Nearly one-third of all measles cases reported in the U.S. since 2020 were reported in the first quarter of 2024.
Measles vaccine coverage has remained below estimated population-level immunity for 3 years.
A sharp uptick in reported measles cases in the United States during the first quarter of 2024 has raised concerns that the country could lose its measles elimination status, CDC researchers said Thursday.
Although the risk for widespread measles transmission in the U.S. remains low because of high population immunity, a more than 17-fold increase in measles cases in the first 3 months of 2024 over the mean number of cases in the same time period from 2020 to 2023 is cause for concern, Adria D. Mathis, MSPH, and colleagues from the CDC’s Division of Viral Diseases wrote in a new study published in MMWR.
Data derived from Mathis AD, et al. Morb Mortal Wkly Rep. 2024;doi:10.15585/mmwr.mm7314a1.
“We have seen measles on the rise globally over the past few years, so the uptick in cases is unfortunately not unexpected, but the current increase is certainly drastic,” Mathis told Healio.
Although travel-related outbreaks still occur, the U.S. was declared to have eliminated endemic transmission of measles in 2000. It would lose that status if an outbreak persists for more than a year.
“Because of the absence of endemic measles virus transmission for 12 consecutive months in the presence of a well-performing surveillance system, as of the end of 2023, measles elimination has been maintained in the United States,” Mathis and colleagues wrote. “However, the rapid increase in the number of reported measles cases during the first quarter of 2024 represents a renewed threat to elimination.”
Measles vaccination rates, like most childhood vaccination rates, fell during the COVID-19 pandemic. A record 40 million children worldwide missed their first or second dose of measles vaccine in 2021.
In the U.S., roughly 95% of children had received routine, state-required vaccines — including the MMR vaccine before the pandemic — but by the 2022-2023 school year, the vaccination rate had declined to 93%, remaining below pre-pandemic levels, while vaccine exemptions reached an all-time high.
The CDC in January issued an alert for health care providers to be on the lookout for measles amid the ongoing increase in cases.
For their study, Mathis and colleagues analyzed data on confirmed measles cases reported to the National Notifiable Disease Surveillance System or directly to the National Center for Immunization and Respiratory Diseases from Jan. 1, 2020, to March 28, 2024.
Overall, 338 confirmed measles cases with rash onset were reported during the study period in 30 U.S. jurisdictions. Ninety-six percent of cases were associated with importation and 61% occurred among U.S. residents who were eligible for vaccination but who were either unvaccinated or whose vaccination status was unknown.
In 2020, just 13 measles cases were reported — all but one before COVID-19 mitigation efforts started in March 2020. A majority of cases in 2021 and 2022 were related to outbreaks, according to the study.
Of 49 cases in 2021, 47 occurred among Afghan evacuees housed at U.S. military bases during Operation Allies Welcome. In 2022, 86 of 121 cases were linked to an outbreak in central Ohio.
There have already been 97 reported cases this year as of March 28 — nearly one-third of the total number of measles cases reported since January 2020, Mathis and colleagues reported. Nearly all of the cases have occurred among people who either were not vaccinated or whose vaccination status was unknown.
Mathis and colleagues attributed the surge to MMR vaccination coverage remaining below 95% — the mark that is widely recommended for measles elimination — for 3 straight years.
In addition to estimating that roughly 250,000 kindergartners have not received the MMR vaccine in the last 3 years, they noted that vaccination coverage rates in 12 states and the District of Columbia were less than 90% and that vaccine exemption rates among kindergartners exceeded 5% in 10 states during the 2022-2023 school year.
“Clinicians have a crucial role in helping to prevent measles and its complications, and maintain the U.S. measles elimination status,” Mathis said. “Their efforts are needed to help encourage routine vaccination and vaccination before international travel, identify communities at risk for measles transmission and rapidly diagnose and report measles cases.”
PERSPECTIVE
We know that measles outbreaks can occur in pockets where childhood immunization rates with the MMR vaccine begin falling below 90% to 95%. Unfortunately, we are starting to see such outbreaks with increasing frequency in parts of the U.S. where vaccine resistance is accelerating. In 2018, in PLoS Medicine, together with colleagues, we identified many such areas when we look at MMR or other childhood immunization rates at the county level — or even school district level — which is unfortunate given that such information turns out to be a fairly good predictor of where measles might strike next.
As vaccine hesitancy accelerated during the COVID-19 pandemic, especially in my state of Texas and neighboring states in the South, we saw thousands of people needlessly perish during the delta and BA.1 omicron waves of SARS-CoV-2 in 2021 and 2022. This happened because so many refused COVID-19 vaccines, even though they protected at high levels vs. death and severe illness. I reported this in my recent book, The Deadly Rise of Anti-Science. My worry now is that this rise in anti-vaccine sentiments spills over to all childhood or adult immunizations. This is why it becomes especially important to track and monitor it. I am concerned about a sharp return of measles and other childhood illnesses.
Measles cases have ticked up in the U.K. following lower rates of MMR vaccination, and the U.S. could see similar outbreaks Carissa Wong & Nature magazine
UK health services are battling an outbreak of measles — causing alarm in a nation that had eliminated the disease in 2017.
On 19 January, the UK Health Security Agency (UKHSA), the public-health authority, declared a national incident over rising cases of measles. The agency has logged more than 300 cases in England since 1 October 2023.
A decline in uptake of the measles, mumps and rubella (MMR) vaccine, which is given in two doses, during the COVID-19 pandemic has spurred the spread of the disease across England and the rest of Europe, while small outbreaks have occurred in a handful of US states.
Measles is caused by a virus and is highly contagious. It is spread through coughing and sneezing. Symptoms include a fever, a runny nose and an itchy rash of red-brown spots. “It’s considered to be one of the most infectious respiratory infections there is,” says population-health researcher Helen Bedford at University College London. Those most at risk include babies, young children, pregnant people and those with a weakened immune system.
Nature explores the uptick in cases.
Why are measles cases rising in the United Kingdom?
Low uptake of the measles vaccine is a key driver of the UK measles cases, say researchers. Around 85% of children in England have received two MMR vaccine doses by five years old, according to data from the National Health Service (NHS). This falls below the vaccination rate of at least 95% needed to achieve ‘herd immunity’ — which substantially reduces disease spread — as recommended by the World Health Organization (WHO).
“It is worrying but not all that surprising to see another measles outbreak within the UK,” paediatrician Ronny Cheung at the Evelina London Children’s Hospital said in a statement to the UK Science Media Centre. “The fact remains that vaccination coverage for children under the age of 5 is now the lowest it has ever been in the past 10 years,” he said.
The COVID-19 pandemic worsened matters, says Bedford. At first, the number of measles cases dipped because of social-distancing measures. But vaccine uptake also dropped, contributing to the latest surge, she says.
Moreover, anti-vaccine messaging during the pandemic caused some people to question vaccine safety, which might have delayed uptake, says Bedford. “People have got more questions, which, unfortunately, due to cuts in public-health funding, aren’t always properly addressed,” she says.
How is the United Kingdom tackling the surge?
On 22 January, the NHS launched a vaccination campaign, urging millions of parents and carers to book vaccine appointments for their children. Health services will contact all parents of unvaccinated children aged 6 to 11. “If parents and young people respond to the information, and the message to get vaccinated, we could stop it in its tracks,” says Bedford
Vaccination rates are lowest in London, where just 74% of children have received two doses of the vaccine. Two doses are 97% effective against catching measles. One local council in the capital has launched a vaccine-awareness campaign in multiple languages to reach more people.
Without further action, the outbreak could spread more widely across the United Kingdom, causing deaths, says Bedford.
When was the last time there was a spike in UK measles cases?
In 2018, a measles outbreak of around 900 cases occurred in England. The previous year, the WHO had declared that the United Kingdom had eliminated the disease, defined as the absence of circulating measles. Despite losing the elimination status, the country gained it again in 2021.
In response to the outbreak, Public Health England, the UKHSA’s predecessor, advised people to get the MMR vaccine. “The only thing that you can do to stop measles spreading is get vaccinated,” says Bedford. “This means catching up people who didn’t have it, including those who didn’t have it 20 years ago,” she says.
What’s happening elsewhere?
Since 1 December, there have been 23 confirmed measles cases in the United States, across Georgia, Missouri, New Jersey and Pennsylvania. Many of the cases were linked to international travellers returning to the country, and reflect a rise in the number of measles cases globally, according to a newsletter sent by the US Centers for Disease and Control and Prevention on 25 January. There were 58 reported US cases last year, down from 121 in 2022. This is much less than the more than 1,200 US infections in 2019.
But Europe is facing a more alarming situation. There was a 45-fold rise in measles cases in the WHO’s European region from 2022 to 2023. In 2023, the region’s 40 member states reported some 42,200 measles cases, up from fewer than 1,000 in 2022.
The rise in cases is also the result of declining national vaccination rates, which fell from 92%, on average, in 2019 to 91% in 2022, according to the WHO.
Globally, the number of measles cases increased by 18% between 2021 and 2022, and deaths from measles increased by 43%, according to a WHO report released last November.
Amid a Rise in Confirmed Cases of Measles, Dr Toni Hazell Emphasises the Importance of Recognising This Highly Contagious Infection in Nine Top Tips for Primary Care
Read this Article to Learn More About:
concerns about a possible measles outbreak in Londonthe complications of measles, and how to make a diagnosisvaccine hesitancy, and talking to parents who are unsure about vaccination.Reflect on your learning and download our Reflection Record.
In 2022, there were 54 confirmed cases of measles in England, whereas in the first half of 2023, there have already been 128 cases.1 Two-thirds of these cases occurred in London, but there has been at least one case in every region of the UK.1
UK Health Security Agency (UKHSA) modelling shows that there are now significant concerns about a large outbreak in London and smaller outbreaks in specific populations elsewhere in the UK.1 Groups at risk include younger people aged 19–25 years (babies born in 1998, the year that Andrew Wakefield’s measles, mumps, and rubella [MMR] paper was published, are now 25 years old), people from undervaccinated communities, and those who are susceptible to measles and have travelled overseas.1
Those who watched Professor Chris Whitty’s briefings during the COVID-19 pandemic may remember how we all got a bit obsessed with the R number. If R is below one, each case of an infection produces less than one secondary case, so the number of infected people declines; conversely, if R is greater than one, cases will increase, as each person infects at least one more.In relation to COVID-19, the R numbers discussed were generally below five;2 the R number for measles is generally cited as somewhere between 12 and 18, and it is therefore extremely infectious.3
This article recaps the signs, symptoms, complications, and management of measles, covering vaccine hesitancy and evidence on the safety of vaccination, in nine top tips for GPs.
1. Take Measles and its Complications Seriously
A key trope of antivaxxers is that the infections that healthcare professionals aim to protect people against through vaccination are harmless ‘rites of passage’ of childhood, and that it is healthier for children to acquire the infections and fight them naturally.4 This is categorically untrue for measles. In developed countries, 10–20% of those who catch measles will experience some sort of complication, and the complication rate is probably higher in developing countries.5 Some complications of measles are shown in Box 1.5
All rights reserved. Subject to Notice of rights. NICE guidance is prepared for the National Health Service in England. All NICE guidance is subject to regular review and may be updated or withdrawn. NICE accepts no responsibility for the use of its content in this product/publication. See www.nice.org.uk/re-using-our-content/uk-open-content-licence for further details
Subacute sclerosing panencephalitis (SSPE) deserves a particular mention here because, unusually, it presents some years after the initial diagnosis of measles.5 A patient with SSPE will present with seizures and a decline in motor, cognitive, and behavioural function around 7 years after their measles infection, and the condition is always fatal.5 If a patient presents with these symptoms, it is worth asking if they have ever had measles, and if they are vaccinated.5
Medical writers around the world could spend years trying to describe what a nasty infection measles is, and they would not come close to the simplicity of Roald Dahl’s description of the death of his daughter Olivia:6
‘Olivia, my eldest daughter, caught measles when she was seven years old. As the illness took its usual course I can remember reading to her often in bed and not feeling particularly alarmed about it. Then one morning, when she was well on the road to recovery, I was sitting on her bed showing her how to fashion little animals out of coloured pipe-cleaners… I noticed that her fingers and her mind were not working together and she couldn’t do anything.
“Are you feeling all right?” I asked her.
“I feel all sleepy,” she said.
In an hour, she was unconscious. In twelve hours she was dead.’
2. Learn to Recognise a Case of Measles
Despite the fact that there are nearly 300,000 licensed doctors in the UK,7 as well as a growing number of other healthcare professionals, it is likely that most will never have seen a case of measles. To see measles regularly, a healthcare professional would need to have been working before 1968, when around 80% of the population contracted measles during childhood.8
Signs and Symptoms
Measles has a prodromal phase, which occurs about 10–12 days after exposure to the virus and lasts for 2–4 days before the rash appears.9 Symptoms include conjunctivitis and those of any viral infection—fatigue, malaise, cough, and a runny nose. During this period, the fever increases to 39°C before decreasing. A maculopapular erythematous rash starts on the face and behind the ears, and then spreads to the torso, limbs, and peripheries (see Figure 1).9 This is a key differentiator from other rashes, such as that of scarlet fever,10 which start on the torso. The rash fades after 5–7 days.9 The patient may also have Koplik spots on the buccal mucosa—these 2–3-mm wide red spots with a white centre are pathognomonic for measles (see Figure 2).9
Figure 1: Measles Rash
Figure 2: Koplik Spots
Risk Factors
Risk factors for contracting measles include being unvaccinated and in contact with a case of measles.9 Those who are vaccinated can occasionally contract the infection (known as a breakthrough case), but this is unusual and causes fewer infections, and the symptoms are usually milder.9
3. Manage Suspected Measles in Primary Care by Isolating Patients and Notifying the Local Health Protection Team
If the patient is systemically unwell enough to need a referral to secondary care, healthcare professionals must make it clear that they suspect measles, as there may be arrangements in place to keep them separate from other patients.11 Similarly, if someone with suspected measles visits the practice, it is necessary to find them somewhere other than the waiting room to wait.12
Public Health Management
Clinicians are required to notify their local health protection team about any suspected case of measles, which will arrange to take swabs.12 Vulnerable contacts will be assessed for possible post-exposure prophylaxis, so if clinicians happen to know that there is a pregnant woman or an immunocompromised person in the household, this is useful information to pass on.12 Healthcare professionals can find their local health protection team using this search tool.13
Disease Management in Primary Care
Management of measles in primary care is entirely symptomatic, and includes rest, adequate fluid intake, and use of paracetamol and ibuprofen for symptom relief.11 Aspirin should be avoided in children aged younger than 16 years.11 The infected person should stay away from school, nursery, or work for at least 4 days after the initial development of the rash, and should avoid contact with infants and those who are not fully immunised, pregnant, or immunosuppressed.11 If there are any signs of complications, medical attention should be sought; these may include shortness of breath, a temperature that cannot be controlled, seizures, drowsiness or an alteration in level of consciousness.11
4. Understand Current Guidance on Reimbursement for Childhood Vaccinations
The 2021/22 GP contract removed exception reporting for vaccinations while maintaining an 87% threshold for Quality and Outcomes Framework points for MMR and introducing a potential clawback of item of service payments for practices that do not maintain an 80% uptake.14 This means that, if parents cannot be persuaded to vaccinate their children, practices will lose out financially through no fault of their own, with concerns raised that some will lose tens of thousands of pounds.14 At the time of writing, calls for payment at lower tiers or the re-introduction of exception reporting for those who refuse have not yet been heeded. This is likely to entrench health inequalities, with practices in areas of high vaccine refusal and a more mobile population (often areas of deprivation) feeling that they cannot afford to spend time trying to increase uptake, as that time will not be resourced.14
5. Be Aware of Myths Linking Vaccination to Autism
In 1998, Andrew Wakefield and colleagues published a paper in The Lancet suggesting that the MMR vaccination was associated with behavioural regression and autism.15 Although the article was disputed almost immediately and later retracted, the damage was done, and MMR uptake rates started to fall.15 It was later revealed that Wakefield had significant conflicts of interest and stood to gain financially from the increased use of single vaccines.16 This is discussed in much more detail in a previous Guidelines in Practice article on vaccination myth-busting.16
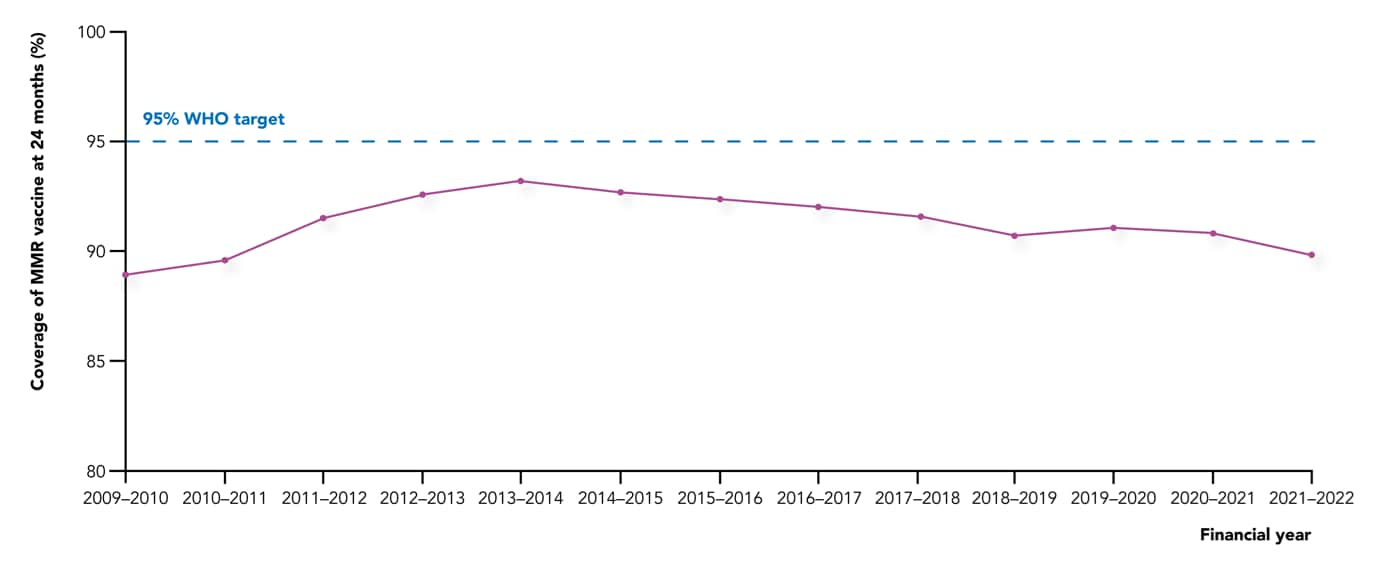
The UK has never met the World Health Organization (WHO) target of 95% coverage with two doses of the MMR.17,18 This is the level considered necessary to achieve and maintain measles elimination.17 The UK came close in 1994, with 92% uptake of the vaccine but, after publication of the Wakefield paper, uptake fell to around 80%.17 It improved in the 2000s and early 2010s and, by 2017, the WHO declared that the UK had eliminated measles, with first-dose coverage reaching 95%.17 However, uptake fell steadily from then, declining more sharply during the COVID-19 pandemic (see Figure 319); in England, it currently stands at 89.5% for the first dose and 85.6% for the second dose, with lower figures in London (82.5% for the first dose at 2 years of age, and 74.1% for both doses at 5 years of age).17 Certain populations have particularly low uptake, and these are being targeted with education campaigns, often involving religious leaders.17,20
Figure 3: MMR Vaccine Coverage at Age 24 Months in the UK, 2009–202219
6. Recognise that Vaccine Hesitancy is still Prevalent
Vaccine hesitancy is significantly related to organised campaigns on social media, including misinformation campaigns that start from outside the UK, particularly from Russia.21 Some studies have indicated a link between the likelihood of receiving the COVID-19 vaccine and the quality of the news articles that an individual liked or shared on X (formerly known as Twitter).22 There have been calls for social media companies to be more proactive in taking down antivaccination content in an attempt to combat the current situation,23 in which some people may be in an online ‘echo chamber’ of people with similar antivaccination views, and are therefore not exposed to accurate information. Some social media platforms have announced that they will reject antivaccination advertisements, and that searches on measles or vaccine safety will now only show links to reputable public health organisations.23
7. Tackle Vaccine Hesitancy with Evidence when Possible
When trying to advise a parent who doesn’t want their child to be vaccinated against measles, it is helpful to know if they are vaccine hesitant or a ‘vaccine denier’. The WHO defines vaccine deniers as ‘people who have a very negative attitude towards vaccination and are not open to a change of mind no matter the scientific evidence’.24 Vaccine deniers are a small subgroup of the wider vaccine hesitancy continuum, and any attempt to change their views will likely fail. The WHO advises that, in a discussion with a vaccine denier, the target audience is the public who are listening to the debate, and the aim is to strengthen their resilience against antivaccine rhetoric.24 In the context of primary care, this target audience may be the other parent or any other adult who is in the room, but if you speak to a true vaccine denier alone, then you are probably wasting your time. Those who are vaccine hesitant, however, may be persuaded, so it is important that clinicians have the facts at their fingertips.
8. Signpost Patients to Data on the Safety of Vaccination
The measles chapter of the UKHSA Green book has a list of useful points that could form the basis of a discussion with a parent who is still worried about autism, including:25
children who have had the MMR vaccine do not have an increased risk of autism compared with unvaccinated children
symptoms of autism are not clustered around the period after the vaccination
when Japan discontinued the MMR vaccine in 1993, the incidence of autism continued to rise
there is no correlation between autism rates and vaccine coverage
no vaccine virus can be detected in children with autism.
9. Appreciate the Legal Situation if Two Parents Disagree
Children are often brought for vaccination by one parent, and practices do not generally contact the other parent to ask for their permission. However, the situation is different if it is known that someone with parental responsibility does not want the child to be vaccinated. In that case, even though vaccination is in the best interest of the child, practices cannot vaccinate unless a court order has been obtained.26,27
Summary
Measles is a potentially fatal disease that is easily preventable—it is tragic that antivaccination sentiment may contribute to a large outbreak and potentially some deaths. Clinicians need to be able to recognise measles, treat the patient in front of them, inform public health, and encourage vaccination to prevent future outbreaks.
Yesterday I got a Google News alert: “Measles.” Yes, measles. In the 21st century. At the height of winter. (Measles typically spreads in spring.) What’s going on?
Two active and unrelated measles outbreaks among unvaccinated people: Philadelphia and New Jersey
A Delaware children’s hospital on alert after an unvaccinated patient exposed 30 others
Two DC airports on alert for an unvaccinated, infected international traveler
An explosion of measles cases in the U.K. in the past month (255 cases)
This sure seems like a lot. Is measles increasing?
A measles case here or there is not abnormal. We see them every year. Cases typically come from international travelers, but sometimes locally acquired outbreaks emerge among unvaccinated pockets.
As you may also notice above, measles has epidemic cycles. It flares up every four to five years—2008, 2011, and 2019. We can also see this pattern during the pre-vaccine era (see below).
It is exactly 5 years since the last flare-up, which suggests this may be a bad year. Of course, the pandemic could throw off patterns, but we aren’t off to a great start.
What is (and is not) a way forward?
Measles is preventable. And, in the PA outbreak, one unvaccinated child went to daycare while infected, defying isolation.
People are disappointed and shocked that fellow parents wouldn’t vaccinate their children. People are angry that their loved ones may get exposed as a result, especially since babies under 12 months old cannot be vaccinated.
I share a lot of the frustration. But I remember what Dr. Sandro Galea said during the pandemic, “We cannot finger-wag our way to a healthier world.”
Is there collective amnesia? Let’s fix it.As generations age, the memory of mid-20th-century diseases like measles fade. This is a blessing and a curse. Some don’t know why this disease is bad or if this vaccine is safe. This is understandable. The onus is on public health—we need to equip trusted messengers to start communicating, as measles is:
The most contagious disease, with an infected person infecting an average of 12-18 others (assuming no immunity in the population). In some cases, a single person has infected hundreds of people.
It’s not “just a fever or a rash.” While most people who get measles will recover, it can harm the body in every way possible. Measles can wipe out a huge fraction of immune memory to other diseases, causing an increase in all-cause deaths.
The risks of infection far outweigh the risks of the vaccine, as shown beautifully by the New York Times below.
(Source: New York Times)
Is this a consequence of individualism? Let’s engage. One of the biggest challenges is the rise of individualism, as it goes against public health’s DNA: a collective response for the good of the population. We desperately need to engage with people who find individualism increasingly important. Develop interventions with them.
Is this due to a recent and dramatic decline in trust? Let’s do something about it. Mistakes were made during the pandemic. Misinformation is supercharged by social media. Bad actors, like the disinformation dozen, drive the majority of anti-vax content. Politics are further dividing individual health. Many people talk about these challenges (it’s even the theme of Davos this week!), but I’m getting increasingly frustrated with inaction.
Bottom line
Unfortunately, measles is off to a great start in 2024. We expect trends to increase.
We need to heed the underlying warning. A laissez-faire approach to public health, on both sides, will not work. Harrowing stories like Roald Dahl’s below will creep into the 21st century. We can do better.
Measles is spreading across Europe wherever immunisation coverage has dropped, the World Health Organization is warning.
The largest outbreaks are being seen in Italy and Romania.
In the first month of this year, Italy reported more than 200 cases. Romania has reported more than 3,400 cases and 17 deaths since January 2016.
Measles is highly contagious. Travel patterns mean no person or country is beyond its reach, says the WHO.
For good protection, it’s recommended that at least 95% of the population is vaccinated against the disease.
But many countries are struggling to achieve that.
Most of the measles cases have been found in countries where immunisation has dipped below this threshold and the infection is endemic – France, Germany, Italy, Poland, Romania, Switzerland and Ukraine.
Preliminary information for February suggests that the number of new infections is rising sharply, says the WHO.
WHO regional director for Europe Dr Zsuzsanna Jakab said: “I urge all endemic countries to take urgent measures to stop transmission of measles within their borders, and all countries that have already achieved this to keep up their guard and sustain high immunisation coverage.”
The European Centre for Disease Prevention and Control says that between 1 February 2016 and 31 January 2017 the UK reported 575 cases of measles.
The MMR (measles, mumps and rubella) vaccine is available on the NHS for babies and pre-school children.
Lagging immunisation
Robb Butler, of the WHO Regional Office for Europe, says there are a number of reasons why vaccination coverage has waned in some regions.
“In some countries, like the Ukraine, there have been supply and procurement issues.”
Then there’s vaccine hesitancy. Some people are fearful of vaccination, while others are complacent or find it an inconvenience, he says.
In France, for example, people need to make an appointment with their doctor to get a prescription, go to the pharmacy to collect the vaccine and then rebook with their doctor to have the jab administered.
“We need to get to the point where we appreciate that people have busy lives and competing priorities.”
Dr Mary Ramsay, Head of Immunisation at Public Health England, said: “England’s uptake of MMR vaccine by five years of age has reached the WHO’s target of 95%.
“In the last year, the measles cases confirmed in England have mainly been in older adolescents and young adults with many linked to music festivals and other large public events. Individuals of any age who have not received two doses of the MMR vaccine, or those who are unsure, should speak to their GP – it’s never too late to have the vaccine and measles can still be serious in adults. We are continuing to invest in programmes which encourage uptake of the vaccine to ultimately consign measles to the history books.”
Measles
Unvaccinated young children are at highest risk of measles and its complications, including death
Measles is spread by direct contact and through the air by coughs and sneezes
The virus remains active and contagious on infected surfaces for up to two hours
The first signs of infection are usually a high fever and cold-like symptoms, such as a runny nose
You may notice small white spots on the inside of the cheeks as well
After several days, a rash develops, usually on the face and neck first and then spreading to the body and limbs
An infected person can pass on the virus to others from four days prior to developing the skin rash to four days after the rash erupts
There is no treatment, but two doses of vaccine can prevent infection in the first place
I am currently reading the Federal Register article on the CDC’s proposed measures for “Control of Communicable Diseases.”
This is REAL.
If you remember the movie, “Contagion,” the CDC’s power grab reads like the script.
Detainment, imprisonment (indefinite), forced medical examinations, forced treatment, forced vaccination…
for MEASLES.
The CDC is lumping MEASLES in with Ebola.
If you have seen the outrage over Colin Kaepernick refusing to stand during the national anthem, and you don’t think he has reason to protest the actions of the United States, you need to read this article. The United States government is rapidly surpassing Hitler in their oppressive and illegal use of force against citizens who refuse to inject themselves or their children with experimental vaccines that have never been tested for carcinogenic or mutagenic effects, or for impairment of fertility.
Our government is so financially invested in vaccines that they are passing rules and regulations to take away your BASIC HUMAN RIGHTS to say NO to forced vaccination – for what is a mild, childhood infection, and for which the death rate in the United States had decreased nearly 100% BEFORE the vaccine was even invented.
If this regulation passes, entire cities could be under forced quarantine and citizens lined up and vaccinated under government force – whenever there is a case of suspected measles identified. That means this will be happening routinely – and especially at the beginning of every school year when recently vaccinated children are spreading measles to their classmates.
Melissa Sfura has put out a very important ACTION ALERT – which I fully support and hope you will attend to.
This is NOT A JOKE.
If you value your liberty and the principles on which the United States was founded, you had better get active NOW and work to protect them.
Vaccine exemption is associated with an increased risk of measles and pertussis, as evidenced by a recent US study.
To assess if vaccine refusal, delay or exemption was linked to outbreaks of measles and pertussis in the US, researchers looked for studies published between January 2000 (post-measles elimination era) and November 2015 for the measles cohort and from January 1977 to November 2015 for the pertussis cohort. [JAMA 2016;315:1149-1158]
There were 18 published studies on measles comprising 1,416 cases in individuals ranging from age 2 weeks to 84 years (178 cases in individuals <12 months). Of these, 56.8 percent (n=804) occurred in individuals with no history of measles vaccination, while 14.1 percent (n=199) occurred in vaccinated individuals. Of 970 cases with detailed vaccination information, 574 cases were in individuals who were age-eligible for the measles vaccine yet did not receive one, with 70.6 percent (n=405) of them unvaccinated due to nonmedical reasons.
Among 32 pertussis outbreaks comprising 10,609 cases in individuals aged between 10 days and 87 years, 24-45 percent of the five largest outbreaks (Arizona in 1988, California in 2010 and 2014, Washington and Oregon in 2012) involved unvaccinated individuals. In eight of 12 reports with data on reasons for non- or undervaccination (fewer than recommended doses), 59 to 93 percent were unvaccinated due to vaccine refusal.
There were reports of pertussis epidemics in communities with high vaccination rates, an occurrence study authors attributed to a decline in immunity. However, there was still an association between vaccine refusal and pertussis risk in some communities, they said.
The authors believe that enforcement of vaccine mandates, be it at a school- or state-level, as well as increasing the difficulty to acquire exemption are crucial to raising vaccination rates in the community. However, they also highlighted the importance of acknowledging reasons for vaccine hesitancy among parents, such as perception on risk of vaccine-preventable diseases and safety of routine vaccination.
This study builds up on previous data that showed an association between vaccine refusal and risk of varicella, pneumococcal disease, measles, and pertussis.
Reported cases of measles worldwide declined from 853,480 to 226,722 over the same time.
“Start Quote
There is much more work to be done as more than 330 deaths (mainly among children) still occur daily from measles ”
Karen MahThe Measles and Rubella Initiative
Currently, 84% of the world’s infants receive the first dose of measles vaccine before their first birthday, according to the WHO.
It says that 145 countries have also introduced a routine second dose of measles vaccine to ensure immunity and prevent outbreaks.
Mass campaigns against measles in 2012 resulted in a further 145 million children being vaccinated against the disease, taking the total number of vaccinated children to more than one billion since 2000.
Threat continues
However, there are still concerns that despite this good news, measles remains a worldwide threat.
The regions of Africa, south-east Asia and Europe all experienced large outbreaks in 2012, and the Americas region had to deal with many imported measles cases.
The Democratic Republic of Congo saw the largest measles outbreak of 2012, with 72,029 reported cases. There were around 18,000 cases in India and 12,000 in Ukraine, while the UK experienced just over 2,000 measles cases.
The WHO says the Africa, Eastern Mediterranean and European regions are not likely to meet their measles elimination targets on time.
Without improved immunisation coverage, outbreaks will continue to occur, it says.
Karen Mah, a spokeswoman for The Measles and Rubella Initiative, a global partnership led by the WHO and UNICEF among others, said there were still too many children dying.
“While estimated measles deaths have dropped significantly since 2000, there is much more work to be done as more than 330 deaths (mainly among children) still occur daily from measles.
“We need to move beyond an 84% global routine immunisation coverage. It’s also vital that parents are fully aware of the benefits of immunisation and the risks associated with not vaccinating children,” she added.
The Measles and Rubella Initiative wants to reduce measles deaths by 95% by 2015 and get rid of measles and rubella in at least five regions of the world by 2020.
In 2012, vaccination coverage among U.S. children aged 19 to 35 months remained near or above theHealthy People 2020targets of 90% for polio, hepatitis B, varicella, and measles, mumps, and rubella, according to an analysis of National Immunization Survey data reported inMMWR.
Coverage with four or more doses of diphtheria, tetanus, and pertussis vaccine, four or more doses of pneumococcal conjugate vaccine, and the full series ofHaemophilus influenzaetype B vaccine were below the 90% goal but remained relatively stable and high (over 80%). Less than 1% of children did not receive any vaccines. Those living in poverty were more likely to be unvaccinated.
A separate article inMMWRdetails 159 cases of measles reported in 16 states in 2013. Most cases (82%) were in unvaccinated individuals, and nearly all were import-associated. Eight outbreaks in communities with unvaccinated persons accounted for more than three quarters of cases.



.jpg)