Adults with type 1 diabetes spent more time in range with empagliflozin 2.5 mg or 5 mg as an adjunctive therapy to hybrid closed-loop insulin therapy compared with placebo, according to a speaker.
“We look at large trials assessing hybrid closed-loop therapy in type 1 diabetes and 34% to 69% of the participants do not actually achieve the target HbA1c post-intervention,” Melissa-Rosina Pasqua, MD, an endocrinologist and PhD candidate at the McGill University Health Center Research Institute in Montreal, said during a presentation at the International Conference on Advanced Technologies & Treatments for Diabetes. “When we look at other ways to reduce HbA1c, SGLT2 inhibitors as an adjunct to insulin therapy have been shown to reduce HbA1c in type 1 diabetes. The caveat is there is risk for diabetic ketoacidosis, particularly euglycemic. … The objective of our study was to assess the effect of low-dose empagliflozin on glucose control in adults with type 1 diabetes on a hybrid closed-loop system who did not otherwise get the target time in range of 70% or more.”
Data were derived from Pasqua MR, et al. OP 027. Presented at: International Conference on Advanced Technologies & Treatments for Diabetes; Feb. 22-25, 2023; Berlin (hybrid meeting).
Researchers conducted a double-blind, crossover, randomized controlled trial enrolling 24 adults with type 1 diabetes and a baseline HbA1c between 7% and 10.5% (50% men; mean age, 33 years). The trial consisted of three 14-day intervention periods in which participants received empagliflozin 2.5 mg (Jardiance, Boehringer Ingelheim/Eli Lilly), empagliflozin 5 mg or placebo as an adjunct to hybrid closed-loop insulin therapy. The order of therapies was randomly sequenced. Continuous glucose monitoring outcomes were obtained during the last 10 days of each intervention period. Morning ketone levels were collected daily.
At the conclusion of the study, adults had a 71.6% time in range with empagliflozin 2.5 mg and a 70.2% time in range with empagliflozin 5 mg compared with a 59% time in range with placebo (P < .0001). The associations were not affected by time of day, as adults had a higher time in range with either empagliflozin dose compared with placebo during both daytime and nighttime.
Time in hypoglycemia did not differ between those receiving empagliflozin 2.5 mg and placebo. Adults had a higher time in hypoglycemia with empagliflozin 5 mg than placebo (1.5% vs. 1%; P = .0051). However, the association of higher time in hypoglycemia with empagliflozin 5 mg compared with placebo was only significant during daytime hours (1.1% vs. 0.7%; P = .0065).
Participants used 54 insulin U per day with empagliflozin 2.5 mg and 52.9 U with empagliflozin 5 mg compared with 59.2 U with placebo. Morning ketone levels were similar with both empagliflozin doses and placebo.
No serious adverse events were reported during the study and there were no episodes of DKA or severe hypoglycemia.
“There were some limitations,” Pasqua said. “It was a short, small study. We powered for time in range, we didn’t power necessarily for ketone data.”
In addition, Pasqua noted the cohort had a mean BMI of 28.8 kg/m2 and insulin requirements that suggested they were mostly low-risk participants. She said studies are being planned to further explore the impact of empagliflozin on time in range in a larger cohort of adults with type 1 diabetes.
In the United States, just half of patients with type 1 diabetes who had overweight or obesity received weight management lifestyle recommendations from providers or engaged in lifestyle modification, data show.
Researchers said the findings highlight the need for more comprehensive clinical guidelines with an emphasis on individualized medicine.
Data derived from: Fang M, et al. Ann Intern Med. 2023;doi:10.7326/M22-3078.
Up to 37% of people with type 1 diabetes have obesity, Michael Fang, PhD, MHS, an assistant professor at Johns Hopkins Bloomberg School of Public Health, and colleagues wrote in Annals of Internal Medicine.
“Survival has significantly improved in patients with type 1 diabetes over the past 2 decades, shifting the health profile of this population,” the researchers wrote. “However, current studies are based on selected populations and have not considered engagement in lifestyle modification.”
Fang and colleagues examined data from 128,571 adults who participated in the National Health Interview Survey.
From 2016 to 2021, the researchers found that 62% of people with type 1 diabetes had overweight or obesity compared with 64% of those without diabetes and 86% of those with type 2 diabetes. Of those with overweight or obesity, people with type 1 diabetes were offered lifestyle recommendations less frequently than those with type 2 diabetes but more frequently than people without diabetes.
“Rates of overweight and obesity in U.S. adults with type 1 diabetes are virtually identical to rates in the general adult population,” the researchers wrote. “Nearly two-thirds of U.S. adults with type 1 diabetes have overweight or obesity. However, only about half of these patients received lifestyle recommendations from providers or engaged in lifestyle modification.”
People with type 1 diabetes were the least likely to manage overweight or obesity with reduced caloric intake or increased physical activity.
The researchers wrote that, for those with type 1 diabetes, weight management “is complicated by insulin use.”
“Dietary and physical activity changes often require adjustments to insulin timing and dosage to prevent hypoglycemia,” they wrote. “Evidence-based guidance on lifestyle modification in type 1 diabetes remains sparse, potentially contributing to low rates of recommendation by providers and low engagement by patients. Robust clinical trials are needed to understand how to promote weight management safely and effectively in persons with type 1 diabetes.”
Fang and colleagues concluded that, for adults with type 1 diabetes in the United States, “the burden of overweight and obesity is substantial and remains poorly managed.”
“The development of more comprehensive clinical guidelines, with an emphasis on individualized patient education, may improve weight management in these patients,” they wrote.
Swedish researchers have begun a clinical study on an approved drug for treating psoriasis that will be tested on patients who were recently diagnosed with type 1 diabetes. The theory is that the drug could preserve the patient’s remaining insulin production.
Marcus Lind, MD, PhD, a professor of diabetology at the University of Gothenburg and chief physician responsible for clinical diabetes research at Sahlgrenska University Hospital and NU-hospital Group, heads the project. He noted that the study could mean a big change in how type 1 diabetes is treated:
“Of the mechanisms now being investigated for immunological treatment of type 1 diabetes, I have the greatest confidence in this one, but I am well aware of how difficult success will be,” he says.
An immunological disease
Type 1 diabetes is one of the most common chronic diseases in children, but the disease can also develop in adults. In the disease, the body’s own immune response destroys beta cells in the pancreas so that the body can no longer produce insulin. People with type 1 diabetes need to take insulin injections or use an insulin pump and strictly track their blood sugar levels for the rest of their lives, which requires a lot of effort.
The beta cells die slowly, so everyone with newly developed type 1 diabetes continues to produce insulin during the first years of the disease.
“They benefit greatly from the remaining insulin their body produces. If they could just maintain this production, treating type 1 diabetes would be much easier. So far, we have not had a good treatment for preventing beta cell death, but we have reason to believe that a medication currently approved for individuals with psoriasis could have a protective effect for individuals with type 1 diabetes,” continued Lind.
Based on immunological patterns in the blood, researchers can currently determine with a high probability who will develop type 1 diabetes (stage 1 of type 1 diabetes) within a few years. About a year before the onset of the disease, they can then see disturbances in the blood sugar pattern with stress tests, even if criteria for diabetes are not met (stage 2 of the disease). When clinical onset occurs, it is classified as stage 3.
Doctoral student Arndís Ólafsdóttir and Professor Marcus Lind, MD, PhD, Sahlgrenska Academy at the University of Gothenburg. [Elin Lindström/University of Gothenburg]
“If we succeed in identifying the immunological mechanism that is central to the destruction of beta cells, we will also be able to screen children and adults in the future and treat them even before the onset of the disease,” pointed out Lind. “The disease will then be prevented from breaking out or counteracted so that it does not begin until much later in life.”
Psoriasis and type 1 diabetes
The drug to be tested affects the immune response in the body by inhibiting interleukin-17, which seems to be an important signaling molecule in the process that destroys beta cells. For the last few years, the drug has been used as a treatment for psoriasis, where a specific type of white blood cells (TRM cells) plays a key role in development of the disease, just as these cells seem to do in type 1 diabetes. Among other things, these cells act through IL-17, which the current treatment affects.
“In fact, research on type 1 diabetes and IL-17 has been going on for almost 20 years. Animal experiments have shown that stimulation of this signaling pathway accelerates the development of type 1 diabetes,” said Lind. “Other studies have shown that this signaling pathway is usually overactivated in people with type 1 diabetes. It will be particularly interesting to evaluate for the first time whether the treatment can protect insulin-producing cells in the pancreas, in light of recent research on TRM cells in newly diagnosed type 1 diabetes, just as in psoriasis.”
Recruitment of individuals with type 1 diabetes for a comprehensive multicenter study has now begun. The study will include adults, between ages 18 and 35, who have been diagnosed with type 1 diabetes in the last three months, where a blood test has shown that they have an ongoing immunological process affecting the beta cells. A total of 127 individuals will be included, with half being randomly assigned to receive IL-17 inhibitors and half receiving a placebo in the control group.
Towards precision medicine
In parallel with the Swedish study now being conducted at the University of Gothenburg, several other studies are underway elsewhere in the world. They are also seeking ways to treat the immunological cause behind type 1 diabetes and not just the symptoms, which until now has been the only treatment option.
As with many other diseases, researchers of type 1 diabetes now appear to be on the verge of precision medicine. Efforts to map different subgroups within type 1 diabetes have just begun to study, for example, a certain gene variation that causes a certain type of islet cell antibodies to first appear.
“It is likely that treatment with IL-17 inhibitors may be more effective for certain subgroups,” explained Lind. “If the results from our study are encouraging, over time we can investigate certain immunological patterns or cell types in the blood that can be used to identify patient groups that respond best to the treatment.”
Could support for type 1 diabetes be as close as your kitchen cupboard? An accumulating body of scientific research appears to point in exactly that direction
One so-called “incurable disease” that afflicts millions of people around the world is type 1 diabetes. Unlike type 2 diabetes, where the body becomes resistant to its own insulin, type 1 is characterized by the inability of the body to produce enough insulin, as the beta cells within the pancreas, which are responsible for the production of insulin (and the proinsulin from which it is made), are either destroyed or seriously impaired. This can happen due to autoimmune issues, bacterial or viral infections, incompatible foods in the diet and chemical exposures (or a combination of any one or more of these factors), to name but a few major triggers.
And yet, plenty of peer-reviewed and published research indicates that plant compounds, including many found within commonly consumed foods, are capable of stimulating beta cell regeneration within the pancreas, and as a result may potentially provide a natural form of treatment –perhaps something the profit-based model of medicine, which thrives on the concept of the incurability of the disease-afflicted human body in favor of symptom management, isn’t eager to hear.
The discovery of the beta cell regenerative potential of various food and compounds is bound to upset a burgeoning diabetes industry, with millions of dollars of public and private money continually being poured into fundraising efforts for a future “cure;” A cure that will presumably be delivered through the prohibitively expensive pharmaceutical, vaccine or biologic (e.g., stem cells, islet cell xenotransplantation) pipeline, which by the very nature of the FDA drug approval process requires the promotion of synthetic (and therefore patentable) compounds over natural ones.
Let’s take a look at a preclinical study on the topic, published in the Canadian Journal of Physiology and Pharmacology[1]. An active fraction of flaxseed, which researchers named Linun usitassimum active fraction (LU6), was found to generate a wide range of benefits in a type 1 diabetes animal model, including the following:
Improved glucose utilization in the liver
Supported normalized glycogenesis (glucose forming activity) in the liver and muscle tissue
Reduced pancreatic and intestinal glucosidase inhibitory activity, which translates into lower post-meal blood sugar elevations
Even more remarkable was the observation that this flaxseed compound normalized plasma insulin and C-peptide levels (C peptide is not C-reactive protein, rather it is a direct indicator of how much insulin is being produced by the beta cells in the body. Learn more), an indication that beta cell function was effectively restored. The researchers described the truly amazing results as follows:
Normalization of plasma insulin and C-peptide levels were observed in diabetic mice, indicating endogenous insulin secretion after the treatment with LU6. The histochemical and immunohistochemical analysis on pancreatic islets suggests the role of LU6 fraction in islet regeneration and insulin secretion as evident in increase functional pancreatic islets producing insulin. Furthermore, significant insulin producing islet formation was also observed in in vitro PANC-1 cells after LU6 treatment, indicating the cellular aggregates to be newly formed islets. This suggests the potential of LU6 fraction in the formation of new islets in vitro, as well as in vivo. Thus, LU6 can be used as a nutraceutical-based first-line treatment for diabetes. [emphasis added]
Keep in mind that this is not the first time that flaxseed has been found to improve blood sugar disorders. We have a few studies on GreenMedInfo.com already indexed on the topic that you can view here: Flaxseed and Diabetes.
Furthermore, we have found a broad range of natural substances experimentally confirmed to stimulate beta cell regeneration, 10 of which are listed below:
Arginine: A 2007 study found that the amino acid L-arginine is capable of stimulating the genesis of beta cells in an animal model of alloxan-induced diabetes.[2]
Avocado: A 2007 study found that avocado seed extract reduced blood sugar in diabetic rats. Researchers observed a restorative and protective effect on pancreatic islet cells in the treated group.[3]
Berberine: A 2009 study found that this plant compound, commonly found in herbs such as barberry and goldenseal, induces beta cell regeneration in diabetic rats, which lends explanation for why it has been used for 1,400 years in China to treat diabetes.[4]
Chard: A 2000 study found that chard extract given to diabetic rats stimulates the recovery of injured beta cells.[5]
Corn Silk: A 2009 study found that corn silk reduces blood sugar and stimulates beta cell regeneration in type 1 diabetic rats.[6]
Curcumin (from Turmeric): A 2010 study found that curcumin stimulates beta cell regeneration in type 1 diabetic rats.[7]Additionally, a 2008 study found that curcumin preserves pancreatic islet cell survival and transplantation efficiency.[8]
Genistein (from soy, red clover): A 2010 study found that genistein induces pancreatic beta-cell proliferation through activation of multiple signaling pathways and prevents insulin-deficient diabetes in mice.[9]
Honey: A 2010 human study found that long-term consumption of honey might have positive effects on the metabolic derangements of type 1 diabetes, including possible beta cell regeneration as indicating by increases in fasting C-peptide levels.[10]
Nigella Sativa (black seed): A 2003 animal study found that black seed consumption led to partial regeneration/proliferation of the beta cells.[11]A 2010 human study also found that the consumption of 1 gram of black seed a day for up to 12 weeks had a broad range of beneficial effects in diabetics, including increasing beta cell function.[12]
Stevia: A 2011 human study found that stevia has anti-diabetic properties, including revitalizing damaged beta cells, and compares favorably with the drug glibenclamide but without the adverse effects
We’ve known for a while that diet can help improve type 2 diabetes, but it’s rare to find an intervention for type 1 diabetes
In recent years, more and more studies have found that there is a vegetable that contains hundreds of active substances with unique effects that can alleviate the symptoms of both type I and II diabetic patients and also benefit the glucose metabolism of healthy people: This food is bitter melon.
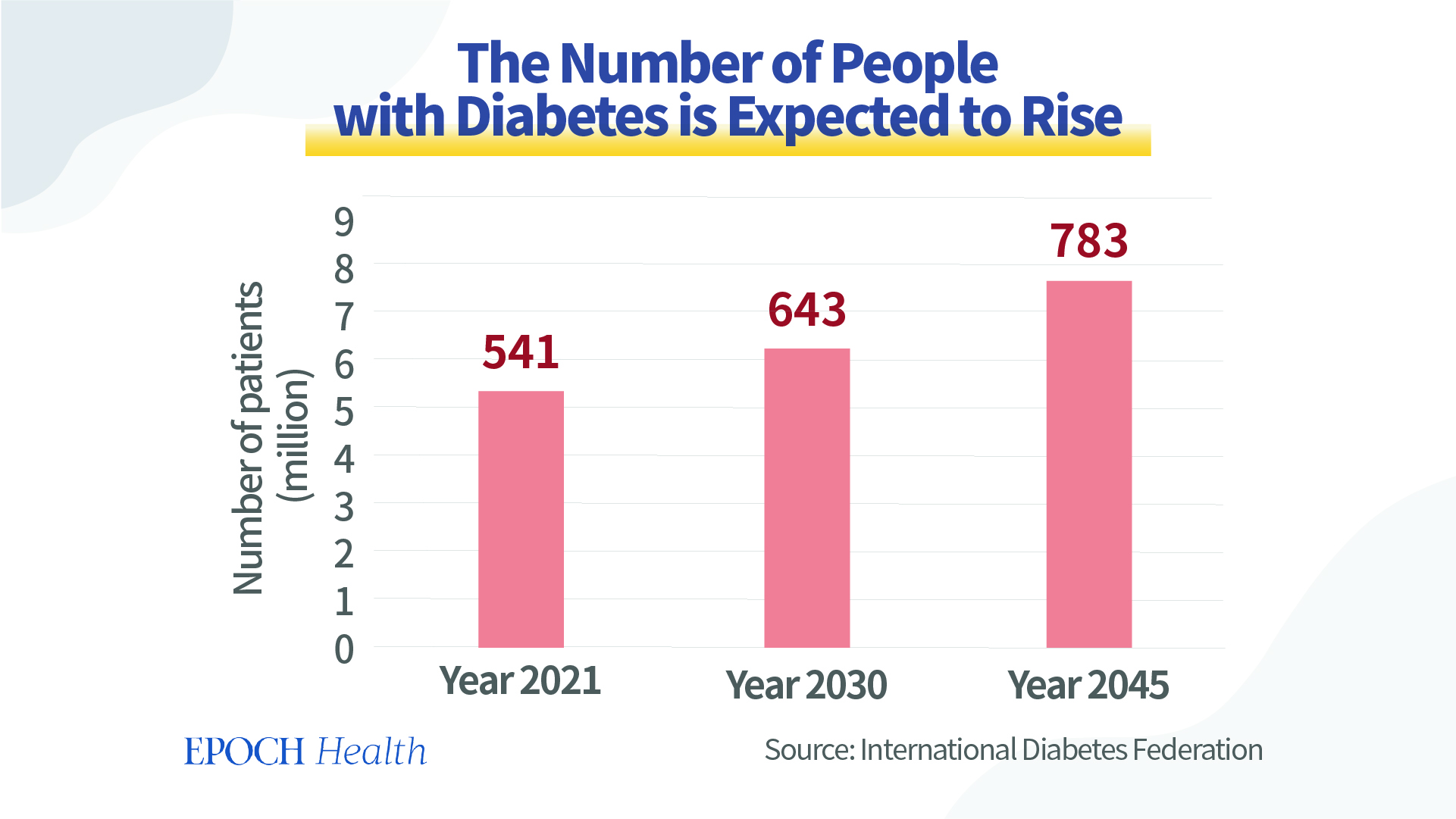
According to the International Diabetes Federation, there were 537 million people with diabetes and 6.7 million diabetes-related deaths worldwide in 2021. This is equivalent to one person dying every five seconds due to diabetes.
In addition, 541 million adults worldwide have impaired glucose tolerance (IGT) and are at high risk of developing type II diabetes. The number of people with diabetes is expected to rise to 643 million by 2030 and to 783 million by 2045.
Diabetes is a chronic disease that can gradually damage the heart, blood vessels, eyes, nerves, and musculoskeletal system, and it is a major cause of kidney failure and blindness.
Diabetes is generally divided into four categories: type I diabetes, type II diabetes, gestational diabetes, and other specific types of diabetes.
Under normal circumstances, cells can absorb sugar and convert it into energy under the “command” of insulin.
In type I diabetes, the insulin-producing beta cells in the pancreas are damaged for various reasons, resulting in a reduced ability to secrete insulin. Since the body lacks insulin, people with type I diabetes have symptoms of high blood sugar and need to inject insulin into their bodies.
Type II diabetic patients mainly have insulin resistance. Their pancreas can produce insulin normally, but the body is insensitive to insulin. Even if the insulin level is sufficient, or even very high, the cells do not receive sufficient instructions to absorb sugar, so the blood sugar does not drop properly. These patients usually need oral hypoglycemic drugs to lower their blood sugar.
Bitter Melon Has a Wide Range of Therapeutic Effects, and Its Anti-Diabetic Effect Has Attracted Attention
In addition to medication, diet and lifestyle management are also important aspects for diabetes treatment. People have also been looking for natural plants that have curative effects on diabetes.
Bitter melon is one of the most prominent of these plants.
Although bitter melon has a peculiar bitter taste, it is still a popular vegetable around the world, often found in farmers’ markets and supermarkets. This is in part because people love the many benefits of this bitter-tasting vegetable and that it has some properties that other vegetables may not have.
The entire plant, especially its seeds and fruits, have been used for thousands of years for healing purposes. As a folk medicine, bitter melon is widely used—it is used to treat toothache, diarrhea, boils, and worms. It’s also antimalarial, and a laxative. It is also used to treat dysmenorrhea, eczema, gout, jaundice, leprosy, hemorrhoids, pneumonia, psoriasis, rheumatism, and scabies. Some people also use it for contraception purposes.
Besides polysaccharides, proteins, peptides, and lipids, bitter melon also contains triterpenoids, saponins, flavonoids, alkaloids, and sterols. These substances have anticancer, antioxidant, anti-inflammatory, antiviral, antibacterial, immune-enhancing, and/or antidiabetic effects.
The anti-diabetic effect of bitter melon is gaining attention and further research worldwide. A search on PubMed, a biomedical literature engine, by using “bitter melon and diabetes” as the keyword showed that the research results published had been increasing in recent years.
These studies show that bitter melon can alleviate and treat type I and type II diabetes to a certain extent. The anti-diabetic effect of bitter melon is achieved by regulating the function of the pancreas and by modulating mechanisms outside of the pancreas.
Bitter Melon Helps Relieve Type I Diabetes by Stimulating Insulin Secretion
1. Components in bitter melon stimulate insulin secretion
Bitter melon extract can also stimulate the secretion of an enzyme in the intestine, which can contribute to the proliferation of islet cells and the secretion of insulin. Islet cells are cells in the pancreas that produce hormones like insulin and glucagon.
2. Bitter melon components can protect islet cells from damage
Triterpenoids and polysaccharides in bitter melon can protect the activity of pancreatic cells from damage, especially oxidative damage.
Researchers have treated pancreatic cells with sugar and then added aqueous extract of bitter melon and found that the aqueous extract of bitter melon was effective in ensuring the survival of pancreatic cells within a certain time frame, compared to the control group without the addition of this substance.
The components in bitter melon can protect the β-cells in the pancreas by down-regulating the activity of some enzymes. Excessive glucocorticoids can damage the β-cells in the pancreas, but bitter melon extract can regulate this hormone, thereby protecting the pancreas and ensuring the secretion of insulin.
3. Bitter melon components promote the repair of pancreatic cells
Bitter melon extract can promote the regeneration of damaged pancreatic cells and restore their number; and oral intake of bitter melon juice can improve the condition and function of the pancreas.
Bitter melon extract can also increase the number and volume of β-cells in the pancreas, thus making the amount of insulin secreted comparable to that of the non-diabetic group.
Bitter melon powder can significantly increase the expression of a gene that regulates the development of the pancreas and stimulates the growth of β-cells in the pancreas.
In addition, animal experiments (pdf) have shown that feeding bitter melon juice to rats with type I diabetes has a good effect on their blood glucose and lipid control.
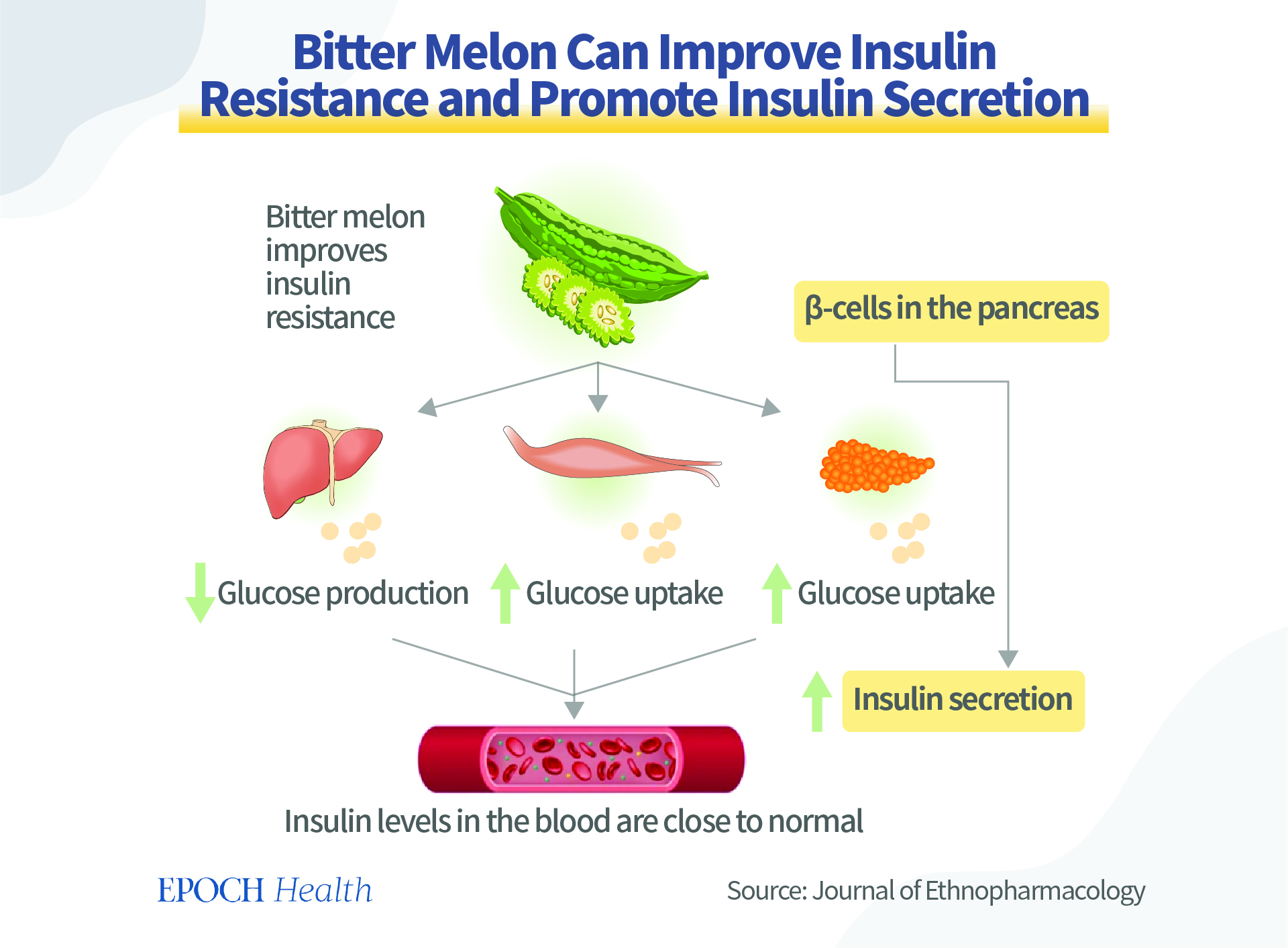
Bitter Melon Can Alleviate Type II Diabetes by Improving Insulin Resistance
Bitter melon can improve insulin resistance by reducing glucose production by the liver, promoting glucose uptake by muscle cells and fat cells, and promoting insulin secretion to lower excessive insulin levels in the blood.
First, several glycosides, polypeptides, and polysaccharides in bitter melon can lower blood glucose.
Second, triterpenoids in bitter melon, such as bitter melon glycosides, and some proteins and peptides can increase the uptake, consumption, and utilization of glucose by cells. Some can be achieved by cooperating with insulin, and some can act independently of insulin.
Third, the bitter melon glucoside and charantin can inhibit the action of some enzymes and delay the absorption of sugar. In addition, the rich fiber of bitter melon can also slow down the absorption of glucose.
Fourth, bitter melon can inhibit the production of glucose by liver cells, as well as inhibit gluconeogenesis (creating glucose from non-carbs) in the liver.
Fifth, bitter melon can inhibit enzymes related to islet resistance, thus regulating insulin resistance.
Bitter Melon Has a Glucose-Lowering Effect and Cardiovascular Protection Function
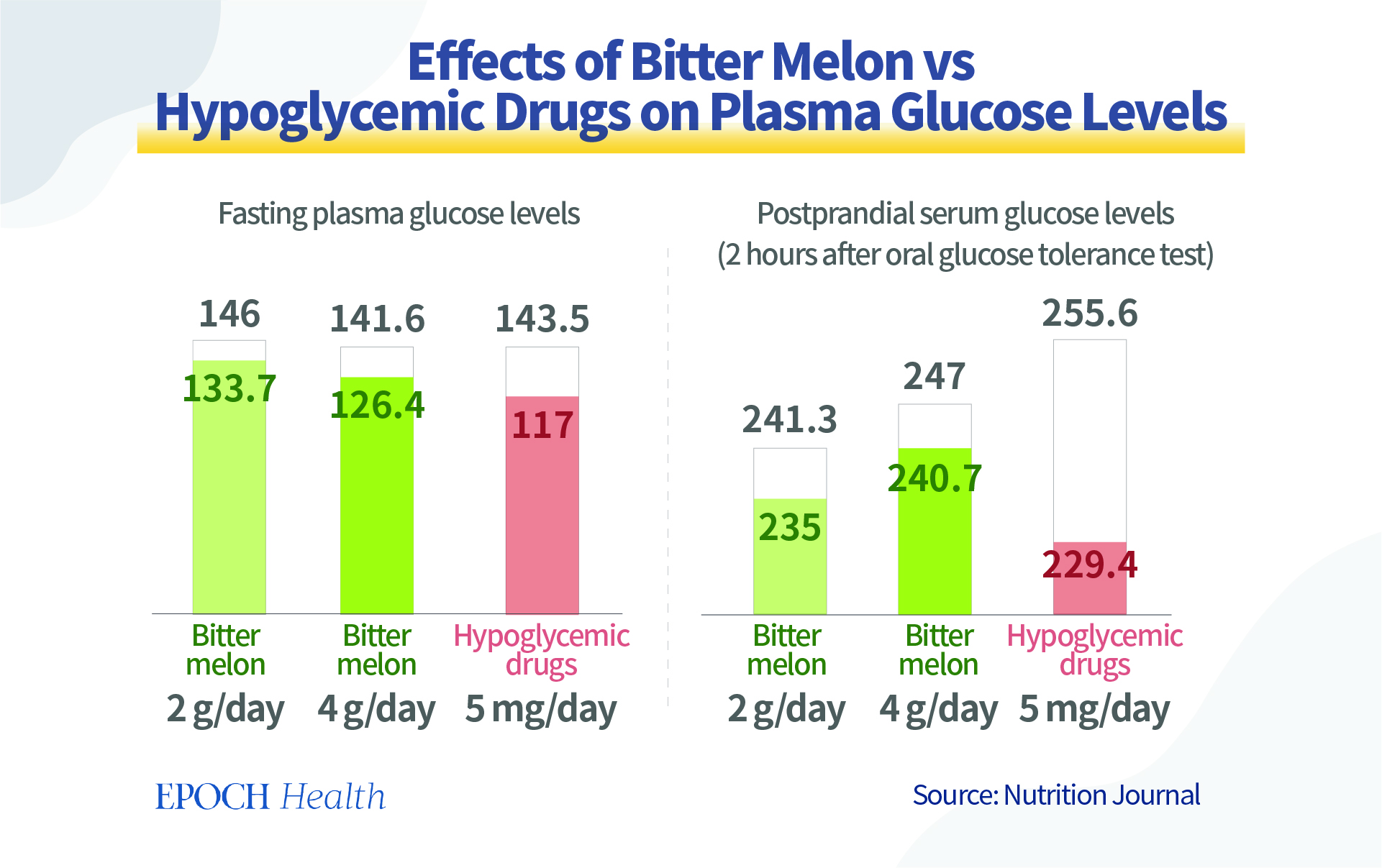
There have been some small clinical trials on the consumption of bitter melon, which showed similar effects to those of hypoglycemic drugs.
In India, a group of patients with type II diabetes who had their oral hypoglycemic medication reduced by half and took bitter melon extract had a greater hypoglycemic effect after secen days than a control group taking a full dose of hypoglycemic medication.
In 100 patients with moderate non-insulin-dependent diabetes (NIDDM) who consumed bitter melon juice, 86 percent of them showed significant reductions in both fasting and postprandial serum glucose levels, and another 5 percent showed reductions in fasting serum glucose.
Another randomized controlled trial in non-insulin-dependent diabetics showed that the effects of taking bitter melon extract were similar to those achieved with the antidiabetic drug rosiglitazone.
Another common glucose-lowering drug is metformin. In a four-week double-blind randomized controlled trial, researchers evaluated the efficacy of bitter melon and metformin in patients with newly diagnosed type II diabetes and concluded that bitter melon had a modest hypoglycemic effect compared to the drug, a conclusion similar to that of another controlled trial using bitter melon and glibenclamide in 2015.
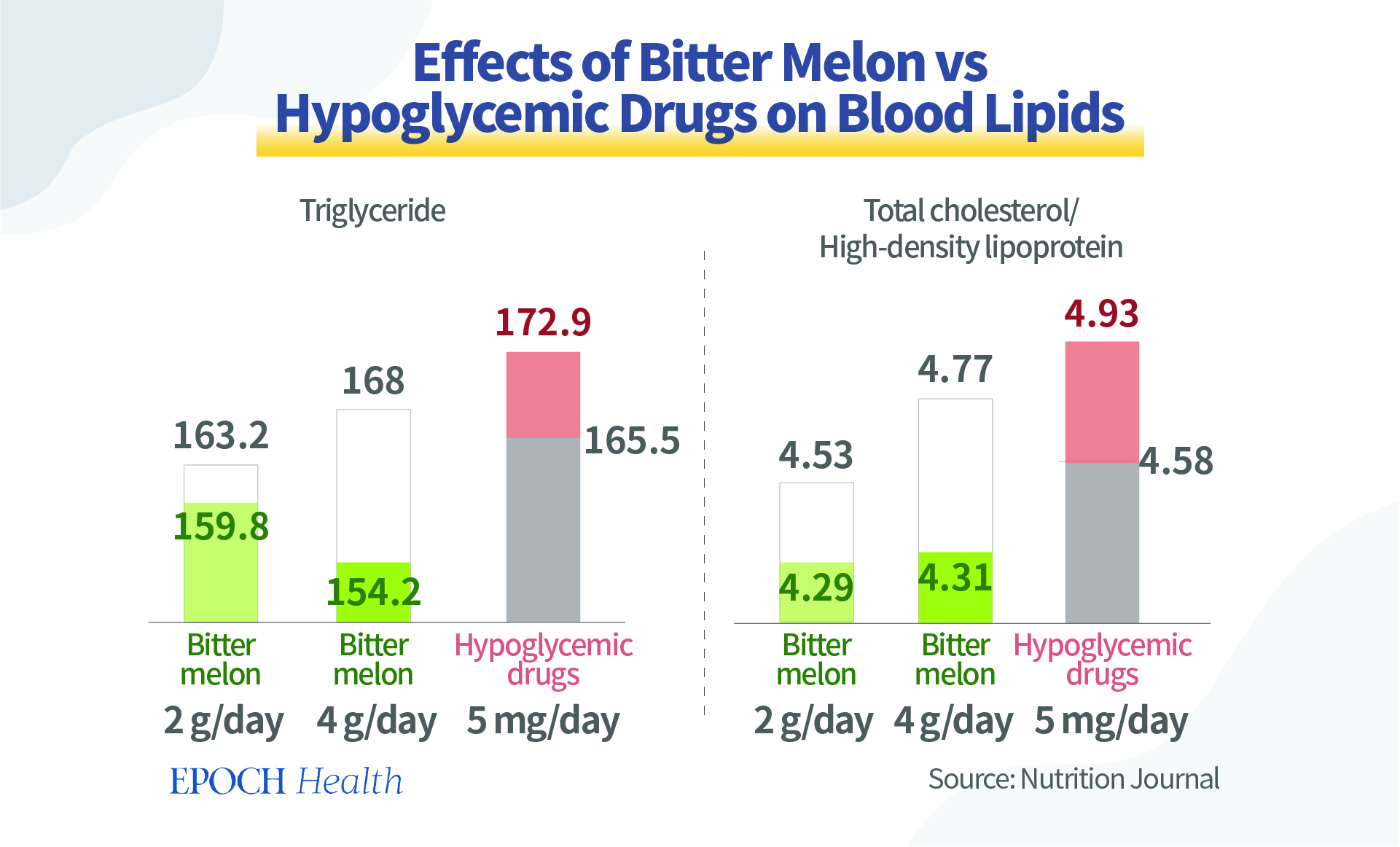
Moreover, a 2015 experiment published in Nutrition Journal further found that triglyceride and total cholesterol levels were significantly lower in those using bitter melon, while blood lipids increased in those taking the drug.
This indicates that bitter melon has a comprehensive effect on diabetics in terms of lipid regulation and metabolism, in addition to lowering sugar. Moreover, bitter melon is a natural food, which can avoid some side effects and harm of drugs to the body.
2 Types of People Need to Take Extra Caution
The bitter melon is a valuable vegetable, but some people need to take extra care when eating it.
Given the hypoglycemic effect of bitter melon, it is best not to ingest bitter melons on an empty stomach.
Moreover, bitter melon has been used in some traditional medicine for abortion and contraception.
Studieshave shown that bitter melon may have a risk of miscarriage and congenital malformation (pdf). Bitter melon also causes a significant decrease in estrogen and progesterone levels, showing anti-fertility and anti-sperm effects. Therefore, bitter melon should be used with caution in diabetic patients who are planning to get or are already pregnant.
It has also been suggested by researchers that removing the seeds when consuming the fresh fruit of bitter melon may reduce the risk of some adverse events.
Aqueous extracts of bitter melon have been found to be more effective in treating diabetes than dried powder. This may be due to the loss and or inactivation of some active ingredients as a result of drying and further processing of the powder. Freeze-dried extracts of bitter melon juice have been used in some human studies because of the relatively good preservation of their biological activity and the ease of handling.
When choosing to acquire the beneficial components of bitter melon through supplements, a daily intake of 3 mg cucurbitane-type triterpenoids may be a reasonable amount, which is the average intake amount of many bitter melon supplementation products.
Do your blood sugars rise early every morning, for no apparent reason? You may be experiencing “dawn phenomenon.” It’s frustrating, but it’s common, and this article will help you with a few strategies for preventing those glucose spikes.
There are several possible causes of a high blood sugar level in the morning:
Dawn phenomenon. This occurs when your body releases a surge of hormones overnight, which then triggers your liver to dump sugar into your blood. This is an entirely natural process, but people with diabetes cannot properly secrete or utilize insulin to counteract the blood sugar rise.
Reactive hyperglycemia, also called the Somogyi effect. This is distinct from dawn phenomenon. It happens when low blood sugar in the middle of the night triggers your liver to dump sugar into your blood in an attempt to stabilize your blood sugar.
Finally, your blood sugar may simply rise overnight for less complex reasons. Perhaps your basal insulin dosage isn’t set quite right, or a late-night meal took hours to cause a glucose spike.
Why Are My Blood Sugars High in the Morning?
Here’s a simple plan for diagnosing the source of high blood sugars in the morning.
Test your blood sugar before you sleep.
Test your blood sugar in the middle of the night.
Test your blood sugar first thing in the morning.
It takes a little bit of effort, but you probably only need to do it a few times to diagnose the issue.
To diagnose either dawn phenomenon or Somogyi effect, experts recommend checking blood sugar levels for several nights, specifically between 3 a.m and 5 a.m.
Compare these three glucose values and find the pattern:
If your blood sugar stayed steady overnight, but rose in the morning, you are likely experiencing dawn phenomenon.
If your blood sugar rose steadily throughout the night, your morning glucose highs may be the result of your diet choices (for example, a carbohydrate-heavy bedtime snack), or a sign that you may want to adjust your insulin and glucose-lowering medication regimen.
If your blood sugar dipped low in the middle of the night, you may be experiencing Somogyi effect.
The best option is to use a continuous glucose monitoring system (CGM). This will give you an entire night’s worth of blood sugar values, making it easy to identify what direction your blood sugar moved while you slept, without having to set an alarm in the middle of the night.
If you think you’ll have a tough time having insurance approve the use of a CGM (especially if you have type 2 diabetes), talk to your healthcare provider about the use of a CGM on loan. Only a few days of data will teach you a lot. Visit our learning page on CGM to learn all about this vital technology.
How to Fix High Blood Sugars in the Morning
The Dawn Phenomenon
More than half of people with diabetes (including both types 1 and 2) are thought to experience dawn phenomenon, and it can lead to significant increases in A1C.
The dawn phenomenon begins when your body secretes a surge of hormones, including growth hormone, cortisol, adrenaline, and glucagon. These hormones start working very early each morning around the same time to prepare your body to wake. Basically, your body is starting the engine, releasing some fuel, and prepping to go for the day.
These hormones trigger the conversion of the liver’s glycogen stores into glucose, which is then dumped into the blood in a process called glycogenolysis.
Source: The University of California, San Francisco
This general process occurs in all humans regardless of whether they have diabetes. In people without diabetes, the body’s natural insulin response prevents the blood sugars from rising. In people with diabetes, though, the body is unable to produce a healthy insulin response, and therefore blood glucose levels spike up.
The Mayo Clinic suggests several strategies you can try to combat the effects of dawn phenomenon:
Use an insulin pump to administer extra insulin during early-morning hours.
Avoid carbohydrates at bedtime.
Adjust your dose of medication or insulin. (If you take a long-acting insulin such as Lantus, be aware it doesn’t last a full 24 hours. This means you may want to try taking it at night or splitting the dose by taking half in the morning and the other half 12 hours later.)
Switch to a different glucose-lowering medication.
Adjust the time when you take your medication or insulin from dinnertime to bedtime.
Dawn phenomenon also contributes to early morning insulin resistance. You may want to limit carbohydrates during the hour or two after you wake up. Insulin-users may need to have a higher insulin-to-carb ratio and take more insulin in the morning than during other parts of the day.
Some patients probably don’t need to be too concerned about dawn phenomenon. If most of your night is spent with normal blood sugars, and you experience a small, temporary increase in the morning, there is likely little to worry about. For those that are otherwise usually in their target blood sugar range, the morning increase is often less than they experience during a typical meal, and even more short-lived.
High Blood Sugars from the Night Before
If you are experiencing high blood sugar in the morning as a result of elevated blood sugar from the night before, there are several things you could try:
Eat fewer carbohydrates during the evening hours.
Add evening exercise like an after-dinner walk.
In consultation with your doctor, increase blood sugar lowering medication or insulin.
Reactive Hypoglycemia (Somogyi Effect)
This is also known as rebound hypoglycemia, or the Somogyi effect. It is less common than dawn phenomenon.
If your blood sugar goes too low overnight, it may explain elevated morning blood sugar levels. Your body essentially goes into panic mode and attempts to save you by secreting counter-regulatory hormones like glucagon and epinephrine (adrenaline), which then trigger the liver to change its reserves of glycogen into glucose. In short, your body senses a low and dumps as much sugar as it can into the blood in an attempt to get enough fuel to function.
Here are some things you could try to reduce this occurrence:
Eat a carbohydrate snack before bed.
Reduce blood sugar-lowering medication or insulin in the evening.
Reduce your long-acting insulin dose.
Change your exercise schedule from afternoon or evening to morning.
Make sure you don’t ignore reactive hypoglycemia. It’s a sign that your blood sugar is approaching dangerous levels overnight.
Over time, your body’s response to low blood sugar levels may change due to hormone changes, leaving your body unable to warn you of low blood sugar symptoms and unable to trigger the liver into dumping sugar into your blood. Also, if other low blood sugar episodes have occurred earlier the same night or excess exercise has taken place, the liver may have already depleted its reserves of glycogen and may not be able to secrete glucose and raise your blood sugar.
Summary
If your blood sugar is high in the morning, it’s important to figure out why. Use a CGM, or an alarm clock and a blood sugar meter, to examine your overnight blood glucose for trends and figure out what’s happening.
I just finished watching Netflix’s smash hit film Purple Hearts. If you’re not familiar with it yet, it’s a romance centered on Cassie, a young woman who’s six months into her type 1 diabetes diagnosis. While at its core this film is a love story, Cassie’s diabetes and her incredible struggle with healthcare in America is the main plot of the film.
People in the diabetes community are saying it’s one of the best representations of diabetes in Hollywood history. So, did it live up to the hype?
If you plan on watching it, be forewarned, SPOILERS are coming up!
WHAT THE FILM GOT RIGHT
For diabetes accuracy, this movie excels! It describes what life is really like for Americans with type 1 diabetes right now, particularly for lower-income individuals or those with part-time or freelance jobs. These were the highlights:
The state of healthcare in America. This is probably the most important aspect of the film.
The movie shows what too many of us already know: that the cost of insulin in America is astronomically high. Cassie needs to pay $300 for long-acting and $220 for short-acting insulins without insurance. $500-plus per month is typical in the United States, if not lower than average.
Because she can’t pay for all of the insulin she needs, Cassie ends up rationing insulin, a potentially deadly strategy that is all too common in the U.S.
The pharmacy couldn’t refill her prescription early unless she paid out of pocket, as the cashier stated her “insurance wasn’t renewed.” While this term isn’t something I’ve personally heard before, the frustration and exasperation with an impossible-to-understand system is very accurate.
Cassie is living with huge medical debt and being forced to choose between paying rent and buying insulin. The stress from her medical debt keeps her up at night — so much so that she’s willing to break the law to get better healthcare to afford insulin.
What life with type 1 diabetes is really like. Finally, a film gets this mostly right!
This is the best Hollywood depiction of type 1 diabetes that I ever remember seeing. It sounds simple, but Cassie checks her blood glucose with a finger poke, squeezes out the blood to put on a test strip, and gives herself insulin — exactly what we really do! So many movies get this fundamental stuff completely wrong.
While some of the scenes seemed overacted and exaggerated, it’s done to make sense for those not living with diabetes watching the film. In general, Cassie’s high and low symptoms are accurate. She’s tired with blurry vision when she realizes she needs a correction. She’s wobbly and disoriented when her blood sugar is dropping.
She sets an annoying alarm to make sure she remembers to administer insulin. We know what it’s like when you forget!
The movie also gets a ton of tiny details right. The way Cassie turns the insulin vial upside down and flicks the bubbles out of the needle. How she bends her leg and rests her arm on her knee to get the “meat” in her tricep to make it easier to inject into her arm. I learned that trick when I was a kid and have used it SO many times in my life! If you’ve done this before, you know exactly what I’m talking about.
She keeps all of her diabetes stuff in her purse. If you looked in my purse right now, you’d find a loose syringe and a backup bottle of insulin with maybe 20 units left in it. Oh, and a juice box, fruit snacks, and a VERY old granola bar that I’m sure have been there for three years. If you know, you know.
How excited she is to go on an insulin pump and continuous glucose monitor (CGM) after struggling for so long without the best tools! Many of us remember how exciting it was to finally win approval from insurance for these expensive but vital devices. Her happy dance says it all!
Keeping her pump in her back pocket and giving a quick correction bolus like we’ve all done a hundred times.
Going low in the middle of the night after unexpected activity, and also seeing zero units of insulin on board (IOB) on her pump screen when she couldn’t remember the last time she ate. They definitely got this one right!
The technology.
Her Medtronic pump and Guardian CGM are the newest versions on the market, the MiniMed™ 770G with SmartGuard™ Auto Mode. The film shows realistic insertions of both the infusion and sensor sites.
You hear Cassie’s CGM alarm and you see the reading: 68 mg/dL with a triple down arrow. I think I can safely say that we’ve all had this experience, where your glucose just drops so quickly that your CGM can’t even keep up. You’re fine one moment and then all of a sudden you feel SUPER low and are stumbling around. This representation is 100 percent authentic.
The diabetes lingo. So many other movies and TV shows get this so incredibly wrong. Cassie spoke like a real person with diabetes.
“Reserve,” the backup insulin vial that has a little bit left just in case
“Short-acting” and “long-acting” insulins
“Go, Big Pharma,” said in a sarcastic tone
The relationships. Cassie is surrounded by well-meaning people who try to be supportive but don’t really understand what she’s going through. Many people with type 1 know exactly what this is like.
Cassie’s mother is supportive and understands how serious the condition is. She asks Cassie to move back home so she can help shoulder the burden. However, she doesn’t understand just HOW expensive Cassie’s insulin is — at one point she gives her daughter $80, not realizing that it’s not even close to what she needs. Even though Mom has the best of intentions, she doesn’t completely understand what it’s like for her daughter.
The pharmacy cashier doesn’t really seem to understand that if Cassie can’t get insulin, she could die. She doesn’t assist or provide any resources for Cassie to get the insulin she needs. This is a common story we hear in the community often. There are resources for people that cannot afford their insulin.
Cassie’s friends and husband give her space to do diabetes things, but don’t really understand or know how to help.
I love that as the romance progresses, Luke begins to understand Cassie’s diabetes better. When he hears her alarms, he runs to grab the glucose gel and quickly learns that T1D can be scary. It’s an accurate relationship scenario.
WHAT WASN’T SO ACCURATE
As realistic as the film’s depiction of diabetes was, it’s still a movie, and there were moments that felt over the top. I have a brother who is a director and editor (he also has type 1!), so I can appreciate that movies need to exaggerate to get the point across and to heighten the drama. A mild low blood sugar that you fix with a few glucose tabs isn’t exactly exciting. One example: The filmmakers had Cassie use a massive syringe, with a needle that was MUCH larger than any needle I’ve ever seen used for insulin.
More importantly, Cassie’s symptoms (or lack thereof) felt exaggerated to me. She’s rationing her insulin so we know she’s going to be high. But the intensity of her symptoms — labored breathing, stumbling, sweating, and exhaustion – make it seem like she’s experiencing diabetic ketoacidosis (DKA). She injects some insulin, and the next day she seems healthy again. That’s just not how that works.
She also rebounded very quickly from that 68 mg/dL triple down arrow to make out with her husband. I think she’s about to find out that physical activity after hypoglycemia usually brings more lows. 😉
MISSED DIABETES OPPORTUNITIES
As good as the movie’s depiction of diabetes was, I felt it could have done an even better job. Here’s what I wish Purple Hearts had shown:
I wanted to see more of those little management moments highlighting how exhausting and all-encompassing T1D is. We are always looking, checking, and adjusting: briefly checking your CGM graph, mindlessly touching your pump or sensor site, or slightly adjusting your pump on your waistband when you sit down. (My brother disagreed. He was glad that the film focused more on character development and their relationships.)
Cassie was never shown bolusing for food or managing her blood sugar around meals. This might have been done on purpose, to avoid the stigma around food and diabetes. But I think it was a missed opportunity to show the reality of how central food is to our condition, and how stressful diabetes makes every meal.
Cassie’s insulin pump is almost never visible. While I often try to hide my insulin pump, you can still see the outline under my clothes, and when I’m around close friends or family, I don’t bother tucking the tubing away. There aren’t many of these moments in the film, and with some of the wardrobe choices, it would have been tough to hide her pump. I feel this doesn’t accurately represent how intrusive and omnipresent a tubed pump is.
The film features a conversation about Cassie and Luke having children. They are sitting around the table in the backyard and Luke’s sister says how great he’d be with kids. There is an awkward pause, and Cassie says nothing. This would have been a nice moment to say something about type 1 diabetes and pregnancy. Again, another lost moment.
I think Purple Hearts did a great job portraying life with type 1 diabetes, both for people from the diabetes community and for viewers just learning about the condition. I hope this movie helps the world better understand what many Americans are facing each and every day.
Adolescents’ risk for developing type 1 diabetes rose with increasing BMI, according to data presented at the American Diabetes Association Scientific Sessions and simultaneously published in Diabetologia.
“There were previous reports on the association between obesity and type 1 diabetes in previous cohorts that included mostly children,” Gilad Twig, MD, PhD, a resident in the department of internal medicine at Sheba Medical Center in Tel Aviv, Israel, told Healio. “We were somewhat surprised to see that the association persisted in adolescents who were perfectly healthy — apart from having abnormal weight — without apparent risk factors for type 1 diabetes.”
Teens in the 75th percentile or higher of BMI have a greater risk of developing type 1 diabetes as adults than those below the 50th percentile of BMI. Data were derived from Zucker I, et al. 1263-P. Presented at: American Diabetes Association Scientific Sessions; June 3-7, 2022; New Orleans (hybrid meeting).
Twig and colleagues conducted a retrospective cohort study of adolescents aged 16 to 19 years who underwent a medical examination prior to military conscription in Israel from January 1996 to December 2016. Data from participants were linked to the Israeli National Diabetes registry. BMI was calculated using height and weight measured at baseline. Participants were placed into age- and sex-matched percentiles based on criteria from the CDC. Participants in the 85th to 94th percentile of BMI were considered to have overweight, and obesity was defined as the 95th percentile or higher.
There were 834,050 men and 592,312 women included in the study. Over a median follow-up of 11.2 years, there were 777 incident type 1 diabetes cases during 15,819,750 person-years, for an incidence rate of 4.9 cases per 100,000 person-years.
The risk for type 1 diabetes gradually increased with higher BMI. In multivariable analysis, adolescents in the 75th to 84th percentile of BMI (adjusted HR = 1.41; 95% CI, 1.11-1.78), with overweight (aHR = 1.54; 95% CI, 1.23-1.94) and with obesity (aHR = 2.05; 95% CI, 1.58-2.66), had an increased risk for type 1 diabetes compared with those in the fifth to 49th percentile of BMI.
“For adolescents with obesity, the risk for type 1 diabetes was approximately doubled,” Twig said. “It is important to remember that in our study, we grouped all those with obesity in the group regardless of obesity severity. Therefore, it is likely that for adolescents with more severe forms of obesity, the actual risk for developing type 1 diabetes is even higher.”
Each 5-unit increase in BMI was associated with a 35% increase in risk for developing type 1 diabetes (aHR = 1.35; 95% CI, 1.24-1.47) and each 1 standard deviation increase in BMI increased the risk for developing type 1 diabetes by 25% (aHR = 1.25; 95% CI, 1.17-1.32).
Twig said future research is planned to identify more risk factors for incident type 1 diabetes in the same cohort.
“We are, in particular, planning to better identify the characteristics of adolescents in whom excessive weight may have a more emphasized role in the development of type 1 diabetes,” Twig said.
Adults and children with type 1 diabetes who used an insulin-only bionic pancreas had reduced HbA1c without increasing hypoglycemia and other improved metrics compared with standard of care, researchers reported.
The Insulin-Only Bionic Pancreas Pivotal Trial achieved key primary and secondary endpoints in adults and children with type 1 diabetes, according to data presented during a mini-symposium at the American Diabetes Association Scientific Sessions.
Source: Adobe Stock
The iLet bionic pancreas (Beta Bionics) is a pocket-sized, wearable, investigational device designed to autonomously determine and deliver insulin doses to control blood glucose levels for people with diabetes. It is designed to be worn like an insulin pump; however, users would enter only their body weight to initialize therapy and would not set any insulin parameters. The device is designed to automatically titrate and infuse insulin without requiring the user to count carbohydrates, set insulin-to-carbohydrate ratios, set insulin basal rates, set correction factors or determine bolus insulin for meals or corrections, according to a company release.
This is a “fairly new and different concept in automation,” Greg Forlenza, MD, associate professor of pediatrics at the Barbara Davis Center for Diabetes at the University of Colorado Anschutz Medical Campus, said during a presentation.
Large, diverse trial
The pivotal trial was designed to evaluate safety and efficacy of the iLet bionic pancreas compared with current standard of care for insulin-treated diabetes over 13 weeks.
“This is the largest randomized controlled trial ever conducted to evaluate the safety and efficacy of an automated insulin delivery system,” Steven J. Russell, MD, PhD, associate professor of medicine at Harvard Medical School and Massachusetts General Hospital, said during the presentation.
The study population consisted of 440 adults and children aged 6 years and older with type 1 diabetes at 16 U.S. sites.
“This randomized trial included a more diverse population of adults with type 1 diabetes than previous pivotal studies of hybrid closed-loop systems with respect to minority representation, method of insulin delivery and HbA1c levels,” Davida Kruger, MSN, APN-BC, nurse practitioner at Henry Ford Health System, said here.
Participants were randomly assigned to the bionic pancreas or to continue their standard of care from January to July 2021. Seventy-seven percent of participants were non-Hispanic white, 10% non-Hispanic Black, 9% Hispanic or Latino and 4% other. The standard of care group was comprised of about one-third on automated insulin delivery systems, one-third on insulin pump therapy with continuous glucose monitoring and one-third on multiple daily injection therapy with CGM, Forlenza said.
The primary outcome was HbA1c at 13 weeks.
Primary analysis results
The primary analysis compared outcomes with the bionic pancreas, using insulin lispro (Humalog, Novo Nordisk) or insulin aspart (NovoLog, Novo Nordisk), with standard of care in 326 adults and children. The remaining 114 adults used the bionic pancreas with rapid-acting insulin (Fiasp, Novo Nordisk).
At 13 weeks, the following outcomes were improved over standard of care:
Significant reduction in HbA1c: At 13 weeks, mean HbA1c was reduced by 0.5% in the bionic pancreas group vs. standard of care (P < .001). In those with baseline HbA1c higher than 7%, the mean HbA1c reduction was 0.7% for the bionic pancreas group vs. standard of care (P < .001).
No increase in hypoglycemia: Those who used the bionic pancreas did not experience any significant increase in average time spent with CGM values less than 54 mg/dL over 13 weeks compared with standard of care (P < .001 for noninferiority).
Increased time in range: Those who used the bionic pancreas had an average of 2.6 hours more time in range (70-180 mg/dL) per day over 13 weeks vs. standard of care (P < .001).
Additional analyses
Kruger reported results from 161 adults using insulin aspart or lispro. In this cohort, mean HbA1c decreased from 7.6% at baseline to 7.1% at 13 weeks in the bionic pancreas group vs. 7.5% in the standard of care group (P < .001). Moreover, HbA1c improvement greater than 0.5% at 13 weeks occurred in 43% of the bionic pancreas group vs. 17% of the standard of care group (P < .001) and greater than 1% in 23% vs. 4%, respectively (P < .001). Greater improvements occurred in those with higher baseline HbA1c levels, Kruger said.
Time in range improved after just 1 day of use of the bionic pancreas, Kruger said. At 13 weeks, those assigned the bionic pancreas spent 11% more time in range (2.6 hours per day) compared with standard of care (P < .001). The researchers reported no difference in time spent below 54 mg/dL.
Seven severe hypoglycemia events were reported in the bionic pancreas group (25.5 per 100 person-years) and two in the standard of care group (14.2 per 100 person-years). No diabetic ketoacidosis events occurred. Thirty hyperglycemia adverse events associated with infusion set failures occurred in the bionic pancreas group (failure rate = 0.9 for 3,203 infusion sets), according to the presentation.
Laurel H. Messer, PhD, presented results from 165 children using insulin aspart or lispro. In the pediatric cohort, mean HbA1c decreased from 8.1% at baseline to 7.5% at 13 weeks in the bionic pancreas group and remained steady at 7.8% in the standard of care group (P < .001). HbA1c improvement greater than 0.5% at 13 weeks occurred in 51% of the bionic pancreas group vs. 17% of the standard of care group (P < .001) and greater than 1% in 29% vs. 6%, respectively (P < .001). As in adults, greater improvements in HbA1c occurred in those with higher levels at baseline.
At 13 weeks, those assigned the bionic pancreas spent 10% more time in range (2.4 hours per day) compared with standard of care (P < .001). Again, there was no difference in time spent with glucose below 54 mg/dL, Messer said.
Laurel H. Messer
Three severe hypoglycemia events were reported in the bionic pancreas group (10.4 per 100 person-years) and one in the standard of care group (7.3 per 100 person-years). No DKA events occurred. There were 30 hyperglycemia adverse events associated with infusion set failures in the bionic pancreas group (failure rate = 3% for 3,420 infusion sets), according to the presentation.
In these analyses, Kruger said the benefits of the bionic pancreas were “more prominent in multiple daily injection users without having a pre-randomization run-in period to initiate pump use, and the benefit was seen across race/ethnicity and socioeconomic status subgroups.”
In another analysis, Russell highlighted a comparison of the bionic pancreas using rapid-acting insulin aspart (n = 114 adults) compared with standard of care (n = 54 adults) and compared with the bionic pancreas using insulin aspart or insulin lispro (n = 107 adults).
“Compared with standard care, HbA1c was improved with the bionic pancreas using fast-acting insulin aspart without increasing CGM-measured hypoglycemia,” Russell said.
At 13 weeks, mean HbA1c decreased from 7.8% to 7.1% in the rapid-acting insulin aspart group and from 7.6% to 7.1% in the insulin aspart/lispro group (P < .001 for both).
“Compared with the bionic pancreas using insulin aspart or lispro, there was no difference in HbA1c, no difference in mean glucose, a 2% difference in mean time in range due to differences during the daytime, an increase in the proportion with time in range greater than 70% and no significant difference in the proportion with an increase in time in range by 5% or more or 10% or more,” Russell said.
In other results, there were no differences between the groups across nine patient-reported outcome surveys, according to Russell.
Jill Weissberg-Benchell, PhD, CDCES, with Ann and Robert H. Lurie Children’s Hospital of Chicago, reported additional patient-reported outcomes. Adults using the bionic pancreas cited reduced diabetes distress, improved fear of hypoglycemia and improved well-being. Among pediatric patients using the device, distress at baseline was associated with a steeper decrease in HbA1c compared with the standard of care group, Weissberg-Benchell said. Parents of the children in the study also reported satisfaction and acceptability of the bionic pancreas, she said.
Taken together, “Compared to a challenging standard of care, the bionic pancreas reduced HbA1c by a clinically significant margin (0.5%) overall and in subgroups; did not increase hypoglycemia; increased time in range by 2.4 to 3.1 hours per day; decreased mean glucose, time above 180 mg/dL and above 250 mg/dL; gave reasonable control of glycemia without CGM input; and autonomously produced and updated an open-loop regimen that gave reasonable control of glycemia,” Russell said.
Adults with type 1 diabetes for 50 years or more are less likely to have distal symmetric polyneuropathy if they performed at least 150 minutes of physical activity weekly, according to study data.
Evan Lewis
“These findings provide strong support to clinicians discussing physical activity with their patients as a strategy to reduce the risk of diabetes complications,” Evan Lewis, PhD, a postdoctoral researcher at the Lunenfeld-Tanenbaum Research Institute, Mount Sinai Hospital, in Toronto, told Healio. “Our findings showed that higher self-reported physical activity lowered the incidence of neuropathy by 12% in individuals with long-standing type 1 diabetes. There is potential that habitual physical activity earlier in the natural history of diabetes could have a more protective effect for nerves, from blood sugar control and support for the health of nerves.”
Source: Adobe Stock
Lewis and colleagues analyzed findings from phase 2 of the Canadian Study of Longevity in Type 1 Diabetes. The study cohort included 75 adults with a type 1 diabetes duration of at least 50 years (55% women; mean age, 66 years). Participants underwent neurologic testing, including a nerve conduction study, and an assessment of the peroneal and sural nerves. The Lifetime Physical Activity Questionnaire was conducted to assess leisure and household physical activities per week.
The findings were published in the Journal of Diabetes and Its Complications.
Of the study cohort, 89% had distal symmetric polyneuropathy, 11% had stage 3 chronic kidney disease and 20% had cardiovascular disease. Participants engaged in a mean of 156 minutes of physical activity per week, with 47% meeting clinical practice guideline recommendations of 150 minutes per week and 37% reporting at least 210 minutes of weekly physical activity.
“We were surprised to see the level of activity in our study group,” Lewis said. “This was a pleasant surprise that almost half of study participants were meeting or exceeding the recommended 150 minutes per week.”
Adults with distal symmetric polyneuropathy performed less physical activity per week compared with those without the condition (141 minutes vs. 258 minutes; P = .015). The prevalence of distal symmetric polyneuropathy was 83% in those who performed more than 150 minutes of physical activity per week compared with 95% in those who reported less physical activity (P = .015). Increased distal symmetric polyneuropathy pain was associated with progressively less physical activity (P for trend = .015).
In correlation analysis, more physical activity was associated with better peroneal and sural amplitude, conduction velocity and peroneal F-wave latency. Each 30 minutes of physical activity resulted in a 0.09 mV higher peroneal amplitude (P = .032) and 0.048 millisecond lower peroneal F-wave latency (P = .022), markers for improved nerve function. Physical activity level was not associated with cardiac autonomic neuropathy.
“This study provides strong rationale for studying the effect of exercise prescription in a clinical setting,” Lewis said. “We are also interested in further investigating the neuroprotective role of exercise and if these benefits are limb-specific or systemic.”