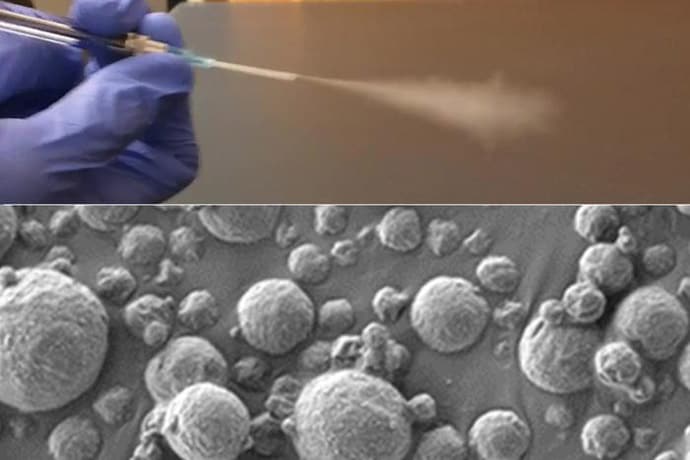
Columbia Biomedical Engineer Ke Cheng has developed a technique that uses inhalation of exosomes, or nanobubbles, to directly deliver IL-12 mRNA to the lungs of mice.
Lung cancer is one of the most common cancers and has one of the lowest survival rates in the world. Cytokines, which are small signaling proteins, such as interleukin-12 (IL-12), have demonstrated considerable potential as robust tumor suppressors. However, their applications are limited due to a multitude of severe side effects.
In a paper published recently in Nature Nanotechnology, Biomedical Engineering Professor Ke Cheng and his research group demonstrate that using nanobubbles, called exosomes, through an inhalation treatment method can directly deliver IL-12 messenger RNA (mRNA) to the lungs. mRNAs are the blueprints for producing specific proteins that participate in a variety of cellular functions.
While scientists have previously used liposomes (tiny fat-based particles) or lipid nanoparticles (LNPs) to deliver mRNA, this method has several problems, including a lack of tissue homing, where the particles do not go to the target organs, and concerns about the potential toxicity after long-term exposure. Over the past 15 years, Cheng’s group has been developing exosomes for use as superior drug delivery carriers over liposomes and LNPs in specific indications.
Innovative Delivery Through Inhalation
Up to now, clinicians have only been able to use IL-12 to treat cancer by injecting it directly into the tumor or into the bloodstream. Cheng’s lab found that having the patient — in this case, mice — inhale IL-12 mRNA in exosomes could not only deliver locally concentrated IL-12 into the lungs but also could better fight the cancer with minimal side effects. The inhalation method is more efficient in building higher concentrations of IL-12 right where it is needed than other ways of delivering mRNA such as using liposomes.
“Exosomes are usually injected systemically into the bloodstream,” said Cheng. “In this new study, we show that inhaled exosomes can efficiently reach the lung and deliver an anti-lung cancer cargo, IL-12 mRNA. This is a major step forward in advancing the development of new inhalable drugs to treat lung cancer, which has one of the lowest five-year survival rates in the world.”
Immune System Activation and Tumor Resistance
Inhaling the nanobubbles with the IL-12 blueprint can kickstart the lung immune cells, turning them into powerful defenders equipped to release substances that directly target and destroy tumor cells. In addition, IL-12 helps train these immune cells to “remember” the unique features of tumor cells. As a result, if the tumor tries to attack again, these well-informed immune cells are ready to recognize and eliminate the tumor swiftly.
Additionally, these supercharged immune cells can spread their newfound knowledge to other, untrained immune cells throughout the body, creating an army of defenders. This means that even if tumor cells try to spread beyond their original location, like the lungs, these prepared immune cells can spot and wipe them out, offering a body-wide defense system against cancer. The mice that inhaled this therapy demonstrated lung tumor suppression as well as heightened resistance against tumor rechallenges.
Combining Efficacy With Simplicity
This strategy stands out as a potent IL-12 mRNA delivery system to the lung microenvironment, say the researchers, and combines simplicity with efficacy against primary tumors and metastases. Compared to other nanoparticle controls, exosomes boost IL-12 expression with mitigated toxicity. And patients are likely to be much happier with simply inhaling the therapeutic rather than receiving intratumoral injections.
Lung cancer is the most lethal cancer, and 85% of cases are classified as non-small cell lung cancer (NSCLC). Metabolic rewiring is a cancer hallmark that causes treatment resistance, and lacks insights into serine/glycine pathway adaptations upon radiotherapy.
Methods
We analyzed radiotherapy responses using mass-spectrometry-based metabolomics in NSCLC patient’s plasma and cell lines. Efficacy of serine/glycine conversion inhibitor sertraline with radiotherapy was investigated by proliferation, clonogenic and spheroid assays, and in vivo using a serine/glycine dependent NSCLC mouse model by assessment of tumor growth, metabolite and cytokine levels, and immune signatures.
Results
Serine/glycine pathway metabolites were significantly consumed in response to radiotherapy in NSCLC patients and cell models. Combining sertraline with radiotherapy impaired NSCLC proliferation, clonogenicity and stem cell self-renewal capacity. In vivo, NSCLC tumor growth was reduced solely in the sertraline plus radiotherapy combination treatment group. Tumor weights linked to systemic serine/glycine pathway metabolite levels, and were inhibited in the combination therapy group. Interestingly, combination therapy reshaped the tumor microenvironment via cytokines associated with natural killer cells, supported by eradication of immune checkpoint galectin-1 and elevated granzyme B levels.
Conclusion
Our findings highlight that targeting serine/glycine metabolism using sertraline restricts cancer cell recovery from radiotherapy and provides tumor control through immunomodulation in NSCLC.
The withdrawal from use of a crucial treatment for lung cancer could severely affect patients, U.K. experts warn.
EGFR+ lung cancer is a type of lung cancer, not linked to smoking, that is caused by one of a number of nonhereditary gene mutations.
One mutation, exon 20, had no effective treatments beyond chemotherapy until a tyrosine kinase inhibitor called Mobocertinib (marketed as Exkivity) was licensed in 2021.
However, the manufacturers withdrew it from use in the United States late last year, and health authorities in the United Kingdom plan to follow suit next month.
EGFR+ campaigners are concerned that people in the United Kingdom with this mutation will now have no treatment options to extend life after chemotherapy.
Even though, according to the Centers of Disease Control and Prevention (CDC), 80–90%Trusted Source of lung cancer cases are linked to smoking, a significant number of lung cancers are not smoking-related.
These cancers often present in younger people and have atypical symptoms, such as shoulder pain, or other musculoskeletal symptoms, rather than the coughing, breathlessness and recurrent chest infections that are usually seen in smoking-related lung cancers.
Several different nonhereditary mutations can lead to EGFR+ lung cancer. The most common are EGFR 19 deletion — where part of the gene is missing — and EGFR L858R point mutation, in which one nucleotideTrusted Source (small unit of DNATrusted Source) is altered.
The exon 20 insertion mutationTrusted Source is the third most common cause of EGFR+ lung cancer, being responsible for up to 10% of cases. People with this mutation generally have a poorer prognosis than people with different mutations.
Prof. Siow Ming Lee, professor of medical oncology at University College London, and consultant medical oncologist at University College London Hospitals (UCLH) told Medical News Today:
“NSCLC patients with the uncommon EGFR+ exon 20 insertion mutations have an unmet need. […] Mobocertinib is a first-in-class, oral tyrosine kinase inhibitor (TKI) specifically designed to selectively target the uncommon epidermal growth factor receptor (EGFR) Exon20 insertion mutations.”
Dr. Gini Harrison, psychologist and research trustee at EGFR+ UK, and EGFR+ survivor, also emphasized how withdrawing mobocertinib from use would severely impact people who rely on it the most.
She explained:
“Mobocertinib is currently the only drug in the U.K. that is licensed for use with this patient group in an NHS [National Health Service] setting. Removing this drug from the market will mean that these patients have no treatment options beyond chemotherapy, which will certainly reduce lifespans and increase mortality rates.”
In early clinical trials, mobocertinib was well tolerated by patients, stopped their cancer from worsening, and increased their survival time, leading to optimism about its potential for people with the exon 20 mutation.
In phase 3 clinical trials, the drug failed to show a significant effect on progression-free survival (PFS). During the trial, 17% of participants stopped the treatment, half of the patients had to take a break in treatment, and 25% needed the dose reduced because of side effectsTrusted Source, although there were no significant safety concerns.
Takeda said in a press release that it was withdrawing the drug because “the Phase 3 EXCLAIM-2 confirmatory trial, […] did not meet its primary endpoint and thus did not fulfil the confirmatory data requirements of the Accelerated Approval granted by the U.S. FDA nor the conditional marketing approvals granted in other countries.”
However, Prof. Lee explained that the trial had its own shortcomings.
“It is unfortunate that when Takeda designed the first-line trial, the investigator did not include a separate trial arm combining Mobocertinib with chemotherapy,“ he told us.
“Instead, they tested a mobocertinib monotherapy arm against standard chemotherapy, despite knowing that the best ORR [tumor objective response rate] achieved as a second line was approximately 30% in pre-treated NSCLC patients,” Prof. Lee noted.
And if health authorities do withdraw this drug from use in the U.K.? Prof. Lee warned:
“Patients relapsing after first-line platinum chemotherapy will no longer be able to access the drug after the official withdrawal of the conditional marketing authorization for mobocertinib, which will occur in March 2024.”
Dr. Harrison also expressed her frustration to MNT, saying that “[t]he withdrawal of Mobocertinib is purely based on the fact that the drug failed to meet its clinical endpoint in a recent clinical trial.“
”It is not being withdrawn due to safety concerns, and indeed, no new safety concerns have arisen since the drug received its initial licence,” she emphasized.
“Instead,” Dr. Harrison explained, “the drug is being withdrawn because it was licensed on the proviso that a positive result was achieved in an RCT [randomised control trial], showing it to be more efficacious than chemotherapy in a first line setting.”
”The recent RCT (EXCLAIM-2) [trial] showed this was not achieved; however, [the drug] was shown to be as effective as chemotherapy in this setting. Given the effectiveness is on par with a licensed, effective treatment, withdrawing the drug entirely seems both unnecessary and harmful to patients,” she added.
Although mobocertinib will not be available for new patients going forward, Prof. Lee gave some reassurance to those already taking the medication.
“Patients initiated on treatment with mobocertinib before its withdrawal will still be able to access the drug through a compassionate use programme free of charge as long as they are deriving clinical benefit from the medication,” he said.
There are alternatives to Mobocertinib in the U.S., but it is the only treatment funded by the National Health Service (NHS) for exon 20 patients in the U.K.
One other drug licensed for use in the U.K. that has shown potential for exon 20 — aminvantamab — is available only privately, so cannot be accessed by those without private insurance or other means of funding, as Dr. Harrison explained.
“AmivantamabTrusted Source is an efficacious drug that is used in standard practice for exon 20 patients in Europe and the USA. It is actually approved for private use by the MHRA in the U.K., but is not currently licensed by NICE. While NICE recognises Amivantamab is likely to be efficacious for exon 20, they deem it too expensive to offer it on the NHS.”
– Dr. Gini Harrison
She called for the drug to be made available to NHS patients: “[r]ecent randomised controlled trials have shown that amivantamab is likely to be a very efficacious alternative to mobocertinib.”
“Given that this drug is already available privately in the U.K., we suggest that there should be a way to expedite NICE approval processes in situations where the withdrawal of a drug from the market leaves a treatment gap and an unmet need for patients,” she added.
The optimal first-line approach to treating non–small cell lung cancer (NSCLC) varies in accordance with a patient’s biomarkers. Comprehensive genomic profiling (CGP) tests can be used to determine the course of first-line treatment best attuned to a patient’s biomarkers, because they concurrently detect single-nucleotide variants, genetic insertions, genetic deletions, copy number amplifications, and fusions. Immune checkpoint inhibitor (ICI) immunotherapies for the treatment of NSCLC require patients to have a specific biomarker profile detectable via CGP—negativity for ALK rearrangement (fusions) and EGFR mutations (alterations L858R/EXON19 deletions)—or to have had prior toxicity or progression on oral therapies targeting mutations in these genes.1 Although CGP results can guide care for multiple types of cancer, empirical data suggest that CGP has the greatest impact on the course of treatment for patients with NSCLC.2
ASCO and NCCN have recommended that biomarker testing for ALK and EGFR at the time of diagnosis of advanced NSCLC, and before the administration of ICIs, be considered the standard of care.3,4 Nonetheless, testing continues to be underutilized, underdiagnosis occurs, and evidence shows that patients receiving contraindicated therapy may experience hyperprogression.5,6 One study found that 64.4% of potentially eligible patients with advanced NSCLC were not benefiting from precision oncology care appropriate for their disease.7 A study examining a population of patients with NSCLC who tested positive for EGFR mutation found that 16.0% initiated treatment before EGFR testing results were available.8 Although the evidence supporting the use of genomically targeted treatments is substantial, the real-world evidence is generally sparse on how using CGP in guiding treatment impacts outcomes and utilization.9
CGP enables physicians to rapidly obtain a comprehensive view of a patient’s biomarkers. In contrast, sequential testing introduces delays into the care process, because the results of initial tests are used to make subsequent testing decisions. A model of genomic testing for patients with metastatic NSCLC found that panel and next-generation sequencing approaches to testing yielded results nearly 3 weeks faster than exclusionary and sequential testing.10
Previous researchers have characterized first-line treatment patterns found in the SEER database pertaining to patients with traditional Medicare health plans, aged ≥65 years, with advanced NSCLC, initially diagnosed between 2007 and 2011.11 Since then, numerous new ICIs have been brought to market, including pembrolizumab (in 2014), nivolumab (in 2014), and durvalumab (in 2017), which are not suitable first-line treatments for patients with ALK rearrangement and EGFR mutation.12 As a consequence, research is needed to explore treatment patterns in an environment in which more options are available.
Previous research has shown that receipt of genomic testing and targeted therapy is associated with significantly longer progression-free survival in a matched cohort of patients with metastatic cancer.5 When EGFR testing for patients with nonsquamous metastatic NSCLC was introduced in Alberta, Canada, there was a significant improvement in overall survival.13 Likewise, a study of patients with diverse refractory cancers who underwent CGP and then were treated in a manner that was either matched or unmatched to their genomic profile concluded that patients receiving matched therapy had longer time-to-treatment failure and observed overall survival.14
The purpose of this study was to assess the consequences of receipt of suboptimal first-line treatment in a population of patients who were determined at some point during their treatment to have ALK rearrangement or EGFR mutation. Although all patients included in the study ultimately received CGP, had they all received it more promptly or the results been uniformly heeded, it is possible that the patients would have experienced better outcomes. To highlight the consequences of optimal versus suboptimal first-line treatment, this study examines the association between the first-line treatment selected and downstream clinical outcomes, utilization, and adverse events.
Discussion
This study found that patients who received suboptimal first-line treatment had significantly worse rwTTNT and rwTTD regardless of whether adjustments were made for potential confounders. Furthermore, patients receiving optimal first-line treatment had significantly lower ED and outpatient utilization at 3, 6, and 12 months and fewer adverse events. Collectively, these findings suggest that ensuring that patients are optimally treated leads to improved clinical outcomes and reduced utilization. In doing so, these findings build upon the literature suggesting that patients should receive CGP before initiating first-line treatment.3,24
Prior analysis has suggested that the use of CGP to guide the treatment of NSCLC is associated with both better patient outcomes and a modest financial impact driven by increased survival.10–12,25–27 Furthermore, patients with EGFR mutations have been shown to have significantly longer time to next treatment or death if they receive an EGFR tyrosine kinase inhibitor as first-line treatment, rather than immunotherapy or chemotherapy.8 The findings of this study build upon the literature by highlighting the inferior outcomes that patients may have if they receive suboptimal first-line treatment. Despite the evidence supporting CGP, patients struggle to access it, particularly in developing countries.27
Patients from states with higher percentages of households living in rural areas were found to have had significantly shorter rwTTNT and rwTTD. Although the urbanicity of the patients in this study is not known, patients from states with proportionally larger rural populations are more likely to come from rural backgrounds themselves. Prior research has found that rural patients have worse access to oncologists and inferior cancer outcomes compared with urban patients.28,29
A few limitations must be considered when interpreting the findings of this study. Patient medical records were not available, and patients were not categorized by stage or subtype of lung cancer in the analysis. Although diagnosis codes listed on claims were used to identify patients with advanced or metastatic lung cancer, it is possible that some patients had claims that were inappropriately coded. Because clinical data were not available, it is unknown why some patients were given suboptimal first-line treatments. It is possible that the patients initiated them while awaiting findings from CGP and then pursued optimal therapy after a washout period. Patients receiving optimal treatment had a significantly lower average Elixhauser comorbidity index (4.55 vs 5.65; P=.001), suggesting that this population was in somewhat better health than the population receiving suboptimal treatment (Table 1). There was likewise a higher proportion of female patients in the optimal group (66.07% vs 54.43%; P=.052), although the difference was not statistically significant using P=.05 as a cutoff. Although the reasons that patients received suboptimal first-line treatment after CGP testing are not documented in the data, a prior study with a similar observation suggested that this may have been due to discrepancies in notifying physicians about test results.8
It is also unclear why no significant differences in inpatient care utilization were observed between the optimal and suboptimal groups. Only procedure codes associated with inpatient care were available, not the diagnosis-related groups into which they are customarily aggregated for billing purposes.30 This omission may have reduced the fidelity of the inpatient care utilization data.
Finally, although the study considered a national sample, the patients were not distributed uniformly across the country. The patients who were included in this study may not have been perfectly representative of American patients with NSCLC, because all included patients had access to CGP and received it. Likewise, all the patients included received a specific CGP test; a different CGP test may have yielded different findings.
Conclusions
In the population examined, when patients with ALK rearrangement or EGFR mutation were provided with optimal NSCLC treatment, they had significantly longer rwTTNT and rwTTD, lower ED and outpatient utilization in the first 12 months, and fewer adverse events. These findings suggest that treatment concordant with CGP findings is associated with better health outcomes. These findings provide further support for the ASCO and NCCN recommendations that treatment of NSCLC be tailored to a patient’s biomarkers as ascertained through CGP
According to a new study in the journal Clinical Cancer Research, patients with non-small cell lung cancer, the most common type of lung cancer, who were treated with neoadjuvant nivolumab had improved five-year recurrence-free and overall survival rates.
Study reports five-year survival outcomes.
Patients with resectable non-small cell lung cancer (NSCLC) who were treated with neoadjuvant nivolumab had improved five-year recurrence-free and overall survival rates compared with historical outcomes.
The research will be published today, February 15, 2023, in Clinical Cancer Research, a journal of the American Association for Cancer Research (AACR), a non-profit organization dedicated to advancing cancer research and improving patient outcomes through education, collaboration, and advocacy..
Patrick Forde, MBBCh, the senior author of the study, is an associate professor of oncology and director of the Thoracic Oncology Clinical Research Program at the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins.
Samuel Rosner, MD, is co-first author of the study and is a medical oncology fellow at the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins and a member of Forde’s research group.
NSCLC Background
NSCLC is the most common type of lung cancer and is a leading cause of cancer-related death worldwide. Despite strides in treating metastatic NSCLC, new treatments for earlier-stage disease have only recently emerged, according to Forde.
Rosner added that there is great interest in optimizing neoadjuvant strategies for earlier-stage NSCLCs that are eligible for surgical resection. Rosner is a medical oncology fellow at the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins and a member of Forde’s research group.
Forde, Rosner, and colleagues previously reported safety and efficacy results from a phase II clinical trial in which patients with stage I-III resectable NSCLC were treated with two doses of neoadjuvant nivolumab. Major pathological responses were observed in 45 percent of patients, independent of tumor PD-L1 expression, and 73 percent of patients whose tumors were surgically resected were recurrence-free 18 months following surgery.
The latest publication reports the final analyses from this trial, including five-year recurrence-free and overall survival rates for the 20 patients who underwent surgical resection.
“To our knowledge, this is the longest follow-up to date for a PD-1/PD-L1 inhibitor in the neoadjuvant setting for any solid tumor,” said Forde.
Study Results
Among the 20 patients who underwent surgical resection, 12 patients (60 percent) remained recurrence-free five years after surgery, and 16 patients (80 percent) were alive, exceeding the 36 to 68 percent five-year survival rate historically observed for patients with stage I-III NSCLC, Rosner noted. Forde added that the observed patient outcomes after neoadjuvant nivolumab were better than those historically observed among patients treated with neoadjuvant chemotherapy.
The authors also identified major pathologic response after neoadjuvant nivolumab as a potential predictive biomarker of recurrence-free and overall survival. Of the nine patients who had a major pathological response after neoadjuvant nivolumab, eight were alive and cancer-free five years after treatment. One patient experienced a recurrence within the first 10 months after treatment but has since been disease-free after definitive chemoradiation. The one death in this subgroup was unrelated to cancer.
In contrast, six of the 11 patients who did not have a major pathological response experienced disease recurrence, and three of these patients died due to their cancer. These results indicate that a major pathological response following neoadjuvant nivolumab may be associated with a lower risk of disease recurrence and death, although the authors caution that these results are preliminary and require further validation in larger studies.
Neoadjuvant nivolumab did not lead to surgical delays, and there was only one late-onset immune-related adverse event, which occurred 16 months after nivolumab treatment and was successfully managed, the authors noted.
“The results from the five-year follow-up analysis indicate that neoadjuvant nivolumab was safe in long-term follow-up and led to encouraging survival in this patient cohort,” said Forde. “The long-term safety and efficacy data from this study provide further support for the use of nivolumab in the neoadjuvant setting.”
Neoadjuvant nivolumab in combination with chemotherapy was approved by the U.S. Food and Drug Administration in March 2022 for the treatment of lung cancer. “Further studies will help us determine whether select patients may benefit from immunotherapy alone,” Forde noted.
“An interesting finding from the analysis was the difference in outcomes between patients with and without a major pathological response,” said Rosner. “Although the sample size was small, the results illustrate the potential power of pathological response as a predictive biomarker.”
Reference: “Five-Year Clinical Outcomes after Neoadjuvant Nivolumab in Resectable Non-Small Cell Lung Cancer” by Samuel Rosner, Joshua E. Reuss, Marianna Zahurak, Jiajia Zhang, Zhen Zeng, Janis Taube, Valsamo Anagnostou, Kellie N. Smith, Joanne Riemer, Peter B. Illei, Stephen R. Broderick, David R. Jones, Suzanne L. Topalian, Drew M. Pardoll, Julie R. Brahmer, Jamie E. Chaft and Patrick M. Forde, 16 February 2023, Clinical Cancer Research. DOI: 10.1158/1078-0432.CCR-22-2994
Lung cancer is the deadliest cancer in the world, largely because so many patients are diagnosed late.
Screening more patients could help, yet screening rates remain critically low. In the United States, only about 6% of eligible people get screened , according to the American Lung Association. Contrast that with screening rates for breast, cervical, and colorectal cancer, which all top 70%.
But what if lung cancer detection was as simple as taking a puff on an inhaler and following up with a urine test?
Researchers at the Massachusetts Institute of Technology (MIT), Cambridge, Massachusetts, have developed nanosensors that target lung cancer proteins and can be delivered via inhaler or nebulizer, according to research published this month in Science Advances. If the sensors spot these proteins, they produce a signal in the urine that can be detected with a paper test strip.
“It’s a more complex version of a pregnancy test, but it’s very simple to use,” said Qian Zhong, PhD, an MIT researcher and co-lead author of the study.
Currently, the only recommended screening test for lung cancer is low-dose CT. But not everyone has easy access to screening facilities, said the other co-lead author Edward Tan, PhD, a former MIT postdoc and currently a scientist at the biotech company Prime Medicine, Cambridge, Massachusetts.
“Our focus is to provide an alternative for the early detection of lung cancer that does not rely on resource-intensive infrastructure,” said Tan. “Most developing countries don’t have such resources” — and residents in some parts of the United States don’t have easy access, either, he said.
How It Works
The sensors are polymer nanoparticles coated in DNA barcodes, short DNA sequences that are unique and easy to identify. The researchers engineered the particles to be targeted by protease enzymes linked to stage I lung adenocarcinoma. Upon contact, the proteases cleave off the barcodes, which make their way into the bloodstream and are excreted in urine. A test strip can detect them, revealing results about 20 minutes from the time it’s dipped.
Nanosensors that target lung cancer proteins can be aerosolized and delivered with an inhaler or nebulizer.
The researchers tested this system in mice genetically engineered to develop human-like lung tumors. Using aerosol nebulizers, they delivered 20 sensors to mice with the equivalent of stage I or II cancer. Using a machine learning algorithm, they identified the four most accurate sensors. With 100% specificity, those four sensors exhibited sensitivity of 84.6%.
“One advantage of using inhalation is that it’s noninvasive, and another advantage is that it distributes across the lung quite homogeneously,” said Tan. The time from inhalation to detection is also relatively fast — in mice, the whole process took about 2 hours, and Zhong speculated that it would not be much longer in humans.
Other Applications and Challenges
An injectable version of this technology, also developed at MIT, has already been tested in a phase 1 clinical trial for diagnosing liver cancer and nonalcoholic steatohepatitis. The injection also works in tandem with a urine test, the researchers showed in 2021. According to Tan, his research group (led by Sangeeta Bhatia, MD, PhD) was the first to describe this type of technology to screen for diseases.
The lab is also working toward using inhalable sensors to distinguish between viral, bacterial, and fungal pneumonia. And the technology could also be used to diagnose other lung conditions like asthma and chronic obstructive pulmonary disease, Tan said.
The tech is certainly “innovative,” remarked Gaetano Rocco, MD, a thoracic surgeon and lung cancer researcher at Memorial Sloan Kettering Cancer Center, Middletown, New Jersey, who was not involved in the study.
Still, challenges may arise when applying it to people. Many factors are involved in regulating fluid volume, potentially interfering with the ability to detect the compounds in the urine, Rocco said. Diet, hydration, drug interference, renal function, and some chronic diseases could all limit effectiveness.
Another challenge: Human cancer can be more heterogeneous (containing different kinds of cancer cells), so four sensors may not be enough, Zhong said. He and colleagues are beginning to analyze human biopsy samples to see whether the same sensors that worked in mice would also work in humans. If all goes well, they hope to do studies on humans or nonhuman primates.
Cigarettes contain dozens of chemicals that cause changes to DNA in lung cells.
If you’re worried about lung cancer, then smoking is incredibly dangerous. The chance of a non-smoker developing the disease is roughly one in 6,000. For someone who smokes regularly, the chances skyrocket to one in five or ten.
And yet, most people who smoke won’t develop lung cancer.
A team of researchers has begun to figure out why. In a small study published Monday in the peer-reviewed journal Nature Genetics, they report that smoking appears to drive a predictable increase in the number of cancer-causing mutations in lung cells — but only up to a point. Once someone had smoked the equivalent of a pack of cigarettes per day for 23 years, the number of mutations stopped rising.
“Our data suggest that these individuals may have survived for so long in spite of their heavy smoking because they managed to suppress further mutation accumulation,” says pulmonologist and genetics researcher Simon Spivack, a co-author on the study. “This leveling off of mutations could stem from these people having very proficient systems for repairing DNA damage or detoxifying cigarette smoke.”
A genomics breakthrough brings mutations into focus
Researchers who study the health effects of cigarette smoke have used all kinds of methods — from giving lab animals high doses of chemicals found in tobacco to combing through archives to determine which diseases smokers get more often — to figure out how the habit affects the body. Those studies have made it clear that cigarettes contain hundreds of harmful chemicals, including dozens of carcinogens.
For decades, researchers didn’t have any way to measure the mutations in lung cells that actually cause lung cancer. Five years ago, researchers at Albert Einstein College of Medicine in New York found a way to overcome technical limitations that had made it impossible to sequence the genome. That is, they figured out how to determine the exact order of the A, T, C, and G molecules of the DNA within a single cell without introducing too many errors in the process.
In this new study, many of the same researchers used that technique to compare lung cells from people who’d never smoked and from people who smoked for years.
Smoking causes mutations to build — but only up to a point
This relatively small study involved just 33 participants, ranging in age from 11 to 86 years old. Roughly half of them were smokers. The rest had never smoked. Doctors collected cells from the linings of their lungs during medically necessary bronchoscopies.
“These lung cells survive for years, even decades, and thus can accumulate mutations with both age and smoking,” says Dr. Spivack. “Of all the lung’s cell types, these are among the most likely to become cancerous.”
The researchers used their new technique to identify the number of mutations in those cells for each person. Then they compared that information to data about how much each participant had smoked over their lifetime, as measured in a unit called “pack years.” One pack year is equivalent to smoking one pack of cigarettes per day for one year. The heaviest smoker in the study had smoked for 116 pack years.
Unsurprisingly, they found that smoking for more pack years tended to correlate with more DNA mutations in lung cells. “This experimentally confirms that smoking increases lung cancer risk by increasing the frequency of mutations,” just as researchers have believed for decades, Spivack says.
But there was a surprise in their data. That close correlation between the number of pack years and the number of mutations disappeared at 23 pack years. After that point, the number of mutations stopped increasing.
“The heaviest smokers did not have the highest mutation burden,” Spivack says. In other words, the participant who’d smoked 116 pack years didn’t have five times the number of mutations as someone else who’d smoked a couple of dozen pack years. “Our data suggest that these individuals may have survived for so long in spite of their heavy smoking because they managed to suppress further mutation accumulation,” Spivack says.
More findings like these could revolutionize how doctors prevent lung cancer
While this is an early finding from a small study, it’s a remarkable fact that might offer insight into why some people get cancer while others don’t.
“This leveling off of mutations could stem from these people having very proficient systems for repairing DNA damage or detoxifying cigarette smoke,” Spivack says.
If researchers can figure out how to identify those people before it’s too late, they can offer targeted help — and give the people most likely to suffer an even better reason not to smoke.
“This may prove to be an important step toward the prevention and early detection of lung cancer risk and away from the current herculean efforts needed to battle late-stage disease, where the majority of health expenditures and misery occur,” Spivack says.
Some people could have “very proficient systems for repairing DNA damage or detoxifying cigarette smoke.”
Cigarettes contain dozens of chemicals that cause changes to DNA in lung cells.Rattankun Thongbun/iStock (left), Shutter2u/iStock (right)
If you’re worried about lung cancer, then smoking is incredibly dangerous. The chance of a non-smoker developing the disease is roughly one in 6,000. For someone who smokes regularly, the chances skyrocket to one in five or ten.
And yet, most people who smoke won’t develop lung cancer.
A team of researchers has begun to figure out why. In a small study published Monday in the peer-reviewed journal Nature Genetics, they report that smoking appears to drive a predictable increase in the number of cancer-causing mutations in lung cells — but only up to a point. Once someone had smoked the equivalent of a pack of cigarettes per day for 23 years, the number of mutations stopped rising.
“Our data suggest that these individuals may have survived for so long in spite of their heavy smoking because they managed to suppress further mutation accumulation,” says pulmonologist and genetics researcher Simon Spivack, a co-author on the study. “This leveling off of mutations could stem from these people having very proficient systems for repairing DNA damage or detoxifying cigarette smoke.”
A genomics breakthrough brings mutations into focus
Researchers who study the health effects of cigarette smoke have used all kinds of methods — from giving lab animals high doses of chemicals found in tobacco to combing through archives to determine which diseases smokers get more often — to figure out how the habit affects the body. Those studies have made it clear that cigarettes contain hundreds of harmful chemicals, including dozens of carcinogens.
For decades, researchers didn’t have any way to measure the mutations in lung cells that actually cause lung cancer. Five years ago, researchers at Albert Einstein College of Medicine in New York found a way to overcome technical limitations that had made it impossible to sequence the genome. That is, they figured out how to determine the exact order of the A, T, C, and G molecules of the DNA within a single cell without introducing too many errors in the process.
In this new study, many of the same researchers used that technique to compare lung cells from people who’d never smoked and from people who smoked for years.
Smoking causes mutations to build — but only up to a point
This relatively small study involved just 33 participants, ranging in age from 11 to 86 years old. Roughly half of them were smokers. The rest had never smoked. Doctors collected cells from the linings of their lungs during medically necessary bronchoscopies.
“These lung cells survive for years, even decades, and thus can accumulate mutations with both age and smoking,” says Dr. Spivack. “Of all the lung’s cell types, these are among the most likely to become cancerous.”
The researchers used their new technique to identify the number of mutations in those cells for each person. Then they compared that information to data about how much each participant had smoked over their lifetime, as measured in a unit called “pack years.” One pack year is equivalent to smoking one pack of cigarettes per day for one year. The heaviest smoker in the study had smoked for 116 pack years.
Unsurprisingly, they found that smoking for more pack years tended to correlate with more DNA mutations in lung cells. “This experimentally confirms that smoking increases lung cancer risk by increasing the frequency of mutations,” just as researchers have believed for decades, Spivack says.
But there was a surprise in their data. That close correlation between the number of pack years and the number of mutations disappeared at 23 pack years. After that point, the number of mutations stopped increasing.
“The heaviest smokers did not have the highest mutation burden,” Spivack says. In other words, the participant who’d smoked 116 pack years didn’t have five times the number of mutations as someone else who’d smoked a couple of dozen pack years. “Our data suggest that these individuals may have survived for so long in spite of their heavy smoking because they managed to suppress further mutation accumulation,” Spivack says.
More findings like these could revolutionize how doctors prevent lung cancer
While this is an early finding from a small study, it’s a remarkable fact that might offer insight into why some people get cancer while others don’t.
“This leveling off of mutations could stem from these people having very proficient systems for repairing DNA damage or detoxifying cigarette smoke,” Spivack says.
If researchers can figure out how to identify those people before it’s too late, they can offer targeted help — and give the people most likely to suffer an even better reason not to smoke.
“This may prove to be an important step toward the prevention and early detection of lung cancer risk and away from the current herculean efforts needed to battle late-stage disease, where the majority of health expenditures and misery occur,” Spivack says.
The saying goes ‘Where there’s smoke, there’s fire.’
Vaping seems to be an exception to that rule, as vapes, or e-cigarettes, use electricity rather than fire to convert vape liquid with substances like tobacco, nicotine, CBD and THC, into a vapor that can be smoked or inhaled.
But does this difference mean that vaping doesn’t increase your risk for lung cancer and other health problems caused by traditional cigarettes? Is vaping truly a case where there’s smoke but no fire?
Vapes differ from cigarettes, in part, because they heat liquids, not solids. Ostrin says cigarettes produce combusted plant matter that can deliver harmful chemicals directly to the lungs, leading to lung tissue destruction and lung cancer.
Still, while he says the vapor from e-cigarettes seems to be less harmful than tobacco smoking, he notes that the long-term health effects of vaping aren’t yet known.
“The effects aren’t really known and some of these epidemiological facts can take decades to really be noticed. We don’t have a great evidence basis because people haven’t been using these heavily for decades yet,” he says.
Another important distinction between traditional cigarettes and vape products is that vape products are not as regulated by the Food and Drug Administration (FDA). Ostrin says this can make it challenging for vape users to understand how much nicotine they are consuming and exactly what is in cannabis vape products like those containing THC and CBD.
Does vaping cause lung cancer?
We know that smoking cigarettes is a risk factor for several types of cancer, including lung cancer, so it is natural to wonder if vaping poses similar risks.
Unfortunately, Ostrin says that it’s still too early to tell exactly how vaping impacts the lungs.
“We don’t really know what we’re delivering into the lungs yet,” he says. “If there are little bits of damage that build up over years, we may not see it for decades.”
Ostrin says there are many chemicals in tobacco smoking that can cause the lung’s epithelial cells to undergo mutations that may lead to cancer. While he notes that vape liquid contains far fewer of these chemicals, it does contain some that can damage cells. However, he says that this hasn’t been shown outside of a laboratory setting.
“Some of these have been shown in a petri dish to cause cells to become inflamed and maybe even undergo mutation, but we don’t have yet the observational and epidemiologic data to show that there are cancers associated with it,” he says.
Cancer risk is only one of the vaping topics researchers are tackling. Ostrin says others include biological questions about vape liquid components and their impact on long-term lung health, whether vaping triggers diseases such as chronic obstructive pulmonary disease (COPD) and asthma, and epidemiologic questions.
“I think there’s an entire spectrum of research that is now kicking off,” Ostrin says.
How else does vaping impact the lungs?
There are several other lung health risks associated with vaping including some that you may have heard about on the news.
The first is EVALI, or e-cigarette or vaping use-associated lung injury. A large outbreak of EVALI occurred in 2019 when thousands were hospitalized with lung scarring and inflammation after using e-liquid thickened with Vitamin E acetate.
Ostrin says this tragedy is an example of how unregulated the vaping industry is.
“People can just go, ‘We’re going to add chemical X, Y, Z because it’s going to give more flavor, more quality,’ and they have no idea about the consequences and short- and long-term damage that these chemicals are causing,” he says.
Vaping has also been linked to a type of lung damage called bronchiolitis obliterans, or popcorn lung, which is caused by a chemical called diacetyl used to sweeten some vape liquids.
Additionally, because vape products are unregulated, they may have contaminants.
“Anybody can make this stuff and can refill these e-cigarettes,” Ostrin says. “We don’t know what sort of contaminants are in them, and there can be nasty stuff in there that can cause serious lung injury and body injury in general.”
Finally, many vape products contain nicotine. Ostrin says that it is concerning that young people who begin vaping could develop nicotine addictions and, subsequently, begin smoking cigarettes as vapes become more regulated and less available.
“Our biggest concern in terms of vaping affecting the lungs is that we’re going to be creating a new generation of nicotine addicts,” he says. “I don’t think we know that for certain, but it is certainly a worry.”
What should you do if you vape?
It may seem harmless to keep vaping, especially while research is still investigating exactly how it impacts the lungs, but quitting vapes and nicotine has concrete benefits.
“Quitting nicotine is going to save you money. It’s going to improve your lung health. It’s better for your heart,” Ostrin says.
He acknowledges that asking someone to quit nicotine is no small task.
“It’s one of the hardest things we ask our patients to do. It’s an incredibly addictive substance,” he says.
“I think the best thing that any pulmonologist would recommend is to not inhale anything except fresh air and medications prescribed to you. Anything delivered into your lungs is a big wildcard,” Ostrin says. “Delivering foreign substances into the lungs is nothing but harmful.”
Lung cancer is the most common cause of cancer-related deaths globally. Although smoking-related lung cancers continue to account for the majority of diagnoses, smoking rates have been decreasing for several decades. Lung cancer in individuals who have never smoked (LCINS) is estimated to be the fifth most common cause of cancer-related deaths worldwide in 2023, preferentially occurring in women and Asian populations. As smoking rates continue to decline, understanding the aetiology and features of this disease, which necessitate unique diagnostic and treatment paradigms, will be imperative. New data have provided important insights into the molecular and genomic characteristics of LCINS, which are distinct from those of smoking-associated lung cancers and directly affect treatment decisions and outcomes. Herein, we review the emerging data regarding the aetiology and features of LCINS, particularly the genetic and environmental underpinnings of this disease as well as their implications for treatment. In addition, we outline the unique diagnostic and therapeutic paradigms of LCINS and discuss future directions in identifying individuals at high risk of this disease for potential screening efforts.
Key points
The global incidence of lung cancer is decreasing in parallel with declining smoking rates in developed countries; however, the incidence of lung cancer in individuals who have never smoked (LCINS) is stable or increasing.
LCINS is the eighth leading cause of cancer-related mortality in the USA and the fifth most common cause of cancer-related deaths worldwide.
LCINS has histological and epidemiological distinctions from smoking-related lung cancers, occurring almost exclusively as adenocarcinomas and most commonly in women and individuals of Asian ancestry.
LCINS are highly enriched for targetable oncogenic alterations, have low tumour mutational burden and low rates of PD-L1 positivity, and lack mutational signatures, even in patients who report passive, secondhand smoke exposure.
LCINS development probably involves interactions between genetic risk, mediated by common and rare germline variants, and environmental exposures, including air pollution and particulate matter, with potential opportunities for broader lung cancer screening.
In the era of precision oncology, the biological underpinnings of LCINS necessitate unique diagnostic and treatment paradigms and warrant consideration of this disease as an important and distinct clinical entity.



/img/iea/3oOpyreKGW/smoking-dna.jpg)

