You probably don’t have to look further than your local drugstore or beauty product supplier to know CBD has taken a starring role in everything from sparkling water and gummies to tincture oils and lotions. Some may even say that cannabidiol (CBD) — which, like THC, is a component of the cannabis plant, but doesn’t contain its psychoactive effects — is the “it” ingredient of our age.
You’ve probably also heard that CBD can help lessen stress, anxiety, and pain. “When people are in pain, they have a stress response, which causes an increase in cortisol and an increase in blood sugar,” says Veronica J. Brady, PhD, CDCES, a registered nurse and an assistant professor at the Cizik School of Nursing at the University of Texas in Houston. Relieving pain can help alleviate the stress response and improve blood sugar levels, as well as aid sleep, she says.
If you’re managing type 2 diabetes, it’s natural to be curious about whether CBD might help you manage those symptoms, too, to help stabilize your blood sugar. In fact, the prevalence of cannabis use increased by 340 percent among people with diabetes from 2005 to 2018, according to one study, which surveyed people on their use of cannabis (CBD or THC, in any form) in the previous 30 days.
But will popping some CBD gummies for diabetes work Some healthcare professionals say CBD may have a role to play, but it’s important to understand that the only health condition CBD has proved effective for is epilepsy in kids. The jury is unfortunately still out, owing to the lack of comprehensive research on CBD for diabetes.
Still, in the aforementioned survey, 78 percent of people used cannabis that was not prescribed by a doctor. “Diabetes patients might still use cannabis for medical reasons, but not have a prescription,” says Omayma Alshaarawy, MBBS, PhD, an assistant professor in the department of family medicine at Michigan State University in East Lansing, who led the study. Recreational use is another factor. She points to a separate study that found that more than 50 percent of people with medical conditions such as diabetes or cancer use cannabis recreationally.
How People With Type 2 Diabetes Are Using CBD
In Nevada, where Dr. Brady used to work as a certified diabetes educator, her patients with type 2 diabetes used CBD for nerve pain. She says patients would use CBD in a tincture or in oils that they rubbed on painful areas, including their feet. Patients could buy CBD at medical marijuana dispensaries, which would offer dosing instructions. “They worried about the impact on their blood sugars,” says Brady.
Ultimately, though, Brady says that her patients reported that CBD reduced their nerve pain and improved their blood sugar. She adds that those people who used CBD oils for nerve pain also reported sleeping better.
Heather Jackson, the founder and board president of Realm of Caring in Colorado Springs, Colorado, a nonprofit that focuses on cannabis research and education, senses a community interest in CBD for diabetes. “In general, especially if they’re not well controlled, people are looking at cannabinoid therapy as an alternative, and usually as an adjunct option,” says Jackson. Callers have questions about CBD for neuropathy pain, joint pain, gastrointestinal issues, and occasionally blood glucose control, according to a spokesperson for Realm of Caring.
The organization receives thousands of inquiries about cannabis therapies a month. It keeps a registry of these callers, where they live, and their health conditions. Jackson says that people with type 2 diabetes are not a large percentage of the callers, but they currently have 540 people with diabetes in their database.
Jackson says that Realm of Caring does not offer medical advice, and it does not grow or sell cannabis. Instead, it offers education for clients and doctors about cannabis, based on its ever-growing registry of CBD users, their conditions, side effects, and administration regimen. “We are basically educating,” says Jackson. “We want you to talk to your doctor about the information you receive.”
Scientific Studies on CBD and Type 2 Diabetes and Barriers to Research
Despite interest among people with type 2 diabetes, large, rigorous studies showing how CBD may affect type 2 diabetes are lacking, says Y. Tony Yang, MPH, a doctor of science in health policy and management and a professor at George Washington University School of Nursing in Washington, DC. Specifically absent are randomized controlled trials, which are the gold standard of medical research.
At the very least, a case report from 2021 suggests that CBD is unlikely to cause harm or worsen diabetes control. (The American Diabetes Association also stresses that CBD should not be considered a replacement for traditional diabetes management.)
Other research suggests the use of CBD for diabetes is indeed worth further study. For example, a small study in the United Kingdom looked at 62 people with type 2 diabetes and found that CBD did not lower blood glucose. Participants were not on insulin, but some took other diabetes drugs. They were randomly assigned to five different treatment groups for 13 weeks: 100 milligrams (mg) of CBD twice daily; 5 mg of THCV (another chemical in cannabis) twice daily; 5 mg CBD and 5 mg THCV together twice daily; 100 mg CBD and 5 mg of THCV together twice daily; or placebo. In their paper, the authors reported that THCV (but not CBD) significantly improved blood glucose control.
Other CBD research is still evolving. Some research on CBD for diabetes has been done in rats, which leads to findings that don’t always apply to human health. Other research has looked more generally at the body’s endocannabinoid system, which sends signals about pain, stress, sleep, and other important functions. Still other studies have looked at marijuana and diabetes, but not CBD specifically.
That there are so few studies of CBD in people with type 2 diabetes has to do with a lack of focus on CBD as an individual component. Historically, cannabinoids (a group of chemicals in the cannabis plant) have been lumped together, including CBD, THC, and more than 100 others. The 1970 U.S. Controlled Substances Act classifies cannabis as a Schedule 1 drug with the highest restrictions, according to the Alcohol Policy Information System. Currently, 38 states allow cannabis for medical use, and 24 states and the District of Columbia have passed legislation allowing cannabis for recreational use, per CNN.
The 2018 Farm Bill removed industrial hemp from the controlled substances list, clearing the way for more production and research of CBD. Meanwhile, growers and manufacturers are better able to isolate CBD, mainly by cultivating industrial hemp that is high in CBD and very low in THC, says Jackson. So, perhaps in the coming years, more research on CBD and diabetes will emerge.
How the FDA Views and Regulates CBD for Disease Treatment
Yet, as evidenced by a previously cited study, people with type 2 diabetes aren’t waiting for further study to hop on the trend. Brady says her patients have been open about using CBD, particularly the younger patients. She says one of her older patients was initially uncomfortable about buying CBD in the same shop that sold marijuana but eventually gave in. Brady adds that many people associate CBD with smoking marijuana, despite their distinctly different effects on the body.
The U.S. Food and Drug Administration (FDA) approved the first CBD medication in 2018, for treating childhood epilepsy. Currently, there is no other FDA-approved CBD medication for diabetes or any other condition, according to the FDA. In December 2018, the FDA said it was unlawful under the Federal Food, Drug, and Cosmetic Act to sell food or dietary supplements containing CBD. But in January 2023 the FDA concluded that a new regulatory pathway for CBD is necessary and that it intends to work with Congress to develop one.
“The FDA, for the time being, has focused its limited enforcement resources on removing CBD products that make claims of curing or treating disease, leaving many CBD products for sale,” wrote Pieter Cohen, MD, and Joshua Sharfstein, MD, in The New England Journal of Medicine. Dr. Cohen is an assistant professor of medicine at Harvard Medical School in Boston, and Dr. Sharfstein is the vice dean for public health practice and community engagement at the Johns Hopkins Bloomberg School of Public Health in Baltimore.
Precautions for People With Diabetes Looking to Try CBD
For the CBD products already on the market, Jackson says it’s often difficult to know what’s inside. One study found that only 30 percent of CBD products were accurately labeled, with under- and over-labeling of CBD content, and some products containing unlisted chemicals such as THC.
Vaping liquids were the most commonly mislabeled CBD products in the study. The Centers for Disease Control and Prevention (CDC) warns that consumers should not purchase any vape products from unregulated and illicit markets or attempt to modify vape products outside of how the manufacturer intended. The Associated Press has shown that some CBD vapes have synthetic marijuana.
Jackson points out that CBD may affect certain cholesterol and blood pressure drugs, and research has detailed these interactions. Other side effects of CBD include tiredness, diarrhea, and changes in weight or appetite, the researchers write.
“What you put in your body is really important,” says Jackson, adding that’s especially true for people with major health conditions like diabetes. Jackson speaks from personal experience as a mom finding CBD treatments for her son’s epilepsy. She says consumers should ask manufacturers whether CBD products are free of mold, pesticides, and other toxins.
“There is little known about cannabis health effects, especially among patients with chronic conditions. Research is growing, but still solid evidence evolves,” says Dr. Alshaarawy. For these reasons, she recommends that patients talk to their doctors so they can discuss the benefits and potential harms of cannabis and monitor their health accordingly.
How to Talk to Your Healthcare Provider About Using CBD for Type 2 Diabetes
Jackson and Brady advise people who are considering CBD for diabetes to ask their providers about the complementary therapy before adding it to their treatment plan. Brady says it’s difficult to find research about CBD and type 2 diabetes, even in her capacity as a diabetes educator. Still, in her experience, if people are looking for a natural way to manage pain, it’s worth a conversation with their healthcare provider. “It’s something that should be talked about, especially if they’re having significant amounts of pain, or really any pain at all associated with their diabetes,” says Brady.
“It’s a reasonable alternative,” says Brady. “As it gains in popularity, there needs to be some information out there about it.
The side effects of cancer therapy continue to cause significant health and cost burden to the patient, their friends and family, and governments. A major barrier in the way in which these side effects are managed is the highly siloed mentality that results in a fragmented approach to symptom control. Increasingly, it is appreciated that many symptoms are manifestations of common underlying pathobiology, with changes in the gastrointestinal environment a key driver for many symptom sequelae. Breakdown of the mucosal barrier (mucositis) is a common and early side effect of many anti-cancer agents, known to contribute (in part) to a range of highly burdensome symptoms such as diarrhoea, nausea, vomiting, infection, malnutrition, fatigue, depression, and insomnia. Here, we outline a rationale for how, based on its already documented effects on the gastrointestinal microenvironment, medicinal cannabis could be used to control mucositis and prevent the constellation of symptoms with which it is associated. We will provide a brief update on the current state of evidence on medicinal cannabis in cancer care and outline the potential benefits (and challenges) of using medicinal cannabis during active cancer therapy.
Despite the excitement that surrounds newer, more targeted agents, the reality for most people with advanced cancer is that chemotherapy will be used, and it will cause a degree of collateral damage to healthy tissues [1]. Clinically, this damage presents as a broad variety of diverse, individualised, and highly dynamic symptoms and side effects. Rarely do these side effects occur in isolation; instead, they present as clusters of related symptoms that are united by common underlying mechanisms, as well as physical and psychosocial/behavioural determinants [2]. With increased accessibility of “big”, real-world data, these symptom clusters have been documented and characterised with greater precision [3]. This has prompted new initiatives to identify early drivers of chronic treatment-related morbidity, with the goal of halting the self-perpetuating nature of inter-related symptom clusters.
Of the many documented side effects of chemotherapy, the breakdown of the mucosal barrier of the gastrointestinal tract (“mucositis”) is one of the earliest and most common. Mucositis is initiated by rapid and extensive DNA damage in highly proliferative stem cells throughout the gastrointestinal mucosa [4]. The resulting apoptosis and inflammation degrades the mucosa, leading to the formation of ulcerative lesions in the mouth, oesophagus, intestines and rectum which severely impair functional capacity. This dysfunction can lead to taste changes, dysphagia, pain and malabsorption; each of which drive anorexia, malnutrition and dehydration [5]. On a cellular level, these breaches in the protective mucosa create an inhospitable environment for resident gut bacteria, leading to loss of commensal species and their protective metabolites including short-chain fatty acids (SCFAs). These changes further weaken the mucosal barrier and permit unrestricted communication between the underlying immune system and luminal compounds (e.g., danger signals). This results in profound local and systemic inflammation which leads to numerous extraintestinal consequences such as fever (“febrile mucositis”) [6], cognitive impairment [7, 8] and fatigue [9]. As such, the destructive changes in the gastrointestinal microenvironment position mucositis as a catalyst for a range of secondary complications, and a key player in a range of symptom clusters.
Despite the impact of mucositis on patients and the healthcare system, it remains without effective intervention, and its range of secondary symptoms/consequences are managed reactively and in isolation [10]. Given the body of evidence that now suggests many symptoms and treatment consequences may be influenced by mucositis, there is an opportunity to control mucositis to mitigate the constellation of impactful symptoms with which it is associated. This review aims to outline a rationale for how, based on its already documented effects on the gastrointestinal microenvironment, medicinal cannabis could be used to control mucositis and prevent its associated symptom cluster. We will provide a brief update on the current state of evidence on medicinal cannabis in cancer care and outline the potential benefits (and challenges) of using medicinal cannabis during active cancer therapy.
Medicinal cannabis: illicit drug, plant, or medicine?
Cannabis has been used medicinally for over 3000 years, primarily for its analgesic properties. The predominant phytocannabinoids in cannabis by amount are Δ9-tetrahydrocannabinol (Δ9-THC or THC) and cannabidiol (CBD), with mainstay medicinal cannabis (MC) preparations containing either or both of these compounds in varying ratios as the active ingredients, either as isolates or whole extracts. However, there remains a vast phytochemical complexity to cannabis aside from just THC and CBD, whereby whole extracts may contain over one hundred different minor phytocannabinoids and terpenes, all of which may vary in their relative expression across a number of cannabis chemotypes and displaying variable retention via different extraction processes [11, 12]. Many of these compounds have been shown to exhibit selective bioactivities that may interact with the efficacy of THC and CBD in MC preparations and may be considerations particularly where full-spectrum botanical extracts are concerned, oft described through the popular term ‘entourage effect’ applied to medicinal cannabis [13, 14]. However, their contribution to the efficacy of most conventional MC formulations where THC and CBD predominate may only be marginal, with a paucity of investigative studies on these cannabis phytochemicals compared to THC and CBD.
Today, over 40 countries have legalised MC, with different access pathways depending on jurisdictional legislation [15]. Despite significant variation across jurisdictions, the medicinal use of cannabis is guided by the formulation (oil, sprays, tablets and flowers). Typically, MC requires prescription for a pre-defined indication or with clear clinical justification for why a certain condition may respond positively to MC. This ambiguity often results in lengthy and administratively burdensome reporting requirements; hence, MC use continues to be a challenging medico-legal entity. The combination of its often high cost, clinician hesitancy and logistic difficulties for supply compared to relative ease of access in the community, is a major driver of why people continue to self-medicate with uncontrolled and non-standardised cannabis products.
Canada was one of the first countries to introduce a MC access programme in 1999. Between 2015 and 2019, the number of registered MC patients in Canada increased from 40,000 to nearly 400,000, an increase attributed to several policy changes that have gradually broadened access to a variety of medicinal cannabis formulations. In December 2015, the first cannabis oil product was launched in the Canadian market and in 2016, the Access to Cannabis for Medicinal Purposes Regulations allowed patients to grow cannabis for personal use [16].
The United States was another early adopter of medicinal cannabis, starting with state-level legalisation in California in 1996. Now, as of February 2023, medicinal cannabis has been legalised in 37 states, 3 territories, and the District of Columbia [17]. In February 2019, Thailand became the first and only nation in Southeast Asia to legalise medicinal cannabis, offering three different categories of cannabis-based products: medicinal-grade cannabis-based medicines, Thai traditional medicine products that contain cannabis as the active ingredient, and folk medicine products prepared by registered folk healers [18].
In 2016, cannabis was rescheduled in Australia to enable access for medicinal purposes. Currently, the majority of cannabis products are classified as “unapproved” therapeutic goods, with two exceptions: Sativex (nabiximols), an oromucosal spray containing equivalent amounts of THC and CBD, and Epidyolex (also known as Epidiolex), a CBD solution with a concentration of 100 mg/mL (Therapeutic Goods Administration, 2020a). The situation in the UK is similar; even though medicinal cannabis was legalised in 2018, it remains challenging for patients to obtain access, with only a limited number of National Health Service prescriptions issued to date [19]. Medicinal products that meet safety, quality and efficacy standards are registered on the Australian Register of Therapeutic Goods (ARTG), however additional pathways such as Special Access Schemes (SAS) and an Authorised Prescriber (AP) scheme facilitate patient access to “unapproved” therapeutic goods, including many other types of MC products currently. This scheme is being increasingly adopted in Australia, with the MC Therapeutic Goods Administration (TGA) dashboard showing an increase in AP applications and a levelling off of SAS-B approvals in the last 2 years.
The “endocannabinoidome” and its relevance to chemotherapy symptoms and side effects
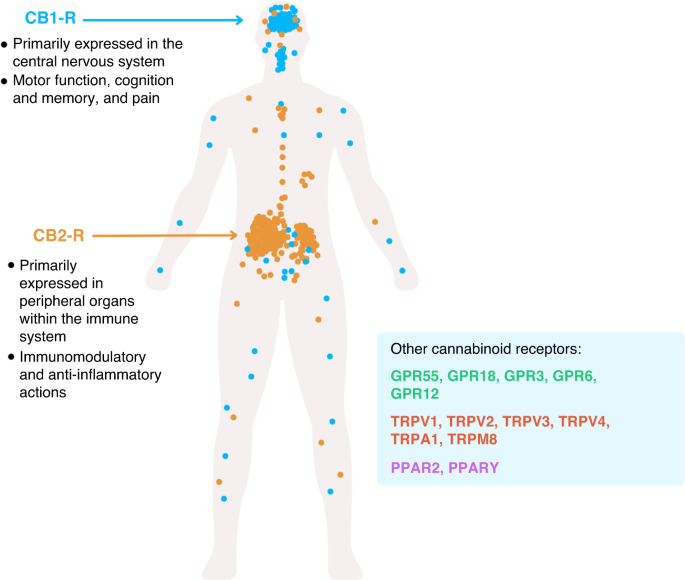
The endocannabinoidome or, in its broader sense, the endocannabinoid system (ECS), is an endogenous network of receptors, enzymes, transporters and ligands, that has largely been recognised for its role in regulating of neurotransmitter release [20]. However, this original concept of the ECS is gradually being replaced by an increasingly sophisticated and complex network capable of regulating numerous biological pathways and functions across a range of organ systems. The interactions that exist within the ECS are critical to central nervous system development, synaptic plasticity and the homeostatic maintenance of cognitive, behavioural, emotional, developmental and physiological processes [20, 21]. These diverse mechanisms are mediated by endogenous cannabinoids which are produced on demand, both physiologically and patho-physiologically, from membrane lipids and are metabolised by fatty acid amide hydrolase (FAAH) and monoacylglycerol lipase (MAGL), respectively [22]. They include the main known endocannabinoids, N-arachidonoylethanolamine (AEA) or anandamide and 2-arachidonoylglycerol (2-AG) produced by phospholipid precursors through activity-dependent activation of specific phospholipase enzymes; N-acyl-phosphatidylethanolamine-selective phosphodiesterase and phospholipase C subsequent production of diacylglycerol via diacylglycerol lipase, respectively [20]. The broadly termed acylethanolamines and acylglycerols interact to a variable extent with cannabinoid receptors including the well-described CB1 and CB2 receptors (CNR1/CNR2) as well as other G-protein-coupled receptors such as GPR55, GPR18, GPR3, GPR6, GPR12, transient receptor potential channels such as TRP vanilloids TRPV1 to TRPV4, TRP ankyrin TRPA1, TRP M member TRPM8 and peroxisome proliferator-activated receptors such as PPAR2, and PPARγ [23]. Although there are diverse receptors with which endocannabinoids interact, CNR1 and CNR2 are functionally characterised both physiologically and with respect to ECS dysfunction.
CNR1 is a G-protein-coupled receptor that is highly abundant within the peripheral and central nervous system, largely present on axon terminals and pre-terminal axon segments [24] (Fig. 1). It is highly abundant in medium spiny neurons in both the dorsal and ventral striatum, and is particularly high on the direct pathway axons as they enter the globus pallidus heading towards the substantia nigra [25]. However, the expression of CNR1 is increasingly diverse, with a range of immune cells (including glia) now understood to express CNR1 [26,27,28] as well as the more immunologically abundant, CNR2. Indeed, there remains debate about the expression of CNR2 which has historically been considered to be mainly expressed in the periphery [29]. Although emerging evidence suggests it is expressed on sensory nerve terminals and microglia in the brain [30].
Fig. 1: Simplified scheme representing the expression pattern of the main cannabinoid receptors, CNR1 and CNR2.
Although not the only components of cannabis, the most commonly studied and clinically utilised components, THC and CBD, are highly lipid soluble and have a poor bioavailability when inhaled (10–35%) or orally ingested and 11–45% [31,32,33]. When THC is consumed by inhalation or mucosal sprays, it is absorbed through the lungs into the bloodstream and concentrations in the plasma will typically peak in less than 10 min [31] and when it is orally congested, concentrations may peak at ~2 h. THC is distributed into well vascularises organs as well as the brain. THC and CBD are highly protein-bound and has a half-life of 25–36 and 18–32 h, respectively [31, 34], with some of the metabolites (THCCOOH) having a very long half-life up to 52 h [35]. Chronic users have much longer half-lives.
THC undergoes extensive first-pass metabolism in the liver by cytochrome P450 (CYP 450) isozymes; these enzymes are also responsible for the metabolism of many anti-cancer drugs and several other commonly used co-medication and are known to cause large inter-individual variability in plasma concentrations for majority of clinically used medications [36]. Therefore, it is particularly important to investigate any potential drug–drug interactions to avoid toxicity or therapeutic failure for any of the medications. THC primarily is metabolised via oxidation by CYP2C9, CYP2C19 and CYP3A4 into several metabolites with 11‐hydroxy‐THC (11‐OH‐THC) and 11‐carboxy‐THC (11‐COOH‐THC) being the most abundant [34, 37]. 11-OH-THC is metabolised by the UGT1A9 and UGT1A10 enzymes and 11-COOH-THC is metabolised mostly by the UGT1A3 and UGT2B7enzyme [34, 35]. CBD is also metabolised in the liver via mostly CYP3A4, CYP2C19 and CYP2C9 and other CYPs to a lesser degree via hydroxylation to form metabolites, 7-OH-CBD and 7-COOH-CBD, which is then undergoes glucuronidation by UGT1A9 and UGT2B7 [31, 34]. The remaining THC, CBD and metabolites can be taken up by fat tissue before it is redistributed into the circulation. More than 65% of THC and CBD will be excreted in faeces and ~20% in the urine [35, 37]. Metabolites excreted in urine have been observed to vary up to fivefold between individuals when drug administration was controlled, demonstrating the variability in metabolism [35].
Inter-individual differences in pharmacogenomics, pharmacokinetics and pharmacodynamics may explain contradictory outcomes from previous studies and accounting for such differences will provide an opportunity for personalised medicine where efficacy can be maximised, and toxicity minimised for various conditions or diseases [38].
Reflecting the breadth of cells upon which ECS receptors are expressed, the ECS regulates a number of critical functions that are well-known to contribute to the side effects of chemotherapy. Most notable is its psychotropic properties, modulating mood, anxiety, cognition, appetite, sleep and pain [39, 40]; all of which are well-documented to be negatively impacted by chemotherapy [1]. Peripheral CB1 expression is also implicated in gastrointestinal inflammation, mucosal defences and gastric motility [41,42,43,44], and thus by extension diarrhoea and constipation, due to its expression on presynaptic cell of sympathetic motor neurons innervating visceral organs leading to reduced noradrenalin release [45]. Further to this, given the immunomodulatory capacity of the ECS, its ability to influence numerous symptoms and side effects of chemotherapy of which many are underpinned by aberrant inflammation, is vast. It is for these reasons that medicinal cannabis, and strategies to augment the ECS, have gained considerable momentum for their potential benefits in people with cancer.
Medicinal cannabis use in cancer care: what is the evidence?
Cannabis use in people with cancer is not uncommon, although it remains difficult to determine exact prevalence due to heterogeneous results published across numerous studies with varied designs. In a study published in 2018, 43% of respondents (at a Canadian cancer centre) reported using “illicit” cannabis for a variety of symptoms and side effects of their treatment [46]. This is similar to a large population-based analysis from 2005 to 2014 in the US, which showed 40.3% of the 826 respondents with cancer having used cannabis in the last 12 months [47]. However, in a larger survey of more than 200,000 people, results indicated that less than 10% of people were using cannabis [48]. Irrespective of self-reported cannabis use, there is a high degree of interest in its potential benefits during cancer care, with 80% of healthcare professionals reporting that they have engaged in conversations with their patients about cannabis [49]. Unfortunately, less than 30% feel equipped to guide their patients citing a lack of clear evidence on its safety and efficacy [49]. This uncertainty undoubtedly stems from the inadequate and highly variable evidence base for cannabis in cancer care, which is dominated by largely observational studies that are subject to inherent biases, powerful placebo effects and diverse confounders, leading to a high rate of false positives [50,51,52]. Similarly, of the limited number of randomised control trials, few are considered high quality and they remain near impossible to compare/synthesise due to inherent differences in design, outcome measures and cannabis products/doses/delivery/formulations used [50]. This has prevented replication and meta-analyses, and the resulting evidence base is therefore inconsistent and largely uninformative.
Although challenging to compare studies, a large number of systematic reviews have been conducted in an attempt to synthesise data and determine its efficacy in symptom control. Notably, there have been few that have been able to perform meta-analysis, reflecting the heterogeneity of available data. The most recent review of cannabis in cancer care reviewed 42 studies (19 randomised, 23 non-randomised), focused on people with cancer receiving palliative care [53]. Among these studies, pain was the most commonly investigated symptom, with highly variable effects reported across the studies. This aligns with a recent systematic review and meta-analysis which investigated the effect of cannabis for pain management in people with cancer, which was unable to form any conclusive recommendation [54]. Accordingly, recent guidelines from the Multinational Association for Supportive Care in Cancer (MASCC) do not recommend the use of cannabinoids for cancer pain, although, it is unclear how this relates to chemotherapy-induced pain which is diverse in its origins [52].
While pain has dominated the landscape for cannabis research in cancer care, emerging evidence exists for its role in chemotherapy-induced nausea and vomiting (CINV), anorexia, cachexia, sleep disturbance and psychological symptoms (depression/anxiety). Doppen and colleagues reviewed the evidence for CINV, reporting generally positive effects across multiple studies using various assessment tools [53]. This is consistent with recommendations from MASCC, which show THC and nabilone are both effective in controlling CINV, however, no more effective than current antiemetic medications [55]. Despite these positive findings, MASCC was unable to form any guideline due to insufficient, high-quality evidence. This is echoed by the American Society for Clinical Oncology (ASCO) who question the quality of current evidence [56]. Despite the lack of clinical recommendation from MASCC and ASCO, it appears that there is discordance between published clinical trial data and anecdotal reports of patient preferences, which tend to favour cannabis over existing antiemetic strategies, even when adverse effects were higher [57, 58].
MASCC maintains a similar stance with respect to anorexia and cachexia, with limited evidence available to inform relevant guidelines. Doppen et al. reviewed 15 studies for cannabis and appetite, with both objective and self-reported benefits reported for nabinol and Marinol, however, several studies reported no or inconsistent effects [53]. Given the heterogeneity in data and approaches, it remains difficult to draw robust conclusions despite the popularised effects of cannabis on appetite stimulation. Similarly, for psychological effects (e.g., on sleep, anxiety, depression), MASCC were unable to make any recommendations with most studies investigating these outcomes as secondary analyses with inconsistent data across studies [51].
While the systematic review by Doppen et al. has provided insight on the current state of evidence regarding cannabis use in cancer care, it has been scrutinised for its methodology and over-simplification of data as “positive” and “negative” effects based on the null hypothesis significance test [50, 53]. As cautioned by Davis and Soni (2022), our approach to cannabis research should be guided by effect sizes that are deemed clinically significant, rather than statistically significant [50]. Furthermore, they highlight the need to be more holistic in our assessment of cannabis for symptom management, avoiding excessively large studies designed with highly restrictive outcomes guided by narrow-minded criteria [50]. With this in mind, and the growing appreciation for symptom clusters in people undergoing chemotherapy, there is a clear rationale to prioritise trial designs that address clusters of related symptoms, rather than single symptoms, to deliver meaningful impacts to the participant’s physical or psychosocial well-being. Critical to these approaches is the inclusion of consumers in cannabis research, to ensure research methodologies are informed by, and consistent with, consumers behaviours and preferences. In line with ensuring consumer engagement, trials should include relevant patient reported outcome measures (PROMs) to ultimately determine if cannabis has a meaningful impact on people with cancer.
Gastrointestinal effects of cannabis: can they be adapted to control mucositis?
Cannabinoids, including both CBD and THC, are increasingly documented for their capacity to modulate gastrointestinal function, owing to the immense control that the ECS has on gastrointestinal homeostasis. Both CNR1 and CNR2 are present in the gastrointestinal tract, largely on enteric nerves and the epithelium, but also on enteroendocrine cells and immune cells [42]. This network of ECS receptors controls gastric motility, and as such, it is now understood that variants in the genes encoding for CNR1 are implicated in diseases characterised by altered motility including irritable bowel syndrome (IBS), particularly diarrhoea-predominant [59]. Both CNR1 and CNR2 are expressed in the gut at medium to high degrees, respectively. Accordingly, it has been shown that agonists of the cannabinoid receptors (CNR1 and CNR2) [60, 61], as well as targeting endocannabinoid degradation [62], minimises experimental colitis and associated visceral hypersensitivity [63]. Furthermore, preclinical investigations have shown that potent agonists of CNR1 (without central nervous system effects) and CNR2 have been shown to control increased gastrointestinal motility caused by stress [64] and inflammation [44]. Similarly, inhibition of anti-diacylglycerol lipase (DAGL) and fatty acid amide hydrolase (FAAH)—two enzymes critical in endocannabinoid metabolism—has been shown to normalise transit time in the context of opioid-induced constipation [65]. Of particular interest to changes in the gastrointestinal microenvironment associated with mucositis is the ability of CNR2 activation [66] and FAAH inhibition [67] to control accelerated gastrointestinal motility induced by lipopolysaccharide—a bacterial product that is causally implicated in chemotherapy-induced diarrhoea.
In addition to its effect on gastrointestinal motility, which has clear applications in controlling chemotherapy-induced diarrhoea, the ECS exerts potent immunomodulatory effects in the gastrointestinal tract controlling intestinal inflammation [41]. Both synthetic CB receptor agonists and endocannabinoids have been shown to impair cellular and humoral immunity by reducing inflammatory cell recruitment, inducing T-cell apoptosis and suppressing the production of numerous pro-inflammatory cytokines and chemokines (e.g., TNF-α, IL-1β, IL-2, IL-6, IL-17, IFN-γ, CCL2 or CXCL10) [41, 68]. Therapeutically, both exogenous administration of cannabis and preventing endocannabinoid degradation by inhibiting FAAH have been shown to reduce colitis [60,61,62,63, 69]. In fact, FAAH inhibition and CB receptor activation have shown efficacy in mouse models of colitis and FAAH knockout mice are less susceptible to experimentally induced colitis compared to wild-type mice [69]. The ability of endocannabinoids (or exogenous cannabis products) to accelerate wound healing in the gut points to their ability to promote intestinal/mucosal barrier function, that is, the bonding of intestinal epithelial cells to create a uniform and restrictive barrier. This mechanism has been confirmed in vitro, with cannabinoids improving or maintaining paracellular permeability (i.e., leakiness) and tight junction protein expression in Caco-2 cells treated with Clostridium difficile toxin A and other barrier-directed insults (e.g., cytokines, EDTA) [41, 70]. These mucoprotective effects have also been reported preclinically, with cannabinoids reported to decrease intestinal permeability (and increase regulatory T-cell recruitment) in experimental colitis induced by dextran sulfate sodium (DSS) [41]. It has also been suggested that cannabinoids can modulate secretory processes in the intestinal epithelium which, when dysregulated, lead to altered osmotic forces and potentially diarrhoea [71,72,73,74].
An emerging area of interest with respect to the gastrointestinal microenvironment is the interaction between the ECS, cannabis and the gut microbiota [43, 75, 76]. The gut microbiota is a collection of micro-organisms (bacteria, viruses and fungi) that reside in the gastrointestinal lumen and mucosal niches, regulating host physiology and immune function. Importantly, these beneficial host-directed effects are best achieved when there is high microbial diversity and enrichment for commensal microbes. Chemotherapy indirectly impacts the diversity and composition of the gut microbiota, through the destruction of their mucosal niches and oxidative stress [77]. As such, a highly dysbiotic microbiota is a hallmark trait of chemotherapy, and an event documented to drive a range of adverse effects including fever, infection, diarrhoea, cachexia, weight loss, anxiety, cognitive impairment, cardiotoxicity and fatigue. Although a relatively new concept, emerging data suggests an interaction between the ECS and the gut microbiota. Most recently, cannabis extracts (CN1, CN2, CN6) were shown to increase microbial diversity and richness in a mouse model of metabolic disease whilst promoting enrichment of microbial taxa associated with health [78]. Further suggesting an ECS-microbiota interaction is the finding that germ-free mice (mice without a microbiota) are deficient in a number of ECS components, including the CNR1 [79]. A microbial taxa of particular interest is Akkermansia muciniphila, a mucus-degrading microbe implicated in gut inflammation [80] and chemotherapy side effects [81, 82]. This microbe is reportedly elevated in response to CNR1 antagonism with the compound SR141716A, although this was only demonstrated in obese mice [76, 83]. Despite this emerging evidence, it is unclear if medicinal cannabis influences the gut microbiota and if this mechanism underpins/delivers meaningful impacts for the host.
Collectively, this body of evidence strongly demonstrates the profound control that the ECS exerts on gastrointestinal function, regulating motility, barrier function and repair, immune function, secretion and potentially the microbiota. These data underscore the potential mucoprotective effects of exogenous cannabinoid administration or augmentation of the ECS. In the context of cancer care, this therefore supports strategies targeting ECS (via direct cannabinoid administration or inhibition of degradation) to control mucositis and promote a more resilient gastrointestinal microenvironment. Despite the scientific strength of this rationale, and the prevalence of mucositis (occurs in ~60% of patients treated with standard chemotherapy), there have been few attempts to explore the mucoprotective properties of medicinal cannabis in cancer care [55]. This may reflect the complexities of using/investigating medicinal cannabis during active cancer treatment.
Using medicinal cannabis during active cancer treatment: precautions, challenges and potential benefits
To minimise both the depth and duration of mucositis, supporting the gastrointestinal microenvironment and controlling the constellation of symptoms with which mucositis is associated, medicinal cannabis should be used during active chemotherapy treatment. Of course, this raises some concerns regarding the possibility of adverse drug interactions with anti-cancer therapies and potential loss of anti-tumour efficacy. There has been limited investigation of how cannabis influences the anti-tumour efficacy of cancer treatment. Cannabis has been investigated for its effect on the pharmacokinetics of irinotecan and docetaxel, with no effects observed [84]. On the other hand, two recently reported observational studies indicate a negative impact of cannabinoids on immune checkpoint inhibitors (ICI) related cancer outcomes [85, 86]. Bar-Sela et al. highlighted in a prospective study that the concomitant use of prescribed cannabis was associated with lower response rates (39% vs 59%), median time to progression (3.4 months vs 13.1 months) and median overall survival (6.4 months vs 28.5 months) when compared to ICI therapy alone [85]. Another retrospective observational study from the same research group reported inferior outcomes for cannabinoid use along with nivolumab (an ICI) when compared to nivolumab among selected solid cancers [86]. While some evidence suggests that cannabis may impair the anti-tumour efficacy of immunotherapy [87, 88], recent evidence suggests cannabis may actually have a synergistic effect with immunotherapy. This has been shown both preclinically and clinically, with median survival in CT26 tumour-bearing mice treated with THC and an anti-PD1 antibody having significantly higher overall survival compared to controls [89]. Authors also reported higher overall survival (numerical, failed to reach statistical significance) in 201 people with non-small cell lung cancer undergoing monotherapy with pembrolizumab who used medicinal cannabis. Although this does not confirm a synergistic effect, it does indicate no detrimental effect. The only study in which a definite synergy has been identified was preclinical, where a combination of cannabigerol and anti-PD-1 resulted in enhanced tumour clearance and increased survival compared to monotherapy in tumour-bearing mice [90]. Given the evidence from low quality clinical trials, well conducted trials are required to assess the efficacy of cannabinoids as anti-cancer therapeutics either alone or in combination with other systemic cancer therapies.
In the context of chemotherapy, although there is no concrete evidence that suggests cannabis may impair its anti-tumour efficacy, given the increasing evidence for immune-mediated mechanisms enhancing chemoefficacy [91], this risk cannot be ignored and should be appropriately built into studies investigating medicinal cannabis in combination with standard chemotherapy. Although it remains exclusively experimental and prone to inflation, there is a growing body of evidence that suggests medicinal cannabis may in fact be a beneficial adjunct to standard chemotherapy, capable of inducing cell death or controlling proliferation by inducing endoplasmic reticulum (ER) stress [92, 93], proteosome inhibition [94], upregulation of matrix metalloproteinases [95] and reactive oxygen species activation [96]. In line with these findings, several studies have outlined the potential for cannabinoids to be used as anti-cancer agents either on their own or in combination with other systemic cancer therapies or radiotherapy [97, 98]. A recent review summarised the anti-cancer effects of cannabinoids to be mediated through multiple pathways including anti-proliferative, pro-apoptotic, pro-autophagy, anti-invasion and metastasis, anti-angiogenesis, and immunomodulation [99]. However, it is important to note that the majority of these findings have only been explored in vitro or in preclinical (animal) models and are subject to inflation in the public domain. As a result, these benefits have not been robustly translated into the clinical setting.
Three human clinical trials reported the results on the role of cannabinoids on patients with recurrent glioma [100,101,102]. Guzman et al. demonstrated that only two of nine patients with recurrent Glioblastoma (GBM) had reduced tumour proliferation when treated with intracranial Δ9-THC alone as monotherapy [100]. Another trial that combined Nabiximols (a mixture of plant-derived THC, CBD and non-cannabinoid compounds) with temozolomide (N = 27) resulted in a numerically higher 2-year overall survival (50% vs 22%, P = 0.13) when compared to placebo/TMZ [101]. Schloss et al. compared two different doses of THC/CBD combination as adjunct to standard treatment of recurrent high-grade gliomas (N = 88) and demonstrated an improved quality of life and an imaging-assessed tumour response in 11% while 34% had stable disease when compared to historical controls [102]. These clinical trials highlight that a small proportion of people with recurrent GBM may benefit from cannabinoids, however, there are no available predictive biomarkers that may identify responders and non-responders.
In addition to the impact on anti-tumour efficacy, the other main risk associated with medicinal cannabis use in parallel to active treatment is drug–drug interactions. Given the predominant role of MC for pain control in cancer care, its interaction with other analgesics is of interest. Evidence suggests that cannabis may in fact enhance opioid-induced analgesia, with synergistic analgesia observed when opioid/cannabinoid ligands are co-administered. In animal studies, either morphine or codeine produces synergistic antinociception when combined with THC [103,104,105,106], and similar synergies have been documented in humans [107]. However, these benefits must be taken in light of evidence that suggests this combination may increase tolerance to both forms of analgesia and increase the risk of “drug-liking” effects [88, 108]. There is also evidence to suggest drug–drug interactions between CBD and the non-steroidal anti-inflammatory, naproxen, although this is limited to in vitro evidence [109]. However, both CBD and THC are metabolised by CYP2C9, suggesting the possibility of impaired drug clearance [109] or renal/liver toxicity. However, there are no data to suggest CBD and THC cause renal/liver toxicity, and in fact there is data to suggest hepatoprotective effects [110] and prevention of cisplatin-induced renal toxicity [111]. However safety profiles of MC in the context of cancer care remains superficially addressed, underscoring the importance of regular renal and liver function tests, appropriately titrated dosing, and studies with co-primary endpoints that address efficacy and safety [88]. These studies should also endeavour to capture the patient experience with respect to milder adverse events such as dry mouth and fatigue/somnolence, given their association with both cancer therapy and MC.
While medicinal cannabis use during active chemotherapy presents some challenges, if approached carefully, there are a number of benefits that can be achieved. These benefits largely relate to the ability to control multiple symptoms early in their aetiology, rather than therapeutically targeting single symptoms that may have developed and persisted well after treatment ends. This holistic approach to controlling multiple symptoms is in line with recent suggestions by the MASCC, and also aligns with the scientific evidence that underpins the clinical phenomenon of symptom clustering [112,113,114].
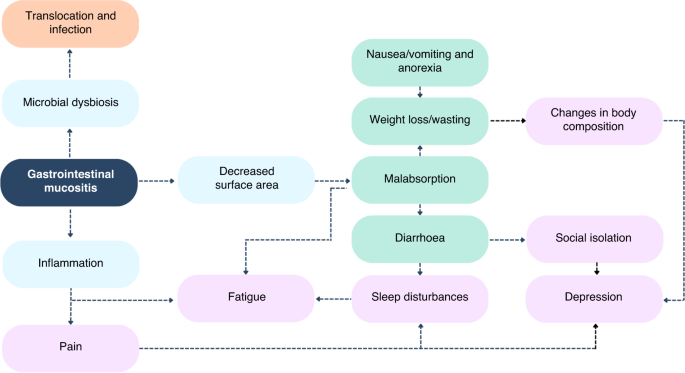
We have outlined a clear rationale for how medicinal cannabis products, or augmentation of the ECS, modulates gastrointestinal function and exerts mucoprotective effects. It is therefore well positioned to target numerous mechanisms known to be involved in mucositis pathobiology and symptomatology. Given the documented role of mucositis and associated changes in the gastrointestinal microenvironment (e.g. gut microbiota dysbiosis) driving a range of intestinal and extraintestinal symptoms, medicinal cannabis in the active stages of chemotherapy may deliver broad-reaching benefits. This is particularly compelling when considering that medicinal cannabis, and the ECS, will likely have paralleled effects on these associated symptoms. For example, mucositis can cause taste changes and pain, leading to reduced oral intake (anorexia) and therefore clinically impactful weight loss. As such, targeting mucositis with cannabis, whilst simultaneously promoting food enjoyment and behaviours, will likely deliver meaningful impacts of weight maintenance and nutritional status. Similarly, diarrhoea and pain due to mucositis is anecdotally thought to cause sleep disturbances [115]. Again, by addressing a biological cause and providing symptomatic relief, the potential for meaningful impacts on patient quality of life is enhanced. This same framework can be applied to numerous, interacting consequences of mucositis and associated symptoms (Fig. 2).
Fig. 2: The centrality of gastrointestinal mucositis to infectious (orange), gastrointestinal (green) and neuropsychological (purple) symptoms commonly reported in people with advanced cancer undergoing chemotherapy.
By approaching symptom management in this manner, the magnitude of benefit is likely to be larger, and thus the health and well-being of people undergoing chemotherapy better maintained. This will deliver knock-on effects to patients, ensuring they remain in the workforce, thus reducing personal financial toxicity, and remain willing/capable of receiving their intended chemotherapy dosing ensuring optimal tumour response and progression-free/overall survival. This indirect effect on treatment efficacy is significant and should not be disregarded. For example, in a recent review of 874 women with advanced breast cancer, chemotherapy dose reductions of >15% significantly increased the risk of mortality [116]. Similarly, a reduction in total cumulative dose of neoadjuvant FEC-D (where it is <85% of intended dosing) decreased the length of survival in women with breast cancer [117]. Similar effects have been reported in ovarian cancer and colon cancer [118,119,120].
When considering the causes of dose reductions or modifications, adverse effects (i.e., side effects) are the most common cause, accounting for 82% of all dose reductions in a recent audit of 584 people undergoing adjuvant chemotherapy for stage III colon cancer [119]. As such, the provision of proactive supportive care that tackles symptom clusters at multiple points in their aetiology and progression is critical. In fact, the provision of supportive care early in symptom aetiology is recommended, with evidence illustrating both quality of life and survival benefits when this approach is adopted [121]. Furthermore, by addressing multiple symptoms concurrently, or targeting common underlying mechanisms of multiple symptoms, polypharmacy (5+ medications) can be reduced. More than 80% of people with advanced care report polypharmacy [122]. This approach is fragmented and places substantial burden on the patient who must navigate multiple medications, increasing their risk of adverse drug interactions and medical misadventure [123]. With recent calls to address the fragmented approach to supportive cancer care and symptom control [124], the ability of MC to transcend multiple symptoms is compelling and advantageous.
In considering how MC can be used to deliver substantive impacts for people undergoing chemotherapy, a number of practical matters must be carefully considered. Firstly, there are a range of cannabis extracts that are available for consumption in a variety of formulations ranging from dry leaves/buds which can be smoked or vaporised, to highly purified and processed isolates [125, 126]. Typically, the more readily accessible cannabis products are in the community, the lower the degree of purification and quality assurance. In light of high rates of self-reported use [16, 46, 48], this underscores the need to deliver evidence that (if shown to be beneficial) will ensure patients can access MC in more appropriate and safe formulations.
Cannabis is commonly available as an oil, which contains or is enriched for CBD and THC, typically in combination with many other cannabinoids and phytochemicals (e.g., terpenes) at varying proportions. Oils are a convenient method of administration and can be directly administered to the oral cavity for rapid mucosal absorption, however, they do require a degree of dexterity and are prone to inaccurate dosing as people typically administer their dose as a number of “drops” [88]. Similarly, sublingual or oral–mucosal sprays can be used. While direct application to the oral mucosa is a common and easy method of administration, it is important to consider how factors like oral mucositis may influence tolerance, as some sprays are prepared in an ethanol diluent which would be painful to apply to an ulcerated oral cavity. Similarly, it is unclear how oral mucositis impacts the rate of absorption. Oils can also be encapsulated for ingestion; however, this method of administration must be considered in the context of dysphagia and nausea/vomiting, which may impact the patient’s ability to swallow a capsule, or intestinal mucositis which may also influence the rate of absorption [127]. This underscores the need to conduct appropriate pharmacokinetic studies to understand how these unique factors associated with cancer, in particular active chemotherapy, impact the uptake and efficacy of cannabis. Further to this, there is evidence that suggests the presence of high-fat food impacts the bioavailability of cannabis, and thus this should be carefully considered in the design of capsules and other formulation strategies [32, 128]. Importantly, these methods of administration result in different clinical effects, particularly with respect to the timing and duration of the response [88]. These should be considered when selecting the time of administration (i.e., time of day) and the symptom or side effect(s) of interest.
In addition to the method of administration, the selection of specific cannabinoids and their relevant doses is critical. This decision needs to be guided by the specific symptom or side effect(s) of interest, with a clear scientific rationale for their use. When considering the MC intervention of interest, it is also important to acknowledge and respect the complexity of medicinal cannabis as an entire entity (i.e., a whole plant) in which the combination of numerous active compounds work cooperatively to elicit benefit. As such, while using synthesised isolates may be attractive from a pharmacological perspective, evidence suggests that the synergy of numerous cannabis compounds, a process referred to as the “entourage effect”, outweighs the benefits that can be gained from a single isolate or molecule.
In the context of mucositis and its constellation of symptoms, the use of CBD and THC (with other cannabinoids and compounds such as terpenes) is likely to be best positioned to deliver meaningful benefits based on their unique yet synergistic effects [13, 129]. Of note, CBD is documented to counteract the undesirable psychotropic effects of THC [130] and may therefore improve adherence. This synergy is in addition to the ability of these compounds to address different but related symptoms. For example, CBD is hypothesised to control self-perpetuating inflammatory pathways that ultimately dictate the depth and duration of mucosal injury to deliver clinically meaningful benefits [62, 131,132,133]. In parallel, THC has the capacity to provide complementary effects to control anxiety, promote food intake/appetite and sleep quality [134,135,136,137]. However, it cannot be ignored that while THC provides potential benefits for the patient, it certainly introduces additional medico-legal complexity, with many countries enforcing strict no-tolerance laws with respect to operating heavy machinery or driving motor vehicles. This may negatively impact patient well-being by impacting their employment prospects, or ability to live independently. It also poses challenges for patients that may have caring duties. Further advice regarding dosing has been summarised by Cyr and colleagues [88].
The future of medicinal cannabis
The field of MC has been and continues to be difficult to navigate, reflecting the legislative challenges, variations in formulations and complexities of this emerging pharmacotherapy [33, 34, 38, 138]. To understand how to appropriately use this plant and its individual components in a therapeutic manner and avoid toxicity, well-designed in vitro and in vivo clinical pharmacology studies are required, particularly due to individual differences [138, 139]. Understanding the clinical pharmacology involved with MC will take the ‘guesswork’ out of the current largely uncontrolled and uncertain approach, which could provide the long wanting ‘safeguard’ for many vulnerable [140] individuals who are not benefiting from current practices and already suffering from poor quality of life due to undergoing cytotoxic chemotherapy and/or many other unpleasant conditions.
It is well-known that there are many cannabis species producing hundreds of compounds of which more than 100 chemicals are known as phytocannabinoids, with THC, CBD, terpenes and flavonoids being mostly abundant [31, 34]. Therefore, in order to provide this ‘safeguard’ with MC therapy, there are two key elements that need to be addressed. The first being, understanding the molecular mechanisms behind both the therapeutic and adverse effects of the various compounds within MC, and the second being, understanding the pharmacogenomics, pharmacokinetics and pharmacodynamics of the various products and formulations between individuals [34, 38, 139].
To achieve this, well-established genetic approaches should be adopted in the field of MC to facilitate precision medicine (‘selecting right drug’) [38, 139] and pharmacokinetic-guided approaches to facilitate precision dosing (‘selecting the right dose’) [31, 34, 141]. For the latter, specifically, exposure-response studies via therapeutic drug monitoring or pharmacogenomics may enable individualised therapy [38, 139], similar to how it has been done for anti-cancer therapeutics [142]. In addition, to provide true individualised or personalised dosing, population pharmacokinetic–pharmacodynamic (POP-PK/PD) models need to be developed to better understand how the population and individuals respond to these compounds, and which covariates (e.g., age, weight, gender, genotype, comedications, etc.) drive any variability in the pharmacokinetics and thus responses [140].
It has been well-documented that clinical trials are limited and of the available data, it is clear that varied design has resulted in the inability to compare and establish conclusive evidence. However, with personalised medicine currently in its peak in many research areas, such as antimicrobials, and anti-cancer drugs [143], it is an ideal time to build on current research and investigate which compounds should be isolated or combined in the appropriate formulations and administered to truly enable personalised MC therapy [34, 38, 139]. This will lead to a better understanding how exactly these compounds exert their effects and how this knowledge can be utilised to treat conditions such as mucositis which in turn has the potential to reduce symptom clustering and an array of treatments which cause additional challenges (polypharmacy, drug–drug interactions, adverse effects, poor quality of life and financial burden) for both the individuals and the healthcare systems. The need and opportunity to investigate how MC therapy can be personalised for individuals suffering from mucositis and other conditions is evident and brings on an exciting future for MC research.
While trial data remain inconclusive, it is likely that individual factors that dictate tolerance and efficacy have contributed to the variable and often contradictory results observed. For example, previous cannabis use is associated with lower anxiety after THC. Similarly genomic factors have been shown to predict the efficacy and tolerability of CBD. In a recent genomic study of patients with treatment-resistant epilepsy, single-nucleotide polymorphisms in certain genes were identified which were associated with a lower response and greater side effects of CBD [141]. The study also revealed genetic variants that were related to the likelihood of CBD-associated diarrhoea [141]. These findings present an opportunity for personalised pharmacogenomics-guided strategies for precise MC treatment that could be particularly advantageous for patients undergoing chemotherapy, already at risk of gastrointestinal side effects such as diarrhoea [141]. Understanding these factors will be critical in optimising the safe and effective use of cannabis in medical practice.
Conclusions
Soon after the discovery of its chemical structure and ability to obtain various compounds from the plant in the late 1900s, as well as the description of the cannabinoid receptors and the endocannabinoid system in the 1990s, cannabis use for medical purposes has increased significantly with a steep rise in the last few years [31, 144]. It is evident that the majority of this use results from illegal access, however, this has been recognised and laws are in a fast-changing phase with several products approved and several others on a registered unapproved list. This provides new opportunities for users and prescribers to access MC products in a legal manner. In cancer care, self-reported cannabis use is prevalent, however, the evidence base is lacking due to inconsistencies in study design and outcomes. Moving forward, it is critical that research efforts integrate appropriate pharmacokinetic and mechanistic sub-studies to understand cannabis biology in the context of cancer and investigate its efficacy in a more holistic sense by considering its impact on clusters of related symptoms. In the context of mucositis, this is a compelling approach given the numerous symptoms that occur secondary to mucosal barrier injury and the already documented benefits medicinal cannabis has on gastrointestinal physiology, inflammation, and dysfunction.
Over a third of adults in the United States don’t get the recommended 7 hours of sleep per night. Trusted Source Centers for Disease Control and Prevention (CDC) As the nation’s health protection agency, CDC saves lives and protects people from health threats. View Source With all that tossing and turning, over-the-counter (OTC) and prescription medications are popular options for improving sleep.
But more people appear to be turning to cannabis as an alternative sleep aid, according to a new 2023 study published in the journal Exploration of Medicine. Currently, 47 states and the District of Columbia have regulations allowing the medical and/or recreational use of cannabis. Trusted Source National Conference of State Legislatures View Source Yet, not much is known about its benefits for sleep.
Researchers examined data from an extensive survey done by a Canadian medical marijuana data company on the use of cannabis among people who have problems sleeping. Participants included over 1,200 people who say they use cannabis to help them sleep. Most survey participants reported having sleep issues for over five years, including trouble falling asleep, feeling tired the next day, and waking up at night.
The researchers looked at the survey results to find out how cannabis affects participant’s sleep and how it makes them feel compared to prescription and OTC sleeping pills. They also looked at how the participants use cannabis and the type of cannabis they prefer to help them sleep. Two of the most well-known cannabinoids are tetrahydrocannabinol (THC), the compound that makes you feel high, and cannabidiol (CBD), which has a calming effect but doesn’t make you feel high.
Over 80% said that cannabis helps them sleep by relaxing their mind and body. More than half said it helps them sleep more deeply. Another 42% reported it allows them to sleep longer, and 36% reported it allowed them to sleep without waking. When asked about average sleep hours per night, 63% said they get 6-8 hours when only using cannabis, compared to 20% or less saying the same when using sleep medicines combined with cannabis, sleep medications alone, or no sleep aids.
The survey found that most people prefer to smoke or vape cannabis compared to using oils or edibles. About 79% said they use THC for sleep, more than other forms like CBD or cannabinol (CBN). The majority (82%) said they don’t take any sleep medications currently, though half had used them in the past. People are more likely to use cannabis in place of sleep medications instead of using both at the same time, the study authors noted.
Cannabis can have side effects, including anxiety and irritability. Still, participants feel more focused and relaxed the next morning compared to taking other sleep aids. Sleep medications can come with side effects such as dizziness, daytime drowsiness, and difficulty concentrating or remembering things.
This study adds to the current knowledge about the effectiveness of cannabis as a sleep aid relative to sleep medicines. For example, a 2022 study showed 39% of people stopped their sleep medication after they started using cannabis. And 71% of them said their sleep improved. Trusted Source National Library of Medicine, Biotech Information The National Center for Biotechnology Information advances science and health by providing access to biomedical and genomic information. View Source However, the study authors note that more research is needed, and their findings may help guide future, more objective and controlled studies.
Summary: A study of 42 runners reveals that using cannabis before exercise can boost mood and enjoyment. The study shows that both THC and CBD can enhance exercise experience, with CBD even outperforming THC in some aspects.
However, THC can make exercise feel more effortful due to increased heart rate. While cannabis may improve enjoyment, it’s not considered a performance-enhancing drug, and its use should be approached with caution.
Key Facts:
Cannabis, both THC and CBD, can enhance the enjoyment and mood during exercise, potentially making it more enjoyable.
CBD, in particular, showed significant benefits in enhancing exercise experience without the impairment associated with THC.
THC can increase heart rate, making exercise feel more challenging, and it’s not recommended for performance enhancement.
Source: University of Colorado
A bit of weed before a workout can boost motivation and make exercise more enjoyable. But if performance is the goal, it may be best to skip that joint.
That’s the takeaway of the first ever study to examine how legal, commercially available cannabis shapes how exercise feels.
The study of 42 runners, published Dec. 26 in the journal Sports Medicine, comes almost exactly 10 years after Colorado became the first state to commence legal sales of recreational marijuana, at a time when cannabis-users increasingly report mixing it with workouts.
“The bottom-line finding is that cannabis before exercise seems to increase positive mood and enjoyment during exercise, whether you use THC or CBD. But THC products specifically may make exercise feel more effortful,” said first author Laurel Gibson, a research fellow with the University of Colorado Boulder’s Center for Health and Addiction: Neuroscience, Genes and Environment (CU Change).
The findings, and previous research by the team, seem to defy long-held stereotypes that associate cannabis with “couch-lock” and instead raise an intriguing question: Could the plant play a role in getting people moving?
“We have an epidemic of sedentary lifestyle in this country, and we need new tools to try to get people to move their bodies in ways that are enjoyable,” said senior author Angela Bryan, a professor of psychology and neuroscience and co-director of CU Change. “If cannabis is one of those tools, we need to explore it, keeping in mind both the harms and the benefits.”
‘A first-of-a-kind study’
In one previous survey of cannabis users, Bryan’s research group found that a whopping 80% had used before or shortly after exercise. Yet very little research has been done at the intersection of the two.
For the study, Bryan and Gibson recruited 42 Boulder-area volunteers who already run while using cannabis.
After a baseline session, in which the researchers took fitness measurements and survey data, they assigned participants to go to a dispensary and pick up either a designated flower strain that contained mostly cannabidiol (CBD) or a Tetrahydrocannabinol (THC) -dominant strain.
THC and CBD are active ingredients in cannabis, with THC known to be more intoxicating.
On one follow-up visit, volunteers ran on a treadmill at a moderate pace for 30 minutes, answering questions periodically to assess how motivated they felt, how much they were enjoying themselves, how hard the workout felt, how quickly time seemed to pass and their pain levels.
On another visit, they repeated this test after using cannabis.
Federal law prohibits the possession or distribution of marijuana on college campuses, so the runners used it at home, before being picked up in a mobile laboratory, a.k.a the ‘CannaVan,’ and brought to the lab.
The runners also wore a safety belt on the treadmill.
‘Not a performance-enhancing drug’
Across the board, participants reported greater enjoyment and more intense euphoria, or ‘runner’s high,’ when exercising after using cannabis.
Surpisingly, this heightened mood was even greater in the CBD group than in the THC group, suggesting athletes may be able to get some of the benefits to mood without the impairment that can come with THC.
Participants in the THC group also reported that the same intensity of running felt significantly harder during the cannabis run than the sober run.
This may be because THC increases heart rate, Bryan said.
In a previous study conducted remotely, she and Gibson found that while runners felt more enjoyment under the influence of cannabis, they ran 31 seconds per mile slower.
“It is pretty clear from our research that cannabis is not a performance enhancing drug,” said Bryan.
Notably, numerous elite athletes—including U.S. sprinter Sha’Carri Richardson— have been prohibited from competing in recent years after testing positive for cannabis.
An NCAA committee recently recommended that it be removed from its list of banned substances.
A different kind of runner’s high
Why does cannabis make exercise feel better?
While natural, pain-killing endorphins have long been credited with the famous “runner’s high,” newer research suggests that this is a myth: Instead, naturally produced brain chemicals known as endogenous cannabinoids are likely at play, kicking in after an extended period of exercise to produce euphoria and alertness.
“The reality is, some people will never experience the runner’s high,” Gibson notes.
By consuming CBD or THC, cannabinoids which bind to the same receptors as the cannabinoids our brain makes naturally, athletes might be able to tap into that high with a shorter workout or enhance it during a long one, she said.
Athletes considering using cannabis should be aware that it can come with risks — including dizziness and loss of balance— and it’s not for everyone.
For someone gunning for a fast 5k or marathon PR, it doesn’t really make sense to use beforehand, Bryan said.
But for an ultrarunner just trying to get through the grind of a double-digit training run, it might.
As a public health researcher, Bryan is most interested in how it could potentially impact those who struggle to exercise at all, either because they can’t get motivated, it hurts, or they just don’t like it.
“Is there a world where taking a low-dose gummie before they go for that walk might help? It’s too early to make broad recommendations but it’s worth exploring,” she said.
Why do people mix weed and workouts?
When researchers asked study participants, here’s what they said:
90.5% It increases enjoyment
69% It decreases pain
59.5% It increases focus
57.1% It increases motivation
45.2% It makes time go by faster
28.6% It improves performance
Abstract
Acute Effects of Ad Libitum Use of Commercially Available Cannabis Products on the Subjective Experience of Aerobic Exercise: A Crossover Study
Objective
The present study aimed to examine the acute effects of legal-market cannabis on regular cannabis users’ subjective responses to exercise in a controlled laboratory environment.
Background
Given the stereotype that cannabis is associated with extreme sedentary behavior, there are concerns that cannabis legalization may exacerbate the US physical inactivity epidemic. However, despite these concerns, recent years have seen considerable public interest in the use of cannabis concurrently with exercise (e.g., running).
Methods
The present study compared participants’ experiences of exercise without cannabis to their experiences of exercise after acute ad libitum use of one of two commercially available cannabis flower products: a Δ9-tetrahydrocannabinol-dominant or a cannabidiol-dominant product. Participants (N = 42) were regular cannabis users between the ages of 21 and 39 years (mean = 30.81 years, standard deviation = 4.72 years).
Results
Although participants reported a more positive affect (p < 0.001), enjoyment (p < 0.001), and runner’s high symptoms (p < 0.001) during their cannabis (vs non-cannabis) exercise appointment, they also reported more exertion (p = 0.04). Pain levels were very low and did not differ between appointments (p = 0.45). Effects appeared to depend, in part, on cannabinoid content; there was a larger difference in enjoyment (p = 0.02), and a smaller difference in exertion (p = 0.02), between the cannabis and non-cannabis exercise appointments among participants in the cannabidiol (vs Δ9-tetrahydrocannabinol) condition.
Conclusions
To our knowledge, this is the first study to investigate the acute effects of commercially available cannabis on subjective responses to exercise in a laboratory environment. Our findings suggest that, among regular cannabis users who use cannabis in combination with exercise, cannabis use prior to exercise may lead to increases in both positive and negative aspects of the subjective exercise experience. Research using diverse samples, exercise modalities, and methodologies (e.g., placebo-controlled trials) is needed to establish the generalizability of these findings.
A study by researchers in the U.S. and U.K. has revealed a previously unknown mechanism by which cannabidiol (CBD)—a non-psychoactive component of cannabis—reduces seizures in many treatment-resistant forms of pediatric epilepsy. Led by researchers at NYU Grossman School of Medicine, the new study, in rodent models, found that CBD blocked signals carried by a molecule called lysophosphatidylinositol (LPI) in neurons. LPI is thought to amplify nerve signals as part of normal function, but can be hijacked by disease to promote seizures.
The new research confirmed a previous finding that CBD blocks the ability of LPI to amplify nerve signals in the brain’s hippocampus, and argues for the first time that LPI also weakens signals that counter seizures, further explaining the value of CBD treatment.
“Our results deepen the field’s understanding of a central seizure-inducing mechanism, with many implications for the pursuit of new treatment approaches,” said corresponding author Richard W. Tsien, PhD, chair of the Department of Physiology and Neuroscience at NYU Langone Health. “The study also clarified, not just how CBD counters seizures, but more broadly how circuits are balanced in the brain. Related imbalances are present in autism and schizophrenia, so the paper may have a broader impact.”
When a neuron “fires” it sends an electrical pulse down an extension of itself until it reaches a synapse, the gap that connects one neuron to the next cell in a neuronal pathway. When the electrical impulse reaches the cell’s end before the synapse, it triggers the release of neurotransmitters that are travel across the gap to reach the next cell. Upon crossing this synapse, such signals either encourage the next cell to fire (excitation), or apply the brakes on firing (inhibition). Balance between the two are essential to brain function; too much excitation promotes seizures, and an imbalance between inhibition and excitation is also implicated in other disorders. “Neuronal circuits require coordination between synaptic excitation (E) and inhibition (I) for proper function,” the authors wrote, ”and disruptions in the excitatory-to-inhibitory (E:I) ratio contribute to epilepsy, autism spectrum disorders, and schizophrenia.”
But while cannabidiol has been shown to reduce seizures in multiple forms of pediatric epilepsies, the mechanism(s) of anti-seizure action remain unclear. “In preclinical models, CBD reduces spontaneous recurrent seizures and regulates the E:I ratio in acute seizures; however, the molecular signaling underlying CBD’s anti-seizure actions remains poorly defined.”
Possible therapeutic targets of CBD encompass ion channels, transporters, and transmembrane signaling proteins, the team noted. Among the proposed candidates are two GPCRs: the cannabinoid receptor CB1R and the receptor GPR55. “In one model, CBD acts at glutamatergic axon terminals, blocking the pro-excitatory actions of the endogenous membrane phospholipid lysophosphatidylinositol, at the G-protein-coupled receptor GPR55 … However, the impact of LPI-GPR55 signaling at inhibitory synapses and in epileptogenesis remains underexplored.”
For their new study, the team looked at several rodent models to explore mechanisms behind seizures. “… we focused on the LPI-GPR55 signaling pathway as a potential modulator of E:I ratio and anti-seizure target of CBD.
To do this they used a variety of techniques that included measuring information-carrying electrical current flows with fine-tipped electrodes, or by investigating the effect of LPI by genetically removing its main signaling partner, or by measuring the release of LPI following seizures. Their collective results confirmed past findings that LPI influences nerve signals by binding to GPR55, on neuron cell surfaces. This LPI-GPR55 presynaptic interaction was found to cause the release of calcium ions within the cell, which encouraged cells to release glutamate, the main excitatory neurotransmitter.
Further, when LPI activated GPR55 on the other side of the synapse, it weakened inhibition, by decreasing the supply and proper arrangement of proteins necessary for inhibition. Collectively, this creates a “dangerous” two-pronged mechanism to increase excitability, say the authors. “We found that LPI triggers aGPR55-dependent dual mechanism to elevate network excitability: a transient elevation in presynaptic excitatory release probability, complemented by a slower sustained reduction of inhibitory synaptic strength,” the investigators stated.
The research team found that LPI-mediated effects on both excitatory and inhibitory synaptic transmission could be blocked either by genetically engineering mice to lack GPR55, or by treating mice with plant-derived CBD prior to seizure-inducing stimuli. While prior studies had implicated GPR55 as a seizure-reducing target of CBD, the current work provided a more detailed, proposed mechanism of action.
The authors propose that CBD blocks a positive feedback loop in which seizures increase LPI-GPR55 signaling, which likely encourages more seizures, which in turn increases levels of both LPI and GPR55. “Our observations suggest a positive feedback loop whereby LPI promotes hyperexcitability, which in turn increases the expression of LPI and GPR55,” they further explained. “We tentatively propose that CBD can extinguish a potentially regenerative loop in which hyperactivity enhances LPI-GPR55 signaling, further shifting the E:I ratio … Our experiments provide new insights on synaptic mechanisms of CBD’s anti-seizure effects.”
The team concluded that CBD could represent a potential therapeutic agent in treatment-resistant epilepsy patients who don’t respond to current drugs, such as benzodiazepines, possibly due to LPI-GPR55 effects.
The proposed vicious cycle also represents one process that could explain repeated epileptic seizures, although future studies are needed to confirm this. Further, the current study examined the plant-based cannabinoid CBD, but the authors note that LPI is part of signaling network that includes endocannabinoids such as 2-Arachidonoylglycerol (2-AG) that occur naturally in human tissues. LPI and 2-AG target receptors also regulated by CBD, but have different actions at the synapse. While LPI amplifies incoming electrical signals, endocannabinoids such as 2-AG respond to increases in brain activity by dialing down the release of neurotransmitters from nerve cells. Interestingly, LPI and 2-AG can be converted into each other through actions of enzymes.
“Theoretically, the brain could control activity by toggling between pro-excitatory LPI and the restorative actions of 2-AG,” said first study author Evan Rosenberg, PhD, a postdoctoral scholar in the Tsein’s lab. “Drug designers could inhibit the enzymes that underpin LPI production or promote its conversion to 2-AG, as an additional approach to control seizures. LPI could also serve as a biomarker of seizures or predictor of clinical responsiveness to CBD, providing an area of future research.”
Susan Weiner, MS, RDN, CDCES, FADCES, talks with Janice Newell Bissex, MS, RDN, FAND, about potential health benefits of cannabis and CBD for diabetes.
It is possible that cannabis may help with blood glucose management, decrease arterial inflammation, improve neuropathy and lower blood pressure, according to Bissex. Navigating the legal and accessibility issues and finding quality guidance are some of the obstacles people face when it comes to cannabinoid therapy for diabetes.
People with diabetes who plan to use cannabis or CBD should work with a provider who understands cannabinoid therapy and start with a low dose with slow, gradual increases.
Weiner:With the legalization in some states of medical and adult use cannabis, and the federal legalization of hemp production, has the use of these products increased among people with diabetes?
Bissex:In an analysis published in 2022 of data from the International Cannabis Policy Study collected in 2018 across Canada and the U.S., researchers found that 27% of people living in North America reported having used medical cannabis to manage pain (53%), reduce anxiety (52%) or improve sleep (46%). Mirroring the general population, use of cannabis and CBD has increased among people with diabetes. A study published in 2020 of findings from the National Survey on Drug Use and Health showed that cannabis use prevalence among adults with diabetes increased 340% from 2005 to 2018. Expanding legalization, decrease in stigma and more awareness of potential benefits have likely contributed to an increase in cannabis and CBD use.
Weiner:Do we know what effects use of these products has on diabetes?
Bissex:Cannabis and CBD interact with the endocannabinoid system, which is involved in lipid and glucose metabolism. CBD targets the body’s G protein-coupled receptors (GPCRs), which are widespread and affect many bodily functions. Most of the medications prescribed for diabetes also target GPCRs.
Inflammation and oxidative stress are factors in the development of and complications from diabetes and other chronic diseases. Cannabinoids found in the cannabis plant have well-documented anti-inflammatory and antioxidant effects. Eating a diet that includes plants, whole grains and healthy fats, managing stress and exercising can also help to keep inflammation and oxidative stress in check.
There are no reports of blood glucose worsening with cannabis use. In fact, an analysis published in 2013 of data from the National Health and Nutrition Examination Survey found that cannabis use is associated with a 16% lower level of fasting insulin and 17% lower insulin resistance. Based on this, it should come as no surprise that cannabis users may have a lower incidence of type 2 diabetes than the general population.
Two of the cannabinoids in the cannabis plant that have been identified as particularly helpful for diabetes are THCv and CBD. In addition, a terpene found in cannabis, beta-caryophyllene, plays a role in lipid and glucose metabolism and has antidiabetic potential.
A 2016 study published in Diabetes Care found that the cannabinoid THCv significantly decreased fasting blood glucose levels. CBD was found to decrease resistin and increase gastric inhibitory polypeptide, which stimulates insulin secretion. Another study, published in 2006, showed that CBD significantly reduced the incidence of diabetes in nonobese diabetic mice (86% vs. 30%). These CBD supplemented mice also displayed a decrease in inflammatory cytokine release.
Weiner:What products are available and how do they differ?
Bissex:Cannabis is most commonly consumed via smoking, vaping, tinctures, capsules and edibles. There are pros and cons to each method. Smoking and vaping provide the fastest relief for severe pain, whereas capsules and edibles are longer lasting with a delayed onset. Tinctures take effect in about 15 minutes and allow for titration of dosing based on how someone is feeling.
As mentioned above, THCv has been shown to decrease fasting blood glucose levels. This cannabinoid is not as commonly found in cannabis products, so searching for a cultivar with higher levels of THCv (such as Doug’s Varin and Durban Poison) will take some research.
CBD may be an easier way to start getting potential benefits for people living with diabetes. There are many CBD companies, but the FDA found that 70% of the CBD products on the market are mislabeled — so buyer beware. Always ask for a certificate of analysis (COA) to make sure what is claimed on the label is actually in the product. I recommend looking for organically grown CBD from the U.S. from a trusted source with someone who can answer questions about appropriate methods of administration and dosing.
There are three types of CBD products to consider. Full-spectrum CBD products contain all the cannabinoids, terpenes and flavonoids in the plant, including THC, the cannabinoid best known for producing the “high.” The maximum amount of THC allowed in hemp CBD products is 0.3%, which is not enough to be intoxicating.
Those who are not comfortable with THC should choose a broad-spectrum product, which contains all the cannabinoids, terpenes and flavonoids in the plant, minus the THC. Isolate CBD contains only the CBD molecule and is not nearly as effective since it lacks the “entourage” or “ensemble” effect — synergy between the components in the plant.
Topical CBD may help with neuropathic pain. One client told me she “woke up with two new feet” after applying a CBD salve before bed.
Weiner:Do these products interact with drugs prescribed to treat diabetes?
Bissex:According to Drugs.com, there are no known interactions between CBD or cannabis and insulin, metformin, glipizide, glimepiride, canagliflozin (Invokana, Janssen), empagliflozin (Jardiance, Boehringer Ingelheim/Eli Lilly) or sitagliptin (Januvia, Merck). Ingestible CBD may interact with medications that are processed by the CYP450 enzyme system, such as warfarin. Using tinctures and topicals will help to avoid the first pass metabolism in the liver to attenuate any risk for interaction.
Weiner:What advice do you give people with diabetes interested in these products?
Bissex:Do your homework and work with a practitioner who understands the science of cannabinoid therapy and can guide you. Always start low and go slow when it comes to dosing. I’ve been to cannabis dispensaries where they’ve recommended a 10 mg THC gummy. This is way too high a dose for anyone not accustomed to using cannabis and would likely cause unwanted side effects, such as rapid heart rate, dry mouth and disorientation. CBD does not cause these uncomfortable side effects, but it is best to start with a low dose.
Exciting research into the potential benefits of CBD and cannabis therapy for diabetes is ongoing. We need more clinical trials to determine the best cannabinoid ratios and dosing. The first step is to legalize this plant to both increase access to cannabis medicine and to allow for more research.
References:
Brook E, et al. Pharmacol Res. 2019;doi:10.1016/j.phrs.2019.01.009.
Danielsson AK, et al. J Diabetes Res. 2016;doi:10.1155/2016/6278709.
Jadoon KA, et al. Diabetes Care. 2016;doi:10.2337/dc16-0650.
Leung J, et al. Psychopharmacology (Berl). 2022;doi:10.1007/s00213-021-06047-8.
Maurya A, et al. Curr Top Med Chem. 2021;doi:10.2174/1568026621666210305102500.
Penner EA, et al. Am J Med. 2013;doi:10.1016/j.amjmed.2013.03.002.
Sexton TR, et al. Drug Alcohol Depend. 2020;doi:10.1016/j.drugalcdep.2020.108035.
Weiss L, et al. Autoimmunity. 2006;doi:10.1080/08916930500356674.
For more information:
Janice Newell Bissex, MS, RDN, FAND, is a holistic cannabis practitioner at Jannabis Wellness and program director of Cannabinoid Medical Sciences at John Patrick University of Health and Applied Sciences in South Bend, Indiana. She can be reached at: jannabiswellness@gmail.com.
Susan Weiner, MS, RDN, CDN, CDCES, FADCES, is co-author of The Complete Diabetes Organizer and Diabetes: 365 Tips for Living Well. She is the owner of Susan Weiner Nutrition PLLC and is the Endocrine Today Diabetes in Real Life column editor. She can be reached at susan@susanweinernutrition.com; Twitter: @susangweiner.
A cancer diagnosis is both devastating and terrifying. Patients are almost always directed towards conventional cancer treatments like surgery, chemotherapy and radiation, and are made to feel that any other, more “natural” treatments are not only ineffective but dangerous.
The truth is, however, that mainstream cancer treatments wreak havoc on the body, leaving it defenseless against disease and breaking it down at the exact time when it needs to be as strong as possible. With its less than impressive success rate of between 2 and 4 percent, along with its devastating effects on the body, it is unsurprising that three out of every four doctors say they would refuse chemotherapy as a treatment option if they themselves became ill.
While doctors like to promote the idea that there are no treatments scientifically proven to work besides the usual surgery/chemotherapy/radiation regimen, the truth is there is a strong body of evidence that many natural, non-invasive treatments are effective in the fight against cancer. One of the most well-researched and solidly proven of all these natural medicines is cannabis.
The miraculous power of cannabinoids
As noted by Dr. Mark Sircus, writing for Green Med Info, there is no confusion about whether marijuana is an effective cancer treatment. Cannabis has been scientifically proven to kill cancer cells without the devastating and body weakening effects of conventional cancer treatments.
The marijuana plant contains about 113 powerful chemical compounds known as cannabinoids. The most well-known of these compounds are tetrahydrocannabinol (THC) – the chemical that induces marijuana’s “high” – and cannabidiol – a non-psychoactive compound which has been extensively studied as a cure for many diseases.
The power of the elements: Discover Colloidal Silver Mouthwash with quality, natural ingredients like Sangre de Drago sap, black walnut hulls, menthol crystals and more. Zero artificial sweeteners, colors or alcohol. Learn more at the Health Ranger Store and help support this news site.
These and other cannabinoids are what make marijuana such a potent anti-cancer treatment, as reported by Green Med Info:
Cannabinoids are found to exert their anti-cancer effects in a number of ways and in a variety of tissues.
Triggering cell death, through a mechanism called apoptosis
Stopping cells from dividing
Preventing new blood vessels from growing into tumors
Reducing the chances of cancer cells spreading through the body, by stopping cells from moving or invading neighboring tissue
Speeding up the cell’s internal ‘waste disposal machine’ – a process known as autophagy – which can lead to cell death
All these effects are thought to be caused by cannabinoids locking onto the CB1 and CB2 cannabinoid receptors. Almost daily we are seeing new or confirming evidence that Cannibinoids can be used to great benefit in cancer treatment of many types.
Scientific studies published in a host of peer-reviewed journals have confirmed marijuana’s powerful ability to fight breast, lung, ovarian, pancreatic, prostate and other cancers.
Scientists are calling for more studies to be done on humans after studying the cancer-fighting effects of chemicals in the drug.
Studies suggest chemicals called phytocannabinoids could stop cancer cells multiplying and spreading, block the blood supply to tumors, and reduce cancer’s ability to survive chemotherapy. …
The new research review admits cannabis has ‘anti-cancer effects’ and says more research needs to be done in real patients to confirm the findings.
It takes real courage to receive a cancer diagnosis and decide not to follow mainstream advice but seek alternative treatments. But even for those who choose to receive conventional cancer treatments like radiation and chemotherapy, cannabis can still be an important part of their overall wellness plan. As Dr. Sircus admonishes, “Every cancer patient and every oncologist should put medical marijuana on their treatment maps.”
A team of Stony Brook University researchers have identified fatty acid binding proteins (FABPs) as intracellular transporters for two ingredients in marijuana, THC and CBD (cannabidiol). The finding, published early online in the Journal of Biological Chemistry, is significant because it helps explain how CBD works within the cells. Recent clinical findings have shown that CBD may help reduce seizures and could be a potential new medicine to treat pediatric treatment-resistant epilepsy.
3D ball and stick molecular model of cannabidiol (CBD)
CBD differs from THC in that it is not psychoactive and does not bind to cannabinoid receptors. Some children who are resistant to conventional antiepileptic drugs have been reported to show improvement with oral CBD treatment. The Stony Brook research team found that three brain FABPs carry THC and CBD from the cell membrane to the interior of the cell. This action enabled them to conduct experiments inhibiting FABPs and thereby reducing anandamide breakdown inside the cells.
“Anandamide, an endocannabinoid, has been shown to have neuroprotective effects against seizures in basic research studies and this may turn out to be a key mechanism of seizure control,” explained Dale Deutsch, PhD, Professor of Biochemistry and Cell Biology and a faculty member of the Institute of Chemical Biology and Drug Discovery at Stony Brook University. “Therefore by CBD inhibiting FABPs, we could potentially raise the levels of anandamide in the brain’s synapses.”
The findings in the paper, titled “Fatty Acid Binding Proteins are Intracellular Carriers for THC and CBD,” stem from the team’s research that spans five years and includes their discoveries that showed anandamide levels were raised in rodent brains using novel drugs targeted to FABPs. In 2013, they received a $3.8 million grant from the National Institute on Drug Abuse, part of the National Institutes of Health (NIH), to target endocannabinoid transporters to develop drugs for pain and inflammation.
The current research involving FABPs as transporters of CBD involves the work of faculty and students from several Stony Brook Departments. The team includes four Professors — Dr. Deutsch, Martin Kaczocha (Anesthesiology), Iwao Ojima (Chemistry and the Institute of Chemical Biology and Drug Discovery), and Stella Tsirka (Pharmacological Sciences). The team also features a post-doctoral fellow (Jeremy Miyauchi in Pharmacological Sciences), a researcher who recently received his PhD (William Berger in Chemistry), a graduate student Matthew Elmes, a research technician Liqun Wang, and undergraduate students Brian Ralph, Kwan-Knok Leung, and Joseph Sweeney, all from the Department of Biochemistry and Cell Biology.