Public health institutions have long walked the difficult line between respecting individual freedoms and protecting society from disease threats — which has sometimes involved restricting those freedoms. This balancing act has often been met with contentious public debate and legal challenges. In perhaps the most famous example, the state’s police power to protect public health was affirmed by the U.S. Supreme Court in its 1905 decision in Jacobson v. Massachusetts. The Court determined that a state may compel vaccination, as a result compromising people’s right to bodily autonomy, for the purpose of promoting public health — thereby upholding the community’s competing right to protect itself from deadly disease.
During the Covid-19 pandemic, negotiating such trade-offs became substantially more complex, given a rapidly changing environment and an evolving body of knowledge about SARS-CoV-2. Particularly early in the pandemic, decisions affecting personal freedoms had to be made quickly, with little opportunity for public deliberation. Public health authorities understandably made decisions by relying on prepandemic planning that was based on previous experience with respiratory viruses. As the pandemic dragged on, however, the continued absence of publicized debate about these trade-offs within public health institutions and among public health experts turned masking into a flash point for the clash between competing rights: the right to bodily autonomy (including the freedom to decide whether to mask) and the right to be protected from the threat of Covid-19. Far too often, discussions about the implications of various masking policies were drowned out by absolutist language on both sides of the debate, suggesting, on the one hand, that mask mandates were an unacceptable infringement on freedoms or, on the other, that choosing not to mask was tantamount to choosing to harm others.
The reality is far more complex, and the all-or-nothing disputes that have predominated during the past 2 years have obscured the difficult choices that public health authorities must make and the range of factors that should be weighed when considering mask mandates. Such factors include, but aren’t limited to, the evidence for the efficacy of masking in communities with a range of Covid-19 transmission rates, the potential downsides of wearing a mask in various social contexts, and which groups of people bear the highest risk of infection. Early in the pandemic, when Covid-19 vaccines weren’t available, when there was limited epidemiologic evidence to inform mitigation policy, and when the risk of infection was high, it was perhaps easier for authorities to reach decisions to implement mask mandates. Matters became more complicated, however, as the pandemic evolved. We believe the decisions that have been made during this later stage of the pandemic — after the introduction of highly effective vaccines, and when the trade-off between the efficacy and the perceived harms of masking in public spaces was more nuanced — warrant reexamination by public health institutions.
One example of public spaces affected by mask mandates are grocery stores. For the average, healthy customer, a mask mandate may serve little purpose if community levels of Covid-19 are low. But the risk calculation is different for cashiers and other essential workers in these spaces. These workers are more likely than members of the general working public to be Black or Latinx, to have incomes below 200% of the federal poverty level, or to live with someone who is 65 years of age or older.1 Such lower-income and marginalized racial and ethnic groups have had disproportionately poor outcomes during the pandemic, as have older adults. In these spaces, the benefits of mask mandates to essential workers may outweigh the inconvenience that masks pose to customers, even if community transmission levels are relatively low. At the same time, such benefits may not outweigh the costs associated with engaging in frequent confrontations with customers over masking. The ability to make these calculations, which are specific to local contexts, might obviate the need for a blanket masking policy; such nuances also suggest that the most useful role for public health institutions may be to provide data to support risk assessments and frameworks that could guide decision making by relevant local leaders.
Another example of public spaces affected by mask requirements and other Covid-related policies are local courthouses. The state has the power to compel people to be present in courthouses as defendants, lawyers, witnesses, and jury members. Given this power to compel, the state has a duty to protect people in these spaces. Criminal defendants are often residing in congregate-living settings (i.e., jails), where Covid-19 outbreaks have spread quickly and with deadly consequences, and many are poor and are members of marginalized racial groups. The state also has a responsibility to citizens who expect their health and safety to be protected while they serve as jurors for their peers.
To fulfill these responsibilities while carrying out essential functions of the legal system during Covid-19 surges in 2020 and 2021, many courts adopted risk-mitigation measures, including virtual court hearings, social distancing in courtrooms, lightened trial schedules and delayed trial dates, mask mandates, and jury-service exemptions for people at high risk for complications of Covid-19 (or people who were particularly fearful of Covid-19).2 But some of these measures may have compromised the rights of people interacting with the legal system. Lightened trial schedules hinder the constitutional right to a public trial without delay. Holding trials virtually or spreading jurors throughout the courtroom to facilitate social distancing may make it too easy for jurors to become distracted and may thus influence judgments.3 Masks may affect jurors’ perception of testimony, thereby potentially compromising the right to a fair trial.4 There is no simple way to balance the right to health and safety with the right to equal access to justice for people compelled to participate in the court system. The role of public health institutions is to advance recommendations based on science, but decisions must ultimately take into account a breadth of concerns, many of which may be beyond the remit of public health authorities. Public health entities shouldn’t make these judgment calls in isolation, particularly without including local stakeholders in the process.
Public health decision making related to Covid-19 has required complicated balancing; some decisions, such as whether to close schools, can have substantial consequences for an entire generation. A confluence of factors that coincided with the beginning of the Covid-19 pandemic — including an impending U.S. federal election and the ascendance of social media as a dominant platform for public conversation — limited the ability of public health practitioners to seriously discuss the trade-offs involved in Covid-related decisions.
As the pandemic evolves, we believe it’s time to shift away from this dynamic and to recognize that pandemic-era decision making requires the transparent balancing of multiple rights. Complex decisions should be widely and publicly debated by public health institutions. Similarly, it would behoove public health practitioners to stop suggesting in social media posts that nuanced questions have universally correct answers. We believe the primary objective of public health institutions during a pandemic — after the early crisis stage has passed — should be to provide data and decision-making frameworks that local partners can use in diverse contexts to weigh various trade-offs. These local partners may include community government leaders, private-sector executives, and stakeholders from civic organizations, school boards, and health care facilities. Public health practitioners can look to previous approaches to pandemic preparedness for rich examples of deliberate public engagement to inform decision making.5 Consideration of multiple perspectives, especially those of the groups most affected by public health policies, will permit more robust decision making and foster increased public trust when decisions that restrict freedoms must be made.
In patients with coronary artery disease who are being evaluated for percutaneous coronary intervention (PCI), procedures can be guided by fractional flow reserve (FFR) or intravascular ultrasonography (IVUS) for decision making regarding revascularization and stent implantation. However, the differences in clinical outcomes when only one method is used for both purposes are unclear.
Methods
We randomly assigned 1682 patients who were being evaluated for PCI for the treatment of intermediate stenosis (40 to 70% occlusion by visual estimation on coronary angiography) in a 1:1 ratio to undergo either an FFR-guided or IVUS-guided procedure. FFR or IVUS was to be used to determine whether to perform PCI and to assess PCI success. In the FFR group, PCI was to be performed if the FFR was 0.80 or less. In the IVUS group, the criteria for PCI were a minimal lumen area measuring either 3 mm2 or less or measuring 3 to 4 mm2 with a plaque burden of more than 70%. The primary outcome was a composite of death, myocardial infarction, or revascularization at 24 months after randomization. We tested the noninferiority of the FFR group as compared with the IVUS group (noninferiority margin, 2.5 percentage points).
Results
The frequency of PCI was 44.4% among patients in the FFR group and 65.3% among those in the IVUS group. At 24 months, a primary-outcome event had occurred in 8.1% of the patients in the FFR group and in 8.5% of those in the IVUS group (absolute difference, −0.4 percentage points; upper boundary of the one-sided 97.5% confidence interval, 2.2 percentage points; P=0.01 for noninferiority). Patient-reported outcomes as reported on the Seattle Angina Questionnaire were similar in the two groups.
Conclusions
In patients with intermediate stenosis who were being evaluated for PCI, FFR guidance was noninferior to IVUS guidance with respect to the composite primary outcome of death, myocardial infarction, or revascularization at 24 months.
Summary: Repeat concussions thicken the structure of skull bones. Researchers theorize the thickening of the skull may occur as the body attempts to better protect the brain from subsequent damage.
Source: Monash University
New research has found that repeated concussions can thicken the structure of skull bones. Previous studies have shown damage to the brain following concussion, but have not looked at the brain’s protective covering.
A Monash-led study published in the journal Scientific Reports by Associate Professor Bridgette Semple from the Monash University’s Central Clinical School Department of Neuroscience, found that repeated concussions resulted in thicker, denser bones in the skull.
It is unclear whether this thickening of the skull is a good thing or a bad thing. In theory, a thicker skull is a stronger skull, suggesting that this may be the bone’s attempt to protect the brain from subsequent impacts.
“This is a bit of a conundrum,” Associate Professor Semple said. “As we know, repeated concussions can have negative consequences for brain structure and function. Regardless, concussion is never a good thing.”
The team hopes that the microstructural skull alterations caused by concussion are now considered by researchers in the field to better understand how concussions affect the whole body.
Concussion is a form of mild traumatic brain injury, and repeated concussions have been linked to long-term neurological consequences.
Most studies focus on understanding how these head injuries affect the brain and its function—but they largely ignore the overlying skull bones that protect the brain.
It is unclear whether this thickening of the skull is a good thing or a bad thing.
Although bones are considered a mostly structural component of the human body, bones are in fact active living tissues that can respond to applied mechanical forces.
Study collaborator Professor Melinda Fitzgerald, from Curtin University and the Perron Institute in Western Australia, has previously shown that repeated concussive impacts lead to subtle problems with memory, and evidence of brain damage.
In this new study, high-resolution neuroimaging and tissue staining techniques were used in a pre-clinical model, and revealed an increase in bone thickness and density, in close proximity to the site of injury.
“We have been ignoring the potential influence of the skull in how concussive impacts can affect the brain,” Associate Professor Semple said.
“These new findings highlight that the skull may be an important factor that affects the consequences of repeated concussions for individuals.”
Future studies are planned, with collaborator and bone expert Professor Natalie Sims from St Vincent’s Institute of Medical Research in Melbourne, to understand if a thickened skull resulting from repeated concussions alters the transmission of impact force through the skull and into the vulnerable brain tissue underneath.
Abstract
Localized, time-dependent responses of rat cranial bone to repeated mild traumatic brain injuries
While it is well-established that bone responds dynamically to mechanical loading, the effects of mild traumatic brain injury (mTBI) on cranial bone composition are unclear.
We hypothesized that repeated mTBI (rmTBI) would change the microstructure of cranial bones, without gross skull fractures.
To address this, young adult female Piebald Viral Glaxo rats received sham, 1×, 2× or 3× closed-head mTBIs delivered at 24 h intervals, using a weight-drop device custom-built for reproducible impact.
Skull bones were collected at 2 or 10 weeks after the final injury/sham procedure, imaged by micro computed tomography and analyzed at predetermined regions of interest. In the interparietal bone, proximal to the injury site, modest increases in bone thickness were observed at 2 weeks, particularly following 2× and 3× mTBI.
By 10 weeks, 2× mTBI induced a robust increase in the volume and thickness of the interparietal bone, alongside a corresponding decrease in the volume of marrow cavities in the diploë region. In contrast, neither parietal nor frontal skull samples were affected by rmTBI.
Our findings demonstrate time- and location-dependent effects of rmTBI on cranial bone structure, highlighting a need to consider microstructural alterations to cranial bone when assessing the consequences of rmTBI.
Summary: Epigenetic traces of childhood trauma can be used as biomarkers to predict the risk of addiction, depression, and a range of other physical and mental health issues 17 years later.
Source: Virginia Commonwealth University
New research from Virginia Commonwealth University’s School of Pharmacy brings the medical community closer to identifying children with the highest need for treatment and intervention following traumatic events.
The study, published in Molecular Psychiatry, found that epigenetic traces of childhood trauma could be used as biomarkers to predict the risk of depression, nicotine dependence, alcohol use disorder and other health issues in people nearly 17 years later.
“If two children are exposed to the same traumatic event, one may experience much more severe consequences than the other as an adult,” said Edwin van den Oord, Ph.D., professor and director of the Center for Biomarker Research & Precision Medicine at the VCU School of Pharmacy, who was the lead author of the study.
“Our biology can sometimes respond to trauma, and by looking at DNA responses associated with trauma, we’ve developed a novel tool for predicting long-term health risks.”
To determine whether a child’s trauma increases their health risks later in life, the research team looked at epigenetics, when adverse experiences trigger molecular modifications to one’s DNA. These changes could help capture the personal impact of trauma on a child.
Epigenetic changes are molecular changes that may influence how a gene is expressed without altering the DNA sequence. One commonly studied epigenetic change is DNA methylation, where a methyl group is added to a DNA molecule.
“Changes to DNA methylation can occur at different points in our lives depending on several factors, such as our development, age, diet, health habits and other life circumstances, like trauma,” said Karolina Aberg, Ph.D., associate director of the Center for Biomarker Research & Precision Medicine and one of the study’s co-authors.
To better understand the epigenetic impact of childhood trauma, the scientists analyzed blood samples, clinical data and other assessments collected as part of the Great Smoky Mountain Study, a 30-year project established by Duke University and the North Carolina Department of Health and Human Services that surveyed hundreds of children and adolescents into adulthood.
“Most participants began their involvement in this study when they were 9 to 13 years old. These individuals are now in their 30s,” Aberg said. “There are few studies in the world that have collected this kind of data for so long.”
The researchers first used the participants’ blood samples to measure almost 28 million individual sites for methylation in their DNA. They then identified methylation changes correlated with reported exposure to trauma, such as serious injuries, sexual violence and actual or threatened risk of death.
Using machine learning to link trauma-related methylation changes experienced in childhood to clinical data collected in adulthood, the team generated methylation risk scores for different adverse consequences. This included psychiatric disorders, physical health issues, substance abuse, poverty and social problems.
Analyses revealed that the risk scores could predict a participant’s health issues and other adversities nearly 17 years after their exposure to trauma.
Analyses revealed that the risk scores could predict a participant’s health issues and other adversities nearly 17 years after their exposure to trauma.
Their results also showed that the methylation risk scores were a better predictor of negative outcomes compared to reports of the occurrence of traumatic experiences. Van den Oord explains that this is possibly because methylation changes capture the person-specific impact of childhood trauma.
“DNA methylation has better predictive power because it’s not just saying whether a child experienced trauma, but rather it’s showing us how that child is responding to trauma,” he said.
The predictive power of the methylation risk scores could also be helpful in situations when a child’s trauma is difficult to assess with standard tools, such as in the case of sexual abuse or neglect, or when children are not able to verbalize the impact of traumatic events.
Looking ahead, the research team aims to test the methylation risk scores on a broad spectrum of populations to further evaluate their clinical potential.
“This study has shown that methylation biomarkers could potentially help identify those most at risk of experiencing trauma-related health issues,” van den Oord said. “If we can determine who is the most in need of preventive care, we can tailor their treatments and support networks to put them on the best path for recovery.”
Abstract
DNA methylation signatures of childhood trauma predict psychiatric disorders and other adverse outcomes 17 years after exposure
Childhood trauma is robustly linked to a broad range of adverse outcomes with consequences persisting far into adulthood. We conducted a prospective longitudinal study to predict psychiatric disorders and other adverse outcomes from trauma-related methylation changes 16.9 years after trauma exposure in childhood.
Methylation was assayed using a sequencing-based approach that provides near-complete coverage of all 28 million sites in the blood methylome. Methylation data involved 673 assays from 489 participants aged 13.6 years (SD = 1.9) with outcomes measures collected at age 30.4 (SD = 2.26).
For a subset of 303 participants we also generated methylation data in adulthood. Trauma-related methylation risk scores (MRSs) significantly predicted adult depression, externalizing problems, nicotine dependence, alcohol use disorder, serious medical problems, social problems and poverty.
The predictive power of the MRSs was higher than that of reported trauma and could not be explained by the reported trauma, correlations with demographic variables, or a continuity of the predicted health problems from childhood to adulthood. Rather than measuring the occurrence of traumatic events, the MRSs seemed to capture the subject-specific impact of trauma.
The majority of predictive sites did not remain associated with the outcomes suggesting the signatures of trauma do not become biologically embedded in the blood methylome. Instead, the long-term effects of trauma therefore seemed more consistent with a developmental mechanism where the initial subject-specific impacts of trauma are magnified over time.
The MRSs have the potential to be a novel clinical biomarker for the assessment of trauma-related health risks.
Summary: Researchers created a molecular atlas of the bearded dragon’s brain and compared it to the mouse brain. Findings reveal, contrary to popular belief, mammalian brains consist of an ancient reptilian brain supplemented with new mammalian features. Both reptilian and mammalian brains evolved their own clade-specific neuron types and circuits from a common ancestral set.
Source: Max Planck Institute
These days, dragons are keeping Game of Thrones fans on their toes. But they are also providing important insights into vertebrate brain evolution, as revealed by the work of Max Planck scientists on the brain of the Australian bearded dragon Pogona vitticeps.
Vertebrate evolution took a major turn 320 million years ago when early tetrapods (animals with four limbs) transitioned from water to land, eventually giving rise to three major clades: the reptiles, the birds (an offshoot of the reptilian tree) and the mammals. Because of common ancestry, the brains of all tetrapods share a similar basal architecture established during early development.
Yet, how variations on this common “Bauplan” contributed to clade-specific attributes remains unclear.
Neuroscientists at the Max Planck Institute for Brain Research in Frankfurt tackled this question by generating a molecular atlas of the dragon brain and comparing it with one from mice.
Their findings suggest that, contrary to popular belief that a mammalian brain consists of an ancient “reptilian” brain supplemented with new mammalian features, both reptilian and mammalian brains evolved their own clade-specific neuron types and circuits, from a common ancestral set.
“Neurons are the most diverse cell types in the body. Their evolutionary diversification reflects alterations in the developmental processes that produce them and may drive changes in the neural circuits they belong to”, says Prof. Gilles Laurent, Director at the Max Planck Institute for Brain Research who led the new study published in Science.
“For example, distinct brain areas do not work in isolation, suggesting that the evolution of interconnected regions, such as the thalamus and cerebral cortex, might in some way be correlated.
“Also, a brain area in reptiles and mammals that derived from a common ancestral structure might have evolved in such a way that it remains ancestral in one clade today, while it is “modern” in the other.
“Conversely, it could be that both clades now contain a mix of common (ancient) and specific (novel) neuron types. These are the sorts of questions that our experiments tried to address”, Laurent adds.
While traditional approaches to compare developmental regions and projections in the brain do not have the necessary resolution to reveal these similarities and differences, Laurent and his team took a cellular transcriptomic approach.
Using a technique called single-cell RNA sequencing that detects a large fraction of the RNA molecules (transcriptomes) present in single cells, the scientists generated a cell-type atlas of the brain of the Australian bearded dragon Pogona vitticeps and compared it to existing mouse brain datasets.
Transcriptomic comparisons reveal shared classes of neuron types
“We profiled over 280,000 cells from the brain of Pogona and identified 233 distinct types of neurons”, explains David Hain, graduate student in the Laurent Lab and co-first author of the study.
“Computational integration of our data with mouse data revealed that these neurons can be grouped transcriptomically in common families, that probably represent ancestral neuron types”, says Hain.
In addition, he found that that most areas of the brain contain a mix of common (ancient) and specific (novel) neuron types, as shown in the figure below.
The Australian bearded dragon Pogona vitticeps. Credit: Max Planck Institute for Brain Research / G. Laurent
Graduate student Tatiana Gallego-Flores used histological techniques to map these cell types throughout the dragon brain and observed (among other) that neurons in the thalamus could be grouped in two transcriptomic and anatomical domains, defined by their connectivity to other regions of the brain.
Because these connected regions have had different fates in mammals and in reptiles, one of these regions being highly divergent, comparing the thalamic transcriptomes of these two domains proved to be very interesting. Indeed, it revealed that transcriptomic divergence matched that of the target regions.
“This suggests that neuronal transcriptomic identity somewhat reflects, at least in part, the long-range connectivity of a region to its targets.
“Since we do not have the brains of ancient vertebrates, reconstructing the evolution of the brain over the past half billion years will require connecting together very complex molecular, developmental, anatomical and functional data in a way that is self-consistent. We live in very exciting times, because this is becoming possible”, concludes Laurent.
Abstract
Molecular diversity and evolution of neuron types in the amniote brain
The existence of evolutionarily conserved regions in the vertebrate brain is well established. The rules and constraints underlying the evolution of neuron types, however, remain poorly understood.
To compare neuron types across brain regions and species, we generated a cell type atlas of the brain of a bearded dragon and compared it with mouse datasets.
Conserved classes of neurons could be identified from the expression of hundreds of genes, including homeodomain-type transcription factors and genes involved in connectivity.
Within these classes, however, there are both conserved and divergent neuron types, precluding a simple categorization of the brain into ancestral and novel areas.
In the thalamus, neuronal diversification correlates with the evolution of the cortex, suggesting that developmental origin and circuit allocation are drivers of neuronal identity and evolution.
Summary: Exposure to air pollution within the first 6 months of life alters a child’s microbiome, increasing the risk for allergies, diabetes, obesity, and influencing brain development.
Source: University of Colorado
Exposure to air pollution in the first six months of life impacts a child’s inner world of gut bacteria, or microbiome, in ways that could increase risk of allergies, obesity and diabetes, and even influence brain development, suggests new University of Colorado Boulder research.
The study, published this month in the journal Gut Microbes, is the first to show a link between inhaled pollutants—such as those from traffic, wildfires and industry—and changes in infant microbial health during this critical window of development.
Previous research by the same group found similar results in young adults.
“This study adds to the growing body of literature showing that air pollution exposure, even during infancy, may alter the gut microbiome, with important implications for growth and development,” said senior author Tanya Alderete, assistant professor of Integrative Physiology at CU Boulder.
At birth, an infant hosts little resident bacteria. Over the first two to three years of life, exposure to mother’s milk, solid food, antibiotics and other environmental influences shape which microorganisms take hold.
Those microbes, and the metabolites, or byproducts, they produce when they break down food or chemicals in the gut, influence a host of bodily systems that shape appetite, insulin sensitivity, immunity, mood and cognition.
While many are beneficial, some microbiome compositions have been associated with Chrohn’s disease, asthma, type 2 diabetes, and other chronic illnesses.
“The microbiome plays a role in nearly every physiological process in the body, and the environment that develops in those first few years of life sticks with you,” said first author Maximilian Bailey, who graduated in May with a master’s in Integrative Physiology and is now a medical student at Stanford University.
Boosting inflammation
For the study, the researchers obtained fecal samples from 103 healthy, primarily breast-fed Latino infants enrolled in the Southern California Mother’s Milk Study and used genetic sequencing to analyze them.
Using their street addresses and data from the U.S. Environmental Protection Agency’s Air Quality System, which records hourly data from monitoring systems, they estimated exposure to PM2.5 and PM10 (fine inhalable particles from things like factories, wildfires and construction sites) and Nitrogen Dioxide (NO2), a gas largely emitted from cars.
“Overall, we saw that ambient air pollution exposure was associated with a more inflammatory gut-microbial profile, which may contribute to a whole host of future adverse health outcomes,” said Alderete.
For instance, infants with the highest exposure to PM2.5 had 60% less Phascolarctobacterium, a beneficial bacterium known to decrease inflammation, support gastrointestinal health and aid in neurodevelopment. Those with the highest exposure to PM10 had 85% more of the microorganism Dialister, which is associated with inflammation.
Disadvantaged communities at higher risk
In a previous study, Alderete found that pregnant Latino women exposed to higher levels of air pollution during pregnancy have babies who grow unusually fast in the first month after birth, putting them at risk for obesity and related diseases later in life.
Infants are particularly vulnerable to the health hazards of air pollution because they breathe faster and their gut microbiome is just taking shape.
“This makes early life a critical window where exposure to air pollution may have disproportionately deleterious health effects,” they write.
Racial minorities and low-income communities, who tend to work, live and attend school in regions closer to busy highways or factories, are at even greater risk. One 2018 Environmental Protection Agency study found that communities of color are exposed to as much as 1.5 times more airborne pollutants than their white counterparts.
At birth, an infant hosts little resident bacteria.
“Our findings highlight the importance of addressing the impact of pollution on disadvantaged communities and point to additional steps all families can take to protect their health,” said Alderete, who hopes her research will influence policymakers to move schools and affordable housing projects away from pollution sources.
The authors caution that more research is needed to determine whether changes in the gut in infancy have lasting impacts, and just what those are. More studies are underway.
Meantime, Alderete advises everyone to take these steps to reduce their exposure to both indoor and outdoor pollutants:
Avoid walking outdoors in high traffic zones
Consider a low-cost air-filtration system, particularly for rooms children spend a lot of time in
If you are cooking, open the windows
And for new moms, breastfeed for as long as possible
“Breast milk is a fantastic way to develop a healthy microbiome and may help offset some of the adverse effects from environmental exposures,” Alderete said.
Abstract
Postnatal exposure to ambient air pollutants is associated with the composition of the infant gut microbiota at 6-months of age
Epidemiological studies in adults have shown that exposure to ambient air pollution (AAP) is associated with the composition of the adult gut microbiome, but these relationships have not been examined in infancy.
We aimed to determine if 6-month postnatal AAP exposure was associated with the infant gut microbiota at 6 months of age in a cohort of Latino mother-infant dyads from the Southern California Mother’s Milk Study (n = 103).
We estimated particulate matter (PM2.5 and PM10) and nitrogen dioxide (NO2) exposure from birth to 6-months based on residential address histories. We characterized the infant gut microbiota using 16S rRNA amplicon sequencing at 6-months of age. At 6-months, the gut microbiota was dominated by the phyla Bacteroidetes, Firmicutes, Proteobacteria, and Actinobacteria.
Our results show that, after adjusting for important confounders, postnatal AAP exposure was associated with the composition of the gut microbiota. As an example, PM10 exposure was positively associated with Dialister, Dorea, Acinetobacter, and Campylobacter while PM2.5 was positively associated with Actinomyces.
Further, exposure to PM10 and PM2.5 was inversely associated with Alistipes and NO2 exposure was positively associated with Actinomyces, Enterococcus, Clostridium, and Eubacterium. Several of these taxa have previously been linked with systemic inflammation, including the genera Dialister and Dorea.
This study provides the first evidence of significant associations between exposure to AAP and the composition of the infant gut microbiota, which may have important implications for future infant health and development.
Summary: A new study sheds light on why humans often use hand movements while talking. Researchers report rhythmic hand gestures affect rib cage movements, leading to a change in lung volume and ultimately aspects of the voice. Infants connect early vocal babbling with hand gestures, demonstrating an early connection between movement and vocal production.
Source: GWZ
Researchers from Radboud University and ZAS Berlin have developed a new perspective on why humans often move their hands rhythmically during speaking.
The perspective published in Neuroscience and Biobehavioral Reviews, suggests that there are striking connections between animal and human behavior when it comes to moving with sounds.
For example, flying bats synchronize their echo-locating vocalization and their wingbeats which can be directly related to how humans synchronize acoustic features of their voice and move their upper limbs.
“When a bat echo-locates while flying, the muscle tensioning that drive the wingbeats also leads to small compressions of the lungs. It becomes more economical for the bat to vocalize during these particular moments of the wingbeat cycle, leading to synchronization,” says researcher Wim Pouw at the Donders Center for Brain, Cognition, and Behavior.
Pouw and his collaborator, Susanne Fuchs from Leibniz-Center General Linguistics (ZAS) suggest that this is comparable to what happens when humans produce rhythmic hand gestures, as another line of research has shown that these hand gestures affect rib cage movements, which slightly change the volume of the lungs, and thereby change aspects of the voice.
“Once we started reading up on very different lines of research, we were astonished how prevalent it is for animals to time their vocalizations together with movements. We discovered that coupling movement and vocalization might be very important for the development of vocal repertoires,” Dr. Fuchs says.
In a particular kind of bird, for example, flightless chicklets have a very typical vocalization. But the vocalization quality drastically changes when the chicklets start using their wings in the nest to practice flying. Vocalization becomes similar to adult vocalizations when they start using their wings for flight.
These systems physically interacted throughout evolution, and this development is in a way mirrored by infants who start to learn to move and vocalize at the same time.
“This is exactly what is found in human infants around nine months of age,” Pouw says. “When infants start to rhythmically ‘babble’ with their hands in an exploratory fashion, they also start to ‘babble’ in speech in the form of reduplicated syllables such as ‘mama’ or ‘papa.’” Rhythmic movements may thus have very early connections with the voice, which explains why movement and sounds are so fundamentally related.
This new perspective of how gesture relates to the voice via interactions with respiration provides an answer to why humans started to move their hands while vocalizing and speaking: These systems physically interacted throughout evolution, and this development is in a way mirrored by infants who start to learn to move and vocalize at the same time.
“Many researchers of communication believe that manual gestures were for showing things,” Pouw says. “But we actually think this not the whole story… in a way gestures are also part of what it means for humans to speak, which is not a passive affair, but an orchestra of movement to generate meaning.”
Abstract
Origins of vocal-entangled gesture
Gestures during speaking are typically understood in a representational framework: they represent absent or distal states of affairs by means of pointing, resemblance, or symbolic replacement. However, humans also gesture along with the rhythm of speaking, which is amenable to a non-representational perspective.
Such a perspective centers on the phenomenon of vocal-entangled gestures and builds on evidence showing that when an upper limb with a certain mass decelerates/accelerates sufficiently, it yields impulses on the body that cascade in various ways into the respiratory–vocal system. It entails a physical entanglement between body motions, respiration, and vocal activities. It is shown that vocal-entangled gestures are realized in infant vocal–motor babbling before any representational use of gesture develops.
Similarly, an overview is given of vocal-entangled processes in non-human animals. They can frequently be found in rats, bats, birds, and a range of other species that developed even earlier in the phylogenetic tree.
Thus, the origins of human gesture lie in biomechanics, emerging early in ontogeny and running deep in phylogeny.
Summary: Circadian rhythm disruption is a psychopathological factor shared by a broad range of mental illnesses.
Source: UC Irvine
Anxiety, autism, schizophrenia and Tourette syndrome each have their own distinguishing characteristics, but one factor bridging these and most other mental disorders is circadian rhythm disruption, according to a team of neuroscience, pharmaceutical sciences and computer science researchers at the University of California, Irvine.
In an article published recently in the Nature journal Translational Psychiatry, the scientists hypothesize that CRD is a psychopathology factor shared by a broad range of mental illnesses and that research into its molecular foundation could be key to unlocking better therapies and treatments.
“Circadian rhythms play a fundamental role in all biological systems at all scales, from molecules to populations,” said senior author Pierre Baldi, UCI Distinguished Professor of computer science. “Our analysis found that circadian rhythm disruption is a factor that broadly overlaps the entire spectrum of mental health disorders.”
Lead author Amal Alachkar, a neuroscientist and professor of teaching in UCI’s Department of Pharmaceutical Sciences, noted the challenges of testing the team’s hypothesis at the molecular level but said the researchers found ample evidence of the connection by thoroughly examining peer-reviewed literature on the most prevalent mental health disorders.
“The telltale sign of circadian rhythm disruption – a problem with sleep – was present in each disorder,” Alachkar said.
“While our focus was on widely known conditions including autism, ADHD and bipolar disorder, we argue that the CRD psychopathology factor hypothesis can be generalized to other mental health issues, such as obsessive-compulsive disorder, anorexia nervosa, bulimia nervosa, food addiction and Parkinson’s disease.”
Circadian rhythms regulate our bodies’ physiological activity and biological processes during each solar day. Synchronized to a 24-hour light/dark cycle, circadian rhythms influence when we normally need to sleep and when we’re awake.
They also manage other functions such as hormone production and release, body temperature maintenance and consolidation of memories. Effective, nondisrupted operation of this natural timekeeping system is necessary for the survival of all living organisms, according to the paper’s authors.
Circadian rhythms are intrinsically sensitive to light/dark cues, so they can be easily disrupted by light exposure at night, and the level of disruption appears to be sex-dependent and changes with age. One example is a hormonal response to CRD felt by pregnant women; both the mother and the fetus can experience clinical effects from CRD and chronic stress.
“An interesting issue that we explored is the interplay of circadian rhythms and mental disorders with sex,” said Baldi, director of UCI’s Institute for Genomics and Bioinformatics. “For instance, Tourette syndrome is present primarily in males, and Alzheimer’s disease is more common in females by a ratio of roughly two-thirds to one-third.”
Age also is an important factor, according to scientists, as CRD can affect neurodevelopment in early life in addition to leading to the onset of aging-related mental disorders among the elderly.
Baldi said an important unresolved issue centers on the causal relationship between CRD and mental health disorders: Is CRD a key player in the origin and onset of these maladies or a self-reinforcing symptom in the progression of disease?
To answer this and other questions, the UCI-led team suggests an examination of CRD at the molecular level using transcriptomic (gene expression) and metabolomic technologies in mouse models.
Circadian rhythms regulate our bodies’ physiological activity and biological processes during each solar day.
“This will be a high-throughput process with researchers acquiring samples from healthy and diseased subjects every few hours along the circadian cycle,” Baldi said.
“This approach can be applied with limitations in humans, since only serum samples can really be used, but it could be applied on a large scale in animal models, particularly mice, by sampling tissues from different brain areas and different organs, in addition to serum. These are extensive, painstaking experiments that could benefit from having a consortium of laboratories.”
He added that if the experiments were conducted in a systematic way with respect to age, sex and brain areas to investigate circadian molecular rhythmicity before and during disease progression, it would help the mental health research community identify potential biomarkers, causal relationships, and novel therapeutic targets and avenues.
This project involved scientists from UCI’s Department of Pharmaceutical Sciences, Center for the Neurobiology of Learning and Memory, Department of Computer Science, Department of Neurobiology and Behavior, and Institute for Genomics and Bioinformatics; as well as UCLA’s Oppenheimer Center for Neurobiology of Stress and Resilience and Goodman-Luskin Microbiome Center.
Abstract
The hidden link between circadian entropy and mental health disorders
The high overlapping nature of various features across multiple mental health disorders suggests the existence of common psychopathology factor(s) (p-factors) that mediate similar phenotypic presentations across distinct but relatable disorders.
In this perspective, we argue that circadian rhythm disruption (CRD) is a common underlying p-factor that bridges across mental health disorders within their age and sex contexts.
We present and analyze evidence from the literature for the critical roles circadian rhythmicity plays in regulating mental, emotional, and behavioral functions throughout the lifespan.
A review of the literature shows that coarse CRD, such as sleep disruption, is prevalent in all mental health disorders at the level of etiological and pathophysiological mechanisms and clinical phenotypical manifestations.
Finally, we discuss the subtle interplay of CRD with sex in relation to these disorders across different stages of life.
Our perspective highlights the need to shift investigations towards molecular levels, for instance, by using spatiotemporal circadian “omic” studies in animal models to identify the complex and causal relationships between CRD and mental health disorders.
Scanning electron micrograph of monkeypox virus (orange) on the surface of infected cells. NIAID
Just over three months ago, public health authorities in the U.K., Europe, and the U.S. began to sound the alarm on the arrival of monkeypox. Since then, this long-neglected tropical disease — which until this year was mostly limited to periodic spillovers in the areas of Western and Central Africa where the virus is endemic — has gone global. As of Aug. 26, 100 countries had reported nearly 47,000 cases, according to the World Health Organization.
Unlike with SARS-CoV-2, they’re not starting from scratch. Monkeypox is not a new virus. It was first discovered in research monkeys at a lab in Denmark in 1958, and identified as a human pathogen in 1970. But with little attention from the international community, monkeypox research received scant funding over the ensuing decades, leaving many key questions about the virus unanswered. The current outbreak, which is unique both in the speed of spread and the ways in which people are becoming infected, has also prompted new ones.
STAT examined some of the most pressing of these questions, many of which won’t be resolved without more time and data. Others may remain mysteries. But at least in some cases, emerging evidence is beginning to provide clues to what the eventual answers may be — clues that are likely to shape how public health agencies and health care systems respond to the current outbreak, and where it goes from here.
Where does the damn thing come from?
One thing we know: Monkeys aren’t the original source of the monkeypox virus. What is the actual reservoir host? That is an important but unanswered question.
A reservoir is a species that can carry a pathogen without being sickened by it. Bats, for instance, are thought to be reservoirs for all sorts of nasty viruses — Marburg virus, its cousins, the various species of Ebola, and untold numbers of coronaviruses, among others. These viruses can be deadly if they manage to make their way from bats to other species, including our own. But there’s no evidence they harm bats in any way.
As we’ve mentioned already, monkeypox got its name because monkeys were the first species seen to be infected with this poxvirus. But it was noticed because the virus made the monkeys ill, meaning they weren’t the reservoir.
Many species of animals can contract monkeypox. Hedgehogs, shrews, squirrels, anteaters, prairie dogs — all these can contract the virus, and, under certain circumstances, transmit it to people.
But all the identified rodents and other small mammals are victims of the virus, not the reservoir, Jean-Jacques Muyembe, the legendary microbiologist who runs the National Institute of Biological Research in the Democratic Republic of the Congo, cautioned during a recent panel discussion hosted by the Harvard Global Health Institute.
The search for the source continues. That fact underscores an important truth about monkeypox. Even if this multi-national outbreak is stopped, monkeypox will remain a threat.
(A quick P.S.: The rapid geographic spread of monkeypox has sparked fears that the virus will get seeded into susceptible species in parts of the world where it hasn’t traditionally been found, enlarging the area in which it is endemic.
The Centers for Disease Control and Prevention and other health authorities have warned people who contract monkeypox to refrain from contact with any pets they might have, for that very reason. And a recently published letter in The Lancet revealed the wisdom of that advice. A dog owned by two gay men in Paris appears to have contracted monkeypox from them.)
Why are lesions localized in some people who contract monkeypox, and disseminated in others?
Some people who contract monkeypox develop lesions over a variety of body parts — the torso, the face, the soles of feet, the palms of hands, and especially in this outbreak, which is occurring mostly in gay and bisexual men who have sex with men, in the anogenital area.
Some of the men infected in this outbreak have had their lesions situated almost exclusively on their penises or in or around their anuses.
Some, perplexingly, have had only a few lesions. Some diagnosed cases have had a single lesion.
Why this puzzling range of manifestations of lesions? This is something science doesn’t currently have an answer for, said Anne Rimoin, a monkeypox expert at the University of California, Los Angeles. “It could be the dose,” she said, referring to the amount of virus a person is exposed to when contracting monkeypox. In other words, it may be a matter of whether exposure was the result of fleeting contact with lesions or a more protracted event. Other factors may include the route of exposure — skin-to-skin or inhaled droplets, for instance. The immune status of the person being infected could also influence this outcome. “But it’s probably a combination of these elements,” Rimoin said.
What role are asymptomatic individuals playing in transmission?
Monkeypox prefers to replicate in the skin and mucous membranes. That’s why scientists tend to find the highest concentrations of virus in the lesions of infected individuals. It’s also why it would be surprising if people without such lesions were spreading monkeypox to others.
But several small studies have begun to raise concerns about that possibility.
During a retrospective screening of anorectal swabs collected from more than 200 asymptomatic men at a sexual health clinic in Paris, French researchers found virus on 13 samples. One of the men later developed an anal rash and the other experienced sore throat and fever. None of the others ever reported symptoms. A similar study, not yet peer-reviewed, from researchers in Belgium found three positive samples out of 224 asymptomatic individuals.
But it’s still not clear whether people without symptoms can pass monkeypox on to others. If they can, then post-exposure ring vaccination strategies might not be sufficient to contain further spread of the virus. (Ring vaccination involves immunizing individuals who have been exposed to monkeypox through close contact with an infected person. The idea is to catch people early enough that their immune systems can nip a potential infection in the bud before they become contagious.)
Getting a better grip on the extent of asymptomatic spread will require much more testing, including at-home, self-administered tests, said Celine Gounder, an infectious disease epidemiologist and editor-at-large for public health at Kaiser Health News.
“We need to start getting tests in people’s hands and making it possible for somebody to swab themselves,” Gounder said. “That would really help us get more data on this question.”
Can monkeypox, like Ebola, pose a post-infection risk of transmission?
Monkeypox is a poxvirus, as its name implies. Ebola is a filovirus. These are different beasts.
And yet a quirk of Ebola viruses — and their close cousin, Marburg virus — is casting a shadow over the current monkeypox outbreak.
Filoviruses can squirrel themselves away in parts of the body where immune system weaponry cannot reach them. These are known as “privileged sites” — the eyeball, synovial fluid (the fluid in joints), spinal fluid, and most importantly for this discussion, the testicles.
From the very earliest days of recorded outbreaks of filoviruses, there was a suspicion that survivors could harbor viruses and pass them to others, primarily through sex. Later, it became clear that viral persistence, as it is called, is a feature of these infections. A portion of people who survive filovirus infections will suffer a relapse later; a Scottish nurse infected when she worked on the West African Ebola outbreak in 2014 had two subsequent resurgences of illness. In other cases, male survivors have infected sex partners months, even years after recovering.
It is not known if monkeypox virus can similarly lodge in testicles and pose a post-infection transmission risk. But the fact that scientists are discovering monkeypox viral DNA in semen, and in one case even managing to grow live virus from semen, is raising the question.
It is thought that monkeypox is a one-and-done infection, that people who survive — as most people do — have life-long immunity. They cannot be reinfected and pose no transmission risk after they recover. But that calculus changes if survivors have monkeypox virus hiding in their testicles or other parts of their bodies.
Because of the unanswered questions, the Health Security Agency in the United Kingdom is recommending men who have had monkeypox wear condoms during sex for at least 12 weeks after recovering. The CDC says wearing condoms is advisable, but at present there is little data on which to make such a recommendation.
Do people who have recovered from monkeypox pose a near-term or longer-term transmission risk? It’s an important question that needs to be answered. With such a large pool of monkeypox survivors to study, this outbreak should provide opportunities to do so.
How well does the vaccine work at reducing symptoms and preventing infections?
Both the CDC and the WHO estimate that the available smallpox vaccines are about 85% effective against monkeypox. But experts caution that the highly cited figure should not be taken at face value, particularly in the context of the current outbreak.
The figure dates back to an observational study involving 245 people infected with monkeypox in Zaire (now the Democratic Republic of the Congo) between 1981 and 1986, and more than 2,000 of their contacts. Individuals who had a visible scar from a jab with the first-generation smallpox vaccine were about seven times less likely to contract monkeypox after exposure to an infected person than those who were unvaccinated.
Another study, also conducted in Zaire in the 1980s by the same WHO monkeypox surveillance team, took a closer look at how the vaccine impacted the severity of symptoms. Among 282 patients — the vast majority of them children under the age of 15 — unvaccinated individuals were twice as likely to have large numbers of lesions crop up, and three times as likely to have multiple lesions in the genital area.
Without a smallpox shot, monkeypox patients sometimes suffered gruesome outcomes, including complications that could turn deadly. The researchers reported that one out of 10 unvaccinated monkeypox patients died, with even higher fatality rates among the youngest children. One 5-year-old boy endured more than 4,500 lesions before succumbing to blood poisoning caused by a secondary bacterial infection. In contrast, none of the vaccinated patients died.
The historic smallpox vaccines administered in these studies are no longer in production. But newer ones, like MVA-BN, a third-generation smallpox vaccine manufactured by Bavarian Nordic, are expected to have similar efficacy against monkeypox, based on studies in people that showed comparable antibody responses. However, they haven’t been directly tested against the disease in clinical trials.
MBA-BN, known in the U.S. as Jynneos, is currently the only vaccine in this country licensed by the Food and Drug Administration to prevent monkeypox infection. Its initial approval for smallpox was based on favorable data from nearly two dozen clinical trials with more than 7,500 participants. But when the agency later approved the vaccine for monkeypox, its decision was based on data from animal experiments, including non-human primate studies. Eighty to 100% of the monkeys who got the jab later survived a lethal dose of the virus, compared to zero to 40% of the placebo group.
“I’m not aware of any good data on vaccine protection,” said Rimoin. Surveillance studies conducted by her group in the 2000s found hints that first-generation shots had been effective; 30 years after mass smallpox vaccination campaigns ceased in central Africa, incidence of monkeypox cases there increased 20-fold.
But she doubts that such data can be extrapolated to the current outbreak — which is primarily spreading through sexual contact. Mucosal surfaces are easier for the virus to infect, and the prolonged contact that happens during sex is likely exposing people to much larger doses of the virus than the groups of people who were studied in western and central Africa in previous decades.
“This is the crux of the problem,” said Rimoin. “I think that we are expecting more from these vaccines than they were designed for. This kind of intense, often repeat, mucosal exposures are very different from animal exposure, household, fomite, or respiratory droplet transmission.”
These perhaps outdated estimates of vaccine effectiveness are based on studies of pre-exposure vaccination. There’s even less data supporting the ring vaccination strategy being deployed by countries including the U.S., the U.K., and Canada. That strategy hinges on having rigorous contact tracing and a long incubation period in which to operate. And while the approach has proven very effective at curbing smallpox it’s not obvious yet that it will work as well for monkeypox.
So far, there’s been just a single observational study looking at the question directly. In a paper released (but not yet peer-reviewed) earlier this month, researchers in France reported that among 276 high-risk contacts who were vaccinated post-exposure, 12 of them later contracted the disease. However it’s hard to say whether these were true breakthrough infections because most of them received their shots more than a week after the exposure, outside the recommended four-day window.
“It’s possible they developed the disease because they were vaccinated a bit too late,” said Michaël Thy, a tropical infectious disease doctor at Paris Cité University who led the study. But he noted that none of the 12 who experienced symptoms required hospitalization, indicating that post-exposure vaccination may reduce the severity of infection, if not infection itself.
The study was small, and all the participants received a single dose of Jynneos so there’s no way to say whether the vaccine cut the risk of infection. The only way to do that is a randomized controlled trial — with some people getting the real deal and some people receiving a placebo shot.
Rimoin is among the researchers racing to set up such a study. If the funding comes through, her group hopes to quickly roll out trial sites in Los Angeles and the Democratic Republic of the Congo.
Until there’s more data, the most important thing that patients should know is that the vaccine, even two doses, does not provide 100% protection, said Thy. “It’s an important part of a combined strategy for lowering the risk of infection, but it’s not the only thing people should be doing.”
Will the virus continue to primarily infect men who have sex with men?
In the U.S. and Europe, monkeypox has so far primarily affected men who have sex with men. But historically, outbreaks that begin in one community do not stay there.
HIV famously spread far beyond gay and bisexual men in the ’80s, fueled in part by officials who ignored early warnings that there was no such thing as a gay disease. In the 2000s, an outbreak of drug-resistant bacteria was first spotted in gay men but ultimately spread to athletes and took its greatest toll on people in prison.
For now, monkeypox’s next move remains unclear. Much of the news is positive: The virus appears to be more difficult to transmit through casual contact than initially feared, narrowing its potential paths. Cases have also been declining in New York, San Francisco, and much of Europe, as more vaccines become available and people minimize their risk of exposure through sex.
“There are some encouraging trends,” said Chris Beyrer, an epidemiologist and incoming director of the Duke Global Health Institute. “If we can contain this epidemic of this outbreak in men who have sex with men, that is our best shot.”
And yet the news is not good everywhere. The monkeypox response has so far been marked by inequities. In North Carolina, 72% of people diagnosed with monkeypox are Black, according to data released earlier this month, but only 24% of vaccines have gone to Black residents — a glaring example of a racial disparity seen in much of the country.
The longer these disparities go unaddressed, the more likely the virus is to stick around and spread broadly, including into prisons and other overcrowded settings, or to even become endemic among animals in North America.
“We have this window of opportunity right now. We have encouraging data that vaccination and behavior change in combination are getting control of the outbreak in New York City,” said Beyrer. “ I wish the rest of the country looked like New York right now.”
When people with monkeypox die, what do they die from?
One thing that is becoming clear in this multi-country outbreak is that the monkeypox case fatality rate is not as high as was previously estimated, at least for clade II viruses (the former West African clade) and when infections are primarily in adults. Figures ranging from 1% to 3% have historically been cited. But out of the nearly 47,000 cases that have been detected so far this year, there have been roughly 15 deaths reported.
Some of the questions we’re exploring here aren’t currently answerable. For this one, there are data — though not enough. In the endemic countries, where most of the monkeypox deaths have occurred, there haven’t always been detailed records of the causes of death. But if you dig into the scientific literature, there are some clues.
In 1987, researchers from the WHO’s long-defunct smallpox eradication unit and the Democratic Republic of the Congo’s monkeypox surveillance team published a major piece of work that charted the disease course of 282 people who contracted the virus between 1980 and 1985. (We referred to this study in the section above on vaccine efficacy.) In the paper, they compared severity of symptoms and outcomes of patients who had previously been vaccinated against smallpox — a vaccine against a related virus that should offer some cross-protection against monkeypox — and those who had not.
There were no deaths among the monkeypox patients who had a smallpox vaccination scar. But among the 250 who did not, there were 27 fatal cases. All the deaths occurred in children under the age of 8, and the case fatality rate was more than twice as high among those 4 years of age and younger than among kids 5 to 9.
Nineteen of the children who died developed bronchopneumonia and pulmonary distress. One developed septicemia, an infection on the blood stream. One developed encephalitis — inflammation of the brain.
A paper on Nigeria’s 2017-2018 monkeypox, published in the journal The Lancet Infectious Diseases in 2019, reported that among 122 cases there, seven had been fatal. Four of those were people who were living with HIV but in whom the disease was untreated at the time of their monkeypox infection. They died rapidly, the authors reported, though they noted a precise cause of death was not available in these cases.
Two other deaths were attributed to secondary bacterial infections of monkeypox lesions, with apparent sepsis — a dangerous condition where the body’s attempt to curb an infection backfires and leads to organ damage. The seventh death was in a one-month-old infant.
A systematic review published in February in PLOS Neglected Tropical Diseases — presciently titled “The changing epidemiology of human monkeypox — A potential threat?” — noted that from the 1970s through the 1990s, 100% of recorded fatal monkeypox cases were in children younger than age 10. But in the first two decades of this century, pediatric deaths declined to 37.5% of monkeypox cases.
And in this outbreak? What have the fatal cases died from?
At least a couple of those patients were younger men — one 31, one 44 — who were not immunocompromised and had no underlying chronic diseases. These occurred in Spain. The men both developed encephalitis.
Some of the deaths have occurred in immunocompromised people. On Tuesday, Texas reported a fatal case in a person who was “severely immunocompromised.” Late last month Brazil recorded a death in a man who had lymphoma; Mexico recently registered a death in a man who was living with HIV. He died from septic shock and pneumonia; his death has not yet been recognized as a monkeypox-related death by the WHO. The autopsy of an Italian tourist who died recently in Cuba reportedly revealed he had sepsis linked to pneumonia and organ damage. A death in Ecuador was attributed to an unspecified pre-existing disease.
For most of the monkeypox deaths that have occurred this year, however, there isn’t a precise cause of death that has made its way into the public domain. In at least some of those cases, scientific papers are probably already in the works. So we’ll need to bide our time to get more answers.
Does having been vaccinated against smallpox decades ago protect against monkeypox today?
The age distribution of cases shows there are far fewer infections among people 60 and older — in other words, people who would have been vaccinated against smallpox when they were kids. But is that the effect of protection from previous vaccination or lower rates of exposure in older men? Or both?
It’s not 100% clear. But it is possible it has more to do with risk of exposure than residual protection from a jab given decades earlier.
The median age of cases in the global outbreak is 36. Men aged 18 to 44 make up 78% of all cases, according to WHO data. They would be too young to have been vaccinated against smallpox when they were children.
It’s apparent from some of the studies we cite in this article (see the references to the study of 282 monkeypox cases in Zaire) that even back in the 1980s, people who had been relatively recently vaccinated against smallpox could contract monkeypox. But they had a milder course of illness when they did.
A study conducted in the United States after an extraordinary monkeypox outbreak in 2003 sheds a little light here. In that event, the first recorded monkeypox outbreak outside of Africa, three of the 47 people who contracted the virus were completely asymptomatic. They had been vaccinated against smallpox when they were young — 13, 29, and 48 years earlier. Five other people previously vaccinated against smallpox developed monkeypox disease in that outbreak, but they had, in the main, fewer lesions than unvaccinated people.
How long does protection from prior smallpox vaccination last? Researchers have estimated that protection against severe disease erodes after about 32 years and protection against fatal disease lasts nearly 52 years. But those estimates are based 1) on protection against smallpox (monkeypox protection from smallpox vaccine starts out already reduced) and 2) calculated using data from a 1903 smallpox outbreak in Australia.
Has the virus changed in any consequential way — or will it?
When scientists started sequencing the viruses behind this outbreak, what was notable was just how many mutations the pathogen had picked up in a few years — and what clues those mutations contained. There was a concern early on that changes to the virus’s genome had made it more transmissible, explaining the unprecedented global spread of the virus. In actuality, though, the research has indicated that the mutations were evidence of a years-long fight with human immune systems, not signs of a fundamental change in the virus. Those genetic scars left over from past battles with immune systems also provided a roadmap for scientists, who used them to estimate that this line of viruses has been spreading among people since perhaps 2016.
Still, scientists are trying to determine if any of the mutations have given the virus some sort of advantage over other forms of the virus, even if at this point there are no obvious signs they did. But one thing they do know is that, as the virus spreads more, it has ever more chances to keep evolving and to perhaps pick up mutations that could make it even more of a threat.
What happens if individual communities contain their outbreaks?
There was a bit of good news last week: The WHO reported that cases globally had declined 21% from a week prior, largely due to a drop in newly confirmed cases from Europe. Even domestically, as we noted above, documented cases are on the decline in New York and San Francisco, as public health officials point to the impact of vaccination campaigns and behavioral changes among those most at risk, including reducing the number of sex partners people have.
Even if individual cities, or countries, can eliminate monkeypox, they won’t be able to move on entirely. They’ll have to continue surveillance to ensure the virus didn’t get established in animals locally — a source for potential future outbreaks. And with the virus still spreading elsewhere — the WHO has noted that infections are still increasing in Africa and Latin America — they’ll have to be on the lookout for reintroductions, particularly as people relax some of the behavioral changes they’ve made.
But if outbreaks are really brought under control in places in North America and Europe, the pressure on those countries to address the global problem of monkeypox will only increase. As the outbreak has shown, viruses that are defined as endemic to certain parts of the world don’t just stay there. Wealthy countries have also been criticized for not doing more to help the African nations that have animal reservoirs of the virus fight the pathogen, even as there were signs of more human-to-human transmission in recent years. Even now, as countries in Europe and North America have scooped up global vaccine supplies, those African countries don’t have access to vaccines. In the world of infectious diseases, memory is often short, and the public can quickly move on when something is no longer deemed a threat to them. We’ll see if this time is different.
Gut pathogens, their histologic features, and a GI pathology and microbiology team approach to diagnosis were the focus of a CAP21 session, “What’s Bugging the Gut?”
Maryam Zenali, MD, Alina Iuga, MD, and Christina Wojewoda, MD, presented a series of cases and highlighted the features, the differential diagnoses, and the integrated workups. Three of their cases follow here, with others to be reported in an upcoming issue.
The patient in the first case is a 14-year-old boy who presented with fever, bloody diarrhea, and abdominal pain. Endoscopic evaluation revealed mucosal edema of the right colon extending to the ileocecal valve and scattered ileocecal ulcers. Due to the severity of symptomatology, a laparotomy was performed shortly thereafter.
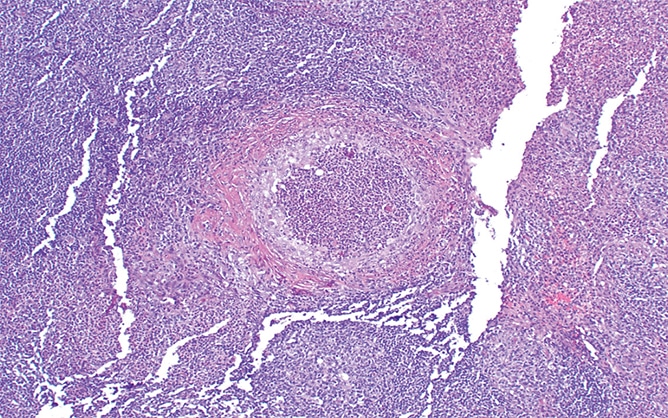
The resection specimen contained suppurative granulomatous appendicitis and active chronic enterocolitis (Figs. 1–3). Granulomatous inflammation was also noted in the endoscopic biopsies of the right colon (Fig. 4), explained Dr. Zenali, assistant professor of pathology, Department of Pathology and Laboratory Medicine, UConn Health.
“The differential diagnoses include infectious disease such as Yersinia, salmonella, or mycobacteria enterocolitis and Crohn’s disease,” she said.
This is where the microbiology laboratory can be of help, said Dr. Wojewoda, director of microbiology at the University of Vermont Medical Center and associate professor, University of Vermont Larner College of Medicine. If the patient had submitted a stool culture before returning for further surgery, she said, they could have diagnosed Yersinia enterocolitica. “Ideally we would incubate the stool at 25 degrees [Celsius] because Yersinia likes to grow at cooler temperatures.” Not every laboratory will automatically culture for Yersinia enterocolitica, “so this is where the pathologist can interact with the GI clinician or surgeon to ensure we know what we are supposed to be looking for.”
If they were to culture for Yersinia, Dr. Wojewoda said, they would look for lactose-negative colonies on the MacConkey agar. “There is a selective and differential agar for Yersinia enterocolitica called CIN agar,” on which red bull’s-eye colonies form. It can take about 48 hours to grow, and then two to 24 hours to identify the organism. PCR studies on stool are available for Yersinia enterocolitica, “although these are usually incorporated into large multiplex panels, which usually are overkill,” she said, “unless you are looking for something rare.”
Yersinia enterocolitica is a Gram-negative rod in the order Enterobacterales (previously Enterobacteriaceae). Yersinia enterocolitica and Yersinia pseudotuberculosis can be found in meats (most commonly pork), dairy products, and water. The CDC estimates it causes almost 117,000 illnesses, 640 hospitalizations, and 35 deaths in the U.S. yearly, with children infected more often than adults.
Fig. 1. Appendix H&E 40×
Yersiniosis often involves the terminal ileum/ileocecal region and mesenteric lymph nodes; it may also affect the appendix. Suppurative and granulomatous patterns are common in Yersinia enterocolitica and in particular in Yersinia pseudotuberculosis, Dr. Zenali said. “Patients can have concurrent mesenteric lymphadenitis. The organism accesses the bowel wall through the microfold [M] cells of the Peyer’s patches, so the inflammatory reaction often initiates from the terminal ileum and ileocecal valve and can further spread to the right colon.”
In immunocompromised patients Yersinia is a severe disease, as it is in patients with iron overload. “We don’t know the exact mechanism for that,” Dr. Zenali said of overload, but “we know the organism needs iron for growth, and its growth is hindered when iron is scant.”
The histology, although suggestive, is not entirely specific for Yersinia infection, and culture and/or PCR are the gold standard for definitive diagnosis.
“Mycobacteria would have caseating granulomas, and you can identify acid-fast bacterium in some of the cases, if not all,” Dr. Zenali said. Mycobacteria also favor the ileocecal valve region, as does salmonella. With salmonella, small, loose to well-formed granulomas, with neutrophilic microabscess, can be seen.
Similar to inflammatory bowel disease/Crohn’s disease, chronic bacterial infection can lead to mucosal architectural distortion. With Crohn’s disease, confluent granulomas are less likely and perianal disease or fistula more common.
Fig. 2. Appendix H&E 100×
Most cases of Y. enterocolitica and Y. pseudotuberculosis are self-limited. If treatment is needed, supportive care might be sufficient. Antibiotics are prescribed for those with more severe disease or intractable symptoms. Severe disease may lead to intestinal perforation.
Fig. 3. Resected bowel H&E 100×
Studies report identification of Yersinia by PCR in the normal colon of asymptomatic patients and also in patients with Crohn’s disease. “So the question is what is the bacterial load,” Dr. Zenali said. “We also have to interpret the results in the context of the clinical presentation.”
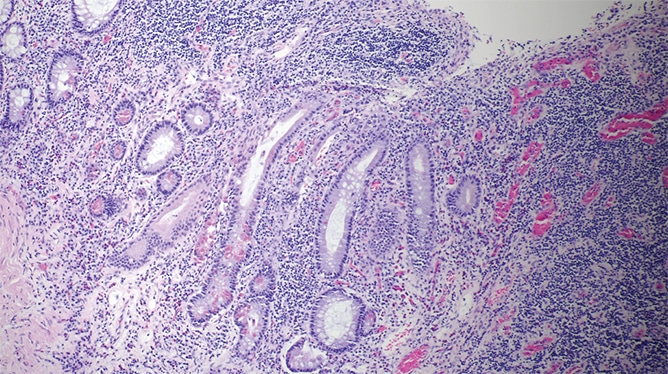
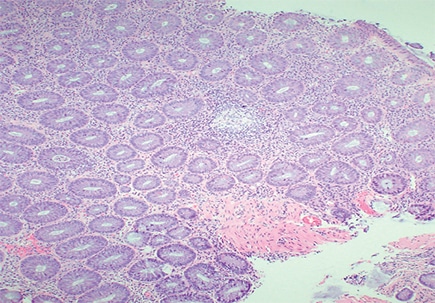
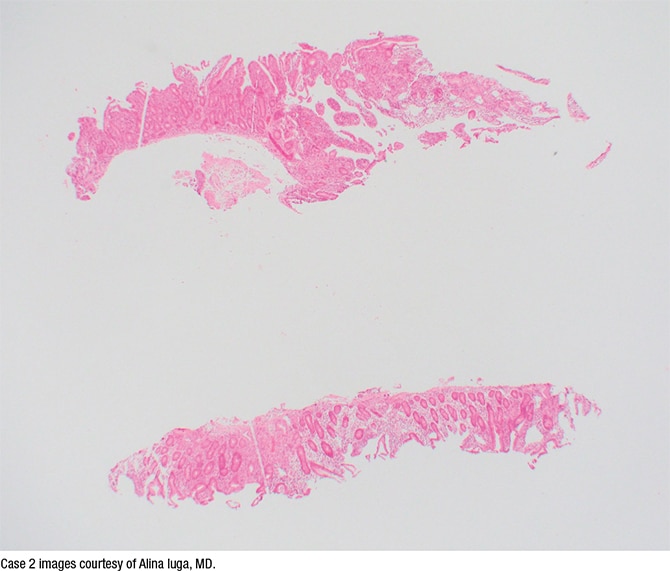
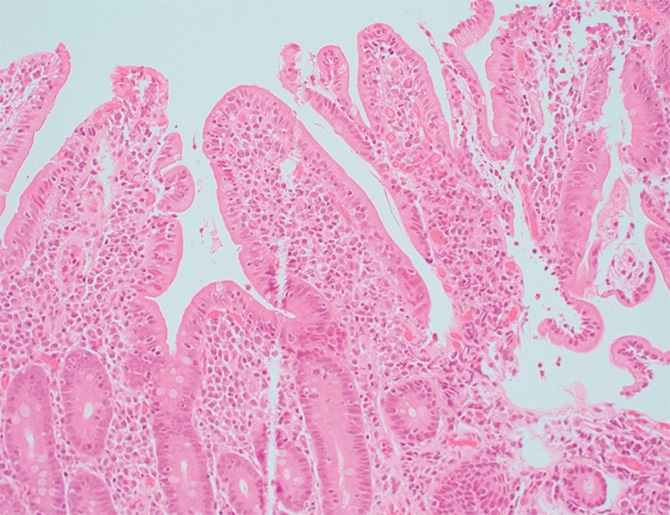
Fig. 4. Right colon biopsy H&E 40× The second case is that of a 35-year-old woman with abdominal pain referred for celiac disease evaluation based on initial histologic findings of the upper gastrointestinal endoscopic samples. The duodenal biopsy showing mild villous blunting is seen in Fig. 5. At higher magnification (Fig. 6) mild intraepithelial lymphocytosis and mild lamina propria expansion by lymphoplasmacytic infiltrate are seen.
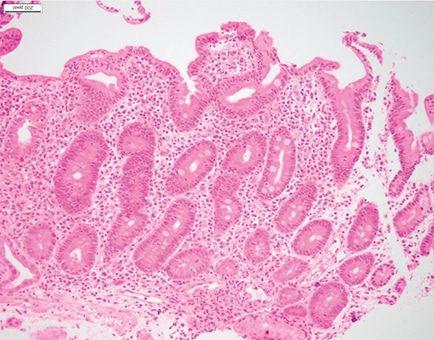
Seen in Fig. 7 is active inflammation consisting of neutrophils in lamina propria and focally in the epithelium. “Active inflammation may be seen in celiac disease as a marker of active disease, in particular in pediatric cases,” said Dr. Iuga, director of gastrointestinal pathology and associate professor, Department of Pathology and Laboratory Medicine, University of North Carolina School of Medicine. “However, when we see it, we should keep in mind the differential diagnosis that includes peptic injury, a drug effect such as NSAIDs, infectious etiology, and even inflammatory bowel disease.”
Fig. 5. H&E stain, 2×
In Fig. 8 small basophilic bodies are seen on the luminal surface of the enterocytes, and thus the differential diagnosis includes infectious parasitic organisms such as Cyclospora cayetanensis, Cystoisospora (Isospora) belli, Cryptosporidium, and Microsporidium. “The first three are members of Coccidia, which is a subclass of microscopic spore-forming, single-celled, obligate intracellular parasites that can infect epithelial cells lining the digestive tract of humans and animals,” Dr. Iuga explained. On histology, they are usually distinguished by size and location. Cryptosporidium (4–6 µm) is usually located at the luminal surface of the enterocytes. Cystoisospora is larger, averaging 20 to 30 µm in size, and Cyclospora measures 8 to 10 µm. They are usually observed inside the enterocytes. “Microsporidia, which average 1.5 to 2 µm, were formerly considered spore-forming protozoa and have been reclassified as intracellular fungi.”
Fig. 6. H&E stain, 20×
In Fig. 9 is a Giemsa stain highlighting the organisms. “Based on the morphologic appearance and the location at the surface of the enterocytes, these are compatible with Cryptosporidium,” Dr. Iuga said.
Here, too, the clinical laboratory can be of help, Dr. Wojewoda added. “If this patient had submitted a stool sample, immunofluorescent microscopy could have been performed. We can do an antigen assay for Cryptosporidium or PCR.”
Fig. 7. H&E stain, 20×
Cryptosporidium is not detected well in a routine ova and parasite exam, “which is something we don’t teach medical students very well,” Dr. Wojewoda said, adding, “I’m working on it.” In a routine O&P exam, Cryptosporidium can look like yeast, which are normal in stool. “This is a time when you can work with your GI, family medicine, and infectious diseases colleagues. Make sure they know that either a Cryptosporidium exam, antigen assay, or PCR assay is a better test.”
If they do an O&P exam, a modified acid-fast stain would be used to differentiate Cryptosporidium from yeast. “When we observe them, the oocysts are approximately four to six microns and very round.”
Multiple Cryptosporidium species can cause disease, she said, but Cryptosporidium parvum and Cryptosporidium hominis are the most common. “We get this via ingestion of unclean food or water that’s been contaminated with stool,” the latter often encountered in water parks. In 2018 there were 748,000 cryptosporidiosis cases.
Cryptosporidium organisms show small basophilic round bodies protruding from the apex of enterocytes, highlighted with Giemsa stain. “Interestingly, they are considered intracellular but extracytoplasmic in location,” Dr. Iuga said. They are located within parasitophorous vacuoles covered by the host’s microvillous membranes. “Histologically,” she said, “the small intestine mucosa can show variable villous atrophy, variable inflammation including cryptitis and lamina propria neutrophilic infiltrate, as well as intraepithelial lymphocytosis and eosinophil infiltrate.”
Fig. 8. H&E stain, 60×
Cryptosporidium can be found in lakes and rivers, especially when the water is contaminated with sewage and animal waste, and it’s resistant to chlorine disinfection and therefore can be present in drinking water. The disease is caused by ingesting infectious oocytes followed by the release of sporozoites that invade enterocytes, primarily in the small intestine. The most common sites of infection are the small intestine and proximal colon, “but they can also infect the distal colon, pancreas, respiratory tract, and, interestingly, the gallbladder and biliary tree. And there are reported cases of sclerosing cholangitis associated with Cryptosporidium infection,” Dr. Iuga said.
Cryptosporidium can cause self-limited diarrhea in immunocompetent patients and chronic diarrhea in immunocompromised patients. “It can also be a cause of malabsorption, lactose intolerance, dehydration, weight loss, and malnutrition in severe cases,” she noted. Infection is managed with supportive therapy, antiprotozoal medication, or antiretroviral therapy in HIV patients or by reducing immunosuppression in other settings.