Survey data show 63% of midlife women reported “not feeling like myself” half the time or more over 3 months.
Symptoms most correlated with “not feeling like myself” included fatigue, overwhelm and low feelings.
The menopausal transition can be associated with a variety of bothersome symptoms, including hot flashes and mood swings, but some women might experience more subtle symptoms that can begin years before the final menstrual period.
“Not feeling like myself” is a phrase often used by women on the path to menopause — when symptoms related to mood or cognition arise that impact their daily lives, according to Nina Coslov, MBA, founder of Women Living Better, an organization focused on understanding and improving the perimenopausal years through education and research.
In a recent survey of more than 1,300 women aged 35 to 55 years who met criteria for the late-reproductive stage or menopausal transition, 63.3% of women reported “not feeling like myself” at least 50% of the time during the past 3 months. Researchers then correlated 61 individual symptoms and symptom-bother scale scores with the phrase “not feeling like myself.”
After accounting for education level and overall stress ratings, “not feeling like myself” was most strongly predicted by the symptom groups of anxiety/vigilance, fatigue/pain, brain fog, sexual symptoms and volatile mood symptoms.
“Because these symptom groups have not been typically associated with the menopausal transition, they may represent inexplicable and unfamiliar feelings and responses for which women lack an explanatory model and thus use the phrase, ‘I’m not feeling like myself,’” the researchers wrote.
The latest survey data build on earlier work conducted by Coslov and colleagues that found women in the late reproductive stage experience symptoms strikingly similar to those often associated with the menopausal transition.
Healio spoke with Coslov about the use of the phrase “not feeling like myself,” the symptoms women report while still having regular menstrual cycles, and the importance of educating clinicians and patients about the late reproductive phase. The latest data from the Women Living Better survey were recently published in Menopause.
Healio: Why center a survey question on the phrase “not feeling like myself”?
Coslov: “Not feeling like myself” was one element in a much bigger survey that we conducted in 2020. This is the seventh paper coming from that survey. “Not feeling like myself” is a phrase I had heard through talking to many people. Women Living Better, which launched in 2018, serves as a repository of people’s experiences through submissions to the website, and that is where a lot of the questions that comprised this survey came from. We tried to use women’s words to describe their symptoms.
I had used the phrase myself early in perimenopause. I remember going for a walk with a friend and saying, “I just don’t feel like myself and I don’t’ know what is going on.”
When we were designing the survey, co-author Marcie K. Richardson, MD, said, “I hear that all the time. It is vague and it is difficult to know what it means.” We discussed how it is much easier during a time-pressed appointment to focus on more straightforward symptoms typically associated with menopause, such as, “Do you have hot flashes? Do you have vaginal dryness?” “Not feeling like myself” is nonspecific. So, we decided to put the question out there.
In this piece of research, we used, in two different statistical approaches to determine what bothersome symptoms were associated with this phrase. The way we asked the question was, “What percent of the time over the last 3 months have you not felt like yourself?” Approximately 63.3% of women reported not feeling like themselves 50% of the time or more. That is a lot.
Healio: Did the number of women who reported not feeling like themselves surprise you?
Coslov: It did a little bit. With this work, we are trying to normalize and validate experiences for women. The hope is that when many women understand that most of these symptoms are part of the perimenopausal period of fluctuating hormones and that it is not a permanent state, they will feel less worried or scared That is not to say that anyone should suffer — when symptoms are disrupting daily activities, seeking medical care can help. But for most women, knowing that these experiences of mood and sleep changes or just feeling “off” are normal can go a long way. That plays into not feeling like myself: Not having an explanatory model for what is happening.
Our research was cross-sectional, it was one point in time, but we had a lot of participants. They were a convenience sample, recruited through email and on social media, who were willing to take a survey about their midlife experience. When we set out to establish what symptoms were correlated, I did not know what would come up. Mood is strikingly associated. So are fatigue and brain fog symptoms. I would have felt so much better if someone had been able to tell me that that these things are commonly associated with perimenopause.
Healio: What does Women Living Better hope to do with these data?
Coslov:We want to normalize and validate what people are experiencing. We had a poster at The Menopause Society Annual Meeting in September about these data, and so many providers came up and said, “I hear this all the time.” Now, they can reference this study. They can follow up with specifics when they hear, “I’m just not feeling like myself.” We hope it will allow patients and providers to feel more connected and help start conversations about mood changes or brain fog. Ultimately, I hope it leads to more successful and satisfying health care interactions for both parties.
Healio: What are your plans going forward, beyond this latest survey data?
Coslov: To me, mood is the most under-researched and most misunderstood area on the path to menopause. Just like in our early work, we would focus on to what degree experiences with mood changes are happening before noticeable, significant menstrual cycles changes vs. after.
Once you say, “Oh, I’ve skipped a period” or, “I’ve had 60 days between periods,” most providers will recognize perimenopause. But for many women, these subtle [hormonal] changes begin before significant menstrual cycle changes. That is when it is most surprising, concerning — unexpected. That is when most health care providers do not identify and validate, and cannot validate, that this is the beginning of the path to menopause.
According to STRAW+10 criteria, the beginning of the menopausal transition is defined as two times where consecutive cycle length differ by 7 days or more. The problem is thatmany people experience the impact of fluctuating hormones before that. That is why I use this broader phrase: the path to menopause. A focus on the late reproductive stage, the official term of what comes before perimenopause as defined by STRAW, has been a major focus of Women Living Better’s effort and research.
We also hope to reach out to more women aged 38 to 42 years. In terms of timing, that age range is the holy grail. Those women need to know what might be coming and that it is generally normal.
Most people regularly commit to a 120 percent life, stretched beyond their limits. (Rido/Shutterstock)
0:006:03
The busy modern person has much to do and worry about every day. Many of us work long hours and get little sleep. The occurrence of three meals a day at set times is increasingly rare. Various life pressures exhaust the body and mind, and issues like insomnia, memory loss, anxiety, fear, and depression are increasingly common. In a word, it’s fatigue.
Many people think that getting more sleep and rest is the answer to all of these ills, but actually, this is not the answer to fatigue, as we learned from Dr. Wu Kuo-Pin, director of Taiwan Hsinyitang Chinese Medicine Clinic.
But isn’t sleep the cure-all we were led to believe?
“There are many causes of fatigue. We need to understand which type of fatigue we have so that we can prescribe the right remedy to get the best results,” Dr. Wu said.
Physiological Fatigue
Physiological fatigue is physical fatigue, which is caused by the body being overworked and unable to properly handle the metabolites produced by the hard work.
“The more waste accumulated in the body, the more muscle soreness,” Dr. Wu said. “The lack of adequate nutrient supply to the tissues and organs will lead to weakness and tiredness of the limbs.”
This kind of physical fatigue is often an occupational disease, which may be caused by maintaining a certain posture or doing a certain kind of action for a long time, the doctor explained. “Therefore, in order to improve physiological fatigue, we should pay attention to whether there are deviations or excesses in posture or movement, and do some stretching exercises to loosen up and to prevent and relieve physiological fatigue.”
Mental Fatigue
The main cause of mental fatigue is prolonged mental stress. Only rest or sleep is not very effective to relieve this type of fatigue.
“It requires holistic solutions of both body and mind to release the pressure or suppressed emotions,” Dr. Wu said. This is what many people seek out therapists for.
“In other words, we must take the weight off our mind and thoroughly solve and let go of the disturbance in order to truly eliminate mental fatigue and restore health.”
Brain Fatigue
Brain fatigue is due to long hours of thinking or focusing on something, which generates the feeling of burnout.
“Excessive use of the brain will cause the brain to consume a lot of oxygen, resulting in a lack of oxygen supply to the brain. Thus, carbon dioxide can not be metabolized smoothly, and the brain fatigue will occur, accompanied sometimes by dizziness, headache, nausea, memory loss, and other symptoms,” Dr. Wu said.
In these cases, sometimes the simple solution of breathing exercises can yield great results.
“When this fatigue occurs, you can stand up and do chest-expanding and deep breathing exercises to inhale a large amount of oxygen into the lungs,” Dr. Wu instructed.
“Then move the cervical spine, and comb the hair so that the blood quickly and smoothly flows toward the brain, eliminating the brain fatigue.”
But these are short term and immediate remedies, not long-lasting ones.
“However, the best way is to readjust the pace of life, review your workload and rest time, and strike a balance between the two,” Dr. Wu added.
Subjective Fatigue
Subjective fatigue can be described as “exhaustion,” a state of feeling powerless about yourself or anything else. Subjective fatigue is usually caused by personal emotions.
“The common situation is that you are very committed to your work over a period of time, but that your efforts are not rewarded or recognized. After a period of time, your enthusiasm and motivation gradually wear off,” Dr. Wu said. This differs from mental fatigue which may have to do more with being overwhelmed, as subjective fatigue results in more of a loss of motivation rather than an anxious state.
“It is necessary to rekindle the enthusiasm. Try to shift part of your attention to other activities, or change your work style and learning methods,” Dr. Wu said, adding that it is a time for learning the importance of “letting go” of things.
“Do not care too much about what others may think of you, and follow your own way of life in order to truly get rid of this pain.”
Fatigue Caused by an Imbalanced Diet
This fatigue is caused by a long-term preference for a certain type of food or not eating a certain type of food, resulting in nutritional imbalance and health problems. Large percentages of Americans today have nutritional deficiencies in many essential minerals and vitamins.
Dr. Wu said explained an ancient view of a balanced diet. “An ancient Chinese medical book—Huangdi Neijing (literally meaning “The Yellow Emperor’s Classic of Internal Medicine”)—talks about the importance of a balanced diet and how to combine different types of food in a balanced way.”
The book says, “The five grains are the main sources for growth; the five fruits provide complementary nourishment; the five livestock are the main sources of energy; and the five vegetables are the main sources of supplement. The intake of them combined in a balanced way will help the body stay healthy and energetic.”
Modern research has also shown that variety is essential to a healthy gut microbiome.
“Huangdi Neijing embodies ancient Chinese wisdom and understanding of the universe and its relationship with the human being. It is the most important ancient text in Chinese medicine as well as a major book of Daoist theory and lifestyle,” Dr. Wu explained.
“Following ancient Chinese wisdom, we need to eat a balanced diet according to each individual’s physique to relieve fatigue and to stay healthy.”
Most people regularly commit to a 120 percent life, stretched beyond their limits. (Rido/Shutterstock)
0:006:03
The busy modern person has much to do and worry about every day. Many of us work long hours and get little sleep. The occurrence of three meals a day at set times is increasingly rare. Various life pressures exhaust the body and mind, and issues like insomnia, memory loss, anxiety, fear, and depression are increasingly common. In a word, it’s fatigue.
Many people think that getting more sleep and rest is the answer to all of these ills, but actually, this is not the answer to fatigue, as we learned from Dr. Wu Kuo-Pin, director of Taiwan Hsinyitang Chinese Medicine Clinic.
But isn’t sleep the cure-all we were led to believe?
“There are many causes of fatigue. We need to understand which type of fatigue we have so that we can prescribe the right remedy to get the best results,” Dr. Wu said.
Physiological Fatigue
Physiological fatigue is physical fatigue, which is caused by the body being overworked and unable to properly handle the metabolites produced by the hard work.
“The more waste accumulated in the body, the more muscle soreness,” Dr. Wu said. “The lack of adequate nutrient supply to the tissues and organs will lead to weakness and tiredness of the limbs.”
This kind of physical fatigue is often an occupational disease, which may be caused by maintaining a certain posture or doing a certain kind of action for a long time, the doctor explained. “Therefore, in order to improve physiological fatigue, we should pay attention to whether there are deviations or excesses in posture or movement, and do some stretching exercises to loosen up and to prevent and relieve physiological fatigue.”
Mental Fatigue
The main cause of mental fatigue is prolonged mental stress. Only rest or sleep is not very effective to relieve this type of fatigue.
“It requires holistic solutions of both body and mind to release the pressure or suppressed emotions,” Dr. Wu said. This is what many people seek out therapists for.
“In other words, we must take the weight off our mind and thoroughly solve and let go of the disturbance in order to truly eliminate mental fatigue and restore health.”
Brain Fatigue
Brain fatigue is due to long hours of thinking or focusing on something, which generates the feeling of burnout.
“Excessive use of the brain will cause the brain to consume a lot of oxygen, resulting in a lack of oxygen supply to the brain. Thus, carbon dioxide can not be metabolized smoothly, and the brain fatigue will occur, accompanied sometimes by dizziness, headache, nausea, memory loss, and other symptoms,” Dr. Wu said.
In these cases, sometimes the simple solution of breathing exercises can yield great results.
“When this fatigue occurs, you can stand up and do chest-expanding and deep breathing exercises to inhale a large amount of oxygen into the lungs,” Dr. Wu instructed.
“Then move the cervical spine, and comb the hair so that the blood quickly and smoothly flows toward the brain, eliminating the brain fatigue.”
But these are short term and immediate remedies, not long-lasting ones.
“However, the best way is to readjust the pace of life, review your workload and rest time, and strike a balance between the two,” Dr. Wu added.
Subjective Fatigue
Subjective fatigue can be described as “exhaustion,” a state of feeling powerless about yourself or anything else. Subjective fatigue is usually caused by personal emotions.
“The common situation is that you are very committed to your work over a period of time, but that your efforts are not rewarded or recognized. After a period of time, your enthusiasm and motivation gradually wear off,” Dr. Wu said. This differs from mental fatigue which may have to do more with being overwhelmed, as subjective fatigue results in more of a loss of motivation rather than an anxious state.
“It is necessary to rekindle the enthusiasm. Try to shift part of your attention to other activities, or change your work style and learning methods,” Dr. Wu said, adding that it is a time for learning the importance of “letting go” of things.
“Do not care too much about what others may think of you, and follow your own way of life in order to truly get rid of this pain.”
Fatigue Caused by an Imbalanced Diet
This fatigue is caused by a long-term preference for a certain type of food or not eating a certain type of food, resulting in nutritional imbalance and health problems. Large percentages of Americans today have nutritional deficiencies in many essential minerals and vitamins.
Dr. Wu said explained an ancient view of a balanced diet. “An ancient Chinese medical book—Huangdi Neijing (literally meaning “The Yellow Emperor’s Classic of Internal Medicine”)—talks about the importance of a balanced diet and how to combine different types of food in a balanced way.”
The book says, “The five grains are the main sources for growth; the five fruits provide complementary nourishment; the five livestock are the main sources of energy; and the five vegetables are the main sources of supplement. The intake of them combined in a balanced way will help the body stay healthy and energetic.”
Modern research has also shown that variety is essential to a healthy gut microbiome.
“Huangdi Neijing embodies ancient Chinese wisdom and understanding of the universe and its relationship with the human being. It is the most important ancient text in Chinese medicine as well as a major book of Daoist theory and lifestyle,” Dr. Wu explained.
“Following ancient Chinese wisdom, we need to eat a balanced diet according to each individual’s physique to relieve fatigue and to stay healthy.”
It may seem obvious but you could be getting too little sleep. That can negatively affect your concentration and health. Adults should get seven to eight hours every night.
Fix: Make sleep a priority and keep a regular schedule. Ban laptops, cell phones, and televisions from your bedroom. Still having trouble? Seek help from a doctor. You may have a sleep disorder.
Fatigue Cause No. 2: Sleep Apnea
2/15
Some people think they’re sleeping enough, but sleep apnea gets in the way. It briefly stops your breathing throughout the night. Each interruption wakes you for a moment, but you may not be aware of it. The result: you’re sleep-deprived despite spending eight hours in bed. Your doctor may order a sleep study to check for this.
Fix: Lose weight if you’re overweight, quit smoking, and you may need a CPAP device to help keep your airway passages open while you sleep.
Fatigue Cause No. 3: Not Enough Fuel
3/15
Eating too little causes fatigue, but eating the wrong foods can also be a problem. Eating a balanced diet helps keep your blood sugar in a normal range and prevents that sluggish feeling when your blood sugar drops.
Fix: Always eat breakfast and try to include protein and complex carbs in every meal. For example, eat eggs with whole-grain toast. Also eat small meals and snacks throughout the day for sustained energy.
Fatigue Cause No. 4: Anemia
4/15
Anemia is one of the leading causes of fatigue in women. Menstrual blood loss can cause an iron deficiency, putting women at risk. Red blood cells (shown here) are needed because they carry oxygen to your tissues and organs.
Fix: For anemia caused by an iron deficiency, taking iron supplements and eating iron-rich foods, such as lean meat, liver, shellfish, beans, and enriched cereal, can help.
Fatigue Cause No. 5: Depression
5/15
You may think of depression as an emotional disorder, but it contributes to many physical symptoms, as well. Fatigue, headaches, and loss of appetite are among the most common symptoms. If you feel tired and “down” for more than a few weeks, see your doctor.
Fix: Depression responds well to talk therapy and/or medication.
Fatigue Cause No. 6: Hypothyroidism
6/15
The thyroid is a small gland at the base of your neck. It controls your metabolism, the speed at which your body converts fuel into energy. When the gland is underactive and the metabolism functions too slowly, you may feel sluggish and put on weight.
Fix: If a blood test confirms your thyroid hormones are low, synthetic hormones can bring you up to speed.
Fatigue Cause No. 7: Caffeine Overload
7/15
Caffeine can improve alertness and concentration in moderate doses. But too much can increase heart rate, blood pressure, and jitteriness. And research indicates too much actually causes fatigue in some people.
Fix: Gradually cut back on coffee, tea, chocolate, soft drinks, and any medications that contain caffeine. Stopping suddenly can cause caffeine withdrawal and more fatigue.
Fatigue Cause No. 8: Hidden UTI
8/15
If you’ve ever had a urinary tract infection (UTI), you’re probably familiar with the burning pain and sense of urgency. But the infection does not always announce itself with such obvious symptoms. In some cases, fatigue may be the only sign. A urine test can quickly confirm a UTI.
Fix: Antibiotics are the cure for UTIs, and the fatigue will usually vanish within a week.
Fatigue Cause No. 9: Diabetes
9/15
In people with diabetes, abnormally high levels of sugar remain in the bloodstream instead of entering the body’s cells, where it would be converted into energy. The result is a body that runs out of steam despite having enough to eat. If you have persistent, unexplained fatigue, ask your doctor about being tested for diabetes.
Fix: Treatments for diabetes may include lifestyle changes such as diet and exercise, insulin therapy, and medications to help the body process sugar.
Fatigue Cause No. 10: Dehydration
10/15
Your fatigue can be a sign of dehydration. Whether you’re working out or working a desk job, your body needs water to work well and keep cool. If you’re thirsty, you’re already dehydrated.
Fix: Drink water throughout the day so your urine is light colored. Have at least two cups of water an hour or more before a planned physical activity. Then, sip throughout your workout, and afterward drink another two cups.
Fatigue Cause No. 11: Heart Disease
11/15
When fatigue strikes during everyday activities, such as cleaning the house or weeding the yard, it can be a sign that your heart is no longer up to the job. If you notice it’s becoming increasingly difficult to finish tasks that were once easy, talk to your doctor about heart disease.
Fix: Lifestyle changes, medication, and therapeutic procedures can get heart disease under control and restore your energy.
Fatigue Cause No. 12: Shift Work Sleep Disorder
12/15
Working nights or rotating shifts can disrupt your internal clock. You may feel tired when you need to be awake. And you may have trouble sleeping during the day.
Fix: Limit your exposure to daylight when you need to rest. Make your room dark, quiet, and cool. Still having sleep issues? Talk with your doctor. Supplements and medications may help.
Fatigue Cause No. 13: Food Allergies
13/15
Some doctors believe hidden food allergies can make you sleepy. If your fatigue intensifies after meals, you could have a mild intolerance to something you’re eating — not enough to cause itching or hives, just enough to make you tired.
Fix: Try eliminating foods one at a time to see if your fatigue improves. You can also ask your doctor about a food allergy test.
Fatigue Cause No. 14: CFS and Fibromyalgia
14/15
If your fatigue lasts more than six months and is so severe that you can’t manage your daily activities, chronic fatigue syndrome or fibromyalgia are a possibility. Both can have various symptoms, but persistent, unexplained exhaustion is a main one.
Fix: While there’s no quick fix for CFS or fibromyalgia, patients often benefit from changing their daily schedule, learning better sleep habits, and starting a gentle exercise program.
Fast Fix for Mild Fatigue
15/15
If you have mild fatigue that isn’t linked to any medical condition, the solution may be exercise. Research suggests healthy but tired adults can get a significant energy boost from a modest workout program. In one study, participants rode a stationary bike for 20 minutes at a mild pace. Doing this just three times a week was enough to fight fatigue.
“Although generally considered asymptomatic, almost half of patients with NASH have clinically significant fatigue which, in turn, has a profound negative impact on the overall patient experience,” Zobair M. Younossi, MD,MPH, president of Inova Medicine Services and professor and chairman of the department of medicine at Inova Fairfax Medical Campus in Virginia, and colleagues wrote in Clinical Gastroenterology and Hepatology. “In this context, ongoing clinical trials aim at finding a drug-based therapy for NASH that may reverse fibrosis and could also potentially improve fatigue. Given that, patient-reported outcome instruments are now commonly included in these trials in order to provide a comprehensive assessment of the impact of the investigational drugs on patients and their experience.”
For 2 years, Younossi and colleagues followed 1,679 patients with biopsy-confirmed NASH, of whom 802 had bridging fibrosis (F3) and 877 had compensated cirrhosis (F4). Fatigue was quantified at baseline with the seven-point Chronic Liver Disease Questionnaire (CLDQ)- NASH fatigue domain, in which lower scores indicate worse fatigue. Time to liver-related clinical events, such as progression to histologic cirrhosis or hepatic decompensation in F3 or F4, was assessed with Cox proportional hazard model.
At a median follow-up of 16 months, investigators observed 15% (n = 123) of NASH F3 patients experienced liver-related events, mostly in progression to histologic cirrhosis, and 3.5% (n = 31) of NASH F4 patients experienced hepatic decompensation. Among F3 patients, the mean baseline CLDQ-NASH fatigue score was 4.77, with those who experienced liver-related events reporting lower baseline scores of 4.47 compared with 4.83. Among patients with F4, the mean fatigue score was 4.56, and in those who decompensated, the scores at follow-up were 3.74 compared with 4.59.
After adjusting for confounders, researchers observed a significant correlation between lower fatigue scores and risk for liver-related or decompensation events (adjusted HR = 0.85; 95% CI, 0.74-0.97, per 1 point in fatigue score in F3; aHR = 0.62; 95% CI, 0.48-0.81 in F4).
“This suggests that, in addition to commonly used clinical parameters, presence of clinically significant fatigue can identify NASH patients at risk for adverse events,” the authors wrote. “Since fatigue also negatively impacts patients [health-related quality of life] and work productivity, it adds to the disease burden related to NASH. Given the critical importance of fatigue in NASH, clinical trials of regimens for NASH should not only show improvement of surrogates of clinical endpoints, such as the stage of fibrosis or resolution of NASH, but also improvement in patient-reported endpoints, such as fatigue.”
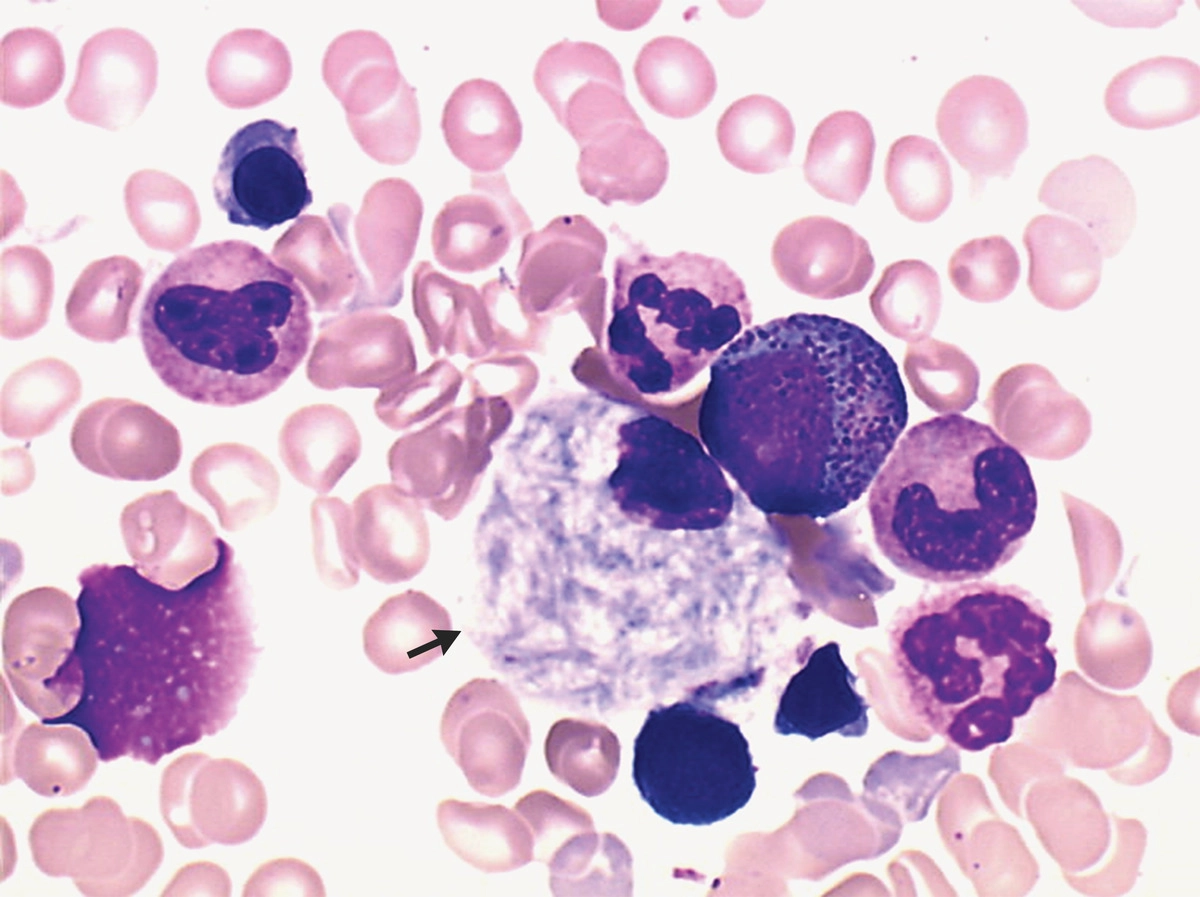
A 73-year-old man presented to the emergency department with a 1-month history of fatigue and diffuse bone pain. He reported no abdominal pain or neurologic symptoms. On physical examination, there was no hepatosplenomegaly. Laboratory studies showed a white-cell count of 1700 per cubic millimeter (reference range, 4000 to 10,000), a hemoglobin level of 5.9 g per deciliter (reference range, 12 to 18), and a platelet count of 111,000 per cubic millimeter (reference range, 120,000 to 180,000). Whole-body magnetic resonance imaging revealed osteonecrosis of the right humerus and right femur. Bone marrow biopsy revealed macrophages with a “wrinkled tissue paper” appearance in the cytoplasm (arrow, May–Grünwald Giemsa staining), a finding consistent with Gaucher’s cells. Further testing identified reduced β-glucocerebrosidase activity and homozygosity with the N370S variant of the GBA gene. Workup for hematologic cancers was negative. A diagnosis of type 1 Gaucher’s disease was made. Gaucher’s disease is an autosomal recessive disease that results in a deficiency of the lysosomal enzyme β-glucocerebrosidase. In type 1 Gaucher’s disease, some patients do not present with symptoms until late adulthood. Clinical features include fatigue, hepatosplenomegaly, pancytopenia, bone pain, osteonecrosis, and — in children — growth retardation. The patient began receiving enzyme-replacement therapy. At 6 months of follow-up, his symptoms had abated and cell counts had improved.
Adults with diabetes experience more fatigue compared with those without diabetes, with diabetic neuropathy being the primary driver for increased fatigue, according to a speaker.
In findings from a study presented at the AACE Annual Scientific and Clinical Conference, researchers used the Norfolk Quality of Life (QOL) – Fatigue tool to measure the cognitive, physical and emotional aspects of fatigue of people with diabetes compared with healthy controls without diabetes.
Adults with diabetes and neuropathy experience significantly more fatigue than those with diabetes and no neuropathy and people without diabetes. Data were derived from Casellini CM, et al. Utilizing a quality of life tool to examine the presence of fatigue in subjects with diabetes mellitus. Presented at: American Association of Clinical Endocrinology Annual Scientific and Clinical Conference; May 12-14, 2022; San Diego.
“We think the Norfolk QOL – Fatigue questionnaire has the potential to identify the impact of chronic diseases such as diabetes and neuropathy on the development of different components of fatigue,” Carolina M. Casellini, MD, assistant professor at the Strelitz Diabetes Center at Eastern Virginia Medical School in Norfolk, Virginia, said during a presentation. “Assessing the different components is especially relevant to clinicians caring for subjects with diabetes as fatigue can interfere with numerous factors affecting diabetes control and diabetes outcomes.”
Casellini and colleagues conducted a cross-sectional survey of adults aged 18 to 79 years living in the Hampton Roads, Virginia, region from 2018 to 2022. Participants included 400 adults with type 1 or type 2 diabetes and 140 healthy controls without diabetes. The Norfolk QOL – Fatigue tool was conducted in-person at the Strelitz Diabetes Center before the COVID-19 pandemic and virtually after the pandemic started. The questionnaire includes 35 items in five domains: subjective fatigue; physical and cognitive problems; depression; reduced activities; and activities of daily living. Respondents scored each item on a scale of zero to four, with a higher score indicating greater fatigue. Demographics including height, weight, BMI, waist circumference and duration of diabetes were self-reported. Participants with diabetes also completed the Norfolk QOL – Diabetic Neuropathy questionnaire to assess the impact of neuropathy on fatigue.
The diabetes group had a higher overall fatigue score in the questionnaire compared with the control group (mean score, 52.83 vs. 29.11; P < .0001) as well as higher scores in all five domains of the fatigue questionnaire. Of those with diabetes, 311 had neuropathy and 89 did not have neuropathy. Participants with diabetes and neuropathy had a higher overall fatigue score (mean score, 59.72 vs. 27.83; P < .0001) and a higher score in all five individual domains compared with those with diabetes and no presence of neuropathy.
Within the control group, women had a higher fatigue score than men. However, no differences between men and women were observed within the diabetes cohort. There were no differences in fatigue score between racial-ethnic groups.
When evaluating other demographics, younger participants were more likely to have a worse fatigue score compared with older adults. No associations were observed for weight, BMI or duration of diabetes.
“There are several theories around this,” Casellini said of the association between higher fatigue and younger adults. “Fatigue symptoms may be perceived as less severe by individuals who experience them for a longer time, and there may be potential generational differences in everyday responsibilities and life stressors.”
Casellini said more studies are needed to assess fatigue in cohorts with other comorbidities and to evaluate the utility of the tool against other tools for evaluating fatigue.
“Although generally considered asymptomatic, almost half of patients with NASH have clinically significant fatigue which, in turn, has a profound negative impact on the overall patient experience,” Zobair M. Younossi, MD,MPH, president of Inova Medicine Services and professor and chairman of the department of medicine at Inova Fairfax Medical Campus in Virginia, and colleagues wrote in Clinical Gastroenterology and Hepatology. “In this context, ongoing clinical trials aim at finding a drug-based therapy for NASH that may reverse fibrosis and could also potentially improve fatigue. Given that, patient-reported outcome instruments are now commonly included in these trials in order to provide a comprehensive assessment of the impact of the investigational drugs on patients and their experience.”
For 2 years, Younossi and colleagues followed 1,679 patients with biopsy-confirmed NASH, of whom 802 had bridging fibrosis (F3) and 877 had compensated cirrhosis (F4). Fatigue was quantified at baseline with the seven-point Chronic Liver Disease Questionnaire (CLDQ)- NASH fatigue domain, in which lower scores indicate worse fatigue. Time to liver-related clinical events, such as progression to histologic cirrhosis or hepatic decompensation in F3 or F4, was assessed with Cox proportional hazard model.
At a median follow-up of 16 months, investigators observed 15% (n = 123) of NASH F3 patients experienced liver-related events, mostly in progression to histologic cirrhosis, and 3.5% (n = 31) of NASH F4 patients experienced hepatic decompensation. Among F3 patients, the mean baseline CLDQ-NASH fatigue score was 4.77, with those who experienced liver-related events reporting lower baseline scores of 4.47 compared with 4.83. Among patients with F4, the mean fatigue score was 4.56, and in those who decompensated, the scores at follow-up were 3.74 compared with 4.59.
After adjusting for confounders, researchers observed a significant correlation between lower fatigue scores and risk for liver-related or decompensation events (adjusted HR = 0.85; 95% CI, 0.74-0.97, per 1 point in fatigue score in F3; aHR = 0.62; 95% CI, 0.48-0.81 in F4).
“This suggests that, in addition to commonly used clinical parameters, presence of clinically significant fatigue can identify NASH patients at risk for adverse events,” the authors wrote. “Since fatigue also negatively impacts patients [health-related quality of life] and work productivity, it adds to the disease burden related to NASH. Given the critical importance of fatigue in NASH, clinical trials of regimens for NASH should not only show improvement of surrogates of clinical endpoints, such as the stage of fibrosis or resolution of NASH, but also improvement in patient-reported endpoints, such as fatigue.”
There is tired, and there is fatigue. Then there is fatigue associated with a rheumatic or autoimmune disease, which is multifactorial and debilitating and has confounded physicians and patients for decades.
“Time and again, I hear my patients say that at some point in the day, they hit the wall, or they feel like they are in quicksand,” Philip J. Mease, MD, of the Swedish Medical Center in Seattle and the University of Washington, told Healio Rheumatology. “They have to stop and rest because they simply cannot function at all, period. It is a bone-crushing weariness.”
It would follow that such a pervasive and significant problem should be addressed routinely in the clinic, if not in research. But data have consistently shown that patients still feel as though their fatigue is not acknowledged sufficiently by their rheumatologist. Or, worse, many patients feel as though their fatigue is ignored or not taken seriously.
One issue is the source. “The reality is that lots of things probably drive fatigue in rheumatic diseases,” Katie Druce, PhD, MSc, BSc, of the Centre for Epidemiology Versus Arthritis at the University of Manchester in the U.K., said in an interview. “There may be differences in the things that initially cause the fatigue — such as inflammation through sickness behavior — and the things that perpetuate it, such as chronic pain and low mood.”
With so many potential etiologies, treating or even managing this comorbidity can be difficult. This could partially explain why patients have felt like their physicians have been unable or unwilling to tackle the problem for so long.
Biologic therapies have helped, regularly demonstrating the capacity to mitigate fatigue to a certain extent. But getting cytokines in order is only part of a successful management regimen. A growing body of data is showing that exercise and wellness behaviors like mindfulness and meditation can improve associated factors such as sleep, pain, anxiety and depression.
However, understanding that wellness can help and actually putting such a regimen into action are two different things, according to Patricia Katz, PhD, professor of medicine and health policy at the University of California, San Francisco. “You can’t just tell a patient they should exercise,” she said. “They need a specific exercise prescription that is tailored to their needs, and that is just not part of training for most rheumatologists.”
Exercise and wellness paradigms are, in fact, evolving. Accordingly, rheumatologists have grown more comfortable discussing them as potential mitigators of fatigue.
In addition, COVID-19 put a spotlight on how mental health comorbidities can induce that ‘bone-crushing’ weariness. When the effectiveness of biologics is factored into the equation, it is possible that patients with rheumatic diseases may finally have hope that the disease comorbidity that is so important to them may be addressed in a meaningful and structured way.
But considerable work needs to be done to iron out the details. It starts with simply understanding why fatigue happens in the first place.
Although exercise routines adopting wellness behaviors can help mitigate the effects of fatigue, implementing these routines among patients is another animal altogether. “You can’t just tell a patient they should exercise,” Patricia Katz, PhD, told Healio Rheumatology. “They need a specific exercise prescription that is tailored to their needs, and that is just not part of training for most rheumatologists.”
Source: University of California, San Francisco.
Down to the Roots
Philip J. Mease
While Mease would not claim to fully understand fatigue as it pertains to the specialty, he offered a starting point for rheumatologists to consider. “I often acknowledge to my patients that having a rheumatic disease is like having a full-time job,” he said, noting the endless stream of doctor visits, medication or injection schedules, lab tests and imaging analyses that can keep patients away from their work, family and support systems. All of this, of course, sits on top of and exacerbates the routine stresses of life.
But it takes more than simply acknowledging fatigue to understand it, according to Leonard H. Calabrese, DO, director of the RJ Fasenmyer Center for Clinical Immunology at the Cleveland Clinic. He offered a reason why so many rheumatologists are loath to even open the dialogue. “We as rheumatologists are so well trained to identify, sort out and treat chief complaints in our patients,” he said. “But we are not nearly as good at evaluating a patient’s chief concerns.”
Desiree Azizoddin, PsyD, of the research faculty in the department of emergency medicine at Brigham and Women’s Hospital and clinical instructor at Harvard Medical School, urged rheumatologists to keep it simple. “Sleep is a big one,” she said. “Patients need to understand sleep hygiene, and that too much sleep or too little sleep can be a signal or a cause of fatigue.”
Azizoddin, who has conducted research in systemic lupus erythematosus, also highlighted stress as a critical component of fatigue. But this is where the etiologic challenges arise. The impact of stress on individuals without a chronic rheumatic disease can be difficult enough to parse out. When a condition like SLE is involved, it can be nearly impossible to understand where the stress of life ends and the stresses associated with the disease begin.
“There are neurological manifestations of lupus disease that can lead to psychiatric disorders and fatigue,” Azizoddin added. “However, they may be underlying conditions, or they may be completely unrelated or they may be genetically driven. Lupus can lead to depression and anxiety, but many patients may have had depression and anxiety before their lupus diagnosis.”
Turning to more clinical explanations, Mease noted that excessive proinflammatory cytokines in the central nervous system can affect various parts of the brain that may be related to the experience of fatigue. He said that TNF may be implicated, along with interleukin-1, IL-17 and IL-23.
Katie Druce
Understanding the exact nature and impact of these cytokines has proven challenging, according to Druce. “We consistently see that symptoms like pain, mood and disability are important, while the relationship with inflammation and disease activity can be less clear,” she said.
Further complicating the picture is that there may be “important subtypes” of fatigue within any disease group, according to Druce. “These subtypes may highlight differing symptom etiologies,” she said. “Some patients have high levels of inflammation but good mental health, while others have high inflammation and poor mental health. While we might be comfortable recommending only immunomodulation for the first group, we might want to try a hybrid immunomodulation and cognitive behavior therapy approach in the second.”
Katz added another layer to the problem. “When a patient has high disease activity, getting that activity under control is always the first target,” she said. Treatment to the target of controlled disease with disease-modifying antirheumatic drugs and, to a greater extent, biologic therapies, often yields benefits in fatigue, as well.
But patients with severe disease are not the only ones who are chronically fatigued. “The harder nut to crack is people who have their disease under control but still experience fatigue that affects their daily lives,” Katz said.
Desiree Azizoddin
“Fatigue does not always correlate with disease activity,” Azizoddin added.
Conventional wisdom would suggest that understanding the root causes of a comorbidity is a good place to start. After that, having a number of tools at hand to assess it would be the next step. Such tools proliferate, along with data investigating their utility, but making sense of that information has also proven challenging.
Missing the Mark
In 2019, Barbacki and colleagues conducted a database review in the Journal of Rheumatology outlining the instruments used to assess fatigue in SLE since 2007, which yielded 37 studies using eight different measures of fatigue. Results showed that the visual analog scale (VAS), Fatigue Severity Scale (FSS) and Functional Assessment of Chronic Illness Therapy – Fatigue (FACIT) fatigue scale were most frequent. Two studies used the Multidimensional Assessment of Fatigue, while one used the Brief Fatigue Index (BFI).
“The FACIT score is a multidimensional questionnaire that gets at different qualities or aspects of fatigue,” Mease said. “It respects the fact that it is not a single item.”
In a paper published in Rheumatology Advances in Practice, Pearson and colleagues conducted a review of published articles to determine the quality and acceptability of PRO measures used to evaluate fatigue in axial spondyloarthritis. While 23 articles yielded evidence for nine fatigue-specific measures, they were unable to identify a fatigue measure specifically targeting the axial spondyloarthritis patient population. “Most measures provide a limited reflection of fatigue,” they wrote.
That said, the Multi-dimensional Assessment of Fatigue, Multi-dimensional Fatigue Inventory-20, FACIT and FSS were the “most comprehensive,” according to their findings. “The limited content and often poor quality of the reviewed measures limit any clear recommendation for fatigue assessment in this population,” they wrote.
Leonard H. Calabrese
Calabrese noted that the Cleveland Clinic uses the Patient-Reported Outcomes Measurement Information System (PROMIS) global fatigue score. “At a glance, I can see how severe fatigue is, and how much interference it is causing,” he said.
Katz acknowledged the utility of many of these parameters. However, she brought it back to basics. “If you are in a clinical setting, the best thing you can do is ask about fatigue,” she said.
A companion point is that as long as a rheumatologist is, in fact, addressing fatigue with their patients, any of these measures could have utility. “It depends on how you want to use it and what you are trying to achieve,” Katz said.
It is also important to understand the difference between measures used in a clinical setting and those used for research, according to Katz. “I understand that doctors have a small amount of time to discuss fatigue, so a simple rating scale, tracked over time from visit to visit, can be effective in learning whether a patient is feeling more or less fatigue,” she said. “In a research setting, we can use a longer questionnaire that has more precision. We can hit our targets a little better and hopefully extrapolate that information to the clinic.”
Rheumatologists have been hitting their targets with greater frequency in recent years, thanks to an evolving therapeutic armamentarium. But truly life-altering improvements in fatigue have continued to be elusive.
Treating to Target
“It is important to give credit where it is due by saying that rheumatologists were, rightly, for a very long time focused on targeting the aspects of rheumatic diseases which were most destructive, such as joint erosions, or most likely to lead to mortality,” Druce said. “It is only now that biologics, biosimilars and treat-to-target paradigms have revolutionized the impact and progression of many rheumatic diseases that there is space to consider some of the previously less urgent symptoms experienced by patients, like fatigue.”
Mease has hope for the capacity of biologics and other DMARDs to play a key role in helping patients combat their fatigue. “We are starting to see that fatigue may even improve before pain relief comes or joint swelling improves,” he said. “We know there is likely a centrally acting mechanism by which various drugs will do this. It is one of the things we are very interested in, how the drugs we use may impact central nervous system function.”
That said, it is still unclear how those mechanisms work. In the meantime, it is important for rheumatologists to manage expectations, according to Mease. “When I speak to patients about reaching targets for improvement in any clinical domain, including fatigue, I tell them that if we get 50% or 70% improvement, we have accomplished something,” he said.
While it can be difficult, Mease also tries to impress upon his patients the limits of therapeutic interventions. “We may not be able to remove the stress from your work or your family, but we can improve inflammation or certain parameters of immune-mediated fatigue,” he said.
If there is one other reason for optimism in hitting fatigue-based targets, it is that the FDA is finally beginning to recognize this comorbidity as a relevant entity, according to Mease. “Over the years, even though fatigue is always measured in trials, it did not make it to the label of our drugs,” he said. “This resistance was not bullheadedness on the part of the FDA; they were not ignoring the phenomenon. They wanted to be careful and note that fatigue can be present for many reasons.”
That changed recently when treatment of fatigue was added as a component to the label of guselkumab (Tremfya, Janssen). Several other drugs are applying to include fatigue on their labels, as well. This may allow clinicians to address the subject in a more structured way and induce a broader conversation about multipronged efforts to deal with fatigue. All of this may help achieve a goal that is so important to patients: breaking the cycle of disease activity, pain, depression and exhaustion that can lead to the most significant fatigue.
Breaking the Cycles
In a review published in Current Opinions in Rheumatology, Katz noted that while disease activity such as inflammation, pain and joint symptoms can yield greater fatigue in patients, this type of disease activity only accounts for “a small portion” of what patients actually feel.
“Instead, factors outside the direct effects of rheumatoid arthritis, such as obesity, physical inactivity, sleep disturbance and depression explain the majority of variation in fatigue,” she wrote.
A growing body of data is validating this conclusion. In a paper published in Lupus, Azizoddin and colleagues reported on a cohort of 116 patients with SLE. Multivariate analysis and stepwise regression analysis results showed significant and independent effects of depression, stress and pain on fatigue.
“Investigators are shooting themselves in the foot when including fatigue as an outcome but not including stress and depression in their models,” Azizoddin said. “We know they are related. This is why fatigue continues to be unsolved.”
In a paper published in the Pakistan Journal of Medical Sciences, Fertelli and colleagues investigated associations between fatigue and sleep quality, pain and depression in 151 patients with knee osteoarthritis and 147 healthy controls. Results showed that the knee OA group showed significantly higher fatigue scores and higher Pittsburgh Sleep Quality Index (PSQI) and Beck Depression Inventory (BDI) total scores compared with controls (P < .05). Moreover, a positive correlation was observed for fatigue score and PSQI, VAS and BDI scores (P < .05). “This fatigue suffered by them affected their sleep quality, pain and depression negatively,” the researchers concluded.
“Fatigue and depression are intertwined so closely that, sometimes, it may be difficult to disentangle them,” Katz said. “The descriptions are pretty similar across diseases.”
Azizoddin believes that rheumatologists can play a critical role in mitigating the synergistic effects of these disease comorbidities. “What physicians say carries weight,” she said. “So, when a physician says, ‘Your sleep and your stress are going to impact your disease and cause you to have more fatigue,’ they are inclined to listen.”
At that point, the physician may have more leverage in motivating the patient to engage in some sort of self-management regimen, whether it is exercise, meditation or a dedicated sleep hygiene routine.
Azizoddin added: “It can be helpful to remind patients that they can and should practice stress-relieving behavioral techniques, such as relaxation, breathing, yoga, and exercise, that can make a big difference.”
Get Well Soon
It does not take a physician with years of training and experience to understand that exercise is beneficial for healthy individuals and those with chronic diseases alike. Nor is it a significant logical leap to assume that wellness behaviors such as meditation or mindfulness can help with the stress, depression or anxiety that come with a chronic disease and may be driving fatigue.
The issue, for many rheumatologists, is that understanding these basic principles of general health and actually prescribing programs to target the specific fatigue experienced by an individual patient are two different animals altogether. In a paper published in Rheumatic and Musculoskeletal Diseases Open, Pope wrote that “specific programs for exercise and behavioral interventions are not standardized.”
But attempts are being made to figure out how to design such interventions to target fatigue.
Sveaas and colleagues wrote a paper in Physical Therapy investigating exercise as a treatment for axSpA. They noted that most programs for this patient population target flexibility rather than high-intensity exercise.
The study included 50 patients assigned a 3-month high-intensity exercise regimen and 50 controls. Results showed that 38 participants in the exercise group followed at least 80% of the program. Initial results showed a significant benefit of exercise on fatigue (mean group differences = –0.4; 95% CI, –0.7 – –0.1), vitality (5.0; 95% CI, 1.1-10.5), mood (–2; 95% CI, –3.7 – –0.04) and general health (9.0; 95% CI, 3.3-14.7).
“When we have completed needs assessments among rheumatologists and patients, we see that rheumatologists are very interested in wellness interventions,” Calabrese said. “The issue is that they do not have the time, expertise or confidence to engage with this kind of therapy.”
Calabrese added that many DOs and MDs are loath to refer their patients to “alternative therapies,” for fear that they may default on immune-based treatment. “We believe that wellness behavioral modification must complement targeted and aggressive therapy,” he said. “We believe it can provide an empowering message to improve not only self-efficacy among patients, but, ultimately, medication adherence.”
This message is starting to gain validation. Further conclusions from the Katz paper showed that the most effective approaches to reducing RA fatigue appear to be behavioral — such as increasing physical activity — or cognitive — such as cognitive behavioral interventions.
Katz suggested that the simple approach may be the best approach. “People just need to move more and sit less,” she said.
Until the mechanism of fatigue is completely understood — and, admittedly, it is entirely possible that it will never be understood — Calabrese encouraged rheumatologists to continue to talk to their patients about it. If they lack the confidence or know-how to follow-up on a wellness regimen, he noted that a wealth of materials is available online, including from the Cleveland Clinic.
But Calabrese believes that the current moment is a “new era in wellness,” with robust data being reported in “high impact” publications. This is not to mention the notion that COVID-19 “taught us that wellness behavior is critical to survival,” he said. “This is all incredibly validating for those of us who have been interested in fatigue for a long time.”
References:
Azizoddin DR, et al. Lupus. 2019;doi:10.1177/0961203318817826.
Barbacki A, et al. J Rheumatol. 2019;doi:10.3899/jrheum.180831.
Fertelli TK, et al. Pak J Med Sci. 2019;doi:10.12669/pjms.35.4.383.
The severity of fatigue that comes with Lyme and other tick-borne illnesses can be difficult to describe because Lyme disease fatigue is a whole different story
When I was sick with COVID-19 in 2020, I continued working (remotely) despite my mild fatigue, shortness of breath, low-grade fever, loss of taste and smell, and persistent cough. Though these symptoms were no walk in the park, they weren’t completely debilitating. For some COVID-19 patients, symptoms have rendered them bedridden, hospitalized, or worse. I was lucky not only to survive early COVID-19, but to have a moderate case.
For me, the fatigue of COVID-19 was nothing compared to the fatigue of Lyme disease. Lyme disease fatigue has become the barometer by which I measure all other fatigue, whether it’s general tiredness or illness-related. The severity of fatigue that comes with Lyme and other tick-borne illnesses can be difficult to describe, because fatigue can be defined many ways. It can mean muscle soreness after a workout, burnout after a long week, or yawns that come when you just didn’t sleep well. Fatigue can also mean general malaise from the pandemic, or sleepiness from any number of stressors. Then there’s feeling like your head is spinning after staying up all night finishing an assignment or tending to a crying baby.
All of these types of fatigue are uncomfortable. No one likes to be tired. But this level of fatigue generally can be solved with a few good nights of rest, a break, or even some caffeine. That’s because the fatigue is caused by external factors, not by illness. Your body has the resources to recover.
Lyme disease fatigue, like the fatigue that comes with many other serious illnesses, is another story. In a survey of over 3,000 chronic Lyme disease patients conducted by lymedisease.org, 59% of patients described their fatigue as “severe” or “very severe.” At my lowest point of illness—which lasted years—that severity meant I was almost completely bedridden. I could walk around my house and go out for a few errands on good days, but sometimes it was too tiring to walk to the mailbox, or to sit up at the dinner table. My body screamed with exhaustion. It felt heavy, as if I was weighted to the bed, and all I wanted to do was sleep. And sleep. And sleep.
The problem was, I could not actually rest. Overrun with Lyme disease bacteria as well as babesiosis, ehrlichiosis, and possible bartonella, my nervous system could not turn off. At one point, I was literally awake for weeks. And while sleep medication, neurofeedback, and cognitive behavioral therapy did help me fall asleep, it took months to catch up on rest. In addition to recovering from severe sleep deprivation, my body was also busy fighting infections. I also had chronic active Epstein-Barr virus, which meant that the shackling fatigue I experienced when I had acute mononucleosis held on during my worst years of tick-borne illness.
My body was so worn out from doing battle that when I did sleep, I often dreamed about how tired I was. I’d be lying in the middle of my college campus too exhausted to get up, or I’d collapse on a ski run while others zoomed past me. In these dreams I craved sleep as desperately as I did when I was awake. In my waking hours, I suffered from brain fog and other neurological complications. I felt like I had skied all day, partied all night, written an entire thesis, and then gotten the flu. For years.
For many Lyme disease patients, fatigue persists during and after treatment, but the good news is that it does get better. Years after feeling shackled to my bed, I am now out living a normal life. I work. I write. I exercise. I socialize. I still keep a strict sleep schedule, and I nap every afternoon. This rest allows me to maintain my restored health, so that hopefully, I will never feel the unbearable fatigue of Lyme disease again.