95% CI 0.42–0.96) (Table 4). TABLE 4. Odds ratios for the association between blood metals and infertility, MIREC study 2008–2011.
| Metals | Levels | n | Crude OR (95% CI) | Adjusted ORa (95% CI) |
|---|---|---|---|---|
| Arsenic, μg/L | log2As/SD | 1784 | 1.14 (0.96–1.34) | 1.13 (0.95–1.35) |
| <0.60 | 600 | 1.00 | 1.00 | |
| 0.60–1.05 | 596 | 1.32 (0.88–1.98) | 1.32 (0.86–2.00) | |
| >1.05 | 588 | 1.29 (0.86–1.94) | 1.27 (0.82–1.97) | |
| Cadmium, μg/L | log2Cd/SD | 1784 | 0.99 (0.84–1.17) | 0.95 (0.77–1.17) |
| <0.15 | 568 | 1.00 | 1.00 | |
| 0.15–0.28 | 590 | 0.98 (0.66–1.46) | 0.89 (0.56–1.35) | |
| >0.28 | 626 | 0.99 (0.67–1.47) | 0.94 (0.60–1.47) | |
| Lead, μg/dL | log2Pb/SD | 1784 | 0.91 (0.77–1.07) | 0.87 (0.73–1.04) |
| <0.50 | 575 | 1.00 | 1.00 | |
| 0.50–0.77 | 578 | 0.61 (0.40–0.92) | 0.57 (0.37–0.87) | |
| >0.77 | 631 | 0.79 (0.54–1.16) | 0.73 (0.48–1.10) | |
| Manganese, μg/L | log2Mn/SD | 1784 | 0.91 (0.78–1.07) | 0.86 (0.72–1.02) |
| <7.69 | 640 | 1.00 | 1.00 | |
| 7.69–10.44 | 576 | 0.75 (0.51–1.11) | 0.74 (0.50–1.10) | |
| >10.44 | 568 | 0.71 (0.48–1.06) | 0.64 (0.42–0.96) | |
| Mercury, μg/L | log2Hg/SD | 1784 | 1.20 (1.01–1.42) | 1.09 (0.90–1.33) |
| <0.42 | 594 | 1.00 | 1.00 | |
| 0.42–1.04 | 586 | 1.41 (0.93–2.13) | 1.20 (0.78–1.85) | |
| >1.04 | 604 | 1.44 (0.96–2.16) | 1.16 (0.74–1.83) |
- Note: Odds ratios derived from multiple logistic regression analysis with multiple imputation (m = 20) for missing covariate information.
- Abbreviations: CI, confidence interval; OR, odds ratio.
- a Adjusted for maternal age, pre-pregnancy body mass index, education, income, country of birth, race and ethnicity, maternal cigarette smoking, plasma lipids and recruitment site.
In the sensitivity analysis stratified by parity (Table S1), the association between lead and shorter TTP remained among nulliparous (aFOR 1.10; 95% CI 1.01–1.21), and parous (aFOR 1.09; 95% CI 1.00–1.19) women. When including parity in the adjusted model (Table S2), results were similar to the main analysis presented in Table 3. The sensitivity analysis stratified by manganese levels yielded similar results in terms of FOR, except for lead where a slight attenuation in the 95% CI occurred in those with manganese concentration above the median (Table S3).
4 DISCUSSION
4.1 Main findings
In this pregnancy-based retrospective TTP cohort study in participants from the Canadian MIREC study, environmental exposure to arsenic, cadmium, manganese and mercury measured during the first trimester were not associated with TTP or infertility. Exposure to lead was associated with a shorter TTP, but the pattern of effect was not consistent with a dose–response relationship.
4.2 Strengths and limitations
The major strengths of this study include its large sample size and the use of biomarkers as an objective measure of total metal exposure. The limitations of this research are related to the retrospective assessment of exposure and outcome, residual confounding and an underlying cohort of women who became pregnant, and therefore excluded those with infertility who did not access fertility treatment or were not successful after treatment.
The measurement of exposure was taken during the first trimester of pregnancy as a proxy for pre-conception exposure. The accuracy of this measure is impacted by the stability of participant’s behaviour in relation to metal exposures, and by physiological changes during pregnancy. Both sources of error would contribute to non-differential exposure measurement error in this study and would tend to bias effect estimates towards the null, given that the measurement of exposure was collected during the first trimester of pregnancy in all participants independent of TTP. Furthermore, most of the metals included have a relatively long half-life (3–4 months for cadmium,34 90 days for lead,35 2–5 weeks for manganese36–38 and 44–80 days for mercury39–41), except for arsenic, which has a half-life of only several hours.42 However, with continuous exposure, concentrations may reach a steady state.33 Concerning the outcome, TTP was collected by questionnaire and relies on subject recall. However, the collection of retrospective TTP is a reliable method when data are collected in the short term, as was the case in the MIREC study.43
There is also the potential for residual confounding, due to the unavailability of some data in the MIREC study, such as menstrual cycle regularity, associated gynaecological conditions and coital frequency. The absence of sociodemographic and biomonitoring data for the male partner in the MIREC study is another limitation. For example, the LIFE study reported that male partners’ metal concentrations were more often associated with reduced couple fecundability compared with female partners’ concentrations.44
In addition, the study population was restricted to women who have had a birth and/or became pregnant, inherently conditioning on fertility. This introduces the potential for collider bias, which occurs when exposure and outcome each influence a common third variable, and that variable is conditioned on in the design or analysis.45 In the MIREC study, participants are restricted to those who have had a birth. Both the exposure (lead) and outcome influence fertility status and could therefore produce a collider bias because the study population has been restricted to those able to conceive.46, 47 However, biologically, there is a wide range of reproductive capacity, even among couples who achieve pregnancy. This heterogeneity is expressed in the gradual decrease in conception rates during successive months of trying,47, 48 which is not a true time effect, but evidence of sorting among individuals who are heterogeneous in their capacity to conceive.48 Heterogeneity among couples raises the possibility that some of this variation may be explained by identifiable factors, supporting the rationale of our study. Finally, as the MIREC cohort consists mainly of healthy mothers of moderate to high socioeconomic status, and Caucasian race and ethnicity,25 metal concentrations and other factors associated with TTP might differ from other populations, limiting the external generalisability of our results.49
4.3 Interpretation
Two studies have evaluated the relationship between metals and TTP, and both were prospective cohort studies of pre-conception couples. The LIFE Study observed a reduction in couple fecundity with higher exposure to cadmium and lead. When assessing individual partner exposure, female cadmium exposure (aFOR 0.78, 95% CI 0.63–0.97) and male lead exposure (aFOR 0.85, 95% CI 0.73–0.98) were associated with a longer TTP. No association was observed with mercury. Except for mercury, geometric mean concentrations of blood metals in MIREC participants (0.21 μg/L for cadmium, 0.62 μg/dL for lead and 0.61 μg/L for mercury) were similar to those reported in the LIFE study (0.21 μg/L for cadmium, 0.66 μg/dL for lead and 0.98 μg/L for mercury).21 The prospective design of the LIFE study, and the difference in sociodemographic characteristics compared with the MIREC study could explain the differences in our results. On the other hand, consistent with our results, the prospective cohort study using preconception enrolment of women from the New York Angler Cohort did not find evidence to support the association between low-level exposure to toxic metals and fecundity, even though the concentrations of metals in the Angler Cohort were higher than in MIREC (4.27 μg/L for arsenic, 1.63 μg/L for cadmium, 1.55 μg/dL for lead).20 However, the small number of participants included in this cohort (n = 80) may have made it underpowered to detect any association.
We remain uncertain about the observed association between lead exposure and a shorter TTP. To our knowledge, no other study has reported a similar finding. The absence of a dose–response when the exposure is modelled as tertiles or restricted cubic splines, suggests a spurious association, which could be a result of the above-mentioned limitations of our study. To further explore this association, we investigated the potential impact of gestational age at the time of sample collection on the association between lead exposure and TTP. This exploration was motivated by the understanding that blood lead concentrations encompass both ongoing exposure and lead stores in bone.50 During pregnancy, heightened calcium demands induce increased bone turnover, leading to the release of lead from bone and subsequent increase in blood lead levels.50–52 Our hypothesis posited a reduced fecundability (longer TTP) for metals in women’s samples collected after 10 weeks of gestation. However, we were not able to demonstrate this, as lead continued to be associated with a shorter TTP independent from the gestational age at the time of interview.
Regarding infertility, authors of an analysis among 124 participants of the 2013–2014 and 2015–2016 National Health and Nutrition Examination Surveys (NHANES) reported an association between log-transformed blood lead (OR 2.60, 95% CI 1.05–6.41) and cadmium (OR 1.84, 95% CI 1.07–3.15) and self-reported infertility.22 The geometric mean of blood lead was lower in this study (0.50 μg/dL) compared with MIREC; however, the geometric mean of blood cadmium (0.26 μg/L) was similar. Another study including a larger sample of 838 participants from the 2013–2018 NHANES reported no association between blood concentrations of cadmium or mercury and self-reported infertility.23 Lead concentrations were associated with infertility in some categories but with no overall dose–response pattern.23 Compared with MIREC, mean concentrations of cadmium and mercury in NHANES were higher (0.45 μg/L for cadmium, 1.15 μg/L for mercury); however, concentrations of lead were the same (0.70 μg/dL). We found a decreased odds of infertility in the second tertile (0.50–0.77 μg/dL) of exposure for lead (OR 0.52, 95% CI 0.33–0.84), but not in those in the highest tertile (>0.77 μg/dL) or when the exposure was modelled as a continuous variable.
5 CONCLUSION
Our study supports the theory that at current environmental levels of exposure, which are low relative to levels seen in other populations, metals are not associated with decreased fecundability or infertility. Further studies are needed to assess the role of lead, if any, on TTP and infertility.

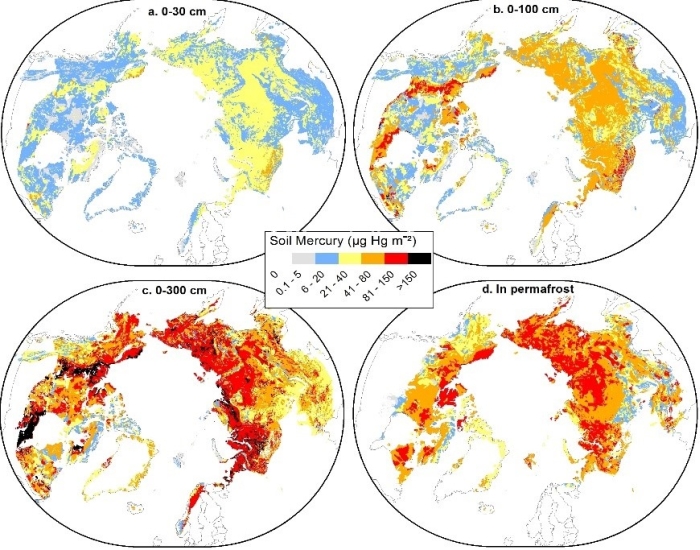 These maps show mercury concentration in micrograms per square metre for four soil depths.
These maps show mercury concentration in micrograms per square metre for four soil depths.