Type 2 diabetes is considered to be one of the major predisposing factors for microvascular and macrovascular diseases. In recent years, the treatment for diabetes has broadened from glycaemic control and has become a more patient-centred approach, in which the hazard of heart failure and atherosclerotic cardiovascular disease is taken into consideration.
Oral diabetic drugs known as inhibitors of sodium-glucose cotransporter-2 (SGLT2) promote the excretion of glucose by impeding the glucose reabsorption by the renal proximal tubules, thereby reducing plasma glucose levels. Based on current recommendations, SGLT2 inhibitors need to be considered as a second-line treatment after Metformin in patients with type 2 diabetes.
Several randomised control trials have manifested that SGLT2 inhibitors can improve cardiovascular outcomes in patients having diabetes.
Sodium diuresis and sodium excretion effects of Dapagliflozin last longer and are more stable compared to those of Empagliflozin. Thus, Dapagliflozin has been found to decrease the 24-hour fluctuation in blood pressure. This, in turn, is associated with a lower risk for cardiovascular diseases.
Currently, studies have reported that SGLT2 inhibitors have beneficial impacts on cardiovascular outcomes, but the effect differs among individual SGLT2 inhibitors.
Dapagliflozin did not enhance plasma noradrenaline and aldosterone levels compared to Empagliflozin, which could be beneficial for the prevention of heart failure.
The recommended dose at which Dapagliflozin must be started is 5 mg once a day, and the dosage can be escalated to 10 mg once daily in patients who require additional glycaemic control. Empagliflozin is recommended at a starting dosage of 10 mg daily.
A clinical study compared the effects of Dapagliflozin and Empagliflozin on cardiovascular outcomes in patients with type 2 diabetes. It was inferred that the risks of developing stroke, heart failure, myocardial infarction, and cardiac-related death were not significantly different among the patients receiving Dapagliflozin or Empagliflozin. It is suggested that SGLT2 inhibitors can decrease the risk of cardiovascular diseases, but the study did not find any significant difference in the effectivity of Dapagliflozin and Empagliflozin
Asthma management in young children aims to achieve good symptom control, maintain normal activity levels, and reduce the risk of asthma exacerbations, impaired lung development, and drug side effects.
Global Initiative for Asthma (GINA) guidelines, 2022, regarding indications of regular controller treatment in children aged ≤5 years with asthma:
Intermittent or episodic wheezing of any severity can be caused by an isolated viral-induced wheezing episode, a seasonal or allergen-induced asthma, or unrecognised uncontrolled asthma. For all of these conditions, wheezing is initially treated with a short-acting beta-2 agonist (SABA) every 4-6 hours as needed until symptoms resolve, usually within 1-7 days. However, there is uncertainty regarding the use of additional drugs in these children, especially when the nature of the episode is unclear. The indications of regular controller treatment in these children:
Regular controller treatment should be started, and the response should be assessed if the history and symptom pattern indicate an asthma, respiratory symptoms are uncontrolled, and/or wheezing episodes are frequent (e.g., ≥3 episodes in a season).
Regular controller treatment might be considered if a child presents with less frequent but more severe episodes of viral-induced wheezing.
A trial of regular controller treatment should be considered to determine whether the symptoms are caused by asthma if the diagnosis of asthma is uncertain, and inhaled SABA therapy or courses of antibiotics need to be repeated frequently, e.g. more than every 6-8 weeks. At this stage, the patient should be referred for specialist advice.
Hypercholesterolaemia is an important modifiable risk feature for cardiovascular disease in both men and women. Compared to men, low-density lipoprotein cholesterol (LDL-C) levels are found to be usually lower in women until menopause, when levels escalate (from a mean of 117 mg/dL to 145 mg/dL), and particles of LDL tend to become more atherogenic. The amount of high-density lipoprotein cholesterol (HDL-C) is about 10 mg/dL higher in women than in men. Low levels of HDL are more predictive of coronary heart disease (CHD) in women when compared to men, particularly in women aged 65 years or more. Moreover, elevated triglycerides may be a more critical risk factor in women (especially older women) compared with men, and, for both sexes, elevated non-HDL-C is regarded as a risk marker for CHD, particularly in patients affected with hypertriglyceridaemia.
Several guidelines recommend the administration of statins as a first-line treatment for lowering cholesterol when diet modifications and exercise are insufficient to treat hypercholesterolaemia.
A clinical study was conducted to evaluate the efficacy and safety of Atorvastatin and Rosuvastatin for the treatment of hypercholesterolaemia.
Treatment with statin produced a dose-dependent reduction in the levels of LDL-C at six weeks; the level of decrease was dependent on the type of statin and dose used.
The American College of Cardiology (ACC)/ American Heart Association (AHA) recommendations on stain intensity:
Intensity
Statin dose
High
Rosuvastatin 20–40 mg
Atorvastatin 40-80 mg
Moderate
Rosuvastatin 5–10 mg
Atorvastatin 10-20 mg
Efficacy:
Results of this clinical study indicated that Rosuvastatin 20 mg produced statistically greater reductions in LDL-C when compared with 20 mg and 40 mg of Atorvastatin. Moreover, 40 mg of Rosuvastatin also produced a statistically more significant lowering in LDL-C compared with 40 mg of Atorvastatin.
Rosuvastatin 20 mg reduced non-HDL-C significantly more than milligram-equivalent doses of Atorvastatin. Similarly, Rosuvastatin 20 mg and 40 mg induced HDL-C in a significant amount in comparison to milligram-equivalent or higher doses of Atorvastatin.
Safety:
All treatments were found to be well tolerated in general, with the same safety profiles across treatments and dose ranges
For the treatment of refractory focal seizures (RFS), the antileptic drug, Levetiracetam has manifested good efficacy and tolerability. The anti-epileptic effect of the drug is most likely due to its binding to synaptic vesicle protein 2a (SV2A), located in presynaptic membranes, modulating the calcium-dependent exocytosis of neurotransmitters into the synaptic gap.
In contrast, Brivaracetam is a highly selective and reversible SV2A ligand having a 15- to 30-fold higher affinity compared to the affinity of Levetiracetam in the human brain. Studies have indicated that Brivaracetam can also be effective and well tolerated as adjunctive therapy in patients with RFS.
A clinical study was conducted to evaluate the efficacy and tolerability of Levetiracetam and Brivaracetam in adults with RFS. The study revealed that both Levetiracetam and Brivaracetam, at various doses, were effective for treating patients with RFS. The maximum efficacy of both drugs seemed to be restricted at the middle dose because the high dose of both drugs (3000 mg Levetiracetam and 200 mg Brivaracetam) did not show higher efficacy than the middle dose.
Furthermore, the majority of statistical differences for adverse effects and the withdrawal of Levetiracetam and Brivaracetam were found at the middle-dose levels, suggesting a dose of more than 2000 mg/d Levetiracetam and 100 mg/d Brivaracetam should be administered cautiously.
The study thus inferred that Levetiracetam might be slightly more effective with a lower probability of dizziness compared with Brivaracetam for patients with RFS.
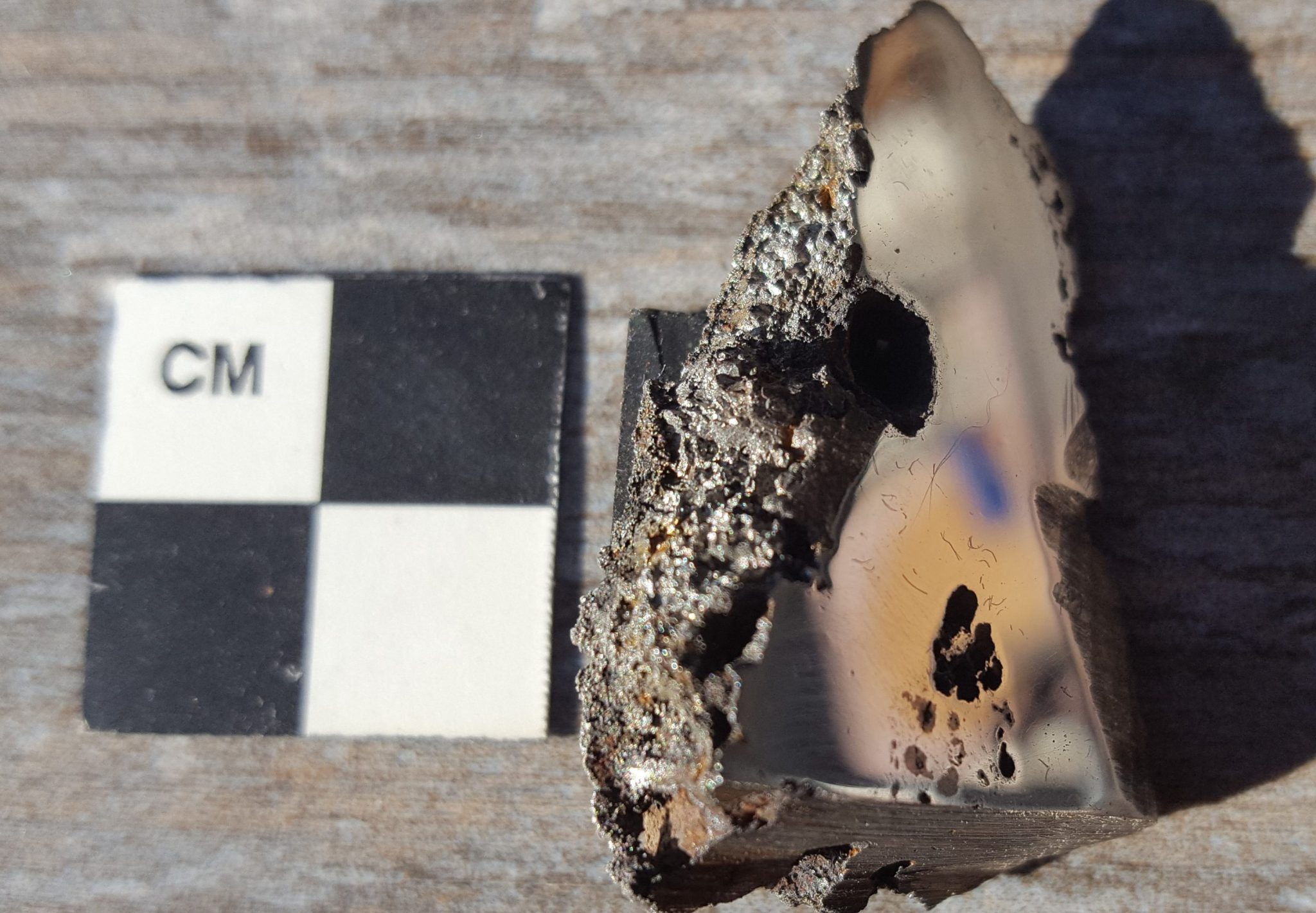
A team of scientists has discovered at least two never-before-seen minerals on Earth from a 15-tonne meteorite that crashed in Somalia. It is the ninth-largest meteorite ever found, but the presence of the exotic alien minerals makes it a special one. As revealed by a statement from the University of Alberta, the new alien minerals were found in a slice of 70 grams of the meteorite that scientists studied. While two minerals have been confirmed by experts, a third mineral is under consideration. However, as noted by U of A scientists, if more samples from the meteorite were to be obtained, there would be many more mineral discoveries. The two newly-found minerals have been named elaliite and elinkstantonite. The meteorite dubbed El Ali crashed in Somalia in 2020.
New, but made previously in a lab
The two minerals are not from Earth and have never before been found on the planet. Nevertheless, scientists did succeed in synthetically crafting them previously in a laboratory. This allowed scientists to spot the new minerals so rapidly, a statement from U of A revealed. The future of the meteorite remains in doubt. The latest news suggests that the meteorite had been moved to China, where a potential buyer could acquire it. Whether or not the new owner would allow sampling of the meteorite in the future remains to be seen. However, it is noteworthy that such meteorites should be primarily available for scientific study and not for collections.
The optimal range of sodium intake for cardiovascular health is controversial.
Methods
We obtained morning fasting urine samples from 101,945 persons in 17 countries and estimated 24-hour sodium and potassium excretion (used as a surrogate for intake). We examined the association between estimated urinary sodium and potassium excretion and the composite outcome of death and major cardiovascular events.
Results
The mean estimated sodium and potassium excretion was 4.93 g per day and 2.12 g per day, respectively. With a mean follow-up of 3.7 years, the composite outcome occurred in 3317 participants (3.3%). As compared with an estimated sodium excretion of 4.00 to 5.99 g per day (reference range), a higher estimated sodium excretion (≥7.00 g per day) was associated with an increased risk of the composite outcome (odds ratio, 1.15; 95% confidence interval [CI], 1.02 to 1.30), as well as increased risks of death and major cardiovascular events considered separately. The association between a high estimated sodium excretion and the composite outcome was strongest among participants with hypertension (P=0.02 for interaction), with an increased risk at an estimated sodium excretion of 6.00 g or more per day. As compared with the reference range, an estimated sodium excretion that was below 3.00 g per day was also associated with an increased risk of the composite outcome (odds ratio, 1.27; 95% CI, 1.12 to 1.44). As compared with an estimated potassium excretion that was less than 1.50 g per day, higher potassium excretion was associated with a reduced risk of the composite outcome.
Conclusions
In this study in which sodium intake was estimated on the basis of measured urinary excretion, an estimated sodium intake between 3 g per day and 6 g per day was associated with a lower risk of death and cardiovascular events than was either a higher or lower estimated level of intake. As compared with an estimated potassium excretion that was less than 1.50 g per day, higher potassium excretion was associated with a lower risk of death and cardiovascular events.
Why is lifelong learning so important for not only unlocking cognitive health benefits, but also maintaining cognitive health?
To find purpose and meaning in life, your ability to explore, discover, and learn is of great assistance. Consider this: You may feel more appreciated and accomplished when you master a new recipe and then prepare that meal for family and/or friends.
Here’s another example: At your next book club meeting, you feel good about being able to share and offer new insights after having read something particularly interesting.
Cognitive Health
At every stage of life, lifelong learning is beneficial, including – and maybe especially – during your golden years.
With age, some people believe that cognitive decline is an absolute – especially if they are already residing in an assisted living setting. This is not true! It doesn’t always have to be a given. Your intellectual, cognitive health can be enhanced courtesy of lifelong learning. Here’s how.
4 Great Ways Learning Improves Your Cognitive Health
1. Nurture The Brain
Nurture your brain by nourishing it in more ways than one. Naturally, this includes eating the right foods and/or taking the right supplements for a healthy brain.
Here are five ways in which you can nurture your brain for better, longer cognitive health:
Get enough sleep every night and make sure it’s quality sleep. This may be easier said than done for some individuals. Do whatever you can and whatever you need to in the pursuit of quality sleep in proper amounts. Buy a new mattress, turn off your electronics, read a good book in bed, etc.
Manage stress as efficiently as possible. To maintain your overall health, it is crucial you discourage relationship conflicts, feelings of insecurity, anger, irritability, frustration, and more, which can all be exacerbated by stress. It can also contribute to panic attacks, phobias, anxiety, depression, and other emotional/mental disorders. Talk to a professional for ideas as to how to handle stress and other mental health issues.
Get the physical activity you need to stay healthy, both physically and mentally. Don’t push yourself past your limits, but, at the very least, try to take at least one walk per day. There are “sit and be fit” routines if you have a hard time standing or moving about. Whether you participate in a retirement living program through your residence or get a group together and pursue something on your own, the important thing is to move!
To discourage cognitive decline, pursue mental stimulation. The adage “use it or lose it” applies to both the human body and mind. Create a brain training program that includes features like improving reaction speed, memory, coordination, executive function, visual perception, and attention.
Eat a balanced diet, making sure to get all of the most important vitamins and minerals for cognitive health. To boost brainpower, eat more zinc, magnesium, calcium, vitamin C/ascorbic acid, B-9/folic acid, and B-1/thiamine.
2. Boost Your Mood
Because your mood helps determine cognitive health, consider the following mood boosters:
Disconnect when you need to – pray, meditate, relax, write in a journal
If you already have a bit of a problem with self-confidence, you may need to boost it before you can maintain it. There are a handful of methods through which some people have built self-confidence:
Get a hobby
Talk yourself up
Set distinct goals and get things done
Concentrate on what you’re good at
Feel accomplished in, and proud of, things you’ve already achieved
You may want to monitor your progress so you can keep an eye on how you’re doing.
4. Be Adaptable
Increasing your adaptability will help you stay healthier all the way around. It can even be of assistance in lessening stress. Here are a handful of suggestions as to how to be more adaptable.
Learn from your successes and your mistakes
Keep a journal
Catalog things that didn’t go quite so well, but also list things you’re proud of
Give yourself a big hug and lots of love
Every day, note things you’re grateful for
Your comfort zone should be expanded
Learn new skills
Set your curiosity free – what have you always wanted to know more about?
Keep inspiration handy
Flex your creative muscles – learn to paint, sing songs, play an instrument
Follow your personal “North Star”
Figure out what “North” means for you. As a human being, what makes you feel fulfilled? What’s your purpose?
Find landmarks. Compared to others, what are your special, unique experiences, skills, and talents?
Make a life map. This will assist you in connecting the dots between where you are today and your “North Star”. Use paper and markers.
Take your big plans and break them down into long term (keep it to one or two core principles), medium (milestones for the next few months), and short (plan for the next week or two) scales.
How does one develop themselves into being a good mentor? Here are a handful of suggestions:
Be or become the most positive role model you can possibly be. From your words and actions, others will observe and learn, provided you – yourself – are on the right path.
Don’t make all the decisions for the person you are mentoring. They need to make their own decisions, even though you may know better. They’re learning; you’re not doing it for them.
Understand the other person’s feelings and perspective – practice empathy. One vital good mentor trait is that of empathy. You can better guide your protégé if you understand how they’re feeling.
Without breaking the confidence of the person you are mentoring, you can deliver criticism in a constructive manner. When addressing your concerns, be tactful and diplomatic. Point out something positive, rather than only shortcomings and mistakes, then offer guidance on improvement.
Communication and listening are both crucial. What are the expectations and aspirations of your protégé? Are they looking for insight, guidance, or support? Your approach should be targeted.
Provide a Sense of Fulfilment
Some of the most successful people were asked how they achieve fulfillment. Here’s what they suggested:
To something bigger than yourself, find a connection.
You are not entitled, so don’t think like it. Take the words “should have” out of your life.
Rather than living in the past, live in the present. Don’t clutter your mind with what has been. Concentrate on here and now.
Do something that makes others feel good. Contribute to others. For other people’s unique experiences, gain a sense of compassion to feel more connected.
Never stop growing. Constantly challenge yourself.
15 Life-Changing Lessons to Learn from Don Miguel Ruiz
1. Be Impeccable With Your Word.
“Be Impeccable With Your Word. Speak with integrity. Say only what you mean. Avoid using the word to speak against yourself or to gossip about others. Use the power of your word in the direction of truth and love.” ~ Don Miguel Ruiz
“When you look at yourself in a mirror, do you like what you see, or do you judge your body and use the word to tell yourself lies? If you believe that you are not attractive enough, then you believe a lie, and you are using the word against yourself, against the truth.”
“You know that if you lie to yourself, surely other people lie to themselves. And if they lie to themselves, they will lie to you also.”
“Don’t Take Anything Personally. Nothing others do is because of you. What others say and do is a projection of their own reality, their own dream. When you are immune to the opinions and actions of others, you won’t be the victim of needless suffering.” ~ Don Miguel Ruiz
“But it is not what I am saying that is hurting you; it is that you have wounds that I touch by what I have said. You are hurting yourself. There is no way I can take this personally.”
“…Nothing that your partner does is personal. Your partner is dealing with her own garbage. If you don’t take it personally, it will be so easy for you to have a wonderful relationship with your partner”
3. Don’t Make Assumptions.
“Don’t Make Assumptions. Find the courage to ask questions and to express what you really want. Communicate with others as clearly as you can to avoid misunderstandings, sadness and drama. With just this one agreement, you can completely transform your life.” ~ Don Miguel Ruiz
“If others tell us something we make assumptions, and if they don’t tell us something we make assumptions to fulfill our need to know and to replace the need to communicate. Even if we hear something and we don’t understand we make assumptions about what it means and then believe the assumptions. We make all sorts of assumptions because we don’t have the courage to ask questions.”
4. Always Do Your Best.
“Always Do Your Best. Your best is going to change from moment to moment; it will be different when you are healthy as opposed to sick. Under any circumstance, simply do your best, and you will avoid self-judgment, self-abuse and regret.” ~ Don Miguel Ruiz
“When we believe in lies, we cannot see the truth, so we make thousands of assumptions and we take them as truth. One of the biggest assumptions we make is that the lies we believe are the truth!”
5. You can only be the main character in your own story.
“The same way that you are the main character of your story, you are only a secondary character in everybody else’s story.” ~ Don Miguel Ruiz
6. Life is but a mirror.
“We only see what we want to see; we only hear what we want to hear. Our belief system is just like a mirror that only shows us what we believe.”
7. The best way to say, “I love you, God,” is to live your life doing your best.
“God is life. God is life in action. The best way to say, “I love you, God,” is to live your life doing your best. The best way to say, “Thank you, God,” is by letting go of the past and living in the present moment, right here and now.” ~Don Miguel Ruiz
Whatever life takes away from you, let it go. When you surrender and let go of the past, you allow yourself to be fully alive in the moment. Letting go of the past means you can enjoy the dream that is happening right now.” ~Don Miguel Ruiz
“If someone is not treating you with love and respect, it is a gift if they walk away from you. If that person doesn’t walk away, you will surely endure many years of suffering with him or her. Walking away may hurt for a while, but your heart will eventually heal. Then you can choose what you really want. You will find that you don’t need to trust others as much as you need to trust yourself to make the right choices.” ~ Don Miguel Ruiz
“I will no longer allow anyone to manipulate my mind and control my life in the name of love.”
“I no longer agree to treat myself with disrespect. Every time a self-critical thought comes to mind, I will forgive the Judge and follow this comment with words of praise, self-acceptance, and love.” ~ Don Miguel Ruiz
“You can have many great ideas in your head, but what makes the difference is the action. Without action upon an idea, there will be no manifestation, no results, and no reward.” ~ Don Miguel Ruiz
13. Your heart can create any amount of love, not just for yourself, but for the whole world.
“People are starving for love, not knowing their heart is a magical kitchen. Open your heart. Open your magical kitchen and refuse to walk around the world begging for love. In your heart is all the love you need. Your heart can create any amount of love, not just for yourself, but for the whole world.
14. Respect is one of the greatest expressions of love.
“When we respect everybody around us, we are in peace with everybody around us.”
“Life is very, very simple and easy to understand, but we complicate it with the beliefs and ideas that we create.”
“We never stop to consider that our beliefs are only a relative truth that’s always going to be distorted by all the knowledge we have stored in our memory.”
MD Anderson researchers presenting key advances in multiple leukemias at ASH 2022
MD Anderson News Release December 12, 2022
Researchers from The University of Texas MD Anderson Cancer Center are presenting compelling findings from three clinical trials at the 2022 American Society of Hematology (ASH) Annual Meeting. These oral presentations highlight encouraging results to advance the use of targeted therapies and novel combinations in multiple types of leukemia, including high-risk and newly diagnosed acute myeloid leukemia (AML) in older and younger patients and Philadelphia chromosome-positive acute lymphoblastic leukemia (ALL). More information on all ASH Annual Meeting content from MD Anderson can be found at MDAnderson.org/ASH.
Older or high-risk patients with newly diagnosed AML respond well to triplet therapy (Abstract 61) Researchers observed encouraging response rates in older or high-risk patients with newly diagnosed acute myeloid leukemia (AML) who were treated with the triplet combination therapy of azacitidine, venetoclax and magrolimab on a Phase Ib/II trial. The newly diagnosed cohort had an 80% overall response rate (ORR), and the median overall survival (OS) was not yet reached at a median follow-up of 9.2 months. Naval Daver, M.D., associate professor of Leukemia, presented study results Dec. 10.
“We are encouraged by the promising evidence of this triplet therapy as a treatment option for older or unfit patients with AML,” Daver said. “We will continue to expand the trial to include more patients, and we have initiated an international Phase III randomized study evaluating the triplet therapy versus the doublet azacitidine-venetoclax. If the study is positive, it could establish a new frontline standard of care for these patients.”
About 50-55% of patients with AML are considered older or unfit for intensive chemotherapy. Frontline treatment with azacitidine and venetoclax achieves response rates of 65-70% in newly diagnosed patients, but most patients will relapse and those with TP53 mutations continue to have poor outcomes, with median OS of less than six months. Magrolimab is an anti-CD47 antibody that works to block the “don’t eat me signal” on leukemia cells. In a previous trial, it demonstrated efficacy with azacitidine in newly diagnosed AML, with an especially encouraging signal of response and survival in frontline TP53-mutated AML.
The current trial enrolled 74 patients across two cohorts. The first cohort enrolled 45 frontline patients aged 75 or older with documented comorbidities that made them ineligible for intensive therapy or with adverse risk factors and/or a TP53 mutation, regardless of age. This cohort included 27 patients with a TP53 mutation and 14 without. The second cohort enrolled 29 patients with relapsed/refractory (R/R) disease.
All patients who received at least one dose of any of the three study drugs were included for response and adverse events. Eighteen patients experienced greater than grade 3 anemia, and the most common non-hematologic side effects were febrile neutropenia, pneumonia, hyperbilirubinemia, transaminitis, creatine elevation and hypokalemia.
In the newly diagnosed cohort, the ORR in patients with and without TP53 mutations was 74% and 93%, respectively. Median OS was not yet reached for either group of patients. Responses in patients with R/R disease with prior venetoclax treatment were modest, and the cohort was closed for futility. Patients with R/R disease without venetoclax exposure still are being enrolled.
The study was funded by Gilead. Daver has served in an advisory role for Gilead. A complete list of collaborating authors can be found within the abstract here.
Chemotherapy-free regimen ponatinib plus blinatumomab effective in patients with newly diagnosed Ph+ ALL (Abstract 213) The chemotherapy-free regimen of ponatinib and blinatumomab achieved high response rates and reduced the need for an allogeneic stem cell transplant for patients with recently diagnosed Philadelphia chromosome-positive (Ph+) acute lymphoblastic leukemia (ALL), according to results from a Phase II trial. One of the lead investigators, Nicholas Short, M.D., assistant professor of Leukemia, presented the findings Dec. 10.
“Traditionally, Ph+ ALL responds poorly to standard chemotherapy and is high-risk for relapse, so these survival results and reduced need for a stem cell transplant are very encouraging,” Short said. “Not only does this regimen appear to be a safe and effective chemotherapy-free option, but it also seems to overcome the historical need for transplant in these patients.”
Patients with Ph+ ALL have historically had poor long-term survival rates. Researchers have found adding tyrosine kinase inhibitors (TKIs), such as ponatinib, to chemotherapy can drastically improve survival. Ponatinib is a third-generation TKI that targets BCR-ABL1 and is traditionally used to treat certain types of chronic myeloid leukemia. Blinatumomab is a CD3-CD19 bispecific antibody that is effective as a single agent in relapsed or refractory Ph+ ALL.
The trial enrolled 40 patients with newly diagnosed Ph+ ALL. Patients with uncontrolled cardiovascular disease or clinically significant central nervous system comorbidities were excluded from the study. The average age of participants was 56 years old.
Of the patients that were evaluable for a hematologic response, 96% had a complete remission or complete remission with incomplete count recovery. Among the 38 patients who were evaluable for complete molecular response (CMR), 68% achieved CMR after one treatment cycle and 87% achieved CMR during the trial period. Molecular responses were rapid, with a majority of patients achieving CMR in the peripheral blood within two weeks of therapy. Only one patient underwent stem cell transplant in first remission.
At a median follow-up of 15 months, event-free and estimated overall survival was 95%. These encouraging outcomes were observed despite the very low rate of transplant in the study. The treatment was well tolerated, and most toxicities were grade 1-2 and consistent with known side effects of the two agents.
The study was funded by Amgen and Takeda Oncology. Short has served in a consulting or advisory role for Takeda Oncology. A complete list of collaborating authors can be found within the abstract here.
Venetoclax with CLIA highly effective in younger patients with newly diagnosed AML, high-risk MDS (Abstract709) The latest results of a Phase II study evaluating the addition of venetoclax to the intensive chemotherapy treatment of cladribine, idarubicin and cytarabine (CLIA) as a frontline therapy demonstrated high rates of disease control and remissions in younger patients with newly diagnosed AML and high-risk myelodysplastic syndrome (MDS). In the study, 96% of patients responded to treatment and 90% had no measurable disease detected in a bone marrow sample. Patrick Reville, M.D., instructor of Leukemia, presented updated results and longer-term follow-up data Dec. 12.
“Venetoclax has been a breakthrough for AML patients that are ineligible for intensive therapy. This data continues to demonstrate the benefit of including venetoclax with the CLIA induction regimen,” Reville said. “This regimen is leading to unprecedented response and measurable residual disease-negativity rates. As we continue to follow participants, we are encouraged by their long-term outcomes and survival.”
The single-center, single-arm trial enrolled 67 patients with a median age of 48. Sixty patients had AML and four patients had high-risk MDS. In addition, three patients had a mixed-phenotype acute leukemia (MPAL).
The composite complete response rate was 96% across all patients and 100% for patients with both MDS and MPAL with a myeloid predominant clone. Most patients went on to receive a subsequent allogeneic stem cell transplant (alloSCT), including 70% of those who responded to treatment.
Encouragingly, with a median follow-up of just over two years, the median duration of response, event-free survival and overall survival have not yet been reached. At 12 months, the estimated event-free survival rate is 70% and the estimated overall survival rate is 86%. Seventy-four percent of responding patients are estimated to have an ongoing response at 12 months.
The most common non-hematologic adverse event that participants experienced was febrile neutropenia, which was managed. Researchers continue to follow patients and study this treatment regimen as a safe and effective induction treatment strategy for this patient population.