KEY POINTS
- Catheter-associated thrombosis is the most common noninfectious complication of implantable venous access devices and can cause superior vena cava syndrome.
- The diagnosis can be confirmed with Doppler ultrasonography or contrast-enhanced computed tomography.
- Anticoagulation with or without catheter removal is the initial treatment of choice; endovascular intervention is reserved for patients who do not respond to anticoagulation.
- Prophylactic approaches to catheter-associated thrombosis are not recommended, and the use of superior vena cava filters in deep vein thrombosis of the upper extremities should be avoided.
A 53-year-old man presented to the emergency department with a 3-week history of throbbing headaches, dizziness and cyanosis, with worsening symptoms over the previous 7 days. The patient had a history of colon cancer 2 years previously and had undergone a total colectomy complicated by a high-output ostomy. A reverse ostomy had been delayed until his body mass index decreased to reduce the risk of complications. He had an implantable venous access device in the right side of his chest that had been implanted for chemotherapy administration, frequent blood work and weekly hydration. Five weeks before presentation, his port had become blocked and he was therefore unable to receive intravenous hydration. His home care nurse had tried unsuccessfully to unblock it with tissue plasminogen activator. While he was waiting for an appointment with his family physician, he had been advised to increase his daily fluid intake to about 2.5–4.0 L per day.
On presentation, the patient had marked orthostatic changes (supine blood pressure 135/85 mm Hg, heart rate 70–90 beats/min; upright sitting blood pressure 80/50 mm Hg, heart rate 140 beats/min). His oxygen saturation was 84% on room air, improving to more than 94% on 3 L of supplemental oxygen. He was afebrile with normal mental status. He had a normal voice tone, and no signs of respiratory distress or stridor. He had marked cyanosis, facial and neck plethora, distended neck veins and engorged superficial chest wall vessels (Figure 1). The port in his right upper chest was tender to palpation. Cardiovascular and respiratory examinations were otherwise normal.
Photographs of the head and upper chest of a 53-year-old man with catheter-associated superior vena cava syndrome, showing (A) facial and neck plethora, and (B) a prominent superficial venous pattern on the chest.
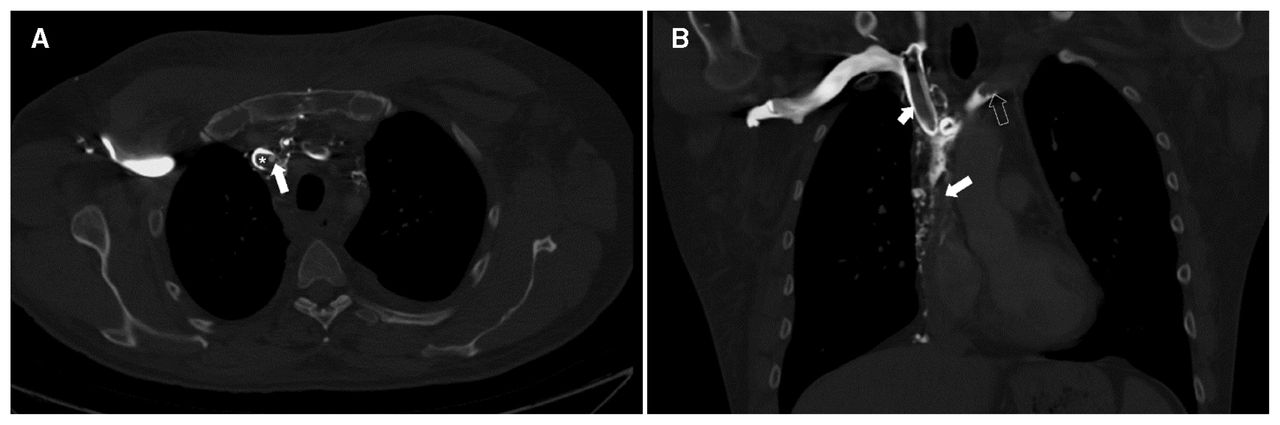
The patient’s complete blood count, coagulation profile, electrolytes, and creatinine were all within the normal range. An ultrasonogram of the upper extremities showed extensive thrombus in the right jugular vein, with minimal residual flow seen on colour Doppler ultrasonography. A computed tomography (CT) chest scan with contrast showed no pulmonary embolism and confirmed thrombus within the lumen of the right internal jugular vein. The superior vena cava (SVC) appeared almost completely occluded immediately above the right atrium distal to the catheter tip, with extensive venous collaterals in the mediastinum, suggestive of SVC syndrome (Figure 2).
(A) An axial contrast-enhanced computed tomography scan of the chest of a 53-year-old man showed obstruction of the superior vena cava secondary to the indwelling catheter (arrow) and the adherent thrombus (*). (B) A coronal contrast-enhanced computed tomography scan of the chest showed extensive thrombus in the right brachiocephalic vein (short arrow), left brachiocephalic vein (empty arrow) and superior vena cava (long arrow), as well as enlarged mediastinal collateral veins.
We started the patient on intravenous crystalloid fluids and subcutaneous low-molecular-weight heparin. We removed the indwelling port as he was able to maintain hydration through oral intake. While in hospital, he underwent a malignancy workup, including CT of his abdomen, testing of his carcinoembryonic antigen level and a colonoscopy, all of which were negative. He continued to do well and was discharged on a 3-month course of edoxaban. At a 6-month follow-up, the patient was symptom-free with substantial improvement in his facial plethora and in his enlarged neck and chest veins (Figure 3).
Photographs of a 53-year-old man, taken 6 months after his initial presentation with catheter-associated superior vena cava syndrome, showing improvement in his (A) head and neck vein distention, as well as (B) his superficial chest wall collateral veins.
Discussion
Thrombotic occlusion of central venous catheters can occur from the formation of a fibrin sheath around the catheter tip, a blood clot inside the catheter lumen, a partial or complete extraluminal venous thrombosis, or any combination of these.1–3 A thrombosis that occludes the vein is referred to as deep vein thrombosis (DVT). Central venous catheters predispose patients to thrombotic vascular occlusion from endothelial damage caused by friction from the catheter, turbulent blood flow or cytotoxic medications.2,4
Superior vena cava syndrome results from blood flow obstruction within the SVC. Malignant occlusion or compression is the most common cause of acquired SVC obstruction. However, with the more frequent use of intravascular devices such as catheters and pacemakers, nonmalignant causes now account for 28% of cases of SVC syndrome.1,2 Our patient’s SVC syndrome was caused by thrombosis associated with his central venous catheter.
Clinical presentation of SVC syndrome depends on the severity and location of the obstruction, and the development of collateral veins. Typical signs and symptoms of SVC syndrome include facial, neck, trunk or upper extremity swelling and pain (40%–100%); shortness of breath (54%–83%); jugular venous distension (27%); dilated anterior chest collateral veins (40%); and hoarseness, chemosis and plethora. Less commonly, patients can have symptoms of cerebral edema, including headache, confusion, dizziness and altered mental status.1,2 Duplex ultrasonography is generally the first investigation when catheter-associated thrombosis is suspected; however, signs and symptoms of SVC syndrome require prompt evaluation with contrast-enhanced CT.1 In some cases, magnetic resonance or direct contrast venography may be required.2,3 The usefulness of D-dimer testing to exclude device-associated DVT is limited for patients with central venous catheters or pacemakers.1
Management of fibrin sheath formation
Fibrin sheath formation is the most common cause of catheter dysfunction and is classically identified by being able to inject into the device, but having difficulty aspirating from it.3 The firstline treatment is administration of tissue plasminogen activator, a thrombolytic agent, into the port chamber or catheter, allowing 30–120 minutes of dwell time. The tissue plasminogen activator catalyzes the conversion of clot-bound plasminogen to plasmin, which then activates the fibrinolysis cascade.5 Thrombolytic agents successfully restore the patency of the central venous catheter in 87%–90% of cases.2,3 If thrombolytics fail, consultation with an interventional radiologist is recommended for consideration of fibrin sheath stripping or investigation for other complications of central venous catheters.6
Catheter-associated thrombosis
Catheter-associated thrombosis is the most common noninfectious complication of implantable venous access devices, and occurs at a rate of 0.76 (among patients with devices for nonmalignant causes) to 1.71 (among patients with malignant disease) thromboses per 1000 catheter-days.7 In patients with malignant disease, the incidence varies between 1.2% and 13%.7
Catheter-associated thromboses account for about 5%–10% of all cases of DVT, with incidence rising owing to increasing use of central intravenous catheters.6 The incidence of pulmonary embolism from a catheter-associated thrombosis in an upper extremity has been estimated at 10%–15% of all cases.8 Post-thrombotic syndrome presenting with upper extremity pain and swelling has been reported in 7%–37% of patients.2,6,8
Patients at higher risk for catheter-associated thrombosis have left-sided device placement, concomitant infection, larger diameter catheters with multiple lumens, peripherally inserted central catheters, catheter tip malposition, a history of DVT or hereditary thrombophilias.1–3 For patients with malignant disease, risk increases with higher-grade and later-stage cancer, as well as with use of the catheter for chemotherapy.9
Management of catheter-associated thrombosis
The treatment of catheter-associated thrombosis improves symptoms, prevents embolization, decreases long-term morbidity and prevents chronic venous occlusion, loss of vascular access, recurrent thrombosis and post-thrombotic syndrome.1 Anticoagulation is the initial treatment for catheter-associated thrombosis involving proximal upper extremity deep veins. Low-molecular-weight heparin reduces the rate of post-thrombotic syndrome and is the preferred initial agent for the treatment of catheter-associated thrombosis.
Long-term anticoagulation with low-molecular-weight heparin is currently recommended for patients with active cancer, given its superiority over vitamin K antagonists, direct oral anticoagulants and warfarin in preventing recurrent thrombosis.1,3,6 Patients without malignant disease can be transitioned to oral anticoagulants after symptomatic improvement. If warfarin is used, its use should overlap with low-molecular-weight heparin for a minimum of 5 days or until a therapeutic international normalized ratio is reached. Limited data support the use of direct oral anticoagulants for catheter-associated thrombosis; however, given comparable outcomes to warfarin in the management of nonmalignant thrombosis in most other contexts, it is a reasonable option.1
Duration of therapy for catheter-associated thrombosis remains controversial. The current guideline recommends treatment for a minimum of 3 months after catheter removal, and longer if the catheter remains in place.1,3 If the catheter is functioning well and is still required, it need not be removed, and anticoagulation should continue while the catheter remains in place.1,3,6 Catheter removal is indicated if the device is no longer needed, is not functioning properly or is associated with infection. If symptoms persist or worsen despite anticoagulation, endovascular management of the thrombus can be considered.1
In patients with extensive catheter-associated thrombosis refractory to anticoagulation, catheter-directed thrombolysis or thrombectomy may be required for symptom management or to preserve the vascular access site. Patients who do not respond to treatment, typically those with little or no improvement after 3 months of anticoagulation, should be referred to medical centres with expertise in interventional radiology and vascular surgery.1 The benefits of endovascular therapy include a high rate of technical success, low risk of restenosis and low occurrence of procedural complications. In a recent meta-analysis, the patency rate for endovascular therapy in patients with benign SVC syndrome was between 75.8% and 86.3%.10
Superior vena cava filters should be considered only in patients with contraindications for anticoagulation as they have been associated with a 3.8% risk of major complications, including 2% risk of pericardial tamponade and 1% risk of aortic perforation.11
Prevention of catheter-associated central venous thrombosis
Routine use of thromboprophylaxis in patients with central venous catheters is not recommended.1 Thromboprophylaxis may be considered in high-risk patients with cancer when the perceived risk of thrombosis outweighs the risk of bleeding and the burden of anticoagulation. 1,9 Central venous catheters should be used only when necessary, and the smallest catheters should be used, with removal when no longer needed.

{kind=link}
{kind=link}
{kind=link}