Immunotherapy is among the most promising new treatment modalities to arise over the last two decades; antibody drugs are delivering immunotherapy to millions of patients with many different types of cancer. Initial success with antibody therapeutics came in the form of direct targeting or cytotoxic antibodies, such as rituximab and trastuzumab, which bind directly to tumor cells to elicit their destruction. These were followed by immunomodulatory antibodies that elicit antitumor responses by either stimulating immune cells or relieving tumor-mediated suppression. By far the most successful approach in the clinic to date has been relieving immune suppression, with immune checkpoint blockade now a standard approach in the treatment of many cancer types. Despite equivalent and sometimes even more impressive effects in preclinical models, agonist antibodies designed to stimulate the immune system have lagged behind in their clinical translation. In this review, we document the main receptors that have been targeted by agonist antibodies, consider the various approaches that have been evaluated to date, detail what we have learned, and consider how their anticancer potential can be unlocked.
Hokkaido University scientists and colleagues in Japan have found a way that could help some patients overcome resistance to an immunotherapy treatment for cancer.
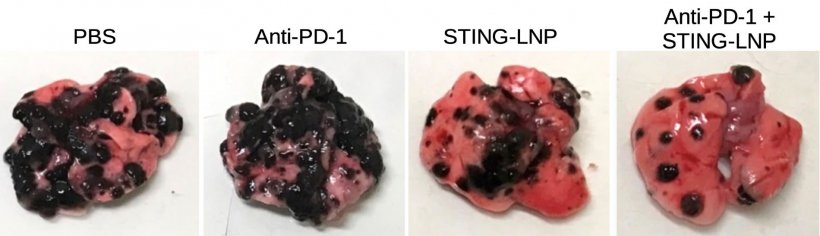
Combination therapy against anti-PD-1-resistant lung cancer. A combination of anti-PD-1 antibodies and stimulator of an interferon gene (STING)-loaded lipid nanoparticles (STING-LNP) had the maximum effect in reducing metastases (black regions) on lungs (pink tissue; far right). STING-lipid nanoparticles alone had a better effect (center right) than anti-PD-1 antibodies (center left), which were as effective as the control saline solution.
The activation of checkpoint proteins on the surfaces of immune cells help regulate the immune response by preventing them from indiscriminately attacking the body’s other cells. But some cancer cells are able to hijack this mechanism, preventing an immune response against them as well. Scientists have recently developed immune checkpoint inhibitors that can counteract this strategy, but some people are resistant to the treatments. Now, scientists at Hokkaido University and Aichi Institute of Technology have found a way around this by developing a specially designed lipid nanoparticle that can carry immunity-triggering molecules into immune cells in the liver called macrophages.
The lipid, called YSK12-C4, has a high affinity for immune cells. When intravenously injected into mice with metastatic melanoma, it was able to deliver signaling molecules, called cyclic dinucleotides, across the cell membranes of their liver macrophages, where they stimulated the production of immune-related proteins called type 1 interferons via a stimulator of an interferon gene (STING) pathway. These were released into the blood, activating another type of immune cell called natural killer cells in the spleen and lung, which produced interferon-gamma inside the lung metastases.
This treatment, on its own, only elicited a mild anti-tumor effect. This is because the type 1 interferons and interferon-gamma triggered the expression of a protein called PD-L1 on the cancer cells. PD-L1 prevents a strong tumor-killing immune response of natural killer cells that express PD-1. Administering an anti-PD-1 immunotherapy treatment, however, prevented the cancer cells from turning off those natural killer cells, which then became armed and able to launch a full-scale attack.
“The findings suggest that our lipid nanoparticles carrying immune-signaling molecules convert the immune status from immunologically cold to immunologically hot,” says Takashi Nakamura of Hokkaido University’s faculty of pharmaceutical sciences. “This could lead to the development of a promising adjuvant that reduces resistance to anti-PD-1 antibody treatment in some cancer patients.” Further studies will need to examine whether the treatment can cause liver toxicity and if different signaling molecules can be used.
However, up to halfTrusted Source of patients with cancer do not respond to ICI treatments. A growing number of studiesTrusted Source show that the gut microbiome may play a role in ICI treatment efficacy.
ResearchTrusted Source shows that mice that lack gut microbiota or that are treated with antibiotics respond less to ICI. StudiesTrusted Source also suggest that replacing microbiota via fecal transplants may increase response from ICI.
It remains unclear which gut bacteria are most effective for increasing ICI response and how gut bacteria improve immune response.
Recently, researchers investigated how gut bacteria diversity influences ICI efficacy in a mouse model of melanoma.
They found that ICI treatment causes inflammation in the digestive system, allowing bacteria to leave the intestines and travel to lymph nodes near tumors, where they activate immune cells.
Dr. Anton Bilchik, surgical oncologist and division chair of general surgery at Providence Saint John’s Health Center and chief of medicine and director of the Gastrointestinal and Hepatobiliary Program at Saint John’s Cancer Institute in Santa Monica, CA, not involved in the study, told Medical News Today:
“Since there is a plethora of research studying the impact of the gut microbiome on the immune system this provides a novel explanation as to how immunotherapy may work outside of the intestinal tract. Furthermore, it shows the deleterious effect that antibiotics may have in reducing the efficacy of immunotherapy by neutralizing bacteria within the gastrointestinal tract.”
For the study, the researchers administered ICI therapy to mice with and without melanoma tumors.
They found that ICI treatment increased inflammation in the digestive tract, which allowed certain bacteria to leave the gut and travel to lymph nodes near the tumor, as well as the tumor site. There, the microbes activated a set of immune cells that killed tumor cells.
The researchers also investigated how antibiotic exposure may affect ICI efficacy. To do so, they treated mice with antibiotics, then implanted them with melanoma tumors and treated them with ICI a week later.
They found that antibiotic exposure reduced gut microbiota movement to lymph nodes, and decreased immune cell levels.
Finally, they investigated whether administering different kinds of bacteria could reverse the effect of the antibiotics on ICI efficacy. They found that treatments with Escherichia coli and Enterococcus faecalis improved ICI efficacy.
MNT spoke with Dr. Andrew Koh, associate professor at the Harold C. Simmons Comprehensive Cancer Center at UT Southwestern, senior author of the current study, about the study’s limitations.
A major limitation, noted Dr. Koh, is that they only used one preclinical cancer model, meaning that further tests are needed to know whether the findings may apply to other cancers, too.
“We believe that our findings could apply to other cancers too, but we have not generated data to support that supposition,” he said.
“There are published dataTrusted Source that different human tumors harbor unique or distinct tumor microbiomes — and many of the predominant taxa are bacteria that typically reside in the gut. So our study may provide a mechanistic link or explanation as to how gut microbiota can travel from the gut and seed different types of human tumors,” added Dr. Koh.
Dr. Guilherme Rabinowits, a hematologist and medical oncologist at Miami Cancer Institute, part of Baptist Health South Florida, not involved in the study, also told MNT that “[i]t is very likely that the findings reported in this study apply to other cancer types, since the gut bacteria translocation is unlikely to be tumor-specific.”
“Unfortunately, without proper testing, it is impossible to say for sure,” he noted.
When asked about other limitations of the study, Dr. Bilchik added that it remains to be seen whether the findings translate to humans.
Dr. Lance Uradomo, an interventional gastroenterologist at City of Hope Orange County Lennar Foundation Cancer Center in Irvine, CA, not involved in the study, also told MNT that “the type of therapy applied for testing melanoma can be linked to adverse side effects, such as colitis.”
“Further study is needed before it is understood if microbiome therapy — and the correct application — is truly effective,” he added.
When asked about the study’s implications, Dr. Koh said that the findings beg the question of whether there may be more direct ways to deliver probiotic treatments to patients than via the intestines.
“Perhaps giving live oral precision probiotics — which are fraught with many logistical challenges, such as maintaining stable engraftment in the human gut, which can easily be derailed by exposure to antibiotics or changes in diet — is not the best way to administer gut microbiota-based therapies,” he noted.
To this end, he noted that his lab is currently developing microbiota-derived therapy that can be administered outside the gastrointestinal tract.
“We hope to submit this story by the end of this year. I have filed two patents and formed a startup company, Aumenta Biosciences, which is developing this technology. Aumenta was awarded its first NIH [National Institutes of Health] grant last year to develop this technology,” he commented.
Checkpoint-blockade immunotherapy has transformed cancer therapeutics but still benefits only a subset of patients. The development of more-robust biomarkers of response could change that.
Immune-checkpoint inhibitors (ICIs) that block the immunoinhibitory receptor PD-1 and its ligand PD-L1 or the immunomodulatory receptor CTLA-4 have had a transformational impact on the care of patients with cancer, offering curative potential for patients who until recently had no suitable therapeutic options. Despite the growing number of regulatory approvals for use of these drugs in a number of different malignancies, it is now becoming clear that many patients who receive ICIs do not benefit from treatment but remain at risk for potentially serious immune-related adverse events. Expanding the benefit of ICIs to more patients and limiting the impact of their adverse effects will require better biomarkers of response and toxicity.
Although high tumor mutational burden (TMB), presence of tumor microsatellite instability (MSI) and mismatch-repair-deficient (dMMR) status, as well as high PD-L1 expression, in tumor cells are well established biomarkers, they are not perfect. For example, some patients with PD-L1-negative tumors do respond to ICI treatment. In the CheckMate 227 trial, the combination of nivolumab (anti-PD-1) plus ipilimumab (anti-CTLA-4) yielded comparable overall survival benefits in patients with non–small-cell lung cancer whose tumors were above or below the PD-L1 expression threshold of 1%. Moreover, differences in defining high PD-L1 and TMB thresholds, as well as variability in sensitivity of detection platforms, can influence patient classification. Notably, TMB estimates have recently been shown to be affected by ancestry, with misclassified TMB-high patients not benefiting from ICI treatment.
The US Food and Drug Administration has also approved specific companion diagnostics to determine TMB-high and MSI-high/dMMR status as tumor-agnostic biomarkers of the response to pembrolizumab (anti-PD-1). Although these tests enable more patients to access this drug, the efficacy of these biomarkers in predicting response varies across different tumor types. Multiple analyses suggest that these biomarkers, at least at particular cut-offs, may not be universally associated with response across tumor types and may not necessarily be generalizable for patients with a specific tumor type, and point to the need for tumor-type-specific composite biomarkers that integrate multiple parameters.
As ICIs are tested for more indications, more trial datasets also exist with the potential to both identify and validate potential determinants of response. However, integrating these data has proven challenging due to heterogeneity in trial inclusion criteria, the types of samples collected, workflows for sampling and data processing, as well as assay selection. Dedicated sites managed by research agencies exist for the deposition of sequencing results, but standardizing these data and obtaining the relevant clinical metadata necessary for useful interpretation can be difficult. Repositories for other types of data commonly generated in ICI trials, such as immunohistochemistry and flow cytometry results, are lacking or not consistently used. The Cancer Immune Monitoring and Analysis Centers–Cancer Immunologic Data Commons (CIMAC-CIDC) Network, which was established by the US National Cancer Institute, is one ongoing partnership aimed at harmonizing methods and big data for potential immunotherapy biomarkers.
In addition to trial-intrinsic differences, restricted access to datasets further complicates biomarker-validation efforts. Although many clinical research journals, including Nature Medicine, require inclusion of data availability or sharing statements in published papers, data access is still often limited and results that are shared may not be fully clinically annotated, which greatly reduces their utility for analysis and validation. For better leveraging of the correlative big data generated in ICI trials, improved strategies must be developed for efficient sharing and harmonization of all major data types while maintaining patient confidentiality. Portals that aggregate trial datasets and permit query-only analysis could be one option.
Numerous other genomic and non-genomic determinants of ICI response have been proposed, and they are often non-redundant. For example, both an intratumoral T cell–inflamed gene-expression profile and TMB have been shown to independently predict the response to pembrolizumab across multiple types of solid tumors. Prospective validation of some of these biomarkers is already underway. In a recent phase 2 trial, patients with advanced soft-tissue sarcomas and intratumoral tertiary lymphoid structures were shown to have better clinical outcomes after pembrolizumab treatment than those of patients without such structures, which suggests that careful selection of patients with tumor types generally considered less responsive to ICIs could actually lead to clinical benefit. Trials such as this one, ideally randomized with direct comparisons to ‘all-comers’ arms, and arms focused on different biomarker combinations, could refine the scope of ICIs while also helping to establish standardized approaches for measuring specific biomarkers.
It is critical that future biomarker-driven trials be thoughtfully designed to maximize the types of correlative data that can be reasonably obtained and analyzed from patient samples, as well as the diversity of the patient population, given the potential effect of ancestry. In particular, determinants of response that are less invasive than tumor-based biomarkers, such as blood TMB and serum IL-8, should be a priority for prospective validation.
The future for ICIs is undeniably bright, with promising recent results in the neoadjuvant setting and for inhibitors of targets beyond PD-1–PD-L1 and CTLA-4, as well as approvals for use in combination with other types of therapy. Intensifying efforts to enhance data standardization, sharing of existing trial datasets, and prospective validation of candidate biomarkers in diverse populations will be crucial for the development of more-effective biomarkers of response to and toxicity of ICIs and to expand the impact of immune-checkpoint-blockade therapies to many more patients with cancer.
Any treatment that uses elements of the body’s immune system to fight cancer is considered cancer immunotherapy. In recent years, as research has revealed many of the basic workings of the immune system and how the immune system interacts with tumor cells, scientists have developed, tested, and demonstrated the effectiveness of an array of immunotherapy techniques, several. Several have shown immense promise in various types of cancer.
There are two general types of immunotherapy: Those that stimulate or “train” the immune system to more effectively target cancer, and those that provide patients with immune system components that help make cancer cells more “visible” to immune cells and more susceptible to attack.
Checkpoint Inhibitors
Over the last decade, new types of immunotherapy, including immune checkpoint inhhibitors, have entered medicine’s arsenal against cancer. They work by releasing the brakes on the immune system’s attack on cancer cells. Such drugs have been shown to be helpful against numerous kinds of cancer, including melanoma skin cancer, non-small cell lung cancer, bladder cancer, kidney cancer, and Hodgkin lymphoma. Researchers are currently testing combinations of checkpoint inhibitors with other drugs, including other types of immunotherapy, to bring these results to patients with other kinds of cancer.
CAR T-Cell Therapy
Another form of immunotherapy that has made headlines in the past few years is CAR T-cell therapy. It works by genetically engineering a patient’s own immune system T cells to better track down and kill cancer cells. Currently, it is approved by the Food and Drug Administration (FDA) for some forms of refractory non-Hodgkin lymphoma as well as pediatric relapsed acute lymphoblastic leukemia (ALL), and is available through clinical trials for other forms of blood cancer.
Vaccines
Vaccines, which consist of substances put into the body to spark an immune response against disease, have recently begun to make their mark against cancer as well. Vaccines to prevent cervical, anal, throat and other cancers linked to infection by the human papilloma virus (HPV) are now a part of standard care for young people.
Vaccines to treat cancer take a variety of forms: Some are made from cancer cells; others, from parts of cancer cells; still others are from specially conditioned immune system cells.
One type of cell-based vaccine involves removing certain immune system cells from a patient’s blood and converting them into dendritic cells, whose job is to display cancer- or infection-related proteins on their surface. The dendritic cells are combined with pieces of tumor cells and, often, other stimulatory proteins and infused back into the patient. The cancer-related antigens on the dendritic cells’ surface spur the patient’s immune system to go on the offensive against cancer cells.
Another approach is constructing a vaccine out of actual cancer cells that have been removed from the patient during surgery. The killed tumor cells are processed in a lab to make them more visible to the immune system, then re-injected into the patient along with immune-stimulating compounds. The patient’s immune system launches a vigorous attack not only on the newly-injected cancer cells but also on similar cells throughout the body.
Monoclonal Antibodies
Among the older types of immunotherapy are monoclonal antibodes, which are lab-made versions of natural immune system proteins that can zero in on specific parts of cancer cells and destroy them. The FDA has approved more than a dozen monoclonal antibodies to treat certain cancers, including some types of leukemia and breast cancer, and others are under study in clinical trials. Agents that yoke antibodies to chemotherapy drugs – producing what are known as conjugate drugs – are designed to deliver a direct hit of chemotherapy to cancer cells and have shown promising results in some cancers, including lymphoma and certain types of breast cancer.
Stem Cell Transplants
Transplants of donor stem cells are a long-proven form of immunotherapy for patients with a blood-related cancer such as leukemia or lymphoma or with certain types of non-cancerous blood disorders. In a transplant, patients are treated with radiation and/or chemotherapy to wipe out the diseased bone marrow or, at lower doses, to suppress cancer cells within the marrow. Patients are then infused with blood-making stem cells from a compatible donor, which migrate to the bone marrow and begin rebuilding the patient’s blood supply. The newly generated blood cells include white blood cells of the immune system that take up the fight against the patient’s cancer cells, a phenomenon known as the graft-versus-leukemia effect.
Stimulating the Immune System
A final category of cancer immunotherapies includes chemicals – many of them natural – that don’t target cancer cells specifically but act as a general stimulant on the immune system, which can invigorate the immune response to cancer. Such substances include cytokines, which are made by some immune system cells to control the growth and activity of other immune system cells; interleukins, a group of cytokines used a signals between white blood cells; and interferons, which help the body resist viral infections and some cancers. Other agents, known as immunomodulating drugs, are thought to work by boosting the immune system, but the mechanism by which they do this isn’t fully understood. Thalidomide is the best-known of these drugs.
Using a new tool for editing genomes, known as CRISPR, researchers have genetically engineered immune cells and improved the ability of these cells to kill cancer cells in mice.
The cells were modified to express proteins on their surfaces called chimeric antigen receptors (CARs), which enabled the cells to recognize and attack cancer cells that expressed the corresponding antigen.
Mesothelin-specific CAR T cells attacking a cancer cell.
In experiments with the mice, immune cells that had been engineered to express CARs using CRISPR were more effective at killing tumor cells than immune cells engineered using conventional methods, the researchers reported in Nature on February 22.
The type of immunotherapy evaluated in the study is CAR T-cell therapy, a form of adoptive cell transfer. With this treatment, a patient’s own T cells, a type of immune cell, are collected from blood, modified genetically to make them better at attacking tumor cells, expanded in the laboratory, and finally returned to the patient.
To explore ways to enhance the effectiveness of CAR T-cell therapies, Michel Sadelain, M.D., Ph.D., of Memorial Sloan Kettering Cancer Center, and his colleagues turned to a technique called CRISPR, which allows researchers to edit genomes with more speed and precision than other approaches.
Creating More Potent T Cells
Conventional approaches for engineering T cells to express a CAR, such as using a retrovirus to deliver the gene, result in the gene being inserted at random locations in the genome.
With these approaches, however, there is a chance that the CAR gene could insert itself in a way that disrupts the normal functioning of the genome, causing unintended consequences, the study authors noted.
By contrast, the CRISPR/Cas9 system allows for the specific placement of genes. Dr. Sadelain and his colleagues used CRISPR to deliver a CAR gene to a precise location in the T-cell genome: the T-cell receptor alpha chain (TRAC) gene.
The TRAC region of the genome includes the gene for the T-cell receptor, which helps the immune cell detect foreign molecules. The CRISPR system edits out part of the TRAC gene in the T cells, allowing the CAR gene to insert there.
When the researchers tested the two kinds of CAR T cells in mouse models of leukemia, those in which the CAR gene had been inserted at the TRAC locus via CRISPR were more effective at destroying tumor cells than those in which it was inserted randomly with a retrovirus.
Experiments suggested that the improved anti-tumor responses of cells engineered using CRISPR was the result, in part, of the “highly regulated CAR expression” in these T cells, noted Dr. Sadelain.
Overcoming “Exhaustion”
In addition, the CAR T cells created with CRISPR were less likely to stop recognizing and attacking tumor cells after a certain time point, a phenomenon researchers call “exhaustion.”
“We found that the level of CAR expression [on T cells] and the dynamic response of the CAR following the recognition of antigens are critical in determining whether exhaustion will occur rapidly,” explained Dr. Sadelain. “Expressing the CAR from the TRAC locus greatly diminished exhaustion, resulting in superior tumor eradication.”
Based on three measures of exhaustion, less than 2% of CRISPR-created T cells showed signs of exhaustion, compared with up to half of conventionally engineered CAR T cells.
“This report describing the use of CRISPR/Cas9 technology to insert a CAR gene into a specific location in the genome is an important advance for the CAR field,” said James N. Kochenderfer, M.D., who develops and tests T-cell therapies in NCI’s Center for Cancer Research (CCR) and was not involved in the study.
“The finding that the location of CAR gene insertion can affect T-cell function is particularly intriguing,” Dr. Kochenderfer continued. “New gene-editing technologies will likely lead to rapid improvement in antigen-targeted T-cell immunotherapies for cancer.”
Looking Ahead
In an accompanying editorial, Marcela V. Maus, M.D., Ph.D., of Harvard Medical School identified three important improvements that CRISPR could potentially bring to T-cell-based therapies, one being more-effective tumor responses.
Second, the targeted nature of CRISPR-mediated CAR integration into the genome might “prove safer than random integration, which carries the potential risk of generating a harmful mutation,” Dr. Maus wrote.
Finally, this approach might “enable off-the-shelf CAR T cells to be made that need not come from a patient’s own T cells,” she continued. “This would enable easier and cheaper manufacture of CAR T cells.”
At Memorial Sloan Kettering, Dr. Sadelain’s team has been modifying its manufacturing techniques to prepare for clinical testing in the future. The researchers believe their findings could have implications for research on diseases other than cancer.
“The biology of CARs still has many secrets and surprises to reveal,” Dr. Sadelain said, adding: “Research on CARs will lead to more effective and safer therapies for a number of diseases.”
A new step in cancer immunotherapy: researchers from the Netherlands Cancer Institute and University of Oslo/Oslo University Hospital show that even if one’s own immune cells cannot recognize and fight their tumors, someone else’s immune cells might. Their proof of principle study is published in the journal Science on May 19th.
The study shows that adding mutated DNA from cancer cells into immune stimulating cells from healthy donors create an immune response in the healthy immune cells. Inserting the targeted components from the donor immune cells back into the immune cells of the cancer patients, the researchers were able to make cancer patients’ own immune cells recognize cancer cells.
The extremely rapidly developing field of cancer immunotherapy aims to create technologies that help the body’s own immune system to fight cancer. There are a number of possible causes that can prevent the immune system from controlling cancer cells. First, the activity of immune cells is controlled by many ‘brakes’ that can interfere with their function, and therapies that inactivate these brakes are now being tested in many human cancers. As a second reason, in some patients the immune system may not recognize the cancer cells as aberrant in the first place. As such, helping the immune system to better recognize cancer cells is one of the main focuses in cancer immunotherapy.
Ton Schumacher of the Netherlands Cancer Institute and Johanna Olweus of the University of Oslo and Oslo University Hospital decided to test whether a ‘borrowed immune system‘ could “see” the cancer cells of the patient as aberrant. The recognition of aberrant cells is carried out by immune cells called T cells. All T cells in our body scan the surface of other cells, including cancer cells, to check whether they display any protein fragments on their surface that should not be there. Upon recognition of such foreign protein fragments, T cells kill the aberrant cells. As cancer cells harbor faulty proteins, they can also display foreign protein fragments – also known as neoantigens – on their surface, much in the way virus-infected cells express fragments of viral proteins.
Outsourcing cancer immunity – arming patient immune cells with immune receptors from healthy donors to attack cancer. Credit: Ellen Tenstad, Science Shaped
To address whether the T cells of a patient react to all the foreign protein fragments on cancer cells, the research teams first mapped all possible neoantigens on the surface of melanoma cells from three different patients. In all 3 patients, the cancer cells seemed to display a large number of different neoantigens. But when the researchers tried to match these to the T cells derived from within the patient’s tumors, most of these aberrant protein fragments on the tumor cells went unnoticed.
Next, they tested whether the same neoantigens could be seen by T-cells derived from healthy volunteers. Strikingly, these donor-derived T cells could detect a significant number of neoantigens that had not been seen by the patients’ T cells.
“In a way, our findings show that the immune response in cancer patients can be strengthened; there is more on the cancer cells that makes them foreign that we can exploit. One way we consider doing this is finding the right donor T cells to match these neoantigens.”, says Ton Schumacher. “The receptor that is used by these donor T-cells can then be used to genetically modify the patient’s own T cells so these will be able to detect the cancer cells”.
“Our study shows that the principle of outsourcing cancer immunity to a donor is sound. However, more work needs to be done before patients can benefit from this discovery. Thus, we need to find ways to enhance the throughput. We are currently exploring high-throughput methods to identify the neoantigens that the T cells can “see” on the cancer and isolate the responding cells. But the results showing that we can obtain cancer-specific immunity from the blood of healthy individuals are already very promising”, says Johanna Olweus.
The number of anticancer immunotherapeutics approved by the U.S. Food and Drug Administration (FDA) is risingrapidly. In fact, the four anticancer immunotherapeutics approved by the FDA in the 12 months covered by the recently released AACR Cancer Progress Report 2015—Aug. 1, 2014, to July 31, 2015—was the greatest number of anticancer immunotherapeutics approved by the agency in any 12-month period to date.
Much of the media attention has focused on FDA-approved anticancer immunotherapeutics like pembrolizumab (Keytruda) and nivolumab (Opdivo), which are referred to as checkpoint inhibitors. As I have explained in a previouspost on this blog, these agents work by releasing brakes on immune cells called T cells, which have the natural potential to recognize and eliminate cancer cells. Research has shown, however, that triggering brakes on T cells is just one way in which tumors can evade destruction by the immune system.
A study just published in the AACR journal Clinical Cancer Research reported results of a phase I clinical trial in which researchers investigated targeting another mechanism by which tumors are thought to avoid cancer-fighting T cells. Specifically, the researchers sought to eliminate cells—called Treg cells—that can inhibit anticancer immune responses.
What are Treg cells and why are they a potential target for cancer treatment?
Regulatory T cells, so-called Treg cells, are a subset of T cells that are defined by expression of two proteins, CD4 and FoxP3. These cells are critical for keeping other immune cells in check; they help prevent the immune system from attacking normal cells and tissues, causing autoimmune disorders.
Preclinical studies have shown that Tregs can also prevent the immune system from attacking tumors and clinical research has shown that these cells accumulate in the tumors of some patients with cancer. These observations led to the idea that eliminating Tregs in patients with cancer might unleash the natural potential of the patient’s cancer-fighting T cells, and to several clinical trials testing this hypothesis.
The Clinical Cancer Research study
In the phase Ia clinical trial reported in Clinical Cancer Research, the researchers evaluated whether using a therapeutic antibody called KW-0761 (mogamulizumab), which targets the protein CCR4, would eliminate Tregs in the blood of patients with lung or esophageal cancer. KW-0761 has been approved in Japan for the treatment of relapsed or refractory adult T-cell leukemia/lymphoma.
Dr. Ueda.
One of the senior authors on the paper, Ryuzo Ueda, MD, PhD, professor in the Department of Tumor Immunology at Aichi Medical College in Nagoya, Japan, explained in a news release that they used KW-0761 because activated FoxP3+CD4+ Tregs that accumulate in tumor tissue have been shown to express CCR4 molecules on their surface.
The research team enrolled seven patients with non–small cell lung cancer and three patients with esophageal cancer in the clinical trial. After analyzing blood samples obtained before the first treatment with KW-0761 and then every four weeks, they found that the number of FoxP3+CD4+ Tregs in the blood of all patients was dramatically reduced following treatment with KW-0761.
There were no dose-limiting toxicities and most adverse events were grade 1 or grade 2, with skin-related adverse events occurring most frequently.
Dr. Nakayama.
“We were pleased to see that infusion of even a small amount of the KW-0761 efficiently depleted Tregs from the peripheral blood for a long time [several months],” said the co-senior author on the study, Eiichi Nakayama, MD, PhD, a professor at Kawasaki University of Medical Welfare in Kurashiki, Japan. “Unfortunately, we observed only a modest induction of antitumor immune responses and no marked clinical responses with KW-0761 monotherapy.”
What happens next?
Nakayama explained that the research team is planning to investigate whether combining Treg depletion with other immunotherapies, such as checkpoint inhibitors, can augment the antitumor immune response in patients with cancer.
However, the authors of a commentary published in Clinical Cancer Research in June 2015 emphasize that we still have much to learn about the role of Tregs in the initiation, development, and progression of different cancer types. They note that some studies point to these cells as not always being “bad guys,” and potentially even helping prevent cancer from developing in some cases by keeping in check inflammation, which can drive cancer initiation.
The number of anticancer immunotherapeutics approved by the U.S. Food and Drug Administration (FDA) is risingrapidly. In fact, the four anticancer immunotherapeutics approved by the FDA in the 12 months covered by the recently released AACR Cancer Progress Report 2015—Aug. 1, 2014, to July 31, 2015—was the greatest number of anticancer immunotherapeutics approved by the agency in any 12-month period to date.
Much of the media attention has focused on FDA-approved anticancer immunotherapeutics like pembrolizumab (Keytruda) and nivolumab (Opdivo), which are referred to as checkpoint inhibitors. As I have explained in a previouspost on this blog, these agents work by releasing brakes on immune cells called T cells, which have the natural potential to recognize and eliminate cancer cells. Research has shown, however, that triggering brakes on T cells is just one way in which tumors can evade destruction by the immune system.
A study just published in the AACR journal Clinical Cancer Research reported results of a phase I clinical trial in which researchers investigated targeting another mechanism by which tumors are thought to avoid cancer-fighting T cells. Specifically, the researchers sought to eliminate cells—called Treg cells—that can inhibit anticancer immune responses.
What are Treg cells and why are they a potential target for cancer treatment?
Regulatory T cells, so-called Treg cells, are a subset of T cells that are defined by expression of two proteins, CD4 and FoxP3. These cells are critical for keeping other immune cells in check; they help prevent the immune system from attacking normal cells and tissues, causing autoimmune disorders.
Preclinical studies have shown that Tregs can also prevent the immune system from attacking tumors and clinical research has shown that these cells accumulate in the tumors of some patients with cancer. These observations led to the idea that eliminating Tregs in patients with cancer might unleash the natural potential of the patient’s cancer-fighting T cells, and to several clinical trials testing this hypothesis.
The Clinical Cancer Research study
In the phase Ia clinical trial reported in Clinical Cancer Research, the researchers evaluated whether using a therapeutic antibody called KW-0761 (mogamulizumab), which targets the protein CCR4, would eliminate Tregs in the blood of patients with lung or esophageal cancer. KW-0761 has been approved in Japan for the treatment of relapsed or refractory adult T-cell leukemia/lymphoma.
Dr. Ueda.
One of the senior authors on the paper, Ryuzo Ueda, MD, PhD, professor in the Department of Tumor Immunology at Aichi Medical College in Nagoya, Japan, explained in a news release that they used KW-0761 because activated FoxP3+CD4+ Tregs that accumulate in tumor tissue have been shown to express CCR4 molecules on their surface.
The research team enrolled seven patients with non–small cell lung cancer and three patients with esophageal cancer in the clinical trial. After analyzing blood samples obtained before the first treatment with KW-0761 and then every four weeks, they found that the number of FoxP3+CD4+ Tregs in the blood of all patients was dramatically reduced following treatment with KW-0761.
There were no dose-limiting toxicities and most adverse events were grade 1 or grade 2, with skin-related adverse events occurring most frequently.
Dr. Nakayama.
“We were pleased to see that infusion of even a small amount of the KW-0761 efficiently depleted Tregs from the peripheral blood for a long time [several months],” said the co-senior author on the study, Eiichi Nakayama, MD, PhD, a professor at Kawasaki University of Medical Welfare in Kurashiki, Japan. “Unfortunately, we observed only a modest induction of antitumor immune responses and no marked clinical responses with KW-0761 monotherapy.”
What happens next?
Nakayama explained that the research team is planning to investigate whether combining Treg depletion with other immunotherapies, such as checkpoint inhibitors, can augment the antitumor immune response in patients with cancer.
However, the authors of a commentary published in Clinical Cancer Research in June 2015 emphasize that we still have much to learn about the role of Tregs in the initiation, development, and progression of different cancer types. They note that some studies point to these cells as not always being “bad guys,” and potentially even helping prevent cancer from developing in some cases by keeping in check inflammation, which can drive cancer initiation.
After mapping out the molecular mechanisms of T-cell antigen recognition, regulation, and function in the 1980s and 1990s, immunologist James P. Allison hypothesized that blocking negative immune regulators (checkpoints) would give the human immune system the power to fight cancer. His testing of this hypothesis in preclinical models led to the clinical development of a new generation of active agents for cancer treatment. In some subgroups of patients, unleashing native immune-system cells to fight cancer now provides a realistic chance of long-term remission. For this seminal work, Allison, a professor at the M.D. Anderson Cancer Center in Houston, has won the 2015 Lasker–DeBakey Clinical Medical Research Award, announced on September 8.
It had been known for more than a century that occasionally when there was evidence that a patient’s immune system had attacked a metastatic cancer, a long-lasting remission occurred. But for a long time, although scientists were aware of the immune system’s role, they had no mechanistic understanding of why the immune system worked in a particular patient and why the immune responses could not reliably be repeated. Recognizing the great success of vaccines in preventing infectious diseases, cancer researchers tested multiple vaccines made up of inactivated cancer cells and tried injecting infectious agents into tumors, with the hope of activating the immune system against the cancer. But evidence of clinical responses to these approaches was mostly anecdotal.
Knowledge of immune-system regulation improved over time and led to the testing of recombinant cytokines, such as interferons and interleukin-2, for activating the immune system against cancer. With these agents, tumor responses became more reproducible and sometimes durable, but they were infrequent (achieved in 5 to 10% of patients) and occurred in very few types of cancers, such as melanoma and renal-cell carcinoma.
Nevertheless, these initial clinical experiences showed that immunotherapy had potential in cancer treatment. Further progress would hinge on an understanding of how immune-system cells recognize cancer cells and are regulated to kill them. In his early scientific career, Allison made important contributions to elucidating the rules of T-cell activation, including defining the structure of the T-cell receptor (TCR) that specifically recognizes antigens1 and demonstrating that the T-cell molecule CD28 provides costimulatory signals necessary for full T-cell activation.2 The TCR and the CD28 molecule are the molecular basis of what we know as immunologic signal 1 (TCR recognition of antigens) and immunologic signal 2 (costimulation), respectively. Both are required to license T cells to specifically kill their target cells T-cell Activation in the Lymph Node.).
But solving the puzzle of how an immune response can lead to the eradication of cancer also required understanding how the immune system is specifically activated by certain antigens mostly foreign to the body, rather than by endogenous antigens. Allison then described the inhibitory function of the checkpoint molecule cytotoxic T-lymphocyte–associated protein 4 (CTLA-4), which blocks immunologic signal 2 and thereby prevents T cells from becoming fully activated. In a series of studies in preclinical models, he demonstrated that blocking CTLA-4 with therapeutic antibodies could unleash an immune response against cancer (Figure 1B).3 With these studies, Allison shifted the paradigm from attempting to activate the immune system (i.e., vaccinating) to releasing the checkpoints that keep it in a negative regulatory mode.
Checkpoint-blockade immunotherapy has arguably been the most exciting advance made in cancer treatment in recent years. High on the list of scientific achievements in the fight against cancer, it has joined the ranks of radical surgery, radiation therapy, chemotherapy, endocrine therapy, and targeted oncogene therapies. Blockade of CTLA-4 with the monoclonal antibody ipilimumab was the first treatment to improve overall survival in patients with metastatic melanoma and has gained worldwide approval for the treatment of that cancer. Further insights into the release of immune inhibitory checkpoints led to the strategy of “releasing” the programmed cell death 1 (PD-1) receptor on T lymphocytes, from which cancer cells protect themselves by expressing the PD-1 ligand 1 (PD-L1).
T-cell Activation in Tumor Milieu.).4 Antibodies blocking PD-1 or PD-L1 are in clinical development for the treatment of more than 30 types of cancer, and pembrolizumab and nivolumab, two antibodies blocking PD-1, have gained approval for the treatment of metastatic melanoma and lung carcinoma. Combining CTLA-4 and PD-1 blockade provides even higher response rates than either approach alone in patients with advanced melanoma,5highlighting the potential of combination immunotherapy based on blocking immune checkpoints to push the limits of what the immune system can achieve.
In the history of cancer treatment, there will be a full chapter dedicated to unleashing the immune system by releasing its negative regulatory checkpoints. That chapter will start with the seminal studies by Allison involving blocking CTLA-4 in mouse models. As the successful clinical development of ipilimumab and PD-1 and PD-L1 blocking antibodies has shown, Allison’s early insight was correct: “What we needed to do was to release the brakes of the immune system to fight cancer.” The obvious risk as we push the limits of this approach to cancer treatment is the appearance of autoimmune side effects, which can be serious. But by learning how to safely utilize combinations of immune activators and checkpoint inhibitors, we should be able to expand the potential of immunotherapy for cancer.