Close to 5 million deaths are associated with antimicrobial resistance (AMR) globally in 2019
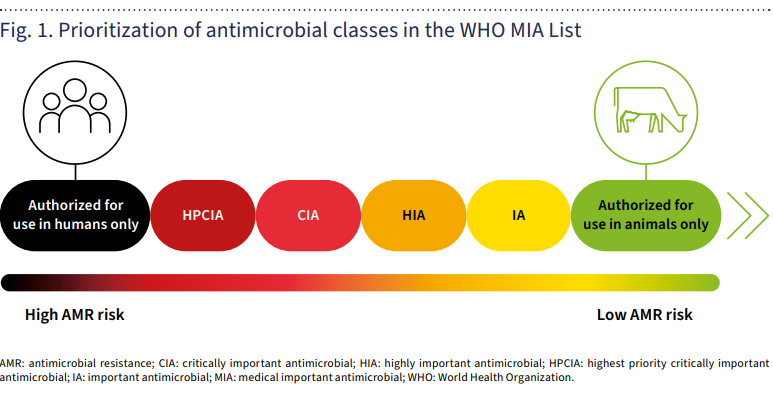
The WHO has released a first-ever list of 21 antimicrobials earmarked as “authorized for use in humans only” – a first for the organization in its efforts to protect overuse and abuse of critical first-line drugs that need to be protected by overuse in animal and plant health sectors – and consequent antimicrobial resistance (AMR).
Significantly, most of the 21 antimicrobials earmarked by WHO as “authorized for use in humans only” include mostly novel compounds developed and authorized over the past six years.
The category “mainly contains newer antimicrobials that are very important in treating serious multidrug-resistant infections in humans,” WHO explains in its guidance. So the new WHO label is effectively a warning sign to the farm industry that they should not be used in animals or plants in the future.
Among the antimicrobials authorized “for use in humans only” are: plazomicin, aminomethylcycline, anti-pseudomonal penicillins with and without β-lactamase inhibitors, carbapenems with or without inhibitors, third- and fourth-generation cephalosporins with β-lactamase inhibitors, sulfones, as well as drugs critical to treating tuberculosis and other mycobacterial diseases.
Some of the older ones on the WHO list, e.g. carbapenems, are not licensed for use in animals in the United States, but are sometimes used in companion animals.
The report aims to provide guidance for authorities in the public health and animal health sectors, veterinarians, prescribers of antimicrobials, and agricultural professionals, as well as classify antimicrobial categories by importance to human use, WHO said.
Reducing risks to human health
Antibiotics are commonly overused in animals—often without the input of veterinarians—to boost their growth and keep them from picking up infections.
A second category of medically important antimicrobials refers to drugs “authorized for use in both humans and animals.”
But this is further broken down into “highest priority critically important antimicrobials (HPCIA),” “critically important antimicrobials (CIA),” “highly important antimicrobials,” and “important antimicrobials.”
Widespread animal use of leading antibiotics has become a major driver of growing ‘superbug’ resistance to common drug treatments, or AMR. In 2019 AMR was associated with the deaths of close to 5 million people globally.
To address these risks, the use of critical antimicrobials needs to be rationalized more systematically in both animal as well as human health. WHO’s drug classifications create an order of priority for doing this, notes an analysis from the University of Minnesota-based Center for Infectious Disease Research and Policy (CIDRAP.)
“The risk to human health is greatest if the antimicrobials listed as ‘authorized for use in humans only’ are used in non-human sectors,” noted the CIDRAP analysis. “Those risks and impacts decline progressively with the use of agents from the other categories.”
“For instance, the criteria for inclusion in the first two medically important antimicrobial categories is whether the antimicrobial class is one of the limited available therapies or the sole available therapy to treat serious bacterial infections and if it’s used to treat bacterial infections possibly transmitted from non-human sources (such as Salmonella and Escherichia coli).
“Among the classes categorized as HPCIA are third- and fourth-generation cephalosporins, quinolones, and polymyxins. The CIA category includes aminoglycosides and macrolides,” CIDRAP noted.
Scale of prioritization of medically important antimicrobials (MIA)
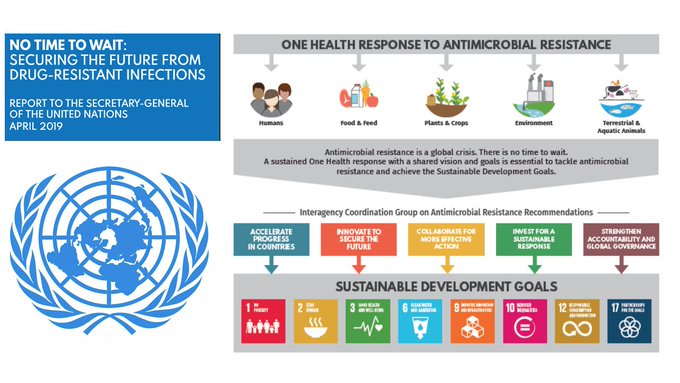
One Health and AMR
A One Health approach
The non-human use of antimicrobials in fact includes a broad range of species, beyond the historical focus on food-producing animals. These include aquaculture, companion animals, and fur-bearing animals. Reducing antimicrobial use in the non-human sector remains vital for preserving the efficacy of these substances, WHO said.
Antimicrobial resistance (AMR) occurs when pathogens like bacteria, viruses, fungi, and parasites no longer respond to antimicrobial medicines, making infections harder to treat while increasing the risk of disease spread, severe illness, and death. Infections typically treated with routine medicines thus become life threatening.
“Because AMR develops and transfers within and among all sectors, minimizing the risk of emergence and transmission of AMR calls for a One Health approach,” WHO explained in the new guidance.
“To improve the responsible and prudent use of antimicrobial agents—and in particular medically important antimicrobial agents—it is thus essential to decrease their inappropriate use across sectors.”
Additionally, the report advocates for the more systematic inclusion of medically important antimicrobials in AMR monitoring and surveillance programs – which continue to be patchy and incomplete in most countries of the world.
New WHO category ‘for use in animals only’
In addition to the existing “highly important antimicrobials” (HIA) and “important antimicrobials” (IA) classifications, the WHO now includes an “authorized for use in animals only.” This group was added to “ensure that all antimicrobials used in animals come under scrutiny as part of the standard evaluation approach, so that they would not be placed in a low priority category by default, without proper assessment of the potential risk of AMR in humans.”
Aspartame is an artificial (chemical) sweetener widely used in various food and beverage products since the 1980s, including diet drinks, chewing gum, gelatin, ice cream, dairy products such as yogurt, breakfast cereal, toothpaste and medications such as cough drops and chewable vitamins.
“Cancer is one of the leading causes of death globally. Every year, 1 in 6 people die from cancer. Science is continuously expanding to assess the possible initiating or facilitating factors of cancer, in the hope of reducing these numbers and the human toll,” said Dr Francesco Branca, Director of the Department of Nutrition and Food Safety, WHO. “The assessments of aspartame have indicated that, while safety is not a major concern at the doses which are commonly used, potential effects have been described that need to be investigated by more and better studies.”
The two bodies conducted independent but complementary reviews to assess the potential carcinogenic hazard and other health risks associated with aspartame consumption. This was the first time that IARC has evaluated aspartame and the third time for JECFA.
After reviewing the available scientific literature, both evaluations noted limitations in the available evidence for cancer (and other health effects).
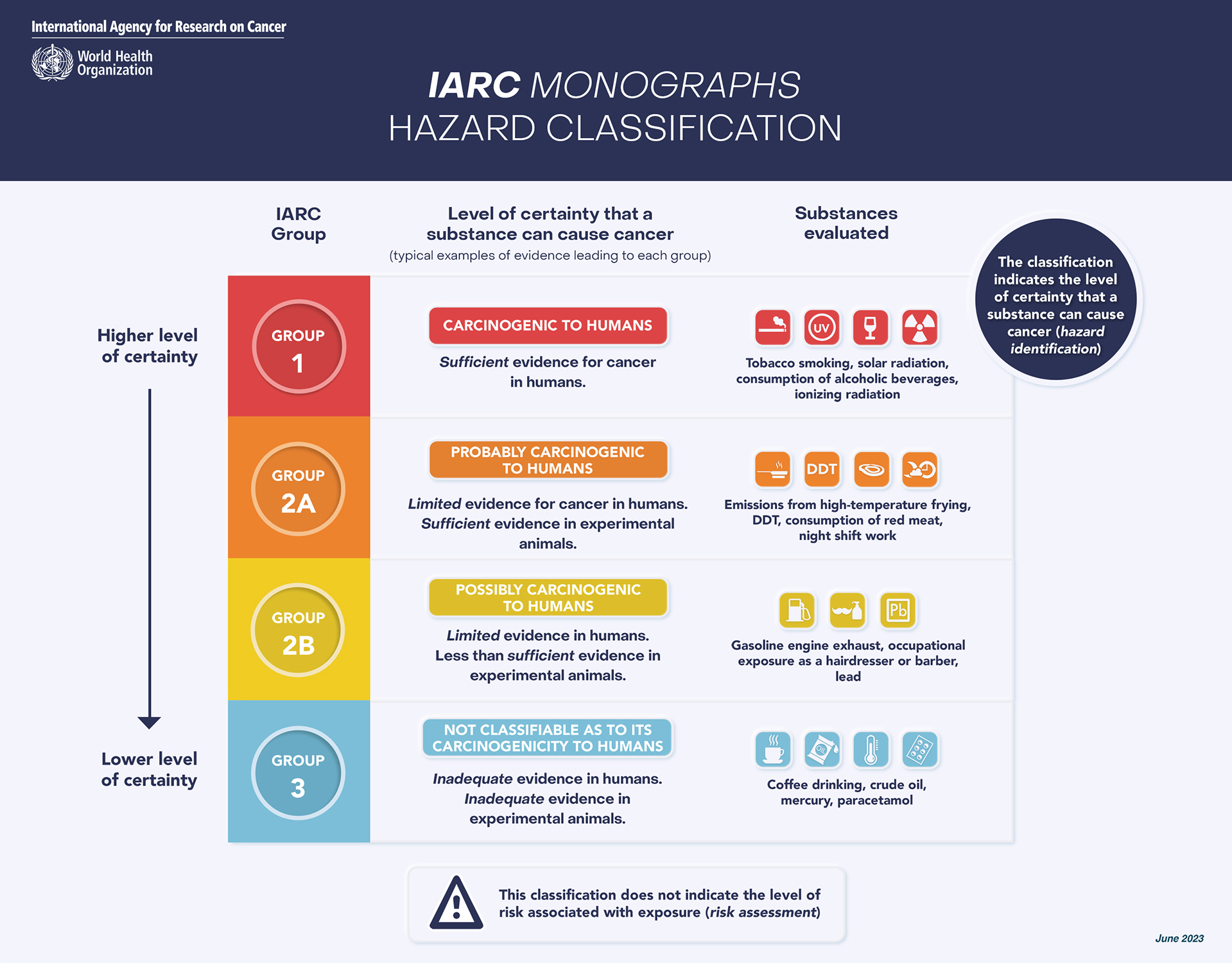
IARC classified aspartame as possibly carcinogenic to humans (Group 2B) on the basis of limited evidence for cancer in humans (specifically, for hepatocellular carcinoma, which is a type of liver cancer). There was also limited evidence for cancer in experimental animals and limited evidence related to the possible mechanisms for causing cancer.
JECFA concluded that the data evaluated indicated no sufficient reason to change the previously established acceptable daily intake (ADI) of 0–40 mg/kg body weight for aspartame. The committee therefore reaffirmed that it is safe for a person to consume within this limit per day. For example, with a can of diet soft drink containing 200 or 300 mg of aspartame, an adult weighing 70kg would need to consume more than 9–14 cans per day to exceed the acceptable daily intake, assuming no other intake from other food sources.
IARC’s hazard identifications are the first fundamental step to understand the carcinogenicity of an agent by identifying its specific properties and its potential to cause harm, i.e. cancer. IARC classifications reflect the strength of scientific evidence as to whether an agent can cause cancer in humans, but they do not reflect the risk of developing cancer at a given exposure level. The IARC hazard evaluation considers all types of exposures (e.g. dietary, occupational). The strength-of-evidence classification in Group 2B is the third highest level out of 4 levels, and it is generally used either when there is limited, but not convincing, evidence for cancer in humans or convincing evidence for cancer in experimental animals, but not both.
“The findings of limited evidence of carcinogenicity in humans and animals, and of limited mechanistic evidence on how carcinogenicity may occur, underscore the need for more research to refine our understanding on whether consumption of aspartame poses a carcinogenic hazard,” said Dr Mary Schubauer-Berigan of the IARC Monographs programme.
JECFA’s risk assessments determine the probability of a specific type of harm, i.e. cancer, to occur under certain conditions and levels of exposure. It is not unusual for JECFA to factor IARC classifications into its deliberations.
“JECFA also considered the evidence on cancer risk, in animal and human studies, and concluded that the evidence of an association between aspartame consumption and cancer in humans is not convincing,” said Dr Moez Sanaa, WHO’s Head of the Standards and Scientific Advice on Food and Nutrition Unit. “We need better studies with longer follow-up and repeated dietary questionnaires in existing cohorts. We need randomized controlled trials, including studies of mechanistic pathways relevant to insulin regulation, metabolic syndrome and diabetes, particularly as related to carcinogenicity.”
The IARC and JECFA evaluations of the impact of aspartame were based on scientific data collected from a range of sources, including peer-reviewed papers, governmental reports and studies conducted for regulatory purposes. The studies have been reviewed by independent experts, and both committees have taken steps to ensure the independence and reliability of their evaluations.
IARC and WHO will continue to monitor new evidence and encourage independent research groups to develop further studies on the potential association between aspartame exposure and consumer health effects.
Without preparedness, the WHO warned, a pandemic from Disease X could cause much more damage than COVID, which has killed more than 7 million worldwide.
Story at a glance
At the recent World Economic Forum, the World Health Organization warned that the world could face a pandemic 20 times worse than COVID-19 in the future.
Scientists use the term Disease X to refer to the hypothetical new pandemic, which they say would most likely be a respiratory virus.
The WHO has already begun some initiatives to protect against a future pandemic, including efforts to support technology sharing and boost disease surveillance between countries.
At the recent World Economic Forum, the World Health Organization issued a warning to world leaders, saying the world could face a pandemic 20 times worse than COVID-19 in the future.
Scientists call it Disease X, a term that recognizes the next global pandemic could come as the result of an unknown pathogen rather than the spread of a currently recognized disease.
Scientists with the WHO held a session last week calling on world leaders to work together to develop strategies to prevent or manage a Disease X pandemic in the future.
Disease X is not real. It is the name given to a hypothetical pathogen that is being used to help plan for future health crises. Global healthcare experts on Wednesday spoke on a WEF panel called “Preparing for Disease X.” The name was coined by the World Health Organization in 2018.
One of the issues raised was developing better communication strategies to reduce misinformation and conspiracy theories, even as some took to X, formerly known as Twitter, to call the session itself a conspiracy against freedom.Ukrainian soldiers developing ‘mouse fever’
Scientists say the most likely culprit for Disease X would be a respiratory virus, possibly one already circulating in animals that hasn’t yet made the jump to humans.
Without preparedness, the WHO warned, a pandemic from Disease X could cause much more damage than COVID, which has killed more than 7 million worldwide.
The WHO has already begun some initiatives to protect against a future pandemic, including efforts to support technology sharing and boost disease surveillance between countries.
While Disease X was the focus of the session, it’s not the only illness that concerns epidemiologists. Other viruses that could potentially cause a pandemic include Ebola, Marburg, Crimean-Congo hemorrhagic fever, Lassa fever, SARS, MERS, Nipah virus, Rift Valley Fever, Zika virus and new evolutions of COVID-19.
Last fall, the World Health Organization and some national drug regulators urged influenza vaccine manufacturers to drop the component known as B/Yamagata from flu vaccines as quickly as possible, citing the fact that this lineage of flu B viruses appears to have been snuffed out during the Covid-19 pandemic.
It might seem like that request would be as simple as deciding to leave blueberries out of a mixed-fruit smoothie. It turns out it is not.
While some experts have claimed that this transition should be doable in time for next fall’s Northern Hemisphere flu vaccination campaigns, the International Federation of Pharmaceutical Manufacturers and Associations, an organization that represents vaccine manufacturers and other pharmaceutical entities, is calling for a longer lead time for the shift, saying it will take flu vaccine makers until the 2025-2026 Northern Hemisphere cycle to be able to make the change across the board. The Southern Hemisphere flu vaccines would follow in the 2026 winter, the IFPMA said.
“There’s a bit of a perception that, ‘Industry, you change the components of the vaccine twice a year. Why is this so complicated?’” said Paula Barbosa, the IFPMA’s associate director for vaccine policy.
“It’s widely different.”
Dozens of manufacturers around the world make hundreds of millions of doses of flu vaccine every year. Most of those products are quadrivalent, meaning they target four types of influenza — the influenza A viruses H1N1 and H3N2, and two lineages of flu B viruses, B/Victoria and B/Yamagata.
The protection against two flu B viruses is a relatively new feature of flu vaccines. Prior to 2012, the vaccines were trivalents — protecting against the two A viruses and one of the Bs. But the choice of which B to target wasn’t always correct, leading in some cases to reduced effectiveness of the vaccines. Over the past 15 years or so, most manufacturers transitioned to a four-in-one vaccine, hoping to improve the protection their products offer.
However, in the years preceding the start of the Covid pandemic, B/Yamagata viruses seemed to lose steam. They were detected less frequently than B/Victoria viruses, and didn’t appear to be evolving as quickly as B/Victoria viruses. (The viral target for B/Yamagata in current flu vaccines dates all the way back to 2013.) The reduction in global travel and social distancing measures taken in 2020 to minimize transmission of Covid-19 drove all flu activity to very low levels for a year or so. The other viruses eventually bounced back, but not B/Yamagata. The last confirmed detection of a B/Yamagata virus was in late March 2020. Hence the recommendation to take it out of the vaccines.
Though some virologists remain unconvinced the lineage is actually gone, increasingly flu experts believe there is no longer a need to include protection against B/Yamagata in flu vaccines.
“There’s no [B/Yamagata] virus circulating, so why include the antigen?” asked Scott Hensley, a University of Pennsylvania professor of microbiology who specializes in influenza. “I think it’s definitely time.”
In the main, the rationale for removing the B/Yamagata component is that it isn’t needed. Why stimulate the immune system to be able to fend off a viral enemy it isn’t going to face? But there is also, at least in theory, some risk involved in using one kind of flu vaccine — live-attenuated vaccines like AstraZeneca’s FluMist — that contains live but weakened B/Yamagata viruses. The concern is that the viruses in the vaccine could reassort — swap genes — with the remaining flu B viruses and reseed B/Yamagata in the world.
“I think specifically for the live-attenuated vaccine it is a bad idea to keep Yamagata in that vaccine,” said Ben Cowling, chair of epidemiology at the University of Hong Kong’s School of Public Health.
Experts who advise the Food and Drug Administration on vaccine policy, the Vaccines and Related Biological Products Advisory Committee, endorsed the idea of removing the B/Yamagata component from flu vaccines as quickly as possible at a meeting in early October. And several objected to the claim, raised during the autumn meeting by an industry representative, that it would take until the 2025-2026 vaccine cycle to accomplish this task.
Barbosa said whereas in some jurisdictions — such as the United States — there’s a reasonably uncomplicated regulatory pathway for making the change, in other countries the process is not as clear cut.
There are roughly 350 trivalent vaccine licenses that either need to be reactivated, updated, or in some cases, applied for from scratch, she said, adding that the transition involves an estimated 170 regulatory agencies that will need to sign off on a combined total of about 1,500 variations that need to be made to existing licenses.
Regulatory dossiers are voluminous and detailed. If a flu vaccine producer changed, for example, the location where it conducted some testing of its product, licensing dossiers need to be amended in all places where that testing is referenced to reflect the change. If new production facilities were built in the period after a company started marketing a quadrivalent flu vaccine — in other words, if trivalent products were never made in that location — the new facilities would need to go through approval for trivalent production.
“So the whole end-to-end manufacturing — including the components of quality and validation in many sites — are [quadrivalent] specific, and now will need to be revalidated and submitted for [trivalent],” Barbosa said. “From a regulatory and procedural standpoint, this is an extremely complex picture.”
Some of the manufacturers are in discussions with not just one regulatory agency, but multiple agencies. Some have production plants in a number of countries; major manufacturers sell flu vaccines to multiple countries.
Sanofi, the world’s largest manufacturer of flu vaccines, makes its products in France, Mexico, China, as well as at two U.S. facilities. CSL Seqirus makes flu vaccines in Australia, the United Kingdom, and the U.S., and sells them to at least 14 countries in North and South America, Europe, Australasia, and Asia. GSK makes flu shots in Canada and Germany that are sold in 30 different countries.
The complexity of the regulatory realities facing manufacturers explains why the industry feels the 2024-2025 flu season target can’t be met and that 2025-2026 is more realistic, Barbosa told STAT in an interview.
“This is evolving information, but that’s what we are working on,” she said. “This change presents companies with a number of practical and technical challenges in implementation.”
The IFPMA is advocating for a synchronized global shift, arguing that to make the change sooner in some but not all countries could jeopardize the ability of manufacturers to fill the orders they get from countries that buy the vaccines.
“To make it very clear, the companies are fully committed to supporting the transition,” Barbosa said. “We just feel that it’s critical that the companies are given the appropriate amount of time to operationalize the proposed changes.”
One of the experts at the October VRBPAC meeting who objected to the IFPMA’s timeline was veteran influenza epidemiologist Arnold Monto of the University of Michigan, who believes the shift can be made — at least for the U.S. market — in time for the 2024-2025 flu vaccine rollout.
“The U.S. is a major user of the vaccines. We may not be able to do it — to get rid of the B/Yamagata — globally. But there seems to be a possibility it could happen in the United States,” Monto said in an interview.
All of the licensed quadrivalent flu vaccines in the U.S. were previously marketed as trivalent formulations — which makes the transition much simpler than if a manufacturer had to apply for a whole new license. None of the manufacturers relinquished those trivalent licenses, FDA spokesperson Cherie Duvall-Jones said via email. Instead they were put on a list of “discontinued products” — a kind of a marketing limbo that keeps a license in play but doesn’t require the manufacturer to pay annual program fees for products it isn’t selling.
There is a process for reactivating such licenses. But the FDA wasn’t especially forthcoming about how that process works, saying simply that manufacturers have to submit official requests to have a product removed from the discontinued product list, after which the FDA will ask a manufacturer to submit “a prior approval supplement.” What is required of a company in this prior approval supplement wasn’t spelled out.
The agency sidestepped the question of whether the FDA would be willing to allow manufacturers supplying the U.S. market to take part in a synchronized transition, following the IFPMA timeline.
“The FDA is working with the influenza vaccine manufacturers to assess their readiness to make available a trivalent vaccine and the timing, but it is premature for FDA to provide specific answers to your questions at this time,” Duvall-Jones wrote.
Individual flu vaccine manufacturers were unwilling to talk much about the situation while in negotiations with the FDA about what they must each do to reactivate their trivalent licenses.
“Given this is an ongoing discussion, we don’t have anything to share at this time,” said Chelsea Tressler, a spokesperson for AstraZeneca.
A spokesperson for Sanofi said the company supports the timeline proposed by the IFPMA.
“While the U.S. FDA has a mechanism in place to speed this process, the majority of countries require us to file new license applications for trivalent products, which then have to be reviewed and approved,” the spokesperson said in an email. “It is important to remember that the continued use of quadrivalent inactivated vaccines presents no safety issue, nor is there any lesser efficacy than a trivalent vaccine.”
Barbosa said the IFPMA and its members are hoping for clearer guidance from the WHO and regulatory agencies when global influenza experts convene in February for the twice-annual meeting to select the strains to be included in the next iteration of flu vaccines. The February meeting picks the strains for the following Northern Hemisphere flu shot; the same experts meet in September to select the strains for the next Southern Hemisphere winter.
As to the question of whether some countries or regions could make the transition on a more accelerated schedule, Barbosa said: “It’s a possibility. And I guess we’ll know more in February.”
Aspartame, one of the most widely used artificial sweeteners in the world, will be declared as a possible carcinogen by the cancer research arm of the World Health Organization (WHO), Reuters reports.
The upcoming July ruling from the WHO group, the International Agency on Cancer Research (IARC), will list aspartame as “possibly carcinogenic to humans.” According to the report, the assessment considers all published evidence, but does not account for the amount a person can safely consume.
It’s ample cause for alarm. The sugar substitute has long been a staple of low or zero calorie drinks like Diet Coke, and is also used in thousands of other products including ice cream, chewing gum, and cereal.
But it’s worth noting that the classification of “possibly carcinogenic” only denotes that there is some evidence that a substance can cause cancer, and that the findings are overall considered inconclusive. There are still two categories above this: “probably carcinogenic,” indicating strong evidence, and simply “carcinogenic,” meaning there is consensus on a proven link.
Those are important distinctions. But no matter the technicalities involved, putting a “possibly” next to cancer is always ominous.
As such, the IARC has repeatedly faced criticism for causing alarm from its rulings. Over the years, it’s faced backlash for categorizing eating red meat or working night shifts as “probably carcinogenic,” as well as using cell phones as “possibly carcinogenic.”
Given the stakes involved, the food industry has already began to speak against the IARC’s impending ruling.
“IARC is not a food safety body and their review of aspartame is not scientifically comprehensive and is based heavily on widely discredited research,” said Frances Hunt-Wood, the secretary general of the International Sweeteners Association, as quoted by Reuters.
Though aspartame has been deemed safe by regulators worldwide for decades, including the US Federal Drug Administration (FDA) and the European Food Safety Authority (EFSA), the substitute has never shaken off its stigma.
For its part, the FDA has repeatedly reviewed aspartame’s safety since it was first approved in the 1970s. In 2021, the agency deemed that “no valid conclusion” could be derived from a major Ramazzini Institute study that supposedly found a link between aspartame and cancer in rodents.
That study, along with a large observational study in France involving 100,000 people that also linked aspartame to cancer, have both been criticized for their methodologies. By and large they’re both outliers among an extensive body of research, but in the IARC’s view, it’s enough to warrant concern.
All in all, it’s a bold decision from the WHO group — but according to Reuters, the intent is to encourage more research into aspartame, not to stoke panic.
Aspartame, one of the most widely used artificial sweeteners in the world, will be declared as a possible carcinogen by the cancer research arm of the World Health Organization (WHO), Reuters reports.
The upcoming July ruling from the WHO group, the International Agency on Cancer Research (IARC), will list aspartame as “possibly carcinogenic to humans.” According to the report, the assessment considers all published evidence, but does not account for the amount a person can safely consume.
It’s ample cause for alarm. The sugar substitute has long been a staple of low or zero calorie drinks like Diet Coke, and is also used in thousands of other products including ice cream, chewing gum, and cereal.
But it’s worth noting that the classification of “possibly carcinogenic” only denotes that there is some evidence that a substance can cause cancer, and that the findings are overall considered inconclusive. There are still two categories above this: “probably carcinogenic,” indicating strong evidence, and simply “carcinogenic,” meaning there is consensus on a proven link.
Those are important distinctions. But no matter the technicalities involved, putting a “possibly” next to cancer is always ominous.
As such, the IARC has repeatedly faced criticism for causing alarm from its rulings. Over the years, it’s faced backlash for categorizing eating red meat or working night shifts as “probably carcinogenic,” as well as using cell phones as “possibly carcinogenic.”
Given the stakes involved, the food industry has already began to speak against the IARC’s impending ruling.
“IARC is not a food safety body and their review of aspartame is not scientifically comprehensive and is based heavily on widely discredited research,” said Frances Hunt-Wood, the secretary general of the International Sweeteners Association, as quoted by Reuters.
Though aspartame has been deemed safe by regulators worldwide for decades, including the US Federal Drug Administration (FDA) and the European Food Safety Authority (EFSA), the substitute has never shaken off its stigma.
For its part, the FDA has repeatedly reviewed aspartame’s safety since it was first approved in the 1970s. In 2021, the agency deemed that “no valid conclusion” could be derived from a major Ramazzini Institute study that supposedly found a link between aspartame and cancer in rodents.
That study, along with a large observational study in France involving 100,000 people that also linked aspartame to cancer, have both been criticized for their methodologies. By and large they’re both outliers among an extensive body of research, but in the IARC’s view, it’s enough to warrant concern.
All in all, it’s a bold decision from the WHO group — but according to Reuters, the intent is to encourage more research into aspartame, not to stoke panic.
A new WHO guideline recommends adults and children reduce their daily intake of free sugars to less than 10% of their total energy intake. A further reduction to below 5% or roughly 25 grams (6 teaspoons) per day would provide additional health benefits.
Free sugars refer to monosaccharides (such as glucose, fructose) and disaccharides (such as sucrose or table sugar) added to foods and drinks by the manufacturer, cook or consumer, and sugars naturally present in honey, syrups, fruit juices and fruit juice concentrates.
“We have solid evidence that keeping intake of free sugars to less than 10% of total energy intake reduces the risk of overweight, obesity and tooth decay,” says Dr Francesco Branca, Director of WHO’s Department of Nutrition for Health and Development. “Making policy changes to support this will be key if countries are to live up to their commitments to reduce the burden of noncommunicable diseases.”
The WHO guideline does not refer to the sugars in fresh fruits and vegetables, and sugars naturally present in milk, because there is no reported evidence of adverse effects of consuming these sugars.
Much of the sugars consumed today are “hidden” in processed foods that are not usually seen as sweets. For example, 1 tablespoon of ketchup contains around 4 grams (around 1 teaspoon) of free sugars. A single can of sugar-sweetened soda contains up to 40 grams (around 10 teaspoons) of free sugars.
Worldwide intake of free sugars varies by age, setting and country. In Europe, intake in adults ranges from about 7-8% of total energy intake in countries like Hungary and Norway, to 16-17% in countries like Spain and the United Kingdom. Intake is much higher among children, ranging from about 12% in countries like Denmark, Slovenia and Sweden, to nearly 25% in Portugal. There are also rural/urban differences. In rural communities in South Africa intake is 7.5%, while in the urban population it is 10.3%.
Reducing sugars intake to less than 10% of total energy: a strong recommendation
The recommendations are based on analysis of the latest scientific evidence. This evidence shows, first, that adults who consume less sugars have lower body weight and, second, that increasing the amount of sugars in the diet is associated with a weight increase. In addition, research shows that children with the highest intakes of sugar-sweetened drinks are more likely to be overweight or obese than children with a low intake of sugar-sweetened drinks.
The recommendation is further supported by evidence showing higher rates of dental caries (commonly referred to as tooth decay) when the intake of free sugars is above 10% of total energy intake compared with an intake of free sugars below 10% of total energy intake.
Based on the quality of supporting evidence, these recommendations are ranked by WHO as “strong”. This means they can be adopted as policy in most situations.
Further reduction to less than 5% of total energy intake: a conditional recommendation
Given the nature of existing studies, the recommendation of reducing intake of free sugars to below 5% of total energy is presented as “conditional” in the WHO system for issuing evidence-based guidance.
Few epidemiological studies have been undertaken in populations with a low sugars intake. Only three national population-wide studies allow a comparison of dental caries with sugars intakes of less than 5% of total energy intake versus more than 5% but less than 10% of total energy intake.
These population-based ecological studies were conducted during a period when sugars availability dropped dramatically from 15kg per person per year before the Second World War to a low of 0.2kg per person per year in 1946. This “natural experiment”, which demonstrated a reduction in dental caries, provides the basis for the recommendation that reducing the intake of free sugars below 5% of total energy intake would provide additional health benefits in the form of reduced dental caries.
WHO issues conditional recommendations even when the quality of evidence may not be strong on issues of public health importance. A conditional recommendation is one where the desirable effects of adhering to the recommendation probably outweigh the undesirable effects but these trade-offs need to be clarified; therefore, stakeholder dialogue and consultations are needed before the recommendation is implemented as policy.
Updating the guideline on free sugars intake is part of WHO’s ongoing efforts to update existing dietary goals to prevent NCDs. The sugars guidelines should be used in conjunction with other nutrient guidelines and dietary goals, in particular those related to fats and fatty acids, including saturated fat and trans-fat.
In March 2014, WHO opened a public consultation on the then draft sugars guideline to seek inputs from all stakeholders. More than 170 comments were received from representatives of government agencies, United Nations agencies, non-governmental organizations, industries and academic institutions as well as other interested individuals. An expert peer review process was also undertaken in 2014. The final guideline was prepared taking into account comments received from the public consultation and expert peer review.
Countries can translate the recommendations into food-based dietary guidelines that consider locally available food and customs. Additionally, some countries are implementing other public health interventions to reduce free sugars intake. These include nutrition labelling of food products, restricting marketing to children of food and non-alcoholic drinks that are high in free sugars, fiscal policies targeting foods and beverages high in free sugars, and dialogue with food manufacturers to reduce free sugars in processed foods.
Taxing sugary drinks can lower consumption and reduce obesity, type 2 diabetes and tooth decay, says a new WHO report.
Fiscal policies that lead to at least a 20% increase in the retail price of sugary drinks would result in proportional reductions in consumption of such products, according to the report titled “Fiscal policies for Diet and Prevention of Noncommunicable Diseases (NCDs)”.
Reduced consumption of sugary drinks means lower intake of “free sugars” and calories overall, improved nutrition and fewer people suffering from overweight, obesity, diabetes and tooth decay.
Free sugars refer to monosaccharides (such as glucose or fructose) and disaccharides (such as sucrose or table sugar) added to foods and drinks by the manufacturer, cook, or consumer, and sugars naturally present in honey, syrups, fruit juices, and fruit juice concentrates.
Obesity on the rise
“Consumption of free sugars, including products like sugary drinks, is a major factor in the global increase of people suffering from obesity and diabetes,” says Dr Douglas Bettcher, Director of WHO’s Department for the Prevention of NCDs. “If governments tax products like sugary drinks, they can reduce suffering and save lives. They can also cut healthcare costs and increase revenues to invest in health services.”
In 2014, more than 1 in 3 (39%) adults worldwide aged 18 years and older were overweight. Worldwide prevalence of obesity more than doubled between 1980 and 2014, with 11% of men and 15% of women (more than half a billion adults) being classified as obese.
In addition, an estimated 42 million children aged under 5 years were overweight or obese in 2015, an increase of about 11 million during the past 15 years. Almost half (48%) of these children lived in Asia and 25% in Africa.
The number of people living with diabetes has also been rising, from 108 million in 1980 to 422 million in 2014. The disease was directly responsible for 1.5 million deaths in 2012 alone.
Need to reduce sugar intake
“Nutritionally, people don’t need any sugar in their diet. WHO recommends that if people do consume free sugars, they keep their intake below 10% of their total energy needs, and reduce it to less than 5% for additional health benefits. This is equivalent to less than a single serving (at least 250 ml) of commonly consumed sugary drinks per day,” says Dr Francesco Branca, Director of WHO’s Department of Nutrition for Health and Development.
According to the new WHO report, national dietary surveys indicate that drinks and foods high in free sugars can be a major source of unnecessary calories in people’s diets, particularly in the case of children, adolescents and young adults.
It also points out that some groups, including people living on low incomes, young people and those who frequently consume unhealthy foods and beverages, are most responsive to changes in prices of drinks and foods and, therefore, gain the highest health benefits.
Using fiscal policies to reduce consumption
Fiscal policies should target foods and beverages for which healthier alternatives are available, the report adds.
The report presents outcomes of a mid-2015 meeting of global experts convened by WHO and an investigation of 11 recent systematic reviews of the effectiveness of fiscal policy interventions for improving diets and preventing NCDs and a technical meeting of global experts. Other findings include:
Subsidies for fresh fruits and vegetables that reduce prices by 10–30% can increase fruit and vegetable consumption.
Taxation of certain foods and drinks, particularly those high in saturated fats, trans fat, free sugars and/or salt appears promising, with existing evidence clearly showing that increases in the prices of such products reduces their consumption.
Excise taxes, such as those used on tobacco products, that apply a set (specific) amount of tax on a given quantity or volume of the product, or particular ingredient, are likely to be more effective than sales or other taxes based on a percentage of the retail price.
Public support for such tax increases could be increased if the revenue they generate is earmarked for efforts to improve health systems, encourage healthier diets and increase physical activity.
A number of countries have taken fiscal measures to protect people from unhealthy products. These include Mexico, which has implemented an excise tax on non-alcoholic beverages with added sugar, and Hungary, which has imposed a tax on packaged products with high sugars, salt or caffeine levels.
Countries, such as the Philippines, South Africa and the United Kingdom of Great Britain and Northern Ireland have also announced intentions to implement taxes on sugary drinks
The World Health Organization (WHO) has quality-assured (prequalified) the novel type 2 oral polio vaccine (nOPV2) after 3 years of being granted Emergency Use Listing (EUL). The vaccine was developed with contributions from scientists at the UK Medicines and Healthcare products Regulatory Agency (MHRA).
The WHO decision follows the delivery of 950 million doses worldwide and scrutiny of the results in immunized populations, affirming the vaccine’s safety and efficacy.
The nOPV2 is a modified version of the oral polio vaccine (OPV) that specifically targets poliovirus type 2. It was developed to mitigate the risk of vaccine-derived outbreaks, which can occur when the weakened virus in the vaccine circulates among under-immunized populations and regains the ability to cause paralysis. It maintains effectiveness against polio while reducing the potential for the virus to mutate and regain virulence, making it a safer option for widespread vaccination campaigns, especially in regions where polio remains a threat.
Genetic modifications to the vaccine, for example, a stabilized RNA stem-loop structure in the 5′ noncoding region that is the major determinant of OPV2 attenuation, were tested through a number of pre-clinical methods (serial passaging, cell culture assays used to estimate temperature sensitivity, testing in transgenic mice models, etc.) before initiating clinical development.
The nOPV2 serves as a crucial shield for children against polio, and its prequalification status by the WHO streamlines access for WHO member countries without the stringent readiness criteria previously mandated under the EUL.
Prequalification guarantees extended and widespread availability for global organizations to supply and distribute the nOPV2 in developing nations.
Poliomyelitis, transmitted mainly through contaminated food and water, particularly threatens infants and young children, potentially leading to severe paralysis or fatality.
The OPVs, including nOPV2, have substantially curbed polio cases globally. They do not require stringent cold storage, facilitating immunization in remote areas.
Three years ago, amid mounting concerns about vaccine-derived outbreaks in Asia and Africa, the nOPV2 became the first vaccine to gain WHO EUL , paving the way for its prequalification today.
The decision signifies a pivotal step forward in fortifying global immunity against polio and reaffirms the collective commitment to ensure children worldwide receive safer and more accessible polio vaccines.
During the summer of 2022, mpox (then known as monkeypox) was spreading rapidly across the US, largely affecting gay and bisexual men who have sex with men (GBMSM).1 Fifteen months later, the outbreak looks very different. Cases are down to an average of approximately 1 to 2 per day (from a peak of 600 per day),2 the summer 2023 wave that was widely predicted did not materialize, and the clusters that occur now are quickly controlled (Figure). How did we get here? And what did the lessons of the mpox response teach us about managing future outbreaks? Even though the biomedical tools (tests, vaccines, and therapeutics) were available at the start of the outbreak, how they were deployed provides important lessons. There are 3 key lessons from the response that can help better manage infectious disease outbreaks in the future.
Based on data from the US Centers for Disease Control and Prevention.
The primary strategy for mpox containment was to take an approach that deeply engaged the community most affected. Rather than the community as the object of a public health intervention, they became the vehicle. The views (often criticisms) of those most affected by the virus were used to inform policy and create shared accountability. One example was creating the equity mpox workshop composed of GBMSM and transgender racial and ethnic minority individuals. This monthly workshop, suggested by a prominent member of the GBMSM community, provided feedback to the White House that helped calibrate the community-driven response. The White House Mpox Response Team (WHMRT) built trust among the community by engaging, listening, and acting on their suggestions. In return, the community became the trusted messengers.
A variety of strategies were used to distribute information from accessible webinars to infographics circulated on social media. These communications allowed local and state public health leaders to transparently answer questions on the minds of community members. One key lesson from the COVID-19 response was that outbreaks create information needs and filling those needs with high-quality, easily comprehensible information is critical to prevent misinformation from propagating. Letting the community identify the information needs and then transparently filling those needs, including acknowledging scientific uncertainty, was critical to managing the mpox outbreak.
A second lesson from the mpox response was that public health responses must be flexible and responsive. Even though vaccines were available in traditional places for administration (such as physician offices and retail pharmacies), the community partners emphasized the importance of also making vaccinations available where those who would most benefit were likely to be present and comfortable. Applying lessons learned in HIV-related outreach, vaccines were offered in safe spaces outside night clubs, pop-up events, social venues, sex parties, and other community-focused events such as Atlanta Black Pride and Southern Decadence.3–5 This level of community engagement enhanced equity in mpox vaccination and better aligned vaccine providers with the community they served, both of which were essential to curbing the outbreak.
Risk assessment is another example of a key change made due to feedback from community partners. After initially using the traditional public health approach of conducting risk assessments before administering vaccines, we quickly heard from community partners that risk assessments are often stigmatizing and could dissuade many of the highest-risk individuals from even engaging. Therefore, the need for extensive risk assessment was removed and trusted partners were leveraged to help identify the people most likely to benefit from vaccines, education, and prevention messaging. We also heard clear concerns that the temporary mark left at the mpox injection site might disclose information on sexuality or gender identity. More flexible clinical guidance was adopted that allowed the vaccine to be administered on less visible parts of the body, and encouraged people to express a preference for the injection site. This seemingly small change may have had a large effect on both creating greater vaccine acceptance and generally building community trust.
The third lesson was the importance of flexible resources and investments in public health infrastructure for preparedness and rapid response during public health emergencies. When the Secretary of the US Department of Health and Human Services determined that mpox had the potential to become an infectious disease emergency, public health officials were able to use the US Centers for Disease Control and Prevention infectious diseases rapid response reserve fund to deploy resources quickly. Public health officials working on HIV and sexually transmitted infections prevention activities were able to conduct mpox prevention work in conjunction with these ongoing activities. Given that the communities most vulnerable to mpox overlap significantly with those most affected by HIV (between 35%-47% of those diagnosed with mpox also had HIV),6 drawing on the capabilities and infrastructure that already existed for HIV proved extremely useful in containing the mpox outbreak. The WHMRT also coordinated activities across the US Department of Health and Human Services and the US Department of Housing and Urban Development to provide additional resources for the response.
Beyond those 3 key elements of the response, there is one more critical issue to consider. As the number of new cases declined during the fall of 2022, there was intense pressure to bring the mpox response to an end and fold it into ongoing public health work around sexually transmitted infections. It is tempting to see declining case numbers as an invitation to declare the effort a success.
Despite what is often a short attention span of policymakers, the White House recognized that declining case numbers or even an end to the declared public health emergency should not end the mpox response. The WHMRT was concerned with the disproportionate effect mpox had on Black and Latino communities and people living with HIV and recognized that mpox required ongoing attention and critical work to prevent resurgence.7 Instead of pulling back, the WHMRT redoubled its efforts in the spring of 2023 to build trust and vaccinate those who were vulnerable. As we neared the summer and seasonal festivities that could increase opportunities for the virus to spread, the team made additional efforts to partner with event organizers and the communities they serve to provide people with a holistic toolkit to inform their decisions about how to keep their summer healthy.8,9 The lack of a second wave of mpox this past summer was due in large part to the ongoing work with the communities most affected and the decision to continue driving awareness. Persistence is the key lesson. Even after the infection numbers decline, it is paramount to prevent outbreak resurgence.
The last few years have been remarkable in how infectious diseases have taken a toll. The lesson from the mpox response is clear: community engagement and flexibility of response are necessary as well as the existing public health infrastructure that can be deployed to manage outbreaks. Medical countermeasures are key, but so are community partnerships, flexibility, and persistence. That is how infectious disease outbreaks should be managed now and in the future.







{kind=link}