Abstract
Objective To determine the harms of ezetimibe in people who need lipid-lowering treatment.
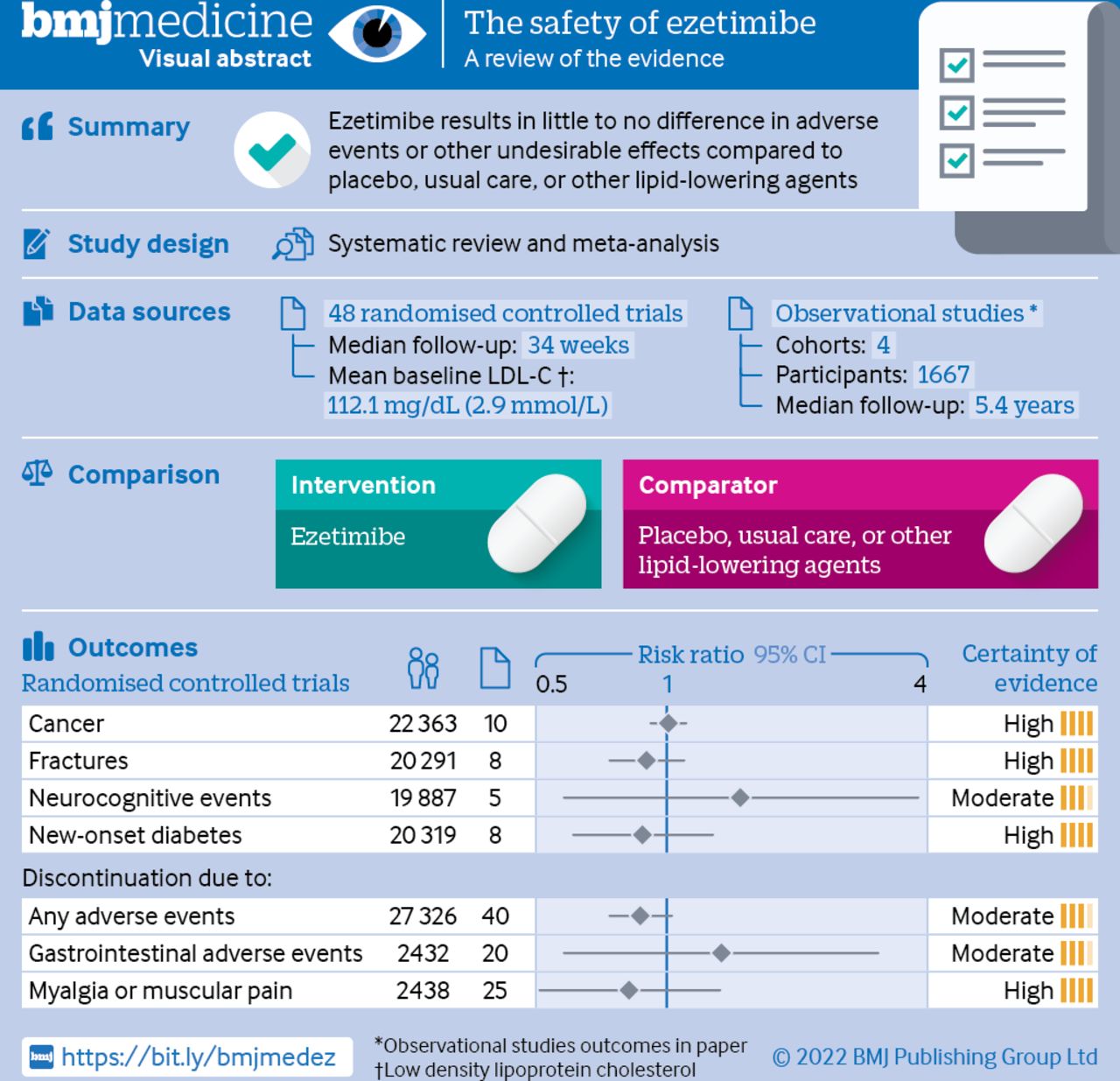
Design Systematic review and meta-analysis.
Data sources Randomised controlled trials and cohort studies.
Eligibility criteria for selecting studies Studies comparing ezetimibe with placebo, standard care, or other lipid-lowering agents in people who need lipid-lowering treatment with a follow-up duration of at least six months (or 24 weeks). The relative effects for potential harms of ezetimibe were pooled by use of random effect pairwise meta-analyses for randomised controlled trials and the evidence from observational studies was narratively summarised. The certainty of evidence was assessed using the Grading of Recommendation Assessment, Development, and Evaluation.
Results 48 randomised controlled trials with 28 444 participants (median follow-up 34 weeks, range 24-312 weeks) and four observational studies with 1667 participants (median follow-up 282 weeks, range 72-400 weeks) were included. The meta-analyses of randomised trials showed moderate to high certainty that ezetimibe was not associated with cancer (relative risk 1.01; 95% confidence interval 0.92 to 1.11), fractures (0.90; 0.74 to 1.10), discontinuation due to any adverse event (0.87; 0.74 to 1.03), gastrointestinal adverse events leading to discontinuation (1.34; 0.58 to 3.08), myalgia or muscular pain leading to discontinuation (0.82; 0.51 to 1.33), neurocognitive events (1.48; 0.58 to 3.81), or new-onset diabetes (0.88; 0.61 to 1.28). The narrative analysis of observational studies provided consistent findings. No credible subgroup effects were identified for the harm outcomes, including shorter versus longer follow-up duration of trials.
Conclusions Ezetimibe results in little to no difference in adverse events or other undesirable effects compared with placebo, usual care or other lipid-lowering agents.
Review registration PROSPERO CRD42020187437.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
http://creativecommons.org/licenses/by-nc/4.0/
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
http://dx.doi.org/10.1136/bmjmed-2022-000134
Statistics from Altmetric.com
1 readers on Mendeley
Request Permissions
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
What is already known on this topic
- Ezetimibe lowers low density lipoprotein cholesterol and reduces cardiovascular risks by blocking the gastrointestinal absorption of dietary cholesterol
- Although ezetimibe is generally safe, there are concerns about its potential harms including cancer, neurocognitive events, fractures, gastrointestinal adverse events, myalgia, muscular pain, and new-onset diabetes
What this study adds
- Adding ezetimibe results in little to no difference in adverse events or other undesirable effects in people who need lipid-lowering treatment
How this study might affect research, practice, or policy
- When deciding to add ezetimibe to statins for lipid-lowering treatment, clinicians can have confidence in the evidence that adverse events are rare
Introduction
Cardiovascular disease is one of the leading causes of death and disability worldwide.1–3 Statins are first line cholesterol-lowering drugs for the reduction of cardiovascular risk but can cause adverse effects such as myalgia, muscular pain, and new-onset diabetes.4 5 Ezetimibe, an oral cholesterol-lowering drug taken after statins, which inhibits intestinal cholesterol absorption and decreases biliary cholesterol secretion, lowers low density lipoprotein cholesterol (LDL-C) by 20%.6–9 Clinical trials and systematic reviews have established that ezetimibe can reduce cardiovascular events.10–13 Guidelines from the European Society of Cardiology14 and American Heart Association15 recommend ezetimibe as a second lipid-lowering drug in addition to treatment with statins when LDL-C treatment goals are not met, or as a single drug in case of statin-intolerance. The number of prescriptions of ezetimibe doubled in North America from 2003 to 2006 for the primary and secondary prevention of cardiovascular diseases.16
Although ezetimibe is well tolerated in clinical practice, some studies suggest concerns regarding potential harms such as cancer, neurocognitive events, fractures, gastrointestinal adverse events, myalgia, muscular pain, and new-onset diabetes.4 17–22 The cause and magnitude of adverse events or undesirable effects of ezetimibe remain unclear. Therefore, we conducted a pairwise systematic review and meta-analysis of randomised controlled trials and observational studies to evaluate the safety of ezetimibe in people who need lipid-lowering treatment. This systematic review quantitatively informed the potential harms of ezetimibe for a parallel clinical practice guideline with risk-stratified recommendations for ezetimibe and PCSK9 inhibitors.23 This guideline forms part of a BMJ Rapid Recommendation and is a collaborative effort by the MAGIC Evidence Ecosystem Foundation (https://magicevidence.org) and The BMJ (box 1).24 For the visual abstract of this paper, see figure 1.
Box 1
Linked articles in this BMJ Rapid Recommendations cluster
- Hao Q, Aertgeerts B, Guyatt G, et al. PCSK9 inhibitors and ezetimibe for the reduction of cardiovascular events: a clinical practice guideline with risk-stratified recommendations. BMJ 2022;377:e069066, doi:10.1136/bmj-2021-069066
- Summary of the results from the Rapid Recommendation process
- Khan SU, Yedlapati SH, Lone AN, et al. Anti-PCSK9 agents and ezetimibe for cardiovascular risk reduction: a systematic review and network meta-analysis. BMJ 2022;377:e069116, doi:10.1136/bmj-2021-069116
- Review and network meta-analysis of all available randomised trials that assessed effects of PCSK9 inhibitors and ezetimibe with or without statin therapy for cardiovascular risk reduction
- Harm reviews
- Wang Y, Zhan S, Du H, et al. Safety of ezetimibe in lipid-lowering treatment: systematic review and meta-analysis of randomised controlled trials and cohort studies. BMJ MED 2022;1. doi:10.1136/bmjmed-2022-000134
- Li J, Du H, Wang Y, et al. Safety of proprotein convertase subtilisin/kexin 9 inhibitors: a systematic review and meta-analysis. Heart 2022; doi:10.1136/heartjnl-2021-320556
- MAGICApp (https://app.magicapp.org)
- Expanded version of results with multi-layered recommendations, evidence summaries, and decision aids for use on all devices

Figure 1
Visual abstract
Methods
Study design
This systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (known as PRISMA) statement and the Meta-analysis of Observational Studies in Epidemiology (known as MOOSE) statement (checklists in online supplemental tables S1 and S2).25 26 We registered the protocol in PROSPERO (CRD42020187437).
Supplemental material
[bmjmed-2022-000134supp001.pdf]
Guideline panel and patient involvement
The BMJ Rapid Recommendation panel,24 including clinicians, methodologists, and patients provided critical oversight over the steps of this review. The panel included cardiologists, general practitioners, general internists, endocrinologists, a geriatrician, methodologists, and three patient partners. Patient partners received personal training and individual support in the methods used throughout the guideline development process. The panel assisted in framing the study question, defining the interventions and comparisons, prioritising outcome measures, and proposing subgroup analyses. Three patient partners were members of the guideline panel that contributed to this systematic review and the associated BMJ Rapid Recommendation.
Data sources
We searched Medline, EMBASE, and Cochrane Central Register of Controlled Trials (CENTRAL) from inception to July 2021. We also searched ClinicalTrials.gov for completed unpublished registered trials with results. The search strategy is shown in online supplemental tables S3 and S4.
Paired reviewers (YW and HD) searched the literature and selected studies through screening titles and abstracts. Potentially eligible papers were screened in full text. In case of conflict, a third reviewer (SL) arbitrated disagreement by discussion. We crosschecked the study inclusion with a previously published systematic review.13
We included randomised controlled trials and cohort studies that compared ezetimibe with placebo, standard care, or other lipid-lowering agents with at least six months (or 24 weeks) follow-up duration. We included studies explicitly reporting data for at least one outcome of interest, including cancer (any type), new-onset diabetes mellitus, neurocognitive events, fractures, myalgia or muscular pain leading to discontinuation, discontinuation due to gastrointestinal adverse events, or discontinuation due to any adverse effect. The longest follow-up duration or the largest population study was included when studies reported on the same or overlapping populations. Only studies published in English were included.
Data were collected in a predefined collection form incorporating study characteristics (eg, first author name, year of publication, study design, sample size, follow-up duration, prevention type, the intervention of control, and background treatment); baseline characteristics (eg, age, sex, body mass index, LDL-C, high density lipoprotein cholesterol, and triglycerides); intervention characteristics (eg, drug dose, treatment duration); and safety outcomes (eg, number of events and patients of each outcome) for randomised controlled trials. If a published trial did not report the outcome information, while the corresponding ClinicalTrials.gov reported relevant data, we collected data from the registry report. When the data in publication and ClinicalTrials.gov conflicted, we used the data from the publication. For observational studies, additional data were collected, including prospective or retrospective design, exposure, data source, and methods for comparability (that is, matching or adjusting for confounding variables). Adjusted effect estimates (that is, relative risks or odds ratios) and corresponding 95% confidence intervals were preferred to raw data of adverse events in observational studies. Paired reviewers (YW and HD) performed the data extraction and a third reviewer (SL) judged the discrepancies if any.
Paired reviewers (YW and HD) assessed the risk of bias for randomised controlled trials using the Cochrane Collaboration’s risk-of-bias assessment tool27 and that for observational studies with the modified Newcastle-Ottawa quality assessment scale.28 We added one item, which we named “other concerns” because some concerns could not be classified into any of the existing eight items in the scale. A third reviewer (SL) was involved in the discussion if any discrepancy occurred.
Statistical analysis
For the included randomised controlled trials, we pooled relative risks and their 95% confidence intervals using the random effects model for all meta-analyses. Statistical heterogeneity was assessed by χ2 and I2 tests with significance defined by χ2 P<0.1 or I2>50%. We used baseline risks for each outcome based on the pooled event rates of included control groups and calculated absolute effects for each outcome at both five years and two years. As a result of limited data reported and low certainty of evidence, we did not pool outcome data quantitatively in the analysis of observational studies but instead conducted a narrative summary of the included studies.
We analysed three subgroup analyses to explore the potentially hypothetical heterogeneity. Firstly, the follow-up duration (<48 v ≥48 weeks) in particular, potential affects of larger relative effects in studies with longer follow-up duration. Secondly, risk of bias (low v high risk), focusing on larger relative effects in studies with high risk. A high risk of bias is defined if at least two high risk items from the Cochrane Collaboration Risk of Bias Tool are noted. Finally, type of control (placebo or usual care v active agents) with larger relative effects in studies with placebo or usual care.
As recommended by reviewers, we exploratorily performed a meta-regression according to different baseline LDL-C concentrations. When the included number of non-zero-event trials surpassed 10, funnel plots, Begg’s rank correlations, and Egger’s linear regression were applied in evaluating publication bias. We used the fixed effects model to pool the data for each outcome as the sensitivity analysis. All data analyses were done using RStudio (R Pack Version 3.6.1).
To evaluate the certainty of evidence, we used the Grading of Recommendation Assessment, Development, and Evaluation (known as GRADE) framework29 and assessed the credibility of subgroup analyses based on the literature.30
Patient and public involvement
Three patient partners were involved in the design of this research.
Results
Included studies
Of 6881 citations of randomised controlled trials, we included 48 with a total of 28 444 participants (figure 2, table 1, and online supplemental tables S6 and S7).11 Follow-up durations ranged from 24 to 312 weeks (median 34 weeks). The mean age of participants was 62.6 years, 71.9% were male, the mean baseline LDL-C was 112.1 mg/dL (2.9 mmol/L), and the mean proportion of individuals using statins at admission was 39.6% (table 1). Of 25 multicentre trials, treatment regimens included ezetimibe in monotherapy (663 participants in 11 trials), ezetimibe plus statin (13 230 participants in 36 trials), and ezetimibe plus fibrate (340 participants in one trial).

Figure 2
PRISMA flow diagram
Table 1
Baseline characteristics of included trials
Of 3625 citations of observational studies, we included four cohort retrospective cohorts with 1667 participants in our narrative summary (figure 2, table 2, and online supplemental table S10).31–34 Follow-up durations ranged from 72 to 400 weeks (that is, 1.38-7.70 years; median 282 weeks (that is, 5.42 years)). The population from two studies were identified from electronic health records.32 34 The mean age of the participants was 59.5 years, 35.6% were male, the mean baseline LDL-C was 191.0 mg/dL (4.9 mmol/L), and 9.7% of participants were using statins at admission. Three studies compared ezetimibe plus statin versus statin alone, and one other compared ezetimibe versus colesevelam.
Table 2
Characteristics of the included observational studies
Risk of bias
We rated the overall risk of bias as low across all 48 included trials; 29 trials raised concerns (online supplemental file 1). We rated 14 (29%) studies as high risk of bias because the number of missing participants was higher than 20% or the analysis was not done by an intention-to-treat protocol. We rated 18 (38%) trials as high risk of bias owing to inadequate masking of participants and personnel, 14 (29%) trials owing to an open label design, and four (8%) trials because the trial design did not have a matching placebo. The overall scores of the Newcastle-Ottawa quality assessment scale were six to seven among the included observational studies, indicating some risks of bias (table 3; online supplemental table S11).
Table 3
Treatments, outcomes, and risk of bias of included observational studies
Meta-analyses of randomised controlled trials
As shown in figure 3, moderate to high certainty evidence indicated that ezetimibe has little to no effect on the risks of cancer (relative risk 1.01; 95% confidence interval 0.92 to 1.11), fractures (0.90; 0.74 to 1.10), discontinuation due to any adverse events (0.87; 0.74 to 1.03), discontinuation due to gastrointestinal adverse events (1.34; 0.58 to 3.08), myalgia or muscular pain leading to discontinuation (0.82; 0.51 to 1.33), neurocognitive events (1.48; 0.58 to 3.81), or new-onset diabetes (0.88; 0.61 to 1.28). We downgraded the certainty of the evidence to moderate for discontinuation due to any adverse events for indirectness because of the composite nature of the outcome. We also downgraded the certainty of evidence of discontinuation due to any gastrointestinal adverse events and neurodegenerative events for imprecision because of wide 95% confidence intervals, which could not support clinical decision making.

Figure 3
Summary of findings for relative and absolute risks of the safety outcomes of ezetimibe. Hollow squares in the certainty rating column represent six rating domains listed in order from left to right including risk of bias, inconsistency, indirectness, imprecision, publication bias, and other concerns. Black squares means that the certainty was downgraded because of that domain. CI=confidence interval
Subgroups and sensitivity analysis
None of the subgroup analyses identified potential subgroup effects in different trials with different follow-up durations, risk of bias, and type of control (online supplemental table S8 and figures S3–S5). For example, the cancer risk did not show heterogeneity across the subgroups of <48 weeks follow-up (relative risk 0.79; 95% confidence interval 0.21 to 3.01) and ≥48 weeks follow-up (1.01; 0.92 to 1.11) with the interaction P value being 0.72. The meta-regression did not identify any association between baseline LDL-C concentrations and outcomes (online supplemental table S13).
The sensitivity analyses supported the robustness of the pooled results using the fixed effects model (online supplemental figures S7–S19). Neither funnel plots nor Begg’s and Egger’s tests for the outcomes of cancer and discontinuation due to any adverse events did not identify signals of publication bias (online supplemental table S9).
Narrative summary of observational studies
Two retrospective studies31 32 suggested that ezetimibe was not associated with an increased risk of new-onset diabetes (adjusted odds ratio 1.01, 95% confidence interval 0.51 to 1.99; adjusted odds ratio via indirect comparison 1.24, 0.65 to 2.39) during the four to six year follow-up duration (table 3). Two studies reported no instances of myalgia or muscular pain during the follow-up duration.33 34 One study with 16 participants reported no cases of discontinuation due to any adverse events including gastrointestinal effects in a 10 month follow-up duration.34 We consider these findings to be very low certainty evidence due to high risk of bias (new-onset diabetes, myalgia or muscular pain leading to discontinuation, discontinuation due to any gastrointestinal adverse events and discontinuation due to any adverse events), indirectness (new-onset diabetes and discontinuation due to any adverse events) and imprecision (myalgia or muscular pain leading to discontinuation, discontinuation due to any gastrointestinal adverse events and discontinuation due to any adverse events).
Discussion
Main findings
Moderate to high certainty evidence shows that ezetimibe has little to no effect on adverse events (compared with no ezetimibe), including cancer, new-onset diabetes, neurocognitive events, fractures, myalgia or muscular pain leading to discontinuation, or discontinuation due to gastrointestinal adverse events or any adverse events.
Drugs that do not cause adverse events are rare in clinical practice.35 Unlike the pleiotropy of targets for other lipid-lowering drugs, ezetimibe lowers LDL-C concentration by blocking the Niemann-Pick C1 Like 1 (NPC1L1) protein, which inhibits intestinal cholesterol absorption, thus mimicking a low cholesterol diet.36 37 Ezetimibe does not directly interact with the lipid metabolism in the liver and other organs and is biologically safe, except for the potential harms of very low cholesterol intake, which remains open to debate.38
Compared with the previous studies
We identified six previous meta-analyses investigating the safety concerns of ezetimibe.39–44 Results for these studies were consistent with our findings, except that Zhao and colleagues44 significantly linked ezetimibe to increased neurocognitive events in their network meta-analysis (network odds ratio 3.94, 95% confidence interval 1.18 to 13.12).
Neurocognitive safety is one of the most important concerns followed by very low LDL-C concentrations.45 Nevertheless, the findings from our meta-analysis of randomised controlled trials did not show an effect of neurodegenerative events in people treated with ezetimibe, nor did the findings from the observational studies. Our study did not show an effect on cancer, a concern that was raised by the SEAS trial.22 We did not note an association with fractures or gastrointestinal effects, events that could be linked to the limited absorption of lipids in intestines.5 20 21 However, discontinuation due to any gastrointestinal adverse events and neurodegenerative events were downgraded to moderate certainty due to wide 95% confidence intervals. New evidence could change our confidence in these effects.46 47
Strengths and limitations
Our study systematically reviewed all ezetimibe trials and cohort studies from literature and ClinicalTrials.gov and engaged a multidisciplinary panel to contextualise our findings into clinical practice. The GRADE approach based on the absolute effects facilitates the application in clinical practice. In trials, we did not identify credible subgroup effects for any of the harm outcomes regarding different follow-up durations. With the support from observational studies with a median follow-up duration of up to 7.7 years, our study supports the long term safety of the drug. Nevertheless, long term surveillance remains necessary.
The key limitation of this study is that the number of some events (that is, gastrointestinal and neurocognitive events) is rare and therefore findings for these events could be imprecise.Unfortunately, the included observational studies to supplement the trial evidence overall provided very low certainty evidence and were not powered to improve precision for these or other harm outcomes. A large scale, population based study could be helpful in the future. However, such rare events might not alter clinical decision making because of the very low absolute baseline risk. The systematic review did not provide direct evidence for people with characteristics that were not represented by the study population (eg, low LDL-C concentration before treatment). People who might not be represented, therefore, should use when considering the direct evidence.
Conclusion
In this systematic review, moderate to high certainty evidence show that treatment with ezetimibe has little to no effect on adverse events compared with no ezetimibe. Nevertheless, the clinical practice warrants long term surveillance of rare events, especially in unrepresented populations from previous studies.
Source: BMJ

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}