Prefusion-stabilized F glycoprotein RSV vaccine reduced incidence of lower respiratory tract illness in infants when given to their mothers during pregnancy, and in older adults.
Respiratory syncytial virus (RSV) infections cause significant morbidity in infants and elders. In two industry-sponsored studies, efficacy of a bivalent prefusion-stabilized F glycoprotein RSV vaccine was evaluated in pregnant women (to prevent disease in their infants) and in older adults.
In the MATISSE study, investigators randomized 7358 pregnant women (median 31.3 weeks’ gestation) to receive vaccine or placebo, then performed disease surveillance in their infants for 12–24 months to assess prevention of medically attended severe RSV-associated lower respiratory tract illness (LRTI) and medically attended RSV-associated LRTI in infants within 180 days of birth (the primary endpoints). Vaccine efficacy (VE) at preventing medically attended severe RSV-associated LRTI was 81.8% at 90 days and 69.4% at 180 days, while VE at preventing medically attended RSV-associated LRTI did not meet prespecified success criteria (57.1% [90 days] and 51.3% [180 days]). Injection-site reactions were more common in the vaccine group (41% vs. 10%) but most systemic reactions were comparable between groups, as was incidence of premature delivery. Four serious adverse events in the vaccine group and one in the placebo group were deemed related to study product.
In the RENOIR study, investigators randomized 34,284 older adults (median age, 67; congestive heart failure, 1.8%; chronic obstructive pulmonary disease, 6.1%) to receive vaccine or placebo. The two primary endpoints were prevention of RSV-associated LRTI with 2 symptoms or with 3 symptoms. At data cutoff, 11 cases of RSV-associated LRTI with 2 symptoms had occurred in the vaccine group and 33 in the placebo group, for a VE of 66.7%; and 2 cases of RSV-associated LRTI with 3 symptoms occurred in the vaccine group and 14 in the placebo group, for a VE of 85.7%. Local reactions were more likely in the vaccine group than the placebo group (12% vs. 7%), but incidence of systemic reactions was similar between groups. Three serious adverse events related to study product occurred in the vaccine group: 1 case each of Guillain-Barré syndrome, Miller-Fisher syndrome, and delayed allergic reaction.
Comment
Administering an RSV vaccine to pregnant women to protect their infants echoes similar approaches against pertussis, tetanus, and influenza. Regarding study limitations, in MATISSE, women with certain high-risk pregnancies were excluded — and in RENOIR, elders at high risk for RSV-associated complications were not well represented. For both studies, surveillance was conducted during the COVID-19 pandemic with its attendant disruption of typical RSV circulation patterns. These interim safety findings (especially in RENOIR) signal the need for close follow-up and intensive post-marketing surveillance, should the vaccine achieve approval and recommendation in the specified populations. An AS01E-adjuvanted prefusion-stabilized F glycoprotein vaccine. opens in new tab was recently approved by the FDA for the prevention of LRTI in persons aged ≥60 years. Regulatory authorities are now evaluating the safety and efficacy of the present unadjuvanted vaccine.
The FDA approved the world’s first vaccine against chikungunya virus.
The vaccine, Valneva’s Ixchiq, was approved for people aged 18 years or older who are at an increased risk for exposure to chikungunya, which is spread by bites from infected Aedes mosquitoes, similar to dengue and Zika. Clinical studies conducted among adolescents aged 12 to 17 years are ongoing, according to the company.
Chikungunya was first identified in 1952 in Tanzania, and the first urban outbreaks were recorded in Thailand and India in the late 1960s and 1970s, according to WHO.
The virus was not detected in U.S. travelers until 2006 and local cases were not reported until 2014, when there were 12 locally acquired infections in Florida and Texas and more than 4,600 cases in U.S. territories, including Puerto Rico and the U.S. Virgin Islands.
“Infection with chikungunya virus can lead to severe disease and prolonged health problems, particularly for older adults and individuals with underlying medical conditions,” Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said in a press release. “[This] approval addresses an unmet medical need and is an important advancement in the prevention of a potentially debilitating disease with limited treatment options.”
The FDA in August extended the review period for the vaccine by 3 months so that Valneva could finalize the design of a phase 4 post-market safety monitoring study that is required as part of the accelerated approval process.
The single-dose, live-attenuated vaccine was approved based on phase 3 trial data showing a 98.9% seroresponse rate 28 days after vaccination, and a 96.3% seroresponse rate sustained 6 months after vaccination.
“The first-ever licensed chikungunya vaccine will play a crucial role in preventing the suffering caused by this debilitating disease,” Richard Hatchett, MD, CEO of the Coalition for Epidemic Preparedness Innovations, said in a press release. “Climate change is intensifying the threat posed by chikungunya, which means safe and effective vaccines are needed now more than ever before.”
Valneva said it anticipates the CDC’s Advisory Committee on Immunization Practices will vote on recommending the vaccine in February 2024, and the company plans to start commercializing it in the U.S. in early 2024.
The mosquito-transmitted disease chikungunya has been responsible for several large outbreaks in the last decade, including a massive one in the Western Hemisphere in 2013-2015 and a large outbreak in Paraguay in the last year.
The acute illness can be distinctly painful because of severe arthralgias and, in some patients, acute arthritis. Even more worrisome is the potential for persistent joint pains and chronic arthritis in some patients, which may persist for months to years.
The approval by the FDA of a live-attenuated chikungunya vaccine offers an exciting new option for the prevention and control of chikungunya in endemic areas and for travelers to regions of the world with ongoing outbreaks or endemic transmission of the virus.
Winter is upon us, and with it may come runny noses, coughing, and congestion. But how do you know if you have just a common cold or one of the three respiratory viruses that make up the “tripledemic” – RSV (respiratory syncytial virus), COVID-19, and influenza?
Based on symptoms alone, it’s difficult to tell which illness you might have. But there are clues that can point you in the right direction: how severe your symptoms are, how long it took for symptoms to set in, what viruses are circulating in your community, and more.
We asked experts to break it down for us.
How Viruses Set Themselves Apart – or Don’t
Nowadays, COVID – especially for people who have received the most recent vaccine – can manifest much like a common cold, so it’s important to keep at-home tests on hand.
“Being vaccinated does keep [these viruses] from striking the chest,” said Panagis Galiatsatos, MD, a pulmonary and critical care doctor at Johns Hopkins. “Vaccinated patients may get a mild cough, but a lot of their symptoms stay more as an upper respiratory issue, like nasal congestion – like a bad cold.” Slideshow
One of the unique symptoms of COVID, particularly in the earlier variations of the virus, was the loss of taste and smell. While this still happens in some cases, this symptom isn’t as common anymore, said Galiatsatos. More often than not, patients who have been vaccinated will report loss of smell or taste due to upper respiratory congestion, whereas in the past “it was more of a neurological invasion of the virus,” he said.
That’s changed because so many of us now have the antibodies that protect us from the more severe consequences of COVID, from either having recovered from a previous infection, getting immunized, or a combination of the two.
Unlike RSV, cold, and flu, COVID may also bring on some gastrointestinal symptoms like nausea, vomiting, and diarrhea. While GI issues are a more uncommon symptom, it can be a sign that you should get tested for COVID.
RSV in healthy people who are not children or over the age of 65 might look like a cold or a mild case of COVID. But for children and seniors, a telltale sign of a potential RSV infection is when a patient is wheezing or they are having asthma flares, said Peter Chin-Hong, MD, an infectious disease expert at the University of California, San Francisco.
What the Timing of Symptoms Can Tell Us
Common cold symptoms tend to come on fairly quickly, explained Chin-Hong. If you get RSV, on the other hand, it may take 4 to 6 days before symptoms show. Flu viruses are a totally different story.
“The special characteristic of flus is the abrupt onset of symptoms,” Chin-Hong said. “You might be minding your own business, feeling OK, and then all of the sudden you get in your car and you feel like you’ve been hit by a dump truck.”
COVID also has some unique symptomatic features. You may not have symptoms at all, or you might have mild, cold-like symptoms for a week before the symptoms worsen and the infection becomes more serious.
“COVID has this biphasic pattern, whereas colds and RSV don’t – it’s when you are kind of doing OK, and then you fall off a cliff,” said Chin-Hong. “That’s why early treatment with Paxlovid or remdesivir is so important because it can prevent that second phase from happening.”
For Galiatsatos, getting tested for COVID should be your first instinct – and getting two negative tests within a 24-hour period should encourage you to seek out a flu test at a local health care facility if you’re able to. Staying on top of testing can get you access to the right antivirals, like Tamiflu, which can shorten symptoms by a day or more. And when you come down with the flu, those couple of days can make a world of difference.
Just assuming you have COVID and not testing could be a mistake, especially if you end up having long-lasting respiratory symptoms of the virus.
“One of the things that broke my heart was so many patients who have come into my clinic with symptoms of long COVID, but they never got tested. I can’t test their antibodies anymore because those antibodies could be from an older infection or vaccine,” said Galiatsatos. “It’s hard to get insurance companies to pay for long COVID tests if there wasn’t a positive COVID test to begin with.”
Moderna announced this week that its respiratory syncytial virus (RSV) vaccine is 84 percent effective at preventing lower respiratory disease in older adults. Scientific American answered common questions about the virus, its treatments and previously tested vaccines in this story from last November.
As flu season picks up and experts weigh concerns about another possible COVID surge, children’s hospitals are already filling with patients with another viral threat: respiratory syncytial virus, or RSV. Even though many people haven’t heard of RSV, pretty much everyone has had it, probably multiple times, says Anthony Flores, chief of pediatric infectious diseases at the University of Texas Health Science Center at Houston and a physician at Children’s Memorial Hermann Hospital. RSV is the leading cause of bronchiolitis—inflammation of the lung’s small airways—in infants, and the virus is so common that nearly all children have encountered it by their second birthday.
“It’s that ubiquitous,” Flores says. “Even adults are exposed to it repeatedly over time, so we develop some immunity to it.” In healthy adults and children, though, RSV typically presents as a common cold, with symptoms similar to those caused by other “common cold” viruses, such as rhinovirus, adenovirus and a couple of common coronaviruses. But that doesn’t mean it’s harmless. RSV costs the U.S. more than $1 billion each year in health care costs and lost productivity, and it can be particularly dangerous for newborn babies and adults older than age 65.
“As we have come to learn, particularly gradually over the last 15 years, this is a virus that annually produces probably about as much illness in adults as does influenza,” says William Schaffner, a professor of medicine at Vanderbilt University Medical Center and medical director of the National Foundation for Infectious Diseases. That’s because our immune system ages along with us. “As we get older, our immune system doesn’t work as well,” Flores says.
The good news is that RSV vaccines are on the way. In fact, Pfizer just announced this week that its maternal RSV vaccine—given during pregnancy so that antibodies are transferred through the placenta to the fetus—was 82 percent effective at preventing severe RSV in babies through three months old. But until the U.S. Food and Drug Administration approves a vaccine, RSV will be one of the unavoidable viruses people encounter each year.
What is RSV, and what are its symptoms?
RSV is an RNA virus made up of 11 proteins, similar to influenza A, another RNA virus whose genes encode the same number of proteins. It infects the nose, throat, lungs and the breathing passages of the upper and lower respiratory system, according to the National Foundation for Infectious Diseases. As the body sends immune cells to virus-infected cells to fight the disease, it causes inflammation in the airways.
Symptoms include a runny nose, reduced appetite, coughing, sneezing, wheezing and sometimes a mild fever—although fever is more common in young infants and older adults. Symptoms show up about four to six days after infection and take one to two weeks to resolve.
How is RSV transmitted?
RSV spreads primarily through respiratory droplets from coughing, sneezing and kissing (transmission by airborne droplets, or aerosols, has not yet been shown). But the virus can also survive for several hours on hard surfaces, including tables and crib rails. Such “fomites” are a more common mode of transmission for RSV than they are for COVID. People infected with RSV are typically contagious for about three to eight days, even if they don’t have many symptoms.
The basic reproduction number, or R0, for RSV is estimated to be around 3, which means a single infection of RSV will lead, on average, to three other infections.
How severe is an RSV infection?
For the average person, RSV is little more than a nuisance, Flores says. “For most of us—children over the age of two and healthy adults—it’s just like a common cold,” Flores says. “It may give us a little bit of a cough and runny nose, maybe a mild fever, but we usually get over it pretty quickly.”
But infants under six months old, and especially those under two months old, have a harder time with RSV. “That’s where we see our highest hospitalization rates [in children]—maybe three or four times higher in that age group than in others,” Flores says. The reason is basic physics. “It has everything to do with the size of their airways,” he says. Their airways simply aren’t wide enough yet to allow airflow with all the inflammation caused by the immune system’s response to the virus.
Even then, only about 1 to 2 percent of children under six months with RSV need hospitalization (usually for a couple of days), and death is rare. An estimated 58,000 U.S. children are hospitalized with RSV each year, and the virus kills about 100 to 500 U.S. children under five each year. (Since the pandemic began, COVID has killed more than 560 children under five, according to the U.S. Centers for Disease Control and Prevention.) Premature babies and those with underlying heart and lung conditions have the greatest likelihood of complications and hospitalization. Premature infants’ lungs tend to be underdeveloped and even less capable of handling the inflammation caused by the virus. In fact, children who meet strict criteria for being at highest risk are recommended to receive the preventive antibody medication palivizumab as an injection into the thigh muscle once a month when RSV is circulating.
Adults older than age 65 are also at risk of severe RSV, although public health officials have only begun to recognize the threat to older adults in the past decade. Every year an estimated 177,000 older adults are hospitalized with RSV, and about 14,000 die from it. For comparison, influenza kills anywhere from 21,000 to more than 44,000 adults older than 65 each year.
Another population at higher risk for complications from RSV are people who are immunocompromised, whether because they have an underlying condition that weakens their immune system or because they take a medication that suppresses it. Those who have had organ transplants, for example, take medications that dampen their body’s immune response to avoid rejection of the new organ. And many of the drugs used to treat autoimmune conditions also weaken the immune system.
Why are cases surging now?
Historically, RSV season was so reliable that children’s hospitals planned staffing around it. It typically ran from about November through April, with the biggest peaks in January and February, depending on local conditions. But the pandemic changed everything. With many people staying home, social distancing, washing hands and wearing masks for most of 2020 and into 2021, RSV—like influenza—never really arrived, and its seasonality has been out of whack ever since.
“All of a sudden, last summer, we had this huge surge of RSV,” Flores says. “At it first baffled everybody, but then it kind of epidemiologically made sense.” Normally, most kids encounter RSV some time in their first year and a half of life and develop some immunity as they recover. The immunity doesn’t last very long, but enough of it lingers that subsequent infections aren’t as severe. But thanks to the social distancing and masking, a whole birth cohort of kids had never been exposed to RSV before. So as society began opening back up in the summer of 2021, all of them were exposed at once, and RSV roared back like it was Christmas in July.
“We tended to see more severe reactions, so we saw more hospitalizations, and I think it’s because we had a larger pool of kids who had never been exposed to RSV in the past,” Flores says. That summer surge eventually settled down, but fast-forward to 2022, and although it’s later in the year, something similar is happening.
On one hand, current pediatric hospitalizations aren’t much higher at Flores’s hospital and many other hospitals than they would be during a typical RSV peak in midwinter. But the problem is that it’s not midwinter yet. With flu cases rising, pediatricians and public health experts are asking themselves the same question: “Are we going to see another surge with COVID later this year and then see a ‘tripledemic’?” Flores says. “That’s the big worry.” Flores doesn’t think a triple surge would necessarily cause more deaths, but it would place a significant burden on the health care system that many places aren’t prepared to weather.
Is there a vaccine for RSV?
There is no approved RSV vaccine yet, but there likely will be soon. Scientists have been working on such a vaccine for half a century, but a disastrous trial in the 1960s resulted in the deaths of two toddlers who caught RSV after receiving the vaccine. It turned out the disease was more severe in those who were vaccinated, and until that mystery was resolved, not much progress occurred. Fortunately, one of the same scientists whose team determined the spike-protein mRNA code for the COVID vaccines, Jason McLellan of the University of Texas, solved the RSV vaccine problem with virologist Barney Graham, then at the National Institutes of Health, about decade ago. Now that work is coming to fruition.
Several pharmaceutical companies began vaccine trials with McLellan’s protein in 2017, and the first successful phase III (late-stage) results came this year. Against severe disease, Pfizer’s vaccine was 86 percent effective and GSK’s was more than 94 percent effective in adults 60 and older.* Between those vaccines and Pfizer’s recent maternal RSV vaccine news, Graham, who is now retired from the NIH, expects to see at least one RSV vaccine approved by the end of 2023, if not sooner.
How is RSV treated?
There is no medication to treat RSV, so the treatment is primarily supportive care for symptoms such as fever and congestion. Those who have trouble breathing may receive a breathing tube or supplemental oxygen through a mask or nose tube. The American Academy of Pediatrics used to recommend steroids for infants, but the data are conflicting on how well they help, so that’s no longer a standard recommendation, Flores says.
There are a couple of reasons therapeutics don’t exist for RSV. First, it’s very difficult to develop effective drugs for respiratory virus infections. Most of the four antivirals available for flu, for example, are fairly new and have limited effectiveness unless given early after infection. Second, so few children die from RSV that therapeutics weren’t as high a priority as developing drugs for other conditions. The recent understanding of how many adults die from RSV and advances in monoclonal antibodies, however, have boosted the pipeline for new RSV treatments.
What should someone do if they think they or a family member has RSV?
Chances are, you won’t know if you have RSV because it will feel like any other cold. You should do “all those things we’ve learned in the pandemic” when you’re sick, Flores says. That means wearing a mask, practicing good hand hygiene, covering your mouth when you sneeze or cough and, for those able to do so, working from home. Many people won’t or can’t stay home from school or work with just a cold, though, so wearing a mask can at least protect others around you while you’re sick, especially those at higher risk for complications. If there’s anything we learned from the way flu and RSV basically disappeared in 2020, Flores says, it’s that masking obviously works.
When should someone with RSV go to the hospital?
As with any other respiratory illness, the biggest sign that one should seek medical attention, regardless of age, is having difficulty breathing, Flores says. In addition, parents should take an infant under six months to the doctor or hospital if the child can’t lie down without breathing difficulty, if they’re sleepier than usual or if they’re difficult to rouse from sleep.
What can one do to protect vulnerable people from RSV?
Infants and young children who were born premature or who have weakened immune systems, chronic lung disease, congenital heart disease or a neuromuscular disorder may qualify to receive the drug palivizumab. Palivizumab is very expensive and in limited supply, so it’s reserved for those at highest risk, who will receive the most benefit from it. When the RSV season was more predictable, at-risk infants would begin receiving palivizumab in late fall, but when RSV’s seasonality shifted in 2021, state public health authorities convened to ensure the drug would become available when cases began rising.
For others at risk, including infants without underlying conditions, older adults and immunocompromised individuals, the same protections they take against COVID are also effective against RSV, as the low rates of RSV in 2020 showed. “When we see these surges like this, [vulnerable people are] absolutely instructed to be more careful,” Flores says. That means not having sick family members visit, washing hands regularly and wearing a mask outside the home to prevent not only COVID but also exposure to all the other seasonal respiratory viruses, including flu and RSV. And of course, Flores says, everyone eligible for a flu vaccine and COVID vaccine should ensure they’re vaccinated and boosted to reduce the risk of developing multiple infections at the same time.
As the days get shorter and the weather colder in the northern hemisphere, health officials have warned of a perfect storm of infectious respiratory diseases over the winter months.
Outbreaks of seasonal diseases like influenza and respiratory syncytial virus (RSV) are already putting pressure on the overburdened NHS. If surges of these illnesses collide with another large COVID wave, we could be facing a public health disaster. Some have called this threat a “tripledemic”.
But how can we realistically expect the winter to play out? To try to answer this question, we can look at the recent and current trends of some of the most common winter infections in the UK.
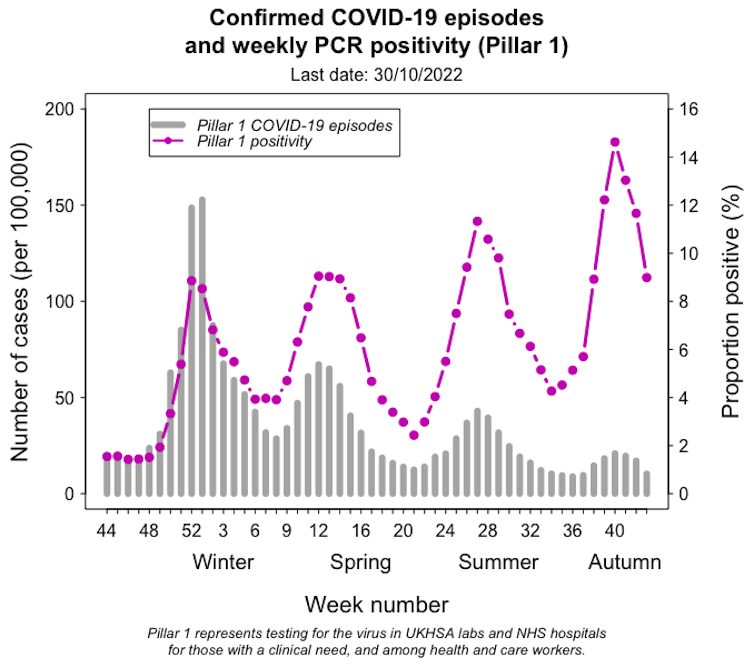
1. COVID-19
Let’s start with the most obvious one, SARS-CoV-2 (the virus that causes COVID-19). The UK has so far been through multiple COVID waves, fuelled by a combination of behavioural changes, emerging variants and waning immunity.
The trajectory of COVID cases in England over the past year.
In contrast to the large epidemic last winter, more recent waves have been relatively small. And despite initial concerns about a significant winter surge this year, the number of COVID cases is currently decreasing. But the pandemic isn’t over yet, and what will happen next is highly uncertain.
So far, there’s mixed evidence as to whether COVID is worse in cold weather. But during winter, people tend to stay indoors more and reduce ventilation, giving viruses more opportunity to spread.
In an optimistic scenario, small-scale outbreaks might continue into the winter as COVID becomes “endemic”.
Previous COVID waves have largely been driven by single dominant variants – alpha and delta in 2020-21 and omicron in 2021-22. This time, the many “descendants” of omicron are multiplying worldwide, and the current spread is instead caused by a mixture of variants peaking in different countries at different times.
But it is possible that if a highly transmissible variant emerges this winter, it might cause another large wave of infections.
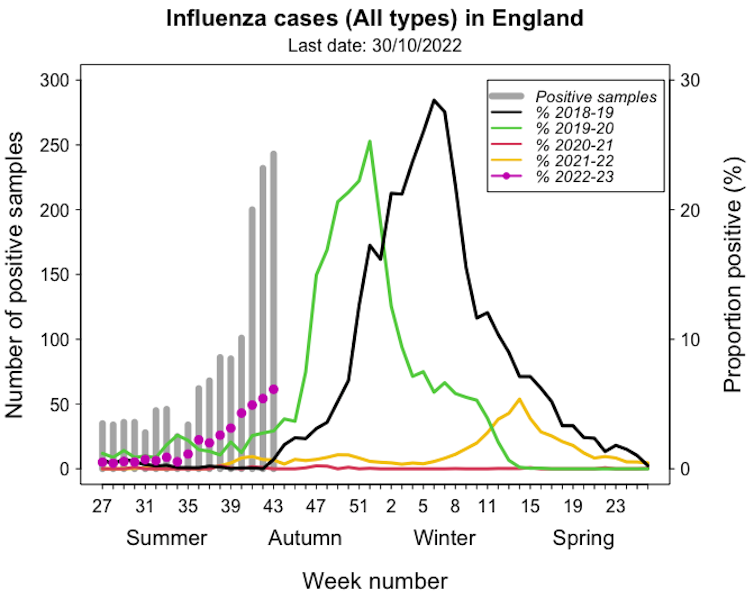
2. Influenza
Seasonal influenza is a respiratory infection caused by four types of viruses, two of which (A and B) are common and can cause severe illness, hospitalisation and death, particularly in vulnerable people.
Not unlike COVID, factors including waning immunity and the evolution of influenza viruses also drive repeated outbreaks.
Influenza infections in England over recent years, compared with the current season.
Flu seasons usually start in November, with cases peaking from December to March. In some years, the outbreaks are particularly severe, as in the UK in 2018.
Flu responded the same way COVID did to non-pharmaceutical interventions, including lockdown restrictions and mask-wearing. The number of cases in the 2020-21 winter was very low. It came back the following season later in the year, but was still limited.
There is concern that the long period during which our bodies were not exposed to the flu might have created an “immunity gap” making us particularly vulnerable this year.
Australia saw the worst seasonal flu outbreak in five years during its recent winter, coinciding with a large COVID surge. While it’s still early to see what the 2022-23 winter will bring in the northern hemisphere, the current outbreak in England is early and large compared with pre-pandemic years.
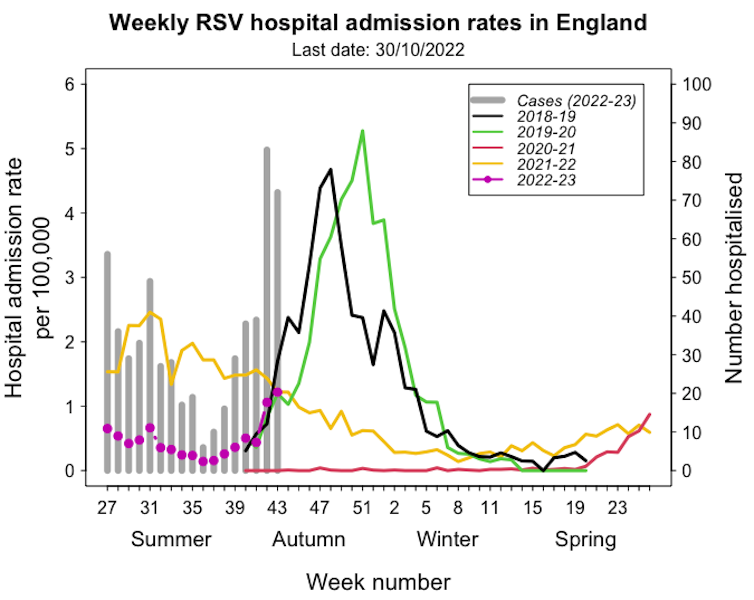
Weekly hospital admissions for RSV in England over recent years, compared with the current season.
In pre-pandemic years it followed a seasonal pattern, with most cases occurring in early winter. After a hiatus in 2020-21, many cases were registered out of season in the summer of 2021. This unusual pattern is again suspected to result from a loss of immunity.
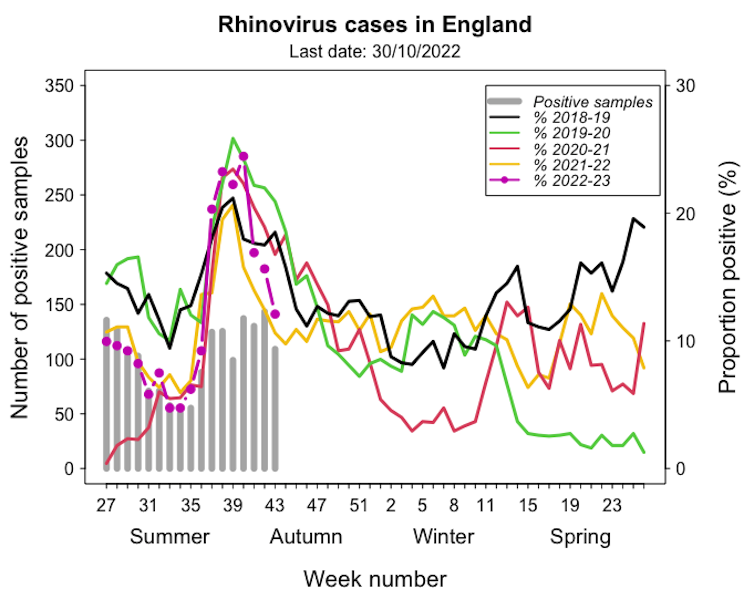
Like flu, the onset of the more benign coronaviruses generally occurs in November, with the peak between January and March. Rhinoviruses and enteroviruses tend to peak in autumn rather than in winter.
Rhinovirus infections in England over recent years, compared with the current season.
The 2021-22 rhinovirus season was similar to pre-pandemic trends, but we’re seeing higher numbers so far this year. The infection is usually mild, and most people quickly recover, but severe cases in vulnerable people can add to the pressure on hospitals.
Protecting ourselves
This winter, the UK will probably face high pressure from respiratory viruses. Cases of seasonal diseases are possibly higher due to the lack of exposure during the lockdowns. In addition, some research suggests COVID infections might affect people’s immunity, putting them at higher risk of infection with other viruses.
To reduce the spread of respiratory viruses, we can continue with measures like ventilation, mask-wearing and hand-washing.
And although we don’t have vaccines available for RSV or common cold viruses, COVID and flu vaccines are an important tool to prevent severe illness this winter.