Literature review highlights benefits, although access is an issue, expert says
Hyperbaric oxygen therapy (HBOT) can help heal bowel fistulas in patients with advanced Crohn’s disease, according to a systematic review and meta-analysis.
Overall, use of HBOT was associated with a 87% clinical response rate for all fistula subtypes, with more than half of the patients achieving clinical remission, or closure of the fistula and complete cessation of drainage, according to Amr Dokmak, MD, of Catholic Medical Center in Manchester, New Hampshire.
“With a pooled overall clinical response rate of 87% and a low adverse event [AE] rate, our review emphasizes the potential clinical benefit and safety of adjunctive hyperbaric oxygen therapy in refractory cases of fistulizing Crohn’s disease,” Dokmak and colleagues stated in their abstract.
However, the analysis was limited by the heterogeneity of the studies and lack of control groups so “randomized control trials [RCT] are needed to substantiate the benefit of hyperbaric oxygen therapy in fistulizing Crohn’s disease,” Dokmak stated.
Syed Adeel Hassan, MD, of the University of Kentucky in Lexington, told MedPage Today that “treating fistulizing disease is very daunting for physicians because usually the only treatment is surgery. Our goal as physicians is to try to treat patients to prevent these fistulas — basically holes in the bowel — from occurring in the first place.”
“Hyperbaric oxygen therapy has been used for a variety of conditions, including things like infections, and this study indicates it can be useful in cases of refractory fistulizing Crohn’s disease,” added Hassan, who was not involved in the study.
He agreed that an RCT would be important to sort out exactly how useful HBOT could be. Hassan also noted that in many parts of the world, including his native Pakistan, access to HBOT devices was sorely limited.
And “the researchers need to look into the mechanisms of action as to why hyperbaric oxygen would benefit these patients,” Hassan suggested.
Dokmak’s group considered data sufficient for their analysis if outcomes were measured clinically, radiologically, or endoscopically. Of the 16 studies, there were four single-case reports, and the largest study had 37 patients who averaged 30.2 HBOT sessions each, they reported.
Among 12 studies (single-case reports excluded), clinical response was reported among 131 of 160 patients; clinical remission was reported in 83 of 139 cases in 10 studies.
The researchers also analyzed outcomes based on the type of fistula. They reported that in 15 studies, the clinical response was seen in 115 of 130 patients diagnosed with perianal fistulas, and that in 13 studies, clinical remission was achieved in 68 of 113 patients with perianal fistulas. In 13 studies where patients who had undergone J-pouch surgery were excluded, the rate of clinical response was seen in 89 of 100 cases, while clinical remissions was observed in 50 of 83 cases (n=11 studies).
Among patients who were diagnosed with enterocutaneous fistulas, clinical response was observed in 21 of 25 cases (n=5 studies) while clinical remission was observed in 14 of 19 cases (n=4 studies).
And among patients who were diagnosed with rectovaginal fistulas, clinical response and remission were seen in four of 14 cases (n=5 studies). Dokmak noted that “rectovaginal fistulas were the fistula type least responsive to hyperbaric oxygen therapy.”
The overall clinical response was 89%, 84%, and 29% for perianal, enterocutaneous, and rectovaginal fistulas, respectively, according to the researchers.
They looked at clinical response rates based on whether patients were treated in the biologic or pre-biologic setting, but there were no significant differences in the time analysis, except for patients with rectovaginal fistula who appeared to do better in the pre-biologic era with a 52% clinical response rate and a 25% response rate in the biologic era.
The pooled number of AEs was low at about 51 per 10,000 HBOT sessions, with aural barotraumaopens in a new tab or window as the most reported AE, according to Dokmak and colleagues
Niacin (vitamin B3) is a biomolecule required by all forms of life. It functions as a precursor to NAD, an enzymatic co-factor in hundreds of metabolic pathways. Niacin is called a vitamin because the body can only synthesize it slowly and therefore requires a small but adequate amount from the diet. The reason that we cannot synthesize adequate amounts of niacin can be traced back to evolutionary pressure. Over millions of years, niacin was readily available from plant- and animal-based foods, so our bodies have evolved to rely on this dietary source. However, larger amounts of niacin than the minimum required by the body are helpful because they allow our metabolic pathways to function at full speed for optimal health and to prevent disease. Some individuals are dependent upon high levels of niacin for health because of their genetic background or because of severe stress. For these individuals, much higher doses of niacin than the minimum dose can prevent and reverse disease. And for the rest of us, high doses of niacin are beneficial — and even necessary — for many aspects of health.
This new expanded edition nearly doubles the original Niacin: The Real Story, (from 228 to now 490 pages). It has several new chapters and appendices and more than 600 references to document recent advances in scientific knowledge about niacin. Several chapters focus on the different forms of the molecule niacin, how it works, safety of niacin supplements, and how to take niacin supplements. Other chapters describe how niacin can help to prevent and reverse a variety of diseases and other conditions, including arthritis, ADHD, many forms of mental illness, cardiovascular disease, aging, alcoholism, Alzheimer’s, cancer, cholera, Huntingdon’s disease, migraine, multiple sclerosis, nephritis (kidney inflammation), Parkinsonism, PTSD, Raynaud’s disease, and a variety of skin conditions. There is a special chapter focused on the recent COVID-19 pandemic: how niacin can help the body recover from infection and reduce the risk of “Long COVID.”
A major focus of the book is how niacin supplements, along with adequate doses of all the other essential nutrients (vitamins and minerals) and a healthy diet that avoids sugar and processed foods, can prevent and even reverse a variety of diseases. This orthomolecular theme is developed in the chapter “Pandeficiency Disease.” This theme is based on avoiding deficiencies of vitamins and minerals that contribute to a wide variety of conditions. Some vitamins are needed only in small milligram or microgram daily doses, but others such as vitamin C and niacin are needed in much higher doses, depending on the body’s state of stress, inflammation, and disease. The optimal dose varies with the individual and the state of inflammation and disease because biochemical stress in the body can deplete vitamin and cause deficiencies — which in turn can cause many different types of disease.
The book contains several interesting and significant new sections and chapters. The chapter entitled “Reversing Arthritis with Niacinamide” has been expanded, now including some of Dr. Kaufman’s notes and a memoir written up as his final unpublished paper. Niacin: The Real Story is the only book in print to present Kaufman’s own case notes and niacinamide protocol details. In these new sections, Dr. Kaufman documents his discovery of niacin and niacinamide treatments during his medical education, along with his observations of the nutritional deficiencies in the typical diet that caused pellagra (caused by a severe deficiency of niacin) and that also tended to cause osteoarthritis.
Many of the patients in the early years of his practice in the 1940s were referred by other physicians who wanted to get rid of their most complaining and difficult patients. At the time, the only treatments for arthritis were aspirin, hot paraffin dips, or heat treatment of joints. With his careful observations of symptomatology, Kaufman realized that most had a niacin deficiency — and these symptoms are summarized in detail. He explains that he soon found that most of these patients had a deficiency of niacin in their diets — proven by rapid improvement after niacinamide treatment. He reported that he treated all his patients with kindness, respect, and adequate doses of niacinamide — and soon after starting niacinamide treatment with up to 2000 mg or more per day, taken in divided doses, the patients “became easy to take care of medically” and had “astonishing improvements in their health.” Kaufman took their complaints seriously and found that a niacin deficiency was independent of family income. Well-to-do families could afford a nutritionally good diet, even if they did not do so.
Although by 1940 enriched flour was fortified with thiamine, niacin, riboflavin and iron, Kaufman realized that for most individuals, the doses of these essential nutrients from foods made with enriched flour were inadequate. So his treatment with adequate doses of niacinamide became more widely appreciated and soon his practice was full. Patients recovered with a “high degree of wellness and maintained this as long as they continued taking niacinamide.”
The new section on Erectile Dysfunction may interest many readers. Adequate doses of niacin taken long-term can help to prevent atherosclerosis, hyperlipidemia, and related coronary disease, and it also is a vasodilator. Because niacin (but not niacinamide) normalizes blood lipids, its long-term circulatory benefits may facilitate a male’s erection. While the vasodilation produced by niacin is not as long as produced by ED drugs, the niacin flush typically lasts about half an hour. But since niacin also helps to improve mood and possibly sexual interest, generally the sense of calmness from a goodly dose of niacin may tend to diminish passion. In a related topic, adequate doses of niacin and the consequential flush that dilates blood vessels have been employed by people to ameliorate Raynaud’s syndrome (cold hands and feet due to reduced blood flow).
There are several new Appendices, including “An Interview with Abram Hoffer, MD, PhD.” Hoffer, a brilliant doctor and scientist, explains that he successfully treated thousands of schizophrenia patients with niacin. He also had excellent success treating depression, and showed that niacin lowered total cholesterol. Hoffer then explains that niacin is not dangerous or toxic at tolerable doses, and that adequate doses of vitamins (in particular, niacin) produce a recovery rate of 90 percent in schizophrenics.
Niacin is a vitamin, not a drug. Each individual may require a different daily dose. Dr. Hoffer says: “A person’s upper limit is that amount which causes nausea, and, if not reduced, vomiting. The dose should never be allowed to remain at this upper limit. The usual dose range is up to 3,000 mg daily, divided into three doses, but occasionally some patients may need more. The toxic dose for dogs is about 5,000 milligrams per 2.2 pounds (1 kilogram) body weight. We do not know the toxic dose for humans since niacin has never killed anyone.” But what about that “niacin flush”? “Most people flush when they first start taking high doses and gradually get adapted to it, unless they stop for a few days and then resume. A few cannot ever get used to it and take no-flush niacin. The intensity of the flush is variable. Generally the people who need it the most flush the least. That includes arthritics, schizophrenics, and elderly people with cardiovascular disease. Some schizophrenics do not flush until they get well — and then they do. But the presence of the flush or its intensity can not be uniquely used measure the need as there are too many variables such as food in the stomach, whether the drink with it is hot or cold, the kind of food, other medication. Antipsychotics reduce the intensity of the flush as do aspirin and antihistamines.”
In this revised edition of Niacin: The Real Story, authors Hoffer, Foster, and Saul clearly present the practical details of niacin treatment. Inevitable physician skepticism, and questions about niacin’s proven safety and effectiveness, are thoroughly addressed in this book. However, this is NOT a biochemistry textbook — to most of us, that is a relief. But since even a basic working knowledge of niacin can profoundly improve the health of so many patients, this vitamin becomes very interesting very quickly.
The book provides vitamin dose protocols and a chapter on safety of niacin, to assist you in learning the proper doses along with supplements of other vitamins and minerals. It explains that by taking niacin at appropriate daily doses, you can prevent and reverse osteoarthritis (the most common form), elevated cholesterol and cardiovascular disease, and several types of mental illness including schizophrenia. You can determine the correct dose by starting at a very low dose, 20 mg (milligrams) per day, and then gradually increasing the dose over several weeks up to 1000 mg/day or more in divided doses. The skin flush that comes with taking a large niacin dose gradually disappears over several weeks. The flush can be avoided by replacing the niacin dose with niacinamide — but this doesn’t help to correct high cholesterol as does niacin.
Scientists cannot always differentiate between research abstracts generated by the AI ChatGPT and those written by human
An artificial-intelligence (AI) chatbot can write such convincing fake research-paper abstracts that scientists are often unable to spot them, according to a preprint posted on the bioRxiv server in late December1. Researchers are divided over the implications for science.
“I am very worried,” says Sandra Wachter, who studies technology and regulation at the University of Oxford, UK, and was not involved in the research. “If we’re now in a situation where the experts are not able to determine what’s true or not, we lose the middleman that we desperately need to guide us through complicated topics,” she adds.
The chatbot, ChatGPT, creates realistic and intelligent-sounding text in response to user prompts. It is a ‘large language model’, a system based on neural networks that learn to perform a task by digesting huge amounts of existing human-generated text. Software company OpenAI, based in San Francisco, California, released the tool on 30 November, and it is free to use.
Since its release, researchers have been grappling with the ethical issues surrounding its use, because much of its output can be difficult to distinguish from human-written text. Scientists have published a preprint2 and an editorial3 written by ChatGPT. Now, a group led by Catherine Gao at Northwestern University in Chicago, Illinois, has used ChatGPT to generate artificial research-paper abstracts to test whether scientists can spot them.
The researchers asked the chatbot to write 50 medical-research abstracts based on a selection published in JAMA, The New England Journal of Medicine, The BMJ, The Lancet and Nature Medicine. They then compared these with the original abstracts by running them through a plagiarism detector and an AI-output detector, and they asked a group of medical researchers to spot the fabricated abstracts.
Under the radar
The ChatGPT-generated abstracts sailed through the plagiarism checker: the median originality score was 100%, which indicates that no plagiarism was detected. The AI-output detector spotted 66% the generated abstracts. But the human reviewers didn’t do much better: they correctly identified only 68% of the generated abstracts and 86% of the genuine abstracts. They incorrectly identified 32% of the generated abstracts as being real and 14% of the genuine abstracts as being generated.
“ChatGPT writes believable scientific abstracts,” say Gao and colleagues in the preprint. “The boundaries of ethical and acceptable use of large language models to help scientific writing remain to be determined.”
Wachter says that, if scientists can’t determine whether research is true, there could be “dire consequences”. As well as being problematic for researchers, who could be pulled down flawed routes of investigation, because the research they are reading has been fabricated, there are “implications for society at large because scientific research plays such a huge role in our society”. For example, it could mean that research-informed policy decisions are incorrect, she adds.
But Arvind Narayanan, a computer scientist at Princeton University in New Jersey, says: “It is unlikely that any serious scientist will use ChatGPT to generate abstracts.” He adds that whether generated abstracts can be detected is “irrelevant”. “The question is whether the tool can generate an abstract that is accurate and compelling. It can’t, and so the upside of using ChatGPT is minuscule, and the downside is significant,” he says.
Irene Solaiman, who researches the social impact of AI at Hugging Face, an AI company with headquarters in New York and Paris, has fears about any reliance on large language models for scientific thinking. “These models are trained on past information and social and scientific progress can often come from thinking, or being open to thinking, differently from the past,” she adds.
The authors suggest that those evaluating scientific communications, such as research papers and conference proceedings, should put policies in place to stamp out the use of AI-generated texts. If institutions choose to allow use of the technology in certain cases, they should establish clear rules around disclosure. Earlier this month, the Fortieth International Conference on Machine Learning, a large AI conference that will be held in Honolulu, Hawaii, in July, announced that it has banned papers written by ChatGPT and other AI language tools.
Solaiman adds that in fields where fake information can endanger people’s safety, such as medicine, journals may have to take a more rigorous approach to verifying information as accurate.
Narayanan says that the solutions to these issues should not focus on the chatbot itself, “but rather the perverse incentives that lead to this behaviour, such as universities conducting hiring and promotion reviews by counting papers with no regard to their quality or impact”.
The BCG vaccine might assist in preventing a range of major diseases
Packing ampoules of the BCG (bacillus Calmette-Guérin) vaccine for tuberculosis in 1931.
The bacillus Calmette-Guérin vaccine against tuberculosis—or simply BCG—is the oldest vaccine in the world that is still currently in use. Millions of infants in Africa and Asia receive the inoculation each year.
The vaccine provides effective protection against tuberculosis (TB), a leading cause of infectious disease deaths worldwide, second only to COVID. Its development began in Lille, France in 1900, when Albert Calmette, an army physician, was working with Camille Guérin, a veterinarian, to understand how TB was transmitted. The team cultured TB bacteria on potato slices and found that after several passages of the microbes from one slice to a fresh one, they became less virulent over time. The researchers started to vaccinate calves with this live, weakened form of TB to protect cattle. By 1921, after 231 passages, the TB strain was stable and nonvirulent for all animals they tested it on.
At the time, French children born in a family in which someone had TB faced a 25 percent chance of dying from the disease within their first year of life. So in 1921 Calmette and Guérin gave the first dose of BCG to a child born into a family with TB, and the child survived. In 1924 a large clinical trial of more than 5,000 French children showed that the BCG vaccine had 93 percent efficacy in preventing death in the first year of life. As a result, it was widely adopted in France and around the world. Different countries developed different strains of the vaccine over time.
In the midst of this progress against TB, something unexpected happened. It was discovered that BCG seemed to furnish benefits beyond protection against TB deaths. A 1927 trial in very young Swedish children showed that BCG reduced early-life mortality by 1931, and the benefit could not be explained by just the reduction in TB deaths. The researcher who reported these results, Carl Naeslund, suggested that BCG might trigger some “nonspecific” immunity—meaning that it protected against other causes of death, too, through unknown means.
In the ensuing century since the vaccine was first developed, laboratory-based immunological studies, epidemiological surveys and clinical trials have documented that these nonspecific effects appear to be real and robust. Other live vaccines, such as the measles vaccine, also show nonspecific effects, though the best-studied ones are for BCG.
Beyond protecting against various infections, researchers are starting to find that the BCG vaccine can also modulate the risk of other diseases in which the immune system goes awry, including type 1 diabetes, cancer, multiple sclerosis and Alzheimer’s disease. Claims about such broad-ranging effects have been controversial but have grown less so in recent years. Open questions still linger, however, as to which patient groups, and for which conditions, the nonspecific effects of BCG might produce a meaningful clinical benefit.
More clinical trials are needed to address these questions, although there has been limited funding and little to no pharmaceutical interest because the vaccine’s patent expired long ago. From a basic science perspective, researchers are also striving to elucidate the mechanisms by which the BCG vaccine works with an eye to using this knowledge to build better vaccines that could confer broad-based immunity.
In October and November 2022, two conferences brought together researchers and policy makers to explore how to better harness BCG’s nonspecific effects for clinical benefit—and to evaluate whether there is sufficient evidence to recommend policy changes to the schedules of vaccinations for children.
One piece of evidence that spurred the current enthusiasm for BCG’s nonspecific effects came from threeclinicaltrials of the BCG vaccine—in 2011, 2012 and 2017—that were conducted by Danish physician-epidemiologist Christine Stabell Benn, anthropologist Peter Aaby and their colleagues. They found that BCG given at birth to children from Guinea-Bissau with low birth weight reduced all-cause mortality in these children by about 40 percent in the first year of life. The reduction in mortality was the result of fewer cases of non-TB infections, which the vaccine protected against in an undetermined way.
In the past two decades, evidence has surfaced that BCG’s nonspecific effects could modulate the risk of a variety conditions that involve the immune system, including type 1 diabetes, cancer, Alzheimer’s and multiple sclerosis. For example, clinician-scientist Denise Faustman and her colleagues performed a clinical trial at Massachusetts General Hospital demonstrating that three doses of BCG can improve blood sugar control in patients with type 1 diabetes, although the effect takes a couple of years to become manifest. Now she is working to understand how BCG affects the immune cells in these patients.
Some compelling longterm data about BCG’s impact on diabetes risk comes from a 2022 epidemiological study by Marie-Claude Rousseau of the National Institute of Scientific Research in Quebec and her colleagues. The researchers used records from Canada’s national health registry to track people who had received the BCG vaccine as children in the 1970s. They found that early-life BCG vaccination did not reduce the risk of diabetes in adolescence, but by the time those children were adults older than age 30, their risk of type 1 diabetes was 35 percent lower than that of people who had not received BCG in early life.
BCG also seems to diminish the risk of cancer. A 60-year follow-up of a clinical trial that began in 1935 among Native American and Alaska Native school-aged children showed that the group that had received BCG in childhood had not only a reduced risk of TB in the ensuing 60 years but also a 2.5-fold lower incidence of lung cancer at the end of the follow-up period. (The original trial, whose first results were published in 1952, was conducted by U.S. Army physician Joseph Aronson. The retrospective record review, from 1992 to 1998, was conducted by his granddaughter Naomi Aronson, director of infectious diseases at the Uniformed Services University in Bethesda, Md. The follow-up study was published in 2019.)
Adding to the growing body of research, an intriguing 2019 study by Hervé Bercovier of the Hebrew University of Jerusalem and his colleagues showed that bladder cancer patients who were treated with BCG in the bladder—a Food and Drug Administration–approved immunotherapy for this type of cancer—had a more than fourfold lower risk of developing Alzheimer’s than those who did not receive the vaccine during a follow-up period of about eight years. Alzheimer’s is challenging to study because of the long time course over which the disease progresses. Still, Jeff Cirillo, an immunologistat Texas A&M University, is conducting a two-year trial to see if BCG vaccination can alter the “cognitive trajectory” of patients with very early-stage Alzheimer’s.
BCG also came into the public eye during the COVID pandemic. Researchers worldwide investigated whether BCG’s nonspecific effects might be harnessed to protect against the disease as a stopgap measure before COVID vaccines became available. The results were mixed, in part, because the trials were done with different strains of the vaccine and in different populations. The trials that showed some efficacy were mostly done in vulnerable populations, such as people with type 1 diabetes or hospitalized elderly patients, whereas the trials that didn’t demonstrate any effect were done in healthy populations, such as health care workers, Faustman explains, who pivoted her trial of BCG’s effects on type 1 diabetes during the pandemic to study the vaccine’s possible protective effects against COVID.
“The way I see the evidence, BCG reduces the risk of new infections in vulnerable groups,” Stabell Benn says. For those with a well-functioning immune system, there is likely little benefit from BCG, but for vulnerable groups, the vaccine can make a difference. It also seems that several doses are needed, she adds.
Mihai Netea, an immunologist and infectious disease clinician who heads the division of experimental medicine at the department of internal medicine at Radboud University Medical Center in the Netherlands, says that BCG hasn’t helped reduce the number of COVID infections, but the evidence suggests that it could reduce disease severity. In a meta-analysis that he, Stabell Benn and Aaby published in Lancet Infectious Diseaseson the effects of live vaccines against COVID, they found that across five trials, there was a 40 percent reduction in overall mortality in those who received BCG, compared with those who did not.
Netea envisions that by deconstructing how BCG actually works, the scientific community could design vaccines that provide better protection than BCG for emerging infectious diseases and a whole host of other conditions, including cancer. “What we should do now is actually build new vaccines in which the nonspecific … protection can reach not 30 or 40 percent but 60 or 70 percent,” he says. “Then, at the next pandemic, we will have something which is on the shelf that can already protect 60 to 70 percent of the population against mortality,” he says, emphasizing the importance of figuring out how BCG actually changes the immune system.
“To me, it is very important to understand, ‘How does it work?’” concurs Maziar Divangahi, a pulmonary immunologist at the McGill International TB Center. Without the mechanism, these nonspecific effects are a “magical” phenomenon. But by figuring out the mechanism, “we could harness the power of that mechanism to advance health in general,” he says.
Broadly speaking, the immune system has two branches: the innate immune system, which provides a first response against infection, and the adaptive immune system, which takes longer to activate and is aimed at specific targets, or antigens. Vaccines typically work by activating the adaptive immune system’s T and B cells and triggering, in the latter, the production of antibodies to a specific antigen such as the spike protein of the coronavirus that causes COVID.
Previously, researchers thought that the generalized response of the innate immune system was optimized for a rapid defense against infection and kept no persistent memory of an invading pathogen. But what Netea and others have shown over the past decade is that the innate immune system is capable of remembering previous encounters and if this system has prior exposure to the BCG vaccines, the next meeting with an invasive pathogen will trigger an enhanced response, such as the production of more signaling molecules called cytokines that attack microbial invaders.
Netea and his colleagues have worked over the past decade to understand this phenomenon, which they call “trained immunity.” They have shown that BCG vaccination causes metabolic changes in immune cells such as monocytes and macrophages, which in turn alter either the placement or removal of chemical, or “epigenetic,” marks on DNA through processes known as methylation and acetylation. These marks serve as bookmarks for immune-related genes in the innate immune system and enhance the monocytes’ production of cytokines when challenged with an infection. “What BCG is doing is putting an epigenetic bookmark in your DNA. So when you need to read it, you already have the bookmark, and the book opens automatically at the right page,” Netea says.
The researchers found that the BCG vaccine does not only affect the epigenetic marks in circulating innate immune cells such as relatively short-lived macrophages, which provide protection by consuming viruses or other invaders. It also alters marks on the DNA in stem cells in the bone marrow that produce new immune cells, which could explain how the effect of the vaccine can persist for many years.
The body of evidence on BCG’s off-target effects is substantial enough now that researchers and policy makers recently convened a workshop in Alexandria, Va., on October 15, 2022, and a meeting in Denmark on November 9–11, 2022, to discuss how to bring this science to bear on public health policy and to optimize the use of the vaccine in public health settings. “If we wanted to be sure that we have the perfect information,” Stabell Benn says, “we will never get going. So this is about finding that cutoff, where you can start and say, ‘We know enough now to move to policy and be reasonably sure that this policy will really truly benefit most of the recipients.’”
Still, the idea of using BCG’s nonspecific effects to treat or prevent a whole host of diseases is not universally accepted. “I’ve never come across a topic that is more polarizing,” says Nigel Curtis, a pediatric infectious diseases physician and BCG researcher at the University of Melbourne and Murdoch Children’s Research Institute in Australia, who calls himself an “agnostic” on the issue of off-target effects. Although there is no question that live vaccines—in particular, BCG—have immune effects beyond their main target, “the bit that remains controversial is to what extent those changes in the immune system are translated to clinically apparent effects,” he explains. In other words, in which populations, and for which conditions, can these off-target effects meaningfully help patients?
In Stabell Benn’s view, sufficient evidence has accumulated for life-saving policy changes to be implemented for some uses. First, in low-income countries where neo-natal mortality is high, BCG should be given at birth rather than months later. Many African countries already vaccinate children with BCG. But only 50 percent of those children receive the vaccine within the first month of life, when they are extremely vulnerable to other infections. Because BCG is given for TB, and children rarely die of TB in the first few months of life, “there’s no incentive for vaccination programs to improve the coverage early on in life,” Stabell Benn explains. But her clinical trials in Guinea-Bissau have shown that receiving the vaccine at birth, rather than months later, can reduce neonatal mortality by about a third. “So you can see that [if you are] coming too late with the vaccine after the neonatal period, the first month of life, you lose a lot of potential for doing a lot of good,” she says.
“My dream would be that we repurpose BCG as a vaccine against neonatal mortality [rather than specifically TB] because that would be a policy change that would really change how it is being used,” she says. Neonatal mortality remains high in Africa, even as child mortality has declined. “So if you can intervene there [in the first month of life], it means many more lives saved in absolute numbers.”
In North America, Europe and Australia, TB is less of a concern, but the vaccine could still be of interest because of its potential to reduce the risk of diabetes, cancer, Alzheimer’s, allergic diseases and other conditions. Both Stabell Benn and Curtis have conducted clinical trials in Denmark and Australia, respectively, showing that BCG vaccination at birth reduces the risk of eczema—especially in babies who are predisposed to the condition because one or both of their parents had it. But before BCG could be recommended as a way to reduce the risk of eczema in babies, regulatory and practical obstacles would have to be overcome. Regulatory agencies would have to review the evidence and approve BCG for a new condition. Also, the vaccine would have to become broadly available, which is not the case in North America, Europe or Australia.
Because BCG is not protected by a patent—a dose would cost about six cents—pharmaceutical companies are not gearing up to conduct the necessary trials to obtain regulatory approval for such use of the vaccine. “The challenges that we face are not really scientific,” says Jaykumar Menon, chair and co-founder of the Open Source Pharma Foundation, a nonprofit attempting to develop affordable therapeutics. “It’s a story of market failure.”
A solution might begin by gaining better insight into the mechanisms of BCG’s off-target effects. Then pharmaceutical companies could improve on the existing vaccine to create a new one for which they would then be able seek patents, Netea says. His group has identified some of the chemical components on the cell wall of BCG that induces trained immunity and developed a nanoparticle on whose surface the BCG-derived components could be placed. The researchers have already shown that the nanoparticle could stimulate trained immunity in animal experiments. Netea envisions that the patentable nanoparticle technology could be the basis for a wholly new vaccine for treating cancer patients—a population in which using the BCG vaccine is usually too risky because such patients are immunosuppressed and might be put at risk by receiving a vaccine made from weakened tuberculosis bacteria. (Bladder cancer is an exception. To treat this type of cancer, BCG is injected into the bladder rather than the bloodstream, and it is evacuated with the urine, so it poses a low risk of infections.)
The “holy grail” of the research that scientists in this area are conducting is not just to understand how vaccines have these effects, Curtis says, but also to use that understanding to design better vaccines and compounds that would target specific conditions, from diabetes to cancer.
Reports that the James Webb Space Telescope killed the reigning cosmological model turn out to have been exaggerated. But astronomers still have much to learn from distant galaxies glimpsed by Webb.
The Webb telescope has spotted galaxies surprisingly far away in space and deep in the past. These four, studied by a team called JADES, are all seen as they appeared less than 500 million years after the Big Bang.
Introduction
The cracks in cosmology were supposed to take a while to appear. But when the James Webb Space Telescope (JWST) opened its lens last spring, extremely distant yet very bright galaxies immediately shone into the telescope’s field of view. “They were just so stupidly bright, and they just stood out,” said Rohan Naidu, an astronomer at the Massachusetts Institute of Technology.
The galaxies’ apparent distances from Earth suggested that they formed much earlier in the history of the universe than anyone anticipated. (The farther away something is, the longer ago its light flared forth.) Doubts swirled, but in December, astronomers confirmed that some of the galaxies are indeed as distant, and therefore as primordial, as they seem. The earliest of those confirmed galaxies shed its light 330 million years after the Big Bang, making it the new record-holder for the earliest known structure in the universe. That galaxy was rather dim, but other candidates loosely pegged to the same time period were already shining bright, meaning they were potentially humongous.
How could stars ignite inside superheated clouds of gas so soon after the Big Bang? How could they hastily weave themselves into such huge gravitationally bound structures? Finding such big, bright, early galaxies seems akin to finding a fossilized rabbit in Precambrian strata. “There are no big things at early times. It takes a while to get to big things,” said Mike Boylan-Kolchin, a theoretical physicist at the University of Texas, Austin.
Astronomers began asking whether the profusion of early big things defies the current understanding of the cosmos. Some researchers and media outlets claimed that the telescope’s observations were breaking the standard model of cosmology — a well-tested set of equations called the lambda cold dark matter, or ΛCDM, model — thrillingly pointing to new cosmic ingredients or governing laws. It has since become clear, however, that the ΛCDM model is resilient. Instead of forcing researchers to rewrite the rules of cosmology, the JWST findings have astronomers rethinking how galaxies are made, especially in the cosmic beginning. The telescope has not yet broken cosmology, but that doesn’t mean the case of the too-early galaxies will turn out to be anything but epochal.
Simpler Times
To see why the detection of very early, bright galaxies is surprising, it helps to understand what cosmologists know — or think they know — about the universe.
After the Big Bang, the infant universe began cooling off. Within a few million years, the roiling plasma that filled space settled down, and electrons, protons and neutrons combined into atoms, mostly neutral hydrogen. Things were quiet and dark for a period of uncertain duration known as the cosmic dark ages. Then something happened.
Most of the material that flew apart after the Big Bang is made of something we can’t see, called dark matter. It has exerted a powerful influence over the cosmos, especially at first. In the standard picture, cold dark matter (a term that means invisible, slow-moving particles) was flung about the cosmos indiscriminately. In some areas its distribution was denser, and in these regions it began collapsing into clumps. Visible matter, meaning atoms, clustered around the clumps of dark matter. As the atoms cooled off as well, they eventually condensed, and the first stars were born. These new sources of radiation recharged the neutral hydrogen that filled the universe during the so-called epoch of reionization. Through gravity, larger and more complex structures grew, building a vast cosmic web of galaxies.
Astronomers with the CEERS survey, who are using the James Webb Space Telescope to study the early universe, look at a mosaic of images from the telescope in a visualization lab at the University of Texas, Austin.Nolan Zunk/University of Texas at Austin
Introduction
Meanwhile, everything kept flying apart. The astronomer Edwin Hubble figured out in the 1920s that the universe is expanding, and in the late 1990s, his namesake, the Hubble Space Telescope, found evidence that the expansion is accelerating. Think of the universe as a loaf of raisin bread. It starts as a mixture of flour, water, yeast and raisins. When you combine these ingredients, the yeast begins respiring and the loaf begins to rise. The raisins within it — stand-ins for galaxies — stretch further apart from one another as the loaf expands.
The Hubble telescope saw that the loaf is rising ever faster. The raisins are flying apart at a rate that defies their gravitational attraction. This acceleration appears to be driven by the repulsive energy of space itself — so-called dark energy, which is represented by the Greek letter Λ (pronounced “lambda”). Plug values for Λ, cold dark matter, and regular matter and radiation into the equations of Albert Einstein’s general theory of relativity, and you get a model of how the universe evolves. This “lambda cold dark matter” (ΛCDM) model matches almost all observations of the cosmos.
One way to test this picture is by looking at very distant galaxies — equivalent to looking back in time to the first few hundred million years after the tremendous clap that started it all. The cosmos was simpler then, its evolution easier to compare against predictions.
Astronomers first tried to see the earliest structures of the universe using the Hubble telescope in 1995. Over 10 days, Hubble captured 342 exposures of an empty-looking patch of space in the Big Dipper. Astronomers were astonished by the abundance hiding in the inky dark: Hubble could see thousands of galaxies at different distances and stages of development, stretching back to much earlier times than anyone expected. Hubble would go on to find some exceedingly distant galaxies — in 2016, astronomers found its most distant one, called GN-z11, a faint smudge that they dated to 400 million years after the Big Bang.
That was surprisingly early for a galaxy, but it did not cast doubt on the ΛCDM model in part because the galaxy is tiny, with just 1% of the Milky Way’s mass, and in part because it stood alone. Astronomers needed a more powerful telescope to see whether GN-z11 was an oddball or part of a larger population of puzzlingly early galaxies, which could help determine whether we are missing a crucial piece of the ΛCDM recipe.
Unaccountably Distant
That next-generation space telescope, named for former NASA leader James Webb, launched on Christmas Day 2021. As soon as JWST was calibrated, light from early galaxies dripped into its sensitive electronics. Astronomers published a flood of papers describing what they saw.
The James Webb Space Telescope, a joint venture of space agencies in the United States, Europe and Canada that took decades to design, build and test, was launched into space on December 25, 2021.Northrop Grumman
Introduction
Researchers use a version of the Doppler effect to gauge the distances of objects. This is similar to figuring out the location of an ambulance based on its siren: The siren sounds higher in pitch as it approaches and then lower as it recedes. The farther away a galaxy is, the faster it moves away from us, and so its light stretches to longer wavelengths and appears redder. The magnitude of this “redshift” is expressed as z, where a given value for z tells you how long an object’s light must have traveled to reach us.
One of the first papers on JWST data came from Naidu, the MIT astronomer, and his colleagues, whose search algorithm flagged a galaxy that seemed inexplicably bright and unaccountably distant. Naidu dubbed it GLASS-z13, indicating its apparent distance at a redshift of 13 — further away than anything seen before. (The galaxy’s redshift was later revised down to 12.4, and it was renamed GLASS-z12.) Other astronomers working on the various sets of JWST observations were reporting redshift values from 11 to 20, including one galaxy called CEERS-1749 or CR2-z17-1, whose light appears to have left it 13.7 billion years ago, just 220 million years after the Big Bang — barely an eyeblink after the beginning of cosmic time.
These putative detections suggested that the neat story known as ΛCDM might be incomplete. Somehow, galaxies grew huge right away. “In the early universe, you don’t expect to see massive galaxies. They haven’t had time to form that many stars, and they haven’t merged together,” said Chris Lovell, an astrophysicist at the University of Portsmouth in England. Indeed, in a study published in November, researchers analyzed computer simulations of universes governed by the ΛCDM model and found that JWST’s early, bright galaxies were an order of magnitude heavier than the ones that formed concurrently in the simulations.
Some astronomers and media outlets claimed that JWST was breaking cosmology, but not everyone was convinced. One problem is that ΛCDM’s predictions aren’t always clear-cut. While dark matter and dark energy are simple, visible matter has complex interactions and behaviors, and nobody knows exactly what went down in the first years after the Big Bang; those frenetic early times must be approximated in computer simulations. The other problem is that it’s hard to tell exactly how far away galaxies are.
In the months since the first papers, the ages of some of the alleged high-redshift galaxies have been reconsidered. Some were demoted to later stages of cosmic evolution because of updated telescope calibrations. CEERS-1749 is found in a region of the sky containing a cluster of galaxies whose light was emitted 12.4 billion years ago, and Naidu says it’s possible the galaxy is actually part of this cluster — a nearer interloper that might be filled with dust that makes it appear more redshifted than it is. According to Naidu, CEERS-1749 is weird no matter how far away it is. “It would be a new type of galaxy that we did not know of: a very low-mass, tiny galaxy that has somehow built up a lot of dust in it, which is something we traditionally do not expect,” he said. “There might just be these new types of objects that are confounding our searches for the very distant galaxies.”
The Lyman Break
Everyone knew that the most definitive distance estimates would require JWST’s most powerful capability.
JWST not only observes starlight through photometry, or measuring brightness, but also through spectroscopy, or measuring the light’s wavelengths. If a photometric observation is like a picture of a face in a crowd, then a spectroscopic observation is like a DNA test that can tell an individual’s family history. Naidu and others who found large early galaxies measured redshift using brightness-derived measurements — essentially looking at faces in the crowd using a really good camera. That method is far from airtight. (At a January meeting of the American Astronomical Society, astronomers quipped that maybe half of the early galaxies observed with photometry alone will turn out to be accurately measured.)
But in early December, cosmologists announced that they had combined both methods for four galaxies. The JWST Advanced Deep Extragalactic Survey (JADES) team searched for galaxies whose infrared light spectrum abruptly cuts off at a critical wavelength known as the Lyman break. This break occurs because hydrogen floating in the space between galaxies absorbs light. Because of the continuing expansion of the universe — the ever-rising raisin loaf — the light of distant galaxies is shifted, so the wavelength of that abrupt break shifts too. When a galaxy’s light appears to drop off at longer wavelengths, it is more distant. JADES identified spectra with redshifts up to 13.2, meaning the galaxy’s light was emitted 13.4 billion years ago.
As soon as the data was downlinked, JADES researchers began “freaking out” in a shared Slack group, according to Kevin Hainline, an astronomer at the University of Arizona. “It was like, ‘Oh my God, oh my God, we did it we did it we did it!’” he said. “These spectra are just the beginning of what I think is going to be astronomy-changing science.”
Brant Robertson, a JADES astronomer at the University of California, Santa Cruz, says the findings show that the early universe changed rapidly in its first billion years, with galaxies evolving 10 times quicker than they do today. It’s similar to how “a hummingbird is a small creature,” he said, “but its heart beats so quickly that it is living kind of a different life than other creatures. The heartbeat of these galaxies is happening on a much more rapid timescale than something the size of the Milky Way.”
But were their hearts beating too fast for ΛCDM to explain?
Theoretical Possibilities
As astronomers and the public gaped at JWST images, researchers started working behind the scenes to determine whether the galaxies blinking into our view really upend ΛCDM or just help nail down the numbers we should plug into its equations.
One important yet poorly understood number concerns the masses of the earliest galaxies. Cosmologists try to determine their masses in order to tell whether they match ΛCDM’s predicted timeline of galaxy growth.
A galaxy’s mass is derived from its brightness. But Megan Donahue, an astrophysicist at Michigan State University, says that at best, the relationship between mass and brightness is an educated guess, based on assumptions gleaned from known stars and well-studied galaxies.
One key assumption is that stars always form within a certain statistical range of masses, called the initial mass function (IMF). This IMF parameter is crucial for gleaning a galaxy’s mass from measurements of its brightness, because hot, blue, heavy stars produce more light, while the majority of a galaxy’s mass is typically locked up in cool, red, small stars.
But it’s possible that the IMF was different in the early universe. If so, JWST’s early galaxies might not be as heavy as their brightness suggests; they might be bright but light. This possibility causes headaches, because changing this basic input to the ΛCDM model could give you almost any answer you want. Lovell says some astronomers consider fiddling with the IMF “the domain of the wicked.”
Introduction
“If we don’t understand the initial mass function, then understanding galaxies at high redshift is really a challenge,” said Wendy Freedman, an astrophysicist at the University of Chicago. Her team is working on observations and computer simulations that will help pin down the IMF in different environments.
Over the course of the fall, many experts came to suspect that tweaks to the IMF and other factors could be enough to square the very ancient galaxies lighting upon JWST’s instruments with ΛCDM. “I think it’s actually more likely that we can accommodate these observations within the standard paradigm,” said Rachel Somerville, an astrophysicist at the Flatiron Institute (which, like Quanta Magazine, is funded by the Simons Foundation). In that case, she said, “what we learn is: How fast can [dark matter] halos collect the gas? How fast can we make the gas cool off and get dense, and make stars? Maybe that happens faster in the early universe; maybe the gas is denser; maybe somehow it is flowing in faster. I think we’re still learning about those processes.”
Somerville also studies the possibility that black holes interfered with the baby cosmos. Astronomers have noticed a few glowing supermassive black holes at a redshift of 6 or 7, about a billion years after the Big Bang. It is hard to conceive of how, by that time, stars could have formed, died and then collapsed into black holes that ate everything surrounding them and began spewing radiation.
But if there are black holes inside the putative early galaxies, that could explain why the galaxies seem so bright, even if they’re not actually very massive, Somerville said.
Confirmation that ΛCDM can accommodate at least some of JWST’s early galaxies arrived the day before Christmas. Astronomers led by Benjamin Keller at the University of Memphis checked a handful of major supercomputer simulations of ΛCDM universes and found that the simulations could produce galaxies as heavy as the four that were spectroscopically studied by the JADES team. (These four are, notably, smaller and dimmer than other purported early galaxies such as GLASS-z12.) In the team’s analysis, all the simulations yielded galaxies the size of the JADES findings at a redshift of 10. One simulation could create such galaxies at a redshift of 13, the same as what JADES saw, and two others could build the galaxies at an even higher redshift. None of the JADES galaxies was in tension with the current ΛCDM paradigm, Keller and colleagues reported on the preprint server arxiv.org on December 24.
Though they lack the heft to break the prevailing cosmological model, the JADES galaxies have other special characteristics. Hainline said their stars seem unpolluted by metals from previously exploded stars. This could mean they are Population III stars — the avidly sought first generation of stars to ever ignite — and that they may be contributing to the reionization of the universe. If this is true, then JWST has already peered back to the mysterious period when the universe was set on its present course.
Extraordinary Evidence
Spectroscopic confirmation of additional early galaxies could come this spring, depending on how JWST’s time allocation committee divvies things up. An observing campaign called WDEEP will specifically search for galaxies from less than 300 million years after the Big Bang. As researchers confirm more galaxies’ distances and get better at estimating their masses, they’ll help settle ΛCDM’s fate.
Many other observations are already underway that could change the picture for ΛCDM. Freedman, who is studying the initial mass function, was up at 1 a.m. one night downloading JWST data on variable stars that she uses as “standard candles” for measuring distances and ages. Those measurements could help shake out another potential problem with ΛCDM, known as the Hubble tension. The problem is that the universe currently seems to be expanding faster than ΛCDM predicts for a 13.8-billion-year-old universe. Cosmologists have plenty of possible explanations. Perhaps, some cosmologists speculate, the density of the dark energy that’s accelerating the expansion of the universe is not constant, as in ΛCDM, but changes over time. Changing the expansion history of the universe might not only resolve the Hubble tension but also revise calculations of the age of the universe at a given redshift. JWST might be seeing an early galaxy as it appeared, say, 500 million years after the Big Bang rather than 300 million. Then even the heaviest putative early galaxies in JWST’s mirrors would have had plenty of time to coalesce, says Somerville.
Astronomers run out of superlatives when they talk about JWST’s early galaxy results. They pepper their conversations with laughter, expletives and exclamations, even as they remind themselves of Carl Sagan’s adage, however overused, that extraordinary claims require extraordinary evidence. They can’t wait to get their hands on more images and spectra, which will help them hone or tweak their models. “Those are the best problems,” said Boylan-Kolchin, “because no matter what you get, the answer is interesting.”
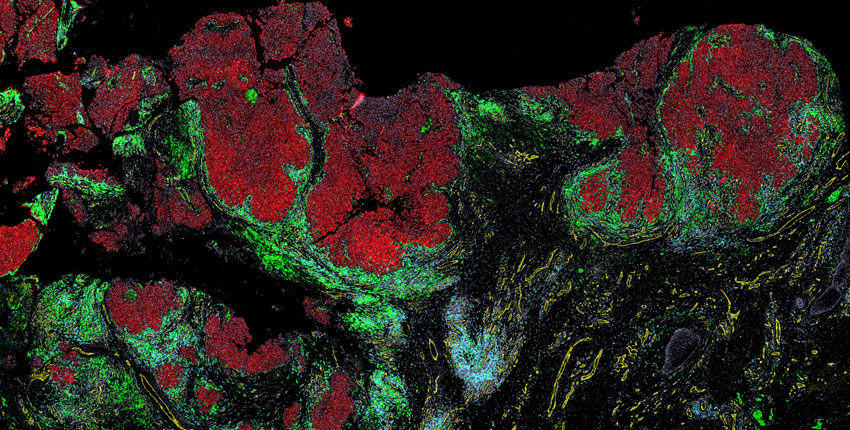
Spatial maps of melanoma reveal how individual cells interact as cancer progresses
Invasive melanoma cells (red) surrounded by two types of immune cells: myeloid cells (green) and T cells (blue). In this case, the immune cells are unable to infiltrate the tumor and kill the cancer cells.
Melanoma is a somewhat unusual cancer—one that blooms before our very eyes, often on sun-exposed skin, and can quickly become deadly as it turns our own skin against us and spreads to other organs.
Fortunately, when caught early, melanoma can often be cured by simple surgery, and there are now better treatments for advanced cases, including immunotherapies that prime a patient’s immune system to fight off the cancer.
However, much remains unknown about melanoma, including the details of how it develops in the earliest stages, and how to best identify and treat the most dangerous early cases.
Now, a team at Harvard Medical School has created spatial maps at the single-cell level that reveal, in unprecedented detail, how melanoma cells and nearby cells, including immune cells, interact as a tumor develops.
The maps, described in Cancer Discovery, offer insights into how interactions between cells change as melanoma advances, and how cancer cells suppress the immune system as they take over.
“The main purpose was to understand the early events in melanoma that lead to the development of a tumor,” said lead author Ajit Nirmal, a research fellow at Harvard Medical School.
The HMS team is building the maps into a melanoma atlas that will be freely available to the scientific community as part of the National Cancer Institute’s Human Tumor Atlas Network. They hope that eventually, the atlas can serve as a jumping-off point for scientists to study how to prevent melanoma and how to treat it in its nascent stages before it becomes full-blown cancer. The ultimate goal of these efforts is to aid doctors in diagnosing melanoma and to help them prescribe tailored treatment based on each patient’s individual tumor profile.
“This was an opportunity to study melanoma at its inception, and collect a resource of information that we can share with the community,” said Sandro Santagata, an HMS associate professor of pathology at Brigham and Women’s Hospital and co-senior author on the paper with Peter Sorger, the HMS Otto Krayer Professor of Systems Pharmacology.
Mapping the unknown
In recent years, a considerable amount of melanoma research has focused on two areas: DNA sequencing of early tumor samples to understand the genetic changes that occur as this particular cancer arises and single-cell RNA sequencing of the tumor’s immediate surroundings—the so-called tumor microenvironment—to profile the types of cells present. However, researchers have remained largely in the dark about how tumor cells and nearby cells are physically arranged in space, and how these cells interact on a molecular level as melanoma develops.
“What we still do not know is how the microenvironment is organized to allow a tumor to grow,” Nirmal said. “In theory, immune cells are supposed to identify tumor cells and kill them off very quickly, but clearly something has gone wrong, and that’s one of the primary reasons why we want spatial resolution.”
Such spatial resolution, along with fine-scale molecular data, became possible to achieve only recently with the advent of more advanced single-cell imaging technologies, including cyclic immunofluorescence, orCyCIF, a multiplexed imaging technique developed by the Sorger lab.
In the new paper, the researchers combined CyCIF imaging data with 3D high-resolution microscopy and fine-scale RNA sequencing to create maps capturing where cells are located and how they interact as normal tissue morphs into melanoma.
“We’re able to see everything from normal skin to early lesions to invasive melanoma, sometimes all in one piece of tissue,” Santagata said. “You end up with this map of how melanoma is developing right in front of you.”
The maps reveal what Santagata describes as “the battle between tumor cells and immune cells” that results in melanoma succumbing when immune cells are victorious, and melanoma progressing when tumor cells win.
Specifically, the maps showed that in the earliest stages of melanoma, so-called precursor lesions were composed of similar types and proportions of cells as normal skin, but these cells had a drastically different pattern of interaction, which included signs of immunosuppression.
“This indicates that there’s probably some level of restructuring within the tumor microenvironment that could potentially aid the development of the tumor,” Nirmal said.
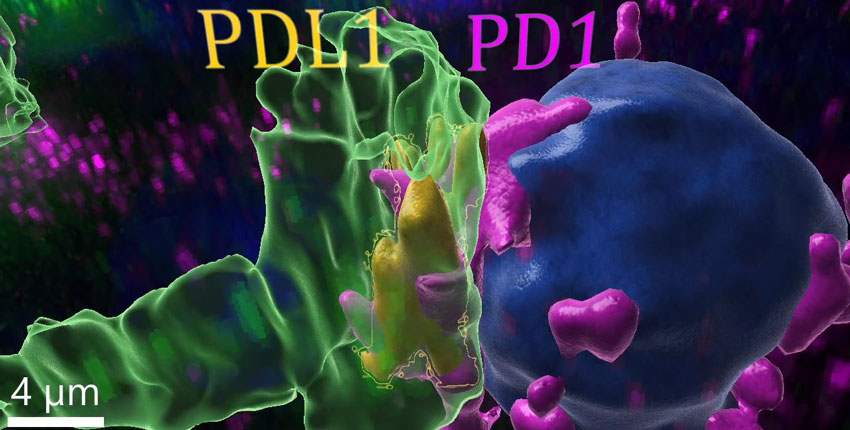
In early melanoma, PD-L1—a protein that suppresses the immune system and allows cancer to flourish—was not expressed in tumor cells but was present in adjacent immune cells called myeloid cells. As the tumor grew, PD-L1-expressing myeloid cells interacted increasingly with T cells primed to kill tumor cells. This interaction between immune cells, rather than between cancer cells and immune cells, may be a mechanism the cancer uses to tamp down the immune system so it can progress unchecked.
“That may mean that the immune system is being suppressed, or inactivated, by itself, and not directly by the cancer,” Sorger said.
A 3D reconstruction of two immune cells—a myeloid cell a killer T cell—interacting. This interaction suppresses the T cell’s ability to destroy cancer cells, thus protecting the tumor from the immune system and allowing it to grow.
Immunotherapies that inhibit PD-L1 and its binding partner PD-1 and thereby unleash the immune system against the tumor have revolutionized treatment for advanced melanoma. However, not all patients with melanoma respond, and these therapies have not been as effective at treating some other cancers. Thus, Sorger hopes that basic research on PD-L1 expression will provide a foundation for understanding which patients with melanoma are most likely to benefit from immunotherapies and how scientists can make the therapies work in more cancers. The insights may also illuminate therapeutic strategies for melanomas that remain resistant to available treatments.
In more advanced melanoma, the state of the cancer cells differed depending on their physical location. Cells in the middle of a tumor that were surrounded by other cancer cells behaved markedly differently from cells on the outer edges of the tumor that could interact with nearby immune cells and stromal cells. This finding suggests that this cellular mixed bag—known as tumor heterogeneity—may partly be due to epigenetic changes that occur in tumor cells as they interact with other cell types, Nirmal said. Understanding tumor heterogeneity is important, he added, for understanding why and how some parts of a tumor survive treatment, while others do not, especially in the context of therapies that target specific molecular pathways.
Zooming out
Taken together, the findings demonstrate that “these local environments involve many more physical interactions between cells than we might have thought,” Sorger said. “The cells are actually in an incredibly dense, communicating network.”
“The neighborhoods of the tumor cells and the interactions between cells tell us how the tumor may progress, and that’s an entirely new form of biomarker that hasn’t been applied before,” Santagata added. “With these new spatial maps, we have the ability to link cellular interactions with physiologic behavior, and, eventually, clinical outcomes.”
We’re able to see everything from normal skin to early lesions to invasive melanoma, sometimes all in one piece of tissue. You end up with this map of how melanoma is developing right in front of you.
Sandro Santagata
HMS associate professor of pathology at Brigham and Women’s Hospital and co-senior author on the paper
With the paper, the researchers are releasing the largest imaging-based melanoma dataset to date—and the entire dataset will be freely available through Minerva, an online visualization tool the lab developed to make complex data easier to understand and use. Now, the team is working on adding more melanoma samples to the project, with the goal of gaining a better understanding of which features and interactions can be considered typical.
“We want to be able to say what happens recurrently, rather than idiosyncratically. Quantity has a quality all its own, and so scaling this is a critical step,” Sorger said.
The researchers are building the maps into an open-source melanoma atlas within the Human Tumor Atlas Network that captures the full range of molecular interactions between cells in different stages of disease. They envision the atlas having a similar impact as earlier atlases of cancer genomics, including The Cancer Genome Atlas. Ultimately, they hope that their work will propel novel insights in melanoma that lead to precision-targeted individualized treatments based on a patient’s tumor characteristics.
“There is no precision medicine without diagnostics,” Sorger said, yet 85 to 90 percent of cancers are diagnosed based on tissue samples alone. He thinks the process of diagnosing and treating melanoma could be improved by incorporating multiplexed imaging techniques, like CyCIF, that provide fine-scale molecular information about the tumor ecosystem and comparing results to a melanoma atlas.
Researchers at Harvard Medical School have combined histology with cutting-edge single-cell imaging technologies to create large-scale 2D and 3D spatial maps of colorectal cancer. The maps layer extensive molecular information on top of histological features to provide new information about the structure of the cancer, as well as how it forms, progresses, and interacts with the immune system.
An overview of colorectal cancer samples used to create 2D and 3D maps.
The maps are part of the team’s broader efforts to create atlases for different cancer types, which will be freely available to the scientific community as part of the National Cancer Institute’s Human Tumor Atlas Network. Previously, the researchers used a similar approach to create in-depth maps of early-stage melanoma, and maps for other cancers are in development. Ultimately, the team hopes that these cancer atlases will propel research and improve diagnosis and treatment.
“Our approach provides a molecular window into 150 years of diagnostic pathology — and reveals that many of the elements and structures traditionally thought to be isolated are actually interconnected in unexpected ways,” said Peter Sorger, PhD, the Otto Krayer Professor of Systems Pharmacology in the Blavatnik Institute at HMS. “An analogy is that before we were just looking at the tail or the foot of the elephant, but now, for the first time, we can start to see the whole elephant at once.” Sorger is co-senior author of the team’s study to map colorectal cancer, which is detailed in Cell, in a paper titled “Multiplexed 3D atlas of state transitions and immune interaction in colorectal cancer.”
Colorectal cancer is relatively slow growing and can often be treated surgically if caught early. However, treatment becomes more difficult if the disease progresses undetected, making it the fourth leading cause of cancer-related deaths in the U.S.
Despite the availability of colorectal cancer screening programs, treatment decisions for individual patients are still largely guided by traditional histology—colorectal cancer is assessed by examining slides of tumor samples under a microscope.
Histology has long been the cornerstone of cancer diagnosis and treatment. Pathologists examine a tumor sample stained with hematoxylin and eosin (H&E) under a microscope and pick out key features to determine the grade and stage of the cancer. This information is used by oncologists to develop a treatment plan, which usually involves some combination of surgery, drugs, and radiation. H&E-based histology is relatively simple, cheap, fast, and can reveal a lot about a tumor.
“Our existing maps of colorectal cancer originate in pathology—over the course of 150 years, we’ve figured out the most important H&E features for diagnosing a patient,” said co-senior author Sandro Santagata, PhD, HMS associate professor of systems biology and associate professor of pathology at Brigham and Women’s Hospital.
A multiplexed image of the colon showing normal cells (left) transitioning into cancer cells (right). The different colors indicate molecular features such as DNA, tumor cells, and immune cells. The researchers hope to study such transitions to learn more about how colorectal cancer forms and progresses.
However, traditional histology has its limits. It doesn’t capture a cancer’s molecular makeup or physical structure, which makes it difficult to fully take advantage of the information cancer researchers have gained over the past 50 years. “Histology is extremely powerful, but we often don’t know what it means in modern molecular terms,” Sorger said. As the authors further pointed out, “ … classical methods provide insufficient information for mechanistic studies and precision medicine … Understanding intra-tumor heterogeneity (ITH) is essential for improving our knowledge of tumor biology and for optimizing diagnosis and therapy.”
Spatial tumor atlases aim to build on this foundation and modern genetic studies, by collecting detailed molecular and morphological information on cells captured in 3D environments. “Atlas construction is made possible by new highly multiplexed tissue imaging methods …” the scientists wrote.
For their newly reported work the team combined histology with single-cell molecular imaging data acquired through a multiplexed imaging technique called cyclic immunofluorescence, or CyCIF. They used this information to create detailed 2D maps of large regions of colorectal cancer. First author Jia-Ren Lin, PhD, platform director in the Laboratory of Systems Pharmacology at HMS, led the effort to stitch these maps together to form a large-scale 3D reconstruction of a tumor. “We use highly multiplexed tissue imaging, 3D reconstruction, spatial statistics, and machine learning to identify cell types and states underlying morphological features of known diagnostic and prognostic significance in colorectal cancer,” the investigators explained. “We show that accurate assessment of disease-relevant tumor structures requires the statistical power of whole-slide imaging (WSI), not the small specimens found in tissue microarrays (TMAs).”
Researchers are combining histological information obtained through traditional pathology (pink and purple) with molecular data acquired through cutting-edge multiplexed imaging (fluorescent green, yellow, red, and blue) to build detailed maps of colorectal cancer.
“Our maps include information on almost 100 million cells from large pieces of tumors, and provide a rather unprecedented look at colorectal cancer,” Santagata said. The maps will allow researchers to start asking key questions about differences between normal and tumor tissues and variation within a tumor, he added, and reveal “exciting architectural features that had never been observed before, as well as molecular changes associated with these features.”
The resulting maps showed that a single tumor can have more and less invasive sections, and more or less malignant-looking regions—resulting in histological and molecular gradients where one part of a tumor transitions into the next. “Within each tumor, there is a wide range of properties of colorectal cancer—we see many different regions and neighborhoods that have distinct characteristics, as well as the transitions between them,” Santagata stated. The authors further noted, “Using 3D reconstruction of serial sections and supervised machine learning, we show that archetypical CRC histologic features are often graded and substantially larger than they appear in 2D.”
From here, Santagata added, scientists can start to explore what drives the differences within individual tumors. For example, the maps showed that immune environments varied dramatically within a single tumor. “They were as different across a single tumor as among tumors—which is important because tumor-immune interactions are what you are trying to target with immunotherapy,” Sorger commented.
“We find that the immune environment can vary substantially within a single tumor and recurrently with margin morphology across specimens,” the authors further stated. “At the tumor invasive margin, where tumor, normal, and immune cells compete, T cell suppression involves multiple cell types and 3D imaging shows that seemingly localized 2D features such as tertiary lymphoid structures are commonly interconnected and have graded molecular properties … Budding regions are the most T cell-rich, but also the most immunosuppressive (with abundant Tregs and PDL1-expressing cells). “Whereas tumor buds have few proliferating cells, tumor cells in deep invasive margins are highly proliferative and have fewer immediately adjacent immune cells.”
Similar to their finding in melanoma, the researchers observed that the T cells tasked with fighting off the cancer were not directly suppressed by tumor cells, but rather by other immune cells in the environment around the tumor. “This gives us a whole new appreciation for how diverse and plastic the tumor environments are—they are rich communities, and we are now better equipped to figure out how they develop,” Santagata said.
The maps also provided new insights into the architecture of the tumors. Scientists had previously identified what they thought were 2D pools of a mucus-like substance called mucin with clusters of cancer cells floating inside. However, in the new study, the 3D reconstruction revealed that these mucin pools are, in fact, a series of caverns interconnected by channels, with finger-like projections of cancer cells. “In 2D views, mucin surrounding bud-like structures is found in pools that appear isolated from each other,” the scientists stated. “In 3D, however, these mucin pools were frequently continuous with each other.” The intertumoral mucin pools, they noted, thus comprise “ … 3D networks that can connect to the intestinal lumen and its microbiome.”
“It’s a wild, new look at these tumor structures that we never really appreciated before,” Santagata said. “Because we can see them in 3D, we have a crisp, clean view of the structures, and we can now study why they are there, how they form, and how they shape tumor evolution.” The authors further noted “Thus, while cancer genetics emphasizes the importance of discrete changes in tumor state, whole-specimen imaging reveals large-scale morphological and molecular gradients analogous to those in developing tissues.”
Ultimately, the goal of these colorectal cancer and other cancer maps in development is to advance research and improve diagnosis and treatment. Precision medicine, which involves tailoring therapy to an individual patient’s cancer, is becoming an increasingly important part of treatment, Sorger noted, yet it can go only so far with pathology and genetics alone.
“The big translational story here is building the knowledge to make precision medicine practical for most patients,” he said. “We are currently working with Brigham and Women’s and the Dana-Farber Cancer Institute to determine how our methods can be used in a clinical setting.”
“This is allowing us to extract a whole additional layer of molecular and structural features that we think will provide diagnostic and prognostic information and improve our ability to target these cancers,” Santagata added.
The researchers want to further refine their ability to create 3D reconstructions of tumors and continue integrating new imaging technologies into their maps. They also want to build a bigger cohort of colorectal cancer samples for mapping and explore the basic biology of the disease that their maps have highlighted. One limitation of the reported study, they acknowledged, is that only one CRC has yet been constructed in 3D, “largely because the process remains manual and slow, and many of the features we describe in 3D—TB fibrils, TLS networks, and invasive margins—would benefit from deeper molecular profiling to better identify cell types and states.” In addition, they noted, “There are many spatial relationships among the 2 x 108 cells in our dataset that we have not yet explored.”
For Sorger, the project represents an unusual collaboration between pathologists, engineers, and computational scientists: As the imaging data rolled in, the computational scientists used machine learning to identify interesting findings that they presented to the pathologists, and the pathologists flagged key features to be parsed with machine learning.
“This was an extraordinarily close conversation between the computational group and the pathology group, going back and forth between the rich history of medicine known to pathologists and modern machine learning methods.” Sorger said. “I think it’s an exciting glimpse of how these computation methods can be used in medicine in the future, wherein you tightly couple biologists and physicians with computation, rather than seeing them as replacements for each other.”
The team chose melanoma and colorectal cancer as a starting point because they are common cancers with unmet medical needs that consist of large, solid tumors and require important treatment decisions. Next, the researchers plan to tackle breast cancer and brain cancer. They also want to train other scientists to use the imaging technologies to build their own cancer maps, which would pave the way for the creation of even more atlases.
“A new era in molecular pathology is beginning, and this is a deep look at a tumor that is showing us how remarkable the findings can be,” Santagata stated.
Excess weight, regardless of polygenic risk score, correlated with an increased risk for colorectal cancer, according to results from a population-based, case-control study.
“Accumulated evidence has shown that a high BMI, as a proxy for excess body weight, is associated with increased CRC risk,” Xuechen Chen, MMed, of the division of clinical epidemiology and aging research at the German Cancer Research Center, and colleagues wrote in JAMA Network Open. “Polygenic risk scores (PRSs), the combination of multiple single nucleotide variations identified in genome-wide association studies, are increasingly used for CRC risk stratification and also are useful to improve limited statistical power in gene-environmental studies that often suffer from weak effects of single risk loci and harsh penalty of multiple comparison corrections.
“Another important issue is that CRC risks associated with excess weight and genetic risk factors are often evaluated separately, and how to communicate CRC risk increased by excess weight compared with the risk associated with background genetic profiles remains to be solved.”
To evaluate both individual and joint associations between BMI and PRSs with CRC, Chen and colleagues evaluated 9,169 participants (median age, 69 years; 61% men), of whom 5,053 had CRC and 4,116 were controls. Study analysis showed PRS and BMI independently associated with risk for CRC.
Compared with the lowest tertile, having a PRS in the top tertile correlated with “significantly increased” odds for a CRC diagnosis (adjusted OR = 2.27; 95% CI, 2.02-2.55), as did a BMI of 25 to 29 (aOR = 1.31; 95% CI, 1.18-1.46) and a BMI of 30 or greater (aOR = 1.71; 95% CI, 1.49-1.97) approximately 10 years prior to diagnosis compared with normal weight.
The risk for CRC increased among individuals with a BMI of 30 or more with low (adjusted OR = 1.97; 95% CI, 1.53-2.56), medium (aOR = 2.79; 95% CI, 2.19-3.56) or high PRSs (aOR = 3.82; 95% CI, 3.03-4.83) compared with individuals who with normal weight and low PRS. Further, those with a high PRS had increased risk for CRC with increasing BMI (<25: aOR = 2.41; 95% CI, 1.98-2.93; 25 to <30: aOR = 3.14; 95% CI, 2.6-3.79 and 30: aOR = 3.82; 95% CI, 3.03-4.82) compared with those who had a low PRS and normal weight.
Researchers estimated that the association between a BMI greater than 30 and the risk for CRC was “equivalent” to having a 41-percentile (95% CI, 29-53) higher PRS. Additionally, researchers noted a BMI of at least 30 had the greatest correlation with stage IV CRC (aOR = 2.21; 95% CI, 1.71-2.84).
“The findings of this case-control study add to the limited evidence on the individual and joint associations of BMI and PRS with CRC,” Chen and colleagues concluded. “The absence of interaction on a multiplicative scale between PRS and BMI, two significant CRC risk factors, provides a great potential for CRC risk classification through their joint consideration, and also underlines the importance of keeping a healthy weight.”
Six minutes of high-intensity exercise might prolong the lifespan of a healthy brain, perhaps delaying the start of Alzheimer’s and Parkinson’s diseases, a new, small study suggests.
Researchers found that short but intense cycling increased the production of a protein called brain-derived neurotrophic factor (BDNF), which is essential for brain formation, learning and memory. It’s thought that BDNF might protect the brain from age-related mental decline.
“BDNF has shown great promise in animal models, but pharmaceutical interventions have thus far failed to safely harness the protective power of BDNF in humans,” said lead study author Travis Gibbons, from the University of Otago in New Zealand.
“We saw the need to explore non-pharmacological approaches that can preserve the brain’s capacity which humans can use to naturally increase BDNF to help with healthy aging,” Gibbons said.
The report was published Jan. 11 in the Journal of Physiology.
BDNF promotes the brain’s ability to form new connections and pathways, and also helps neurons survive. Animal studies have shown that increasing the availability of BDNF boosts cognitive performance, such as thinking, reasoning or remembering.
For this study, the researchers wanted to look at the influence of fasting and exercise on BDNF production in humans.
Working with a dozen men and women, the investigators compared fasting, low-intensity cycling for 90 minutes, six-minute high-intensity cycling, and a combination of fasting and exercise.
Brief but vigorous exercise was the most efficient way to increase BDNF compared to one day of fasting with or without lengthy, low-intensity exercise, the researchers said.
BDNF increased four to five times more compared to fasting, which showed no BDNF change, or prolonged activity, which showed a slight increase in BDNF.
More work is needed to better understand these findings, the study authors noted.
The researchers hypothesize that the brain switches its favored fuel source for another to meet the body’s energy demands. This could mean metabolizing lactate instead of glucose during exercise, which potentially could initiate pathways that lead to more BDNF in the blood.
The BDNF boost could be due to an increased number of blood platelets, which store large amounts of BDNF. This is more heavily influenced by exercise than fasting, they explained.
Ongoing research will further study the effects of calorie restriction and exercise.
“We are now studying how fasting for longer durations, for example up to three days, influences BDNF,” Gibbons said in a journal news release. “We are curious whether exercising hard at the start of a fast accelerates the beneficial effects of fasting. Fasting and exercise are rarely studied together. We think fasting and exercise can be used in conjunction to optimize BDNF production in the human brain.”
A new study that shows the harm to the liver of eating fast food might provide people with motivation to eat less of it in the new year.
The study found that eating at least 20% of total daily calories from fast food can increase the risk of nonalcoholic fatty liver disease, a potentially life-threatening condition where fat builds up in the liver. The disease can lead to cirrhosis and its complications, including liver failure and liver cancer.
People with obesity or diabetes are more vulnerable to the harmful effects of fast food on the liver, although the general population is not immune to the harm.
“My hope is that this study encourages people to seek out more nutritious, healthy food options,” says lead investigator Ani Kardashian, MD, with Keck Medicine at the University of Southern California.
“At a policy level, public health efforts are needed to improve access to affordable, healthy, and nutritious food options across the U.S. This is especially important as more people have turned to fast foods during the pandemic and as the price of food as risen dramatically over the past year due to food inflation,” she says.
The researchers analyzed data on diet and fatty liver measurements for nearly 4,000 adults.
Nearly 30% of them got 20% or more of their total daily calories from fast food, such as burgers, fries, pizza, and the like.
They found that people with obesity or diabetes who take in one-fifth or more of their daily calories from fast food had severely high levels of fat in their liver, compared with those who eat less or no fast food.
The general population had moderate increases in liver fat when one-fifth or more of their diet was made up of fast food.
The findings are particularly “alarming” given the increase in fast-food consumption over the past 50 years, regardless of socioeconomic status, Kardashian says.
“If people eat one meal a day at a fast-food restaurant, they may think they aren’t doing harm. However, if that one meal equals at least one-fifth of their daily calories, they are putting their livers at risk,” she says.
For people who have limited options and need to eat fast food, “there are healthy choices at most restaurants; you just need to be smart about reading labels, watching calories, and ordering the healthier options,” says Nancy Reau, MD, with Rush University Medical Center in Chicago, who wasn’t involved in the study.
Lisa Ganjhu, DO, with NYU Langone Health in New York City, agrees.
“I am a firm believer that fast food can cause fatty liver. It goes hand in hand, and I counsel and coach my patients on healthy diet and exercise, and I’ve been pretty successful,” she says.
“If my patient is eating at McDonald’s a lot, I basically walk through the menu with them and help them find something healthy. When patients see the benefits of cutting out fat and reducing carbohydrate, they are more apt to continue,.”