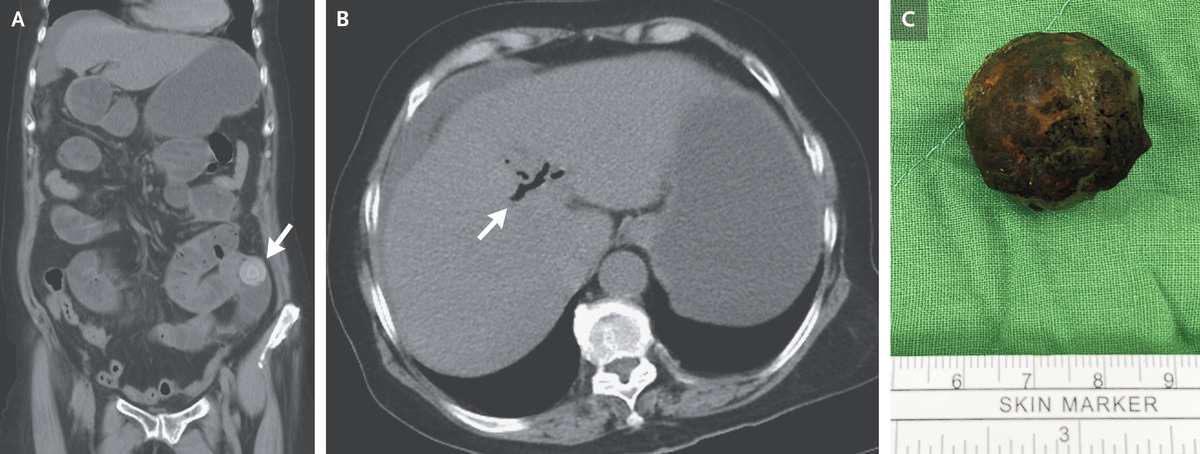
A 74-year-old woman with hypertension presented to the emergency department with a 3-day history of epigastric pain, nausea, vomiting, fever, chills, weakness, and poor appetite. She also reported having had no bowel movements or flatus for the past 2 days. Her blood pressure was 150/128 mm Hg, and her heart rate 144 beats per minute. An abdominal examination revealed tenderness in the periumbilical region and in the left lower quadrant, with voluntary guarding and rebound tenderness. There was no jaundice. Computed tomography of the abdomen revealed obstruction of the ileum caused by a gallstone (Panel A, arrow) and pneumobilia (Panel B, arrow). This combination of radiologic findings — an ectopic gallstone, small-bowel obstruction, and pneumobilia — is known as Rigler’s triad and aroused concern about gallstone ileus. Gallstone ileus is an uncommon cause of small-bowel obstruction, wherein a gallstone passes through a biliary–enteric fistula and becomes impacted within the intestinal lumen. The patient underwent a laparotomy, which confirmed gallstone ileus, and an enterotomy was performed to remove the gallstone (Panel C). Broad-spectrum antibacterial agents were administered after the procedure. The patient was discharged home on postoperative day 11 and was referred for an outpatient cholecystectomy.