Summary: Fibroblast growth factor receptor inhibitors, commonly used in cancer treatment, could effectively reduce neurological symptoms in patients with post-treatment Lyme disease syndrome. The study shows these inhibitors can decrease inflammation and cell death in brain and nerve tissues affected by Lyme disease.
This discovery paves the way for potential treatments aimed at the persistent neuroinflammation seen in some patients after standard antibiotic therapy. With promising initial results, further research is essential to move these findings from the lab to clinical applications.
Key Facts:
Lyme disease can cause persistent neurological symptoms such as memory loss and fatigue, known as post-treatment Lyme disease syndrome, even after antibiotics.
The study found that targeting FGFR pathways with specific inhibitors can significantly reduce inflammation and neuronal damage in tissue samples infected with Lyme disease bacteria.
The research, supported by the Bay Area Lyme Foundation and resources from the Tulane National Primate Research Center, marks a critical step toward developing new interventions for chronic Lyme disease complications.
Source: Tulane University
Tulane University researchers have identified a promising new approach to treating persistent neurological symptoms associated with Lyme disease, offering hope to patients who suffer from long-term effects of the bacterial infection, even after antibiotic treatment.
Their results were published in Frontiers in Immunology.
Lyme disease, caused by the bacterium Borrelia burgdorferi and transmitted through tick bites, can lead to a range of symptoms, including those affecting the central and peripheral nervous systems.
While antibiotics can effectively clear the infection in most cases, a subset of patients continues to experience symptoms such as memory loss, fatigue, and pain—a condition often referred to as post-treatment Lyme disease syndrome.
Principal investigator Geetha Parthasarathy, PhD, an assistant professor of microbiology and immunology at the Tulane National Primate Research Center, has discovered that fibroblast growth factor receptor inhibitors, a type of drug previously studied in the context of cancer, can significantly reduce inflammation and cell death in brain and nerve tissue samples infected with Borrelia burgdorferi.
This discovery suggests that targeting FGFR pathways may offer an exciting new therapeutic approach to addressing persistent neuroinflammation in patients with post-treatment Lyme disease syndrome.
“Our findings open the door to new research approaches that can help us support patients suffering from the lasting effects of Lyme disease,” Parthasarathy said.
“By focusing on the underlying inflammation that contributes to these symptoms, we hope to develop treatments that can improve the quality of life for those affected by this debilitating condition.”
Researchers treated nerve tissue with live or inactivated Borrelia burgdorferi, followed by an application of FGFR inhibitors. Study results revealed a significant reduction in both inflammatory markers and of cell death.
While further research is needed to translate these findings into clinical treatments, the study represents an important step forward in understanding and potentially managing the complex aftermath of Lyme disease.
Funding: This study was funded by the Bay Area Lyme Foundation and supported with resources from the Tulane National Primate Research Center base grant of the National Institutes of Health, P51 OD011104.
Abstract
Fibroblast growth factor receptor inhibitors mitigate the neuropathogenicity of Borrelia burgdorferi or its remnants ex vivo
In previous studies, we showed that fibroblast growth factor receptors (FGFRs) contribute to inflammatory mediator output from primary rhesus microglia in response to live Borrelia burgdorferi.
We also demonstrated that non-viable B. burgdorferi can be as pathogenic as live bacteria, if not more so, in both CNS and PNS tissues. In this study we assessed the effect of live and non-viable B. burgdorferi in inducing FGFR expression from rhesus frontal cortex (FC) and dorsal root ganglion (DRG) tissue explants as well as their neuronal/astrocyte localization.
Specific FGFR inhibitors were also tested for their ability to attenuate inflammatory output and apoptosis in response to either live or non-viable organisms. Results show that in the FC, FGFR2 was the most abundantly expressed receptor followed by FGFR3 and FGFR1.
Non-viable B. burgdorferi significantly upregulated FGFR3 more often than live bacteria, while the latter had a similar effect on FGFR1, although both treatments did affect the expressions of both receptors.
FGFR2 was the least modulated in the FC tissues by the two treatments. FGFR1 expression was more prevalent in astrocytes while FGFR2 and FGFR3 showed higher expression in neurons.
In the DRG, all three receptor expressions were also seen, but could not be distinguished from medium controls by immunofluorescence. Inhibition of FGFR1 by PD166866 downregulated both inflammation and apoptosis in both FC and DRG in response to either treatment in all the tissues tested.
Inhibition of FGFR1-3 by AZD4547 similarly downregulated both inflammation and apoptosis in both FC and DRG in response to live bacteria, while with sonicated remnants, this effect was seen in one of the two FC tissues and 2 of 3 DRG tissues tested.
CCL2 and IL-6 were the most downregulated mediators in the FC, while in the DRG it was CXCL8 and IL-6 in response to FGFR inhibition. Downregulation of at least two of these three mediators was observed to downregulate apoptosis levels in general.
We show here that FGFR inhibition can be an effective anti-inflammatory treatment in antibiotic refractive neurological Lyme. Alternatively, two biologics may be needed to effectively curb neuroinflammation and pathology in the CNS and PNS
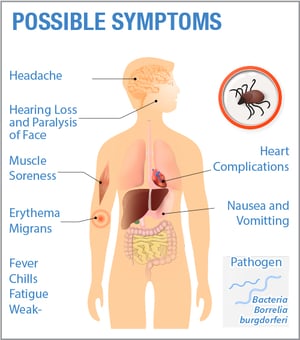
Lyme disease symptoms are wide-ranging, with more than a hundred different symptoms recorded. Symptoms can also change over time, as the bacteria spreads throughout the body. To make things more confusing, Lyme disease symptoms will also vary from patient-to-patient.
Lyme disease can mimic hundreds of other conditions since its symptoms mirror many medical problems such as multiple sclerosis, arthritis, chronic fatigue syndrome or lupus, and is sometimes known as “The Great Imitator” because of this. Click here for a more complete list of possible symptoms.
Symptoms can play a key role in diagnosing Lyme disease. Due to the lack of an accurate diagnostic test, many patients are diagnosed based on a combination symptoms and diagnostic testing. This makes it extremely important for patients to keep track of all the symptoms they experience, to share with their healthcare provider.
When do Lyme disease symptoms appear? Learn about the Stages of Lyme disease:
Lyme disease symptoms can vary based on stage of the disease (early, late, post-treatment, or chronic) and if other tick-borne infections are present and can change over time.
Symptoms in acute Lyme disease
Acute Lyme disease (aka: early localized LD) occurs days to weeks after the initial tick bite and infection, in which the bacteria have not yet spread from the site of infection in the skin.
The most common symptoms in acute (aka: early localized) Lyme disease are the ones people are most familiar with, because they are symptoms often shared with other illnesses; however, it’s important to recognize that they could indicate Lyme, and you should see a Lyme-treating physician right away.
Erythema migrans (AIR-ih-THEEM-ah MY-grans) rash or EM rash. This rash begins at the site of the tick bite about a week after the bite, and gradually expands. Note: The center of the rash may clear, giving the rash the appearance of a “bulls-eye.” Rashes may take on many different shapes and not all rashes will have a bulls-eye appearance. There can be multiple rashes on the body. While a rash is characteristic of Lyme disease, many people will not develop a rash at all.
Fever
Fatigue
Aches
Chills
Swollen lymph nodes
Other flu-like symptoms
Symptoms in early disseminated Lyme disease
Early disseminated Lyme disease occurs days to months after infection, in which the bacteria have begun to spread. There is a wide range of possible symptoms at this stage, including:
Severe headaches and neck stiffness
Arthritis, especially in the knees or other large joints
Muscle aches and pains
Heart palpitations or shortness of breath (Lyme carditis)
Facial paralysis on one or both sides (also known as Bell’s palsy)
Numbness or tingling in the hands or feet
Extreme fatigue
Symptoms in late stage Lyme disease
Late stage Lyme disease, which can include post-treatment, chronic, and neurological, occurs months to years after infection, in which the bacteria have spread throughout the body.
The symptoms of late disseminated disease are similar to those of early disseminated disease, but may be more extensive, more severe, and longer lasting. Late symptoms may also include:
neurologic features including vertigo or dizziness,
difficulty sleeping
mental fogginess
difficulty following conversations
difficulty processing information
Some common questions …
When should you see a doctor for Lyme disease?
As soon as you have visual proof of a tick bite (remember to save the tick and send in for testing) or you suspect Lyme disease based on the symptoms listed above, consult a Lyme treating physician. The sooner treatment is started after a tick bite, the more effective it is.
Do symptoms of Lyme disease come and go? Is it OK to stop treatment if symptoms disappear?
No. The absence of symptoms does not mean the disease is gone. It’s important to consult with your doctor even if symptoms disappear.
How long do Lyme disease symptoms last? Do you ever get rid of Lyme disease? What if symptoms persist after treatment?
It’s important to remember that up to 20% of those diagnosed and treated early will continue to have symptoms. This means that even if you have undergone treatment, you could still have Lyme disease. Keep track of all symptoms and share with your healthcare provider.
It remains unclear why some patients, despite antibiotic treatment, continue to experience symptoms of Lyme disease. Possible explanations include persistence of antibiotic-tolerant bacteria, autoimmunity triggered by prior infection with the Lyme bacteria, or perhaps co-infection with other tick-borne pathogens. These mechanisms of chronic disease are not mutually exclusive.
What if you suspect Lyme disease and have never been diagnosed or treated?
If you suspect Lyme disease, even though you don’t recall a tick bite or a rash, it’s important to consult with a Lyme physician right away. Untreated, Lyme disease can spread to other parts of your body for several months to years after infection, causing arthritis and nervous system problems.
Lyme disease is an illness caused by the bacterium Borrelia burgdorferi. These bacteria are carried by the black-legged tick, also known as the deer tick (pictured). When an infected tick bites you, it can transfer bacteria under the skin, leading to infection. If diagnosed and treated early, many patients recover. However, if not diagnosed or treated early, Lyme disease can develop into a chronic illness that leads to long-term, serious health problems and reduced quality of life. In rare cases, Lyme disease can result in death.
About Lyme Disease
While Lyme disease was named for the town in Connecticut where it was first identified, Lyme disease-carrying ticks are found throughout the United States (US). The highest concentrations of black-legged ticks are found in the northeast, mid-Atlantic, and upper Midwest regions of the US. In recent years, confirmed cases of Lyme disease have been reported in every state. Most recent estimates are of 476,000 new cases of Lyme in the US every year. Scientists estimate that two million people could suffer from post-treatment Lyme disease at the end of 2020. Lyme disease has also been found in 80 countries.
How Do You Get Lyme Disease?
Lyme disease is transmitted through the bite of an infected black-legged tick. Ticks look for hosts to feed–hosts can include pets, deer, mice, birds, squirrels, some reptiles, and yes, people.
The length of time for a tick to transmit disease can vary based on the type of tick and the stage of the tick (nymph vs. adult, for example). Experimental studies have shown that the Powassan virus, transmitted by black-legged ticks, can be transmitted within 15 minutes of attachment. Research shows that Lyme-causing bacteria takes more than 24 hours to transmit from tick to host, but there are many debates and caveats on exact transmission time. Most importantly, it’s important to remove an attached tick as soon as it’s found, and to remove it properly to avoid the spread of pathogens.
Who Is Most At Risk for Lyme Disease?
Children aged 3 to 14 are at the greatest risk for contracting Lyme disease, due in part to being more active outdoors, with more than 200 cases per day. The next age group most at risk is people over 50, who are also more involved in outdoor leisure activities like gardening, hiking, or playing golf. People who work outdoors for a living, including landscapers, utility workers, and farmers have an occupational risk for a tick bite. Pets who go outdoors, like dogs and cats, may bring ticks into the house and should be checked upon entering the home. Think of your pet as a “tick taxi.”
Ticks are not just a suburban problem; they are everywhere including urban areas and cities. Many people get bitten by a tick in their own yards and local parks. While you are most likely to be bitten by a tick during the warmer months, ticks can be active year-round and are active at any temperature above 34 degrees Fahrenheit.
How is Lyme Disease Diagnosed?
If you developed a bulls-eye rash due a tick bite, you have Lyme disease. For patients you don’t develop or recall a rash, the disease is typically diagnosed by a combination of clinical diagnostics and blood work. However, given the high-rate of inaccuracy with current Lyme disease diagnostic tests, about 50%, it’s crucial to consult with a Lyme-treating healthcare provider that can evaluate all your symptoms and medical history to make an accurate diagnosis. Click here to learn more about how to diagnose Lyme disease. Click here to learn more about the symptoms of Lyme disease.
Cases of Lyme Disease Are on the Rise
It’s estimated that there are 476,000 new cases of Lyme disease in the U.S. each year. There is a near 25x increase of annually reported cases since 1982. All tick-borne disease cases have more than doubled in the last 13 years.
Cases of Lyme continues to outpace other infectious diseases in the U.S. by significant margins. In fact, there are 618% more new cases of Lyme disease in the U.S. than Hepatitis B, Hepatitis C, and West Nile Virus combined. This doesn’t even take into account the growing number of other tick-borne infections.
Lyme disease can deplete your vitamin D levels–which ironically, are essential in your recovery. Read about the positive effects of Vitamin D and techniques to increase it.
While kayaking recently, a friend noticed that I was getting a lot of sun on my face and asked if I wanted a hat. “No thanks,” I replied. “I’m wearing sunscreen, and I want to soak up as much vitamin D as I can.”
There were summers during my convalescence from tick-borne illness when I couldn’t be in the sun at all, due to the phototoxicity of the medication I was on. Doxycycline, the most common antibiotic used to treat Lyme disease, can cause you to be very sensitive to the sun. When I was on doxycycline or other antibiotics in the same family, my face would feel like it was on fire if I was exposed for more than five minutes. I spent summers bundled in protective shirts, under hats and umbrellas in the shade.
A former camp counselor who spent every day in the sun before I got sick, summers in the shade were not my style. Now that I am in remission, I want to (carefully) get as much sun as possible, making up for lost time and summer glow. But it’s not just sun-kissed cheeks that I’m after. I literally am trying to soak up vitamin D, provided by the sun, because I know that Lyme disease can cause a deficiency in that vitamin.
The Lyme disease bacteria, Borrelia burgdorferi, directly reduces vitamin D receptor expression in immune cells. Low vitamin D can be involved in immune dysfunction and autoimmunity, so Lyme patients who are already struggling with compromised immune systems may be further compromised by a vitamin deficiency. As Clinical Nutritionist Lindsay Christensen, MS, CNS, LDN, CKNS explains in her blog post “Lyme Disease Nutrition Tips for Optimal Immune Function,” Vitamin D3 is “essential for healthy immune function. Within the innate immune system, vitamin D3 supports the production of cathelicidin, an antimicrobial peptide (protein) that protects the body against bacteria, viruses, and fungi. Vitamin D3 also regulates dendritic cells, which are immune cells that ‘bridge the gap’ between the innate and adaptive immune system branches and may help defend the body against Borrelia.”
In other words, the very vitamin that can be depleted by Lyme disease is also necessary to help fight it.
So what should Lyme patients do? First, make sure your doctor is monitoring your vitamin D levels. A blood test can tell you whether you have a deficiency. If you do, sunshine, and certain foods like egg yolks and fatty cold-water fish, can help you get vitamin D. You also may need to supplement with vitamin D3 to maintain what Christensen describes as “an optimal vitamin D3 level of 40-60 ng/mL, which is tighter than the 30-60 ng/mL range suggested by most labs.”
Testing vitamin D levels can also help a Lyme Literate Medical Doctor (LLMD) determine if you have Lyme disease, if you have symptoms but have not yet been diagnosed. Though not a definitive diagnostic marker (low vitamin D is also seen in other conditions like multiple sclerosis), low vitamin D can be a tip-off that Lyme disease could be the cause of your symptoms.
Vitamin D is not the only vitamin that can be affected by Lyme disease, or that you may need more of to help fight tick-borne illness. Many Lyme patients have a vitamin B12 deficiency. Others have anemia or low ferretin. It’s important that your doctor do regular blood work to check for any nutritional deficiencies, and then you can determine together how to best supplement them, to support your overall healing. In the meanwhile, as long as you’re not on a phototoxic drug, sticking your face in the sun can’t hurt!
Trends in some regions are clear, but insect biology, climate quirks, and public health preparedness will determine whether outbreaks occur.
Late last November, a young man walked into Renee Salas’ emergency room with a circular rash spreading across his leg. Salas, an attending physician at Massachusetts General Hospital in Boston, treated him for possible Lyme disease from a tick bite—a diagnosis that bloodwork later confirmed.
Field crews at the Connecticut Agricultural Experiment Station track the diversity and abundance of disease-carrying mosquitoes using traps baited with a yeast–hay infusion mixed with water. They also use traps that attract the mosquitoes using dry ice and light. Image credit: Connecticut Agricultural Experiment Station.
At the start of her career in the early 2000s, Salas would never have suspected Lyme so late in the year. Ticks used to be a summer problem. But since the 1990s, a warmer climate has shortened winters, extending Lyme’s duration and expanding its reach throughout New England. Incidence of the infection has nearly doubled. “I think about it all times of year now,” Salas says. “I have to consider Lyme for every rash.”
Lyme isn’t the only disease whose range and seasonality is shifting, at least in part, as a result of climate change. Although the impact will likely vary based on a variety of factors, some clear trends are emerging. High latitudes and altitudes seem poised for the most dramatic spikes in disease risk. Warmer and wetter conditions in these places have started to lure ticks and mosquitoes up mountainsides and across borders into areas once too cold and dry to support them.
Some diseases are already shifting. The 2021 Lancet Countdown report, published in October, highlighted a 39% increase in the number of months suitable for malaria transmission in some highland areas of the world since the late 1950s (1). The area of coastline suitable for Vibrio bacteria, which can cause gastroenteritis, severe wound infections, and sepsis, also increased from 2011 to 2021 in several high-latitude regions according to the report, including the Baltics, the Atlantic Northeast, and the Pacific Northwest.
But while northern climes are becoming more susceptible to disease transmission, communities aren’t necessarily doomed to experience bad outbreaks, says biochemist and biomedical scientist Marina Romanello, the research director of the Lancet report. “The risk depends on the public health measures,” she says, among other factors. Public health measures can include surveillance of known diseases, as well as emergency preparedness and response plans in the event of a localized outbreak, and other measures. Even so, as environments become more and more inviting for disease transmission, “managing the risk gets more and more difficult.”
Moving Up Mountains
It’s no wonder that disease ranges are shifting; their geographic boundaries have always been climate-sensitive, says theoretical and computational ecologist Mercedes Pascual at the University of Chicago in Illinois. Tick vectors that spread Lyme disease and mosquito vectors that spread dengue, malaria, chikungunya, Zika, West Nile, and a host of other diseases are cold-blooded arthropods with small bodies, meaning that their internal temperatures track environmental temperatures quickly, says disease ecologist Courtney Murdock at Cornell University in Ithaca, NY. Where the vectors can go in many cases determines where the diseases can go. Many physiological traits—most importantly, how long vectors are alive, infectious, and biting—are limited or driven by temperature, as is the speed that a pathogen can develop and be transmitted from the host’s gut into a person’s bloodstream, Murdock says.
By the 1980s and ’90s, infectious disease outbreaks had already worsened in some places. But the link to climate change wasn’t conclusive. In 2014, Pascual coauthored one of the first studies to strongly suggest that warming at high altitudes in Ethiopia and Colombia had exacerbated malaria outbreaks since the 1970s (2). Historically, alpine mountain communities were too cold for the Anopheles mosquitoes that transmit the malaria parasite. But by the 1990s, case numbers had ballooned.
Many researchers suspected that drug resistance drove the rise in cases. But when Pascual and coauthors plotted the elevation and timing of each malaria case against yearly climate data, they found that outbreaks had marched up and down the mountains closely tracking year-to-year variations in temperature. Then, based on the tight correlation between temperature variation and outbreak size, the researchers went on to project that Ethiopia would experience an additional 410,000 malaria infections annually per 1 degree Celsius of warming. Extrapolating from the localized 2014 findings to the entirety of Ethiopia’s highlands, Pascual estimates that climate change has probably already contributed 5 to 6 million malaria cases to the country’s national burden since the 1970s (3).
Around 2010 or so, medical entomologist Philip Armstrong also noticed mosquitoes on the move in New England. Rather than shifting up mountainsides, though, Armstrong saw southerly mosquito species, native to the US Mid-Atlantic, turning up in states farther north than their historical ranges. Armstrong leads the long-term mosquito monitoring program at the Connecticut Agricultural Experiment Station in New Haven, where field crews have tracked the diversity, abundance, and diseases carried by the roughly 50 mosquito species in Connecticut since 1997, beginning with 37 trapping sites statewide. The network expanded to 87 in 2001, after West Nile arrived in North America, and now totals 108.
“The risk depends on the public health measures.”
—Marina Romanello
In the evenings from June to October, the crews hang light traps in trees, baited with dry ice, which evaporates tendrils of carbon dioxide to lure female mosquitos searching for a blood meal. The next morning, researchers collect mosquitoes, identify them, and separate them into vials by species and study site. Then they grind up the insects. Liquid from the mosquito mash is injected into mammal cell lines, and if the cells begin to die after a few days then the researchers test those mosquitoes for a variety of cell-killing viruses, including the common West Nile and Eastern Equine Encephalitis (EEE), as well as Zika and others.
Since 2003, the experiment station has detected three new mosquito species in Connecticut, all of them common in more southern states, and “clearly” moving north, Armstrong says—although he notes that studies have yet to prove that the species’ arrival was driven by warming. Three more Mid-Atlantic mosquito species, which were rare in New England 20 years ago, have become established and abundant, according to a 2020 report by Armstrong’s group based on data from the 87 trapping sites in operation since 2001 (4). Disease-carrying species are among the new arrivals, such as the little brown Culex erraticus, known carrier of West Nile and EEE in other, more southeastern, states. Although C. erraticus hasn’t yet been detected with either virus in Connecticut, “it’s certainly possible that these new species may affect the transmission [of] endemic viruses,” Armstrong notes, “We just haven’t seen it yet.”
Across the country, researchers project that the fungal disease Valley fever, primarily endemic to the US Southwest and dry regions of Central and South America, will climb north this century. Most US cases today are concentrated in Arizona’s major cities and in California’s Central Valley—places with the ideal semi-arid conditions to support the Coccidioides fungus. Residing on and just beneath the crusty desert topsoil, the fungus can infect human lungs, causing joint pain, flu-like symptoms, and meningitis. A 2019 study used state health department data, reporting cases of the disease across the Southwest and pairing them with climate projections under two possible warming scenarios to predict where Valley fever may turn up by 2035, 2065, and 2095. That work found that as semi-arid regions shift north, so too should outbreaks (5).
Under a scenario in which the world continues high levels of CO2 emissions, Valley fever cases will likely move out of the US Southwest and up to the Canadian border by 2095. Image credit: Morgan Gorris.
Thread-like Coccidioides grow sporadically across the landscape. A fraction of the diameter of a human hair, field mycologists can’t easily spot the fungi. So, the 2019 study relied on confirmed Valley fever case reports as a proxy. Lead author Morgan Gorris compared case numbers from health departments in California, Arizona, Nevada, New Mexico, and Utah between 2000 and 2015 with a map of climatic conditions across the Southwest. She found that counties with more than 10 Valley fever cases per 100,000 residents all had mean temperatures over 51.3 degrees Fahrenheit (10.7 Celsius) and received less than 600 millimeters of precipitation per year.
Today, counties meeting those climatic criteria are sprinkled throughout the Southwest and even up into the Central Plains of Colorado, Oklahoma, Nebraska, and Kansas—areas once thought to be too far north to be at risk for Valley fever. And the fungus may keep moving. In the same 2019 article, Gorris, a postdoctoral Earth system scientist at Los Alamos National Laboratory near Santa Fe, NM, examined moderate and severe future climate warming scenarios across the United States. She found that under the severe climate warming scenario, suitable conditions for the fungus could reach as far north as the US–Canadian border by the end of this century. It’s only been a few years since Gorris’ article came out, and it remains too soon to see a huge rise in cases, says climate scientist Andrew Comrie at the University of Arizona in Tucson. He suspects that the fungus is already quietly trekking north, as desert-like conditions spread up the Mountain West. But dry expanses of Nevada, New Mexico, Utah, and Colorado are so sparsely populated that any range shift will likely go unnoticed, Comrie notes, until an outbreak hits a major city, such as Salt Lake City or Las Vegas, north of the fungus’ current range.
Concerning Curves
Although many studies make projections about one or two diseases over relatively small geographic areas, one research group tried to tease apart global patterns of climate impacts on thousands of diseases (6). Jeremy Cohen, a postdoctoral wildlife ecologist at Yale University in New Haven, CT, used a database of more than 2,000 combinations of host and parasite species from more than 10,000 field surveys of wildlife disease prevalence around the world. He used statistical models to predict how a number of different factors, including short- and long-term temperatures at survey sites, as well as various host and parasite traits, could simultaneously affect the disease prevalence in wildlife.
It’s well known that local weather, especially temperature, influences the prevalence of disease at a given survey site. But would, say, five degrees of warming have the same consequences for a disease in a high-latitude boreal forest as it would in a low-latitude tropical one? Or, Cohen wondered, would the regional climates of those places modulate the relationship between temperature and disease in each location? “There’s been an assumption that the effects of temperature on disease are relatively consistent,” he says.
Cohen’s models suggest that climate can be a major factor. In cool climates, such as high latitudes and elevations, Cohen’s models predict that there may be “pretty dramatic increases in disease risk under climate change.” Temperate areas, on the other hand, may see only a muted increase in risk, and some tropical areas might actually see a decrease in risk. One reason: Warming in already-hot places could exceed the temperature maxima for parasites to survive and function, Cohen says (7, 8).
The risk of mosquito-borne diseases could also decline in the hottest parts of the tropics, Murdock says. Because mosquitoes are so small, their internal body temperatures track the environmental temperature quickly. And this temperature determines the rate of mosquitoes’ metabolism, their cellular processes, how fast they develop, and how long they live, as well as how quickly a pathogen can replicate inside of the mosquito host, making the mosquito infectious. Every mosquito species has a thermal range in which it can survive and transmit disease.
At the cold end of this range, mosquito populations might grow too slowly or the pathogens might replicate too slowly to spread a disease. But as temperatures warm in cool regions of the world, mosquitoes could become more abundant and the pathogens they transmit may replicate faster, potentially leading to higher disease transmission, Murdock says. But if it’s too hot, the mosquitoes may die before they can pass on the pathogen. In some cases, researchers expect that when cooler places warm to moderate temperatures, they’ll see big mosquito-borne disease booms. Already-hot places might see a decline.
What’s more, some tropical mosquitoes didn’t evolve with the big seasonal temperature swings common to more temperate climes, notes Murdock. “These mosquitoes might have a lower capacity to evolve tolerance to increases in temperature or increased climate variation,” she says. It’s possible that some mosquitoes could change their behavior to modulate their temperature, perhaps by sheltering in favorable microclimates. But further research will have to determine how likely or feasible that may be, says Murdock.
Because roughly two thirds of human diseases come from wildlife, including the SARS-CoV-2 virus that causes COVID-19, HIV, West Nile, Lyme disease, and Ebola, it’s especially important to track the factors that promote outbreaks in animals, Cohen says, to get a sense of the variety of conditions that are likely to promote wildlife disease.
Even so, existing modeling studies don’t agree as to how diseases will respond to climate change. Wildlife veterinarian Lydia Franklinos, a doctoral student at University College London, in the United Kingdom, coauthored a 2019 literature review that analyzed 46 modeling studies aiming to predict climate effects on mosquito-borne disease risk over various geographic and temporal scales. Just 54% of the studies predicted a positive correlation between climate change and rising incidence of disease. As a result, she says, “no consensus exists” on how climate change will impact mosquito-borne disease risk (9). Franklinos suggests that future modeling should take into account mosquito biology, as well as factors including land use change, human population density, and socioeconomic considerations such as poverty and healthcare access.
Nevertheless, some mosquito populations seem likely to shift. In the United Kingdom, where Franklinos works, the Culex mosquitoes that carry West Nile fever could become more common in rural areas, as warmer, rainier winters riddle the countryside with flooded fields (the genus’ preferred breeding grounds). The mosquitoes that carry dengue and chikungunya, Aedes albopictus and Aedes aegypti, are also likely to spread in the United Kingdom; they tend to like urban areas, often breeding in the tiny puddles that collect in old tires and plastic trash. For all three species, warming trends in London and other northern cities, and their surrounding rural areas, hold the promise of survivable winters (10).
High- and Low-Tech Solutions
Technological interventions could help mitigate spread, at least in some cases. In May of last year, Florida saw the first introductions of genetically modified Aedes aegypti mosquitoes in the United States, following trials in Brazil, Panama, the Cayman Islands, and Malaysia. Using a gene drive method, UK-based Oxitec is leading the release of male mosquitoes, which don’t bite, that carry a gene lethal to mosquito offspring. Of course, such transgenic interventions remain controversial and their effectiveness is still a matter of debate.
The benefit of these techniques is that they can deliver control measures to mosquito breeding grounds that conventional spraying might overlook, Murdock says. But these approaches require that researchers know where the populations are and how they’re connected, so that males are released in the right locations to pass the lethal gene widely enough to crash the population. Whether the technology will spread efficiently in the field also depends on the behavior of modified males. They’ll need to be robust enough to compete with wild-type males to breed. “There’s probably not going to be a silver bullet that cleans up all of our disease problems,” she says of the gene drive technology, emphasizing the need for a combination of strategies, while adding that having “more tools in our kit for controlling mosquitoes is going to be important.”
The best solution right now is likely better public health preparation. “You set up a seasonal surveillance system to detect the first case,” says epidemiologist Jan Semenza, who’s at the Heidelberg Institute of Global Health in Germany, and then immediately isolate and treat that patient to prevent spread. Once tick or mosquito populations are established they will be difficult to eliminate, adds Semenza. “We need sophisticated early warning systems to contain an outbreak,” he says, “and prevent cross border transmission.”
The severity of fatigue that comes with Lyme and other tick-borne illnesses can be difficult to describe because Lyme disease fatigue is a whole different story
When I was sick with COVID-19 in 2020, I continued working (remotely) despite my mild fatigue, shortness of breath, low-grade fever, loss of taste and smell, and persistent cough. Though these symptoms were no walk in the park, they weren’t completely debilitating. For some COVID-19 patients, symptoms have rendered them bedridden, hospitalized, or worse. I was lucky not only to survive early COVID-19, but to have a moderate case.
For me, the fatigue of COVID-19 was nothing compared to the fatigue of Lyme disease. Lyme disease fatigue has become the barometer by which I measure all other fatigue, whether it’s general tiredness or illness-related. The severity of fatigue that comes with Lyme and other tick-borne illnesses can be difficult to describe, because fatigue can be defined many ways. It can mean muscle soreness after a workout, burnout after a long week, or yawns that come when you just didn’t sleep well. Fatigue can also mean general malaise from the pandemic, or sleepiness from any number of stressors. Then there’s feeling like your head is spinning after staying up all night finishing an assignment or tending to a crying baby.
All of these types of fatigue are uncomfortable. No one likes to be tired. But this level of fatigue generally can be solved with a few good nights of rest, a break, or even some caffeine. That’s because the fatigue is caused by external factors, not by illness. Your body has the resources to recover.
Lyme disease fatigue, like the fatigue that comes with many other serious illnesses, is another story. In a survey of over 3,000 chronic Lyme disease patients conducted by lymedisease.org, 59% of patients described their fatigue as “severe” or “very severe.” At my lowest point of illness—which lasted years—that severity meant I was almost completely bedridden. I could walk around my house and go out for a few errands on good days, but sometimes it was too tiring to walk to the mailbox, or to sit up at the dinner table. My body screamed with exhaustion. It felt heavy, as if I was weighted to the bed, and all I wanted to do was sleep. And sleep. And sleep.
The problem was, I could not actually rest. Overrun with Lyme disease bacteria as well as babesiosis, ehrlichiosis, and possible bartonella, my nervous system could not turn off. At one point, I was literally awake for weeks. And while sleep medication, neurofeedback, and cognitive behavioral therapy did help me fall asleep, it took months to catch up on rest. In addition to recovering from severe sleep deprivation, my body was also busy fighting infections. I also had chronic active Epstein-Barr virus, which meant that the shackling fatigue I experienced when I had acute mononucleosis held on during my worst years of tick-borne illness.
My body was so worn out from doing battle that when I did sleep, I often dreamed about how tired I was. I’d be lying in the middle of my college campus too exhausted to get up, or I’d collapse on a ski run while others zoomed past me. In these dreams I craved sleep as desperately as I did when I was awake. In my waking hours, I suffered from brain fog and other neurological complications. I felt like I had skied all day, partied all night, written an entire thesis, and then gotten the flu. For years.
For many Lyme disease patients, fatigue persists during and after treatment, but the good news is that it does get better. Years after feeling shackled to my bed, I am now out living a normal life. I work. I write. I exercise. I socialize. I still keep a strict sleep schedule, and I nap every afternoon. This rest allows me to maintain my restored health, so that hopefully, I will never feel the unbearable fatigue of Lyme disease again.
Lyme disease is exceedingly difficult to treat, due to its well-known shape-shifting (pleomorphic) abilities, with conventional antibiotics often failing to produce a long-term cure. Could the commonly used natural plant Stevia provide a safer, and more effective means to combat this increasingly prevalent infection?
A promising new preclinical study has revealed that whole stevia leaf extract possesses exceptional antibiotic activity against the exceedingly difficult to treat pathogen Borrelia Burgdorferi known to cause Lyme disease. The study found,
Stevia whole leaf extract, as an individual agent, was effective against all known morphological forms of B. burgdorferi.”
At present, the CDC acknowledges that at least 300,000 are infected with Lyme disease, annually, with the conventional standard of care relying on antibiotics that are not only toxic but increasingly coming under scrutiny for addressing only surface aspects of the infection, often leaving antibiotic-resistance Lyme disease deep within the system to continue to cause harm.
burgdorferi has a complex life cycle, and can exist in radically different forms: spirochetes, spheroplast (or L-form which lacks a cell wall), round bodies or cyst form (which allows for dormancy and escaping PCR detection), and highly antibiotic-resistant biofilms. This pleomorphic property makes conventional treatment exceptionally difficult because while some conventional antibiotics are effective against forms with a cell wall such as spirochetes, they are ineffective against those without a cell wall. This enables B. burgdorferi to change form to evade eradication through conventional means. Also, biofilm formation creates a significant barrier against most conventional antibiotics, even when used in combination, and has been recently suggested to be the most effective mechanism of resistance.
The researchers directly compared an alcohol extract of a whole stevia leaf product commonly found on the U.S. retail market to conventional antibiotics, and assessed their respective abilities to kill the various forms of Borrelia burgdorferi, including so called “persister” forms.
The study pointed out that, according to the CDC, about 10-20% of Lyme disease patients treated with antibiotics for the recommended 2-4 weeks experience adverse health effects, such as fatigue, pain, or joint and muscle aches. In some of these patients, the adverse effects last for more than 6 months. These patients are often labeled with “chronic Lyme disease,” or “post treatment Lyme disease syndrome.” While the adverse effects of antibiotics, including their destruction of beneficial microbes in the gut, may account for this syndrome, another possibility is that the drugs drive antibiotic-resistant forms of the disease deeper into the system, resulting in enhanced disease-associated malaise.
Given the well-known challenges of eradicating B. burgdorferi through conventional antibiotics, the researchers explored the potential for stevia as an antimicrobial.
Stevia is not normally considered an anti-microbial agent, but all plants possess in-built phytochemical defense systems which protect them against infection, and which by consuming them, we ourselves can sometimes harness and benefit from. The researchers elaborate on this point:
The leaf extract of Stevia possesses many phytochemicals, which include austroinullin, β-carotene, dulcoside, nilacin, rebaudi oxides, riboflavin, steviol, stevioside, and tiamin with known antimicrobial properties against many pathogens [40, 42, 43]. The role of these compounds is mainly to protect the plant from microbial infection and adverse environmental conditions [38–43].”
The researchers explored Stevia’s potential effectiveness against B. burgdorferi cultures, comparing it to three common antibiotics sometimes used to treat Lyme disease: doxycycline, cefoperazone, daptomycin, as well as their combination.
The study results were summarized as follows:
The susceptibility of the different forms was evaluated by various quantitative techniques in addition to different microscopy methods. The effectiveness of Stevia was compared to doxycycline, cefoperazone, daptomycin, and their combinations. Our results demonstrated that Stevia had significant effect in eliminating B. burgdorferi spirochetes and persisters. Sub-culture experiments with Stevia and antibiotics treated cells were established for 7 and 14 days yielding, no and 10% viable cells, respectively compared to the above-mentioned antibiotics and antibiotic combination. When Stevia and the three antibiotics were tested against attached biofilms, Stevia significantly reduced B. burgdorferi forms. Results from this study suggest that a natural product such as Stevia leaf extract could be considered as an effective agent against B. burgdorferi.”
Notably, the study found that the most antibiotic resistant form of B. burgdorferi, the biofilm form,actually increased in mass when individual antibiotics were administered. Stevia, on the other hand, reduced the biofilm mass on both tested surfaces (plastic and collagen) by about 40%.
It is also interesting to note that the stevoside extract, by itself, was not found to be an effective antimicrobial agent against B. burgdorferi; nor did it have any effect on resistant cells. Mass market stevia products, including Coca-cola’s Truvia (ironic branding, considering it does not have the truly therapeutic property of whole stevia), would not, therefore, have the medicinal property associated with the whole herb extract. This speaks, of course, to the well known principle in natural medicine that the activity of the whole can not be reproduced through a part, nor is the therapeutic activity of the whole identical to that of the sum of its parts.
While this is only a preliminary study and should not be interpreted to mean the consumption of whole stevia extract will result in clinical improvements comparable or superior to conventional antibiotics, it opens the door to future research on the topic. That said, anyone who is considering natural ways to prevent Lyme disease infection, or to support as an adjunct therapy conventional treatments of the disease, could utilize this safe, food-based substance as a potential means of support and synergy. Certainly, there is little if any indication that stevia could cause harm, unlike conventional treatments. See our stevia research section here for more information.
Prevention is the best medicine, and essential oils work to both prevent and help control Lyme disease.
Lyme disease’s widespread presence is increasing in the U.S with 300,000 + people becoming infected every year. More common than breast cancer, we know that proper prevention is the best medicine. Of all the natural therapies on the market, the scientific literature suggests that essential oils are ideal tools to have on hand. In addition to bug-defeating benefits, some oils may help with the control of Lyme if it is contracted, as well.
Causes and Symptoms of Lyme Disease
Lyme disease is traditionally viewed as mainly being a tick-borne illness caused by the spirocheteBorrelia burgdorferi. Although, there is recent research proving that it is also sexually transmitted, most authorities agree that tick bites are responsible for a vast majority of the cases seen in doctors’ offices. Typically only some swelling and minor itching remain after a bite occurs and the tick is safely removed. If the tick is carrying Lyme, however, other symptoms will emerge.
The most recognizable indication of Lyme is the “bulls-eye” rash that spreads around the bite like a target, though many individuals never see a rash so don’t let that be your only indication! Other initial symptoms of Lyme include flu-like aches and pains.
If not treated right away, Lyme disease can advance into more chronic conditions like arthritis, sore muscles and joints, memory problems, headaches, numbness or weakness, and severe fatigue. (1)
Truth be told, Lyme is a rather serious matter so first off, tick bites should be avoided plus monitored closely if prevention fails.
Top Essential Oils for Lyme Disease Prevention
The key to avoiding Lyme disease is prevention. Even if the chronic symptoms of the disease can be avoided, the symptoms and treatment of Lyme can be a challenge. No one wants to deal with the discomfort and hassle, and no one should have to live with the long-term effects because they can be debilitating.
Northern US coastlines, the Mid-Atlantic, Wisconsin, and Minnesota are areas especially prone to Lyme-carrying ticks, though all states are vulnerable. (2) In order to prepare your family for the possibility of tick bites and prevention of Lyme, consider applying a diluted blend of these essential oils in addition to your typical lemon, eucalyptus and citronella oils, for a varied approach that will keep ticks guessing.
1. Clove
Citronella is usually the first that comes to mind when we think of bug repellants, because it is included in most store-bought candles and sprays as the go-to bug repellent. For ticks, though, citronella may not be the first go-to.
Case in point, a 2014 study of the effect that citronella and clove oils have on ticks, clove came out on top. While citronella was reasonably effective, clove outperformed it substantially withover 90% efficacy! (3)
DIY Tip:Clove oil can be used in outdoor diffusions where ticks may be prominent, direct sprays, ground/surface treatments, and diluted in topical prevention applications. Try adding 8 drops of clove essential oil per 1 oz of coconut oil and apply throughout your body before hiking and spending time outdoors.
2. Oregano
Oregano is a popular kitchen herb that has a strong essential oil profile. Known as an antibacterial/antibiotic oil with strong effects on the skin that require dilution, oregano essential oil finds its way into bug control and Lyme prevention, as well.
Sharing major compounds carvacrol and eugenol with clove oil, it has also tested well against ticks in at least one recent study. (4)
As a bonus in topical applications, oregano has antibacterial effects to bring to the table – important when Lyme is a bacteria! Topical applications could give you a head start in warding off Lyme before it has a chance to settle in.
DIY Tip: Because oregano can be harsh on skin, be sure to dilute it very well and use it as part of a larger blend.
3. Vetiver
Vetiver and citronella are comparable plants with a similar aroma that can be used in similar ways. And, again, like clove, vetiver essential oil seems to be more effective against ticks than citronella.
In tests against ticks and their larvae, vetiver essential oil was tested for its effectiveness. Whether it is because of resistance built up against the more commonly used treatmentsor whether vetiver has always been this good, vetiver was able to keep ticks at bay even better than standard treatments. (5)
DIY Tip: Mix 30 drops of vetiver in a 16 oz spray bottle with tap water. Spray around the openings to your home (windows, doors, etc.); use diluted topically with clove.
4. Garlic
If you’ve intentionally eaten garlic to keep the vampires and mosquitoes away, you already know about its potent aromatic effects. Researchers looked into this more closely by extracting the essential oil from garlic bulbs to test against ticks. Upon exposure to garlic essential oil, tick mortality rates were nearly 100%! (6)
DIY Tip: If garlic essential oil is not available, consider including a DIY garlic oil infusion in your ground and surface treatments. And when all else fails, some extra homemade fresh garlic bread is always warranted!
DIY Lyme Prevention Plan
You can’t go unprotected if you’re going to be in areas of high risk and exposure to ticks. With so many oils appearing more effective than commercial options, it seems essential oil formulations are the smarter choice.
Effective Strategy For Fighting Ticks and Lyme Disease
Keep this simple “lotion” of diluted oils on hand to apply on exposed skin whenever tick exposure will be high. Hikers, campers, and others enjoying outdoor activity that will take you into the woods should be considered at risk. Remember that these oils are powerful, so you should keep them away from your eyes and mouth.
Simply blend:
4 oz carrier oil of choice
40 drops total of a blend of tick-repelling essential oils (vetiver, clove, oregano, ylang ylang, and some citrus for scent balance are all useful)
Blend, pour into a glass spritzer bottle, and spray periodically to ankles, arms, etc.
Treating Lyme with Essential Oils
Sometimes, even when we do all we can, the worst happens. Lyme disease can strike at any time, and you should be prepared to find a physician who can work with you in that worst-case scenario. These doctors are referred to as Lyme Literate, and as Dr. Cindee Gardner pointed out in an interview, they still may not be aware of the range of alternative treatments that are available for Lyme.
In Dr. Gardner’s practice, she uses everything from homeopathy to herbs to essential oils. (7) Some of it is directly connected to Lyme as a bacteria, while a lot of it is related to symptom control. You should find these oils beneficial in your plan of attack:
Citrus for antimicrobial as well as energizing effects
Various blends of your favorite oils into massages for pain
With the vast variety of symptoms and broad actions of essential oils, the list of symptoms and useful oils could continue on for days. To defeat Lyme disease, simply remember to begin with prevention, seek help promptly if infection is suspected, and use your carefully selected essential oil medicine cabinet.
Lyme disease is exceedingly difficult to treat, due to its well-known shape-shifting (pleomorphic) abilities, with conventional antibiotics often failing to produce a long-term cure. Could the commonly used natural plant Stevia provide a safer, and more effective means to combat this increasingly prevalent infection? A promising new preclinical study has revealed that whole stevia leaf extract possesses exceptional antibiotic activity against the exceedingly difficult to treat pathogen Borrelia Burgdorferi known to cause Lyme disease. The study found, Stevia whole leaf extract, as an individual agent, was effective against all known morphological forms of B. burgdorferi.” At present, the CDC acknowledges that at least 300,000 are infected with Lyme disease, annually, with the conventional standard of care relying on antibiotics that are not only toxic but increasingly coming under scrutiny for addressing only surface aspects of the infection, often leaving antibiotic-resistance Lyme disease deep within the system to continue to cause harm.
burgdorferi has a complex life cycle, and can exist in radically different forms: spirochetes, spheroplast (or L-form which lacks a cell wall), round bodies or cyst form (which allows for dormancy and escaping PCR detection), and highly antibiotic-resistant biofilms. This pleomorphic property makes conventional treatment exceptionally difficult because while some conventional antibiotics are effective against forms with a cell wall such as spirochetes, they are ineffective against those without a cell wall. This enables B. burgdorferi to change form to evade eradication through conventional means. Also, biofilm formation creates a significant barrier against most conventional antibiotics, even when used in combination, and has been recently suggested to be the most effective mechanism of resistance.
The new study was published in the European Journal of Microbiology & Immunology and titled, “Effectiveness of Stevia Rebaudiana Whole Leaf Extract Against the Various Morphological Forms of Borrelia Burgdorferi in Vitro,” and conducted by researchers from the Department of Biology and Environmental Science, University of New Haven, West Haven, CT. The researchers directly compared an alcohol extract of a whole stevia leaf product commonly found on the U.S. retail market to conventional antibiotics, and assessed their respective abilities to kill the various forms of Borrelia burgdorferi, including so called “persister” forms. The study pointed out that, according to the CDC, about 10-20% of Lyme disease patients treated with antibiotics for the recommended 2-4 weeks experience adverse health effects, such as fatigue, pain, or joint and muscle aches. In some of these patients, the adverse effects last for more than 6 months. These patients are often labeled with “chronic Lyme disease,” or “post treatment Lyme disease syndrome.” While the adverse effects of antibiotics, including their destruction of beneficial microbes in the gut, may account for this syndrome, another possibility is that the drugs drive antibiotic-resistant forms of the disease deeper into the system, resulting in enhanced disease-associated malaise. Given the well-known challenges of eradicating B. burgdorferi through conventional antibiotics, the researchers explored the potential for stevia as an antimicrobial. Stevia is not normally considered an anti-microbial agent, but all plants possess in-built phytochemical defense systems which protect them against infection, and which by consuming them, we ourselves can sometimes harness and benefit from.
If you’ve had Lyme disease then you probably don’t know that most Lyme disease tests are very inaccurate. The CDC has been trying to cover this up for a long time now.
Lyme disease affects the immune system by slowing it down. Doctors are turning against their patients because they are afraid of losing their practices. The CDC and insurance companies will do anything to keep Lyme disease from being diagnosed, treated, or widely recognized. Lyme is considered to “only” be transmitted by ticks infected with the bacteria.
The CDC says they are under-reported and they believe there are 300,000 to half a million cases every year. This would make Lyme disease about twice as common as breast cancer and 6 times more common than HIV/AIDS. Lyme becomes chronic when it hasn’t been caught in the early stages. The CDC and the ISDA denies that chronic Lyme even exists and will continue to do because of insurance companies that hate spending money and time treating patients.
The bacteria that causes Lyme is called Borrelia burgdorferi, which has a cork-screw shaped which is known as a spirochete. This Lyme spirochete is a cousin to the Treponema pallidum, which causes syphilis. A new study suggests that Lyme disease could be sexually transmitted. Presented at the annual Western Regional Meeting, “The study — presented at the annual Western Regional Meeting of the American Federation for Medical Research — a collaborative effort by an international team of scientists — tested semen samples and vaginal secretions of three groups of patients to investigate whether passing Lyme disease to a partner through unprotected sex is a possibility. The study observed control subjects without evidence of Lyme disease, random subjects who tested positive for Lyme disease, and married heterosexual couples engaging in unprotected sex who tested positive for the disease. The presence of B. burgdorferi and identical strains of the bacterium were of particular interest to the researchers in unprotected sex in spouses.”

 Lyme disease can mimic hundreds of other conditions since its symptoms mirror many medical problems such as multiple sclerosis, arthritis, chronic fatigue syndrome or lupus, and is sometimes known as “The Great Imitator” because of this.
Lyme disease can mimic hundreds of other conditions since its symptoms mirror many medical problems such as multiple sclerosis, arthritis, chronic fatigue syndrome or lupus, and is sometimes known as “The Great Imitator” because of this.  The most common symptoms in acute (aka: early localized) Lyme disease are the ones people are most familiar with, because they are symptoms often shared with other illnesses; however, it’s important to recognize that they could indicate Lyme, and you should see a Lyme-treating physician right away.
The most common symptoms in acute (aka: early localized) Lyme disease are the ones people are most familiar with, because they are symptoms often shared with other illnesses; however, it’s important to recognize that they could indicate Lyme, and you should see a Lyme-treating physician right away.






.jpg)

