The concomitant use of atogepant for preventive and ubrogepant for acute migraine treatment was found to be safe and well-tolerated over 12 weeks, according to research presented at the American Academy of Neurology annual meeting.
Patients often take atogepant for prevention of migraine plus ubrogepant for acute treatment, Jessica Ailani, MD, director of the MedStar Georgetown Headache Center and a professor in the department of neurology at Georgetown University Medical Center, said in a presentation. Sometimes they are each prescribed by two different providers.
A 24-week study showed no new safety issues when ubrogepant was added to atogepant for treatment of migraine. Image: Adobe Stock
“We thought, ‘What does their liver look like?’” she said. “We wanted to see, if we purposely put people on a combination of these treatments, what would happen to safety and tolerability.”
In the phase 4 TANDEM study, patients with episodic migraines received atogepant 60 mg once daily for 12 weeks. Then ubrogepant 100 mg was added as needed for breakthrough migraines for 12 weeks, according to the study. A second ubrogepant dose or another medication could be taken for unresolved headaches within 24 hours.
A total of 262 participants were treated in the first period of the study (Safety Population 1), and 218 continued into the second period (Safety Population 2).
“There was similar data across the board relative to frequency of use of ubrogepant,” Ailani said.
A treatment-emergent adverse event (TEAE) was seen in 49.6% of participants in Safety Population 1 vs. 43.1% in Safety Population 2. The most common TEAEs included COVID-19, fatigue, nausea, decreased appetite and constipation.
“Percentages are on the low side for atogepant when we add ubrogepant in,” she said. “No hepatic safety issues were seen in the combination group.”
Ailani concluded: “Concomitant use of ubrogepant and atogepant was safe and well-tolerated over a 12-week period. Overall safety results across 24 weeks were consistent with the safety profile of atogepant alone. No new safety issues were identified across the 24-week study.”
During the discussion period, Ailani noted that patients with uncontrolled cardiac disease, meaning those who experienced a myocardial infarction or stroke in the last 6 months, would not have been included in the trial.
“And you wouldn’t see uncontrolled hypertension come up in this short-term trial,” she said.
It’s never your fault when you get a migraine headache, but you can try skipping these common initiators.
Danger! There are at least two foods in this image that could trigger a migraine.
Migraines are the worst. If you don’t get them, think of them like a hangover without the party before. Sounds are louder, smells more pungent and lights extra bright. There’s also nausea, dizziness and, obviously, a killer headache.
While neurologists are still debating the exact causes of migraines, certain foods and drinks are known to trigger an attack in many. For me, blue cheese and white wine can bring them on, while my brother can’t eat anything with artificial sweeteners. Unlike most lists of foods to avoid, migraine triggers aren’t necessarily unhealthy if you don’t have the condition.
Getting A Migraine Isn’t Your Fault
There’s a lot of stigma around migraines; people who experience them are often dismissed as having “just a headache.” But let’s be clear: Migraine is a neurobiological disease caused by a genetic predisposition. Folks with migraine didn’t do anything to make themselves ill.
“[While] some foods are somewhat more likely to trigger an attack, it is important to state that no one ever should feel responsible for their migraine attack,” explained Dr. Thomas Berk, a neurologist, headache specialist and medical director of New York-based Neura Health. “You didn’t do anything to cause your migraine.”
People experiencing migraines have a hyperexcitable and reactive nervous system, according to Berk, which means that a series of stressors or triggers can bring on an attack. While there are some common ones, like certain types of foods and changes in hormone levels, everyone’s triggers are unique.
“A migraine trigger refers to any external or internal factor that contributes to the onset of migraine symptoms,” said Dr. Danielle Wilhour, a neurologist and migraine specialist at UCHealth Neurosciences Center in Aurora, Colorado. “Combining multiple factors is probably a more potent influence.”
Because migraine is a complex disorder, simply avoiding certain foods won’t be the key to preventing an attack.
“While dietary changes can be helpful, a more holistic approach that focuses on healthy lifestyle and a balanced diet is crucial,” Wilhour explained. “In some cases, medical interventions may be necessary for effective migraine management.”
Despite the complexity of migraines, knowing which foods and beverages are common triggers can help inform and prevent future attacks. With that in mind, here are the five most common migraine-triggering foods and beverages.
1. Alcohol
We all know that too many glasses of wine with dinner or too many after-work cocktails can give anyone a nasty headache, but for folks with migraine, as little as a single glass can cause an attack. Why? The reason isn’t clear, according to Wilhour.
“While alcohol itself, as well as its metabolites, are potential factors in some instances, it’s also plausible that certain components in various alcoholic beverages may serve as triggers,” she said. “Alcohol is known to cause vasodilation, causing blood vessels to swell.”
Adult beverages can be dehydrating, which may also cause an attack. Some folks find that they can enjoy certain types of hard liquor but can’t drink wine, or vice versa.
If you’re partial to a glass of vino, you should know that red wine is more often linked to an immediate attack, due to the naturally occurring compound tyramine. Tyramine is found in a few other migraine triggers as well, including dark chocolate and aged cheese.
“Migraine attacks have also been speculated to be associated with the presence of some biogenic amines (histamine, tyramine, phenylethylamine, etc.) which could theoretically trigger a headache,” said Dr. Teshamae Monteith, an associate professor of clinical neurology and the chief of the headache division at the University of Miami Miller School of Medicine.
2. Chocolate
The cocoa in chocolate is believed to influence serotonin release, possibly contributing to migraines.
Skip the box of chocolates for your migraine-affected Valentine! Chocolate is considered the most popular food-based trigger. However, neurologists are debating whether craving bonbons before an attack is part of the prodome (or pre-attack phase of a migraine) or a trigger.
Whichever it is, one potential reason could be the cocoa.
“Cocoa is thought to influence serotonin release, possibly contributing to migraine pathogenesis,” Wilhour explained. “Although chocolate contains serotonin and its precursor tryptophan, with higher levels in 85% cocoa content, existing studies haven’t confirmed a direct link to migraine induction.”
3. Caffeine (Too Much Or Too Little)
When I first got diagnosed with migraines, my neurologist recommended that I down a shot of espresso at the onset of an attack to help stop it. As a teenager with infrequent access to Italian coffee shops, that didn’t quite work for me. But caffeine is sometimes used to treat migraines, even in certain over-the-counter medications.
Too much caffeine can also bring on a migraine. “Caffeine acts by impacting a molecule called adenosine by blocking its receptor,” Monteith explained. “It can reduce brain electrical activity, widen blood vessels and alter sleep. Naturally, adenosine levels increase during acute migraine attacks but can also be trigged by adenosine infusions.”
Like alcohol, caffeine has a dehydrating effect, which can trigger a migraine. For healthy adults, the Food and Drug Administration recommends consuming no more than 400 milligrams in a day, or four to five cups of coffee. For managing migraines, you may want to drink less, according to Berk.
“Regulating caffeine can be helpful as it is a vasoconstrictor and can be used to acutely treat a migraine attack,” Berk said. “Typically we recommend that patients with migraine limit caffeine to a cup of coffee (or caffeinated tea) at the same time each day (preferably before noon to ensure good sleep).”
Since regular consumption of coffee, tea or even your favorite energy drink can create dependence, skipping your afternoon cup of joe can also cause an attack.
3. Aged Cheese
Though it’s delicious, aged cheddar could be a migraine trigger.
Some aged cheese contains tyramine, which is developed as the cheese ferments. This means that the older (and smellier) the cheese is, the more tyramine it has.
“It is believed that elevated levels of tyramine can trigger migraines in susceptible people,” Wilhour said. “Tyramine is known to affect blood pressure and may influence the release of neurotransmitters like norepinephrine, which can be involved with migraines.”
Common offenders include aged cheddar, manchego, and blue cheeses like Gorgonzola and Stilton. (It turns out that many cheeses are aged, so do a little research before your next trip to the grocery store.)
4. Cured And Processed Meats
Breakfast favorites like bacon and sausage, as well as “girl dinner” staples like salami and prosciutto, might be worth skipping, as these can contain nitrates and nitrites.
“Nitrates can be converted into nitric oxide, which is a signaling molecule that plays a role in the regulation of blood flow,” Wilhour said. “Changes in blood flow are associated with migraines, and nitric oxide production may contribute to these changes. Additionally, nitrates may activate the trigeminal nerve (a nerve which is involved in the migraine pain pathway) and cause inflammatory neuropeptide release.”
Blame it on the gut microbiome: A 2016 study found that people with migraines may have higher levels of the bacteria that help break down nitrates. More bacteria mean more nitric oxide, which has a demonstrated association with migraines. Researchers hope to one day create a probiotic mouthwash that can re-balance bacteria levels.
5. Fasting (Not A Food, I Know)
While not a food or beverage, the experts I spoke with noted that skipping a meal is one of the most common migraine triggers. A 2018 study reported that “fasting is among the best studied and most reliable natural migraine triggers and becomes more common with longer fasts.”
When we miss a meal or two, our blood sugar drops. For some folks, even small changes in glucose levels can interfere with pain receptors in the brain’s lining. (There are no pain receptors in the brain itself.) To stave off migraines, keep protein-packed snacks on hand if you know you will be running late.
And if you forgot your emotional support water tumbler at home, that can also lead to a migraine. When the body dehydrates, fluid leaves the brain, causing friction in the meninges and potential pain.
Close-up of mid adult woman suffering from sinus headache
In addition to severe pain from headache, migraine can cause a number of debilitating symptoms that range from nausea and vomiting to sensitivity to light and sound.¹ These symptoms can make it significantly harder for patients to work or perform basic tasks, and can negatively affect their overall quality of life.
Patients experiencing chronic migraine may not be fully aware of the factors that can trigger a migraine or increase its severity and frequency. As a result, they may not know that certain lifestyle factors could be contributing to their migraine progression.
Educating patients on what factors can mitigate or exacerbate migraine can be helpful to those with migraine and those with loved ones who experience migraine. It has been estimated that over 10% of people worldwide are affected by migraine.¹ With such a significant number of people experiencing the debilitating effects of chronic migraine, it is beneficial to understand some of the factors, in a patient’s control or otherwise, that can affect migraine progression and what they can consider doing to mitigate the effects. When discussing migraine with patients, what are some risk factors for progression you should mention?
Dehydration
Dehydration can affect migraine progression, frequency, and severity in a number of ways. In a 2021 study published in Current Pain and Headache Reports, researchers examined associations between dehydration and headache, finding that women who drank more water (and overall fluids) had reduced severity and frequency of migraine attacks.² While not necessarily a cause of migraine, dehydration also has the potential to both worsen migraine effects and be caused by migraine symptoms such as nausea and vomiting.
The researchers noted that while intravenous fluid use during a migraine attack is unclear in terms of efficacy, fluid intake as part of a long-term migraine management plan could be beneficial. Other studies have found similar results; researchers of a 2023 study in the Journal of Neurology concluded that hydration was among the possible risk factors for migraine progression and that less water intake was associated with more migraine disability and longer headache duration.³
Certain migraine triggers for patients are also associated with dehydration. For example, alcohol and coffee are common triggers that are also known to cause dehydration.⁴ For patients with these triggers, hydration should be a large component of long-term management.
Tobacco
Tobacco use is commonly considered a risk factor for migraine progression and severity, and recent research has identified demonstrable evidence in support of that claim. A 2023 study in Current Pain and Headache Reports examined existing data about migraine and tobacco, finding that current smokers tended to have more headaches than those who formerly or have never smoked.⁵
The researchers also found a number of tobaccos can be particularly dangerous for patients with migraine, noting that smoking and migraine are independent risk factors for stroke that can become amplified when combined. Smoking is often used as a coping mechanism for stress, another common migraine trigger. In addition, the stress induced by migraine symptoms may make it more difficult for patients to actively work on smoking cessation.
While they acknowledged that more data was needed to determine if there is a strong correlation between smoking cessation and improved migraine symptoms, it is still beneficial to overall patient health. The researchers of the aforementioned Journal of Neurology study similarly concluded that smoking tobacco was a migraine progression risk factor, and that cessation should be considered as part of migraine management.³
Sex
A patient’s sex may determine if they are more likely to experience migraine and how severe it is. Women are more likely to experience migraine attacks and migraine-related disability than men.³ Part of this may be hormonal; hormone changes during menstruation or pregnancy have shown to be migraine triggers for some.⁴ It may be helpful to discuss documenting migraine frequency with female patients to determine if this is a potential trigger.
Obesity
Research has suggested that being overweight and obesity may be correlated with an increased risk of chronic migraine.³ A 2022 study on the neurobiology of migraine progression in Neurobiology of Pain claimed there was a nearly two-fold increase in risk for developing chronic migraine in patients who are obese.⁶ The researchers, though, acknowledged that the underlying pathophysiology that may explain this is not firmly established.
Health care professionals working with obese patients who have migraine may want to mention diet as a way to help manage migraine. Many foods, like processed and cured meats, have been shown to trigger migraine attacks in certain patients, while inconsistent meal schedules may also be triggers.⁴ Putting a stronger effort into dietary health may not just benefit patients wanting to work on their obesity, but could be helpful in identifying their migraine triggers.
Medication Overuse
Overusing medication, even migraine medications, can cause significant migraine progression. Acute medication in particular, such as simple analgesic and opiates, can put patients at risk of medication overuse headache.⁶ This can be tricky for patients and health care professionals alike, as medication overuse can be both a cause and consequence of medication overuse headaches. As a result, it has been suggested that acute medication in patients with migraine should be taken under 10 days a month with patients being mindful of whether they need an increase in their medication.³
Patient education – regarding medication overuse and other risk factors – is crucial in helping to limit migraine attacks and progression. Health care providers treating patients experiencing migraine should encourage open communication about triggers and whether migraine attacks are worsening to best determine if an outside factor is exacerbating the progression.
Could migraine increase the risk of inflammatory bowel disease? A new study found a link. Michela Ravasio/Stocksy
More than 1 billion people around the world have at least one migraine attack each year.
Previous research shows that migraine can potentially increase a person’s risk for several health issues, including gastrointestinal conditions.
New research from Seoul National University College of Medicine in South Korea says there may also be a link between migraine and an increased risk for inflammatory bowel disease (IBD).
Now, researchers from Seoul National University College of Medicine in South Korea say there may also be a link between migraine and an increased risk for irritable bowel disease (IBD), which is an umbrella term that includes Crohn’s disease and ulcerative colitis.
According to Dr. Brooks D. Cash, professor and chief of the division of Gastroenterology, Hepatology, and Nutrition at UTHealth Houston in Texas, who was not involved in this study, the field of gastroenterology has recognized for many years that migraine has been associated with many chronic gastrointestinal syndromes and diseases.
“The data in this report supports previous reports of an association between migraine headaches and IBD,” Dr. Cash told Medical News Today.
Dr. Rudolph Bedford, a board-certified gastroenterologist at Providence Saint John’s Health Center in Santa Monica, CA, who was also not involved in this study, told MNT that the research results were not surprising.
“[With] inflammatory bowel disease we do see some extra-intestinal manifestations including things involving the eye or ocular findings, which may be neurogenic in nature, so it wasn’t surprising,” Dr. Bedford added.
This is not the first study to look at a connection between migraine and IBD.
A study published in March 2021 of people in the United States found a higher prevalenceTrusted Source of migraine or severe headaches among adults with IBD than in those without.
Research published in March 2023 reported an increased prevalence of IBD in people with migraine with and without aura.
For the current study, researchers analyzed data from more than 10 million people through the nationwide healthcare system for South Korean citizens. About 3% of the study population had IBD.
Through the data, scientists found the incidence of IBD was significantly higher in people who had migraine compared to those who did not.
Scientists also reviewed the data through subgroups of Crohn’s disease and ulcerative colitis incidences. People with migraine in both subgroups had a higher risk of developing either condition when compared to people without migraine.
After a migraine diagnosis, researchers found people were at a higher risk of developing Crohn’s disease, with a significant rise after a 5-year follow-up.
Additionally, within the subgroups, scientists reported that the impact of migraine on the risk of developing ulcerative colitis was more prominent in men than women.
Based on these findings, the research team suggests that people with migraine be monitored carefully for the development of IBD.
However, Dr. Cash stated that the data presented do not convincingly support that approach or recommendation.
“The odds ratios that were reported in this study, which can be thought of as the increased odds of an outcome (e.g., developing IBD) with a given exposure (e.g., migraine headaches), were consistently between one to two, which is not far from definitive and can be easily misinterpreted or misrepresented,” he explained.
“The results are, at best, suggestive of an association between migraines and IBD, which we were already aware of based on previous research and deserve to be further evaluated. However, the minimal increase in the odds of developing IBD reported in this study is not sufficient to recommend increased monitoring of patients with migraines for the development of Crohn’s disease or ulcerative colitis.”
Dr. Bedford said it is important to identify potential health issues that may trigger IBD, as a doctor may be able to mitigate the symptoms of IBD if they know what may be associated with it.
“Migraines can be very debilitating and you may want to identify those people with migraines,” he continued. “We don’t normally question patients with inflammatory bowel disease whether or not they have migraine headaches, so it probably rates as something that should be done more frequently.”
“These results add to an already relatively robust body of research suggesting that chronic pain syndromes are statistically more common in patients with chronic GI syndromes or diseases,” Dr. Cash said.
“We do not have enough information or proof yet to establish a causal relationship either way. But this data can be used to explain some therapeutic approaches that may benefit both GI and neurologic symptoms in patients with migraines,” he added.
Regarding the next steps for this research, Dr. Cash said that mechanistic data evaluating the possible reasons for these consistent observations of association is needed.
“Right now, all we have are hypotheses,” he continued. “Are there changes in the gut-brain communication pathways or sensory perceptions in the enteric and central nervous systems? Is the gut microbiome involved? Are there psychological and stress-mediated factors at play?”
“Once clinical relationships such as these have been identified, we need to move toward trying to explain why those relationships may exist,” Dr. Cash added. “That, in turn, may lead us to develop more targeted and effective therapies that can address multiple symptoms/syndromes.”
Dr. Bedford suggested researchers look for an association between IBD flares and migraine occurring at the same time. As migraine is associated with serotonin release, he encouraged researchers to examine how the serotonin transporters within the GI tract, small bowel, and colon might play a role.
“I think just questioning our patients in terms of quality of life issues — is there any way that we can mitigate their migraine headaches, potentially preventing their inflammatory bowel disease flare, or vice versa, is certainly something to look into,” Dr. Bedford said.
Migraine recurrence can cause significant pain and negatively affect a patient’s quality of life. What preventative measures should patients know about?
Patients with recurrent migraines often experience significant impairment as a result of their condition, which negatively affects their quality of life.¹ When discussing migraine prevention with your patients, they may ask about preventive measures and whether they require lifestyle changes or a more targeted treatment approach.
There are a number of options for patients seeking to prevent migraine recurrence that may be worth mentioning. Be sure to have a thorough discussion with them about their migraine history and overall health to determine whether lifestyle changes and medications are worth exploring for migraine prevention.
What should your patients know about how certain preventative measures affect migraine?
Food Management
Food management, in the context of migraine prevention, is about noticing the ways your diet affects your migraine; for example, keeping track of whether certain foods have seemingly triggered a migraine or if you’ve been eating meals at consistent times.² A consistent meal schedule may help keep migraine in check, whereas fasting can increase risk. In addition, keeping a food journal that also tracks migraine occurrences may help patients recognize potential triggers to avoid.
A 2020 study in Headache: The Journal of Head and Face Pain examined the role diet and nutrition play in migraine triggers and prevention. The researchers found that diets that eliminate certain foods may help reduce migraine risk.³ Specifically, alcohol and caffeine were often associated with an increased risk of migraine, therefore reducing consumption of both may help reduce migraine. The investigators also suggested that low-fat diets may be effective at reducing migraine, although they acknowledged more in-depth research is needed.
Other data the researchers analyzed suggested that diets rich in omega-3 polyunsaturated fatty acids show potential to reduce migraine frequency, and that ketogenic diets and diets that eliminate IgG-positive foods may also help depending on triggers. Discussing with your patients how different foods and nutrients affect migraine and overall quality of life may help to create a structured diet centered on preventing migraine.
Sleep Management
Migraines can potentially be triggered by a lack of quality sleep.² Therefore, prioritizing healthy sleep habits is key – and another instance in which keeping a journal may help identify what’s causing a lack of sleep and triggering migraines. Patients may find that distractions like their phone can affect their sleep. They might also find do exercise and dietary habits prior to bed play a role.
Patients experiencing migraine may also have comorbid sleep disorders, which can exacerbate one another. A 2021 study published in the International Journal of Molecular Sciences examined the association between migraine and sleep disorders, finding that insomnia, obstructive sleep apnea, and parasomnia were among the most common sleep disorders in patients with migraine.⁴ Per the researchers, patients with migraine and insomnia often have increased migraine attack frequency and pain intensity. The investigators also claim that, among parasomnias, sleepwalking has been associated with migraine and somnambulism has a higher rate in patients with migraine with aura.
Health care professionals may consider informing their patients of the ways sleep disorders may affect migraine and how to address the problem.
Stress
A common mnemonic device when discussing lifestyle changes for reducing migraine triggers is SEEDS: Sleep, Exercise, Eat, Diary, and Stress.⁵ Stress can be a trigger for migraine attacks, and if patients are finding an association between stress and migraine incidence, they may benefit from relaxation and mindfulness techniques. Patients may seek mental health care treatment if stress becomes overwhelming, or may opt to journal about their stress.
Beta Blockers
While lifestyle changes can be beneficial, many patients still require additional treatment to prevent migraine. Beta blockers, often used to treat blood pressure, may be an option. One beta blocker, propranolol, is a common first-line treatment for migraine and is seen as one of the most effective options.¹ As it is also used to regulate blood pressure, beta blockers may be considered for patients with migraine and cardiovascular disease.
Other options include atenolol, metoprolol, nadolol, and timolol.⁶ Though they may be effective, they also come with potential side effects patients should know about. These include fatigue, shortness of breath, nausea, insomnia, and low physical tolerance for exercise.
Various studies have come to similar conclusions about beta blockers – that they are potentially an effective option but may lead to side effects. A 2023 study in the Journal of Headache and Pain reviewed the comparative effectiveness of different migraine medications, including beta blockers.⁷ The researchers concluded that beta blockers were likely effective at creating a 50% or greater reduction in monthly migraine days for patients, but also had a higher likelihood of adverse events than other treatment options.
Antidepressants
Certain antidepressants have shown promise in their ability to prevent migraine, particularly amitriptyline.¹ Venlafaxine is another option that has been used for migraine. Side effects, depending on the antidepressant used, can include fluctuations in weight, dry mouth, and sedation.⁶
Calcitonin Gene-Related Peptide Therapies
Treatments that focus on inhibiting the calcitonin gene-related peptide (CGRP) to block the pain signal are designed specifically for the treatment of migraine.⁶ Some studies have suggested that antibodies inhibiting the CGRP or its receptor are among the most effective treatments at reducing monthly migraine days while posing a lesser risk of adverse events.⁷
Ultimately, patients will need to discuss with their health care professional the ways their migraine is affecting them and the specific triggers they’ve noticed to determine the best course of action for prevention
A Chronic pain is bad enough on a normal day, but crummy weather can make already achy joints and hips that much more painful. Tied to changes in the barometric pressure resulting from storms, the cold, and dreary forecasts, pain-based weather is a significant concern on a day-to-day basis for millions of people. Now, researchers from the University of Georgia report that roughly 70 percent of respondents in a recent poll would change their daily behavior based solely on weather-based pain forecasts.
“We’re finding more consistent relationships between weather patterns and pain, so it seems more possible to make weather-based pain forecasts,” says lead study author and geography/atmospheric sciences lecturer Christopher Elcik in a media release. “This study was to survey and see what the audience was for this type of forecast.”
In all, researchers surveyed over 4,600 people. Among respondents who identified as migraine sufferers, 89 percent pointed to weather as something that impacts their pain level, and another 79 percent cited weather as a trigger for their pain. Meanwhile, among respondents with other conditions, 64 percent also said weather patterns could trigger pain and an astounding 94 percent identified weather as an influential pain factor.
This latest report builds on previous research that focused on specific weather patterns and pain-related conditions in an attempt to measure public interest in a weather-based pain forecast, as that may be indicative of high or moderate risk for migraines or chronic pain.
“I see how much people can be affected by these types of pain, so if I can provide someone with insight into the level of risk for a day, maybe people can take steps to prevent the pain from happening,” Elcik comments. “There are preventative measures people can take if risks are higher.”
Hypothetically, if the risk of weather-related pain were high, more than half of respondents said they were likely to take preventive measures (medication, rest, avoiding compounding triggers). Another 47 percent with migraines and 46 percent of those with pain-related conditions were also “extremely likely” to take the same measures.
Notably, desire for a forecasting tool was very high; 72 percent of those living with migraines and 66 percent with pain-related conditions said they would alter their behavior by canceling plans or taking preventive measures in the event of a weather-based pain forecast. Some respondents even said they already use online tools to predict weather-related pain.
One example is AccuWeather’s arthritis or migraine forecast, which predicts low-to-high pain risk according to atmospheric conditions. These existing tools, however, offer few details regarding the variables considered or how the predictions are actually produced.
A person’s likelihood to continue with plans also depended heavily on the length of the activity in question. If plans were roughly 30 minutes long, 57 percent of respondents with migraines and 52 percent of those with pain-related conditions said they would be “extremely likely” to continue plans even if there were a moderate risk of pain. About 43 percent from each group said they would continue even with the highest risk forecast.
When it came to an activity lasting more than three hours, on the other hand, that number declined to roughly 23 percent for moderate risk and 18 percent for high risk among those with migraines. For people living with other pain-related conditions, 23 percent would follow through with a three hour plus activity in the face of a moderate risk of weather pain and 21 percent would continue despite the highest risk. Generally speaking, as the level of risk increased, so did the likelihood to alter plans.
“This was across the board,” Elcik notes. “Everyone was more likely to cancel plans if the forecast risk was higher.”
While additional research and studies are necessary in order to create a reliable pain-based weather forecast, Elcik believes this study highlights the urgent importance of developing such a resource.
“This publication shows there’s an audience that’s willing and eager to try something new, and there are probably many more people who would benefit—more than we even thought,” the researcher concludes. “I think these results can push other researchers to also look at similar, larger-scale weather phenomena and help the community better understand how the atmosphere does impact pain.”
Cyclic migraine is when a person only experiences migraine symptoms during certain periods or cycles. They do not have migraine episodes outside these periods.
Migraine is a condition that involves experiencing headaches or episodes with specific characteristics. Migraine symptoms include throbbing and pulsating pain on one side of a person’s head. They can be very painful and interfere with a person’s daily activities.
With cyclic migraine, people experience migraine symptoms in cycles. They may have symptoms that occur daily for a few weeks before being symptom-free for weeks or months at a time. Some treatments may help with cyclic migraine.
This article discusses the symptoms, causes, and triggers of cyclic migraine. It also discusses a person’s risk factors and how doctors diagnose and treat the condition.
People with different kinds of migraine may have different symptoms. People with cyclic migraine usually have 10 or more episodes of migraine symptoms every month. These episodes occur daily or almost daily for several weeks. They then ease off for a few weeks or months at a time.
Most scientists believe that abnormal changes in a person’s brain cause it to become inflamed. This inflammation causesTrusted Source the activation of nerves and the release of neurochemicals, including serotonin and CGRP, which mediate pain. Migraine may also have a genetic cause.
At present, there is little scientific research into the causes of cyclic migraine specifically.
Although scientists do not yet know what causes migraine, there are some common riskTrusted Source factors for the condition. Migraine is more common among females and people between the ages of 15 and 55 years. Migraine may often become less severe and less frequent as a person gets older.
People are more likely to have migraine if they have a close family member who has the condition. There is little formal research into the specific risk factors for cyclic migraine.
There is little formal guidance on treatments for cyclic migraine specifically.
Older sources claim treatments for cyclic migraine include lithium. More current sources also state that lithium may help people with cyclic migraine. However, people taking this medication need careful professional monitoring of their blood level and thyroid function.
Other treatments for cyclic migraine may include some or all standard migraine treatments. These includeTrusted Source:
preventive medication to stop migraine episodes from occurring
People with cyclic migraine have migraine symptoms that occur in periods of weeks or months at a time. Outside of these cycles, they do not have migraine.
There is little recent formal research into cyclic migraine. Treatments and diagnosis methods for migraine may help people with cyclic migraine.
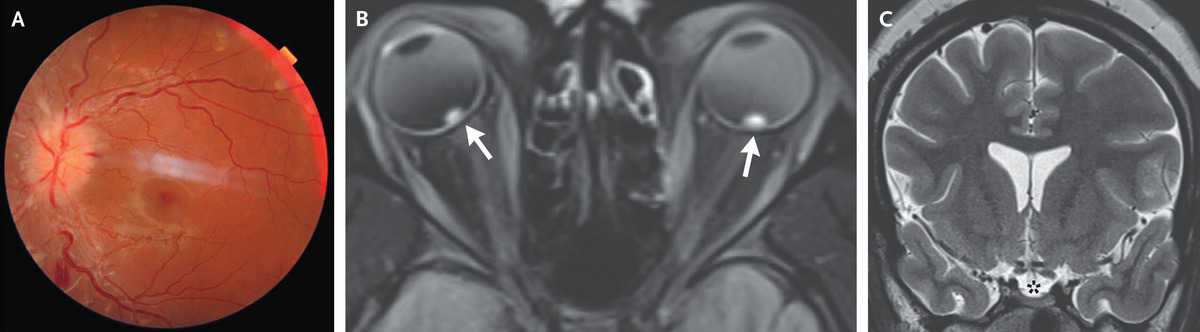
A 25-year-old woman with severe obesity presented to the emergency department with a 1-week history of blurred vision, transient visual obscurations, daily headaches, and intermittent whooshing sounds. Her body-mass index (the weight in kilograms divided by the square of the height in meters) was 57. On neurologic examination, optic-disk swelling and retinal hemorrhages were present in both eyes (Panel A, left eye). The results of visual-field and cranial-nerve testing were normal. Magnetic resonance imaging and venography of the head revealed flattened posterior globes with marked elevation of the optic-nerve heads (Panel B, arrows), an empty sella (Panel C, asterisk), and stenoses of the transverse sinuses without obstruction or thromboses — all of which were suggestive of elevated cerebrospinal fluid pressure. A lumbar puncture was notable for an elevated opening pressure of 55 cm of water (reference range, 10 to 20); the results of the cerebrospinal fluid analysis were normal. A diagnosis of idiopathic intracranial hypertension was made. Idiopathic intracranial hypertension is a disorder associated with obesity that manifests with symptoms resulting from increased intracranial pressure, including headaches, diplopia, visual field defects, and pulsatile tinnitus. Treatment with high-dose acetazolamide was started, and counseling on weight loss was provided. At a 1-month follow-up visit, the patient’s papilledema had decreased, and treatment with acetazolamide had been continued.
The FDA has approved Pfizer’s Zavzpret, a calcitonin gene-related peptide receptor antagonist nasal spray to treat migraine with or without aura in adults.
According to a company press release, approval was based on results of two randomized, double-blind, placebo-controlled studies that established the safety, efficacy and tolerability profiles of the intranasal therapeutic. In these studies, Zavzpret (zavegepant) was superior to placebo on the co-primary endpoints of pain freedom and freedom from most bothersome symptoms at 2 hours post-dose. The drug also demonstrated pain relief as early as 15 minutes in a prespecified secondary endpoint compared with placebo.
The FDA has approved Pfizer’s novel nasal spray to treat migraine in adults. Image: Adobe Stock
“The FDA approval of Zavzpret marks a significant breakthrough for people with migraine who need freedom from pain and prefer alternative options to oral medications,” Angela Hwang,MBA, chief commercial officer and president of global biopharmaceuticals business at Pfizer, stated in the release.
Zavzpret was well-tolerated in these trials, per the release, with the most common adverse reactions of taste disorders, nausea, nasal discomfort and vomiting reported in at least 2% of trial participants. Hypersensitivity reactions, including facial swelling and urticaria, have also been reported.
According to Pfizer, Zavzpret is expected to be available in pharmacies in July 2023.
Summary: Using oral transmucosal delivery of eletriptan hydrobromide delivers faster and more effective relief for migraine sufferers.
Source: Malmo University
In order for migraine medication to be effective, it is vital that the active substance is released into the bloodstream immediately. The pills currently on the market today pass through the body’s metabolism which means the effectiveness is lessened and there is a delay to the relief.
A research team at Malmö University believes they can get around this by means of a shortcut in the mucous membrane in the mouth.
The active substances in migraine medicine are known as triptans. This is a collective name for tryptamine-based drugs that react with serotonin receptors and thereby inhibit certain signalling substances in the brain that can prompt the experience of pain. Serotonin is one of the most important signalling substances in the human nervous system and affects, among other things, sexual behaviour, appetite, sleep and pain.
In the research project Oral transmucosal delivery of eletriptan for neurological diseases, Sabrina Valetti and her research colleagues have chosen to work with eletriptan hydrobromide (EB), which is the triptan that has the least toxic effect on the heart.
“A regular triptan pill must pass through both the stomach and the liver, where a large part of the metabolism takes place. Studies show that more than half of the triptan dose is broken down on the way before it reaches the blood. We have investigated the possibility of getting EB directly into the blood vessels of the mouth through the mucosa under the tongue,” explains Valetti, who leads the project at the Biofilms Research Center for Biointerfaces.
Serotonin is one of the most important signalling substances in the human nervous system and affects, among other things, sexual behaviour, appetite, sleep and pain
“We know from patient studies that it is important for the substance to reach maximum concentration in the blood within two hours in order to have an effect. So we investigated what the expected concentration of EB was with our method after this time. We saw that the expected concentration was higher in the 3D human cells than those provided by regular migraine pills. This was also the case for the pig mucosa, but only if the pH value was raised,” she says, and continues:
“Our body has a buffer system that regulates and balances temporary pH variations and we saw no toxic effect on the mucosa during a four-hour period when the pH value was increased from 6.8 to 10.4. But what we don’t know is whether this is experienced as unpleasant in the mouth or not.”
The biggest challenge lies in the fact that the mucous membrane is a relatively thick tissue and a barrier that should protect us from a variety of external attacks. Last autumn, they therefore carried out tests where they examined in detail the lipids, which are believed to play a decisive role in pig mucous membrane in order to gain a better understanding of this particular barrier effect.
Abstract
Oral transmucosal delivery of eletriptan for neurological diseases
Migraine is a highly prevalent neurological disease affecting circa 1 billion patients worldwide with severe incapacitating symptoms, which significantly diminishes the quality of life. As self-medication practice, oral administration of triptans is the most common option, despite its relatively slow therapeutic onset and low drug bioavailability.
To overcome these issues, here we present, to the best of our knowledge, the first study on the possibility of oral transmucosal delivery of one of the safest triptans, namely eletriptan hydrobromide (EB).
Based on a comprehensive set of in vitro and ex vivo experiments, we highlight the conditions required for oral transmucosal delivery, potentially giving rise to similar, or even higher, drug plasma concentrations expected from conventional oral administration.
With histology and tissue integrity studies, we conclude that EB neither induces morphological changes nor impairs the integrity of the mucosal barrier following 4 h of exposure.
On a cellular level, EB is internalized in human oral keratinocytes within the first 5 min without inducing toxicity at the relevant concentrations for transmucosal delivery. Considering that the pKa of EB falls within the physiologically range, we systematically investigated the effect of pH on both solubility and transmucosal permeation.
When the pH is increased from 6.8 to 10.4, the drug solubility decreases drastically from 14.7 to 0.07 mg/mL. At pH 6.8, EB gave rise to the highest drug flux and total permeated amount across mucosa, while at pH 10.4 EB shows greater permeability coefficient and thus higher ratio of permeated drug versus applied drug. Permeation experiments with model membranes confirmed the pH dependent permeation profile of EB.
The distribution of EB in different cellular compartments of keratinocytes is pH dependent. In brief, high drug ionization leads to higher association with the cell membrane, suggesting ionic interactions between EB and the phospholipid head groups. Moreover, we show that the chemical permeation enhancer DMSO can be used to enhance the drug permeation significantly (i.e., 12 to 36-fold increase).
Taken together, this study presents important findings on transmucosal delivery of eletriptan via the oral cavity and paves the way for clinical investigations for a fast and safe migraine treatment.