Researchers from CCR have discovered that extrachromosomal DNA — small particles of DNA that exist outside of chromosomes — can intensify tumor cell diversity and aggressiveness. The finding, published January 30, 2023, in Cancer Discovery
, helps explain how tumor cells can take on different characteristics, even within the same patient, that make the cancer more difficult to treat.
Typically, two chromosome copies are divided equally into each new cell during cell division, but ecDNA can segregate unequally, explains Anish Thomas, M.D., MBBS, Lasker Clinical Research Scholar in the Developmental Therapeutics Branch. Thus, one daughter cell can get more copies of the ecDNA than the other.
It was this trait that made ecDNAs intriguing to Thomas, whose group studies small cell lung cancer (SCLC), an aggressive form of lung cancer marked by resistance to chemotherapy and poor patient prognosis. Postdoctoral fellow Lorinc S. Pongor, Ph.D., had observed that certain SCLC cells contained abundant copies of a cancer-associated gene called MYC, which acts like a volume control for a broad range of genes that regulate tumor growth.
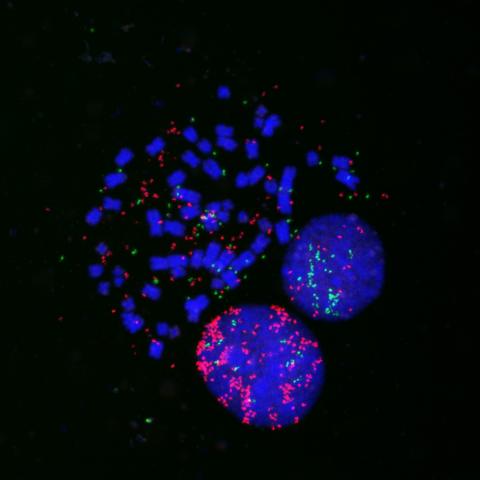
In collaboration with research biologist Darawalee Wangsa, Ph.D., and Thomas Ried, M.D., Senior Investigator in the Genetics Branch, the team confirmed that the extra copies of MYC in SCLC were housed outside the chromosome in ecDNA. They also found that the most common gene rearrangement in SCLC, called an RLF-MYCL fusion, is housed on ecDNA.
To investigate further, the researchers developed a non-invasive method to identify the presence of ecDNA in the blood plasma of patients with SCLC. They then looked at the number of MYC copies in multiple tumors from a patient with detectable ecDNA shortly after the patient passed away.
The patient’s tumor cells from different metastatic sites varied in their ecDNA content. Importantly, the tumor cells that had evolved into a more aggressive cell type contained ecDNA that allowed for many extra copies of MYC.
The researchers next step is to decipher how these genetic factors work together with the tumor’s environment to influence tumor cell aggressiveness. They also plan to investigate how ecDNAs might actively drive tumor metastasis in SCLC, with a continued focus on the amount of MYC in cells.
Thomashopes that their non-invasive detection of tumor ecDNA can one day be used to identify patients who are more likely to develop aggressive disease. While this is the first study to describe ecDNAs in SCLC, “fundamentally, it provides more insight into how tumors become diverse and aggressive, and how a single treatment might not be effective at hitting all the different types of tumor cells,” Thomas says.
