A major bottleneck in early detection is the molecular heterogeneity between ovarian cancer (OC) patients, which limits the likelihood of identifying individual biomarkers that are shared among patients. In a new study “A personalized probabilistic approach to ovarian cancer diagnostics,” published in Gynecologic Oncology, researchers from Georgia Institute of Technology have addressed this challenge by applying machine learning (ML) on patient metabolic profiles to identify biomarker patterns for personalized OC diagnosis.
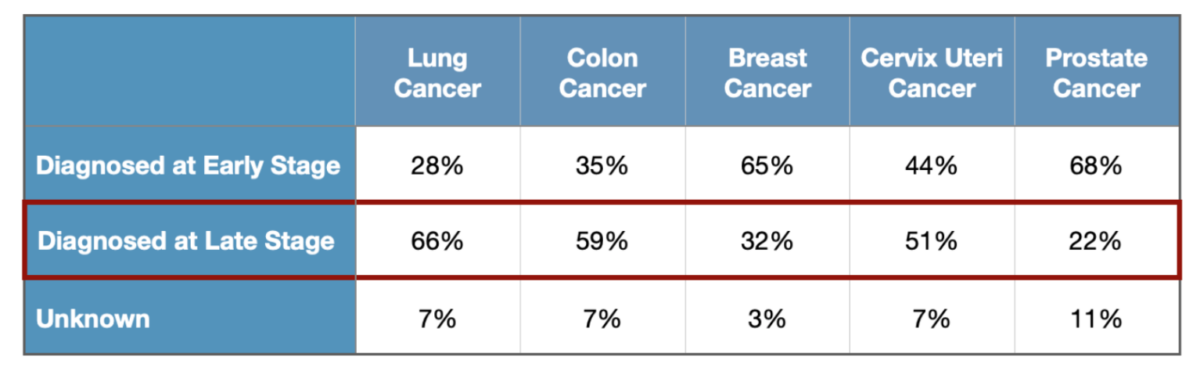
While early diagnosis is often crucial for successful cancer treatment, accurate diagnostics is especially challenging for diseases, such as OC, which progress rapidly yet display little clinical symptoms during the early stages of disease. While the average five-year survival rate for late-stage ovarian cancer patients with treatment is only 31%, that number rises to over 90% when the cancer is detected and treated early.
The Georgia Tech researchers developed ML-based classifiers that were able to distinguish cancer from control samples with 93% accuracy when tested over 564 patient samples from Georgia, North Carolina, Philadelphia, and Western Canada.
John McDonald, professor in the School of Biological Sciences at Georgia Tech and corresponding author of the study, told IPM, “the big buzz in therapeutics is targeting individual genes for personalized therapy. That can work if you have the same target in all of the patients with that disease, but that may not be the case. When we look at the success of targeted immune therapies in OC, it only works in about 5% of patients because the patients are so heterogeneous.”
While profiling individual patients addresses the challenge of patient heterogeneity, McDonald highlights that there’s a need to “know what you’re looking for.”
“You can do trial and error, but my feeling is that artificial intelligence (AI) is going to fill that gap by assigning a computer to look at the patterns,” McDonald continued.
Since only seven percent of the thousands of metabolites circulating the human blood have been characterized, pinpointing the specific molecular processes underlying an individual’s metabolic profile remains a challenge, thereby limiting a path for therapeutic development.
However, ML-based predictive models can use the large data set of uncharacterized metabolites that have been accurately identified by mass spectrometry to recognize metabolic patterns to assist in OC diagnostics.
“Historically, you don’t need to understand the cause and effect relationships to make predictions. For most of medical history, predictions were made based on correlations. We don’t need to know why these metabolites are changing,” said McDonald.
While McDonald acknowledges that a ML approach using multi-omic data would be ideal for learning patterns underlying disease, scalability and complexity are currently limiting factors.
The team used metabolic profiles as an alternative because they represent a biological “end point” that accounts for the combinatorial effects of molecular changes, including but not limited to, protein level, epigenetic control, diet and lifestyle, and more.
Based on the accuracy of their ML approach, the research team developed what they believe to be a clinically useful approach to OC diagnosis, where a patient’s individual metabolic profile is used to determine a probability of developing OC. For example, a patient whose metabolic profile scores within a low likelihood cancer range would be recommended for yearly monitoring. In contrast, a patient whose metabolic profile scores within a range where over 90% of patients have previously been diagnosed with OC would be recommended for immediate screening and treatment.
McDonald described that this probabilistic approach to diagnostics is more clinically informative than binary (yes/no) tests.
In terms of entering the clinic, McDonald said the diagnostic test has entered trials with various clinics in Georgia to prospectively evaluate the validity and utility of the test. In addition, a start-up company, named MyOncoDx, is being formed with the intent to market the technology after completion of requisite trials and FDA approval.
McDonald estimates that “it could be a year or so” before the test will be generally available.