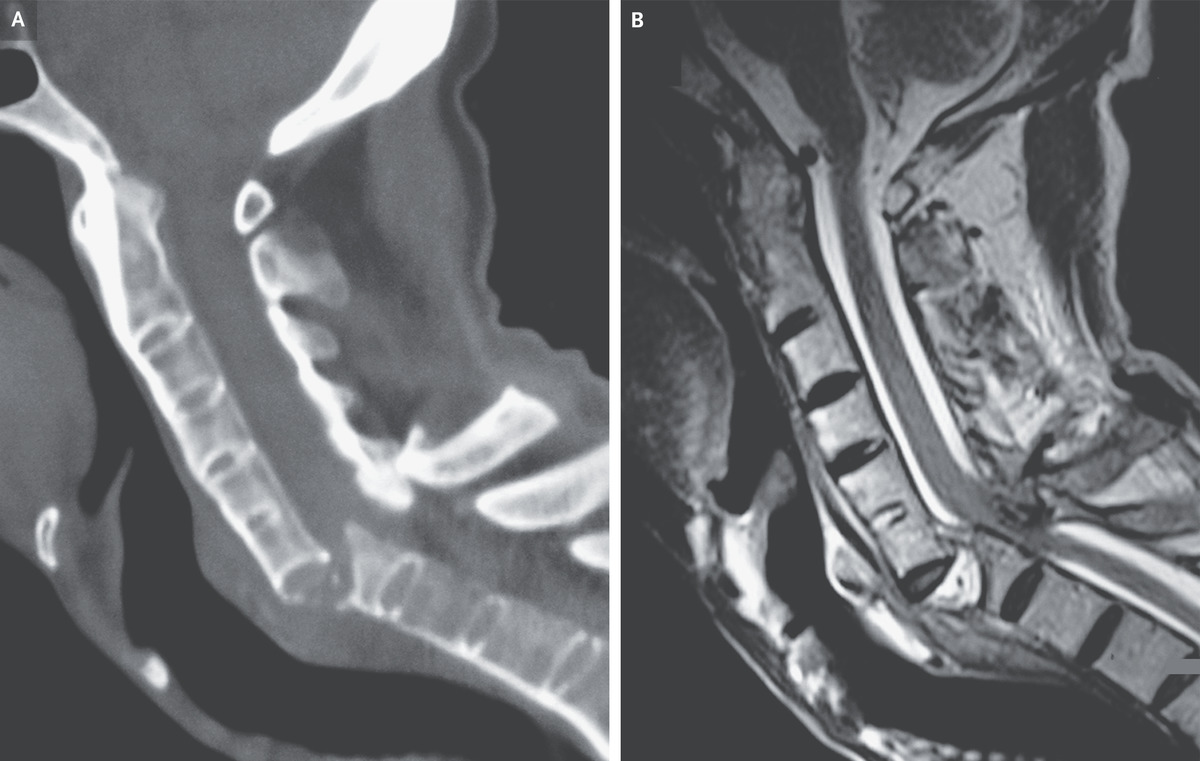
A 60-year-old man with a history of ankylosing spondylitis presented to the emergency department with neck pain and paralysis of the arms and legs after a fall. During the previous 5 years, he had not received treatment for the ankylosing spondylitis. At presentation, the blood pressure was 80/40 mm Hg and the heart rate was 56 beats per minute. Findings on physical examination were consistent with acute compression of the lower cervical spinal cord. Vasopressors were infused to treat neurogenic shock, and bladder catheterization was performed to treat acute urinary retention. Computed tomography of the cervical spine showed fused vertebrae with a displaced fracture — also known as a chalk-stick fracture — at the level of C6–C7 (Panel A). Magnetic resonance imaging of the cervical spine confirmed spinal cord compression at that level (Panel B). Ankylosis of the vertebrae results in increased bone fragility and risk of pathologic fracture. Neck or back pain after even minor trauma should prompt cross-sectional imaging to evaluate for serious injury. Surgical decompression and fusion of the spine were performed. Postoperatively, the patient regained function of his upper limbs but died from pneumonia 5 weeks later.
Among patients with various inflammatory conditions, exposure to glucocorticoids at doses as low as 5 mg per day may be associated with increased fracture risk, according to findings published in the Journal of Bone and Mineral Research.
“Fracture risk progressively increased with increasing levels of glucocorticosteroid exposure,” Akhila Balasubramanian, PhD, director with the Center for Observational Research at Amgen Inc., told Endocrine Today. “These trends were seen in the overall population as well as in patients younger than 50 years. We observed that fracture incidence in patients younger than 50 years who were exposed to glucocorticosteroids was as high as that observed in older (> 50 years) unexposed patients. Fracture risk decreased within months of steroid discontinuation.”
Balasubramanian and colleagues utilized the Truven Health MarketScan Commercial Claims and Encounters Database to follow 403,337 patients aged 18 to 64 years with rheumatoid arthritis (10%), asthma/chronic obstructive pulmonary disease (74%), irritable bowel disease (9%), multiple sclerosis, lupus and sarcoidosis. The researchers stratified fracture incidence rates per 1,000 person-years by prednisone-equivalent doses. They used Cox’s proportional hazard models to evaluate risk by daily and cumulative dose, and by time since cessation of glucocorticoids, adjusted for baseline characteristics.
At the end of follow-up, 72% patients had received systematic glucocorticoids during the study, according to researchers, with 69% of those exposed younger than 50 years. Sixty percent of exposed patients received cumulative doses of less than 675 mg (equivalent to 7.5 mg per day for 90 days), and 81% had short-term exposures between 1 and 90 cumulative days. Researchers identified 4,405 post-index fractures in the cohort, including 1,547 clinical vertebral fractures and 685 hip fractures.
Compared with incidence rates during unexposed time, fracture incidence approximately doubled in the presence of glucocorticoid exposures, even at the lowest daily doses of less than 5 mg per day (incidence rate = 9.33 per 1,000 person-years; 95% CI, 7.29-11.77) vs. unexposed (incidence rate = 4.87, 95% CI, 4.72-5.02), according to researchers. Results persisted in patients both older and younger than 50 years.
Unadjusted fracture incidence increased with increasing exposure for all exposure metrics, with very modest increases for peak dose, the researchers wrote.
Fracture incidence in patients with cumulative doses of 5,400 mg or higher (equivalent to 7.5 mg per day for 2 years), or patients with more than 365 days of glucocorticoid exposure, were nearly twice that of patients with cumulative doses ranging from 2,700 mg to 5,400 mg cumulative dose, or 81 to 365 days of glucocorticoid exposure. Fracture incidence in these patients with the highest doses and exposures were nearly triple that of unexposed patients, according to researchers.
Comparable patterns were revealed for clinical vertebral fractures and hip fractures, although daily dose for hip fractures did not exhibit the dose-response trend, the researchers wrote.
Adjusted HRs suggested significantly elevated fracture risk at daily doses as low as less than 5 mg per day, as well as a dose-response increase in fracture risk with increased cumulative dose. The risk at cumulative doses of less than 5,400 mg were roughly 2.5-fold higher vs. no exposure. Adjusted analyses stratified by cumulative dose corroborated the increased fracture risk at daily doses as low as less than 5 mg at cumulative doses greater than 5,400 mg.
Age-stratified descriptive analyses found a dose-dependent increase of fracture incidence with higher cumulative exposure to glucocorticoids in patients younger than 50 years and in patients aged 50 years or older.
In individuals younger than 50 years, there was a fracture incidence rate range of 2.44 per 1,000 person-years in never-exposed patients to five to six per 1,000 person-years in those with the highest cumulative exposures. Patients aged 50 years and older had incidence rate ranges between roughly six and 17 per 1,000 person-years based on exposure levels. There was an increase in fracture incidence rates at the lowest daily doses in both the younger and older patients; however, the older age group only showed a clear dose-response pattern of fracture incidence with higher daily doses. At doses of 5,400 mg or higher, patients younger than 50 years had incidence rates of 5.69 (95% CI, 4.32-7.35), whereas older patients had incidence rates of 17.10 (95% CI, 14.97-19.45).
Fracture risk decreased significantly within months after glucocorticoid discontinuation, according to researchers.
“The literature indicates that bone loss and associated fracture risk is often not well managed among patients using glucocorticosteroid therapy,” Balasubramanian said. “Based on the findings of our study as well as previous studies, physicians treating their patients with glucocorticosteroid therapy would be well advised to monitor and manage the bone health of these patients, including consideration of appropriate treatments for reduction of fracture risk.” – by Jennifer Byrne
For more information:
Akhila Balasubramanian, PhD, can be reached at aromano@webershardwick.com.
Disclosures: Amgen supported this study. Balasubramanian reports she is an employee of and stockholder in Amgen. Please see the study for the other authors’ relevant financial disclosures.
Correction: Sixty-nine percent of those exposed younger than 50 years, and the risk at cumulative doses of less than 5,400 mg were roughly 2.5-fold higher vs. no exposure. Endocrine Today regrets the error.
Glucocorticoids are used to treat many chronic inflammatory conditions. Adverse effects of long-term glucocorticoid therapy include disruption of bone remodeling, decrease in bone mineral density and increased fracture risk. Most patients on glucocorticoids are not being treated to mitigate the undesirable skeletal effects. A better understanding of the skeletal effects of glucocorticoids in diverse groups of patients may lead to more effective treatment.
The report by Balasubramanian and colleagues described the findings of a retrospective analysis of a large administrative claims database with chronic inflammatory diseases. This included more than 400,000 patients who were newly diagnosed with rheumatoid arthritis, asthma/chronic obstructive lung disease, inflammatory bowel disease, multiple sclerosis, lupus or sarcoidosis, 72% of whom had exposure to glucocorticoids.
Over 5 years with more than 2.4 million person-years of observation, 4,405 incident fractures were identified, including 1,547 clinical vertebral fractures and 685 hip fractures. Fracture rates were elevated in patients younger than 50 years of age as well as in those 50 years and older. The risk of fractures was greater with increasing levels of glucocorticoid exposure, but the risk was also elevated with prednisone equivalent doses of less than 5 mg per day. Fracture risk decreased within months of stopping glucocorticoids.
This study adds to the body of knowledge concerning the adverse skeletal effects of glucocorticoids. The findings suggest that we should be vigilant for potential skeletal harm with glucocorticoids, even in younger patients treated with low doses. Pharmacological therapy for glucocorticoid-induced osteoporosis should be used according to well-established guidelines. It is reassuring that fracture risk rapidly diminishes with discontinuation of glucocorticoids.
E. Michael Lewiecki, MD
Director of New Mexico Clinical Research & Osteoporosis Center Director of Bone Health TeleECHO at University of New Mexico Health Sciences Center
Publication of the National Institute for Health and Care Excellence (NICE) guidelines on use of antiosteoporosis agents for the secondary prevention of osteoporotic fractures in 2005, coupled with the release of generic alendronate shortly thereafter, led to a spike in use of bisphosphonates in England and Wales and a clinically meaningful reduction in subsequent fractures among hip-fracture patients, a new large-scale observational study indicates.
“It is clear that the guidance, coupled with the availability of a low-cost bisphosphonate, drove a major change in prescribing by general practitioners,” senior author of the work, Andrew Judge, MD, University of Oxford, United Kingdom, says in a statement.
“It is unclear how much this was due to the new guidance and how much due to generic alendronic acid arriving on the market, but it is notable that prescriptions for alendronic acid clearly outstrip those for other treatments, suggesting that it had a part to play,” he adds.
The study results were published online July 6 in the Journal of Bone and Mineral Research.
Lead author Samuel Hawley, DPhil candidate, University of Oxford, United Kingdom, and colleagues conducted the REFReSH study by identifying 10,873 individuals who had sustained a hip fracture in England or Wales anywhere between April 1999 and September 2012.
The prescribing patterns of physicians for osteoporosis treatments among hip-fracture patients in England and Wales were then tracked following publication of the NICE guidelines in January 2005 and for the first three years following the introduction of generic alendronate, which came shortly thereafter.
The publication of the guidelines and the release of generic alendronate were considered the “intervention,” and prescribing and fracture rates were documented before and after the start of the intervention period.
Overall, Mr Hawley and colleagues estimate there was a 17.2% absolute increase in the use of antiosteoporosis agents within a year of patients sustaining their initial hip fracture across the 3-year observational interlude.
This increase represented a relative increase of 79% compared to the “preintervention” period.
The incidence of subsequent major refracture, defined as fractures of the hip, pelvis, proximal-humerus, rib, spine, or wrist/forearm, prior to the intervention was stable at 6.3%.
Following the intervention, “there was a significant (P = .001) downward trend by -0.19% per 6 months,” Mr Hawley notes.
This downward trend translated into an approximate 14% relative decrease in the risk of major refracture rates over a period of 3 years after the start of the intervention period.
The same trend was seen for subsequent hip fracture.
Initially, hip refracture rates were stable at a rate of 3.8% prior to the introduction of the intervention. Following the intervention, there was again a downward trend in hip refracture rates of -0.17% for every 6 months (P = .001), which translated into a 22% reduction in hip fractures over a period of 3 years.
Mr Hawley and colleagues caution that while the observed decrease in the incidence of refracture rates did dovetail with an increase in prescriptions for bisphosphonates, “we have not been able to establish whether increased prescribing caused the reduction in subsequent fracture.”
However, as they also note, evidence from randomized controlled trials suggests that alendronate does reduce the risk of hip fracture relative to placebo.
Other changes in the UK healthcare system, including initiation of the Fracture Liaison Service model of care, may also have contributed to the decline in fractures over the study interval, they suggest.
Bisphosphonate therapy, the first-line treatment for patients with osteoporosis, usually doesn’t restore normal bone-mineral density (BMD) and sometimes is not well-tolerated. Teriparatide (Forteo; a parathyroid hormone analog that stimulates bone formation when injected daily) and denosumab (Prolia; a long-acting injectable agent that inhibits bone resorption) are approved for treating patients with osteoporosis and high fracture risk. Combinations of bisphosphonates with teriparatide have proven to be no more effective than either agent alone, but the combination of teriparatide and denosumab has not been studied.
In a partially industry-funded study, investigators randomized 100 postmenopausal women at high risk for fracture to receive teriparatide (20 µg subcutaneously daily), denosumab (60 mg subcutaneously every 6 months), or both for 1 year. At 12 months, BMD increased significantly more in the combination group than in the monotherapy groups at the lumbar spine (9.1% vs. 6.2% and 5.2%, respectively) and at the hip. Serious adverse events in all three groups were deemed to be unrelated to study treatments.
Comment: Although only indirect comparisons can be made, combination teriparatide and denosumab seems to increase BMD more than other approved therapies do. However, this combination would need to substantially improve clinical outcomes — not just surrogate markers — to justify its very high cost (about US$9000 annually, compared with $100 annually for alendronate). Although BMD is a reliable predictor of fractures, in future studies, researchers will need to assess directly the effects of combination teriparatide and denosumab on fractures and its long-term safety.
In a 2007 study, once-yearly infusions of the bisphosphonate drug zoledronic acid (Reclast, Aclasta) lowered the incidence of fractures in postmenopausal women (JW Gen Med May 2 2007). Now, in another industry-sponsored randomized trial, 1199 men (age range, 50–85) at high risk for fractures received zoledronic acid (5-mg dose, given intravenously at baseline and at 12 months) or placebo. The study was open to men with osteoporosis defined by bone-density testing and to men with osteopenia plus one to three mild-to-moderate vertebral fractures identified by lateral spine radiographs.
At 2 years, the proportion of men with new radiographic vertebral fractures was significantly lower in the zoledronic acid group than in the placebo group (1.6% vs. 4.9%). A small difference in incidence of symptomatic vertebral or nonvertebral fractures (1.0% vs. 1.8%) did not reach significance. About 20% to 25% of zoledronic acid recipients developed fever, myalgia, or arthralgia (compared with about 5%–10% of placebo recipients), but the duration of these adverse effects was not reported. No cases of jaw osteonecrosis or atypical femoral fractures were noted, but myocardial infarction occurred in nine zoledronic acid recipients and in two placebo recipients (P=0.03).
Comment: A once-yearly infusion of zoledronic acid significantly lowered the incidence of radiographic vertebral fractures, but not clinical fractures, in this 2-year study in men. Infusions of this drug are known to cause transient flu-like symptoms; however, the small excess of myocardial infarctions was unexpected and is of some concern. In the trial in women that was cited above, zoledronic acid recipients experienced a higher incidence of serious atrial fibrillation (but not myocardial infarctions).