Immune checkpoint inhibitors did not produce increased pregnancy, fetal and neonatal adverse events compared with other anticancer drugs.
Anti-PD1, anti-CTLA4 combo resulted in overreporting of preterm birth.
Use of immune checkpoint inhibitors for pregnant women with cancer may be safer than previously thought, according to study results published in JAMA Network Open.
Patients treated with immune checkpoint inhibitors (ICIs) did not experience significantly more pregnancy-related, fetal or neonatal adverse events compared with those who received other anticancer therapies.
Data derived from Gougis P, et al. JAMA Netw Open. 2024;doi:10.1001/jamanetworkopen.2024.5625.
“It is the beginning of a journey to search for the best information available to help navigate difficult decisions ahead, especially when recommendations regarding life-saving cancer treatment can appear to be at odds with the needs of the pregnancy and growing fetus,” Alisa Kachikis, MD, MSc, assistant professor at University of Washington, and Linda O. Eckert, MD, adjunct professor at University of Washington, wrote in an accompanying editorial about the findings.
They said the study “offers some hope in an area where data are otherwise sparse.”
Background and methodology
Only 0.1% of pregnancies occur during active cancer treatments, with breast cancer, cervical cancer, Hodgkin disease, malignant melanoma and leukemia being the most common types, according to background information provided by Paul Gougis, MD, department of medical oncology at Pitié Salpêtrière Hospital, Paris, and colleagues.
However, managing these cancers can be difficult as clinicians must balance the health of the patient and the fetus.
ICIs have proven effective in cancer care and researchers expect them to be used more often in this population in the future.
“Currently, the use of ICIs during pregnancy is discouraged due to the absence of safety data obtained in the pregnancy setting,” Gougis and colleagues wrote. “Given the major benefits associated with ICIs, data from large-scale studies exploring the toxic effects of these agents during pregnancy are crucial.”
Researchers acquired study data from VigiBase, WHO’s pharmacovigilance database that has accumulated more than 30 million case reports from 130 countries since 1967.
They evaluated 45 different adverse events in reports of women with a pregnancy-related reaction and interaction with at least one anticancer drug.
The final analysis included 3,558 reports (48.1% from the U.S.; mean age, 28.7 years; 2.6% had ICIs exposure).
Reporting odds ratio (ROR) of women having any pregnancy-related, fetal and neonatal adverse outcomes while receiving ICIs compared with other anticancer drugs served as the study’s primary endpoint.
Results and next steps
The ICI group had a 41.8% report rate of pregnancy, fetal and neonatal adverse events compared with 57.1% in the other anticancer drug cohort (ROR = 0.54; 95% CI, 0.35-0.82).
No significant overreporting of adverse events occurred in the ICI group for any of the 45 outcomes evaluated.
In the evaluation of ICI treatments, overreporting of preterm birth did occur when women received a combination of anti-PD1 and anti-CTLA4 compared with other anticancer medications (80% vs. 23%; ROR = 13.87; 95% CI, 3.90-49.28).
However, anti-PD-L1 and anti-CTLA4 did not produce overreporting of preterm birth when used individually.
Researchers noted 3.3% of ICI reports had suspected immune-related complications.
“One mother developed a combination of antiphospholipid syndrome, pneumonitis and thyroiditis associated with spontaneous abortion,” they wrote. “One report mentioned fetal pneumonitis, possibly immune-related and leading to neonatal respiratory distress syndrome. One newborn experienced intrauterine growth restriction, preterm birth and transient congenital hypothyroidism.”
Study limitations included lack of various data points, including timing of exposure to medications and tumor characteristics.
“The risk-benefit evaluation for both the mother and the fetus or newborn should be discussed case by case considering the oncologic urgency,” researchers wrote.
Kachikis and Eckert stressed the need for more research.
“While this study is a step forward, more studies on cancer treatment in pregnancy and funding for reproductive health research are needed to mitigate the fraught nature of these difficult decisions,” they wrote.
Chronic kidney disease (CKD) is associated with an increased risk of adverse pregnancy outcomes, but the risk at different stages of CKD (defined by estimated glomerular filtration rate, eGFR) compared with women without CKD has not been quantified in large cohorts.
Objectives
To quantify the association between CKD and adverse pregnancy outcomes according to CKD definition, CKD stage and presence or absence of diabetes.
Search strategy
A systematic search of EMBASE and MEDLINE from inception to 5 January 2023.
Selection criteria
English-language randomised controlled trials as well as cohort and case–control studies investigating adverse pregnancy outcomes in pregnant women with CKD.
Data collection and analysis
Two reviewers conducted independent data extractions. A random-effects model was used to estimate risk.
Main results
We included 19 studies with 3 251 902 women. Defining CKD using eGFR or serum creatinine produced results with greater effect size but wider confidence intervals. Compared with CKD stages 1–2, women with CKD stages 3–5 have a greater risk, but also greater imprecision in the risk estimate, of the following outcomes: pre-eclampsia (OR 55.18, 95% CI 2.63–1157.68, vs OR 24.74, 95% CI 1.75–348.70), preterm birth (OR 20.24, 95% CI 2.85–143.75, vs OR 8.18, 95% CI 1.54–43.46) and neonatal intensive care unit admission (OR 19.32, 95% CI 3.07–121.68, vs OR 9.77, 95% CI 2.49–38.39). Women with diabetic kidney disease, compared with women without diabetic kidney disease, have higher risks of maternal mortality, small-for-gestational-age neonates, pre-eclampsia and gestational hypertension.
Conclusions
There is heterogeneity in the definition of CKD in pregnancy. Future studies should consider ways to standardise its definition and measurement in pregnancy.
1 INTRODUCTION
Chronic kidney disease (CKD) is a major public health problem, with associated morbidity, mortality and reduced quality of life.1 Globally, the age-standardised prevalence of CKD for women is between 9.6% and 12.5%.2 Approximately 3%–6% of women of childbearing age are affected by CKD, with 3% of all pregnancies occurring in women with CKD.3 A leading cause of CKD is diabetes mellitus. Diabetic kidney disease affects 2%–8% of pregnancies complicated by pre-existing diabetes,4 whereas diabetes mellitus is present in 1 in 250 pregnancies.5
The stages of CKD are based upon estimated glomerular filtration rate (eGFR), and the grades are based upon proteinuria. Stage-1 and -2 CKD is defined by an eGFR of >60 mL/min/1.73 m2 with markers of kidney damage (e.g. proteinuria).6 Stages 3–5 have an eGFR of <60 mL/min/1.73 m2 or a urinary albumin-to-creatinine ratio of >30 mg/g.7 Other methods of assessing CKD include the assessment of damage to the renal parenchyma identified on histopathological examination and renal function, measured prior to or after pregnancy.8, 9
The assessment of CKD in pregnancy is complicated. The Modification of Diet in Renal Disease (MDRD) study formula and the Chronic Kidney Disease Epidemiology Collaboration (EPI-CKD) formula used to calculate eGFR are not reliable in pregnancy, as the normal range of serum creatinine during pregnancy differs to that outside of pregnancy.10–12 Therefore, these formulae are not recommended to assess renal function in pregnancy. Furthermore, as many women affected by CKD are not diagnosed before pregnancy, most women will not have had a pre-pregnancy renal function assessment. This lack of assessment coupled with hyperfiltration in pregnancy, which when present interferes with the standard definitions, limits the available information on baseline renal function. Moreover, there is substantial variation in the definition of CKD and its assessment prior to and during pregnancy.
Although the terms diabetic nephropathy and diabetic kidney disease are often used interchangeably, diabetic nephropathy is the classic term used for disease caused by hyperglycaemia affecting the glomerulus, whereas diabetic kidney disease can be considered a broader term that includes disease outside the glomerulus.13 Much of the older literature used the terminology of diabetic nephrology; however, the terminology of diabetic kidney disease is now thought to better reflect the complexity and heterogeneity of renal disease in diabetic patients.14
Previous meta-analyses have acknowledged heterogeneity in the definition of CKD between studies but have opted to combine all studies because of the paucity of data.15–17 The meta-analyses performed by Zhang et al. and Al Khalaf et al. did not quantify the association between CKD and adverse pregnancy outcomes according to the definition of CKD, though they had quantified the association according to the presence or absence of diabetes.15,17 Zhang et al. also assessed the effect of CKD stages 1, 2 and 3 on the strength of association.15 Piccoli et al. focused on pregnant women with immunoglobulin A (IgA) nephropathy alone.16 Furthermore, these meta-analyses did not differentiate between CKD stages 1–2 and CKD stages 3–5. Owing to these issues, the accurate interpretation of previous systematic reviews in relation to the severity of CKD is limited.7 Women with diabetes have significantly increased risks of adverse outcomes compared with healthy women, and those with diabetic kidney disease have some of the most complicated pregnancies. However, comparison according to CKD with and without diabetes has not previously been performed. The objective of this systematic review and meta-analysis is to quantify the risk of adverse pregnancy outcomes in women with CKD compared with women without CKD, specifically addressing the varying definitions and stages of CKD, and the presence or absence of diabetic kidney disease.
DISCUSSION
4.1 Main findings
Our systematic review and meta-analysis of 19 studies included over 3.2 million women and 26 671 women with CKD. To our knowledge, our study is the first to assess the impact of variation in the definition of CKD used among studies on the derived risk estimate in the meta-analysis. We found studies that defined CKD using eGFR or serum creatinine produced results with greater effect sizes but wider confidence intervals, compared with studies that defined CKD with ICD codes, biopsies, serum creatinine or eGFR and proteinuria. In our subgroup analyses, we show that women with diabetic kidney disease have higher risks of adverse pregnancy outcomes, including a 35-fold increase in the risk of maternal mortality, in comparison with women with CKD. We also confirm that women with CKD stages 3–5 have an increased risk of preterm birth, pre-eclampsia and NICU admission, compared with women with CKD stages 1–2. Our subgroup analysis on the setting and timing showed that studies conducted in single centres before the year 2000 had higher risks of adverse pregnancy outcomes, compared with population-based studies conducted after the year 2000.
4.2 Strengths and limitations
The main strength of our study is our subgroup analysis on CKD definitions, CKD stages and diabetic kidney disease to facilitate a clearer clinical interpretation. Our large sample size resulted from a comprehensive search that included all relevant systematic reviews to date. Our robust methodology included the use of separate reviewers to conduct independent screening, data extraction and quality assessment. We had strict inclusion and exclusion criteria and excluded patients with renal transplantation and systemic lupus erythematosus nephropathy. This is because patients in both populations are often subject to severe immunosuppression which would introduce selection bias to our study.
The potential for confounding by proteinuria, the use of eGFR in pregnancy and dynamic serum creatinine levels in pregnancy could not be completely adjusted for or excluded, which increases the bias in our review. Other potential unmeasured confounding factors could have affected the association of CKD with the measured adverse pregnancy outcomes, such as diabetes control, blood pressure control, concomitant prescription drug usage in pregnancy and family history. Another limitation is our definition of studies on CKD stages 3–5. With the low number of patients with CKD stages 3–5, we classified a study as performed in a population with CKD stages 3–5 if the study population consisted of >30% of patients with CKD stages 3–5. This was an arbitrarily selected threshold, as most of the included studies either did not report the CKD stage of their study population, owing to their method of CKD definition, or predominantly had a study population comprising patients with CKD stages 1–2. Other limitations include potential publication bias because the review was limited to studies reported in English language only and the lack of inclusion of grey literature. We were unable to systematically control for confounding as we could not stratify by adjusted and unadjusted risk ratios because of a lack of adjusted data. Adjusting for potential confounding factors, such as age, ethnicity, body mass index and socio-economic status, would have been helpful to ascertain whether the observed association is affected by confounding. As a proportion of the included studies were retrospective, it is possible that the data collected was limited through incomplete, inaccurate or inconsistent historical data, which could have affected whether the case and control groups were ascribed correctly. To further complicate the situation, the heterogeneity between the study designs can potentially overestimate or underestimate the association between CKD and adverse outcomes through differences in study population.
4.3 Interpretation
In keeping with current literature, our pooled analysis showed that CKD is associated with an increased risk of perinatal mortality, preterm birth, gestational hypertension, pre-eclampsia, SGA neonates, Caesarean delivery and NICU admission. Zhang et al. and Khalaf et al. also investigated the impact of CKD on adverse pregnancy outcomes.15, 17 Both meta-analyses indicated that CKD is associated with an increased risk of preterm birth, Caesarean delivery, pre-eclampsia and SGA neonates. Khalaf et al. reported that the cause of the kidney disease might confer different risks in pregnancy.17
The heterogeneity in CKD definition limits the value of the outcomes measured in previous meta-analyses, as the meta-analysis of data collected using different CKD definitions produces information of limited clinical significance. In this study, we found that the use of eGFR or serum creatinine to define CKD produced results with greater effect sizes but wider confidence intervals, compared with other definition groups, such as using ICD codes to define CKD, across most outcomes. During pregnancy, serum creatinine, eGFR and proteinuria all change dynamically, which limit their clinical value for diagnosing CKD in pregnancy. In this study, we noted that only a few studies had pre-pregnancy measurement and serial measurements throughout various time points in pregnancy. Most of the included studies only had a single measurement in patients previously diagnosed with CKD, which limits the internal validity of these studies. Furthermore, there were no details on how the patients were diagnosed with CKD initially. CKD is often under-recorded as CKD can be difficult to diagnose.43
As eGFR is not validated for use in pregnancy, creatinine clearance in pregnancy has been suggested for assessing renal function; however, it is cumbersome, time-consuming and impractical on a large scale, as it requires 24 h of urine collection. Therefore, some practitioners prefer to use serum creatinine to assess renal function in pregnancy.10 However, we would still face the issues of pregnancy-related changes in creatinine clearance, the classification of severity and the identification of appropriate thresholds. As such, there is a need to identify more accurate methods for assessing renal function during pregnancy. Alternatively, a better understanding of the interpretation of gestational changes in eGFR during pregnancy and its association with pregnancy outcomes could improve the clinical utility of eGFR. This might be useful, as eGFR is widely used, easily available and familiar to clinicians.
Our subgroup analysis demonstrated that pregnancies affected by diabetes and CKD are at a higher risk of FGR or SGA neonates, compared with non-diabetic CKD pregnancies. In contrast, women with diabetes during pregnancy, especially those without optimal glycaemic control, are usually at risk of having large-for-gestational-age babies or macrosomia.44 One possible explanation may be the cardiovascular remodelling associated with poor glycaemic control.45 If maternal glycaemic control was suboptimal and persisted for prolonged periods during pregnancy, placental insufficiency may occur and lead to FGR or SGA neonates.46 Unfortunately, the degrees of adequate glycaemic control were not fully reported in the studies we assessed to confirm the underlying mechanism for this association. Another potential mechanism may be related to the association of CKD with pre-eclampsia, which is known to be associated with FGR caused by placental dysfunction.47
Although we found a 35-fold increase in the pooled risk of maternal mortality in diabetic kidney disease, there was only a small number of women who died. Moreover, there were inherent differences between single-centre cohort studies and the population studies. Interestingly, our study found that pregnant women with CKD and diabetes were not at a higher risk of preterm delivery, Caesarean delivery, perinatal mortality or having newborns that needed NICU admission, compared with pregnant women with CKD alone. This could be associated with increased antenatal surveillance in women with CKD and diabetes.
In our subgroup analysis of CKD stages, we found that women with CKD stages 3–5 had a higher risk of preterm birth, NICU admission and pre-eclampsia, but not of SGA neonates. These findings are in keeping with those reported by Khalaf et al.17 It is worth noting that the estimated effect for CKD stages 3–5 had wider confidence intervals compared with that for CKD stages 1–2. Although CKD stages 1–2 had an increased risk of adverse pregnancy outcomes, this is a population with a relatively normal GFR and there may be confounding from the cause of CKD. For example, diabetes mellitus is independently associated with adverse pregnancy outcomes.44 Further risk of bias arises from the underestimation of renal function using calculated eGFR in pregnancy, which is not currently recommended for clinical use.10
Our subgroup analysis on setting suggest that single-centre cohort studies produced higher risk estimates that are more imprecise. This may be because single-centre cohort studies are smaller in scale compared with population-based studies. For the subgroup analysis on time, studies conducted before the year 2000 generally had higher risks of adverse pregnancy outcomes, except for preterm birth, compared with population-based studies conducted after the year 2000. The effects observed cannot be attributed to a specific intervention or change in practice but may reflect the general improvement in care over time. We speculate that the higher level of preterm birth in the more recent studies may be associated with the trend over time of more women with complex medical comorbidities now conceiving.
5 CONCLUSION
There is heterogeneity in the definition of CKD in pregnancy. In the future, researchers need to consider ways to standardise the definition and measurement of CKD. As there are only limited options for assessing renal function during pregnancy, there is a need to develop new or modify existing methods of assessing renal function. Furthermore, as serum creatinine is not tested in all pregnancies, and ideally should be quantified prior to pregnancy, the diagnosis of CKD in pregnancy remains challenging. As serum creatinine is a relatively inexpensive test and can provide earlier diagnosis and management of CKD in pregnancy, routine serum creatinine measurement in all pregnant women should be considered by policymakers, as it would improve care for CKD in pregnancy and has been shown to be feasible in early pregnancy.48 As all women with CKD should have regular follow-up appointments to monitor for complications in pregnancy, we suggest that women considered at very high risk within the CKD group should have even more strict follow-up with increased antenatal surveillance.
A doctor uses a hand-held Doppler probe on a pregnant woman to measure the heartbeat of the fetus on Dec. 17, 2021, in Jackson,
Babies born to mothers who contracted a COVID-19 infection while pregnant have “unusually high rates” of respiratory distress at birth or shortly after, a Nature Communications study found.
While studies have shown contracting COVID during pregnancy has been associated with adverse outcomes for both mothers and newborn babies, the authors of the study found there is growing concern for longer-term consequences for babies after they are born.
Previous studies found there were risks of maternal hypoxia and multiorgan failure, which may lead to premature delivery, as well as stillbirth and neurodevelopmental issues — but the recent study found that if a mother is exposed to COVID, it may inflame a newborn’s airway and lead to slower breathing rates, pale or blueish skin, flaring nostrils or a retraction of the chest with each breath.
While the study finds the virus creates an increased risk for respiratory issues for babies after birth, the risk of a mother transmitting the COVID-19 virus in utero remains low.
More than 200 women with COVID-19 were enrolled in the study in Los Angeles. None of the babies tested positive for the infection at birth, but about 17 percent were diagnosed with respiratory issues, which is higher than average for newborns.
Infants who were experiencing respiratory distress stayed in the hospital for about 24 days, Dr. Olivia Man, the study’s author, told NBC News, who first reported on the study.
The point of time the mother contracted COVID during the pregnancy did not have an impact on whether the infant experienced respiratory distress.
Vaccination played a part in the study’s results. Unvaccinated mothers had three times the odds of respiratory distress in their babies compared with mothers who had at least one dose of the COVID vaccine.
If a mother contracts the infection, her body will produce more cytokines, which are involved in the body’s immune response and trigger inflammation. Inflammation in the mother may activate inflammation cells in the infant.
Man told NBC News that the doctors believe the COVID infection in the mother will cascade from the mother to the infant, who is “responding to their mother’s own inflammation.” Long-term consequences are not known yet, but Man said it could include asthma.
Not all mothers who contract COVID while pregnant will experience negative outcomes with their babies.
The Centers for Disease Control and Prevention said it is safe for a pregnant mother to receive the COVID vaccine at any point in the pregnancy, and it helps build antibodies that will protect the baby from contracting the virus.
Summary: Pregnant women and new mothers with schizophrenia are three times more likely to visit the emergency room as a result of being victims of interpersonal violence, a new study finds.
Source: CMAJ
Pregnant and postpartum people with schizophrenia have a more than threefold increase in the risk of an emergency department visit for interpersonal violence, compared with those without schizophrenia, according to a new study in CMAJ.
Interpersonal violence can include physical, sexual and psychological abuse by a family member, intimate partner, acquaintance or stranger.
“Though we found a threefold increased risk for individuals with schizophrenia, we also found that the majority of people, both with and without schizophrenia, are screened for interpersonal violence during pregnancy,” says lead author Kelly Leslie, a fourth-year psychiatry resident at the University of Toronto. “This suggests there are many opportunities for health care providers to intervene and prevent harm to these patients and their children.”
About 1 in 5 (20.7%) women with schizophrenia experience physical or sexual violence during their lifetime, about 9 times the risk for those without serious mental illness. However, little is known about their risk during the perinatal period.
Pregnant individuals with schizophrenia were equally likely to be screened for (74.3% v. 73.8%), yet more likely to self-report (10.2% v. 2.4%), interpersonal violence.
Led by researchers from ICES and Women’s College Hospital, the study included more than 1.8 million pregnant people aged 15–49 years, of whom 4470 had been diagnosed with schizophrenia. People with schizophrenia were more likely to live in a lower-income neighbourhood, to have other psychiatric and chronic medical conditions, and to have had an emergency department (ED) visit for interpersonal violence in the 2 years before their pregnancy.
Key findings:
Overall, 3.1% of people with schizophrenia had an ED visit for interpersonal violence during pregnancy and the first year postpartum, versus 0.4% of those without schizophrenia.
Pregnant individuals with schizophrenia were equally likely to be screened for (74.3% v. 73.8%), yet more likely to self-report (10.2% v. 2.4%), interpersonal violence.
Among study participants who were screened and did not disclose interpersonal violence in pregnancy, schizophrenia was associated with a sixfold increase in the risk of experiencing an ED visit for interpersonal violence in both pregnancy and postpartum.
The study suggests “that routine violence screening in antenatal care settings is an important opportunity for intervention to prevent severe physical, psychological and social harm to these patients and their children,” writes Dr. Simone Vigod, head of psychiatry, Women’s College Hospital and a professor at the Temerty Faculty of Medicine, University of Toronto, with coauthors.
Abstract
Risk of interpersonal violence during and after pregnancy among people with schizophrenia: a population-based cohort study
Background: Schizophrenia is associated with increased risk of experiencing interpersonal violence. Little is known about risk specifically around the time of pregnancy.
Methods: This population-based cohort study included all individuals (aged 15–49 yr) listed as female on their health cards who had a singleton birth in Ontario, Canada, between 2004 and 2018. We compared those with and without schizophrenia on their risk of an emergency department (ED) visit for interpersonal violence in pregnancy or within 1 year postpartum. We adjusted relative risks (RRs) for demographics, prepregnancy history of substance use disorder and history of interpersonal violence. In a subcohort analysis, we used linked clinical registry data to evaluate interpersonal violence screening and self-reported interpersonal violence during pregnancy.
Results: We included 1 802 645 pregnant people, 4470 of whom had a diagnosis of schizophrenia. Overall, 137 (3.1%) of those with schizophrenia had a perinatal ED visit for interpersonal violence, compared with 7598 (0.4%) of those without schizophrenia, for an RR of 6.88 (95% confidence interval [CI] 5.66–8.37) and an adjusted RR of 3.44 (95% CI 2.86–4.15). Results were similar when calculated separately for the pregnancy (adjusted RR 3.47, 95% CI 2.68–4.51) period and the first year postpartum (adjusted RR 3.45, 95% CI 2.75–4.33). Pregnant people with schizophrenia were equally likely to be screened for interpersonal violence (74.3% v. 73.8%; adjusted RR 0.99, 95% CI 0.95–1.04), but more likely to self-report it (10.2% v. 2.4%; adjusted RR 3.38, 95% CI 2.61–4.38), compared with those without schizophrenia. Among patients who did not self-report interpersonal violence, schizophrenia was associated with an increased risk for a perinatal ED visit for interpersonal violence (4.0% v. 0.4%; adjusted RR 6.28, 95% CI 3.94–10.00).
Interpretation: Pregnancy and postpartum are periods of higher risk for interpersonal violence among people with schizophrenia compared with those without schizophrenia. Pregnancy is a key period for implementing violence prevention strategies in this population.
Since the rollout of the experimental COVID shots, U.S. health officials have adamantly claimed the shots are safe for pregnant women and their unborn babies
Meanwhile, now-released Pfizer court-ordered, released data — which the Food and Drug Administration wanted to hide for 75 years — reveal the miscarriage rate among women whose pregnancy outcomes were known was 87.5%. The true rate may be higher or lower, as Pfizer did not record or report pregnancy outcomes for 238 of the 274 women known to be pregnant during the trial
A CDC-sponsored study that was widely used to support the claim that the shot is safe during pregnancy misreported the data. The actual miscarriage rate in that paper was 82%
As of August 12, 2022, the U.S. Vaccine Adverse Event Reporting (VAERS) database listed 4,941 miscarriages post-COVID jab. For comparison, the fetal death reports for all other vaccines reported to VAERS in the last 30 years is 2,239
Israeli research found the Pfizer COVID jab impairs male fertility for three months after each dose, dropping sperm concentration by 15.4% and total motile count by 22.1%, compared to baseline
Since the rollout of the experimental COVID shots, U.S. health officials have adamantly claimed the shots are safe for pregnant women, and have been urging all pregnant women to get the jab “to protect themselves and their babies.” To this day, the U.S. Centers for Disease Control and Prevention recommends the COVID shot for:1
“… people who are pregnant, breastfeeding, trying to get pregnant now, or might become pregnant in the future.”
The CDC further recommends:2
“People who are pregnant should stay up to date with their COVID-19 vaccines, including getting a COVID-19 booster when it’s time to get one.”
And claims:3
“Evidence continues to build showing that:
COVID-19 vaccination during pregnancy is safe and effective.
There is currently no evidence that any vaccines, including COVID-19vaccines, cause fertility problems in women or men.”
All the while, they’ve had Pfizer data showing the shots cause shocking rates of miscarriage which, adding insult to injury, have been blatantly miscategorized as a “recovered/resolved” adverse effect.4 Who in their right mind would consider DEATH a resolved side effect unless they had a depopulation agenda in mind all along?
I don’t see how this could be described as anything but a criminal cover-up. The only reason we know any of this is because U.S. District Judge Mark Pittman ordered the U.S. Food and Drug Administration to release Pfizer documents at a rate of 55,000 pages per month. The FDA and Pfizer had asked to release the documents at a pace of 500 pages per month, which meant it would take 75 years to disclose them all.5
Criminal Cover-Up
Dr. Naomi Wolf recently reported that an analysis of Pfizer data revealed 44% of the women in the trial suffered miscarriages.6 That statistic turns out to have been the result of a miscalculation,7 as Pfizer listed the miscarriages in two separate columns, resulting in them being counted twice.
We’ve repeatedly found Pfizer’s data collection and reporting to be all over the place, and seemingly on purpose, to make hazards more difficult to ascertain. Wolf admitted the error and took down the original report. However, while fact checkers are gloating over the perceived victory, there’s plenty of other evidence in the Pfizer material to demonstrate these shots should be banned for all time.
In an August 20, 2022, Substack article, Dr. Pierre Kory addressed other, “absolutely horrifying,” findings on miscarriages found in the Pfizer data dumps:8
“… let’s do a dive on just one page of the many thousands. See below, Section 5.3.6, Page 12 of the document called ‘Cumulative Analysis of Post-Authorization Adverse Event Reports.’
Looking at the first bullet under the header: Pregnancy cases: 274 cases including:
In this paragraph, at first read, it is just a list of adverse events and numbers, detailed in a way that is confusing at best, and obfuscating at worst. I think it is the latter because, if you do some simple arithmetic trying to parse that paragraph, you end up with this:
270 pregnancies were reported in vaccinated women during the first 12 weeks of the vaccine campaign. In 238 of them, ‘no outcome was provided.’ So, they only knew the outcome of 32 pregnancies reported. What happened in those 32 pregnancies they followed up on?
My hands are literally trembling as I write this, but here goes. In these 32 pregnancies, there were:
• 23 spontaneous abortions
• 2 spontaneous abortions with intra-uterine death
◦So, 25 of the 32 pregnancies with known outcomes resulted in a miscarriage, a rate of 78%. Note that miscarriage normally occurs in only 12-15% of pregnancies
• 2 premature births with neonatal death
• 1 spontaneous abortion with neonatal death
• 1 normal outcome
Note that this only adds up to 29 known outcomes, but then they note that ‘two different outcomes were reported for each twin’ and then they talk about ‘fetus/baby cases as separate from mother cases.’ I have no idea how to interpret this explanation of outcomes, so it may have been one or two less (or more) deaths then.
So, of the 32 pregnancies they knew the outcome of, 87.5% resulted in the death of the fetus or neonate. Burying this data in the way and not alerting the world to what they found, is criminal activity …”
To be perfectly clear, the failure to record and report the outcomes of 238 out of 274 pregnancies during a drug trial is simply unheard of. It’s shockingly unethical. And the fact that both the Food and Drug Administration and the CDC accepted this, and claim there’s “no evidence” of harm to pregnant women and their babies is proof positive of reprehensible maleficence.
There’s no fixing what’s gone wrong at the FDA and CDC. Their credibility with the public is ruined beyond any possible recovery. The CDC can review and reorganize itself all it wants, but it changes nothing. They are, to this day, urging pregnant women to take a shot that they KNOW will cause babies to die. Calling it a dystopia of epic proportions is a profoundly serious understatement.
CDC-Sponsored Study Also Tried to Hide Data
Need more evidence? How about the fact that the CDC-sponsored study9 published in The New England Journal of Medicine (NEJM) in April 2021 — which was widely used to support the U.S. recommendation for pregnant women to get injected — also obfuscated data to hide a shockingly elevated miscarriage rate.
According to this paper, the miscarriage rate within the first 20 weeks of pregnancy was 12.5%, which is only slightly above the normal average of 10%. (Looking at statistical data, the risk of miscarriage drops from an overall, average risk rate of 21.3% for the duration of the pregnancy as a whole, to just 5% between Weeks 6 and 7, all the way down to 1% between Weeks 14 and 20.10)
However, there’s a distinct problem with this calculation, as highlighted by Drs. Ira Bernstein, Sanja Jovanovic and Deann McLeod, HBSc, of Toronto. In a May 28, 2021, letter to the editor, they pointed out that:11
“In table 4, the authors report a rate of spontaneous abortions <20 weeks (SA) of 12.5% (104 abortions/827 completed pregnancies). However, this rate should be based on the number of women who were at risk of an SA due to vaccine receipt and should exclude the 700 women who were vaccinated in their third-trimester (104/127 = 82%).”
In other words, when you exclude women who got the shot in their third trimester (since the third trimester is after week 20 and therefore should not be counted when determining miscarriage rate among those injected before week 20), the miscarriage rate is 82%. (The errors in that NEJM article were also reviewed in a Science, Public Health Policy and the Law paper12 published in November 2021.)
Of those 104 miscarriages, 96 of them occurred before 13 weeks of gestation, which strongly suggests that getting a COVID shot during the first trimester is an absolute recipe for disaster. So, here was yet another attempt to hide the fact that more than 8 in 10 pregnancies may be terminated as a result of the jab.
As of August 12, 2022, the U.S. Vaccine Adverse Event Reporting (VAERS) database listed 4,941 miscarriages post-COVID jab.13 For comparison, the fetal death reports for all other vaccines reported to VAERS in the last 30 years is 2,239.14
Birth Rates Are Suddenly Plummeting Worldwide
In addition to miscarriages, we’re also looking at abruptly plummeting birth rates, suggesting the COVID jabs are having an adverse impact on future fertility as well.
“They are large drops, and they are occurring, almost like clockwork, approximately 9 months after pregnant women around the world started to be vaccinated,” Kory notes.15
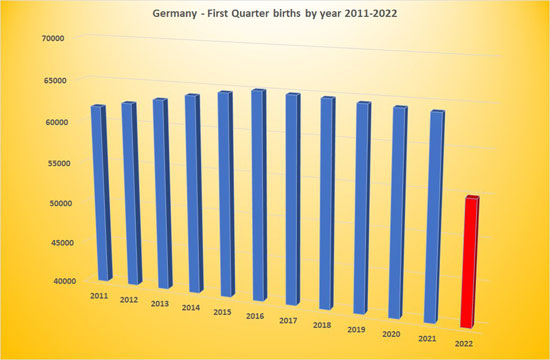
For example, Germany recently released data showing a 10% decline in birth rate during the first quarter of 2022.16
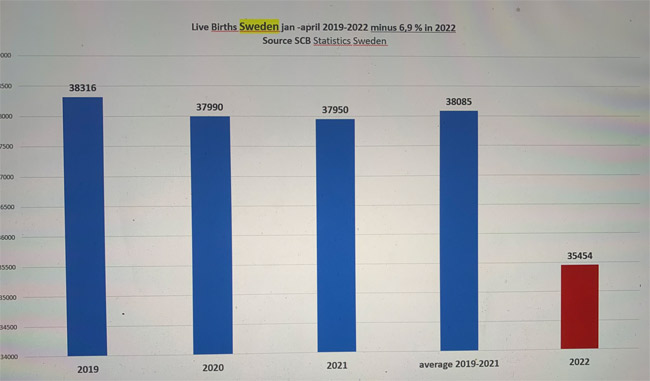
The live birth rate graph for Sweden looks much the same, with a 14% drop:17,18 According to Gunnar Anderson, a Swedish professor in demographics at Stockholm University, “We have never seen anything like this before, that the bottom just falls out in just one quarter.”19
Between January and April 2022, Switzerland’s birth rate was 15% lower than expected, the U.K.’s was down by 10% and Taiwan’s was down 23%.20,21,22 In Hungary, MP Dúró Dóra has expressed concern about a 20% drop in birth rate during January 2022, compared to January 2021.23
The U.S. is also showing signs of a drop in live births. Provisional data from North Dakota show a 10% decline in February 2022, 13% reduction in March and an 11% reduction in April, compared to the corresponding months in 2021.24
In the five countries with the highest COVID jab uptake, fertility has dropped by an average of 15.2%, whereas the five countries with the lowest COVID jab uptake have seen an average reduction of just 4.66%.
In a July 5, 2022, Counter Signal article, Mike Campbell reported that in the five countries with the highest COVID jab uptake, fertility has dropped by an average of 15.2%, whereas the five countries with the lowest COVID jab uptake have seen an average reduction of just 4.66%. Below is a chart from Birth Gauge25 on Twitter comparing live birth data for 2021 and 2022 in a large number of countries.
Many Women Report Menstrual Irregularities Post-Jab
High rates of menstrual irregularities post-jab are also a warning sign that reproductive capacity may be impacted. As of August 12, 2022, there were 31,443 VAERS reports of menstrual disorders.26
Changes include heavier and more painful periods27 and changes in menses length, as well as unexpected breakthrough bleeding or spotting among women on long-acting contraception or those who are postmenopausal and haven’t had a period in years or even decades.28
Health officials have tried to brush off the reports, but a study published in Obstetrics & Gynecology — funded by the National Institute of Child Health and Human Development (NICHD) and the National Institutes of Health’s Office of Research on Women’s Health — confirmed an association between menstrual cycle length and COVID-19 shots.29
According to the authors, it’s possible that the immune response created by the mRNA shots affect the hypothalamic-pituitary-ovarian axis, which plays a well-known role in the timing of a woman’s cycle:30
“Our findings for individuals who received two doses in a single cycle supports this hypothesis. Given the dosing schedule of the mRNA COVID-19 vaccines in the United States (21 days for Pfizer and 28 days for Moderna), an individual receiving two doses in a single cycle would have received the first dose in the early follicular phase.
Cycle length variability results from events leading to the recruitment and maturation of the dominant follicle during the follicular phase …”
Other Disturbing Evidence
A Japanese biodistribution study for Pfizer’s jab also showed the COVID spike protein from the shots accumulate in female ovaries and male testes,31,32 and there’s credible concern that the COVID jabs will cross-react with syncytin (a retroviral envelope protein) and reproductive genes in sperm, ova and placenta in ways that may impair fertility and reproductive outcomes.
A Pfizer-BioNTech rat study33 revealed the injection more than doubled the incidence of preimplantation loss (i.e., the risk of infertility), and led to mouth/jaw malformations, gastroschisis (a birth defect of the abdominal wall) and abnormalities in the right-sided aortic arch and cervical vertebrae.34,35 As noted by The Exposé:
“With this being the case, how on earth have medicine regulators around the world managed to state in their official guidance that ‘Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy’? And how have they managed to state ‘It is unknown whether the Pfizer vaccine has an impact on fertility’?
The truth of the matter is that they actively chose to cover it up. We know this thanks to a Freedom of Information (FOI) request36 made to the Australian Government Department of Health Therapeutic Goods Administration (TGA).”
You can read more about that in The Exposé’s July 19, 2022, article, “FOIA Reveals Pfizer & Medicine Regulators Hid Dangers of COVID Vaccination During Pregnancy After Study Found It Increases Risk of Birth Defects & Infertility.”37
We’re also seeing a sudden uptick in infant mortality. The Exposé38 highlighted data from Scotland, showing neonatal deaths were 119% higher above the annual norm in March 2022.
Male fertility is also under attack by these bioweapons. Israeli research39,40 published in the journal Andrology found the Pfizer COVID jab temporarily but significantly impairs male fertility, dropping sperm concentration by 15.4% and total motile count by 22.1%, compared to baseline pre-jab.
Both eventually recovered, some three months after the last jab, but if you destroy a man’s sperm for three months every time he gets a COVID shot, you’re significantly reducing the probability of him fathering a child for a good part of any given year and the stats reviewed above support this.
Remember, the mRNA shots are recommended at three-month intervals for the original series, and boosters are now being recommended at varying intervals thereafter. In the video above, Amy Kelly, project director for the Daily Clout’s Pfizer document analysis team, reviews this study and other post-jab male fertility concerns.41
End the COVID Shots Now, Before It’s Too Late to Recover
In October 2021, when the FDA was voting on whether to authorize the COVID jab for children aged 5 through 11, Dr. Eric Rubin, an FDA advisory panel member, Harvard professor and editor-in-chief of the NEJM, stated:42
“We’re never going to learn about how safe this vaccine is unless we start giving it. That’s just the way it goes … And I do think we should vote to approve it.”
So, in this and other instances, they’ve openly admitted that anyone who takes the jab is part of an experiment. Yet at the same time, the FDA and CDC have insisted that the jabs are perfectly safe — all while in possession of data showing they’re anything but! In conclusion, I agree with Kory, who writes:43
“… when a new medicine or device is introduced, you must first assume any adverse effects or deaths reported to be related to the intervention until proven otherwise. That is what I am doing here.
We must assume the vaccines are impacting fertility unless some other provable or credible explanations for a sudden drop in month to month birth rates. So stop the shots until you can prove they are not …
Too many young people dying,44 too many becoming disabled, too many pregnancies resulting in fetal or neonatal death as above, and now we find out that if we continue with this vaccine obsession, they will not be replaced. This is a humanitarian catastrophe heaped atop the one caused by dangerous gain-of-function research.
When will the world wake up to this rapidly unfolding horror? For those of us who know what is going on, it is hard not to feel helpless as we are forced to watch increasingly apparent and widespread needless death. But we will continue to try to get these truths out despite the massive censorship and propaganda overwhelming the globe.
We have a moral and ethical obligation and take that responsibility seriously no matter what befalls us. Stop the vaccines, now. And if we can’t stop them, we must try to convince everyone we know to no longer agree to get vaccinated. Their lives and our future depend on it.”
Environmental exposures heightened by climate change adversely affect maternal and newborn health, and women are “particularly vulnerable” to these effects, according to a speaker at The Pregnancy Meeting.
“This last year, the climate crisis overtakes pandemics in terms of the greatest worry for global experts,” Jeanne A. Conry, PhD, MD, president of the International Federation of Gynecology and Obstetrics, said in her presentation.
Organizations such as the World Economic Forum in 2021 and the World Meteorological Organization in 2018 identified their environmental concerns, including failure to take action against climate change and extreme weather conditions causing loss of life and biodiversity, she said.
Conry, who is also on the board of directors for the Heartland Health Alliance and The Forum Institute, said that children and pregnant women are among the communities most impacted by natural disasters brought about by climate change.
“Women and children are 14 times more likely to die than men in a natural disaster,” Conry said. “If we look historically at the 2004 tsunami in Asia, 70% of the deaths were women; if we look at the Bangladesh cyclone in 1991, 90% of the deaths were women.”
Disasters such as these can disrupt women’s access to medical supplies and natural resources such as food, especially in the case of pregnant women.
“Pregnant women may be particularly susceptible to dehydration and being displaced from their homes,” Conry said. In low- and middle-income countries where manual labor is common, they may also be subjected to heat and drought.
Elements of climate change
Climate change is a factor in air pollution — higher temperatures increase the amount of allergens and harmful pollutants in the air — which Leonardo Trasande, MD, MPP, and colleagues found in 2016 was associated with preterm births.
They found “approximately 3% of preterm births nationally — about 15,000 deliveries — could be attributed to air pollution,” Conry said. “The costs then are about $5 billion, of which $760 million is spent on direct medical care.”
Increasing global temperatures also play a role in the burden of climate change on women and children.
“Five international articles reviewed found that heat is associated with preterm birth… and four of these international studies showed that heat is associated with low birth weights,” Conry said.
Flooding caused by rising temperatures — and subsequently higher sea levels and the risk for natural disasters such as typhoons — exposes people to pollution and toxic substances; induces stress, anxiety and food insecurity; and interferes with cultural norms, particularly in low-income countries, she said.
“In Bangladesh, some of the research has shown that women are affected disproportionately — culturally, their inhibitions, inadequate social services and inability to seek hygiene is of serious concern,” Conry said.
Rising temperatures have also dried out vegetation, leading to more intense wildfires around the world.
“I live in the fire area of California… so I see the impact on air quality, I see the disruption in family life,” Conry said. “Hospitals are evacuating women at the last minute and evacuating the entire hospital with moments to save people; nurses are putting laboring patients in the back of their car to get them out of the fire. This is the reality that we’re seeing right here, right now, around the world.”
Role of OB/GYNs
Conry mentioned that obstetricians and gynecologists are in a unique position to raise awareness to educate and advocate for mitigation strategies.
“We need to step up, be leaders and share the message that the environmental exposures are a concern for the health of women,” she told Healio. “We are very well-versed in diseases like diabetes and hypertension and their impact on health, but the moment we discuss environmental effects, physicians draw a blank look and say they do not have the evidence. I try to remind them there will never be a double-blind study to look for cause and effect — we cannot control exposures as we do other variables in research studies.”
Nearly a third of those in a prospective study had clinically relevant depressive symptoms
Despite treatment with antidepressant medication, a significant proportion of women still reported symptoms of anxiety and depression during pregnancy, according to a prospective study.
Among a group of 88 women who took selective serotonin reuptake inhibitors (SSRIs), about a third had clinically relevant symptoms of depression during pregnancy and the postpartum period, reported Gabrielle Mesches, MS, of the Northwestern School of Medicine in Chicago, and colleagues.
Around 40% of pregnant women who took SSRIs also had higher levels of anxiety, with a substantial number experiencing increasing symptoms throughout pregnancy, the team found.
“The assumption is that if women are taking antidepressants in pregnancy, they are well. That’s not always the case,” study co-author Katherine Wisner, MD, also of Northwestern, told MedPage Today.
She explained that depressive symptoms during pregnancy are associated with a number of adverse outcomes, including preterm birth, hypertension, cesarean delivery, low birth weight, neonatal intensive care unit admission, and social and emotional impacts on infants.
If women treated with antidepressants throughout pregnancy are not in remission, they should be offered additional treatment, such as therapy, stress management. or mindfulness interventions, Wisner added. “I really believe that, in addition to medication, some kind of additional treatment should be offered in pregnancy.”
The researchers conducted a prospective, longitudinal cohort study to assess monthly patterns of anxiety and depression during pregnancy. Participants were enrolled at one of three urban academic centers or one rural health center. Pregnant women were included if they had at least one prior episode of major depressive disorder, were not in a current episode, and were treated with sertraline, fluoxetine, citalopram, or escitalopram. Women with bipolar disorder or probable antenatal depression were not included.
Participants completed assessments once a month from study entry (less than 18 weeks’ gestation) through delivery, and again at 6 and 14 weeks postpartum. The study investigators used a series of screening tools, including the 10-item Edinburgh Postnatal Depression Scale and the 7-item Generalized Anxiety Disorder Scale, to assess depression and anxiety symptom severity during pregnancy and postpartum, measuring the changes in these outcomes over time. The team adjusted for covariates including body mass index, race, age, and psychiatric comorbidities.
Women were grouped into “trajectories” — or patterns — of depression and anxiety based on the severity of their symptoms. Depressive symptoms were categorized as minimal, mild, or subthreshold (or clinically relevant), and anxiety symptoms were categorized as asymptomatic, minimal, breakthrough (or increasing), or mild.
Overall, 88 women enrolled in the study and 77 provided complete perinatal and postpartum data. All the study participants identified as female, rather than transgender, non-binary, or other. Women were 34 years old on average, and the mean gestational age was approximately 13 weeks. About 90% of participants were white.
A majority of patients were also diagnosed with at least one psychiatric comorbidity. Nearly 80% had a lifetime anxiety disorder, 10% had a substance abuse disorder within the last year, and 16% had a lifetime eating disorder.
Approximately 18% of women who took SSRIs during pregnancy had minimal depressive symptoms, 50% had mild, and 32% had subthreshold, or clinically relevant, depressive symptoms. Regarding anxiety, 7% of women were asymptomatic, 53% had minimal, 18% had increasing, and 23% had mild symptoms.
Symptoms of depression correlated with anxiety, the researchers found. For example, of all women who had clinically relevant symptoms of depression, nearly 70% scored into the two highest levels of anxiety groups.
Study limitations, Mesches and co-authors said, included that the findings are generalizable only to SSRI-treated women like those in the study — i.e., who are predominantly white, married, and have higher levels of education. Additionally, 11 women in the study were lost to follow-up, which prevents a complete picture of postpartum effects, the team noted.
Pregnant women who report a penicillin allergy can safely undergo penicillin skin testing and incremental drug challenges without adverse effects in their pregnancy, according to a study published in Annals of Allergy, Asthma & Immunology.
The need for delabeling
Beta-lactam antibiotics are first-line treatment for preterm pre-labor rupture of membranes (PROM), chorioamnionitis and prophylaxis for cesarean deliveries among other conditions in pregnancy, according to the researchers. Although approximately 10% of the population report a penicillin allergy, the researchers continued, more than 90% of patients with reported penicillin allergy can safely tolerate it after a complete evaluation.
“There are two reasons for this,” Jumy (Olajumoke) Fadugba, MD, FAAAAI, study author, chief of section of allergy and immunology at Penn Medicine, andassociate professor of clinical medicine and fellowship program director of allergy and immunology at the University of Pennsylvania Perelman School of Medicine, told Healio.
Jumy (Olajumoke) Fadugba
“One is that some people’s original rash/hives may have been due to the illness itself, especially viral illness in children,” she said. “The other reason is that even people who had a true allergic to a penicillin antibiotic in their youth often ‘outgrow’ it. The further out you are from the original reaction, the less likely you are to still be allergic to it.”
People with a penicillin allergy label have significantly worse clinical outcomes than those who don’t have one, Fadugba continued. Additionally, patients who use more broad-spectrum antibiotics have more microbial antibiotic resistance, which is a rising public health problem, and gut infection such as Clostridium difficile, she said.
Allergists should then try and test patients for penicillin allergy, Fadugba said. If the test is negative, allergists should then remove the label so these patients can receive appropriate antibiotics for their condition.
“Pregnant women are a particularly important population to try and delabel because during the course of pregnancy, delivery and right after delivery, there are many reasons why a pregnant woman may need a penicillin or related beta-lactam antibiotic,” Fadugba said.
Approximately one-third of pregnant women eventually need penicillin or a related antibiotic, Fadugba said, adding that penicillin allergy during pregnancy is associated with increased rates of cesarean delivery, post-cesarean wound complications and increased hospital stays.
Even though the American College of Obstetricians and Gynecologists recommends that women with penicillin allergy be evaluated before delivery, penicillin allergy testing during pregnancy was infrequent when this study was initiated, with persistent hesitancy to test or refer pregnant women, Fadugba said.
“There are reports that some doctors are concerned about the safety of testing pregnant women and may worry about an adverse effect on the woman or baby,” she said.
The study’s results
Noting previous studies showing that pregnant women could undergo penicillin testing successfully, the researchers set out to demonstrate that the skin test for penicillin and the oral challenge for amoxicillin do not result in worse outcomes for mother and child.
The single-center, retrospective electronic chart review involved 136 pregnant women (mean age, 32.5 years; standard deviation, 4.2; 78% white) referred to an outpatient allergy and immunology clinic for penicillin allergy evaluation, where they were risk-assessed via a screening questionnaire through the electronic medical record about their allergy history.
According to the study, 112 women said a penicillin antibiotic was the index drug, and four women reported that cephalosporin caused their drug reaction. These reactions occurred more than 5 years before in 91% of the cases and more than 10 years before in 85% of the cases.
These reported reactions included unspecified rash (44%), hives (39%), angioedema or facial swelling (4%), shortness of breath (4%), throat symptoms (1%), prolonged gastrointestinal symptoms (< 1%) and dizziness (< 1%).
Providers at the clinic then performed skin prick and intradermal testing per standard protocol on 133 of the women. Penicillin skin testing (PST) was negative for 129 (97%) of them. Three (2%) of the participants had suboptimal intradermal histamine. Avoidance was recommended for the one patient with a positive PST.
Next, 133 of the participants took a two-step or three-step oral incremental drug challenge (IDC) to amoxicillin or oral penicillin V during the same visit. All participants passed the IDC, and their penicillin label was removed.
The researchers then followed 135 of these women during their pregnancy, with 68 (50%) of them using at least one beta-lactam during delivery. Specifically, 47 (35%) used penicillin and 34 (25%) used cephalosporin. Of the 68 women, 67 (97%) tolerated treatment without reactions.
The patient with a reaction experienced immediate nausea and itching after receiving penicillin V with no documented changes in vital signs or observed rash or angioedema. After successful treatment with diphenhydramine and ondansetron, a penicillin label was added back to her chart.
During the postpartum period, 21 (15%) of the participants who were evaluated for penicillin allergy received antibiotics, and 14 of them (10%) used beta-lactams. There were no adverse drug reactions reported.
Compared with a control group of 1,349 women with a penicillin allergy label who were not evaluated for penicillin allergy, the participants (mean age, 32.5 years; standard deviation, 4.2; 78% white) who were evaluated saw no difference in gestational age at delivery (38.8 weeks in the evaluation group vs. 38.5 weeks in the control group).
Also, there were no differences in neonatal birth weight (3,185 g vs. 3,174 g) or risks for cesarean section (OR = 1.3; 95% CI, 0.88-1.96). The researchers further found no association between evaluation and preterm labor, gestational hypertension, preeclampsia, eclampsia, placental abruption or PROM, nor were there any differences in the risk for having a pregnancy complication between the groups (OR = 1.4; 95% CI, 0.84-2.36).
The researchers concluded that pregnant women could be evaluated for penicillin allergy safely via PST and oral IDC and potentially see their penicillin allergy label removed, enabling them to benefit from the use of these antibiotics without increased risk for adverse pregnancy outcomes.
“We found that penicillin testing in pregnant women was not associated with worse outcomes for the woman and baby,” Fadugba said. “The findings were not surprising, but rather confirmed what we expect.”
Next steps for care, research
When pregnant patients have a penicillin or amoxicillin allergy on their record, providers should discuss the importance of having this label addressed and should refer patients to a specialist — usually an allergist — who can perform testing with the required expertise in a safe environment where the patient can be monitored for a reaction, Fadugba said.
“Allergy specialists will hopefully use this data to support the idea that penicillin testing in low-risk pregnant patients does not result in worse outcomes for mother and child and may therefore perform testing more readily in appropriate patients,” she said.
However, Fadugba also noted that providers first need to take a good history of their patients to ensure they are at very low risk for having a severe hypersensitivity reaction before undergoing testing. She also said that there were disproportionately fewer nonwhite (African American and Hispanic) pregnant women who underwent evaluation during the study.
“An important future endeavor would be to identify potential barriers that patients may face to being evaluated for their allergy and to address these barriers in order to benefit a broader patient population,” she said.
For more information:
Jumy (Olajumoke) Fadugba, MD, FAAAAI, can be reached at olajumoke.fadugba@pennmedicine.upenn.edu.
These results are in further support of the safety of PST in pregnancy. I think it is also helpful to see that disproving penicillin allergy in pregnancy can affect antibiotic choice postpartum as well.
My own experience is that PST in pregnancy is safe and well-tolerated. It also can lead to more appropriate use of antibiotics during pregnancy, peripartum and postpartum.
In our health system, we have set up a rapid referral system to evaluate pregnant women with penicillin allergy during pregnancy. This study and others show that penicillin evaluations in pregnancy should be standard of care.
Because the data on penicillin evaluations in pregnancy shows that it is safe and effective, I would be more worried about leaving a penicillin allergy label without an evaluation as we know the label is associated with many adverse outcomes.
Next, I think it would be interesting to see an analysis of a large dataset to determine if a mother’s penicillin status has an impact on immediate neonatal outcomes.
Allison C. Ramsey, MD
Chair, American Academy of Allergy, Asthma & Immunology Adverse Reactions to Drugs, Biologicals and Latex Committee
Allergy and clinical immunology, Rochester Regional Health
Clinical assistant professor of medicine, University of Rochester School of Medicine and Dentistry
Environmental exposures heightened by climate change adversely affect maternal and newborn health, and women are “particularly vulnerable” to these effects, according to a speaker at The Pregnancy Meeting.
“This last year, the climate crisis overtakes pandemics in terms of the greatest worry for global experts,” Jeanne A. Conry, PhD, MD, president of the International Federation of Gynecology and Obstetrics, said in her presentation.
Organizations such as the World Economic Forum in 2021 and the World Meteorological Organization in 2018 identified their environmental concerns, including failure to take action against climate change and extreme weather conditions causing loss of life and biodiversity, she said.
Conry, who is also on the board of directors for the Heartland Health Alliance and The Forum Institute, said that children and pregnant women are among the communities most impacted by natural disasters brought about by climate change.
“Women and children are 14 times more likely to die than men in a natural disaster,” Conry said. “If we look historically at the 2004 tsunami in Asia, 70% of the deaths were women; if we look at the Bangladesh cyclone in 1991, 90% of the deaths were women.”
Disasters such as these can disrupt women’s access to medical supplies and natural resources such as food, especially in the case of pregnant women.
“Pregnant women may be particularly susceptible to dehydration and being displaced from their homes,” Conry said. In low- and middle-income countries where manual labor is common, they may also be subjected to heat and drought.
Elements of climate change
Climate change is a factor in air pollution — higher temperatures increase the amount of allergens and harmful pollutants in the air — which Leonardo Trasande, MD, MPP, and colleagues found in 2016 was associated with preterm births.
They found “approximately 3% of preterm births nationally — about 15,000 deliveries — could be attributed to air pollution,” Conry said. “The costs then are about $5 billion, of which $760 million is spent on direct medical care.”
Increasing global temperatures also play a role in the burden of climate change on women and children.
“Five international articles reviewed found that heat is associated with preterm birth… and four of these international studies showed that heat is associated with low birth weights,” Conry said.
Flooding caused by rising temperatures — and subsequently higher sea levels and the risk for natural disasters such as typhoons — exposes people to pollution and toxic substances; induces stress, anxiety and food insecurity; and interferes with cultural norms, particularly in low-income countries, she said.
“In Bangladesh, some of the research has shown that women are affected disproportionately — culturally, their inhibitions, inadequate social services and inability to seek hygiene is of serious concern,” Conry said.
Rising temperatures have also dried out vegetation, leading to more intense wildfires around the world.
“I live in the fire area of California… so I see the impact on air quality, I see the disruption in family life,” Conry said. “Hospitals are evacuating women at the last minute and evacuating the entire hospital with moments to save people; nurses are putting laboring patients in the back of their car to get them out of the fire. This is the reality that we’re seeing right here, right now, around the world.”
Role of OB/GYNs
Conry mentioned that obstetricians and gynecologists are in a unique position to raise awareness to educate and advocate for mitigation strategies.
“We need to step up, be leaders and share the message that the environmental exposures are a concern for the health of women,” she told Healio. “We are very well-versed in diseases like diabetes and hypertension and their impact on health, but the moment we discuss environmental effects, physicians draw a blank look and say they do not have the evidence. I try to remind them there will never be a double-blind study to look for cause and effect — we cannot control exposures as we do other variables in research studies.”
In an urgent Health Advisory on Sept. 29, the CDC strongly recommended that women who are pregnant, who were recently pregnant, who are trying to conceive or who may become pregnant in the future get vaccinated against COVID-19.
Healio spoke with Nora Colburn, MD, an infectious disease specialist at The Ohio State University Wexner Medical Center and assistant professor at The Ohio State University College of Medicine, to find out more about the CDC’s recommendation and how physicians treating these women can encourage them to get vaccinated.
Healio: What prompted the CDC to make these recommendations?
Nora Colburn
Colburn: As of Sept. 27, more than 125,000 laboratory-confirmed COVID-19 cases have been reported in pregnant people, including more than 22,000 hospitalized cases and 161 deaths. The highest number of COVID-19-related deaths in pregnant people (n = 22) in a single month of the pandemic was reported in August. Data from the COVID-19-Associated Hospitalization Surveillance Network (COVID-NET) for 2021 indicate that approximately 97% of pregnant people hospitalized (either for illness or for labor and delivery) with confirmed SARS-CoV-2 infection were unvaccinated. As of Sept. 18, only 31% of pregnant women were fully vaccinated.
Healio: Why are these recommendations necessary?
Colburn: Pregnant women are at high risk for severe disease from COVID-19, which puts them at risk for admission to the ICU, being put on a ventilator and death. Vaccination is the absolute best way to avoid serious illness, hospitalization and death.
Healio: What are the risks that COVID-19 specifically presents to pregnant and postpartum women?
Colburn: In addition to the risks for severe illness and death, there is an increased risk for serious adverse pregnancy and neonatal outcomes. These include preterm birth and admission of the baby to a NICU. When a baby is born early, they can have serious, long-lasting health consequences from prematurity. Other adverse pregnancy outcomes, such as stillbirth, have been reported.
Healio: Have you seen vaccine hesitancy among your own patients who are pregnant or who plan on becoming pregnant? If so, why have they said they are hesitant?
Colburn: I have seen vaccine hesitancy in many patients, including pregnant and postpartum women. During pregnancy, women must avoid certain medications and foods to avoid serious infections in themselves or the fetus. It is understandable to pause to make sure a medication or vaccination is safe. Many patients do not know all the data that have been published regarding the safety and efficacy details of the vaccines. There is also a tremendous amount of false information on social media and the internet about the seriousness of COVID-19 and the vaccines.
Healio: What common myths have you seen related to the vaccine and pregnancy?
Colburn: One common myth circulating on the internet is about infertility. This is an incredibly cruel rumor that taps into the natural fear that many people have of not being able to conceive in the future. There is absolutely no evidence that any vaccine, including the COVID-19 vaccines, cause infertility.
Healio: How do you respond to these concerns?
Colburn: First, I listen carefully to my patient’s concerns and questions with empathy and without judgment. After I have identified their questions and concerns, I answer them truthfully and reference the high-quality data that have been published in a way that is easily understandable. The vaccine protects not only the mother’s health, but also the baby’s health. Women can pass protective antibodies to their babies through the placenta and breastmilk when they are vaccinated.
I also try to make the conversation very personal. When speaking to pregnant women, I often share that I was pregnant during the pandemic and understand their concerns about wanting to protect their baby, especially during such a frightening and tumultuous time. The vaccine was not yet available when I was pregnant, but I wish I could have been vaccinated then so I could have passed on protective antibodies to my baby. I also share that I am fully vaccinated, my family is fully vaccinated, and when my infant son is old enough, he will be vaccinated.
Healio: Now that these recommendations have been released, what can doctors do to encourage more women to get vaccinated?
Colburn: Doctors should talk to their patients at every visit and urge them to get vaccinated. We must be trusted sources of information for our patients and combat the huge amount of misinformation on the internet. The CDC has several resources on its website to help doctors address vaccine myths and encourage their patients to get vaccinated. The CDC and many professional societies such as the Infectious Diseases Society of America have resources on their websites about how to talk to patients about the COVID-19 vaccine.