New research suggests that regularly adding table salt to food could increase the risk for gastric cancer. Cara Dolan/Stocksy
Gastric cancer can be serious and is related to several risk factors, including dietary choices.
A recent study found that people who regularly added salt to food at the table had a 41% higher risk for gastric cancercompared to those who rarely or never added salt.
Reducing salt intake can help reduce the risk of gastric cancer, and those at a higher risk may benefit from seeking appropriate follow-up.
Gastric cancer — also known as stomach cancer — is the fifth most commonTrusted Source cancer in the world. While not as common in the United States, it still makes up about 1.5%Trusted Source of new cancer cases diagnosed annually.
Doctors and experts are interested in identifying risk factors for gastric cancer so that people can seek high-quality care early.
A recent study published in Gastric Cancer examined data from over 470,000 individuals to see how the frequency of adding salt to food related to cases of gastric cancer.
The authors found that participants who always added salt to food were at a higher risk for gastric cancer than participants who rarely or never added salt to food at the table.
This study adds to data about the risk salt poses for gastric cancer in non-Asian populations, as most research in this area has been in Asian populations.
As research moves forward, doctors may be able to ask people about their frequency of adding salt to foods as a simple indicator to monitor salt intake and related gastric cancer risk, aiding public health messaging.
This prospective study used data from the UK Biobank, including 471,144 participants in its analysis.
They excluded participants who were missing data on adding salt to food, body mass index (BMI), or urinary sodium or potassium levels. They also excluded participants who had cancer at baseline and participants who had kidney disease.
Participants filled out baseline questionnaires to indicate how often they added salt to food, excluding the salt they used while cooking. Participants could respond with never/rarely, sometimes, usually, or always.
Researchers further measured participants’ urinary sodium, creatinine, and potassium levels. They were also able to estimate 24-hour urinary sodium excretion.
They accounted for several covariates, including physical activity levels, age, education level, ethnicity, sex, and alcohol use. They were also able to take into account red meat consumption and fruit and vegetable intake. The median follow-up period with participants was 10.9 years.
During the follow-up time, 640 cases of gastric cancer among participants were documented. In general, participants who reported always adding salt to food at the table were more likely to be past or current smokers, have a high level of alcohol intake, and have a lower education level.
Researchers found that participants who always added salt at the table were at 41% higher risk for gastric cancer compared to participants who never or rarely added salt to food at the table.
While they found that adding salt to food more often was associated with increased 24-hour urinary sodium levels, they did not find a significant association between 24-hour urinary sodium levels and gastric cancer.
They also found that in a subset of 198,900 participants, responses to the frequency of adding salt at the table positively correlated with daily sodium intake levels.
The results suggest that examining the frequency of added salt use at the table may be a simple way to assist in identifying individuals with high salt intake who may, in turn, be at risk for gastric cancer.
Anton Bilchik, MD, PhD, surgical oncologist, chief of medicine, and Director of the Gastrointestinal and Hepatobiliary Program at Providence Saint John’s Cancer Institute in Santa Monica, CA, not involved in this study, told Medical News Today “[t]he study provides further evidence of the association between diet, particularly one rich in salt and gastric cancer.” He added:
“It has been suggested that one of the major causes of gastric cancer in Asian countries is from fish high in salt content. Much less is known about the association of salt intake and gastric cancer in Western countries. It is well known that excessive use of salt is associated with a higher risk of hypertension and cardiovascular disease. This study provides additional evidence that salt routinely taken with meals increases the risk of developing gastric cancer. It is therefore imperative that people be aware of the deleterious effects of excessive salt intake.”
Many factors contribute to someone’s risk for gastric cancer, including smoking, increased age, obesity, and family history.
Researchers of the current study note that higher salt intake has been associated with a higher risk for gastric cancer in Asian studies.
However, there have not been many studies in this area among Western population groups.
Bilchik offered the following insight to MNT:
“Gastric cancer is very serious especially if it presents at an advanced stage. It is one of the most common cancers in Asian countries and there is therefore greater emphasis on screening measures than in Western countries. Also, the pattern of presentation is different with patients from Western countries presenting more often with cancer in the upper part of the stomach, a more challenging location to manage than Asian countries where cancers are more often found in the lower part of the stomach. This may be related to a higher incidence of obesity and gastroesophageal reflux disease in Western countries — risk factors for upper gastric cancer.”
This study has several limitations. First, it cannot prove that increased salt consumption causes gastric cancer. It also relies on participant reporting, which does not always produce the most accurate data, and they did not have complete data on salt intake in foods.
The UK Biobank is also not necessarily reflective of the general population, so research with other groups with greater diversity may be warranted, and the results cannot be generalized. The link between salt intake and gastric cancer risk may be stronger than observed in this study.
Researchers also used an estimation method to measure 24-hour urinary sodium levels, which does not always accurately represent this level.
They further note that the case numbers were inadequate to examine the effect of possible modifiers like sex, age, ethnicity, smoking status, or Helicobacter pylori infection.
There is the possibility for residual confounding, and future research can also focus more on gastric cancer subtypes.
This data continues to support the idea that excess salt intake is associated with an increase in gastric cancer risk. However, there are many other reasonsTrusted Source to limit salt intake. For example, consuming too much sodium can also increase the risk of high blood pressure and kidney problems.
People can work towards making wiser choices regarding salt consumption to reduce their overall salt intake.
This can include working with a registered dietitian who can help with individualized strategies.
Registered dietitian Karen Z. Berg, not involved in this research, offered the following insights on salt reduction ideas to MNT:
“People get so caught up in their habits that they add salt to an already salty food. Taste your food first, and hopefully more often than not, you won’t have to add salt. Also, I tell people not to cook with salt. Use spices instead to enhance flavors. Salt can be added later if you absolutely feel like it’s necessary. Your taste buds get used to salt, and the more you add salt to your food, the more you’re going to want it. So I tell people to really be conscious of that and try to ween themselves off of salt as much as possible.”
Trastuzumab is the only first-line treatment targeted against the human epidermal growth factor receptor 2 (HER2) approved for patients with HER2-positive advanced gastric cancer. The impact of metabolic heterogeneity on trastuzumab treatment efficacy remains unclear.
Methods
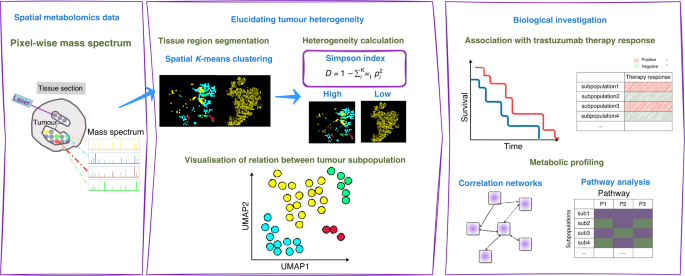
Spatial metabolomics via high mass resolution imaging mass spectrometry was performed in pretherapeutic biopsies of patients with HER2-positive advanced gastric cancer in a prospective multicentre observational study. The mass spectra, representing the metabolic heterogeneity within tumour areas, were grouped by K-means clustering algorithm. Simpson’s diversity index was applied to compare the metabolic heterogeneity level of individual patients.
Results
Clustering analysis revealed metabolic heterogeneity in HER2-positive gastric cancer patients and uncovered nine tumour subpopulations. High metabolic heterogeneity was shown as a factor indicating sensitivity to trastuzumab (p = 0.008) and favourable prognosis at trend level. Two of the nine tumour subpopulations associated with favourable prognosis and trastuzumab sensitivity, and one subpopulation associated with poor prognosis and trastuzumab resistance.
Conclusions
This work revealed that tumour metabolic heterogeneity associated with prognosis and trastuzumab response based on tissue metabolomics of HER2-positive gastric cancer. Tumour metabolic subpopulations may provide an association with trastuzumab therapy efficacy.
Background
Gastric cancer (GC) is currently the fourth most common cause of cancer-related deaths globally [1]. Trastuzumab, a recombinant humanised monoclonal antibody directed against the human epidermal growth factor receptor 2 (HER2), is the only targeted agent approved for the first-line treatment of patients with HER2-positive advanced GC [2]. Trastuzumab combined with platin–fluoropyrimidine chemotherapy improves survival outcomes in HER2-positive GC [2]. Nevertheless, only a subgroup benefits from the addition of trastuzumab to chemotherapy. The overall response rate of the combined therapy is less than 50%, indicating that a considerable proportion of HER2-positive cancers are resistant to HER2 inhibition [3]. Optimising the selection of HER2-targeted regimens by identifying patient subpopulations who would benefit from trastuzumab could be cost-effective and would spare some patients unnecessary exposure to ineffective treatments.
Molecular heterogeneity exhibits a variety of biological behaviours in cancers [4]. Exploring the patterns of molecular heterogeneity are necessary to design personalised targeted regimens to increase patient response [5,6,7,8]. GC has a high level of genomic and phenotypic variability even within individual tumours, and this underlying heterogeneity is considered as a major cause for the frequent failure of biomarker-based clinical trials [9,10,11]. High incidence of HER2 heterogeneity was observed in GC and it was associated with chemotherapy [12] and trastuzumab efficacy [13]. Several studies uncovered proteomic subpopulations that were linked to patient survival in GC [14,15,16]. Metabolic reprogramming has been recognised as one hallmark that can be used to prevent therapeutic resistance [17]. Metabolomics, a predictor of drug therapeutic response in cancers [18, 19], can generate metabolite profiles and also combine this information with changes in crucial metabolic pathways, such as Warburg effect, altered amino acid/lipid/drug metabolism, generation of drug-resistant cancer stem cells, and immunosuppressive metabolism [17]. Metabolite profile was considered an important factor besides HER2 status in assessing the initial response to trastuzumab treatment for GC patients [20, 21]. Specifically, one study revealed tumour metabolic heterogeneity within HER2/neu-positive and HER2/neu-negative GC cells [22]. Nonetheless, the impact of intratumoural and intertumoural metabolic heterogeneity on trastuzumab response in HER2-positive advanced GC remains unclear. Matrix-assisted laser desorption/ionisation–imaging mass spectrometry (MALDI–IMS) enables the imaging of different molecular classes in their histopathological context and thus the allocation of molecular profiles to specific tumour cell types [23,24,25]. This high cellular specificity is behind the increasing popularity of IMS and its proven ability to identify diagnostic and prognostic biomarkers [26,27,28]. Additionally, MALDI–IMS is an omics technique that allows for the global characterisation of the spatial metabolomics [29, 30], which offers an opportunity to demonstrate the drug-resistant tumour profile with metabolic heterogeneity and discovering the alteration in the tumour microenvironment [17]. Combined with statistical tools, MALDI-IMS constitutes a unique tool to reveal a priori tumour subpopulations that are not distinguishable using conventional histopathological methods, but which are molecularly distinct [31,32,33].
We apply spatial metabolomics and K-means clustering method to identify metabolically distinct tumour subpopulations of HER2-positive advanced GC from routinely preserved pretherapeutic biopsies, and assess their relationships with the response to trastuzumab treatment. The workflow of this study is shown in Fig. 1.
Fig. 1: Schematic overview of the de novo identification of metabolic heterogeneity and tumour subpopulations.
Discussion
In the present study, we discovered heterogeneity in a series of patients with HER2-positive advanced GC based on tissue metabolomics. We defined nine distinct metabolic subpopulations. Of the nine subpopulations, two subpopulations were associated with favourable prognosis and trastuzumab sensitivity, and one subpopulation was associated with poor prognosis and trastuzumab resistance. Additionally, tumour metabolic heterogeneity was associated with prognosis and trastuzumab response. To our knowledge, this study is the first to investigate the impact of metabolic heterogeneity on the trastuzumab treatment efficacy and survival in HER2-positive advanced GC. A higher degree of tumour metabolic heterogeneity associated with a better prognosis and trastuzumab sensitivity. This observation is in line with previous studies [12, 38]. One study described the high incidence of intratumoural HER2 heterogeneity in a large series of 322 patients with GC in detail by performing HER2 immunohistochemistry (IHC) and fluorescence in situ hybridisation (FISH) and evaluating the gene copy number individually in distinct areas with different IHC staining intensity. In addition, they further revealed that HER2 heterogeneous positivity was associated with longer survival than the homogeneous [12]. Another study consistently reported proteomic heterogeneity and their positive correlation with prognosis in HER2-positive breast cancer patients treated with trastuzumab [38]. Moreover, they revealed that high heterogeneity of tumours could reflect the presence of heterotypic components including infiltrating immune cells, which facilitated the response to treatment [38]. This could be the possible explanation of the observed correlation between a higher metabolic heterogeneity and a better outcome in HER2-positive advanced GC in the present study. Taken together, those studies together with us demonstrated the association of tumour heterogeneity of the molecular expression with trastuzumab response, indicating that molecular heterogeneity should be taken into consideration when clinical therapeutic decision of trastuzumab is made. The most significant pathways among nine tumour subpopulations were related to nucleotide metabolism and carbohydrate metabolism, which are revealed to be highly spatially organised and could be visualised as different molecularly defined regions. Major changes in nucleotides and nucleotide metabolism have been linked to patient survival. Typically, cancer cells have deactivated crucial DNA damage response signalling routes and often rewire their metabolism and energy production networks [39, 40]. Anabolic metabolism of DNA was identified as an important downstream effect of the HER2 oncogene in breast cancer [41]. In GC, one study characterised GC with metabolomic features and identified three tumour-specific subtypes. One tumour-specific subtype comprised enriched DNA metabolism, and it predicted a benefit when initiating trastuzumab therapy [20]. Another study identified DNA metabolism as a factor influencing response to HER2-targeted trastuzumab therapy, and the changes in DNA metabolism found in patient tissues were validated in a HER2-positive/sensitive and HER2-positive/resistant GC cell model [21]. The nucleotide metabolites GDP and GMP showed significant effect on survival in the GC patients treated with trastuzumab therapy [21]. This study is consistent and found that the subpopulation with downregulated nucleotide metabolism (subpopulation 4) was associated with a resistance to trastuzumab therapy.
Meanwhile, correlated metabolites within the trastuzumab-sensitive subpopulaiton 9 comprise different carbohydrate compounds, such as D-Glucosamine, D-Fructose 6-phosphate and D-Glucose 1-phosphate. These compounds are involved in different pathways contributing to tumour cell survival [42, 43]. D-glucosamine and and its derivatives have shown their anti-tumour effects on cell proliferation, cell death and angiogenesis in human bodies, although the precise function and mechanism remains to be clarified [43]. Additionally, carbohydrate metabolism is the major HER2-related altered metabolic pathway, and the association of glucose metabolism with HER2-positive breast cancer was confirmed [44, 45]. Gluconeogenesis in HER2-positive breast cancer was upregulated for energy supply, resulting in enriched consumption of related amino acids [46]. In particular, previous studies support our observation in the metabolite networks that the metabolites succinate, sn-glycerol 3-phosphate, 5’-Methylthioadenosine and diphosphate showed significant importance in distinguishing trastuzumab-sensitive and trastuzumab-resistant patients, which can be interpreted as the potential biomarkers for the trastuzumab therapy response [20, 21]. However, these new potential metabolite biomarkers and their related metabolisms have not yet fully investigated in GC. A greater understanding of these metabolite biomarkers in the future could reveal detailed insights into the molecular changes underlying GC disease, metabolic responses to treatments, and mechanisms leading to trastuzumab therapy response.
One challenge in identifying metabolic heterogeneity for their association with trastuzumab response is the limited number of tumour samples. All patients must have HER2 positivity, trastuzumab treatment, and adequate follow-up. Industry-sponsored controlled clinical trials do exist; however, the availability of these studies for independent research is unfortunately limited. Although the number of tumour samples is limited in the current study as well, the samples and associated data still offer some advantages. The tissue specimens in this study were collected from many sites. Furthermore, HER2 testing was centrally performed with the highest quality standards [34]. This ensured that the inclusion criteria were validated for each tumour sample. In conclusion, we demonstrated the importance of considering tumour metabolic heterogeneity in HER2-positive advanced GC for optimising patient management. Consequently, tumour metabolic heterogeneity showed an impact on trastuzumab efficacy and patient outcomes. These findings should be validated in larger independent cohorts, and additional molecular correlative analysis are warranted.
Overexpression of PIEZO2 stood out as an independent risk factor for men with gastric cancer (GC) who had poor overall survival in a study led by researchers from Tongji University School of Medicine and Shanghai University of Traditional Chinese Medicine. Interestingly, the biomarker did not have the same impact in women, and patients had a better prognosis with poorly differentiated tumors and increased PIEZO2 expression. Further, this research suggests that PIEZO2 could be a good target for immunotherapy.
The study appears in Scientific Reports and the lead authors are Yun-Chao Zhang and Min Yang.
PIEZO2 genes in GC, they report, were mostly implicated in inflammation, immunological response, and tumor metastasis. The gene had a negative correlation with cell stemness (stem cell-like properties) and mutation levels in GC patients and a positive correlation with immune cell infiltration and gene expression in the tumor microenvironment. These findings, they suggest, point to PIEZO2 as a potential new immunotherapy target.
Gastric cancer (GC) is estimated to be the fifth most common cancer worldwide, and the fourth most deadly. Current treatments include: endoscopic examination, gastrectomy, and chemotherapy or adjuvant chemotherapy or neoadjuvant therapy. Although outcomes have improved, they are still very poor and there is an urgent need for biomarkers to guide treatment, particularly as immunotherapy is introduced for this disease.
A transmembrane protein, PIEZO2 is crucial for the quick response of somatosensory neurons to mechanically generated currents. There’s evidence that abnormal expression of PIEZO2 may be related to the progression of cancer. The gene has been specifically linked to GC, however, there are still lots of questions about the use of immunotherapy, potential mechanisms of immune function, and prognostic subgroup analysis in this disease.
This study uses bioinformatics analysis of the clinical data in the Online database of cancer genes and GSE54129 to analyze the clinical characteristics of PIEZO2 expression. The team studied the correlation of PIEZO2 with immune cell infiltration, immune-related genes, and immune checkpoint genes. Predicted the performance of PIEZO2 in immune checkpoint blocking therapy.
The University of California Santa Cruz (UCSC) Genome Browser Database was used to retrieve the standardized pan-cancer dataset, and for each sample, the PIEZO2 gene expression data were extracted. The difference in PIEZO2 between tumor and normal tissues was assessed using the TCGA and GSE54129 datasets. The team further retrieved the expression data of the PIEZO2 gene’s marker genes and a total of 60 genes from the immune checkpoint pathway.
The researchers write, “We demonstrated a strong correlation between PIEZO2 and immune cells. The majority of immune checkpoint and immunological-related genes were associated with PIEZO2 expression.”
With respect to tumor stemness, The team “… examined the important PIEZO2 and tumor stemness markers in clinical patients. PIEZO2 was shown to be inversely linked with DMPss, DNAss, ENHss, and EREG.EXPss, EREG-METHss, RNAs, MSI, purity, and TMB in GC.”
They add that, “PIEZO2 might be used as an immunotherapy target.”
Laparoscopy-assisted distal gastrectomy noninferior for both relapse-free, overall survival
Relapse-free survival (RFS) data at 5 years showed that laparoscopy-assisted distal gastrectomy (LADG) was noninferior to open distal gastrectomy (ODG) in locally advanced gastric cancer, according to a phase II/III randomized trial from Japan.
Among 500 randomized patients, the 5-year RFS rate was 75.7% in the LADG group and 73.9% in the ODG group, with a hazard ratio of 0.96 (90% CI 0.72-1.26, noninferiority 1-sided P=0.03), reported Tsuyoshi Etoh, MD, PhD, of Oita University in Yufu, Japan, and colleagues.
There was also no significant difference in overall survival (OS) between the two groups (81.7% vs 79.8%, respectively, HR 0.83, 95% CI 0.57-1.21, P=0.34), they noted in JAMA Surgeryopens in a new tab or window.
“LADG with D2 lymph node dissection for locally advanced gastric cancer, when performed by qualified surgeons, was proved noninferior to ODG,” they wrote. “This laparoscopic approach could become a standard treatment for locally advanced gastric cancer.”
Since laparoscopic gastrectomy for locally advanced gastric cancer “is technically demanding,” a strength of the study was the fact that participating surgeons were required to have Endoscopic Surgical Skill Qualification System (ESSQS) certification (established by the Japan Society for Endoscopic Surgery to enable surgeons to maintain their laparoscopic technical skills), and to have performed a specified number of both laparoscopic gastrectomy and open gastrectomy procedures. Thus, Etoh and colleagues were able to “ensure high-quality surgical interventions in this trial.”
However, in a commentary accompanying the study,opens in a new tab or window Daniel B. Hoffman, MD, and Eric K. Nakakura, MD, PhD, both of the University of California San Francisco Helen Diller Family Comprehensive Cancer Center, noted that since the surgeons participating in the trial were required to have ESSQS certification with additional training, “this may not reflect the reality of gastric cancer care in Western countries, where lower gastric cancer incidence and a lack of centralization of gastrectomies to high-volume centers limit individual surgeon experience.”
They also pointed out several other features of the study that should be considered before applying the results to Western populations.
For example, they noted that the median body mass index (BMI) among the study population was 22.5, and the exclusion of patients with a BMI ≥30 means the study population as a whole was less overweight than those seen in Western studies. They also pointed out that neoadjuvant chemotherapy is usually provided to patients with locally advanced gastric adenocarcinomas in Western countries, whereas in this study, patients were exclusively given adjuvant chemotherapy.
The Japanese Laparoscopic Surgery Study Group conducted this open-label, multicenter, prospective study from November 2009 through July 2016. Eligible patients had histologically proven gastric adenocarcinoma, a BMI less than 30, an Eastern Cooperative Oncology Group performance status of 0 or 1 (considered potentially curable by distal gastrectomy), and a clinical diagnosis of muscularis propria, subserosa, and serosal exposure, N0-2 without bulky node metastasis, or M0 lesions without involvement of other organs.
Of the 502 patients included in the full-analysis set, 254 were in the ODG group and 248 were in the LADG group. Patients in the ODG group had a median age of 67, and 66.1% were men. Patients in the LADG group had a median age of 64, and 68.1% were men. The median follow-up for all patients after randomization was 67.9 months.
In both groups, distal gastrectomy with D2 lymph node dissection was performed, according to Japanese treatment guidelines. Staging laparoscopy in the ODG group was recommended for patients at high risk of peritoneal dissemination, and adjuvant chemotherapy was administered 1 year postoperatively when pathological stages II and III (with some exceptions) were confirmed after surgery.
In the full-analysis set, 27.7% in the LADG group and 28.3% in the ODG had recurrence, death, or curability C (definite residual disease). When curability C was excluded from the events, the 5-year RFS rate was 79.9% in the LADG group and 77.6% in the ODG group.
No significant differences were seen in the incidence of intraoperative complications. Any postoperative complications were observed in 11.5% of the LADG group and 10.7% of the ODG group, while those of grade 3 and higher were observed in 3.5% and 4.7%, respectively (P=0.64).
Paclitaxel plus ramucirumab (PTX + RAM) is the standard second-line chemotherapy for unresectable advanced or recurrent gastric cancer (AGC). Nanoparticle albumin-bound paclitaxel (nab-PTX) is an improved, more convenient form of PTX and is non-inferior to PTX. Although some retrospective and single-arm phase II studies regarding nab-PTX + RAM have been reported, comparative studies are lacking. Here, we compared the efficacy and toxicity of nab-PTX + RAM and PTX + RAM using propensity score matching.
Methods
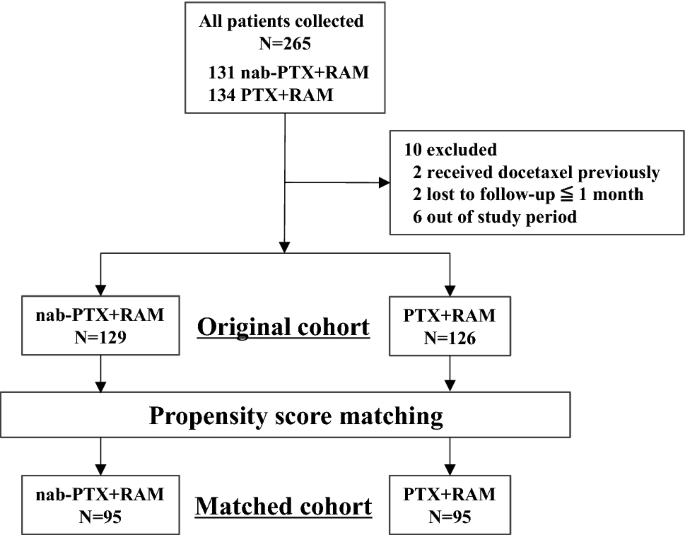
Clinical data of 265 patients treated for AGC with nab-PTX + RAM or PTX + RAM were retrospectively collected. Nab-PTX was administered at dosages of 100 mg/m2, replacing PTX in the standard PTX + RAM regimen. Progression-free survival (PFS), overall survival (OS), and toxicity were compared using 1:1 propensity score matching.
Results
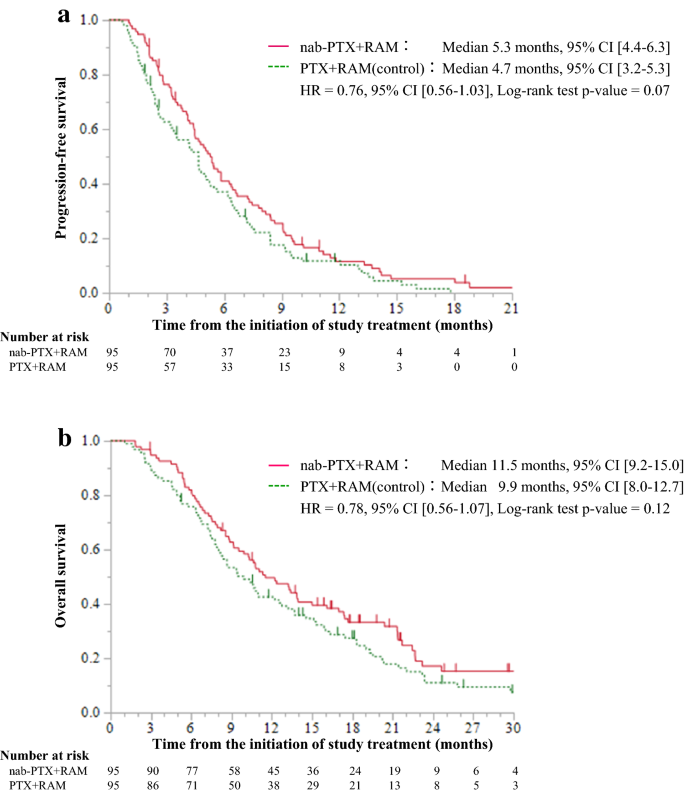
In total, 190 (72%) patients were matched. The median PFS was 5.3 [95% confidence interval (CI) 4.4–6.3] and 4.7 (95% CI 3.2–5.3) months in the nab-PTX + RAM and PTX + RAM groups, respectively [hazard ratio (HR) = 0.76, 95% CI 0.56–1.03, p = 0.07]. The median OS was 11.5 (95% CI 9.2–15.0) and 9.9 (95% CI 8.0–12.7) months, respectively (HR = 0.78, 95% CI 0.56–1.07, p = 0.12). Grade 3 and 4 neutropenia was observed more frequently in the nab-PTX + RAM group (72% vs. 56%, p = 0.03). No treatment-related deaths occurred.
Conclusions
Nab-PTX + RAM exhibited more favorable trends in terms of PFS and OS but was more myelosuppressive than PTX + RAM. As neutropenia is commonly manageable toxicity, nab-PTX + RAM presents a treatment alternative for AGC. Further studies including randomized, controlled studies are warranted.
Introduction
Fluoropyrimidine plus platinum is the recommended standard first-line chemotherapy for unresectable advanced or recurrent gastric cancer (AGC) according to several guidelines [1,2,3]. The RAINBOW trial [4] demonstrated the superiority of weekly administration of paclitaxel plus ramucirumab (PTX + RAM) over weekly PTX in overall survival (OS) in previously treated AGC patients, after which PTX + RAM became the standard second-line chemotherapy.
Nanoparticle albumin-bound paclitaxel (nab-PTX) is a solvent-free albumin-bound, 130 nm particle form of PTX. Since nab-PTX is free of polyethoxylated castor oil and hydrated ethanol, patients are at lower risk of hypersensitivity compared to when PTX is administered [5]. Therefore, nab-PTX is administered for a shorter time than PTX without premedication and patients with alcohol intolerance can be treated with it [5]. Thus, nab-PTX is more beneficial and convenient than PTX in clinical practice.
The ABSOLUTE trial demonstrated the non-inferiority of weekly nab-PTX to weekly PTX in OS (median, 11.1 vs. 10.9 months; hazard ratio [HR = 0.97, 97.5% confidence interval (CI) 0.76–1.23; non-inferiority p = 0.0085], and improved trends in progression-free survival (PFS) (respective median, 5.3 vs. 3.8 months; HR = 0.88, 95% CI 0.73–1.06; p = 0.17) and overall response rate (ORR) (33% vs. 24%, p = 0.10) as second-line chemotherapy for AGC [5]. In addition, a single-arm phase II trial of nab-PTX + RAM and two retrospective studies of nab-PTX + RAM and PTX + RAM demonstrated promising and similar efficacy, respectively, as second-line chemotherapy for AGC [6,7,8]. Thus, nab-PTX + RAM is expected to be an alternative treatment to PTX-RAM and could be used instead of PTX + RAM in Japan. However, no comparative study of nab-PTX-RAM and PTX-RAM has been conducted thus far.
Here, we retrospectively analyzed the outcomes of the two treatments using propensity score matching to minimize the bias of patient backgrounds.
Patients and methods
Study design and patients
This was a multicenter retrospective study conducted at four institutions (National Hospital Organization, Shikoku Cancer Center, Matsuyama, Ehime, Japan; University of Tsukuba, Tsukuba, Ibaraki, Japan; Himeji Red Cross Hospital, Himeji, Hyogo, Japan; Kobe City Medical Center General Hospital, Kobe, Hyogo, Japan).
The major inclusion criteria were as follows: (a) unresectable advanced or recurrent gastric cancer (including esophagogastric junction cancer), (b) histologically confirmed adenocarcinoma, (c) age: ≥ 20 years, (d) Eastern Cooperative Oncology Group performance status (ECOG PS) of 0–2, (e) evaluable lesions, (f) refractoriness to first-line chemotherapy with the fluoropyrimidine-based regimen (including relapse ≤ 24 weeks after the final administration of fluoropyrimidine-based adjuvant chemotherapy), (g) receiving nab-PTX + RAM or PTX + RAM as second-line chemotherapy, and (h) initiation of second-line chemotherapy between January 2017 and June 2020. The major exclusion criteria were as follows: (i) history of previous administration of taxane or angiogenesis inhibitors and (j) lost to follow-up within 1 month of starting nab-PTX + RAM or PTX + RAM treatment.
Treatment
The nab-PTX + RAM regimen consisted of administration of 100 mg/m2 of nab-PTX intravenously over 30 min on days 1, 8, and 15 along with 8 mg/kg of RAM intravenously on days 1 and 15 of each 28-day cycle. The only premedication permitted was the histamine H1-receptor blocker prior to RAM infusion on days 1 and 15. The PTX + RAM regimen consisted of administration of 80 mg/m2 of PTX intravenously over 60 min on days 1, 8, and 15, along with 8 mg/kg of RAM intravenously on days 1 and 15 of each 28-day cycle. The permitted premedication was steroids and histamine H1 and H2-receptor blockers on days 1, 8, and 15. The attending physician determined each patient’s regimen. Nab-PTX + RAM was preferentially selected for the patients with alcohol intolerance, allergies, and underlying conditions (diabetes mellitus, non-tuberculosis mycobacterial infection, and so on) to avoid steroid use. In addition, drug cost, physician’s experience, and institution policy to reduce treatment time affected the choice of regimen. Dose reductions, including the initial dose, and skipping or delaying administration, were also determined according to each physician’s discretion. Treatment was continued until disease progression, unacceptable toxicity, patient refusal, or a physician’s decision to discontinue.
Endpoints and assessment
Efficacy was evaluated based on PFS, OS, and tumor response. Toxicity was evaluated according to the proportion of patients with Grade 3 or 4 adverse events (AEs). PFS was defined as the time from the initiation of study treatment to disease progression or death due to any cause. Disease progression was defined as radiological or clinical cancer progression. The patients underwent radiological examination every 8 ± 2 weeks. Patients who continued study treatment and discontinued treatment without disease progression were censored at the last confirmation of non-progressive disease by radiological examination. OS was defined as the time from the initiation of study treatment to death due to any cause. Survivors were censored at last contact. Tumor response was assessed based on the Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST ver. 1.1) [9] for patients with measurable lesions. ORR was defined as the proportion of patients who had the best response of complete response or partial response. Disease control rate (DCR) was defined as the proportion of patients who had the best response of complete response, partial response, or stable disease. AEs were graded based on the Common Terminology Criteria for Adverse Events version 5.0 (CTCAE ver. 5.0) [10]. Disease progression was decided by each physician. Tumor response and AEs were also assessed by each physician. Relative dose intensity (RDI) was defined as the ratio of actually delivered dose to the standard dose of drugs from the first to the last administration.
Statistical analysis
At first, we defined all patients who met the inclusion and exclusion criteria as the original cohort. Patient backgrounds and treatments are both known to affect efficacy and survival [11, 12]. Therefore, we used 1:1 propensity score matching to balance the patient background characteristics between the two treatment groups. Propensity scores were estimated using a multivariable logistic regression model that included six covariates [ECOG PS, histological tumor differentiation, presence of primary tumor, number of metastatic sites, peritoneal metastasis, and serum lactate dehydrogenase (LDH) level]. These covariates were identified by the multivariate analysis for OS in the original cohort (cutoff p < 0.20), and adopted confirming correspondence to the reported prognostic factors [11,12,13]. Then, the patients matched using the scores were defined as the matched cohort. The patient characteristics of the two treatment groups were compared using standardized differences. The efficacy and toxicity of the groups were compared in the matched cohort. Inverse probability of treatment weighting (IPTW) analysis was also performed as sensitivity analysis in the original cohort. Survival curves were generated using the Kaplan–Meier method. The PFS and OS rates were compared using the log-rank test. HR and 95% CI were estimated using the Cox proportional hazards model, as was subgroup univariate analysis. Fisher’s exact test was used to compare the ORR, DCR and toxicity of the groups. Wilcoxon rank sum test was used to compare the RDI and actually delivered dose of the groups. The follow-up time was estimated using the reverse Kaplan–Meier method. A standardized difference of < 0.10 was defined as statistically not different or well balanced [14]. All p values were two-sided, and statistical significance was set at p < 0.05. Statistical analyses were performed using JMP® 13 (SAS Institute Inc., Cary, NC, USA) and SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA).
Results
Patients
The flow chart for patient selection is shown in Fig. 1. Data of 265 patients treated with nab-PTX + RAM or PTX + RAM as second-line chemotherapy were collected from four institutions. After ineligible patients were excluded, 129 and 126 patients from the nab-PTX + RAM and PTX + RAM groups, respectively, were analyzed as the original cohort. The background characteristics of the patients in each treatment group are shown in Table 1. There were some imbalances between the two treatment groups, with the nab-PTX + RAM group exhibiting worse background characteristics (undifferentiated tumor, multiple number of metastatic sites, presence of primary tumor, peritoneal metastasis, and a high LDH level). After 1:1 propensity score matching, 190 (72%) patients were matched as 95 pairs. In this matched cohort, the patient background characteristics were balanced between the two treatment groups (Table 1).
In the matched cohort, 94 (99%) and 95 (100%) patients in the nab-PTX-RAM and PTX + RAM groups, respectively, discontinued study treatment. The most common reason for treatment discontinuation was disease progression, which affected 88 (93%) patients in each group (Online Resource 1). At the data cutoff time for analyses (September 2021), the median follow-up time for OS was 24.8 and 29.9 months in the nab-PTX + RAM and PTX + RAM groups, respectively. During the study period, 72 (76%) and 82 (86%) patients died in the nab-PTX + RAM and PTX + RAM groups, respectively.
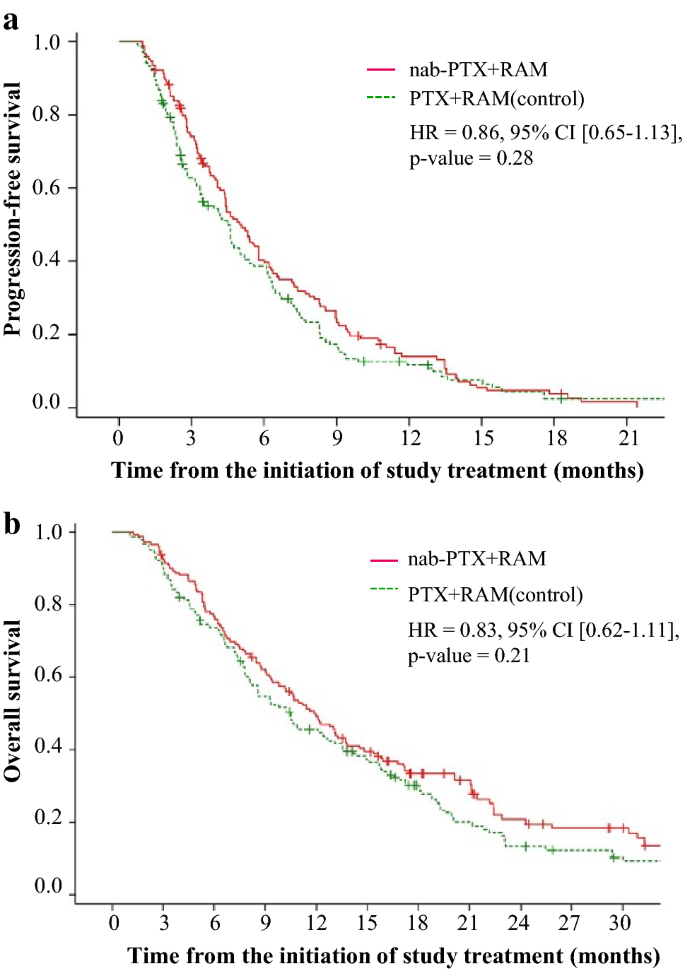
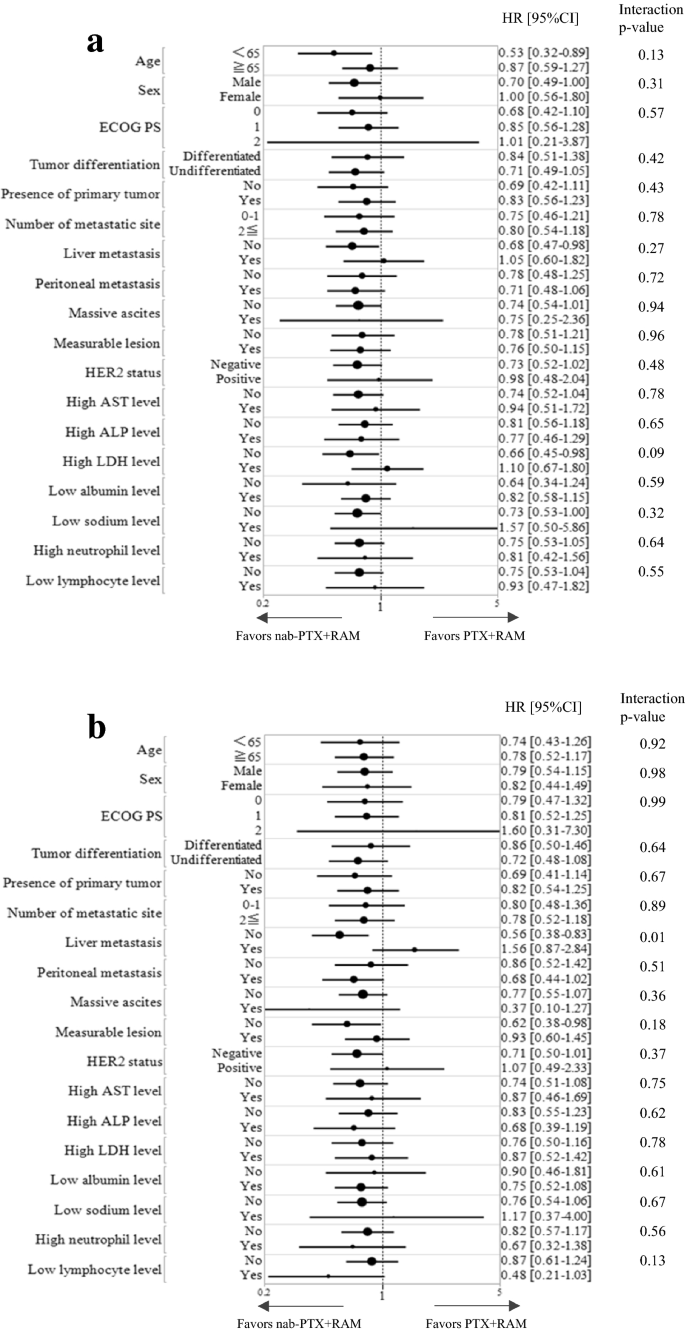
The median PFS was 5.3 (95% CI 4.4–6.3) and 4.7 (95% CI 3.2–5.3) months in the nab-PTX + RAM and PTX + RAM groups, respectively (HR = 0.76, 95% CI 0.56–1.03, p = 0.07) (Fig. 2a). The median OS was 11.5 (95% CI: 9.2–15.0) months in the nab-PTX + RAM group and 9.9 (95% CI 8.0–12.7) months in the PTX + RAM group (HR = 0.78, 95% CI 0.56–1.07, p = 0.12) (Fig. 2b). According to IPTW analysis, the HR of nab-PTX + RAM versus PTX + RAM for PFS was 0.86 (95% CI 0.65–1.13, p = 0.28) and that for OS was 0.83 (95% CI 0.62–1.11, p = 0.21) (Fig. 3). Subgroup analyses generally tended to favor nab-PTX + RAM in terms of PFS and OS (Fig. 4). The ORR was 40% and 37% in the nab-PTX + RAM and PTX + RAM groups, respectively (p = 0.84), and the DCR was 87% and 77% (p = 0.29), respectively (Table 2). Online Resource 2 shows the waterfall plots of tumor shrinkage of each patient. The mean depth of response was −21% (95% CI −12% to −30%) in the nab-PTX + RAM group and −14% (95% CI −3% to −25%) in the PTX + RAM group.
The proportion of patients with Grade 3 or 4 AEs in the nab-PTX + RAM group was higher than in the PTX + RAM group (86% vs. 69%, p < 0.01) (Table 3). The most common AE was a decrease in neutrophil count and more patients in the nab-PTX + RAM group developed this condition than in the PTX + RAM group (72% vs. 56%, p = 0.03). The incidence of febrile neutropenia was comparable between the groups (8% vs. 9%, p = 1.00). Grade 3 and 4 anemia tended to occur more frequently in the nab-PTX + RAM group than in the PTX + RAM group (26% vs. 17%, p = 0.15). No hypersensitivity reactions or treatment-related deaths occurred during either treatment.Table 3 Adverse events ≥ Grade3
The median RDI of taxane was 63% [interquartile range (IQR) 49–83] and 66% (IQR 51–83) in the nab-PTX + RAM and PTX + RAM groups, respectively (p = 0.50). The median actually delivered dose of taxane was 190 mg/m2/cycle (IQR 147–249) and 158 mg/m2/cycle (IQR 121–199) in the nab-PTX + RAM and PTX + RAM groups, respectively (p < 0.01). The median RDI of RAM was 85% (IQR 67–100) and 89% (IQR 71–100) in the nab-PTX + RAM and PTX + RAM groups, respectively (p = 0.28). The median actually delivered dose of RAM was 169 mg/m2/cycle (IQR: 134–200) and 178 mg/m2/cycle (IQR: 141–200) in the nab-PTX + RAM and PTX + RAM groups, respectively (p = 0.28).
Post-study treatment
Approximately 81% and 64% of patients in the nab-PTX + RAM and PTX + RAM groups received third-line chemotherapy and 40% and 34% received fourth-line chemotherapy, respectively. The proportions of patients by treatments in the nab-PTX + RAM and PTX + RAM groups were as follows: immune checkpoint inhibitors (nivolumab or pembrolizumab), 72% and 57%; irinotecan, 29% and 27%; trifluridine/tipiracil, 24% and 11%; and trastuzumab deruxtecan, 11% and 5% (Online Resource 3).
Discussion
To our knowledge, this is the first study to compare the efficacy and toxicity of nab-PTX + RAM versus PTX + RAM as second-line chemotherapy in multicenter and propensity score-matched patients with AGC. Nab-PTX + RAM exhibited more favorable trends in efficacy and more myelosuppressive AEs in toxicity, compared with PTX + RAM.
In terms of efficacy, nab-PTX + RAM exhibited favorable trends in PFS and OS compared to PTX + RAM, despite no statistically significant differences being observed. Sensitivity analyses using IPTW revealed similar results. The PFS and OS rates of the PTX + RAM group in our study were comparable to those observed in the RAINBOW trial [4]. In addition, as shown in Online Resource 4, the PFS and OS of nab-PTX + RAM in the previous two retrospective studies appeared favorable compared with those of PTX + RAM, or at least non-inferior. Forest plots of subgroup analyses of PFS and OS generally tended to favor nab-PTX + RAM. Nab-PTX appeared to have a better effect on peritoneal metastasis than PTX according to the exploratory subgroup analysis of the ABSOLUTE trial [15] and a retrospective study on nab-PTX + RAM and PTX-RAM [7], presumably due to the drug formulation of nab-PTX. However, this interaction between peritoneal metastasis and treatment was not observed in our study or in another retrospective study [8], and remained controversial. The ongoing P-SELECT trial (WJOG10617G) [16], a multicenter randomized phase II trial of nab-PTX + RAM versus PTX + RAM in second-line chemotherapy for AGC patients with peritoneal metastasis, may elucidate this finding. The current study demonstrated that ORR, DCR, and depth of response were comparable between the two treatments, which is equivalent to the results of other studies [7, 8].
Regarding toxicity, the proportion of patients with Grade 3 and 4 AEs was statistically higher in the nab-PTX + RAM group than in the PTX + RAM group. These were predominantly manageable hematological toxicities, such as a neutrophil count decrease and anemia. Although the RDIs of taxane and RAM were compatible between the two treatments, the actually delivered dose of taxane was statistically higher in the nab-PTX + RAM group than that in the PTX + RAM group, which seemed to explain the increase of hematological toxicities in the nab-PTX + RAM group. A retrospective study showed that the neutrophil count decrease observed in the patients receiving weekly PTX was strongly associated with better efficacy [17], and a prospective study demonstrated that PFS rates were better in patients treated with neutropenia-guided dose-escalation weekly PTX than in those receiving standard-dose weekly PTX [18]. Taken together with these findings, the higher incidence of neutrophil count decreased in nab-PTX + RAM might not be a disadvantage for efficacy. Considering that less than 10% of patients discontinued study treatment due to unacceptable toxicity and that treatment-related death did not occur due to either treatment, both treatments appear feasible in clinical practice. No hypersensitivity reactions were observed in either treatment group. As indicated in “Methods”, the only permitted premedication for nab-PTX + RAM was a histamine H1-receptor blocker, making this result remarkable. In addition, nab-PTX can be used in patients with alcohol intolerance and has a shorter administration time. Nab-PTX + RAM is, therefore, more convenient than PTX + RAM in clinical practice.
The proportions of patients who received later-line chemotherapy, primarily immune checkpoint inhibitors and trifluridine/tipiracil, differed between the two treatment groups. We speculated the main reason for the difference was the approval of nivolumab and trifluridine/tipiracil during the study period. They were approved as treatment for AGC in Japan in September 2017 and August 2019, respectively. As nab-PTX + RAM has been currently selected more frequently, the patients administered nab-PTX + RAM were considered to have more chance to access these drugs.
The present study has several limitations. First, this was a non-randomized retrospective study, and the sample size was small. Although we used propensity score matching to balance the patient background characteristics in the treatment groups, we could not adjust for unmeasured confounding factors, which might have affected the results. In addition, the sample size shrank further when matched pairs were made, which weakened the statistical power. Second, as mentioned above, the difference in proportion receiving post-study treatment might have partly affected OS. Considering this bias, OS data should be interpreted with caution.
In conclusion, nab-PTX + RAM exhibited favorable trends in terms of PFS and OS compared with PTX + RAM. Although hematological toxicity was of concern, it was manageable. Based on these results, further studies including randomized-controlled studies are warranted.
Liquid biopsy of circulating tumor DNA (ctDNA) is an “efficient” way to monitor resistance to trastuzumab (Herceptin, Genentech) and spot emerging resistance mechanisms in metastatic human epidermal growth factor receptor 2 (HER2)-positive gastric cancer, according to a study from China.
Up to 23% of gastric cancers are HER2+, but the response rate of these tumors to trastuzumab is limited, and any resistance to the drug happens rapidly during treatment, De-Shen Wang, MD, PhD, Department of Medical Oncology, Sun Yat-sen University Cancer Center, Guangzhou, China, told Medscape Medical News.
“Currently, the underlying mechanism of trastuzumab resistance remains unclear, and strategies to overcome resistance are urgently needed,” said Wang.
“We found that liquid biopsy-based ctDNA profiling could promisingly predict the tumor shrinkage and progression, and the underlying mechanism for innate resistance and acquired resistance of Herceptin might be different due to the differences of observed HER2 copy numbers,” Wang added.
Researchers evaluated the consistency between molecular alterations in solid tumor biopsies and liquid (plasma) biopsies by sequencing a panel of 416 cancer-related genes from 78 patients with gastric cancer (46 HER2+ and 32 HER2–). They also performed longitudinal analyses of 97 serial plasma samples collected from 24 patients who were HER2+ to track resistance during trastuzumab treatment and validate candidate resistance genes identified.
The molecular alterations detected in plasma provided a “good representation of the status of the tumor tissue, particularly at advanced stages,” the authors report in their article.
HER2 somatic copy number alterations (SCNA) were “highly consistent” with fluorescence in situ hybridization data, and the detected HER2 copy number variation was better than the plasma carcinoembryonic antigen level at predicting tumor shrinkage and progression, they note.
Most patients with innate trastuzumab resistance had high HER2 SCNA during progression compared with baseline, while HER2 SCNA decreased in patients with acquired resistance, they found.
PIK3CA/R1/C3 or ERBB2/4 mutations contributed “greatly” to resistance and led to worse progression free survival, whereas ERBB4 S774G mutation increased sensitivity to trastuzumab, Wang said.
The researchers also identified and confirmed NF1 as a resistance-related gene and found evidence that the combination of the HER2 inhibitor lapatinib (Tykerb, GlaxoSmithKline) and MEK/ERK inhibitor selumetinib (AstraZeneca) might overcome trastuzumab resistance.
“We propose that ctDNA profiling could provide helpful information to monitor the occurrence, dissect the potential molecular mechanisms, and provide helpful clues to therapy development for Herceptin resistance,” Wang told Medscape Medical News.
However, the technique, and this study, has several limitations, the authors note. First, although the 416-gene panel covered the majority of solid tumor-related genes, patients might have developed a mutation in a gene not covered by the panel. It’s also possible that the function of a protein encoded by a certain gene was regulated at the transcriptional, translational, or even post-translational level, and thus was not detected by DNA sequencing, they explain.
Second, they note that cell-free DNA (cfDNA) from plasma contains both cfDNA released from normal cells and ctDNA from limited tumor cells, leading to a lower tumor DNA content in the whole plasma cfDNA sample in most cases, which generates large amounts of “noise” and limits ctDNA detection sensitivity.
“A higher sequencing coverage depth might improve the detection sensitivity of ctDNA profiling to a certain extent but would not completely solve the problem due to the limited number of original tumor DNA molecules present in the cfDNA sample,” the authors suggest.
Objective Operative link on gastritis assessment (OLGA) staging for gastritis ranks the risk for gastric cancer (GC) in progressive stages (0–IV). This prospective study aimed at quantifying the cancer risk associated with each gastritis stage.
Design A cohort of 1755 consecutive patients with dyspepsia underwent initial (T-0) oesophagogastroduodenoscopy with mapped gastric biopsies, OLGA staging and assessment of Helicobacter pylori infection. Patients were followed for 55 months (median); patients with stages II III and IV underwent a second endoscopy/restaging (T-1), and those with stages 0 and I were followed clinically and through in-depth clinical and record checking. Endpoints were OLGA stage at T-1 and development of gastric epithelial neoplasia.
Results At T-0, 77.6% of patients had stage 0, 14.4% stage I, 5.1% stage II, 2.1% stage III and 0.85% stage IV. H. pylori infection was detected in 603 patients at T-0 and successfully eradicated in 602 of them; 220 had a documented history of H. pylori eradication; and 932 were H. pylori naïve-negative. Incident neoplastic lesions (prevalence=0.4%; low-grade intraepithelial neoplasia (IEN)=4; high-grade IEN=1; GC=2) developed exclusively in patients with stages III–IV. The risk for epithelial neoplasia was null in patients at stages 0, I and II (95% CI 0 to 0.4), 36.5 per 1000 person-years in patients at stage III (95% CI 13.7 to 97.4) and 63.1 per 1000 person-years in patients at stage IV (95% CI 20.3 to 195.6).
Conclusions This prospective study confirms that OLGA staging reliably predicts the risk for development of gastric epithelial neoplasia. Although no neoplastic lesions arose in H. pylori-naïve patients, the H. pylori eradication in subjects with advanced stages (III–IV) did not abolish the risk for neoplastic progression.
Peritoneal carcinomatosis is an increasingly common finding in gastric carcinoma. Previously, patients were treated as terminal, and median survival was poor. The use of cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) in this context is still highly debatable.
OBJECTIVE:
The aim of this study was to evaluate the long-term outcomes associated with CRS and HIPEC, and define prognostic factors for cure, if possible.
PATIENTS AND METHODS:
All patients with gastric carcinomatosis from five French institutions who underwent combined complete CRS and HIPEC and had a minimum follow-up of 5 years were included in this study. Cure was defined as a disease-free interval of more than 5 years from the last treatment until the last follow-up.
RESULTS:
Of the 81 patients who underwent CRS and HIPEC from 1989 to 2009, 59 had a completeness of cytoreduction score (CCS) of 0 (complete macroscopic resection), and the median Peritoneal Cancer Index (PCI) score was 6. Mitomycin C was the most commonly used drug during HIPEC (88 %). The 5-year overall survival (OS) rate was 18 %, with nine patients still disease-free at 5 years, for a cure rate of 11 %. All ‘cured’ patients had a PCI score below 7 and a CCS of 0. Factors associated with improved OS on multivariate analysis were synchronous resection (p = 0.02), a lower PCI score (p = 0.12), and the CCS (p = 0.09).
CONCLUSION:
The cure rate of 11 % for patients with gastric carcinomatosis who are deemed terminal emphasizes that CRS and HIPEC should be considered in highly selected patients (low disease extent and complete CRS).
The aim of this study was to determine the anticancer effects of seven licorice compounds in MKN-28, AGS, and MKN-45 gastric cancer cells and human gastric epithelium immortalized cells. We also explored the mechanism of action of licochalcone A (LCA), the most cytotoxic licorice compound, by analyzing its influence on cell cycle progression and apoptosis. The results indicated that LCA was the most cytotoxic licorice compound of those tested, and it inhibited gastric cancer cells growth in a dose-dependent manner, with an IC50 value of approximately 40μM. LCA affected gastric cancer cell viability by blocking cell cycle progression at the G2/M transition and inducing apoptosis. LCA treatment increased the expression of Rb and decreased the expression of cyclin A, cyclin B and MDM2 in MKN-28, AGS and MKN-45 cell lines. In addition, LCA-induced apoptosis by its effects on the expression of PARP, caspase-3, Bcl-2 and Bax. These data provide evidence that LCA has the potential to be used in the treatment of gastric cancer.